Blood and serum testing and investigations

Laboratory examination may be divided into two general categories: screening and diagnostic. Screening studies are intended to identify individuals with disease in the early and asymptomatic stages. By definition, screening studies must be relatively simple and inexpensive, and are useful only when used to identify a disease which is relatively frequent (diabetes mellitus, anaemia, syphilis, blood disorders). Diagnostic examinations provide more specific information. The distinction between screening and diagnostic laboratory examination is not always rigid or absolute.
It must be remembered that laboratory examinations provide information that contributes to the diagnostic process. Seldom is this information of value by itself. The results must be interpreted in conjunction with other information that is available about the patient. It should also be noted that a laboratory value outside the normal range does not necessarily indicate disease. That value may represent normal for that specific patient. Usually, normal values are determined by testing supposedly healthy people, and these results are used to calculate the mean and normal range. Variables are not considered, and as a consequence, normal ranges are not always valid for all patients. Conversely, if a clinical diagnosis appears valid and is not substantiated by laboratory results, the tests should be repeated to rule out the possibility of laboratory error.
Haematology
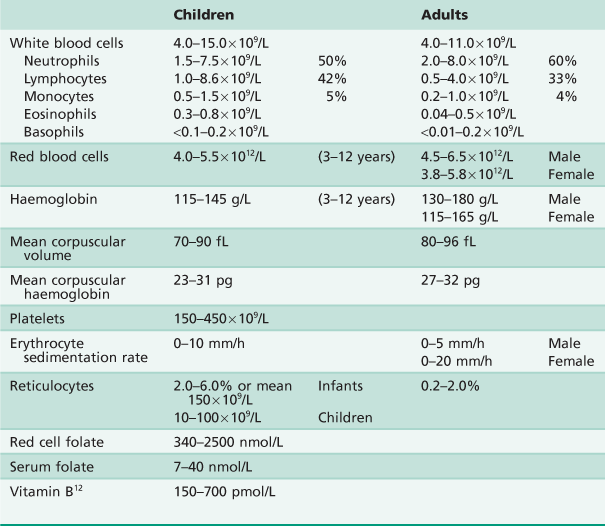
Full blood count
A full blood count (FBC) usually includes a white blood cell count (WBC), red cell blood count (RBC), haemoglobin (Hb), haematocrit (Hct) and red blood cell indices (mean corpuscular haemoglobin, mean corpuscular volume, mean corpuscular haemoglobin concentration and platelet count).
Platelet function tests are rarely ordered, usually only in consultation with a haematologist. If one asks for FBC and ‘differential’, one will also receive a breakdown of the RBC and WBC as listed on the form. If an FBC detects anaemia, then one should request serum ferritin, red cell folate and serum vitamin B12. However, in interpretation of these results, one should seek counsel, as they are difficult.
Coagulation and bleeding tests
Problems relating to bleeding are relatively infrequent in dental practice. Most inherited defects will usually have been identified early in life, and so it is usually acquired bleeding problems about which the dentist must be aware. Screening studies will identify whether there is a bleeding problem, and in which of the three systems it is, namely, platelets, coagulation or vascular abnormalities.
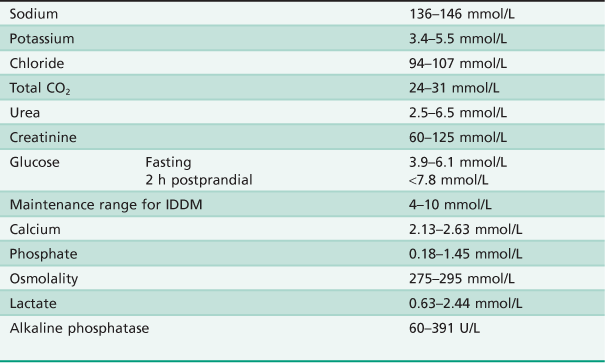
Clinical chemistry
It is not appropriate to simply request a multi-blood analysis in the hope of finding a diagnosis or abnormality. The following abbreviations are often used when ordering tests, but will obviously differ from one institution or laboratory to another.
| EUC | Electrolytes, urea, creatinine |
| LFTs | Liver profile, including serum proteins |
| CA | Calcium |
| PHOS | Inorganic phosphate, alkaline phosphatase |
Liver function tests
Table A.4
| Total bilirubin | 2–21 mmol/L |
| Total protein | 63–79 g/L |
| Albumin | 35–53 g/L |
| Alkaline phosphatase (ALP) | 30–115 U/L |
| γ-Glutamyl-transpeptidase (γGT) | |
| Male | 8–43 U/L |
| Female | 5–30 U/L |
| Alanine aminotransferase (ALT) | 7–47 U/L |
Iron studies
These tests are used when there is a suspicion of an underlying anaemia. The request for iron studies provides information regarding serum iron, total iron binding capacity and percentage iron saturation.