Women’s health
Background
Women have unique healthcare needs ranging from pregnancy to menstrual disorders. Most of these conditions are outside the remit of the community pharmacist and specialist care is needed. However, a small number of conditions can be adequately treated OTC, providing an accurate diagnosis is made. This chapter explores such conditions and attempts to outline when referral should be made.
History taking
As with all conditions that present in the community pharmacy, it is essential to take an accurate history from the patient. However, the patient might feel uncomfortable or embarrassed about discussing symptoms especially in a busy pharmacy. Male pharmacists may find that this level of embarrassment is heightened.
Cystitis
Cystitis literally means inflammation of the bladder, although in practice cystitis refers to inflammation of urethra and bladder. Before moving on to discuss cystitis in women further it is prudent to mention that men can also suffer from cystitis. However, in men cystitis is uncommon because of the longer urethra, which provides a greater barrier to bacteria entering the bladder; fluid from the prostate gland also confers some antibacterial property. This is especially so in men under the age of 50. After 50 years of age urinary tract infections in men become more common due to prostate enlargement.
Prevalence and epidemiology
Urinary tract infections (UTI) are one of most common infections treated in general medical practice and will affect up to 15% of women each year. Patients aged between 15 and 34 account for the majority of cases seen within a primary care setting and it is estimated that up to 50% of all women will experience at least one episode of cystitis in their lifetime; half of whom will have further attacks. Certain factors do increase the risk of a UTI: in young women, frequent or recent sexual activity and previous episodes of cystitis; the use of diaphragms or spermicidal agents; advancing age; and diabetes (can indicate poor diabetic control). Additionally, cystitis affects 1 to 4% of pregnant women (Le et al 2004).
Recurrent cystitis (usually defined as three episodes in the past 12 months or two episodes in the past 6 months) is relatively common even though no identifiable risk factors are present.
Aetiology
Infection is caused, in the majority of cases, by the patient’s own bowel flora that ascend the urethra from the perineal and perianal areas. Bacteria are thus transferred to the bladder where they proliferate. The most common bacterial organisms implicated in cystitis are Escherichia coli (>80% of cases), Staphylococcus (up to 10%) and Proteus. However, several studies have shown that up to 50% of women do not have positive urine cultures according to traditional criteria (>105 bacteria per mL of urine), although they do have signs and symptoms of infection. These patients with ‘low count bacteriuria’ are classed as having a urinary tract infection.
Arriving at a differential diagnosis
The majority of patients who present in the community pharmacy will have acute uncomplicated cystitis (Table 5.1). and accurately made a self-diagnosis. The pharmacist’s aims are therefore to confirm a patient self-diagnosis, rule out upper urinary tract infection (pyelonephritis) and identify patients who are at risk of complications as a result of cystitis. Asking symptom-specific questions will help the pharmacist to determine if referral is needed (Table 5.2).
Table 5.1
Causes of cystitis symptoms and their relative incidence in community pharmacy
| Incidence | Cause |
| Most likely | Acute uncomplicated cystitis |
| Likely | Pyelonephritis |
| Unlikely | Sexually transmitted disease, oestrogen deficiency |
| Very unlikely | Medicine induced cystitis, vaginitis |
 Table 5.2
Table 5.2
Specific questions to ask the patient: Cystitis
| Question | Relevance |
| Duration | Symptoms that have lasted longer than 5 to 7 days should be referred because of the risk that the person might have developed pyelonephritis |
| Age of the patient | Cystitis is unusual in children and should be viewed with caution. This might be a sign of a structural urinary tract abnormality. Referral is needed Elderly female patients (>70 years) have a higher rate of complications associated with cystitis and are therefore best referred |
| Presence of fever | Referral is needed if the person presents with fever associated with dysuria, frequency and urgency, as fever is a sensitive indicator of an upper urinary tract infection |
| Vaginal discharge | If a patient reports vaginal discharge then the likely diagnosis is not cystitis but a vaginal infection |
| Location of pain | Pain experienced in the loin area suggests an upper urinary tract infection |
Clinical features of acute uncomplicated cystitis
Cystitis is characterised by pain when passing urine and causes frequency, urgency, nocturia and haematuria. The diagnostic probability of cystitis is over 90% if patients exhibit dysuria and frequency without vaginal discharge or irritation. In addition, the patient might report only passing small amounts of urine, with pain worsening at the end of voiding urine. Symptoms usually start suddenly. Suprapubic discomfort not associated with passing urine might also be present but is not common. Haematuria, although common, should be viewed with caution because it might indicate stones or a tumour. Such cases are best referred.
Conditions to eliminate
Pyelonephritis: The most frequent complication of cystitis is when the invading pathogen involves the ureter or kidney by ascending from the bladder to these higher anatomical structures. The patient will show signs of systemic infection such as fever, chills, flank or loin pain and possibly nausea and vomiting. Referral is needed to confirm the diagnosis, exclude pelvic inflammatory disease and issue appropriate treatment (7-day course of ciprofloxacin 500 mg twice daily).
Unlikely causes
Sexually transmitted diseases: Sexually transmitted diseases can be caused by a number of pathogens, for example Chlamydia trachomatis and Neisseria gonorrhoea. Symptoms are similar to acute uncomplicated cystitis but they tend to be more gradual in onset and last for a longer period of time. In addition pyuria (pus in the urine) is usually present.
Oestrogen deficiency (atrophic vaginitis): Postmenopausal women experience thinning of the endometrial lining as a result of a reduction in the levels of circulating oestrogen in the blood. This increases the likelihood of irritation or trauma leading to cystitis symptoms. If the symptoms are caused by intercourse, symptomatic relief can be gained with a lubricating product. Referral for possible topical oestrogen therapy would be appropriate if the symptoms recur.
Very unlikely causes
Medicine induced cystitis: Non-steroidal anti-inflammatory agents (NSAIDs; especially tiaprofenic acid), allopurinol, danazol and cyclophosphamide have been shown to cause cystitis.
Vaginitis: Vaginitis exhibits similar symptoms to cystitis, in that dysuria, nocturia, and frequency are common. It can be caused by direct irritation (e.g. use of vaginal sprays and toiletries) All patients should be questioned about an associated vaginal discharge. The presence of vaginal discharge is highly suggestive of vaginitis and referral is needed.
Figure 5.1 will aid the differentiation of cystitis from other conditions.
 Trigger points indicative of referral
Trigger points indicative of referral
Cystitis
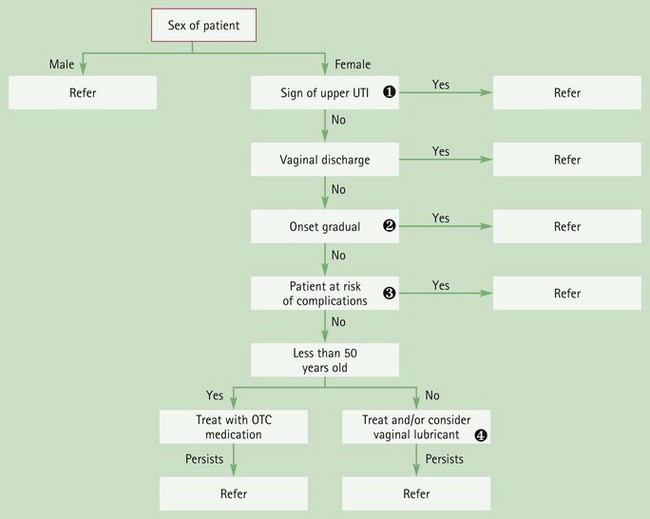
Fig. 5.1 Primer for differential diagnosis of cystitis. Involvement of the higher urinary tract structures
Involvement of the higher urinary tract structures
Symptoms such as fever, flank pain, nausea and vomiting suggest conditions such as pyelonephritis. Gradual onset
Gradual onset
STDs should be considered in patients whose symptoms are not sudden. At-risk patients
At-risk patients
Patients at risk of developing upper UTI include those with diabetes, pregnant women, the immunocompromised, the elderly and those patients in whom symptoms have been present for more than 5 to 7 days. Patients over 50 years old
Patients over 50 years old
Oestrogen deficiency might account for the patient’s symptoms resulting in local atrophy of the vagina.
Evidence base for over-the-counter medication
Current OTC treatment is limited to products that contain alkalinising agents, namely sodium citrate, sodium bicarbonate and potassium citrate. (Applications to reclassify trimethoprim and nitrofurantoin in the UK have been made but were withdrawn due to pressure from medical groups.) Alkalinising agents are used to return the urine pH back to normal thus relieving symptoms of dysuria. However, they have dubious efficacy with little trial data to support their use. Only one trial by Spooner (1984) could be found to support their efficacy. Spooner concluded that, when treated with a 2-day course of Cymalon, 80% of patients with cystitis for whom there was no clear clinical evidence of bacterial infection did gain symptomatic relief.
Cranberry juice
Cranberry juice is a popular alternative remedy to treat and prevent urinary tract infections, although few clinical trials have been performed to substantiate or refute its clinical effectiveness. A Cochrane review (Jepson & Craig 2012) identified 10 studies comparing cranberry juice or cranberry tablets to placebo. The review found cranberry products significantly reduced the incidence of UTIs at 12 months, particularly in women who suffer recurrent infections. However, drop out rates in the trials were high suggesting many patients may not be able to tolerate cranberry juice long term. The authors concluded that there was evidence that cranberry juice did offer some protection against recurrence of urinary tract infections in women that suffer symptomatic UTIs. However, it is still unclear what amount and concentration needs to be consumed, nor how long patients should take it for.
The same authors also reviewed the use of cranberry juice in the treatment of existing UTIs (Jepson et al 1998, updated in 2010). However, they were unable to find any RCTs that met their criteria. The authors concluded that there was no good evidence yet to support the use of cranberry juice for the treatment of UTIs.
Studies involving cranberry juice were not associated with any serious adverse events but widespread use of cranberry juice has resulted in the identification of a possible interaction with warfarin, although evidence is currently (2012) conflicting. Until evidence is conclusive it would seem prudent that patients on warfarin should be advised not to take products containing cranberry.
Practical prescribing and product selection
Prescribing information relating to cystitis medicines reviewed in the section ‘Evidence base for over-the-counter medication’ is discussed and summarised in Table 5.3 and useful tips relating to patients presenting with cystitis are given in Hints and Tips Box 5.1.
 Table 5.3
Table 5.3
Practical prescribing: Summary of medicines for cystitis
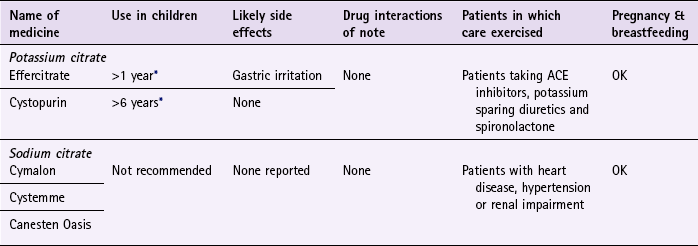
ACE, angiotensin converting enzyme.
*Children should not be treated for UTI by pharmacists as unusual in this age group.
Alkalinising agents
All marketed products are presented as a 2-day treatment course. The majority are presented as sachets (Effercitrate are dissolvable tablets) and the dose is one sachet to be taken three times a day, although potassium citrate can be bought as a ready-made solution (the dose is 10 mL three times a day diluted well with water) They possess very few side effects and can be given safely with other prescribed medication, although in theory products containing potassium should be avoided in patients taking angiotensin-converting enzyme inhibitors, potassium-sparing diuretics and spironolactone. However, in practice it is highly unlikely that a 2-day course of an alkalinising agent will be of any clinical consequence. They can also be prescribed to most patient groups and can be given in pregnancy although most manufacturers advise against prescribing in pregnancy, presumably on the basis that pregnant women have a higher incidence of complications resulting from cystitis. The manufacturers of Effercitrate and Cystopurin state they can be used in children but good practice would dictate that children under 16 should be referred to a medical practitioner.
References
Jepson, RG, Williams, G, Craig, JC. Cranberries for preventing urinary tract infections. Cochrane Database of Systematic Reviews. (Issue 10):2012. [Art. No.: CD001321. DOI: 10.1002/14651858.CD001321.pub5].
Jepson, RG, Mihaljevic, L, Craig, JC. Cranberries for treating urinary tract infections. Cochrane Database of Systematic Reviews. (Issue 4):1998. [Art. No.: CD001322. DOI: 10.1002/14651858.CD001322].
Le, J, Briggs, GG, McKeown, A, et al. Urinary tract infections during pregnancy. An Pharmacother. 2004;38(10):1692–1701.
Spooner, JB. Alkalinisation in the management of cystitis. J Int Med Res. 1984;12:30–34.
Vaginal discharge
Background
Patients of any age can experience vaginal discharge. The three most common causes of vaginal discharge are bacterial vaginosis, vulvovaginal candidiasis (thrush) and trichomoniasis (Table 5.4). As thrush is the only condition that can be treated OTC, the text concentrates on differentiating this from other conditions.
Prevalence and epidemiology
It has been reported that sexually active women have a 75% chance of experiencing at least one episode of thrush during their childbearing years, and half of these will have more than one episode. Most cases are acute attacks but some women will develop recurrent thrush defined as 4 or more attacks each year. The condition is uncommon in prepubertal girls unless they have been receiving antibiotics. In adolescents it is the second most common cause of vaginal discharge after bacterial vaginosis.
Aetiology of thrush
The vagina naturally produces a watery discharge (physiological discharge), the amount and character of which varies depending on many factors, such as ovulation, pregnancy and concurrent medication. At the time of ovulation the discharge is greater in quantity and of higher viscosity. Normal secretions have no odour. The epithelium of the vagina contains glycogen, which is broken down by enzymes and bacteria (most notably lactobacilli) into acids. This maintains the low vaginal pH, creating an environment inhospitable to pathogens. The glycogen concentration is controlled by oestrogen production; therefore any changes in oestrogen levels will result in either increased or decreased glycogen concentrations. If oestrogen levels decrease glycogen concentration also decreases, giving rise to an increased vaginal pH and making the vagina more susceptible to opportunistic infection such as Candida albicans; 95% of thrush cases are caused by C. albicans. The remaining cases are caused by C. glabrata although symptoms are indistinguishable.
Arriving at a differential diagnosis
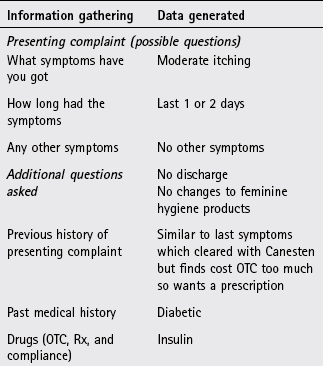
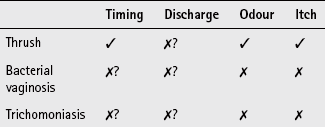
Many patients will present with a self-diagnosis and the pharmacists’ role will often be to confirm a self-diagnosis of thrush. This is very important as studies have shown that misdiagnosis by patients is common (Ferris et al 2002) and can have important consequences because other conditions can lead to greater health concerns. For example, bacterial vaginosis has been linked with pelvic inflammatory disease (PID) and the preterm delivery of low-birth-weight infants and C. trachomatis can cause infertility. Symptoms of pruritus, burning and discharge are possible in all three common causes of vaginal discharge. Therefore no one symptom can be relied upon with 100% certainty to differentiate between thrush, bacterial vaginosis and trichomoniasis. However, certain symptom clusters are strongly suggestive of a particular diagnosis. Asking symptom specific questions will help the pharmacist to determine if referral is needed (Table 5.5).
Table 5.5
Specific questions to ask the patient: Vaginal discharge
| Question | Relevance |
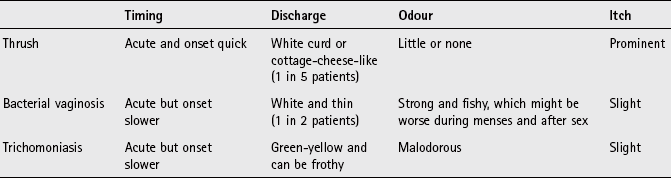
| Discharge | Any discharge with a strong odour should be referred. Bacterial vaginosis is associated with a white discharge that has a strong fishy odour and trichomoniasis is malodorous with a green-yellow discharge. By contrast, discharge associated with thrush is often described as ‘curd-like’ or ‘cottage cheese-like’ with little or no odour |
| Age | Thrush can occur in any age group, unlike bacterial vaginosis and trichomoniasis, which are rare in premenarchal girls. In addition, trichomoniasis is also rare in women aged over 60 |
| Pruritus | Vaginal itching tends to be most prominent in thrush compared with bacterial vaginosis and trichomoniasis where itch is slight |
| Onset | In thrush, the onset of symptoms is sudden, whereas bacterial vaginosis and trichomoniasis onset tends to be less sudden |
Clinical features of thrush
The dominant feature of thrush is vulval itching. This is often accompanied with discharge (in up to 20% of patients). The discharge has little or no odour and is curd-like. Symptoms are generally acute in onset.
Conditions to eliminate
This is the commonest cause of vaginal discharge, in a community pharmacy setting; it must be eliminated as a cause of symptoms, as treatment requires antibiotics (metronidazole 400 mg twice daily for 5 to 7 days). The exact cause of bacterial vaginosis is unknown although Gardnerella vaginalis is often implicated. Approximately half of patients will experience a thin white discharge with a strong fishy odour. Odour is worse after sexual intercourse and may worsen during menses. Itching and soreness are not usually present. Certain risk factors include multiple sexual partners, low social class and race (more common in black women).
Unlikely causes
Trichomoniasis: Trichomoniasis, a protozoan infection is primarily transmitted through sexual intercourse. It is uncommon compared to bacterial vaginosis and thrush. Up to 50% of patients are asymptomatic. If symptoms are experienced a profuse, frothy, greenish-yellow and malodorous discharge accompanied by vulvar itching is typical. Other symptoms can include vaginal spotting, dysuria and urgency. Referral for metronidazole (400 mg bd for 5 to 7 days) is required.
Cystitis: Dysuria can affect up to one in three women with vaginal infection. However, the patient will often be able to sense that it is an external discomfort, rather than an internal discomfort located in the urethra or bladder that occurs with urinary tract infections.
Atrophic vaginitis: Symptoms consistent with thrush in postmenopausal women, especially vaginal itching and burning, may be due to atrophic vaginitis. However, clinically significant atrophic vaginitis is uncommon in postmenopausal women, and should be referred to rule out malignancy.
There are also several factors that predispose women to thrush that require consideration prior to instigating treatment.
Medicine-induced thrush
Broad-spectrum antibiotics, corticosteroids, immunosuppressants and medication affecting the oestrogen status of the patient (oral contraceptives, HRT, tamoxifen and raloxifene) can predispose women to thrush. It is therefore not unusual to see a patient prescribed at the same time as receiving antibiotics.
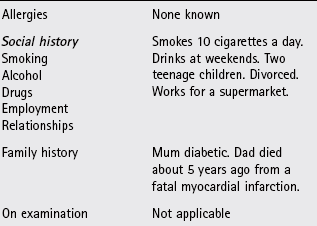
Diabetes
Patients with poorly controlled diabetes (type 1 or 2) are more likely to suffer from thrush because hyperglycaemia can enhance production of protein surface receptors on C. albicans organisms. This hinders phagocytosis by neutrophils, thus making thrush more difficult to eliminate.
Pregnancy
Hormonal changes during pregnancy will alter the vaginal environment and have been reported to make eradication of Candida more difficult. Topical agents are safe and effective in pregnancy but OTC licensed indications do not allow sale to pregnant women and therefore these patients must be referred to the GP.
Recurrent thrush (four or more episodes per year)
After treatment a minority of patients will present with recurrent symptoms. This may be due to poor compliance, misdiagnosis, resistant strains of Candida, undiagnosed diabetes or the patient having a mixed infection. Such cases are outside the remit of community pharmacy and have shown to be difficult to treat. Often specialist care is needed through genitourinary medicine clinics.
Figure 5.2 will help in the differentiation of vaginal thrush from other conditions in which vaginal discharge is a major presenting complaint.
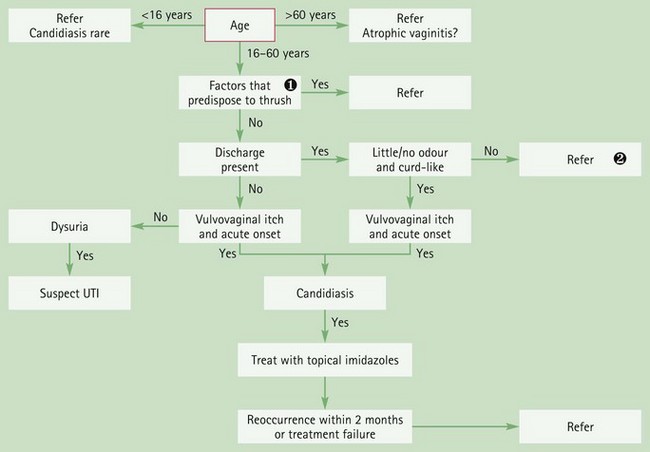
Fig. 5.2 Primer for differential diagnosis of vaginal thrush. If the person is pregnant or has diabetes then referral is the most appropriate option. If the person is suffering from medicine-induced candidiasis the prescriber should be contacted to discuss suitable treatment options and, if appropriate, alternative therapy. Discharge that has a strong odour and is not white and curd-like should be referred, as trichomoniasis or bacterial vaginosis are more likely causes.
Trigger points indicative of referral
Thrush
| Symptoms/signs | Possible danger/reason for referral |
| Discharge that has a strong smell | Suggests bacterial vaginosis or trichomoniasis |
| Diabetics | Might suggest poor diabetic control |
| OTC medication failure Patients predisposed to thrush Recurrent attacks |
Suggests underlying problem or misdiagnosis |
| Women under 16 and over 60 | Thrush unusual in these age groups |
Evidence base for over-the-counter medication
Topical imidazoles and one systemic triazole (fluconazole) are available OTC to treat vaginal thrush. They are potent and selective inhibitors of fungal enzymes necessary for the synthesis of ergosterol, which is needed to maintain the integrity of cell membranes.
Imidazoles and triazoles have proven and comparable efficacy with clinical cure rates between 85 and 90%. Additionally, cure rates between single or multiple dose therapy and multiple day therapy show no differences (Nurbhai et al 2007, updated in 2009). Treatment choice will therefore be driven by patient acceptability and cost.
Practical prescribing and product selection
Prescribing information relating to medicines for thrush reviewed in the section ‘Evidence base for over-the-counter medication’ is discussed below and summarised in Table 5.6; useful tips relating to patients presenting with thrush are given in Hints and Tips Box 5.2.
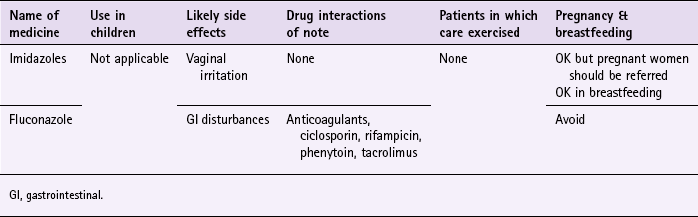
Topical imidazoles (clotrimazole, econazole, miconazole)
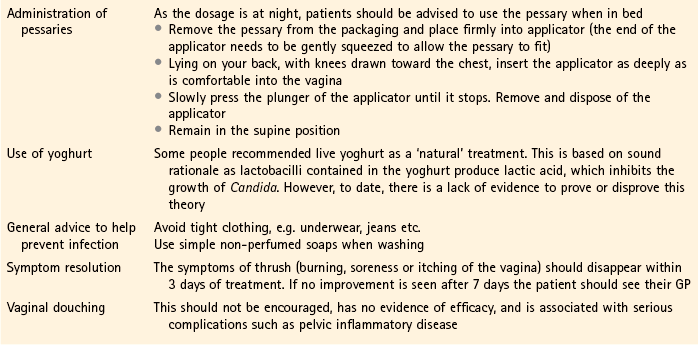
A number of formulations are available for local application including creams, vaginal tablets and pessaries. Pharmacists and the public are probably most familiar with the Canesten range of products. All internal preparations should be administered at night. This gives the medicine time to be absorbed and eliminates the possibility of accidental loss, which is more likely to occur if the person is mobile. Slight irritation on application is infrequently reported (about 5% of users) and has been linked to the vehicle and not the active ingredient. Systemic absorption is minimal and therefore there are no interactions of note, although they may damage latex condoms and diaphragms. Consequently the effectiveness of such contraceptives may be reduced. Topical imidazoles do have a number of product licence restrictions which should be observed when recommending these products and are listed in Table 5.7.
Table 5.7
Product licence restrictions – topical imidazoles
| Product licence restriction | Rationale |
| Is under 16, or over 60, years of age | Thrush less common in these age groups |
| Has systemic symptoms | Suggests infection from a cause other than thrush |
| Has symptoms that are not entirely consistent with a previous episode (e.g. discharge is coloured or malodorous, there are ulcers or blisters) | Suspect bacterial vaginitis or trichomoniasis |
| Has had two episodes in 6 months, and has not consulted her GP about the condition for more than a year | Good practice as repeat infection may be due to misdiagnosis or predisposing risk factors |
| May be pregnant or is breastfeeding | Safe in both pregnancy and breastfeeding, although thrush is more common during pregnancy and it is also important to rule out gestational diabetes. |
| Has had a previous sexually transmitted infection (or her partner has) | Rule out STD |
| Has had abnormal menstrual bleeding or lower abdominal pain | Symptoms not suggestive of thrush |
| Does not experience complete resolution of symptoms after 7 days of treatment | Imidazoles are highly effective and continuing symptoms point to misdiagnosis |
Fluconazole (e.g. Diflucan One, Canesten oral)
Fluconazole is a single oral dose treatment that can be taken at any time of the day. (Note: there are also combination packs containing oral fluconazole and a tube of topical clotrimazole.) Fluconazole is generally well tolerated but can cause gastrointestinal disturbances, such as nausea, abdominal discomfort, diarrhoea and flatulence in up to 10% of patients. There are a number of established clinically important drug interactions with fluconazole. These include anticoagulants, ciclosporin, rifampicin, phenytoin and tacrolimus. However, these drug interactions relate to the use of multiple-dose fluconazole and the relevance to single-dose fluconazole has not yet been established. It would be prudent to avoid these combinations until further evidence is available with single-dose fluconazole.
References
Ferris, DG, Nyirjesy, P, Sobel, JD, et al. Over-the-counter antifungal drug misuse associated with patient-diagnosed vulvovaginal candidiasis. Obstet Gynecol. 2002;99:419–425.
Nurbhai, M, Grimshaw, J, Watson, M, et al. Oral versus intra-vaginal imidazole and triazole anti-fungal treatment of uncomplicated vulvovaginal candidiasis (thrush). Cochrane Database of Systematic Reviews. (Issue 4):2007.
Brown, D, Binder, GL, Gardner, HL, et al. Comparison of econazole and clotrimazole in the treatment of vulvovaginal candidiasis. Obstet Gynecol. 1980;56:121–123.
Eschenbach, DA, Hillier, S, Critchlow, C, et al. Diagnosis and clinical manifestations of bacterial vaginosis. Am J Obstet Gynecol. 1988;158:819–828.
Fidel, PL, Sobel, JD. Immunopathogenesis of recurrent vulvovaginal candidiasis. Clin Microbiol Rev. 1996;9:335–348.
Ferris, DG, Dekle, C, Litaker, MS. Women’s use of over-the-counter antifungal medications for gynecologic symptoms. J Fam Pract. 1996;42:595–600.
Floyd, R, Hodgson, C. One-day treatment of vulvovaginal candidiasis with a 500-mg clotrimazole vaginal tablet compared with a three-day regimen of two 100-mg vaginal tablets daily. Clin Ther. 1986;8:181–186.
Lebherz, TB, Goldman, L, Wiesmeier, E, et al. A comparison of the efficacy of two vaginal creams for vulvovaginal candidiasis, and correlations with the presence of Candida species in the perianal area and oral contraceptive use. Clin Ther. 1983;5:409–416.
Schembri, G, Malu, M. Vaginal discharge: recommended management in general practice. The Prescriber. 2010:37–44. 19 May
Sobel, JD, Faro, S, Force, RW, et al. Vulvovaginal candidiasis: epidemiologic, diagnostic, and therapeutic considerations. Am J Obstet Gynecol. 1998;178:203–211.
Spence, D, Melville, C. Vaginal discharge. Br Med J. 2007;335:1147–1151. (1 December), doi:10.1136/bmj.39378.633287.80
Embarrassing problems. http://www.embarrassingproblems.com/problem/vaginal-vulva-problems.
NHS Sex and young people. http://www.nhs.uk/Livewell/Sexandyoungpeople/Pages/Sex-and-young-people-hub.aspx.
Primary dysmenorrhoea (period pain)
Background
Menstruation spans the years between menarche to menopause. Typically this will last 30 to 40 years, starting around the age of 12 and ceasing around the age of 50. The menstrual cycle usually lasts 28 days but this varies and it can last anything between 21 and 45 days. Menstruation itself lasts between 3 and 7 days. Individuals can also exhibit differences in menstrual cycle length and blood flow. Dysmenorrhoea is usually categorised as primary or secondary; primary dysmenorrhoea (PD) is defined as menstrual pain without organic pathology whereas in secondary dysmenorrhoea an identifiable pathologic condition can be identified.
Prevalence and epidemiology
PD is very common in adolescents but exact prevalence rates vary due to differing definitions of dysmenorrhoea used in studies. However, it is likely to affect over 50% of women, and 7 to 15% of these women report symptoms severe enough to cause school and work absence.
Aetiology
Overproduction of uterine prostaglandins E2 and F2-alpha are major contributory factors in causing painful cramps. Prostaglandin production is controlled by progesterone and before menstruation starts progesterone levels decrease allowing prostaglandin production to increase, and if over-produced cramps occur. Ovulation inhibition can also improve symptoms (by using the oral contraceptive pill) as it lessens the endometrial lining of the uterus reducing menstrual fluid volume and reducing prostaglandin production.
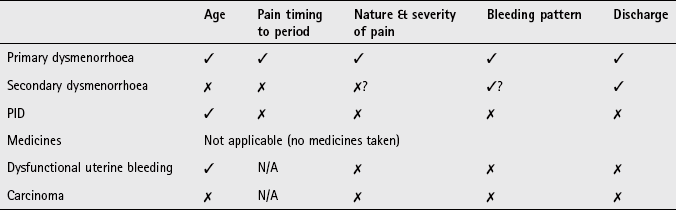
Arriving at a differential diagnosis
The main consideration of the community pharmacist is to exclude conditions that have a pathologic cause (secondary dysmenorrhoea). Fortunately, by far and away the most likely problem seen in primary care is PD (Table 5.8).
Table 5.8
Causes of period pain and their relative incidence in community pharmacy
| Incidence | Cause |
| Most likely | Primary dysmenorrhoea |
| Likely | Secondary dysmenorrhoea |
| Unlikely | Pelvic inflammatory disease, dysfunctional uterine bleeding |
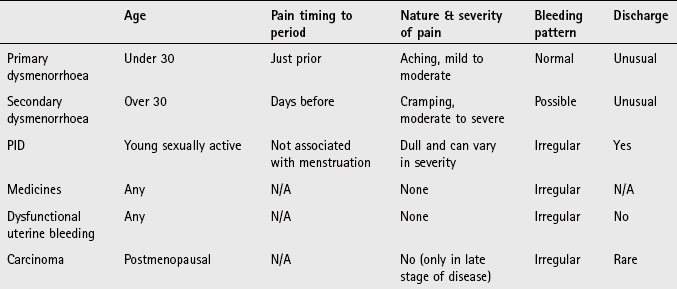
It is essential to take a detailed history of the patient’s menstrual history as PD is a diagnosis based on exclusion. The frequency, severity and relationship of symptoms to the menstrual cycle need to be established. Asking symptom-specific questions will help the pharmacist to determine if referral is needed (Table 5.9).
Table 5.9
Specific questions to ask the patient: Primary dysmenorrhoea
| Question | Relevance |
| Age | PD is most common in adolescents and women in their early twenties. Secondary dysmenorrhoea usually affects women many years after the menarche, typically after the age of thirty |
| Nature of pain | A great deal of overlap exists between PD and secondary dysmenorrhoea but generally PD results in cramping whereas secondary causes are usually described as dull, continuous diffuse pain |
| Severity of pain | Pain is rarely severe in PD; the severity decreases with the onset of menses. Any patient presenting with severe lower abdominal pain should be referred |
| Onset of pain | PD starts very shortly before or within 24 hours of the onset of menses and rarely lasts for more than 3 days. Pain associated with secondary dysmenorrhoea typically starts a few days before the onset of menses |
Clinical features of PD
A typical presentation of PD is of lower abdominal cramping pains shortly before (6 hours) and for 2 or possibly 3 days after the onset of bleeding. Commonly associated symptoms include fatigue, back pain, nausea and/or vomiting and diarrhoea. It is classically associated with young women who have recently (6–12 months) started having regular periods. However, there may be a gap of months or years between menarche and onset of symptoms. This is due to as many as 50% of women being anovulatory in the first year (and still 10% of women 8 years after the menarche). This is important to know, as anovulatory cycles are usually pain free.
Conditions to eliminate
Secondary dysmenorrhoea (e.g. endometriosis): Endometriosis simply means presence of endometrial tissue outside of the uterus. The exact incidence of endometriosis is unclear; however, it is the most common cause of secondary dysmenorrhoea. Reports suggest it may occur in up to 50% of menstruating women but many are asymptomatic. Any person over the age of 30 either presenting for the first time with dysmenorrhoea or has noticed worsening symptoms should be viewed with caution. Patients experience lower abdominal pain (aching rather than cramping), that usually starts 5 to 7 days before menstruation begins and can be constant and severe. The pain often peaks at the onset of menstruation. Referred pain into the back and down the thighs is also possible.
Unlikely causes
Pelvic inflammatory disease: PID is an important cause of infertility and ectopic pregnancy with many women being asymptomatic and only diagnosed during infertility investigation. It most commonly occurs in sexually active women aged between 15 and 24 years old. Symptomatic cases show variable clinical presentation but it is associated with dull bilateral lower abdominal pain and dysmenorrhoea (with pain greatest premenstrually). Other symptoms such as fever, malaise, vaginal discharge, irregular menses and dyspareunia are often present.
Dysfunctional uterine bleeding: Dysfunctional uterine bleeding is a non-specific medical term defined as abnormal uterine bleeding that is not due to structural or systemic disease and includes conditions such as amenorrhoea (lack of menstruation) and menorrhagia (heavy periods); with the majority of cases attributable to menorrhagia. The pharmacist should ask the patient if their periods are different than usual.
Evidence base for over-the-counter medication
Non-steroidal anti-inflammatories
The use of NSAIDs would be a logical choice because raised prostaglandin levels cause PD. In multiple clinical trials they have been shown to be effective in 80 to 85% of women. A Cochrane review by Marjoribanks et al (2010) concluded that NSAIDs were significantly more effective in relieving moderate to severe pain associated with PD compared to placebo. However, there was little evidence of superiority of any individual NSAID.
Hyoscine butylbromide (Buscopan)
In one study, Buscopan was given to 17 patients in a double-blind placebo-crossover trial. The study failed to demonstrate a significant effect compared to placebo, or the comparator drug – aspirin, although in the authors’ opinion Buscopan was a good alternative to NSAIDs.
Alverine (Spasmonal) is licensed for the treatment of dysmenorrhoea. It is an anticholinergic antispasmodic that relaxes the uterine smooth muscle; however, there is a lack of published evidence regarding its efficacy.
Low-dose combined oral contraceptives
Although not available OTC, oral contraceptives have been reported to be beneficial in treating PD. A Cochrane review (Wong et al 2009) identified 10 trials, and found improvements in pain compared to placebo (OR = 2.01; 95% CI 1.32–3.08). Therefore, if standard OTC treatment is not controlling symptoms adequately the patient is best referred as contraceptives provide an alternative treatment option.
Other treatment options
A number of alternative treatments have been tested in PD, most notably transcutaneous electrical nerve stimulation (TENS), acupuncture, exercise and dietary supplements. Of these, high frequency TENS appears to have the strongest body of evidence to support its use (Proctor et al 2002), acupuncture appears promising (Smith et al 2011), and the evidence for exercise is uncertain (Brown & Brown 2010). A wide range of dietary intervention is frequently recommended and includes vitamin B and E, fish oils and magnesium. Most trials were conducted on low patient numbers and have reported limited or no benefit except vitamin B1 (thiamine – 100 mg), which saw a significant proportion of women with no pain compared with placebo (Proctor et al 2001). The Chinese herbal remedy toki-shakuyaku-san, taken for at least 6 months, may also reduce dysmenorrhoea.
Practical prescribing and product selection
Prescribing information relating to the medicines reviewed in the section ‘Evidence base for over-the-counter medication’ is discussed and summarised in Table 5.10; useful tips relating to patients presenting with PD are given in Hints and Tips Box 5.3.
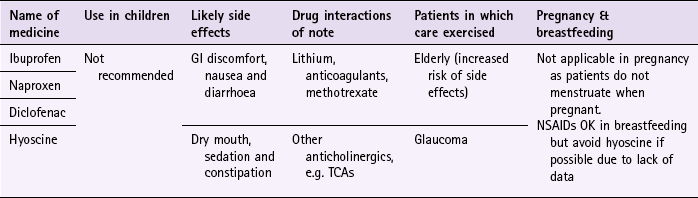
Ibuprofen
There are a plethora of marketed ibuprofen products (e.g. Nurofen and Cuprofen) all of which have a standard dose for the relief of PD. Adults should take 200 to 400 mg (one or two tablets) three times a day, although most patients will need the higher dose of 400 mg three times a day. Because ibuprofen is only used for a few days each cycle it is generally well tolerated. However, gastric irritation is possible and ibuprofen can cause peptic ulcers or bronchospasm in asthmatics who have a history of hypersensitivity to aspirin or NSAIDs. Ibuprofen can interact with many medicines although the vast majority are not clinically significant (see Table 5.10).
Naproxen (Feminax Ultra)
Naproxen is indicated for primary dysmenorrhoea for women aged between 15 and 50 years old. The dose is two tablets (500 mg) initially, followed 6 to 8 hours later by a second tablet (250 mg) if needed. No more than three tablets should be taken in a 24-hour period. The same side effects, cautions and contraindications with ibuprofen apply to naproxen.
Diclofenac Potassium (Voltarol Pain-Eze)
Diclofenac Potassium is indicated for the relief of period pain. It can be given to people aged over 14 years old. The dose is two tablets initially, followed by one or two tablets every 4 to 6 hours as needed. No more than six tablets (75 mg) should be taken in any 24-hour period. The same side effects, cautions and contraindications with ibuprofen apply to diclofenac.
Hyoscine hydrobromide (Buscopan Cramps)
The dosage frequency for adults is two tablets four times a day. It is contraindicated in patients with narrow-angle glaucoma and myasthenia gravis and care should be exercised in patients whose conditions are characterised by tachycardia (for example, hyperthyroidism and cardiac problems). Anticholinergic side effects such as dry mouth, visual disturbances and constipation can be experienced but are generally mild and self-limiting. Side effects are potentiated if it is given with tricyclic antidepressants, antihistamines, butyrophenones, phenothiazines and disopyramide.
References
Brown, J, Brown, S. Exercise for dysmenorrhoea. Cochrane Database of Systematic Reviews. (Issue 2):2010. [Art.No.: CD004142. DOI: 10.1002/14651858.CD004142.pub2].
Marjoribanks, J, Proctor, M, Farquhar, C, et al. Non-steroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database of Systematic Reviews. (Issue 1):2010. [Art. No.: CD001751. DOI: 10.1002/14651858.CD001751.pub2].
Proctor, M, Murphy, PA. Herbal and dietary therapies for primary and secondary dysmenorrhoea. Cochrane Database of Systematic Reviews. (Issue 2):2001. [Art. No.: CD002124. DOI: 10.1002/14651858.CD002124].
Proctor, M, Farquhar, C, Stones, W, et al. Transcutaneous electrical nerve stimulation for primary dysmenorrhoea. Cochrane Database of Systematic Reviews. (Issue 1):2002. [Art. No.: CD002123. DOI: 10.1002/14651858.CD002123].
Smith, CA, Zhu, X, He, L, et al. Acupuncture for primary dysmenorrhoea. Cochrane Database of Systematic Reviews. (Issue 1):2011. [Art. No.: CD007854. DOI: 10.1002/14651858.CD007854.pub2].
Wong, CL, Farquhar, C, Roberts, H, et al. Oral contraceptive pill for primary dysmenorrhoea. Cochrane Database of Systematic Reviews. (Issue 4):2009. [Art. No.: CD002120. DOI: 10.1002/14651858.CD002120.pub3].
Auld, B, Sinha, P. Dysmenorrhoea: diagnosis and current management. The Prescriber. 2006:33–40.
Harlow, SD, Ephross, SA. Epidemiology of menstruation and its relevance to women’s health. Epidemiol Rev. 1995;17:265–286.
Kemp, JH. ‘Buscopan’ in spasmodic dysmenorrhoea. Curr Med Res Opin. 1972;1:19–25.
Endometriosis UK. http://www.endo.org.uk/
Endometriosis SHE Trust. http://www.shetrust.org.uk/
Royal College of Obstetricians and Gynaecologists. http://www.rcog.org.uk/
Premenstrual syndrome
Background
Premenstrual syndrome (PMS) is a broad term that encompasses a wide range of symptoms – both physical and psychological. Symptoms range from mild to very severe; severe symptoms, especially mood symptoms, affect approximately 5% of patients and can interfere with day-to-day functioning and relationships. In these women a diagnosis of premenstrual dysphoric disorder is given.
Prevalence and epidemiology
The exact prevalence of PMS is hard to determine because of varying definitions attributed to PMS and the number of people that do not seek medical help. Surveys have shown that over 90% of women have experienced PMS symptoms but only a fifth seek medical help, yet 13 to 25% have taken time off work because of PMS symptoms. There appears to be no marked racial or ethnic differences in the prevalence but age appears to be a risk factor – most women tend to be over 30 years old.
Aetiology
The precise pathophysiology of PMS is still unclear. A number of theories have been put forward, for example excess oestrogen, a lack of progesterone or ovarian function. Most researchers now believe PMS is a complex interaction between ovarian steroids and the neurotransmitters serotonin and GABA.
Arriving at a differential diagnosis
Owing to the varying and wide-ranging symptoms associated with PMS the pharmacist must endeavour to differentiate PMS from other gynaecological and mental health disorders. Careful questioning of when the symptoms occur and what symptoms are experienced will hopefully give rise to a differential diagnosis of PMS, although this might not be easy. It is important not to focus on one cycle’s symptoms but ask the patient to describe their symptoms over previous cycles. A diary over three cycles should be maintained to allow a fuller picture of symptoms to be elucidated (symptom diaries are available such as the Daily Record of Severity of Problems – see www.rcog.org.uk). Asking symptom-specific questions will help the pharmacist to determine if referral is needed (Table 5.11).
Table 5.11
Specific questions to ask the patient: Premenstrual syndrome
| Question | Relevance |
| Onset of symptoms | Symptoms that are experienced 7 to 14 days before, and that disappear a few hours after the onset of menses, are suggestive of PMS |
| Age of patient | PMS is most common in women aged in their 30s and 40s |
| Presenting symptoms | Patients with PMS will normally have symptoms suggestive of mental health disorders such as low mood, insomnia and irritability. This can make excluding mental health disorders such as depression difficult. However, the cyclical nature of the symptoms in conjunction with symptoms such as breast tenderness, bloatedness and fluid retention point to PMS |
Clinical features of PMS
Many symptoms have been attributed to PMS, although the most common symptoms are listed in Table 5.12.
Conditions to eliminate
Abdominal cramps and suprapubic pain might be experienced by PMS sufferers, although these symptoms are uncommon. Key distinguishing features between PMS and primary dysmenorrhoea are the lack of behavioural and mood symptoms in primary dysmenorrhoea and the difference in timing of symptoms in relation to the menstrual cycle.
Mental health disorders
Depression and anxiety are common mental health disorders, which often go undiagnosed and can be encountered by community pharmacists. Patients with PMS might experience symptoms similar to such conditions, namely low or sad mood, loss of interest or pleasure and prominent anxiety or worry. Other symptoms may include disturbed sleep and appetite, dry mouth and poor concentration. However, the symptoms are not cyclical and are not associated with other symptoms of PMS such as breast tenderness and bloatedness.
Evidence base for over-the-counter medication
There are many drug and non-drug treatments advocated for the treatment of PMS, yet most lack evidence from well conducted randomised controlled trials. A lack of evidence or no evidence exists to support the use of reflexology, exercise, chiropractic manipulation, bright light therapy and relaxation. With regard to herbal, vitamin or mineral supplementation, only calcium supplements have good evidence of effectiveness (Whelan et al 2009). Calcium supplementation at doses of 1200 mg per day for 3 months has shown that overall PMS symtoms are significantly reduced in the luteal phase compared to placebo (Ward & Holimon 1999).
Trials involving vitamin B6 have shown that overall symptoms of PMS improve over a period of 2 to 6 months and also help with behavioural/mood symptoms such as depression (Wyatt et al 1999). Caution is needed in the reviews findings as most included trials were of poor quality.
Practical prescribing and product selection
Prescribing information relating to medicines for PMS reviewed in the section ‘Evidence base for over-the-counter medication’ is discussed and summarised in Table 5.13.
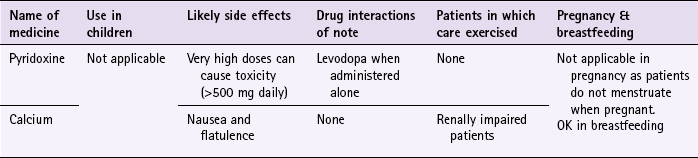
Calcium
Calcium supplementation should provide at least 1200 mg of elemental calcium per day. It is important to ensure that a product taken by the patient provides the required amount of elemental calcium. For example, a calcium lactate 300 mg tablet provides only 39 mg of elemental calcium; calcium carbonate 1.25 g tablets (e.g. Calcichew) provide 500 mg of elemental calcium per tablet. Calcium supplements can cause mild gastrointestinal disturbances such as nausea and flatulence. If the patient is taking tetracycline antibiotics or iron then a 2-hour gap should elapse between doses to avoid decreased absorption of the antibiotic or iron.
Vitamin B6 (pyridoxine)
There is no definitive dose of vitamin B6 required to alleviate symptoms of PMS. However, doses of up to 100 mg daily have been shown to help reduce symptoms. Side effects are extremely rare with doses at this level, although at higher doses it can cause numbness and peripheral neuropathy. A number of drug interactions have been observed in patients taking vitamin B6, most notably phenytoin, phenobarbital and levodopa. Only the vitamin B6/levodopa interaction is significant and should be avoided. Although doses as low as 5 mg vitamin B6 will reduce the effects of levodopa, the problem of this interaction in clinical practice is almost always negated as combinations of levodopa/carbidopa (Sinemet) or levodopa/benserazide (Madopar) are unaffected by vitamin B6.
References
Ward, MW, Holimon, TD. Calcium treatment for premenstrual syndrome. Ann Pharmacother. 1999;33:1356–1358.
Whelan, AM, Jurgens, TM, Naylor, H. Herbs, vitamins and minerals in the treatment of premenstrual syndrome: a systematic review. Can J Clin Pharmacol. 2009;16(3):e407–e429.
Wyatt, KM, Dimmock, PW, Jones, PW, et al. Efficacy of vitamin B-6 in the treatment of premenstrual syndrome: systematic review. Br Med J. 1999;318:1375–1381.
RCOG, Management of premenstrual syndrome. 2007. Royal College of Obstetricians and Gynaecologists. Available at. http://www.rcog.org.uk/files/rcog-corp/uploaded-files/GT48ManagementPremensturalSyndrome.pdf. (accessed 7 November 2012)
Gianetto-Berruti, A, Feyles, V. Premenstrual syndrome. Minerva Ginecol. 2002;54:85–95.
Thys-Jacobs, S, Starkey, P, Bernstein, D, et al. Calcium carbonate and the premenstrual syndrome: effects on premenstrual and menstrual symptoms. Am J Gynecol. 1998;179:444–452.
Heavy menstrual bleeding (menorrhagia)
Background
NICE guidance (January 2007) defines heavy menstrual bleeding (HMB) as ‘excessive menstrual blood loss which interferes with a woman’s physical, social, emotional and/or material quality of life, and which can occur alone or in combination with other symptoms’. Other definitions exist and include excessive menses in an otherwise normal menstrual cycle that are associated with clots, the use of towels rather than tampons and dysmenorrhoea. Blood loss can be measured and is used in research (menorrhagia is defined as 60 to 80 mL of blood loss per cycle) but is impractical in a clinical setting. Although heavy blood loss is rarely associated with sinister pathology the impact on quality of life can be considerable.
Prevalence and epidemiology
The prevalence of HMB is difficult to establish due to varying definitions. However, 5% of women aged between 30 and 49 years old consult their GP each year (Vessey et al 1992) and a third of women describe their periods as heavy.
Aetiology
In approximately half of cases no identifiable cause can be found for HMB. Identifiable causes can result from uterine and pelvic pathology (e.g. fibroids, polyps and carcinoma), systemic disorders (e.g. hypothyroidism) and iatrogenic factors (e.g. medication and intrauterine devices).
Arriving at a differential diagnosis
The main consideration of the community pharmacist is to exclude sinister pathology. A detailed history of the patient’s menstrual cycle is essential. Asking symptom-specific questions will help the pharmacist to determine if referral is needed (Table 5.14).
Table 5.14
Specific questions to ask the patient: HMB
| Question | Relevance |
| Timing of bleeding | Symptoms that might suggest structural or pathological abnormality include bleeding at times other than menses |
| Effect on quality of life | An assessment should be made to determine what effect menstrual bleeding is having on the patient |
| Symptoms in relation to normal cycles | Patients will show cycle-to-cycle variation in the amount of blood loss. It is important to discuss with the patient this normal variation and to determine from the patient if she feels blood loss is within the normal range |
Clinical features of HMB
The key symptom will be blood loss that is perceived to be greater than normal. The patient’s bleeding pattern should be the same as during normal menses but heavier.
Conditions to eliminate
Medicine-induced menstrual bleeding
Occasionally, medicines can change menstrual bleeding patterns (Table 5.15). If an adverse drug reaction is suspected then the pharmacist should contact the prescriber and discuss other treatment options. Additionally, the incidence of menstrual pain is higher in patients who have had an intrauterine device fitted.
 Table 5.15
Table 5.15Endometrial and cervical carcinoma
Characterised by inappropriate uterine bleeding, and usually occurs in postmenopausal women. Bleeding starts as slight and intermittent but over time becomes heavy and continuous. Discharge and pain are rare. Irregular bleeding between periods, especially if associated with postcoital bleeding, is extremely significant and suggests pre-cancerous/cancer of the cervix.
Evidence base for over-the-counter medication
Tranexamic acid has been in clinical use in the UK for approximately 30 years and has established itself as a clinically effective medicine in decreasing menstrual blood loss. It reduces blood loss by up to 50%.
Practical prescribing and product selection
Tranexamic acid is an antifibrinolytic and stops the conversion of plasminogen to plasmin – an enzyme that digests fibrin and thus brings about clot dissolution. NICE guidance states that if the patient history suggests no abnormalities then drug treatment can be given (Hints and Tips Box 5.4). This is either hormonal (currently still POM) or non-hormonal (NSAIDs or tranexamic acid). In common with more recent POM to P deregulations the manufacturer has produced guidance for pharmacy staff and placed certain restrictions on its sale over the counter (see http://www.femstrual.co.uk/pharmacy/femstrual-protocol.html). As an OTC product it is restricted to women with a history of heavy bleeding who have regular (21–35 day) cycles that show no more than 3 days individual variability in cycle duration.
Tranexamic acid (e.g. Femstrual)
Tranexamic acid should be taken once bleeding starts. The dose is two tablets 3 times a day for a maximum of 4 days. The dose can be increased to two tablets 4 times a day in very heavy menstrual bleeding. The maximum dose is eight tablets (4 g) daily. Side effects are unusual. Those reported include mild nausea, vomiting and diarrhoea (affecting between 1 and 10% of patients).
Visual disturbances and thromboembolic events have been reported but are very rare. The causal relationship of thromboembolic events and tranexamic acid is unclear and NICE guidance states that no increase in the overall rate of thrombosis has been identified with those taking tranexamic acid. Nevertheless, women at high risk of thrombosis have been excluded from pharmacy supply. Tranexamic acid should not be taken in patients on anticoagulants, taking the combined oral contraceptive, unopposed oestrogen or tamoxifen. In breastfeeding, one small unpublished study suggests that only low levels of tranexamic acid pass into breast milk and that waiting 3–4 hours before breastfeeding will minimise any risk.
References
NICE guidelines. Heavy menstrual bleeding (Jan 2007). Available from http://www.nice.org.uk/guidance/index.jsp?action=byID&o=11002. [(accessed 7 November 2012)].
Vessey, MP, Villard-Mackintosh, L, McPherson, K, et al. The epidemiology of hysterectomy: findings in a large cohort study. Br J Obstet Gynaecol. 1992;99(5):402–407.
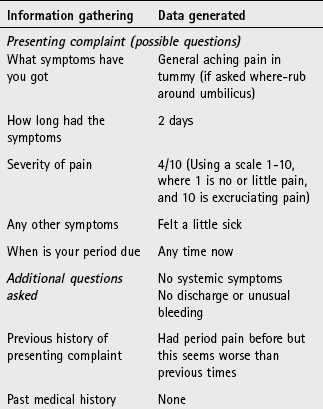
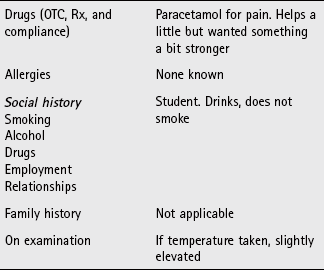
The following questions are intended to supplement the text. Two levels of questions are provided; multiple choice questions and case studies. The multiple choice questions are designed to test factual recall and the case studies allow knowledge to be applied to a practice setting.
Multiple choice questions
5.1. Primary dysmenorrhoea affects?
5.2. When do PMS symptoms usually begin?
5.3. What percentage of women of childbearing age will experience an episode of thrush?
5.4. What medication can precipitate thrush?
5.5. Which condition predisposes patients to pyelonephritis?
5.6. Dysuria accompanied with fever and flank pain is indicative of?
5.7. What symptoms are commonly associated with primary dysmenorrhoea?
a. Lower abdominal cramping pain that starts 7 to 10 days before onset of the period
b. Lower abdominal cramping pain that starts 2 to 3 days before onset of period
c. Lower abdominal cramping pain that starts 6 to 12 hours before onset of period
d. Lower abdominal griping pain that starts 2 to 3 days before onset of period
e. Lower abdominal griping pain that starts 6 to 12 hours before onset of period
5.8. Which of the following medicines can interact with phenytoin?
Questions 5.9 to 5.11 concern the following patient groups:
Select, from A to E, which of the patient groups:
5.9. Are most likely to suffer from endometriosis
5.10. Are unlikely to suffer from cystitis
5.11. Should be referred automatically if they have vaginal discharge
Questions 5.12 to 5.14 concern the following conditions:
Select from A to E, which of the conditions:
Questions 5.15 to 5.17: for each of these questions one or more of the responses is (are) correct. Decide which of the responses is (are) correct. Then choose:
5.15. A pharmacist should refer patients with vaginal candidiasis when:
5.16. Which of the following symptoms are associated with premenstrual syndrome?
5.17. Which of the following medicines can cause menstrual bleeding?
Questions 5.18 to 5.20: these questions consist of a statement in the left-hand column followed by a statement in the right-hand column. You need to:
A If both statements are true and the second statement is a correct explanation of the first statement
B If both statements are true but the second statement is NOT a correct explanation of the first statement
C If the first statement is true but the second statement is false
D If the first statement is false but the second statement is true
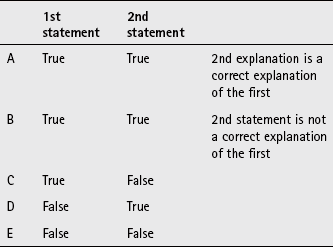
| First statement | Second statement |
| 5.18 Cystitis is uncommon in men | They have a shorter urethra than women |
| 5.19 Vaginal discharge is uncommon in children under 12 | Antibiotic therapy may precipitate attacks in this age group |
| 5.20 Imidazoles have similar cure rates | Symptoms tend to resolve in about 3 days |