TEMPOROMANDIBULAR JOINT
After reading this chapter the student will be able to:
• describe the structure of the temporomandibular joint, the condyles and the temporal fossa, the articulating disk, and the capsule
• discuss the function of the temporomandibular joint and the role of the masticatory muscles
OVERVIEW
This chapter discusses articulation between the condyles of the mandible and temporomandibular fossa of the temporal bone. The temporomandibular joint (TMJ) allows the mandibular condyles to move in both gliding and hinge actions. Therefore, instead of being a stationary hinge, the joint slides along the inclined plane while functioning also as a hinge joint. The complex motion of the joint can be observed during mastication. TMJ problems can be associated with pain in the related muscles of the jaws and neck.
The anatomy, histology, and function of the various structures related to jaw function are described in this chapter. The TMJ includes (1) the right and left condylar heads of the mandible, (2) the articulating surfaces of the mandibular condyles and the temporal fossae, (3) a disk that intervenes between the fossa and condyle, and (4) a capsule and supportive ligaments. The capsule enclosing this joint serves as a stabilizer, making complex function possible.
The fibrous articular disk divides the joint in two. The upper half is involved in sliding action, and the lower functions as a hinge action. The joint is supported anteriorly by a tendinous attachment of the capsule and the lateral pterygoid muscle, laterally by the lateral or temporomandibular ligament, medially by the sphenomandibular ligament, and posteriorly by the stylomandibular ligament. The TMJ functions as a ginglymoarthrodial joint, indicating that it moves as a sliding and hinge joint.
Myofascial pain dysfunction (MPD) is a syndrome that has received attention. It has been defined as a complex problem relating to neuromuscular concepts, occlusal concepts, muscle balance, tooth morphology, and guidance and psychophysiologic factors. Much remains to be learned about the normal and abnormal stomatognathic system.
 CLINICAL COMMENT
CLINICAL COMMENTSTRUCTURE
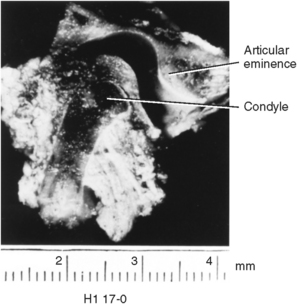
The right and left heads of the mandibular condyles articulate in the temporomandibular or glenoid fossae. At birth, the heads of the condyles are round and covered with a thick layer of cartilage. The cartilage front is uneven with spikes of cartilage projecting into the underlying marrow space. Bone forms around these spikes of cartilage, so the head of the condyle is porous (Fig. 13-1, A). During development, the condyle grows in a lateral direction, changing into an ovoid shape by maturity, which is attained at age 25 (Fig. 13-1, B). The oval condyle consists of a smooth, bony surface, which is covered with a layer of fibrous connective tissue in the adult. The cartilage serves as a growth site in the condyle.
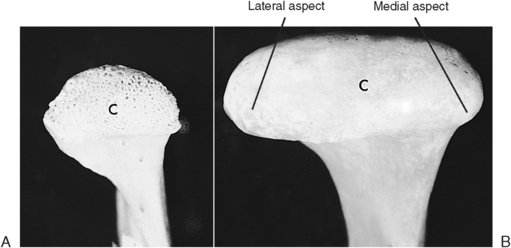
Fig. 13-1 A, Condyle (C) of a 6-year-old child. Perforations on surface are created by cartilage cap, which is missing because of tissue preparation. B, In the adult, smooth bony surface of condyle (C) illustrates lateral growth.
New cartilage cells arise from near the surface of the perichondrium, which covers the condyle. The cartilage cells grow and divide, and the cells deeper in the cartilage die as the cartilage that surrounds these cells calcifies (Fig. 13-2, A). The calcified cartilage is then replaced by bone from the underlying ramus (Fig. 13-2, B). This process continues during development with a gradual thinning of the cartilage layer, and at maturity the cartilage has been replaced by bone (Fig. 13-2, C).
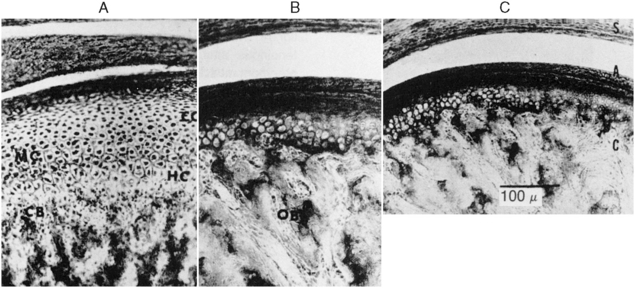
Fig. 13-2 Histology of condylar cartilage A, Showing the wide band of cartilage that appears during the postnatal period. EC, Reserve cartilage zone; HC, hypertrophy cartilage zone; MC, multiplication cartilage zone. B, Cartilage has thinned considerably. OB, Bone formation. C, Thin cartilage zone underlying the perichondrium in an 18-year-old patient.
The heads of the condyles and the heads of the long bones differ in that long bones form secondary ossification centers (Fig. 13-3). Secondary ossification centers produce cartilage-bone junctions termed epiphyseal lines, where the lengthening of long bone occurs. No epiphyseal line is formed in the condyles. The heads of the condyles, however, accomplish growth much like that of long bones. Differentiation of new cartilage cells first appears, then cartilage matrix around these cells develops, which is then replaced by bone. Another difference in long bones is that the cartilage cells are organized in long rows as they approach the bony junction, whereas in the condyles the chondroblasts are scattered. The chondroblasts go through similar changes of cell enlargement, cartilage matrix calcification, and bony replacement (see Fig. 13-3). This ability to modify the shape of the condyles through cartilage-bone remodeling allows adaptation to functional stress.
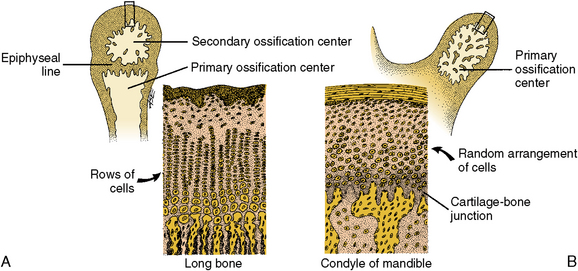
Fig. 13-3 Diagram comparing the head of a long bone and condyle. A, Cartilage of a long bone showing straight vertical rows of cartilage cells, young cells to maturing ones, top to bottom. Bone replaces cartilage at the junction of these two tissues. B, Random arrangement of cells in a condyle, which accomplishes same result as rows of cells. As in long bone, at the conclusion of this process in the condyle, bone replaces cartilage at the junction shown.
Temporomandibular Fossa
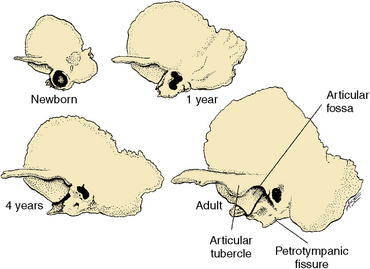
The fossa is composed of an anterior part in the form of an eminence and a posterior part, a depression or cavity on the inferior part of the temporal bone. This fossa is located at the posterior medial aspect of the zygomatic arch (Fig. 13-4). The anterior wall of the fossa is smooth and forms a tubercle in which the condyles slide during articulation. On the posterior wall of the fossa is the petrotympanic fissure. This is the junction of the temporal and parietal bones. Some authors report that the origin of elastic fibers, which insert into the posterior part of the disk, is on the posterior wall of this fissure. These elastic fibers may function in retraction of the disk. The temporomandibular fossa is where the condyles are positioned at rest (see Fig. 13-4).
Upper and Lower Compartments
The TMJ cavity is divided into upper and lower compartments by the articular disk (Fig. 13-5). The upper compartment is bound by the articular fossa above and by the disk below. The lateral, medial, and posterior boundaries are enclosed by the capsule that outlines the TMJ. The lower compartment is bound superiorly by the disk and inferiorly by the head of the disk. The two compartments differ in action.
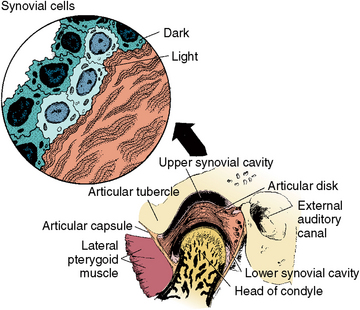
Fig. 13-5 Temporomandibular joint with a thin anterior and thicker posterior articular disk. Observe the position of the capsule anteriorly and posteriorly and the upper and lower synovial compartments in relation to the lateral pterygoid muscle and external auditory canal. The upper and lower compartments that are not under shearing or compressive forces are lined with synovial cells. In the upper diagram are examples of light and dark synovial cells, which function to lubricate movements of condyles.
In the upper compartment is a gliding action between the condylar head and the articular eminence, and in the lower compartment is a hinge action between the undersurface of the disk and the rotating surface of the head of the condyle (see Figs. 13-5 and 13-6).
Articular Disk
The articular disk is a dense, collagenous, fibrous pad between the condylar heads and the articular surfaces (see Figs. 13-5 and 13-6). When the jaw opens, each condylar head moves from the articular fossa and slides along the articular plane to the articular eminence while resting on the intervening articular disk (Fig. 13-7, A). The head of the condyle rotates during the sliding action (Fig. 13-7, B). This allows the two movements of the TMJ, which are a smooth, gliding action and a hinge action. The articular disk is a soft pad of fibrous tissue. It is thin and avascular in its center, but thicker and vascular around the margin (Fig. 13-8). The articular disk attaches to the inner wall of the capsule anteriorly and posteriorly, but not medially and laterally, which is where it attaches to the head of the condyle. This structural design requires the disk to be immobile when the head of the condyle moves.
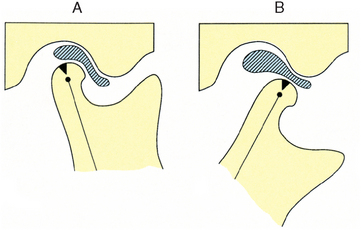
Fig. 13-7 The two actions of the temporomandibular joint. A, Pathway of movement of the condylar head along the slope of the articular eminence. B, Rotary movement of the condyle as the mouth is opened. Actions occur simultaneously.
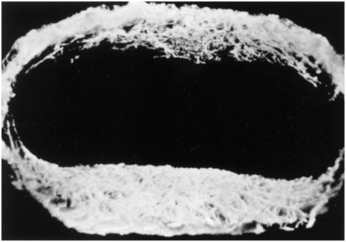
Fig. 13-8 Articular disk with vascular channels injected with latex and surrounding tissue removed. This preparation illustrates that the vascular network is only in the periphery of the disk and not to any extent in the center of the disk. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
The disk is covered with a thin layer of synovial cells and is known as a synovial membrane. This membrane secretes a synovial fluid, which moistens both the upper and lower surfaces of the articular pad and the lining of both compartments (Fig. 13-9). The synovial membrane lining is associated with numerous capillaries and lymphatics along the surface of the disk, especially in the periphery. Synovial fluid is a distillate of the blood, having a high viscosity that provides lubrication and allows freedom of condylar movement. The disk can perforate in its center, or the center can contain a few cartilage cells and islands of cartilage, especially in older age.
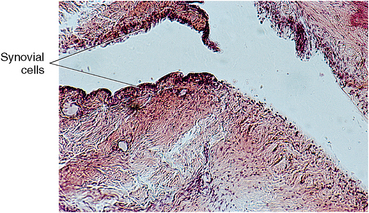
Fig. 13-9 Histology of lateral posterior aspects of the disk illustrating dark-stained synovial cells that line the joint cavity and disk.
The TMJ is a complex and precisely integrated bilateral joint that functions in speech, mastication, and deglutition. You can perceive the downward and forward sliding action of the condylar heads by placing the fingers on them as you open the jaw. This sliding action can also be felt during symmetric protrusion and retrusion or asymmetric lateral shift.
Capsule and Ligaments
A fibrous capsule encloses the TMJ like a cuff. This capsule is composed of an inner lining, or synovial layer, and an outer loose ligamentous layer that is fibrous and tough and supports articulatory movements. The attachment superiorly is to the temporal bone around the limits of the articular eminence and the fossa, and the capsule attaches around the neck of the condyle (Fig. 13-10, A). Fibers of the capsule fuse with the fibers of the lateral pterygoid muscle anteriorly, and laterally the capsule is strengthened by the lateral ligament or temporomandibular ligament (Fig. 13-10, B). Medially, the sphenomandibular ligament supports the joint (Fig. 13-10, C). This ligament arises superiorly from the spine of the sphenoid bone and extends downward on the medial side of the ramus to insert on the lingula, which is a spine of bone arising from the rim of the mandibular foramen (Fig. 13-10, C). Posteriorly, the stylomandibular ligament arises from the styloid process and inserts on the posterior border of the ramus (see Fig. 13-10, B and C). The lateral ligament and the capsule work in concert to support the joint and limit excursions of the condyles to the normal range. The other two ligaments, the sphenomandibular and stylomandibular, also serve as support. Mandibular movements involve interplay of the morphology of the teeth and the action of muscles and ligaments surrounding the TMJ.
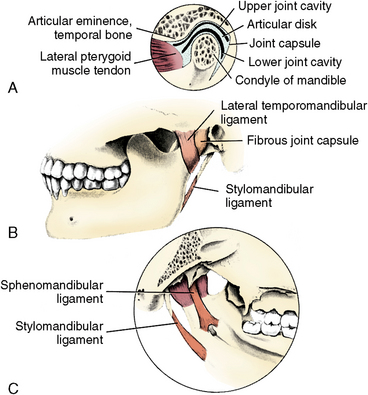
Fig. 13-10 Components of the temporomandibular joint (TMJ). A, Relationship of various TMJ compartments and the capsular ligament. B, Lateral view of the lateral fibrous joint capsule showing the relationship of the stylomandibular ligament to the mandible. C, Medial view illustrating the location and attachment of the sphenomandibular ligament of the TMJ.
Vascular Supply
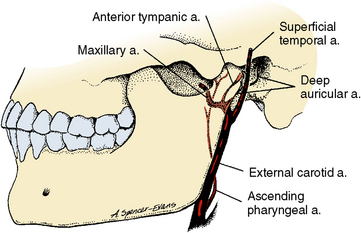
The blood supply to the TMJ is from four arteries, including (1) branches of the superficial temporal artery, (2) deep auricular artery, (3) anterior tympanic artery, and (4) ascending pharyngeal artery (Fig. 13-11). All these vessels converge on the joint, penetrate the capsule, and send branches into the network of vessels in the periphery of the disk and the posterior area of the joint. Figure 13-8 shows that the disk is oval and has more blood vessels in the anterior and posteriorareas than the lateral or medial surfaces. Interestingly, the blood vessels do not enter the fibrous covering of the head of the condyle (see Fig. 13-11), as do blood vessels in some other joints.
Innervation
The nerve supply to the TMJ arises from the branches of the mandibular division of the trigeminal nerve, specifically the auriculotemporal, masseteric, and deep temporal branches (Fig. 13-12). These are the same nerves supplying the muscles of mastication that function with this joint movement, and they help to ensure coordination of function of the muscles and joint. Both large myelinated and smaller nonmyelinated nerves enter the capsule and disk, and they supply all surfaces of the condylar head, fossa, disk, and capsule (see Fig. 13-12). Pain, temperature, touch, and deep pressure nerve terminals are found within the joint. Elaborate encapsulated terminals have been found in the connective tissue associated with the synovial folds and in the disk. Figure 13-13 shows four types of nerve terminals located in the TMJ.
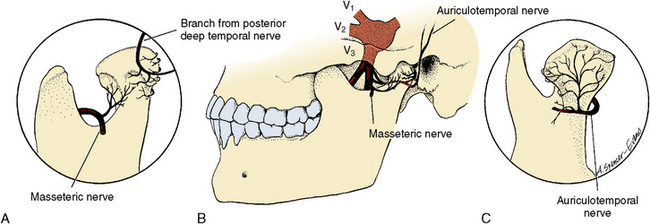
Fig. 13-12 Nerve supply to the temporomandibular joint (TMJ). Mandibular division of the fifth nerve supplies all surfaces of the TMJ through the auricular, temporal, masseteric, and deep temporal nerve branches. A, Anterolateral view. B, Lateral view. C, Posterior view.
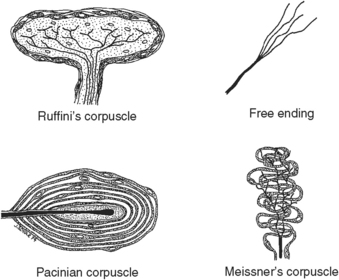
Fig. 13-13 Types of nerve endings in the temporomandibular joint. The four types are Ruffini’s or temperature endings; the pacinian, which is a deep pressure receptor; free nerve endings, which are pain endings; and Meissner’s corpuscles, which are touch receptors. These are representative of the variety of mechanoreceptors found in capsule, disk, and soft tissues of the joint that are also involved in proprioception.
Muscles of Mastication
The eight powerful muscles of mastication include four on each side of the jaw. Each muscle has a different location, and therefore the direction of fiber contraction results in a different functional relationship. Three of the muscles on each side—the medial pterygoid, the masseter, and the temporalis—exert vertical forces in closing the jaw, whereas the lateral pterygoid muscles protract the mandible and stabilize the joint. These muscles do not function alone but work as a group with the suprahyoid muscles and tongue muscles. Free movements of the mandible relate to the interplay of masticatory muscles and the morphology of the teeth, whereas masticatory movement is the synergistic action of the three groups of muscles—the elevators, depressors, and protractors—that function together and at different times during mastication of food.
Following are more details about the muscles of mastication:
1. The medial pterygoid arises from the medial surface of the lateral pterygoid plate and inserts on the inferior surface of the ramus and on the angle of the mandible. The blood supply is from the maxillary artery, and the nerve supply is from the mandibular division of the trigeminal nerve. This muscle protracts and elevates the mandible (Figs. 13-14 and 13-15).
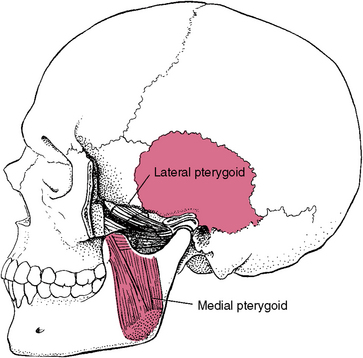
Fig. 13-14 Lateral view of the medial pterygoid muscle of mastication. The medial pterygoid functions in elevation and protraction of the condyle. This muscle functions in concert with the masseteric muscle, forming a sling.
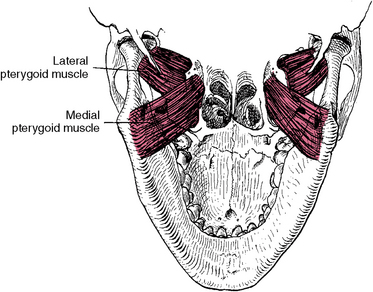
Fig. 13-15 Inferior view of the medial and lateral pterygoids to illustrate attachments to the mandible and base of the skull. The medial pterygoid arises from the lateral pterygoid plate and inserts in the inferior angle of the mandible. The lateral pterygoid arises from the greater wing of the sphenoid and the lower head from the lateral pterygoid plate. These muscles insert in the neck of condyle and capsule.
2. The lateral pterygoid has two heads, the upper arising from the greater wing of the sphenoid and the lower from the pterygoid plate. They insert into the front of the neck of the condyle and the capsule. The blood supply is from the maxillary artery, and the nerve supply is from the pterygoid branch of the mandibular nerve. Both heads of this muscle protrude the mandible and pull the articular disk forward (see Figs. 13-14 and 13-15).
3. The temporalis muscle fibers originate from the floor of the temporal fossa and temporal fascia. These muscle fibers insert on the anterior border of the coronoid process and anterior border of the ramus of the mandible (Fig. 13-16). The blood supply is from the superficial temporal and maxillary arteries, and the nerve supply is from the deep temporal branches of the mandibular nerve. The temporalis muscle elevates and retracts the mandible and clenches the teeth.
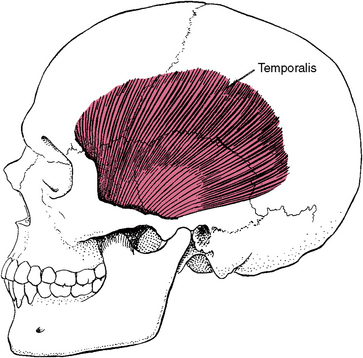
Fig. 13-16 Temporalis muscle of mastication. The temporalis muscle functions in elevation of the jaw, retraction of the mandible, clenching of the teeth, and side-to-side movements of the jaw.
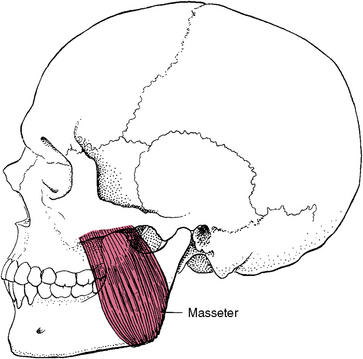
4. The masseter muscle has a deep and superficial part. The superficial fibers originate from the anterior two thirds of the lower border of the zygomatic arch, and the deep fibers originate from the medial surface of the same arch. The superficial fibers are at right angles to the occlusal plane of the posterior teeth, and the deep fibers are directed downward and slightly anteriorly. This muscle inserts into the lateral surface of the coronoid process of the mandible, the upper half of the ramus, and the angle of the mandible. The blood supply is from the superficial temporal and the maxillary arteries, and the nerve supply comes from the mandibular division of the trigeminal nerve. The masseter muscle elevates the jaw and clenches the teeth (Fig. 13-17).
A functional relationship of the occlusion of the teeth is expressed through the muscles of mastication. A detailed history and physical examination help the clinician provide an accurate diagnosis. Clinicians must rely on their own judgment in the treatment of patients with TMJ pain.
 Consider the Patient
Consider the PatientREMODELING OF TEMPOROMANDIBULAR JOINT ARTICULATION
Articular remodeling is the morphologic adaptation of the joint in response to environmental stress. The articular surfaces of the TMJ have been shown to adapt to minimize the effects of the stressful mandibular function. Presence of cartilage on the condyle and the fossa allows the TMJ to withstand stress better than other fibrous joints. Progressive remodeling occurs with proliferation of the articular cartilage and production of intercellular matrix followed by its mineralization. The cartilage is then resorbed as it is replaced by bone (Fig. 13-18). This may happen in one or both of the condylar heads and articular eminences and may relate to any changes in structure of the articular surfaces. In some cases, remodeling may begin in the proliferative zone, causing an increase of cartilage on the surface, which may then become mineralized and be replaced by bone at the zone of resorption. Functional adaptation is the response of chondrogenesis and osteogenesis to withstand the effects of mastication resulting from compression. In aging, with decreased proliferation, these changes may be degenerative.
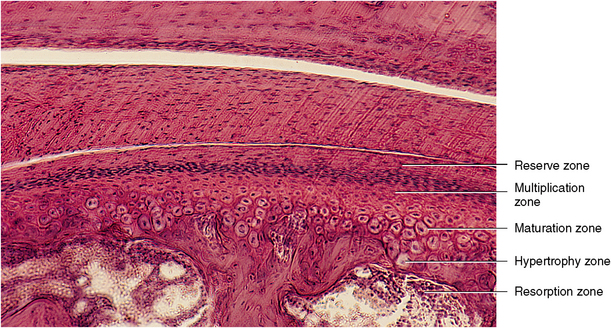
Fig. 13-18 Histologic view of the head of the condyle and the overlying articular disk. The head of the condyle exhibits a perichondrium and zones of cartilage formation and resorption. The reserve cartilage cell zone overlies the multiplication zone, zone of cartilage cell hypertrophy, and zones of cartilage resorption and bone replacement. (From Avery JK: Oral development and histology, ed 3, Stuttgart, 2002, Thieme Medical.)
Myofascial pain dysfunction (MPD) continues to be an area of concern because of varying opinions about treatment. Because much remains to be learned about both the normal and abnormal functions of the TMJ, more progress in the treatment of MPD is expected.
Discussion: Several approaches exist, but occlusal adjustment is usually the treatment of choice because of the prevalence of malocclusion. The administration of a mandibular anesthetic could help alleviate the pain. During this injection, the needle pathway is through the mucosa and the buccinator muscle and lateral to the medial pterygoid muscle, and the anesthetic is deposited near the mandibular foramen.
SELF-EVALUATION QUESTIONS
1. Name the three supporting ligaments of the TMJ.
2. What is the role of the TMJ capsule?
3. Describe the two different functions of the upper and lower compartments of the TMJ.
4. How do the heads of the condyles change as a person grows and matures?
5. What are the functions of the two heads of the lateral pterygoid muscle?
6. What is the significance of the sling muscles, and is this a function of the muscles’ location and innervation?
7. What are the location and function of the temporalis muscle?
8. What is the significance of the TMJ’s and the masticatory muscles’ having the same innervation?