Cranial Nerves IX, X, XII
The Mouth
MOUTH AND TONGUE: WHAT TO DO
Ask the patient to open his mouth.
Ask the patient to put out his tongue.
MOUTH: WHAT YOU FIND AND WHAT IT MEANS
• Gum hypertrophy: phenytoin therapy.
• Red, ‘beefy’ tongue: vitamin B12 deficiency.
• Large tongue: amyloidosis, acromegaly, congenital hypothyroi- dism.
• Saliva pooling in mouth: indicates swallowing difficultly.
• Small tongue: with fasciculations = bilateral lower motor neurone lesion; motor neurone disease (progressive bulbar palsy type), basal meningitis, syringobulbia.
• Small tongue: with reduced speed of movements = bilateral upper motor neurone lesion—often associated with labile emotions, increased jaw jerk: pseudobulbar palsy.
• Small tongue: with fasciculations and reduced speed of movements = mixed bilateral upper and lower motor neurone lesions; motor neurone disease (progressive bulbar palsy type).
• Tongue deviates to one side = weakness on the side it moves towards.
– With unilateral wasting and fasciculation: unilateral lower motor neurone disease (rare). Causes: syringomyelia, basal meningitis, early motor neurone disease, foramen magnum tumour.
– With normal bulk: unilateral upper motor neurone weakness (common)—associated with hemiparesis: strokes, tumours.
• Tongue moves in and out on protrusion (‘trombone’ tremor): cerebellar disease, essential tremor, extrapyramidal syndromes.
PHARYNX: WHAT TO DO
Look at the position of the uvula.
If you cannot see the uvula, use a tongue depressor.
Ask the patient to say ‘Ahh’.
Look at the uvula.
Additional testing:
If the patient is alert and co-operative and sitting up and swallowing appears safe, ask the patient to swallow (provide a glass of water).
GAG REFLEX: WHAT TO DO
Afferent: glossopharyngeal nerve. Efferent: vagus.
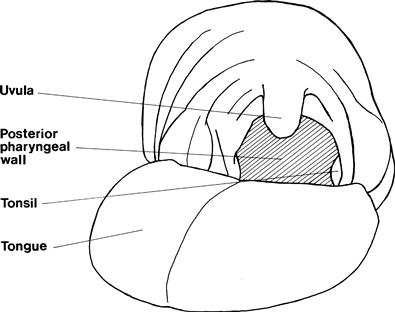
• Touch the pharyngeal wall behind the pillars of the fauces (Fig. 13.1).
• Watch the uvula; it should lift following the stimulus.
• Ask the patient to compare the sensation between two sides.
LARYNX: WHAT TO DO
Ask the patient to cough.
Listen to the onset.
Listen to the speech (see Chapter 3).
Laryngoscopy
Direct visualisation of the vocal cords can be achieved through laryngoscopy, which allows the position of the vocal cords and their movement to be assessed. This normally requires an ENT opinion.
LARYNX: WHAT YOU FIND
• Gradual-onset cough—bovine cough: suggests vocal cord palsy.
• Bubbly voice and cough: suggests combined cord palsy and pharyngeal pooling due to X nerve lesion.
• Swallow followed by coughing indicates aspiration due to poor airway protection: suggests X nerve lesion.
• Unilateral cord palsy: recurrent laryngeal palsy or vagal lesion.
PHARYNX AND LARYNX: WHAT IT MEANS
• Tenth nerve palsy may be due to lesions in the medulla: look for associated ipsilateral cerebellar signs, loss of pain and temperature in the face on the same side and on the body on the opposite side, and an ipsilateral Horner's (lateral medullary syndrome).
– Extramedullary and intracranial: look for associated XI cranial, IX cranial nerves.
– N.B. Left-sided recurrent laryngeal palsy may arise from mediastinal or intrathoracic pathology.
• Bilateral lower motor neurone X occurs in progressive bulbar palsy (a variant of motor neurone disease (MND)): look for associated tongue fasciculations and mixed upper and lower motor neurone signs without sensory loss in the limbs.
• Bilateral pharyngeal weakness and/or bilateral vocal cord weakness can also occur in myasthenia gravis. This weakness is usually fatigable.