Motor System
Reflexes
BACKGROUND
A tendon reflex results from the stimulation of a stretch-sensitive afferent from a neuromuscular spindle which, via a single synapse, stimulates a motor nerve, leading to a muscle contraction. Tendon reflexes are increased in upper motor neurone lesions and decreased in lower motor neurone lesions and muscle abnormalities.
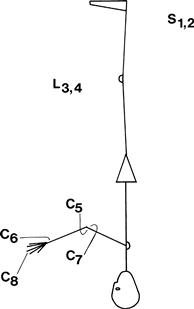
The root values for the reflexes can be recalled by counting from the ankle upwards (Fig. 19.1).
Reflexes can be graded:
WHAT TO DO
Use the whole length of the patella hammer; let the hammer swing. Ensure the patient is relaxed. Avoid telling the patient to relax, as this is guaranteed to produce tension.
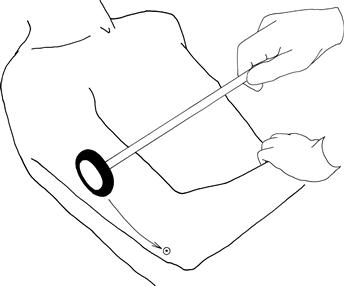
Biceps
Place the patient's hands on his abdomen. Place your index finger on the biceps tendon; swing the hammer on to your finger while watching the biceps muscle (Fig. 19.2).
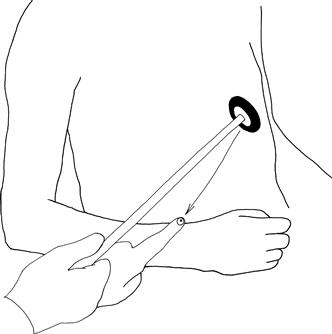
Supinator
(N.B. Bad name for this reflex; the muscle involved is brachioradialis.)
Place the arm flexed on to the abdomen, place the finger on the radial tuberosity, hit the finger with the hammer and watch the brachioradialis (Fig. 19.3).
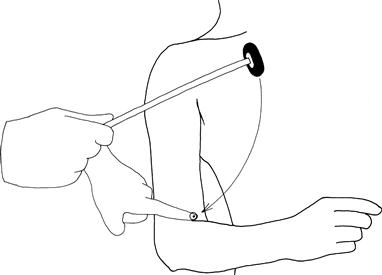
Triceps
Draw the arm across the chest, holding the wrist with the elbow at 90 degrees. Strike the triceps tendon directly with the patella hammer; watch the muscle (Fig. 19.4).
Finger reflex
Hold the hand in the neutral position, place your hand opposite the fingers and strike the back of your fingers.
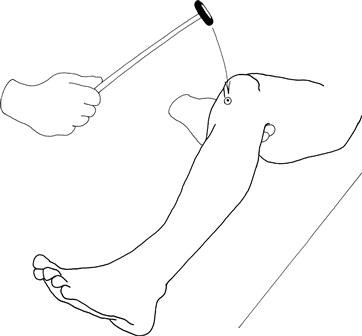
Knee reflex
Place the arm under the knee so that the knee is at 90 degrees. Strike the knee below the patella; watch the quadriceps (Fig. 19.5).
Ankle reflex
Hold the patient's foot at 90 degrees with a medial malleolus facing the ceiling. The knee should be flexed and lying to the side. Strike the Achilles tendon directly. Watch the muscles of the calf (Fig. 19.6A).
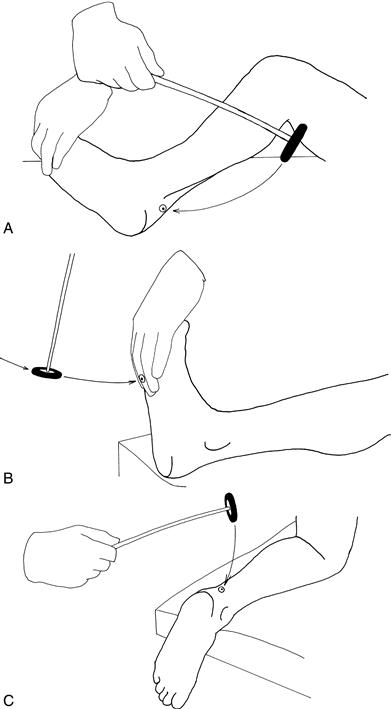
Ankle reflex alternatives
1. With the patient's legs straight, place your hand on the ball of his foot with the ankles at 90 degrees. Strike with your hand and watch the muscles of the calf (Fig. 19.6B).
2. Ask the patient to kneel on a chair so that his ankles are hanging loose over the edge. Strike the Achilles tendon directly (Fig. 19.6C).
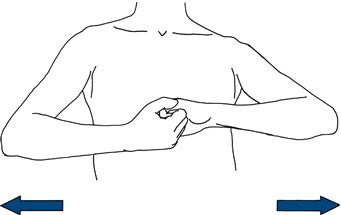
Reinforcement
If any reflex is unobtainable directly, ask the patient to perform a reinforcement manœuvre. For the arms, ask the patient to clench his teeth as you swing the hammer. For the legs, ask the patient either to make a fist, or to link hands across his chest and pull one against the other, as you swing the hammer (Fig. 19.7).
 TIP
TIP
An absent reflex sounds dull. It's worth listening as well as watching.
WHAT YOU FIND AND WHAT IT MEANS
• Increased reflex or clonus: this indicates an upper motor neurone lesion above the root at that level.
– generalised: indicates peripheral neuropathy
– isolated: indicates either a peripheral nerve or, more commonly, a root lesion
– bilateral absent ankle reflexes: most commonly indicates a peripheral neuropathy; also occurs with bilateral S1 nerve root lesions or, very rarely, bilateral sciatic nerve lesions.
• Reduced reflexes (more difficult to judge): occurs in a peripheral neuropathy, muscle disease and cerebellar syndrome. N.B. Reflexes can be absent in the early stages of severe upper motor neurone lesion: ‘spinal shock’.
• Reflex spread: the reflex tested is present but this response goes beyond the muscle normally seen to contract; for example, the fingers are seen to flex when the supinator reflex is tested or the hip adductors are seen to contract when testing the knee reflex. Reflex spread indicates an upper motor neurone lesion occurring above the level of innervation of the muscle to which the reflex spread.
• An inverted reflex: a combination of loss of the reflex tested with reflex spread to muscle at a lower level. The level of the absent reflex indicates the level of the lesion. For example, a biceps reflex is absent but produces a triceps response. This indicates a lower motor neurone lesion at the level of the absent reflex (in this case C5) with an upper motor neurone lesion below indicating spinal cord involvement at the level of the absent reflex.
• Pendular reflex: this is usually best seen in the knee jerk where the reflex continues to swing for several beats. This is associated with cerebellar disease.
• Slow relaxing reflex: this is especially seen at the ankle reflex and may be difficult to note. It is associated with hypothyroidism.
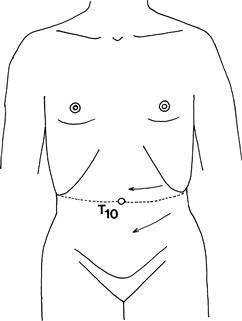
ABDOMINAL REFLEXES
What to do
Using an orange stick, lightly scratch the abdominal wall as indicated in Figure 19.8. Watch the abdominal wall; this should contract on the same side.
PLANTAR RESPONSE
What to do
Explain to the patient that you are going to stroke the bottom part of his foot. Gently draw an orange stick up a lateral border of the foot and across the foot pad. Watch the big toe and the remainder of the foot (Fig. 19.9).

What you find
• The toes all flex—flexor plantar response: negative Babinski's sign—normal.
• Hallux extends (goes up), the other toes flex or spread: extensor plantar response or positive Babinski's sign.
• Hallux extends (goes up), the other toes extend and ankle dorsiflexes: withdrawal response. Repeat more gently or try alternative stimuli (see below).
• No movement of the hallux (even if the other toes flex): indicates no response.