Reproductive System
On completion of chapter 10, the reader should be able to:
• Discuss the basic anatomic structures associated with the male and female reproductive systems.
• Briefly explain the role of general radiography, mammography, diagnostic medical sonography, computed tomography, and magnetic resonance imaging in the diagnosis and treatment of reproductive system disorders.
• Compare and contrast breast imaging modalities, including diagnostic versus screening mammography, localization techniques, and sonography.
• Differentiate among the major congenital anomalies of the female reproductive system.
• Describe the various neoplastic diseases of both the female and male reproductive systems in terms of etiology, incidence, signs and symptoms, treatment, and prognosis.
• Differentiate among the common disorders during pregnancy and explain the role of diagnostic medical sonography in the management of the gravid female.
FEMALE REPRODUCTIVE SYSTEM
The female reproductive system consists of one pair of ovaries, which are the primary sex organs, and the secondary sex organs, which include one pair of fallopian tubes, the uterus, the vagina, and two breasts (Fig. 10-1). The primary function of the system is to provide a female reproductive cell (the ovum), hormones, and a site for the development of the zygote.
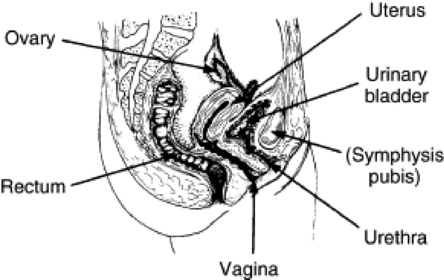
The external genitalia (the vulva) include the mons pubis, the labia majora and minora, the clitoris, the openings of the urethra and vagina, and the perineum. The vagina connects the external genitalia with the uterus and is the mode of exit for menstrual fluids and conception products.
The uterus is a pear-shaped organ whose primary purpose is to provide an environment for fetal growth and development. Located within the pelvic cavity, it can be divided into the upper portion, termed the fundus; themidportion, termed the body;and the lower portion, termed the cervix.The cervix connects the uterine cavity with the upper vagina. Anatomically the uterus is flexed so that the cervix and lower portion of the body lie anterior to the rectum. The body of the uterus follows the contour of the posterior urinary bladder wall. The upper portion, or fundus, normally lies superior to the bladder. The walls of the uterus include an inner, endometrial layer; a middle, muscular, myometrial layer; and an outer layer termed the parietal peritoneum.In actuality, the parietal peritoneum drapes over the fundus and upper three fourths of the body but does not enclose the lower fourth of the body or the cervix. The actual cavity within the uterus is fairly small and can be well visualized with ultrasonography. It is divided into the internal os, leading to the cervical canal, and the external os, which opens into the vagina. The uterus is held in place within the pelvic cavity via eight ligaments. Occasionally, lack of proper uterine support is present, and a device known as a pessary(Fig. 10-2) is inserted into the vagina to provide proper support.

Fig. 10-2 A pessary, inserted into the vagina for uterine support, is readily visible on this abdominal radiograph of an 88-year-old woman.
The fallopian tubes extend from the upper, outer edges of the uterus and expand distally into the infundibulum located close to, but not attached to, the ovaries. Suspended in place by the broad ligament, they are 8 to 12 cm long and tend to fall behind the uterus. These tubes serve as a passageway for the mature ova and are the normal site of fertilization. In a normal pregnancy the fertilized ovum continues to travel through the fallopian tube and implants into the endometrium of the uterus.
The ovaries are the primary reproductive glands and are responsible for ovulation and for secretion of estrogen and progesterone. Attached to the broad ligament and the posterior uterine wall, each ovary contains numerous graafian follicles enclosing ova. After puberty, several graafian follicles and ova grow and develop each month. Normally only one follicle matures, migrates to the surface of the ovary, and degenerates, thus expelling a mature ovum. This is termed ovulation.
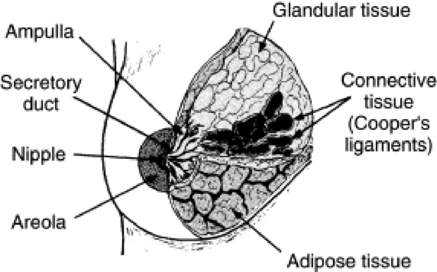
The breasts, like the fallopian tubes, uterus, and vagina, are also secondary sex organs. Breast parenchyma differs according to age and parity. Women in their 20s and 30s, especially nulliparous women, have dense, fibroglandular parenchyma that may hide breast masses on both physical and mammographic examination. However, as age and parity increase, the breast tissue undergoes what is known as involutional change.Involution is the conversion of glandular breast tissue into adipose tissue. As a result of this slow process, the breast changes its architecture and fibroglandular tissue is replaced with fat. Usually this process begins at the back of the breast and progresses forward to the nipple. Involution aids the radiographer and the interpreting physician because fatty tissue is radiolucent and enhances the radiographic visibility of many breast masses.
Anatomically the breasts are attached via connective tissue to the pectoral muscles that give the breast its contour and shape. The breast consists of about 12 lobes separated by connective tissue, much like the spokes of a wheel. The lobes are further divided into lobules clustered around small ducts. These small ducts join to form larger ducts, which terminate at the nipple (Fig. 10-3). The breasts function as accessory reproductive glands to secrete milk for the newborn infant. During pregnancy, changes in the estrogen and progesterone levels prepare the breasts for lactation. Approximately 3 days after delivery, a lactogenic hormone stimulates the secretion of milk.
IMAGING CONSIDERATIONS
One of the most common radiographic studies of the female reproductive system is the hysterosalpingogram.It is an examination performed for screening of the nongravid(nonpregnant) woman, especially in cases of suspected infertility. A common finding in cases of infertility is nonpatent fallopian tubes. In addition, although it does not define the extent of certain conditions such as endometriosis, it is useful in revealing the shape of the uterus and certain characteristics of the fallopian tubes other than their patency. Hysterosalpingography is performed by injecting approximately 5 to 10 mL of an opaque medium into the uterine cavity. Spillage of the contrast media from the fallopian tubes indicates their patency (Fig. 10-4). Typically, hysterosalpingography is used for diagnostic purposes, but it can also be used therapeutically for restoring tubal patency or to dilate or stretch the fallopian tubes.

Fig. 10-4 Free spillage of contrast medium bilaterally in this 38-year-old woman indicates uterine tubes are open in this hysterosalpingogram.
An adjunct procedure that has potential to replace the conventional hysterosalpingogram is known as sonohysterography.This examination is similar to hysterosalpingography in procedural approach; however, with sonohysterography,normal saline is injected into the uterus instead of an iodinated contrast agent. Because saline is devoid of complications associated with iodinated contrast agents, the procedure may be better tolerated by the patient. The current application for sonohysterography has been the use of saline to pry apart the layers of the endometrium in order to reveal abnormalities within the uterus. The saline fluid is expelled via the fallopian tubes and can also indicate their patency. This procedure is viewed via the transvaginal sonographic probe as a physician injects the saline. With real-time images, the dynamics of the reproductive system can be assessed without radiation dose to the patient.
Mammography
The use of mammography as a diagnostic procedure for symptomatic patients is well documented. Mammography provides important information about specific clinical problems such as a breast mass, pain, nipple discharge, and abnormalities of the skin and lymph nodes. With modern mammographic equipment and techniques, radiation exposure is minimal, and there is no evidence to suggest significant risk to women over 35 years of age. If a risk does exist, it is thought to be so minimal that it has never been observed, only inferred, scientifically.
The use of mammography in asymptomatic patients for screening purposes is based on its ability to detect nonpalpable breast lesions at an early stage when they are too small to be identified by physical examination. Current literature suggests that mammography can detect some cancers 2 years before they are palpable; survival depends on tumor size and lymph node involvement. It is generally agreed that women 50 years of age and older should undergo regular mammographic screening, because in this age range the breast tissue is less sensitive to radiation and the incidence of breast cancer increases with age. This also takes advantage of the involutional process, making occult lesions easier to identify on a radiograph. The benefits far outweigh associated risks from radiation exposure.
Mammography is also a valuable examination tool in the detection and evaluation of breast disease in individuals with augmentation prostheses. Although experience with augmentation mammoplasty patients is limited, current research indicates that mammography can demonstrate both palpable and nonpalpable breast lesions. In order to provide screening mammography for these patients, it is important to displace the implant so that the native breast tissue can be imaged and assessed for disease. To demonstrate the underlying breast parenchyma in these individuals, implant displaced views are required. Technologists are encouraged to use the Eckland maneuver to displace the implant from the native breast tissue to radiograph as much native breast tissue as possible. The Eckland maneuver is accomplished by having the technologist apply pressure at the area of the nipple and then carefully begin to roll the native breast tissue away from the implant. The implant displaced view is performed for both the craniocaudal and mediolateral projections of the breast. Once the implant is pushed upward away from the native breast tissue, the compression paddle is used to continue to hold the implant so that the native breast tissue can be more fully imaged. Because of the variations in patients’ breast tissue and their implants, manual exposure techniques are commonly used.
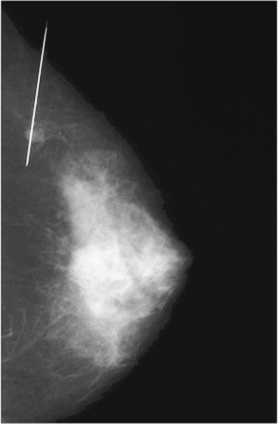
Needle guidewire localization is a specialized procedure to identify nonpalpable, mammographically detected abnormalities of the breast. It helps direct the surgeon to the lesion in question and allows excision of the suspect tissue for biopsy. Needle guidewire localizations cause minimal morbidity, with complications including hematoma formation, intraoperative wire dislodgement, and wire breakage. The development and refinement of localization techniques have greatly increased the percentage of positive findings on surgical biopsy and allow more accurate diagnosis and treatment of early-stage carcinoma of the breast. Fine-needle and large-core biopsy techniques offer an alternative to surgical biopsy as an initial step in investigation of breast masses. These procedures are performed on an outpatient basis by the mammographer and radiologist or surgeon in the mammography area using a specially designed stereotactic localization unit. Ductal lavage of the breast may also be performed in cases of suspected intraductal disease to obtain a specimen for laboratory analysis. Use of sonographic-guided aspiration and biopsy is also common because sonography has the ability to visualize the area in question and note whether the area has been completely removed while the needle or biopsy gun is still in situ. This may prevent additional punctures into the patient’s skin during the biopsy procedure.
Sonography
Sonography is the primary modality for examining the gravid and nongravid female reproductive system because of its excellent accuracy and because it presents no radiation hazards to the fetus or mother. Not only is sonography applicable in pregnancy, but it is also useful in normal gynecologic examinations to visualize reproductive organs or to follow the progress of a regimen of fertility medication.
The transabdominal pelvic sonogram requires a distended urinary bladder to serve as an “acoustic window” for good visualization of the pelvic organs. In addition, the fluid within the urinary bladder helps to displace bowel gas away from the area of interest. Sonography of the uterus and ovaries has been greatly enhanced by the use of a transvaginal transducer, which provides more accurate clinical information as a result of the magnification of obtained images of the internal pelvic structures. The most common indications for sonography in the nongravid female include evaluation of pelvic, uterine, and ovarian masses because sonography can give information about mass size, location, internal characteristics, and the effect on surrounding organs. Obstetrically, sonography is the method of choice in visualizing the position of the placenta, multiple gestations, and ectopic pregnancies, and determining gestational age. It is used to assist and guide the physician during amniocentesis and is invaluable in assessing fetal abnormalities such as anencephaly, hydrocephaly, congenital heart defects, polycystic kidney disease, urinary tract obstructions, and GI tract obstructions as well as determining fetal death.
Sonography is an excellent modality for differentiating cystic masses from solid masses within the breast. However, sonography has limitations in the diagnosis of malignant breast disease because of the solid nature of most breast cancers. Recently researchers and clinicians have made great strides in the use of sonography to evaluate the dense breast for disease. In order to reduce the radiation dose to these young patients, research continues in order to perfect an accurate and safe screening modality. However, currently breast sonography is not advocated as a screening modality for breast cancer because of the difficulty in consistently differentiating between a solid benign mass and malignant disease.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is now often used in conjunction with sonography in the evaluation of the female pelvis (Figs. 10-5 and 10-6). MRI, like sonography, uses no ionizing radiation and is noninvasive. MRI gives detailed information regarding pelvic, uterine, and ovarian masses (Fig. 10-7). In cases of ovarian cancer, MRI accurately demonstrates proliferation into other pelvic structures. In addition, multiple leiomyomas can be detected and localized in a short period of time.
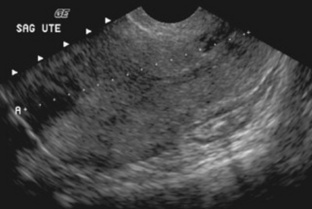
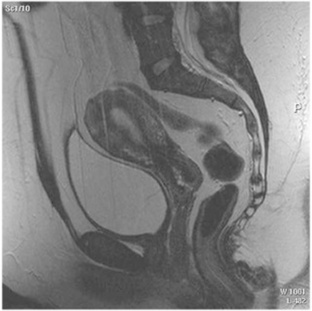
Fig. 10-6 An example of a sagittal T2-weighted magnetic resonance image of a normal female pelvis demonstrating the bladder and uterus.
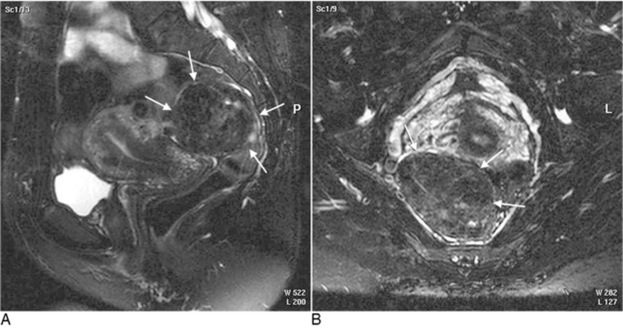
Fig. 10-7 AA sagittal T2 fat-suppressed magnetic resonance imaging (MRI) scan demonstrating a large mass, most likely a subserosal fibroid, posterior to the endocervical junction. B, An axial T2 fat-suppressed MRI image depicting the large subserosal fibroid shown in A.
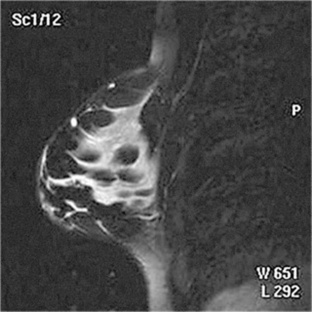
MRI is increasingly being used to assist in differentiating between malignant and benign solid lesions within the breast. Fat suppression imaging is used before and after contrast enhancement. This technique suppresses the normal, fatty tissue of the breast, allowing easier identification of malignant masses through contrast enhancement (Fig. 10-8). MRI is also used to detect faulty or leaking breast implants. Again, fat suppression imaging is used to suppress the normal breast tissue and detect the presence of silicone in the surrounding tissues.
Computed Tomography
Computed tomography (CT) of the pelvis and abdomen is often performed to diagnose diseases of the female and male reproductive systems. It is quite helpful in assessing neoplastic growth and abscess formation resulting from inflammatory processes. It is often used in conjunction with transvaginal sonography to evaluate ovarian lesions, especially cystic teratomas in females, and is used extensively in staging female reproductive cancers. In the male patient, CT is also used in conjunction with sonography to demonstrate anomalies of the seminal vesicles and prostate gland. CT–positron emission tomography (PET) fusion studies are also of value in the diagnosis and staging of neoplastic disease of reproductive system, as well as the assessment of disease progression.
CONGENITAL ANOMALIES
Congenital anomalies of the female reproductive system occur in approximately 1% to 2% of women. The most common anomaly is the bicornuate uterus,paired uterine horns that extend to the fallopian tubes (Figs. 10-9 and 10-10). A unicornuate uterusoccurs when the uterine cavity is elongated and has a single fallopian tube emerging from it. Often the kidney on the side of the missing fallopian tube is also absent. Uterus didelphysis a rare congenital anomaly with complete duplication of the uterus, cervix, and vagina. The most serious complication of these anomalies is problems with reproduction, although various surgical corrections can be performed.

In a normal woman the fundus of the uterus lies anterior to the cervix and away from the rectum and is said to be anteverted.Occasionally the normal uterus may lie in an abnormal position. If the uterus is more vertical than normal, it is said to be retrovertedand points backward toward the bowel. If the uterus is completely bent back and lies against the rectosigmoid region of the bowel, it is said to be retroflexed.A uterus that is tilted vertically forward is anteflexed,and it lies on top of the urinary bladder. Although neither position is normal, they are generally of little clinical significance.
INFLAMMATORY DISEASES
Pelvic inflammatory disease(PID) is a bacterial infection of the female genital system, specifically the fallopian tubes. One third of cases are caused by gonococcus, one third are caused by a mixture of infections, and the last third of cases are caused by Staphylococcusor Streptococcusbacteria. The disease may result from an unsterile abortion or introduction of a pathogen from other sources. This inflammation is generally bilateral, and without treatment the infection spreads to the peritoneum, resulting in bacteremia. Tuboovarian abscess formation may also occur with PID, often resulting in sterility. The clinical presentation of this entity involves pelvic pain and tenderness, guarding, and/or rebound tenderness. Patients often have fever and chills, elevated white count, nausea and vomiting, and purulent cervical discharge.
The most common treatment of PID is aggressive antibiotic therapy, but healing often results in scarring and obstruction of the fallopian tubes, which predisposes the individual to ectopic pregnancy because of the tubal narrowing. Rupture of the fallopian tubes because of infection can result in septic shock and can be a life-threatening situation. Sonography is commonly indicated as an imaging method for determining the presence of infection and the extent of the disease (Fig. 10-11). Severe cases with abscess formation may also require surgical intervention.
Mastitis
Inflammation of the breast, or mastitis, is most often caused by Staphylococcus aureus.Acute mastitis begins when bacteria gain access to the breast tissue via the ducts. This bacterial route of infection occurs because of cracks or fissures in the nipple that may develop during the first weeks of lactation and the subsequent nursing of an infant. Common signs and symptoms of mastitis include pain, redness, and swelling of the affected breast, elevated temperature, and, in severe cases, abscess formation. Mastitis is treated medically with antibiotic therapy and heat application to the affected breast. Risk factors for lactational mastitis are diabetes, steroid use, cigarette smoking, and inverted nipples. Mammography is difficult to perform on these patients because of the substantial engorgement of the breast tissue. Mammographic imaging to document mastitis can result in higher patient doses owing to the thickness of the tissue and is of little value in the diagnosis and treatment of mastitis.
NEOPLASTIC DISEASES
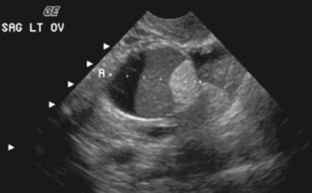
Simple ovarian cysts are fairly common in women within the reproductive age group. They are frequently asymptomatic but can cause abdominal aching and pressure. Acute, sharp abdominal pain may indicate rupture or hemorrhage of the cyst. They include follicular ovarian cysts and corpus luteum ovarian cysts. The formation of follicular and corpus luteum cysts occurs as a part of the normal menstrual cycle. Follicular ovarian cystsresult from faulty resorption of the fluid from incompletely developed follicles (Fig. 10-12). Corpus luteum ovarian cystsoccur when resorption of any blood leaked into the cavity after ovulation leaves behind a small cyst. Changes in the size of follicular and corpus luteum cysts occur quickly and vary with the menstrual cycle. These cysts may occasionally increase in size and cause pelvic discomfort or abnormal pressure on the urinary bladder. These cysts are readily visible with sonography, MRI (Fig. 10-13), and CT (Fig. 10-14) of the pelvis. Treatment is generally not necessary because they often disappear completely without medical intervention.
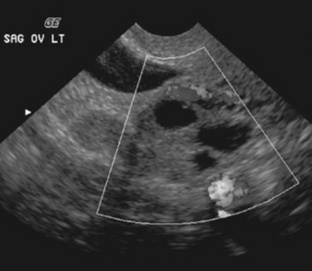
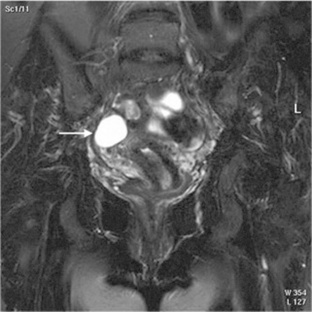
Fig. 10-13 A coronal T2-weighted fat-suppressed magnetic resonance image of the female pelvis demonstrating a cyst of the right ovary (arrow).

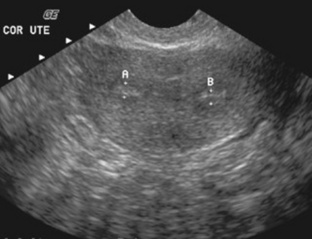
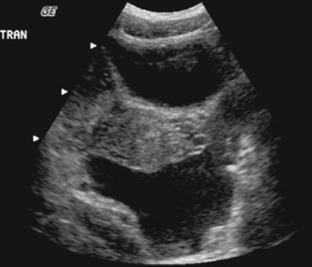
Fig. 10-14 A computed tomographic examination of a female pelvis demonstrating bilateral cysts. The patient is currently taking fertility drugs.
Multiple cystic masses may indicate endometriosis,a disease caused by the presence of endometrial tissue or glands outside the uterus in abnormal locations within the pelvis. External endometriosis commonly involves the ovaries, uterine ligaments, the rectovaginal septum, and the pelvic peritoneum; however, it may also attach to the rectal wall, the ureters, or the urinary bladder. Endometriosis is believed to arise from lymphatic spread, seeding from retrograde menstruation, or direct surgical spread. The endometrial implants appear to respond to normal hormonal stimuli and are clinically significant in women between the ages of 20 and 40. The external endometrial tissue implants contain normal functioning endometrium. Responsive to hormonal changes, it continues to bleed cyclically. These blood-filled cysts (also referred to as chocolate cysts)are often visible on ultrasonic examination. Longstanding endometriosis results in the development of fibrosis, adhesions, scarring, and eventually sterility. Common signs and symptoms include pelvic and low back pain, dysmenorrhea, intermittent constipation and diarrhea, and infertility. Although sonography is useful in the diagnosis of endometriosis, a positive diagnosis is generally made via laparoscopy. Mild cases of endometriosis may be treated with hormone therapy; severe cases generally require surgical therapy.
Polycystic ovariesconsist of enlarged ovaries containing multiple small cysts. The ovaries are bilaterally enlarged and have a smooth exterior surface, with the multiple cysts lying just below the outer surface. Polycystic ovaries are often associated with Stein-Leventhal syndrome, a fairly rare disease. Women with Stein-Leventhal syndrome rarely ovulate because of an endocrine abnormality that inhibits maturation and release of the ovarian follicle. In addition, these individuals may experience amenorrhea and sterility. The primary treatment is use of drugs to induce ovulation.
Benign cystic teratomasof the ovary, often called dermoid cysts, account for approximately 15% to 25% of ovarian tumors and are the most common type of germ cell tumor containing mature tissue. These masses arise from an unfertilized ovum that undergoes neoplastic change. Cystic teratomas are composed of tissue derived from the ectoderm, endoderm, and mesoderm, and they often contain hair, thyroid tissue, keratin, sebaceous secretions, and occasionally teeth (Fig. 10-15). Cystic teratomas have only a 1% to 2% chance of containing malignant cells. Some of the complications associated with a cystic teratoma are torsion of the mass and in some cases bleeding that can result in rupture and severe peritonitis. The treatment for cystic teratomas is surgical removal of the mass.
Cystadenocarcinoma
Cystadenocarcinomais a malignant tumor of the ovary, accounting for more than 60% of all ovarian cancers (Figs. 10-16 and 10-17). It primarily occurs in perimenopausal and postmenopausal women over age 40. Cystadenocarcinoma is the second most commonly diagnosed female genital carcinoma, occurring in 1 out of 70 women in the United States. It is the most lethal gynecologic malignancy, and the prognosis depends on the stage at which the tumor is discovered. Late stage tumors that have broken through the capsule of the ovary carry a very poor prognosis.
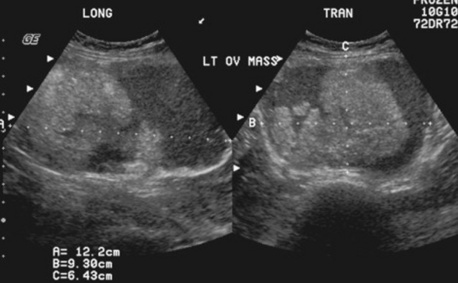

Fig. 10-17 Computed tomographic image of an ovarian mass in the female pelvis that confirms the mass seen on the sonogram.
The cause of this neoplasm is unknown. However, known risk factors include a diet high in fat, a history of late childbearing or nulliparity, delayed menopause, a family history of cancers of the endometrium, breast, or colon, and the presence of an inherited autosomal dominant gene known as the BRCA gene.Sonographic evaluation demonstrates a rough, irregular ovarian surface, with the tumor often containing both cystic and solid areas. Serous tumors are frequently bilateral; mucinous tumors are more likely to be unilateral.
The signs and symptoms of cystadenocarcinoma are very vague and include urinary bladder or rectal pressure, back pain, and bloating. In many cases the disease is completely asymptomatic and discovered only on routine pelvic examination. This tends to delay diagnosis and treatment, thus reducing the chance for cure. As a woman’s age increases, the probability of an enlarged ovary testing positive for ovarian cancer increases proportionately. These tumors often spread to other pelvic organs, the small intestines, the omentum, the stomach, and less frequently the liver and lungs, resulting in associated ascites and pleural effusions. Common treatment of cystadenocarcinoma includes surgery in combination with chemotherapy or radiation therapy.
Carcinoma of the Cervix
Cervical carcinomaor dysplasia is a common malignancy of the female genital system caused by an abnormal growth pattern of epithelial cells around the neck of the uterus. It is the third most common carcinoma of the female genital organs and the eighth most common malignancy in U.S. women. Cervical intraepithelial neoplasias (CINs) are classified or staged as mild (I), moderate (II), or severe (III) and are generally diagnosed by a Pap smear and confirmed by surgical biopsy. Cervical cancer is essentially a sexually transmitted disease, as a history of multiple sexual partners or prior sexually transmitted infections predisposes women to this disease. The development of cervical cancer is strongly associated with infection with human papillomavirus type 16, 18, 31, 33, 35, or 39. Associated risk factors include cigarette smoking and immunodeficiency. Multiple clinical trials are ongoing to investigate vaccines against the different strains of the virus. To date, Gardasil (Quadrivalent Human Papillomavirus Recombinant Vaccine) is the only FDA-approved vaccine and it is effective in preventing HPV types 6, 11, 16 and 18. This is a major breakthrough as HPV 16 accounts for almost half of all cervical cancers. Gardasil is currently available for young females aged 9 to 26 years to vaccinate against HPV and cervical cancer.The National Cancer Institute is also supportive of programs developing a therapeutic vaccine for those already infected with HPV.
Symptoms commonly associated with cervical dysplasiainclude abnormal bleeding, especially postcoitally. In addition, impaired renal function resulting from ureteral obstruction is often seen. If the cancer is invasive, radiography of the chest, urinary system, and skeletal system, in combination with CT or MRI of the abdomen and pelvis, is performed to assist in staging the disease. The treatment of cervical dysplasia varies according to the classification. Pap smears allow early detection of this disease, thus improving the chance of cure and survival. The 5-year survival rate ranges from 90% for stage I dysplasia to less than 15% for advanced disease. The primary treatments are radiation therapy and surgical intervention. Chemotherapy may also be administered in combination with radiation therapy to act as a radiosensitizer.
UTERINE MASSES
Leiomyomasare benign, solid masses of the uterus that develop from an overgrowth of the uterine smooth muscle tissue. They are present in approximately 30% of all women and in 40% to 50% of women over the age of 50 years. Uterine fibroids are the most common benign tumors of the female genital system. Symptoms include uterine enlargement and distortion, low back pain, pressure on the bowel and bladder, intermenstrual bleeding, and acute pain. The cause of this neoplasm is unknown; however, leiomyomas tend to grow under the influence of estrogen, may enlarge during pregnancy, and stop growing at menopause. After menopause, leiomyomas are replaced largely by fibrous scar tissue, leading to the misnomer uterine fibroids.In addition, they often contain radiographically visible calcifications (Fig. 10-18). The tumors vary in size and number (usually occurring in multiples). Seventy percent to 80% of uterine fibroids are located in the wall of the uterus. They can be asymptomatic until they grow large enough to place pressure on surrounding structures, and they are usually detected on pelvic examination. Sonography, CT, and MRI are all useful in confirming the presence of leiomyomas. Sonographically they appear as sharply circumscribed, encapsulated lesions and may contain cystic areas. Malignant transformation is rare, and treatment depends on patient symptoms, ranging from no treatment to surgical removal of the uterus.

Adenocarcinoma of the Endometrium
Adenocarcinoma of the endometrium is by far the most common malignancy of the uterus, accounting for more than 80% of all endometrial cancers. It is often termed endometrial carcinomaof the uterus, and it is histopathologically different from cervical carcinoma. Endometrial cancer is one of the most common cancers of the female reproductive system, second only to breast cancer. The incidence of adenocarcinoma of the endometrium has remained fairly static; the disease ranks as the fourth most common malignancy in women, occurring mainly in postmenopausal women and increasing in incidence with age. The development of this neoplasm has strong ties to hormonal changes within the woman and is more common in nulliparous women. Obesity is a major risk factor, as are tamoxifen use, late menopause, and a family history of breast or ovarian cancer or a history of previous pelvic radiation therapy.
Adenocarcinoma of the endometrium is usually preceded by endometrial hyperplasia. It then passes through an in situ stage before reaching its final invasive stage, often completely filling the uterine cavity. The cancer is graded according to cellular differentiation and staged according to the extent of the disease. The most frequent symptom is irregular or postmenopausal bleeding. Treatment varies with the stage of the disease. Stage 0 is curable via hysterectomy, and stages I and II are usually treated with a combination of surgery and radiation therapy, with a 5-year survival rate ranging from 70% to 95%. Stage III and IV endometrial adenocarcinomas are best treated with chemotherapy, but they have a lower 5-year survival rate of 10% to 60%.
BREAST MASSES
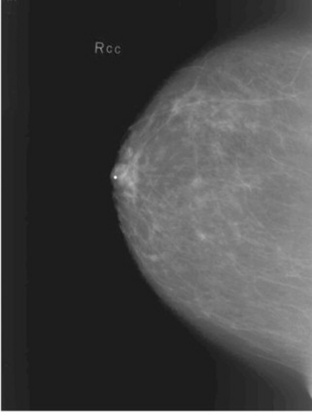
A fibroadenomais a common benign breast tumor. It is usually unilateral and consists of a solid, well-defined mass that does not invade surrounding tissue. The neoplasm is formed by an overgrowth of fibrous and glandular tissue and is commonly located in the upper, outer quadrant of the breast. Fibroadenomas almost always occur in women under the age of 30 years and most frequently in those aged 21 to 25 years. Fibroadenomas appear to be estrogen dependent and may grow rapidly during pregnancy. These lesions are often painless and can usually be moved about within the breast. Mammography, in conjunction with physical breast examination and sonography, plays a vital role in the detection of fibroadenomas (Figs. 10-19 and 10-20) and is useful in distinguishing them from mammary dysplasia (fibrocystic breast disease) and breast carcinoma. Surgical removal of the lesion is curative.

Fibrocystic Breasts
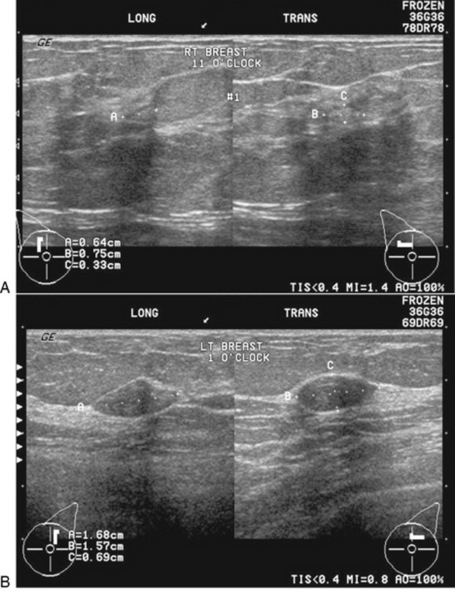
An overgrowth of fibrous tissue or cystic hyperplasia results in fibrocystic breasts.This is the most common disorder of the female breast and occurs to some degree in 60% to 75% of all women. This condition may be unilateral; however, it is most frequently bilateral, with variably sized cysts located throughout the breasts (Figs. 10-21 and 10-22). The severity of this disorder varies greatly, and it is believed to result from fluctuations in the hormone levels during the menstrual cycle. The most common sign or symptom associated with fibrocystic breasts is a mass or masses that increase in size and tenderness immediately before the onset of the menstrual period. The texture of the breast tissue is ropy and thick, especially in the upper outer quadrant of the breast. Sonography is extremely useful as a follow-up to mammography in differentiating solid masses from cystic masses in women with fibrocystic breasts (Fig. 10-23). Large cysts are commonly aspirated for cytologic evaluation of the fluid. If the aspiration is unsuccessful, surgical biopsy is often performed. Although controversy exists about the correlation between fibrocystic breasts and an increased incidence of breast cancer, it is well known that a fibrocystic condition may mask a coexistent cancer. Treatment of the condition is largely symptomatic, including a monthly breast self-examination and proper support.

Carcinoma of the Breast
Breast carcinomais a very common malignancy among women in the United States and the second leading cause of cancer deaths in women, behind only lung cancer. Current literature suggests that one of every eight women in the United States will develop breast cancer during her lifetime, with an increased incidence between the ages of 30 and 50. The incidence continues to rise throughout the postmenopausal years because of changes in estrogen levels, with the mean age for breast cancer being age 60. Approximately 60% of all palpable lesions occur in the upper, outer quadrant of the breast.
Although the exact cause of breast cancer is unknown, it is believed to be a multifactorial disorder. Heredity, endocrine influence, oncogenic factors (such as viruses), and environmental factors (such as chemical carcinogens) appear to play a role in the development of this disease. The amount of biologically available estrogen and progesterone is a key endocrine factor in the development of breast cancer. Those individuals with an early onset of menstruation (menarche) or late menopause and women with a first pregnancy after the age of 30 are at a higher risk for developing breast cancer. Women using oral contraceptives or estrogen replacement therapy over a 10-year period also have a very small increase in the risk of developing breast cancer. In terms of heredity, a family history including a parent, sibling, or child with breast cancer increases a woman’s risk to two to three times that of the normal population. In addition, women who carry BRCA1or BRCA2, two known breast cancer genes, and men who carry BRCA2are also at an increased risk for developing breast cancer.
Breast cancers may be classified as in situ carcinoma, ductal carcinoma in situ, lobular carcinoma in situ, invasive ductal or lobular carcinoma, or inflammatory carcinoma. Breast cancers generally are discovered as a lump in the breast by the patient. With the exception of inflammatory breast cancer, which is very virulent and associated with diffuse inflammation and breast enlargement, most begin as slow-growing, relatively painless masses, but as they grow, they may infiltrate the suspensory ligaments, causing them to shorten and retract the overlying skin. Physical signs of advanced breast cancer include nipple retraction and distorted breast contour. The neoplasm may infiltrate and block lymphatic vessels, the major route of metastases, especially to the axilla. This infiltration causes edema in the overlying skin and enlargement of the axillary or supraclavicular lymph nodes. As the infiltrating breast carcinoma blocks the lymphatic exchange, the skin’s pores open to allow the fluid to escape, therefore causing a rough skin texture from chafing and pore enlargement. The skin edema is known as a peau d’orangeappearance. As the tumor progresses, it may attach to surrounding fascia and ulcerate the surrounding skin.
Mammography plays a very important role in the diagnosis and management of breast cancer. In asymptomatic women, a routine screening mammogram can reduce breast cancer mortality by up to 30%. It has also been reported that breast cancer mortality could be reduced by as much as half if all women older than 40 years of age received annual screening mammograms. However, annual screening of women between the ages of 40 and 50 years remains controversial. Many breast tumors commonly appear radiographically as dense, irregular, stellate masses that infiltrate surrounding tissue (Fig. 10-24). Many of these neoplasms contain numerous microcalcifications that are radiographically visible (Fig. 10-25). In some instances, fine-needle aspiration with a cytologic evaluation may be sufficient to make a definitive diagnosis. Core needle biopsy or incisional biopsy is often performed to obtain a specimen of suspect tissue for further evaluation. For patients requiring an incisional biopsy, needle localization of mammographically detected, nonpalpable cancerous breast lesions is reliable in directing the surgeon to the lesion in question and allows excision of the suspect tissue. The tissue specimen is radiographed and forwarded to a pathologist for histologic evaluation. Statistics demonstrate that this method of localization causes minimal morbidity, and the development and refinement of mammographic localization has greatly increased the percentage of positive findings on surgical biopsy. This invasive technique allows more accurate diagnosis and treatment of early-stage carcinoma of the breast. If the tumor can be removed before the lesion is palpable, the survival rate is greatly increased. Specimens are routinely analyzed for estrogen and progesterone receptors because receptor status information is useful in determining a course of therapy. Patients with estrogen-receptor positive (ER+) tumors have a better prognosis and tend to benefit from endocrine therapy.
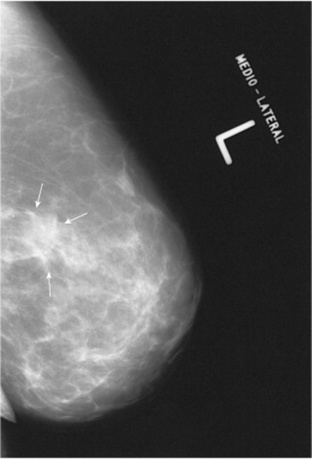
Fig. 10-24 Mammogram of the left breast of a 63-year-old woman demonstrating a stellate mass commonly associated with carcinoma of the breast. Notice the irregular borders of the mass.
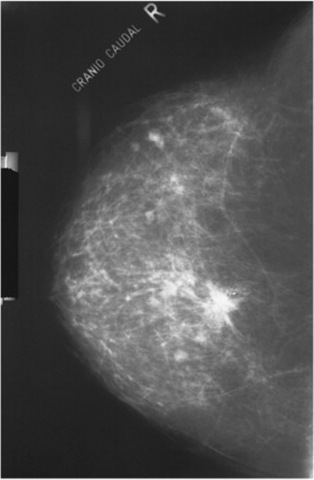
Fig. 10-25 Mammogram of the right breast in an elderly woman demonstrating a stellate mass containing microcalcifications commonly associated with carcinoma of the breast.
As discussed earlier in this chapter, MRI may be used to detect breast cancer. PET is often used as a valuable adjunct imaging method for predicting the clinical outcome in patients who have been previously treated for breast cancer. Use of 18-fluorodeoxyglucose (FDG) PET can provide both qualitative and quantitative information to help detect the primary tumor and in the identification of tumor spread via the lymphatic system, with a potential to actually reduce the need for lymph node dissection. It is useful in assessing breast tumor metabolism and biologic behavior.
Treatment of breast carcinoma depends on the extent of the disease. Once the carcinoma is confirmed by biopsy, an axillary lymph node resection is performed to assist in management of the disease. The 10-year survival rate for patients without node involvement is over 80% but drops to about 40% in patients with one to three positive nodes and to about 25% in patients with four or more positive nodes. Much controversy exists in terms of determining the best approach to management and treatment of breast cancers. In the past 40 years the 5-year survival rate for breast cancer has remained virtually unchanged. Currently two surgical options are recommended for invasive breast cancers: (1) modified radical mastectomy and (2) breast-conserving surgery followed by radiation therapy. Both methods require axillary lymph node resection, and there is not a significant difference in the survival rate between these two surgical options. Inflammatory cancers are usually treated with a combination of chemotherapy and radiation therapy.
Treatment with an established combination of chemotherapeutic drugs is considered standard care for premenopausal women with lymph node involvement. The chemotherapy may be continued for months or years after the primary therapy, but the adjuvant therapy may decrease the chance of death by 35% in this patient population. Breast carcinomas are also classified by a hormone receptor test. Many tumors require hormones for continued growth, and these carcinomas may undergo temporary regression if hormonal balances are altered.
DISORDERS DURING PREGNANCY
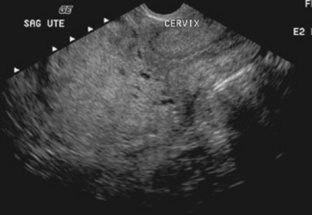
Diagnostic medical sonography is often used as positive proof of a pregnancy, in addition to aiding in the diagnosis of multiple and ectopic pregnancies. With the use of transvaginal sonography, the sac and early fetal pole can been seen, and a fetal heart detected, at as early as 3 weeks of gestation. Sonographic examination may be indicated if the pregnant uterus is too small or too large for the calculated delivery date. Depending on the obstetrician’s philosophy, many pregnant women may also receive a sonogram at 6 to 8 weeks of gestation to screen for fetal anomalies. Additional laboratory tests such as amniocentesis, chorionic villus sampling, and DNA analysis are performed in cases of suspected congenital anomalies of the fetus. Infant deaths are usually attributed to congenital anomalies or prematurity. Premature delivery may be associated with many anomalies of pregnancy. Examples include multiple pregnancies, placental anomalies, preeclampsia and eclampsia, and congenital anomalies of the uterus, such as bicornuate uterus or cervical incompetence. Preeclampsia is the development of hypertension in combination with proteinuria or edema and usually occurs after the twentieth week of gestation. The condition in which convulsions occur in a female patient with preeclampsia is termed eclampsia.Cervical incompetence can be demonstrated via sonography of the cervix during the first trimester of pregnancy.
Amniotic Fluid
Amniotic fluid is produced by various physiologic functions within the mother and the fetus. The amount of amniotic fluid present varies with the stage of pregnancy. Oligohydramniosoccurs when too little amniotic fluid is present, and polyhydramniosoccurs with an excess of amniotic fluid. The normal fetus swallows several hundred milliliters of fluid per day. This fluid is absorbed by the fetal intestines, with a portion excreted via the fetal urinary system and a portion transferred across the placenta into the mother’s circulatory system. The major source of amniotic fluid arises from the fetus urinating fluid once the kidneys are developed. Therefore, oligohydramnios often results from poor fetal kidney function or blockage of the ureters associated with congenital anomalies of the fetal urinary system. If a fetus is unable to swallow because of anencephaly or a high gastrointestinal obstruction, polyhydramnios may occur. It is also an indication of severe growth retardation and fetal death.
Ectopic Pregnancy
Ectopic pregnancyrefers to the development of an embryo outside the uterine cavity. It occurs in approximately 10% to 15% of 1000 pregnancies. The most common site for an ectopic pregnancy is the fallopian tube (Fig. 10-26), but it may also occur in the ovary, cervix, or abdominal cavity. In the case of a tubal pregnancy, the fallopian tube distends to accommodate the growing embryo, causing blood vessels to rupture. This may produce serious internal hemorrhage and can be life-threatening. If a tubal pregnancy goes untreated, the embryo will develop and survive for only 2 to 6 weeks.
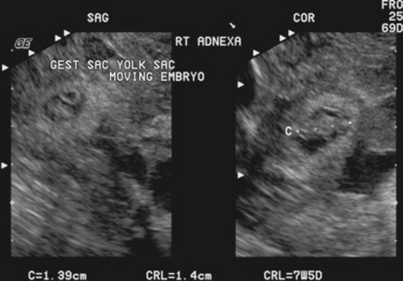
Common signs and symptoms associated with ectopic pregnancy are the same as those of early pregnancy, but distension of the tube causes acute abdominal pain and tenderness. If internal hemorrhage occurs, loss of blood can cause fainting and shock. Ectopic pregnancies are more common in women who have had PID or have a partial obstruction of the uterine tube. The cause of tubal pregnancies is obstruction of the normal passageway for the ovum. Although sonography is useful in assessing ectopic pregnancies, diagnosis is confirmed via laparoscopy. The treatment is surgical removal of the embryo and the affected uterine tube.
Disorders of the Placenta
The placenta is a temporary organ associated with pregnancy. Its purpose is to exchange nutrients and oxygen from mother to fetus and waste products from fetus to mother for excretion. If a woman begins to bleed during the third trimester of pregnancy, ultrasonography should be performed to evaluate the placenta, because this places both the mother and fetus at high risk. The most common causes of third-trimester bleeding are placenta previa and abruption of the placenta. Placenta previais a condition in which the implantation of the placenta leaves part or all of the cervical os covered. Several degrees are recognized: total, partial, marginal, and low-lying. These degrees of previa are related to the position of the placenta in relation to the internal cervical os. In cases of placenta previa (Fig. 10-27), the mother experiences painless vaginal bleeding during the later stages of pregnancy because of the partial separation of the placenta from the uterine wall. Hemorrhage can occur, and this condition can be life-threatening to both the mother and fetus. Sonography is a good method of determining placenta location in cases of suspected previa and is useful in the management of the pregnancy. Normal delivery cannot occur in patients with placenta previa, so a cesarean section is normally performed.
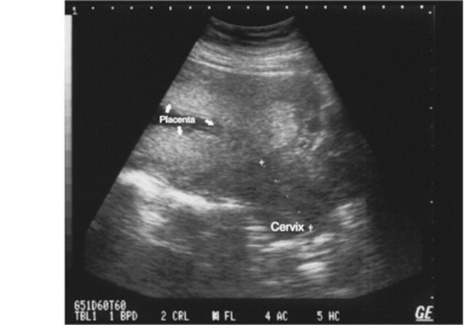
Fig. 10-27 Placenta previa seen on this sagittal sonogram view reveals the placenta covering the internal os of the cervix.
Occasionally a normally implanted placenta may prematurely separate from the uterus. This condition is termed placental abruptionand may be life-threatening to the fetus. Predisposing factors for abruption include history of a prior abruption, pregnancy-induced hypertension, smoking, alcohol abuse, cocaine abuse, external abuse, and multiple gestation. Placental percretais a condition in which the placenta extends into the myometrium, causing an unduly firm attachment that bleeds at delivery because it will not separate normally. In rare cases, failure of the placenta to separate after birth results in a need for an immediate hysterectomy.
Hydatidiform Mole
Hydatidiform molerepresents an abnormal conception in which there is usually no fetus. It occurs in about one in 2000 pregnancies in North America, although the incidence is much greater in certain other parts of the world for unknown reasons. Often the patient’s presenting sign is a uterine size that is inappropriate for dates. With this condition the uterus is filled with cystically dilated chorionic villi that resemble a bunch of grapes (Fig. 10-28). These villi absorb fluid and become swollen, demonstrating a characteristic pattern on a sonogram as well as absence of heart sounds. Usually these conceptions abort spontaneously in the second trimester. If they do not, suction curettage is done, and most patients require no further treatment. Approximately 80% of molar pregnancies follow a benign course, but 15% to 25% can develop invasive disease.
MALE REPRODUCTIVE SYSTEM
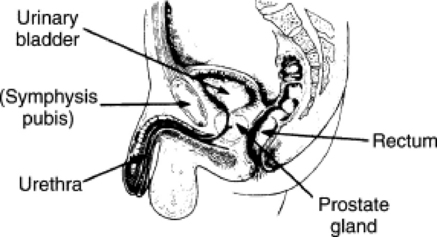
The male reproductive system is composed of glands, ducts, and supporting structures. The glands of the male reproductive system include a pair of testes, a pair of seminal vesicles, a pair of bulbourethral glands, and one prostate gland. The testes are enclosed by a white, fibrous covering within the scrotum. They are responsible for the production of sperm and the secretion of hormones, mainly testosterone. The prostate gland lies just inferior to the bladder, and the urethra actually passes through this gland (Figs. 10-29 and 10-30). The prostate gland is responsible for secreting the majority of the seminal fluid and is normally about the size of a walnut.

The ducts that connect the glands include a pair of epididymides, a pair of vasa deferentia, a pair of ejaculatory ducts, and one urethra. The testes are divided into lobules that contain seminiferous tubules, which converge into larger ducts and emerge at the head of the epididymis. The epididymides lie superior and lateral to the testes and serve as a passageway for sperm. They are also responsible for secreting a portion of the seminal fluid. The vasa deferentia extend from the epididymides and pass through the inguinal canal into the pelvic cavity. They pass superior to the bladder and continue down the posterior surface of the bladder to join the ducts emerging from the seminal vesicles. This junction forms the ejaculatory ducts. These ducts eventually empty into the urethra, which is responsible for delivering the seminal fluid to the exterior of the body.
IMAGING CONSIDERATIONS
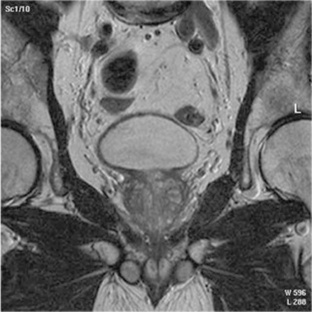
Radiographic investigation of the male reproductive system is limited mainly to urethrograms and intravenous urography. However, sonography is commonly used to evaluate testicular masses or an enlarged scrotum and to help differentiate between, on one hand, epididymitis and orchiditis and, on the other, testicular torsion. Nuclear medicine is also useful in distinguishing between epididymitis and testicular torsion. Prostatic sonography via a rectal probe is used to evaluate nodules and guide the physician during biopsies of the prostate. MRI of the male pelvis is performed to evaluate the seminal vesicles, the prostate gland, and the scrotum (Fig. 10-31). MRI is useful in detecting and staging prostate cancer in men having a positive (+4) prostate-specific antigen (PSA) laboratory test. A specialized rectal coil is used in examining the prostate gland; however, high-field MRI units may be able to detect pathology without the use of the rectal coil. MRI is also useful in evaluating testicular cancer and can determine if the cancer is present in one or both testicles. This differentiation is especially important for young men who still plan to have children.
CONGENITAL ANOMALIES
As the end of gestation occurs, the male testes normally descend through the inguinal canal into the scrotum. Cryptorchidismis a condition of undescended testes. The rate of malignancy is much greater in men with this condition, so the treatment involves either bringing the testicle down and fixing it surgically or removing it. Sonography is often used to locate the testicle. Although MRI is more expensive than sonography, it may also be of value in the diagnosis of this anomaly because of its superior ability to differentiate tissue.
NEOPLASTIC DISEASES
Prostatic hyperplasiais a common benign enlargement, palpable through the rectum, of the prostate gland caused by the development of discrete nodules within the organ. Although enlargement may be determined by a digital rectal examination, the results may be misleading, so a laboratory blood test to assess serum PSA should be performed. Results may demonstrate a moderate elevation in PSA, depending on the degree of enlargement and urinary obstruction. The cause of prostatic hyperplasia is unknown, but the condition is thought to be caused by hormonal changes associated with aging in that it generally affects men after age 50. The benign nodules most frequently occur in the median lobe and central portions of the lateral lobes of the prostate gland. Because of this location, the nodules often compress the portion of the urethra passing through the prostate gland, thus interfering with urination.
Symptoms associated with this disorder include difficulty in starting, stopping, and maintaining a flow of urine and inability to completely empty the bladder. Residual urine retained in the bladder tends to become infected, threatening the kidneys with infection. In some cases, urinary tract obstructions may result from an overgrowth of the prostate gland. The most common treatment of prostatic hyperplasia is partial excision of the prostate gland, although nonsurgical treatment is available for some cases. A transurethral resection of the prostate (TURP)is performed by passing an endoscope through the urethra to core out the gland. Prostatic enlargement may be demonstrated on an intravenous urographic examination as a filling defect at the base of the bladder. Hyperplastic changes are also readily visible on MRI and CT examinations of the pelvic area (Fig. 10-32). There is no conclusive evidence to suggest that development of prostatic hyperplasia increases an individual’s chance of developing prostatic carcinoma.
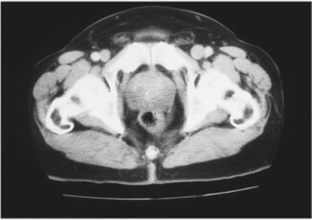
Fig. 10-32 Pelvic computed tomography of a 68-year-old man demonstrating prostatic hyperplasia. Notice the indentation into the urinary bladder.
Many men over the age of 50 develop small, multiple calcifications within the prostate. These are termed prostatic calculiand may be radiographically visible on plain abdominal or pelvic images. The development of these calculi is of no clinical significance.
Carcinoma of the Prostate
Adenocarcinoma of the prostateis a common cancer in men. It most frequently affects elderly men, with the incidence increasing with age. The cause of prostate cancer is unknown, but it generally affects the outer group of prostate glands and occurs more frequently in the posterior lobe of the prostate. This disease is most often diagnosed by physical examination and an elevation of acid phosphatase levels in the blood. In cases of suspected prostatic disease, MRI or sonographic imaging may be used to determine the location and extent of the disease (Fig. 10-33). Common signs and symptoms associated with prostate cancer include urinary tract obstructions, a hard, enlarged prostate on rectal palpation, and low back pain, often caused by metastatic spread to the pelvis and lumbar spine.

Fig. 10-33 An axial T2-weighted magnetic resonance image demonstrating enlargement of the posterior left portion of the prostate by prostate carcinoma.
Some types of prostate cancer are fairly dormant, but others are very aggressive and yield a higher mortality rate. If it is diagnosed at an early stage, the initial treatment is surgical removal of the tumor. In addition, this neoplasm is highly testosterone dependent, so the testes are often removed along with the prostate. In some instances, female hormones may be administered to control the growth of the tumor by interfering with testosterone. A new treatment modality involves planting radioactive seeds in the prostate, guided by ultrasound, to destroy the tumor.
Prostate cancer is staged A to D and graded I to III, depending on the extent of the disease. It tends to infiltrate surrounding structures early and extensively, particularly the skeletal system. Skeletal metastases occur in approximately 75% of all cases and manifest on plain radiographs as sclerotic lesions within the bone (Fig. 10-34). Bone pain in an elderly man should particularly raise suspicion about prostate cancer. As the third leading cause of cancer deaths in men, it has a 5-year survival rate of approximately 33%.

Testicular Masses
Testicular torsion occurs if a testicle twists on itself, inducing severe pain and swelling. Failure to correct this surgically in an immediate fashion can result in severe compromise of testicular vascularity. The condition is often evaluated with a nuclear medicine scan, which shows decreased uptake on the affected side (Fig. 10-35). Inflammation of the epididymis, or epididymitis, can similarly lead to scrotal swelling. This inflammation of the epididymis and testis (epididymo-orchitis)may result from a bacterial infection such as a urinary tract infection or gonorrhea or may be secondary to the placement of an indwelling urinary catheter. In addition to scrotal edema, signs and symptoms include scrotal pain and erythema. The resulting increased blood flow can be detected with sonography or a nuclear medicine scan, which demonstrates increased uptake (Fig. 10-36).
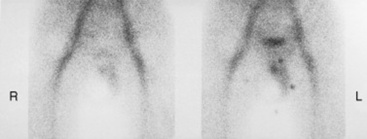
Fig. 10-35 Torsion as seen on a nuclear medicine testicular scan, which reveals a relative absence of blood flow to the right testicle.
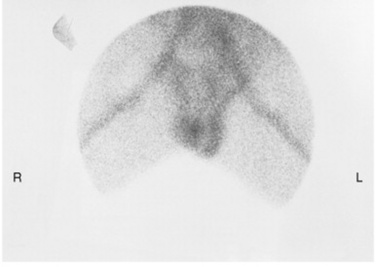
Fig. 10-36 Epididymitis as revealed on a testicular scan, which shows increased uptake in the left testicle.
Benign masses of the testes may be associated with epididymo-orchitis. Other common benign masses include hydroceles and spermatoceles. Hydrocelesare common intrinsic scrotal masses, sometimes congenital in nature, caused by a collection of fluid in the testis or along the spermatic cord (Fig. 10-37). They may appear as a painless scrotal swelling, or they may demonstrate inflammation in combination with epididymitis and be quite painful. Spermatoceles,or spermatic cysts, are fluid-filled, painless scrotal masses within the testis adjacent to the epididymis (Fig. 10-38). Sonography may be used to differentiate between benign hydroceles or spermatoceles and solid, malignant neoplasms.
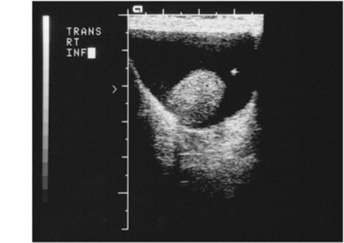
Fig. 10-37 A hydrocele is visualized as the dark collection of fluid surrounding the testicle, as seen on a sonogram of this 52-year-old man.
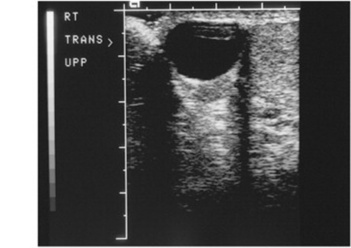
Fig. 10-38 A spermatocele, evidenced by a large fluid collection on the epididymis, as seen on a testicular sonographic scan of this 33-year-old man.
Malignant testicular tumors constitute ap- proximately 1% of all male cancers. Such tumors represent the most common malignancy among 15- to 34-year-olds, and the condition has a peak incidence around age 30 and a second smaller peak around age 75. The cause of malignant tumors of the testes is unknown, but research has shown a strong hereditary association. The most common signs include enlargement or palpable hardness of the testis. As with other cancers, testicular tumors are staged I to III, depending on the size and extent of the disease. All types of malignant testicular neoplasms are treated with surgical resection. Chemotherapy, radiation therapy, or both may be used in conjunction with surgery, depending on the type and staging of the disease. There are four types of malignant germ cell tumors; seminomas, embryonal carcinomas, teratomas, and choriocarcinomas.
Testicular seminomasarise from the seminiferous tubules and account for approximately 40% of malignant testicular tumors (Fig. 10-39). Seminomas grow rapidly but tend to remain localized for a fairly long time before metastasizing. These neoplasms have an excellent prognosis because of their extreme radiosensitivity. If treated with radiation therapy, seminomas carry a 10-year survival rate of approximately 90%.
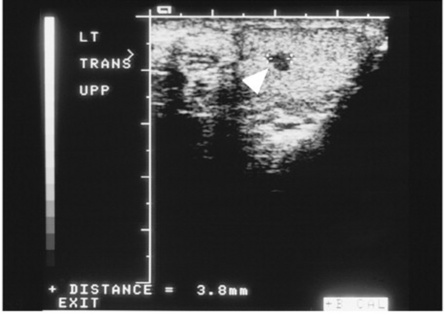
Fig. 10-39 The hypoechoic mass seen in the superior aspect of the testicle on this testicular sonogram of a 31-year-old man is strongly suggestive of a seminoma.
Testicular teratomasarise from primitive germ cells and account for approximately 25% of the malignant testicular masses (Fig. 10-40). These neoplasms are composed of various cell types such as connective tissue, muscle, and thyroid glandular tissue. Teratomas are associated with a poorer prognosis than seminomas and carry a 10-year survival rate of approximately 50% to 75%. Like seminomas, teratomas are highly malignant, spreading to the renal hilum via lymphatics and hematogenous spread.
Fig. 10-40 A large, echogenic heterogeneous mass in the right testicle is highly suspicious for a teratoma in the testicular sonogram of this 27-year-old man.
Approximately 20% of malignant testicular tumors are testicular embryonal carcinomas.They are smaller than seminomas; however, they are very invasive and metastasize fairly quickly. Embryonal carcinomas carry a 10-year survival rate of approximately 35%.
Testicular choriocarcinomasmake up the smallest portion of malignant testicular tumors, accounting for only 1% of malignant neoplasms of the testes. However, choriocarcinomas are very small and aggressive neoplasms. They are often nonpalpable and metastasize very early. Choriocarcinomas carry the worst prognosis, with a 10-year survival rate of approximately 10%.
REVIEW QUESTIONS
4 The formation of which of the following cystic ovarian masses may occur as a part of the normal menstrual cycle?
6 Diagnosis of which type of neoplastic disease is often made via a Pap smear and confirmed by surgical biopsy?
11 Describe how breast parenchyma changes with age and parity and the effect these changes have on radiographic visibility of potential masses.
12 Identify two purposes for requiring a patient to have a full bladder for female transabdominal sonographic examination.
13: Describe the benefit versus the risk of radiation exposure from routine mammography.
14: What would be the danger of leaving cryptorchidism untreated? 15. A 60-year-old man presents to his physician with complaints of frequent urination, particularly at night. An intravenous pyelogram (IVP) is ordered. The only visible abnormality is a filling defect at the base of his bladder. What is the likely cause?