Cranial Nerves
The Eye 1 – Pupils, Acuity, Fields
BACKGROUND
Examination of the eye can provide very many important diagnostic clues for both general medical and neurological diseases.
Examination can be divided into:
3 Acuity
Abnormalities may arise from:
• Ocular problems, such as dense cataracts (lens opacities). These are not correctable with glasses but are readily identifiable on ophthalmoscopy.
• Optical problems: abnormalities of the focal length of the focusing system in the eye, commonly called long- or short-sightedness. These can be corrected by glasses or by asking the patient to look through a pinhole.
• Retinal or retro-orbital abnormality of vision which cannot be corrected using lenses. Retinal causes are often visible on ophthalmoscopy.
It is essential to test acuity with the patient's correct glasses.
4 Fields
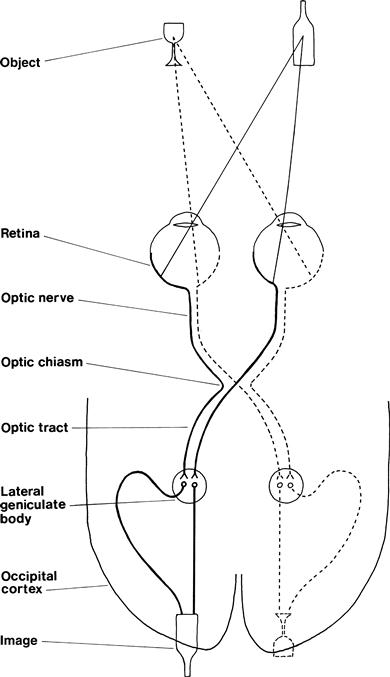
The organisation of the visual pathways means different patterns of visual field abnormality arise from lesions at different sites. The normal visual pathways are given in Figure 7.1.
The visual fields are divided vertically through the point of fixation into the temporal and nasal fields. Something on your right as you look ahead is in the temporal field of your right eye and the nasal field of your left eye.
The visual fields are described from the patient's point of view.
Field defects are said to be homonymous if the same part of the visual field is affected in both eyes. This can be congruous (the field defects in both eyes match exactly) or incongruous (the field defects do not match exactly).
Testing the fields is very useful in localisation of a lesion (Table 7.1).
Table 7.1
| Type of defect | Site of lesion |
| Monocular field defect | Anterior to optic chiasm |
| Bitemporal field defect | At the optic chiasm |
| Homonymous field defect | Behind the optic chiasm |
| Congruous homonymous field defect | Behind the lateral geniculate bodies |
The normal visual fields for different types of stimuli are very different. The normal field for moving objects or large objects is wider than for objects held still or small objects. The normal field for recognition of coloured objects is more limited than for monochrome. It is useful to test this on yourself. Look straight into the distance in front of you and put your hands out straight to your side. Wiggle your fingers and, keeping your arms straight, gradually bring your arms forward until you can see your moving fingers. Repeat this holding a small white object, and then with a red object until you can see that it is red. You will appreciate the different normal fields for these different stimuli.
1 GENERAL
WHAT TO DO
Look at the patient's eyes and note any difference between the two sides.
Look at the level of the eyelid; particularly note asymmetry.
• If an eyelid is lower than normal, this is referred to as ptosis; it can be partial or complete (if eye is closed).
• If an eyelid is higher than normal, usually above the level of the top of the iris, this is described as lid retraction.
Look at the position of the eye.
• Is there protrusion (exophthalmos) or does the eye appear sunken (enophthalmos)? If you are considering exophthalmos, it is confirmed if the front of the orbital globe can be seen when looking from above.
Beware the false eye—usually obvious on closer inspection.
WHAT IT MEANS
• Ptosis. Common causes: congenital, Horner's syndrome (ptosis always partial), third nerve palsy (ptosis often complete) (see below); in older patients, the levator muscles can become weak or detached from the lid, producing age-related ptosis. Rarer causes: myasthenia gravis (ptosis often variable), myopathy.
• Exophthalmos. Common causes: most frequently, dysthyroid eye disease—associated with lid retraction. Rarely: retro-orbital mass.
2 PUPILS
WHAT TO DO IN A CONSCIOUS PATIENT
(For pupillary changes in an unconscious patient, see Chapter 27.)
Look at the pupils.
• Are they regular in outline?
• Are there any holes in the iris or foreign bodies (e.g. lens implants) in the anterior chamber?
Shine a bright light in one eye.
• Look at the reaction of that eye—the direct reflex—and then repeat and look at the reaction in the other eye—the consensual reflex.
• Ensure that the patient is looking into the distance and not at the light.
Place your finger 10 cm in front of the patient's nose. Ask the patient to look into the distance and then at your finger.
Look at the pupils for their reaction to accommodation.
FURTHER TESTING
Swinging light test
What to do
Shine a bright light into one eye and then the other at about 1-second intervals. Swing the light repeatedly between the two. Observe the pupillary response as the light is shone into the eye.
What you find and what it means
• The pupil constricts as the light is shone into it repeatedly: normal.
• The pupil on one side constricts when the light is shone into it and the pupil on the other side dilates when the light is then shone into it: the side that dilates has a relative afferent pupillary defect (often abbreviated to RAPD). This is also sometimes called the Marcus Gunn pupil. N.B. This lesion is always unilateral.
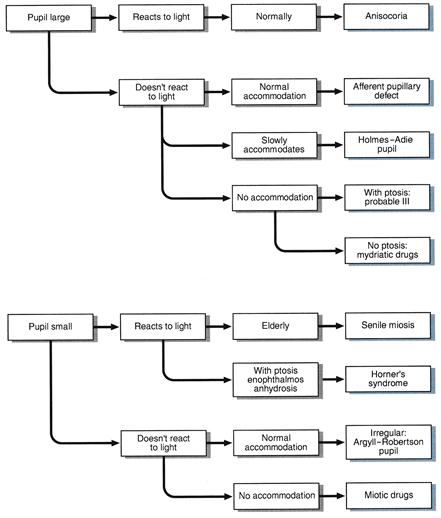
WHAT IT MEANS
• Anisocoria: pupils unequal but normally reacting—normal variant.
• Senile miosis: normal age-related change.
• Holmes–Adie pupil: degeneration of ciliary ganglion of unknown cause; may be associated with loss of tendon reflexes.
• Afferent pupillary defect: lesion anterior to the optic chiasm. Common cause: optic neuritis. Rarer causes: compression of the optic nerve, retinal degenerations.
• Relative afferent pupillary defect: partial lesion anterior to the optic chiasm. Causes: as for afferent pupillary defects.
• Horner's syndrome (miosis, partial ptosis, enophthalmos and loss of hemifacial sweating): lesion to sympathetic fibres. This may occur:
– Centrally: in the hypothalamus, the medulla or the upper cervical cord (exits at T1). Common cause: stroke (N.B. lateral medullary syndrome), demyelination. Rarely: trauma or syringomyelia.
– Peripherally: in the sympathetic chain, in the superior cervical ganglion or along the carotid artery. Common causes: Pancoast's tumour (apical bronchial carcinoma), trauma. Rare cause: carotid dissection. Sometimes no cause is found.
• Argyll–Robertson pupil: probably an upper midbrain lesion; now very rare. Common causes: syphilis, diabetes mellitus. Rarely: multiple sclerosis (MS).
3 ACUITY
WHAT TO DO AND WHAT YOU FIND
Can the patient see out of both eyes?
Acuity can be tested in several ways.
(i) Using Snellen's chart
• Stand the patient 6 m from a well-lit chart. Ask him to read down from the largest letters to the smallest.
• Record the results: distance in metres or feet from chart; distance in metres or feet at which letters should be seen.
For example: 6/6 when the letter is read at the correct distance or 6/60 when the largest letter (normally seen at 60 m) is read at 6 m, or 20/20 and 20/200 when these acuities are measured in feet.
(ii) Using a near vision chart (Fig. 7.3)
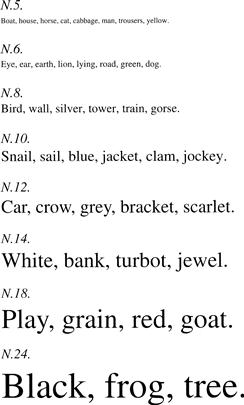
(iii) Using bedside material such as newspapers
Test as in (ii) and record the type size read (e.g. headlines only, all print).
If unable to read largest letters:
See if the patient can:
• Count fingers. Ask how many fingers you are holding up.
• See hand movements. Ask him to say when you move your hand in front of his eye.
• Perceive light. Ask him to say when you shine a light in his eye.
Ask the patient to look through a pinhole made in a card.
If acuity improves, the visual impairment is refractive in origin and not from other optical or neurological causes.
A new development
Ophthalmologists are increasingly using LogMAR (logarithm of the minimum angle of resolution) charts to measure acuity. There are a number of different LogMAR chart designs. They are read in the same way as a Snellen chart. However, the result is expressed as the logarithm of the minimum angle or resolution, which in turn is the inverse of the Snellen ratio. For example, for Snellen acuities:
4 FIELDS
WHAT TO DO
Assess major field defects
• Ask the patient to look with both eyes at your eyes.
• Put your hands out on both sides approximately 50 cm apart and approximately 30 cm above eye level. Extend your index finger (Fig. 7.4). Your fingers should now be in the patient's upper temporal fields on both sides.
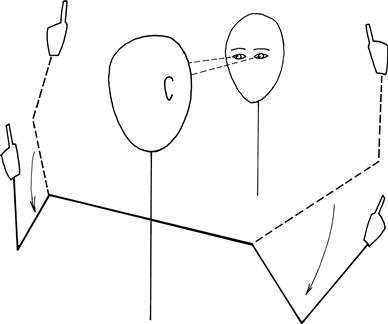
• Ask the patient to indicate which index finger you move: right, left or both.
If one side is ignored when both fingers are moved together but is seen when moved by itself, then there is visual inattention.
Test each eye individually
What to test with?
Large objects are more easily seen than small objects; white objects are more easily seen than red. Thus, fields will vary according to the size and colour of the target used.
Central vision is colour (cones) and peripheral vision is monochrome (rods).
A combination of wiggling fingers (described above) and red pin provide the most sensitive and specific bedside test for field defects.
• Sit just under one arm's length away from the patient at the same level.
• Cover the patient's right eye and ask him to look at your right eye with his left eye. This is so you are certain of his point of fixation throughout the test.
• Tilt the patient's head to get the eyebrows and nose out of the way.
Using a red pin (recommended):
• Imagine there is a plane, like a vertical sheet of glass, halfway between you and the patient (Fig. 7.5A). You are going to compare your visual field on that plane with the patient's visual field on that plane. The field to red is about 30–40 degrees from the point of fixation.
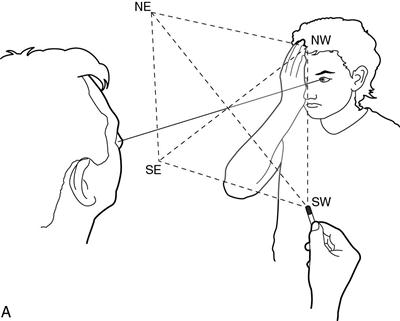
• Hold the red pin within that plane beyond where you can see it as red. Move it within the plane towards the point of fixation. Ask the patient to tell you when he can see it as red.
• Bring the pin slowly from four directions: northeast, northwest, southeast and southwest (where north/south is the vertical). Compare the patient's visual field to your own.
• To find the blind spot, move the pin from the point of fixation halfway between you, laterally along the horizontal meridian until you find your own blind spot. Ask the patient to tell you when the pin disappears.
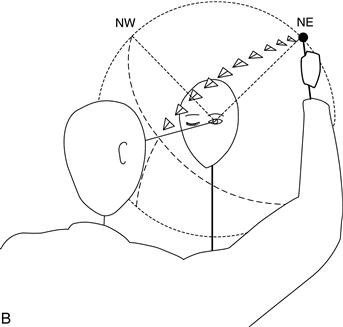
Alternative technique using a white pin:
• Imagine a sphere of radius 30 cm centred on the patient's eye.
• Bring a white pin in towards the line of fixation along an arc of a sphere centred on the patient's eye (Fig. 7.5B).
• Ensure the pin cannot be seen where you start (usually behind the plane of the eyes). Ask the patient to tell you when he first sees the pin.
• Initially bring the pin slowly from four directions, northeast, northwest, southeast and southwest (where north/south is the vertical).
Once you find a field defect
Define the edges.
Bring the pin from where it cannot be seen to where it can be seen.
When there is a homonymous hemianopia
The macula needs to be tested.
Bring the pin horizontally from the side with the defect towards the point of fixation.
• If the pin is seen before it gets to the midline, there is macular sparing.
• If the pin is only seen once it crosses the midline, there is no macular sparing.
Describe the field loss from the patient's point of view.
Central field defects—scotomas—and the blind spot (the field defect produced by the optic disc) are usually found using a red pin.
 TIP
TIP
If a patient complains of a hole in his visual field, it is often easier to give him the pin and ask him to place it in the hole in his vision.
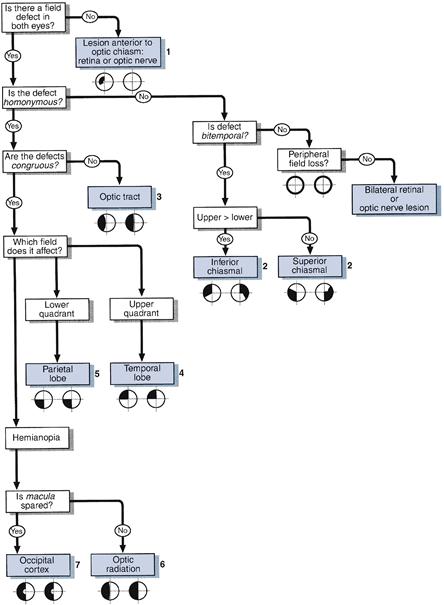
WHAT YOU FIND
See Figure 7.7.
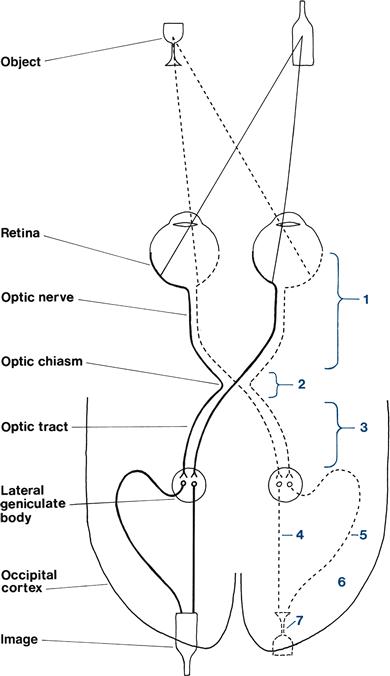
Figure 7.7 Visual pathways with sites of lesions marked. Numbers match those in Figure 7.6
(i) Defect limited to one eye
Constricted field
• Tubular vision: the size of the constricted field remains the same regardless of the distance of the test object from the eye.
• Scotoma: a hole in the visual field—described by its site (e.g. central or centrocaecal— defect connecting the fixation point to the blind spot) and shape (e.g. round or ring-shaped).
• Altitudinal defect: a lesion confined to either the upper or the lower half of the visual field but crossing the vertical meridian.
(ii) Defect affecting both eyes
• Bitemporal hemianopias: defect in the temporal fields of both eyes. Note carefully if the upper or lower quadrant is more marked.
• Homonymous quadrantanopias: defect in the same quadrant of vision of both eyes. Classified as congruous or incongruous (see above).
• Homonymous hemianopias: defect in the same hemifield in both eyes. Classified according to degree of functional preservation in the affected field (e.g. able to see moving targets), whether congruous or incongruous, and whether macula-sparing or not.
Describe your findings: for example, ’This man has normal pupillary response to light and accommodation. His visual acuities are 6/6 on the right and 6/12 on the left. He has a right homonymous hemianopia which is congruous and macula-sparing.‘
WHAT IT MEANS
See Figures 7.6 and 7.7.
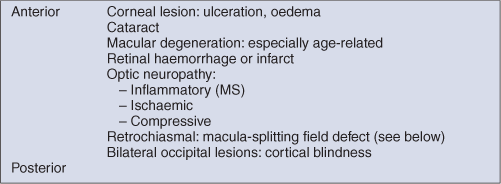
(i) Defect limited to one eye: indicates ocular, retinal or optic nerve pathology.
• Constricted field: chronic papilloedema, chronic glaucoma.
• Tubular vision: does not indicate organic disease—suggests conversion disorder.
• Scotoma: MS, toxic optic neuropathy, ischaemic optic neuropathy, retinal haemorrhage or infarct.
• Enlarged blind spots: papilloedema.
• Altitudinal defects: suggest vascular cause (retinal infarcts or ischaemic optic neuropathy).
(ii) Defect affecting both eyes: indicates a lesion at or behind the optic chiasm, or bilateral prechiasmal lesions.
– Upper quadrant > lower: inferior chiasmal compression, commonly a pituitary adenoma
– Lower quadrant > upper: superior chiasmal compression, commonly a craniopharyngioma.
The common causes for the lesions referred to below are cerebral infarcts, haemorrhages, tumours or head injuries.