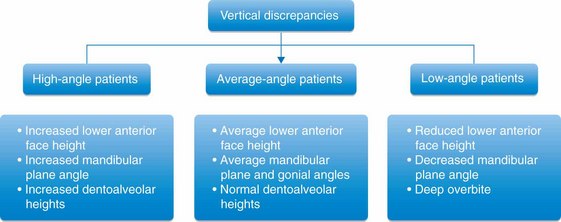
Vertical discrepancies
The vertical dimension of face is often altered, either intentionally or nonintentionally, during orthodontic treatment of various dentofacial problems by the extrusion or intrusion of teeth and by growth modification and orthognathic surgery. These changes have a great impact on the way the mandible rotates, either open or closed, with corresponding alterations in maxillomandibular dental relationships, lip and tongue function and, importantly, the facial aesthetics. Therefore, before the initiation of orthodontic therapy, it is vital for the clinician to clearly define the treatment goals related to the vertical dimension of face and design a detailed individualized treatment strategy and mechanics plan based on sound biomechanical principles.
The orthodontic literature related to the management of sagittal discrepancies and to certain extent transverse discrepancies is replete with research, case studies and publications. However, for the most part in the past and still to a large extent in the present, there has been much less research and discussion on the treatment of vertical problems. A large variation in craniofacial growth in the vertical dimension should play a prominent role in orthodontist's approach to the diagnosis and treatment of malocclusion. The relevance of assessing the vertical dimension to clinical practise is to determine if there is a vertical component contributing to the development of a problem. In a clinical practise, vertical discrepancies are often considered to be the most difficult dentofacial problems to treat. To successfully treat vertical discrepancies, it is important for the clinician to have good understanding of the factors having the greatest influence on the vertical dimension problem. The author believes that in dealing with malocclusions with abnormal vertical component, the simplicity or complexity of the force system is not the deciding factor in producing the best treatment results. Rather, clinicians should have sound knowledge of facial growth and development, interplay between the horizontal and vertical growth, function of the lips and tongue etc.
Development of a vertical problem
Facial growth in relation to the cranial base proceeds along a vector with variable amounts of horizontal and vertical growth. It is important to consider, understand and appreciate the value of vertical growth, as it relates to anteroposterior growth. Vertical growth carries the chin downward, while anteroposterior growth carries it forward (Fig 4.1). The major sites of bony additions contributing to the facial growth include the facial sutures, maxillary alveolar processes, mandibular condyle and mandibular alveolar processes.1 If vertical growth increments at the facial sutures and the maxillary and mandibular alveolar processes exceed the condylar growth, the mandible would rotate backward. However, if growth at the condyle exceeds the total vertical growth at the facial sutures and alveolar processes, the mandible would rotate forward.2 These growth changes significantly alter the lower facial height and the position of chin horizontally and vertically.
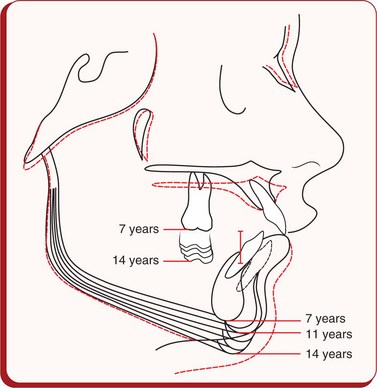
Figure 4.1 Cephalometric superimpositions showing the chin position as a result of growth changes in a patient between 7 and 14 years of age. It was observed that the chin moved downward and forward till the age of 11 years; thereafter, it was displaced downward and backward as a result of less condylar growth and more vertical growth in the molar area.
Growth
For the facial proportions and the occlusal relationships to be normal, the components of the craniofacial complex consisting essentially of the cranial base, nasomaxillary complex and the mandible should exhibit harmonious growth and should maintain a reasonable proportion in size and form. It is well recognized that the spatial position of the maxillary dentition is influenced by the eruption pattern of the teeth and the growth of the maxilla and its contiguous bones. It is also affected by the growth of the anterior cranial base, the area between the pituitary fossa and the internal plate of the frontal bone, to which the maxillary complex is attached. The growth at the sphenoethmoidal suture significantly contributes to the increase in depth of the anterior cranial base and upper face until the suture closes by the age of 7 years.3 After the age of 7 years, further growth in this area until adulthood takes place by surface remodelling of bone on the frontonasal surface, with the sella to the internal plate of the frontal bone dimension unchanged.4
After the cessation of anterior cranial base growth at an early age, the anterior half of the craniomaxillary complex is displaced in an anterosuperior direction by the growth at the spheno-occipital suture until the suture closes after puberty.5 This expression of growth shows a great degree of variation in the direction and rate among individuals. The spatial position of the mandibular dentition is determined by the growth of the mandible and its relationship to the temporal bone. It has been shown that the relationship of the mandible to the anterior border of the foramen magnum (Ba-Ar) does not vary.6 Condylar head, being the primary growth centre of the mandible, grows in upward and backward directions with the resultant downward and forward displacements of the mandible and carries the mandibular dentition away from the vertebral column and cranial base. Therefore, the growth at the spheno-occipital synchondrosis displaces the maxillary complex anterosuperiorly, while the growth at the mandibular condyle displaces the mandible downward and forward (Fig 4.2). These two diverging growth vectors create a space for vertical facial growth, alveolar growth and tooth eruption. Annual incremental growth of various craniofacial components is shown in Figure 4.3.
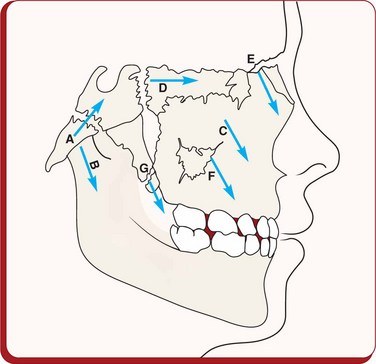
Figure 4.2 Growth at the spheno-occipital synchondrosis during the first decade displaces the maxillary complex anterosuperiorly, while the mandibular condylar growth displaces the mandible anteroinferiorly producing diverging growth vectors to create a space for vertical facial growth, alveolar growth and tooth eruption. Cartilaginous growth: A, spheno-occipital synchondrosis; B, reflection of mandibular condylar growth; C, nasal septum; D, sphenoethmoidal; E, frontomaxillary; F, zygomaticomaxillary; G, pterygopalatine. Image courtesy: Coben SE. Am J Orthod 1966; 52(1):5–26.
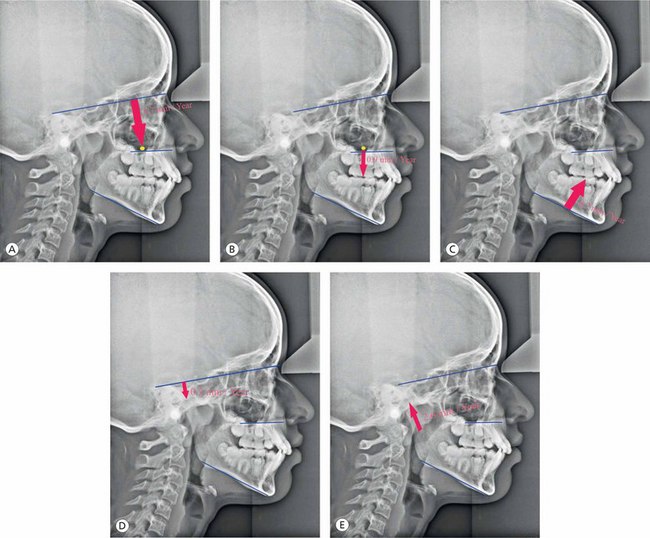
Figure 4.3 Annual incremental growth of various craniofacial components. (A) Average basal maxillary vertical displacement. (B) Vertical maxillary dentoalveolar growth. (C) Mandibular vertical dentoalveolar growth. (D) Vertical displacement of the articular fossa. (E) Condylar growth.
The mandible demonstrates a great degree of variation in the direction of its growth in the normal population as shown in studies on facial growth by Björk and Skieller using metallic implants.7–13 The most common direction of condylar growth is vertical with some anterior component; however, the posterior growth is less frequently observed. Patients with upward and forward growth of the condyle are usually characterized by reduced anterior face height and deep overbite, as seen in Class II division 1 malocclusion. Patients with extreme cases of upward and forward growth of the condyle exhibit a skeletal deep bite, as observed in Class II division 2 malocclusion. Typically, the maxillary and mandibular dentitions are characterized by considerable degree of mesial migration of teeth with some amount of mandibular incisor proclination. Patients with a more posteriorly directed mandibular condylar growth demonstrate a pronounced increase in lower face height and an anterior open bite. The erupting posterior dentition is generally vertical, and quite often, the anterior teeth may even become more proclined with time.
It is important for the clinician to consider, understand and recognize the importance of mandibular growth rotation, as it relates to anterior facial height (AFH) and overbite relationship. Björk11 suggested that under normal situations, the fulcruming point for anterior mandibular growth rotation is located at the incisors (Fig 4.4). In the absence of proper incisal contact due to lip dysfunction, finger sucking habit or severe sagittal jaw discrepancy, the fulcruming point moves posteriorly along the occlusal plane leading to the development of skeletal deep bite. In patients with posterior condylar growth rotation, the fulcruming point is located near the mandibular condyles, with the development of anterior open bite and increased anterior face height.
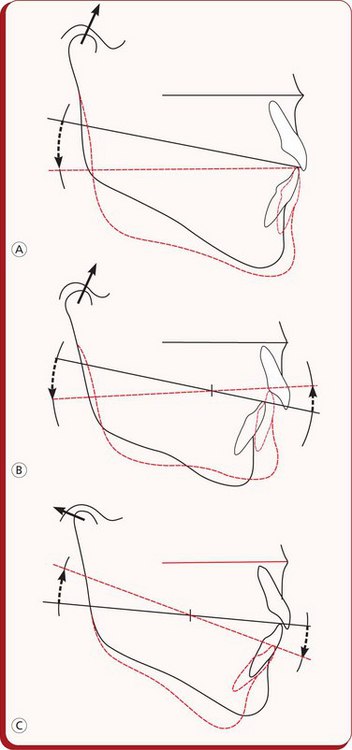
Figure 4.4 Diagrammatic illustration of mandibular growth rotations.
(A) Patients with a stable occlusion demonstrate anterior rotation of the mandible with the fulcrum point located at the incisors.
(B) Patients with lack of anterior occlusion tend to have the fulcruming point located posteriorly along the occlusal plane. (C) In patients with posterior mandibular rotation, the fulcruming point is located near the mandibular condyles. Image courtesy: Björk A. Am J Orthod 1969; 55:585–599.
In addition to the condylar growth direction, differences in AFH and posterior facial height (PFH) development do play an important role in the development of vertical skeletal discrepancies (Figs 4.5 and 4.6). These differences significantly contribute to rotational growth or to changes in mandibular position, influencing the position of the chin.14 The research findings show that the dentoalveolar heights are significantly greater in long AFH patients and smaller in short lower AFH group.15,16 The excessive maxillary posterior dentoalveolar development may be associated with weaker masticatory musculature in high-angle patients compared with stronger musculature associated with low-angle patients.
Environmental factors
The role of certain environmental factors like swallowing, breathing and tongue posture in altered vertical dimension still continues to be the subject of debate. However, breathing problems due to large adenoids, tonsils, deviated nasal septums etc are frequently associated with high-angle patients, which alter mandibular posture, creating more room for posterior teeth eruption. It has been shown that the removal of adenoids and tonsillectomy have resulted in closing of the mandibular plane (MP) angle and reduction in the anterior face height.17,18 The significance of tongue posture and tongue thrust has been evaluated by many with regard to its role as a causative factor in the development of malocclusion.
Diagnosis of vertical discrepancies
Vertical discrepancies consist of various components of the craniofacial complex and are often associated with abnormalities in other planes of space. Their accurate diagnosis is a key element in the design of any successful treatment plan. In order to plan an appropriate treatment strategy, the clinician should localize and quantify any skeletal and dental contributions, vertical and sagittal variations and the role of abnormal function to the development of vertical problems.
Facial evaluation
Facial evaluation should begin with a systematic, three-dimensional assessment of the frontal and profile views in the vertical, sagittal and transverse planes. The goal of this assessment is to establish an accurate description of the aesthetic, skeletal and occlusal abnormalities, as well as functional disorders. Based on the extraoral features, patients with vertical discrepancies may be broadly classified as long-face and short-face patients.
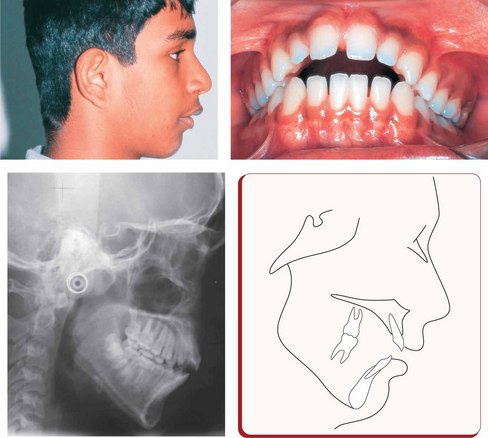
Long-face patients are usually characterized by leptoprosopic facial form and dolichocephalic head form, increased lower facial height, narrow alar bases, prominent nasal dorsum, retrognathic mandible, orthognathic or prognathic maxilla, incompetent lips with mentalis strain, shallow mentolabial sulcus and flattened or recessive chin. Such patients usually exhibit Class II malocclusion with the appearance of mandibular deficiency and are often associated with excessive gingival display upon smile.
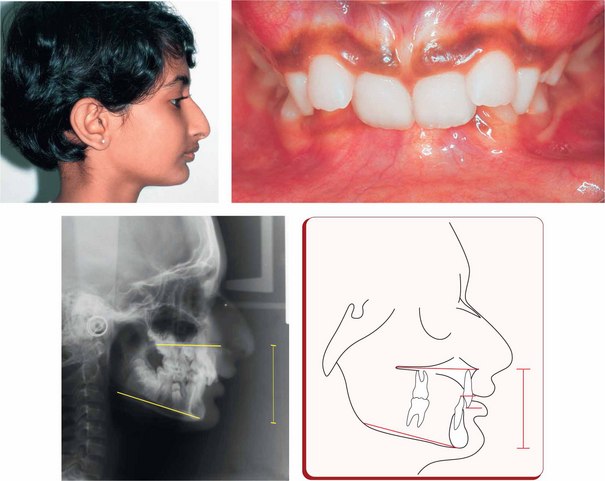
Short-face patients can be found in Angle's Class II and Class III malocclusions. Short-face patients with the most common Class II malocclusion present with decreased lower anterior face height, normal upper lip length, obtuse nasolabial angle, acute mentolabial sulcus, retruded mandible and adequate or excessive soft tissue chin. Short-face patients having Class III malocclusion exhibit many opposite facial characteristics with decreased lower anterior face height, short upper lip, acute nasolabial angle, prognathic appearing mandible and obtuse mentolabial sulcus.
Intraoral examination of the long-face patients reveals maxillary – mandibular dentoalveolar protrusion, upright and supraerupted maxillary and mandibular incisors, excessive eruption of posterior teeth, anterior open bite, high and narrow palate with posterior crossbite etc. Intraoral features common to short-face patients of both Angle's Class II and Class III groups include excessive deep overbite and deep curve of Spee. The maxillary and mandibular incisors are often upright exhibiting a bidentoalveolar retrusion.19 A short face in these patients is often caused by overclosure of the mandible either due to vertical maxillary deficiency or due to deficient teeth eruption in either the maxilla or the mandible.
Functional assessment
An assessment of function is a very important part of the clinical examination for planning treatment of vertical discrepancies. Associated disorders involving airway, speech and tongue function should be carefully evaluated. It has been generally recognized that environmental factors that are responsible for keeping the maxillary and mandibular teeth apart promote elongation of the posterior teeth, leading to an increase in lower face height. Excessive posterior dentoalveolar development in the maxilla is considered to be associated with weaker musculature in high-angle patients compared with stronger musculature in low-angle patients.20
Morphologic characteristics
Classifying patients into high-angle or long-face patients and low-angle or short-face patients is just a broad understanding of vertical discrepancies. Patients with vertical problems should be further analyzed cephalometrically to identify and locate the structures at fault, which mainly contribute to the development of a problem (Fig 4.7). Their understanding is essential to define the treatment goals and plan a treatment strategy to resolve them. Vertical discrepancies can be divided into those that are dentoalveolar in nature and into those that are predominantly skeletal as a result of the growth patterns of the jaws.
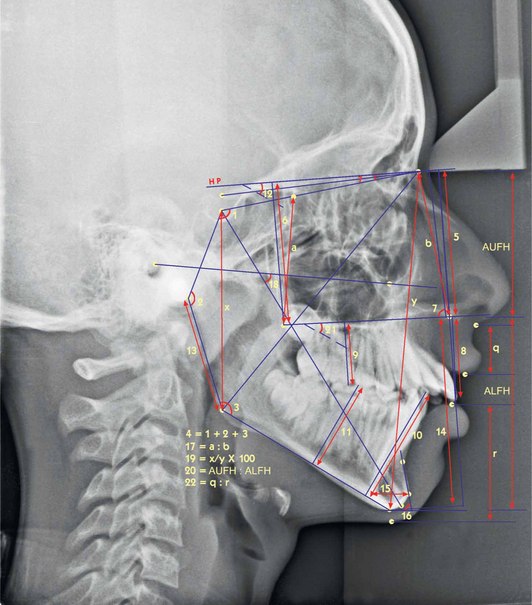
Figure 4.7 Cephalometric assessment of vertical discrepancies. 1. Saddle angle (N-S-Ar); 2. Articular angle (S-Ar-Go); 3. Gonial angle (Ar-Go-Me), upper gonial angle (Ar-Go-N) and lower gonial angle (N-Go-Me); 4. Björk's sum = saddle angle (N-S-Ar) + articular angle (S-Ar-Go) + gonial angle (Ar-Go-N); 5. Distance between N and ANS (perpendicular to HP); 6. Distance between N and PNS (perpendicular to HP); 7. J angle-angle between palatal plane and perpendicular to N-Se passing through N'; 8. Upper incisor edge to nasal floor (NF) (perpendicular distance to NF); 9. Upper first molar mesiobuccal cusp tip to NF (perpendicular distance to NF); 10. Lower incisor edge to mandibular plane (MP) (perpendicular distance to MP); 11. Lower first molar mesiobuccal cusp tip to MP (perpendicular distance to MP); 12. MP-HP (angle); 13. Length of mandibular ramus (Ar-Go); 14. Distance between ANS and Gn (perpendicular to HP); 15. Width of symphysis measured at Pg, parallel to true horizontal; 16. Symphysis angle-angle between line passing through point B and Pog and true horizontal; 17. Ratio of posterior maxillary height (E-PNS) to anterior maxillary heights (N-ANS); 18. Angle between FH plane and y-axis (S-Gn); 19. Jarabak's ratio posterior facial height (S-Go)/anterior facial height (N-Me) × 100; 20. Anterior upper facial height (vertical distance from N to ANS): anterior lower facial height (vertical distance from ANS to Me); 21. Angle between palatal plane (ANS-PNS) and mandibular plane; 22. Upper lip length (subnasale to stomion superior): lower lip length (stomion inferior to soft tissue menton).
Cephalometric assessment
• The cranial flexure angle (N-S-Ar), articular angle (S-Ar-Go) and gonial angle (Ar-Go-Me) are often used to determine the growth pattern of an individual. The mean value of sum of these angles is 396° ± 4°; high values are suggestive of a vertical growth pattern, whereas low values indicate horizontal growth pattern.21,22
• The gonial angle, having a mean value of 130° ± 7°, is a good indicator of vertical or horizontal growth pattern. An increased value shows that the individual is backward growth rotator, while a decreased value indicates a forward rotator.21,23 To be more precise, if the ratio of the upper gonial angle (Ar-Go-Na) to the lower gonial angle (Na-Go-Me) is more than 75%, it is considered a horizontal growth rotation; however, higher lower gonial angle indicates a vertical growth pattern.21
• The MP angle (Go-Me – true horizontal) having a mean value of 27° ± 5° is one of the most commonly used parameters. It is increased in patients with a vertical growth pattern, while horizontally growing patients exhibit low angle.
• An assessment of symphysis morphology is useful in determining the growth pattern of an individual. The width of symphysis, measured at pogonion (Pg) parallel to the true horizontal, has a mean value of 16.5 ± 3 mm, with greater values in horizontally growing patients and smaller values in vertically growing patients.23 The symphysis angle, formed by the line passing through point B, Pg and the true horizontal, having a mean value of 75° ± 5°, is acute in a forward growth rotational pattern and obtuse in a backward rotation.23,24
• In an individual with average facial growth, the ratio of posterior face height (S-Go) to anterior face height (Na-Me) is 65%, with higher values in a forward growth pattern and smaller values in a backward growth pattern.
• The vertically growing patients tend to have a ratio of posterior to anterior maxillary height higher than 90%, while in horizontally growing patients, this ratio is lower than 90%.
High-angle patients are usually characterized by the following:
• Rotation of palatal plane down posteriorly
• Short ramus height or decreased posterior face height
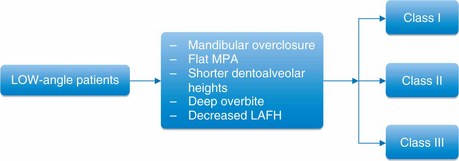
Low-angle patients are usually characterized by the following:
Vertical Class II types
While assessing various problems in vertical dimension, it is essential for the clinician to understand their impact on the sagittal dimension. Björk11 described morphologic method of predicting growth rotation from a single cephalogram and found seven structural signs for predicting forward or backward growth rotation.
1. Inclination of the condylar head: the condylar head curves forward in forward rotator, while it is straight or slopes up and back in backward rotator.
2. Curvature of the mandibular canal: the mandibular canal is curved in forward rotator and straight in backward rotator.
3. Shape of the mandibular lower border: in forward rotator, it is curved downward, whereas in backward rotator, it is notched.
4. Inclination of the symphysis (anterior aspect just below point ‘B’): this slopes backward in forward rotator and forward in backward rotator.
5. Interincisal angle: this angle is vertical or obtuse in forward rotator and acute in backward rotator.
6. Interpremolar or intermolar angles: these angles are vertical or obtuse in forward rotator and acute in backward rotator.
7. Anterior lower face height: this height is short in forward rotator and long in backward rotator.
Of these seven original signs, four of the variables when combined give the best prognostic estimate of mandibular growth rotations.24
These parameters are as follows:
1. Mandibular inclination: this can be assessed by the gonial angle measurement, the inclination of the lower border or a proportion between posterior and AFH.
2. Shape of the lower border: the backward rotator has convex or notched lower border as against the concave lower border of the forward rotator.
3. Inclination of the symphysis: if the symphysis points behind nasion or posterior to nasion, a forward rotational pattern is likely present. If it points forward or anterior to nasion, it is an indication of backward rotation.
4. Intermolar angle: in backward growth rotation, the premolars and molars are more inclined, while in the forward growth rotation, these teeth are more upright to one another.
Class II malocclusions with vertical discrepancies have been identified as having five vertical types25 (Fig 4.8).
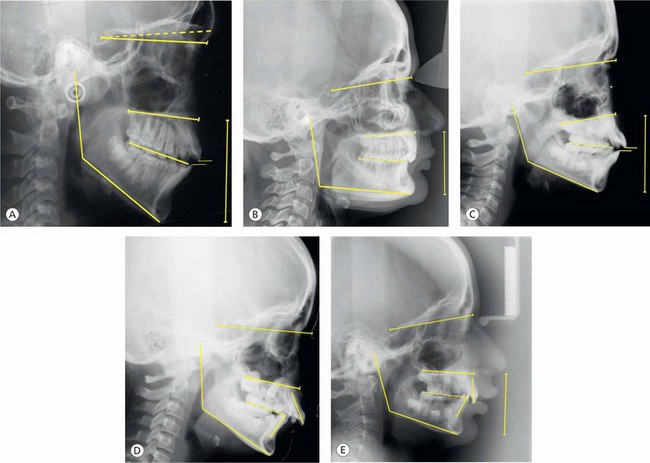
Figure 4.8 Differential diagnosis of vertical discrepancies. Class II malocclusions having five vertical types based on the research by Moyers et al25: (A) Type 1, (B) Type 2, (C) Type 3, (D) Type 4 and (E) Type 5.
Type 1: it is characterized by the disproportionately increased anterior face height than by the posterior face height. The palate may be tipped downward, and the anterior cranial base tends to be upward. The mandibular and functional occlusal lines are steeper than normal. This vertical type of Class II malocclusion is also called high-angle case or long-face syndrome.
Type 2: it displays more horizontal or nearly parallel mandibular, functional occlusal and palatal planes. The gonial angle is small, and the anterior cranial base is horizontal. The patient displays a ‘square face’ with more vertical incisor position and skeletal deep bite.
Type 3: patients having type 3 vertical pattern exhibit a palatal plane that is tipped upward anteriorly resulting in a decreased anterior upper face height and an open bite. When it is associated with steep MP angle, a severe skeletal open bite is developed.
Type 4: it is a rare type of Class II malocclusion having palatal and functional occlusal planes that are tipped downward, and the mandible plane is almost normal. The gonial angle is relatively obtuse. The maxillary incisors are tipped labially, and the mandibular incisors are lingually inclined. Patients usually exhibit high lip line on the maxillary alveolar process.
Type 5: the features of this type include the palatal plane that is tipped downward with normal mandibular and functional occlusal planes. The gonial angle is smaller than normal. This leads to skeletal deep bite. The maxillary incisors are almost vertical, and the mandibular incisors are severely labially placed.
Treatment planning
Establishing accurate diagnosis is an integral part of designing a successful treatment strategy. An ideal treatment plan maximizes treatment results and shortens the treatment duration. Defining treatment goals – facial, skeletal and dental – is the best way to approach treatment planning for the vertical discrepancies. At the treatment planning stage, as the clinician gets involved into an important process of reexploration of the available relevant diagnostic information, several critical factors must be considered.
• A careful evaluation of the vertical proportions of the face to determine long lower face height (high angle) or short lower face height (low angle) is the first step in the treatment planning process. Control of the vertical dimension is considered the most important factor in successfully treating high-angle patients. These patients usually have a tendency to further bite opening during treatment as a result of significantly less bite force than low-angle patients.26 The treatment of such patients should result in

Conversely, a vertical discrepancy patient involving a disproportionately short lower facial height would have different and opposite treatment goals and approach.
• Determine whether the malocclusion is dentoalveolar or skeletal. It is possible to have abnormalities of teeth in vertical dimension without affecting the lower anterior face height. It is also important to identify the dentoal-veolar compensation masking the underlying severe vertical skeletal discrepancy. In the maxilla, the angle between the palatal plane and the maxillary occlusal plane (mean 10° ± 3°) describes the extent of compensatory or dysplastic development, while in the mandible, it is described by the measurement between the MP and the mandibular occlusal plane (mean 20° ± 4°).27
• Vertical discrepancy is not a single entity and involves many components. Identification of their involvement is essential to formulate an effective treatment strategy.
• Age of the patient and the severity of malocclusion significantly influence the treatment planning process. It is recommended to ascertain the growth potential of the patient based on the useful diagnostic information. It is not only the differences in condylar growth direction but also the result of differences in AFH and PFH development that significantly contribute to two extreme growth patterns – long face and short face.
• Identification of aetiological factors responsible for the development of a vertical discrepancy and the role of neuromuscular dysfunctions are of great value in planning a treatment. Though the role of environmental factors like abnormal tongue posture, swallowing and mouth breathing is still a subject of debate, it needs serious consideration.
• The dentofacial aesthetics is considered one of the main reasons for patients to undergo orthodontic treatment. The vertical discrepancies, especially the skeletal involvement, expressed clinically either as a long-face problem or as a short-face problem, significantly contribute to the impairment of facial aesthetics. Therefore, aesthetic benefits of proposed treatment plan should be analyzed, and if required, necessary alterations should be incorporated to maximize facial aesthetics.
• Clinicians are quite often faced with the difficult task of treating patients with anterior open bite or deep bite with subsequent challenge to retention. Various treatment modalities have been used to address these problems; however, the success of any therapy is ultimately measured by long-term stability. The best way to approach any vertical discrepancy is to identify the areas of potential relapse and take appropriate measures to enhance stability.
Treatment of vertical discrepancies
While dealing with the patients with vertical problems, it must be recognized that all cases cannot be treated in a similar manner due to extreme variation in facial pattern and morphological characteristics. The facial pattern is not constant since it is changed by growth and by orthodontic treatment. Also, the effects of vertical growth increments on different facial types are different. Therefore, in patients with compromised AFHs, the relative methods of mandibular rotation (opening versus closure) as a part of orthodontic treatment should be recognized as either desirable or undesirable.
For the purpose of discussion, treatment of vertical discrepancies can be grouped and explained under following categories (Fig 4.9):
1. Vertical discrepancies with increased lower anterior face height or long-face patient
2. Vertical discrepancies with normal vertical dimension of face
3. Vertical problems with decreased lower AFH or low-angle patient
Management of long-face patients
Treatment of excessive lower facial height or long-face patients depends on an accurate diagnosis that requires precise identification of various components. As opposed to simple open bite malocclusions that do not include skeletal components, high-angle patients have underlying skeletal problems that have proven to be extremely challenging for orthodontists. The clinician should expect a great degree of variation of traits among individuals; some show severe anterior open bite, while others, despite the underlying severe skeletal discrepancy, exhibit less severe open bite due to dentoalveolar compensation (Fig 4.10). Dentoalveolar compensation that masks discrepancies in all three planes of space should be measured cephalometrically to design an appropriate treatment strategy.

The most consistent morphologic characteristics in the maxillary zone include excessive anterior and posterior dentoalveolar heights;28 the palatal plane angles tend to be flatter due to decreased upper AFHs;29 however, upper PFHs appear to be unchanged. The maxillary length is usually shorter,29 and the width is reduced with a tendency for posterior crossbites.14 The most constant morphologic features in the mandibular region include steeper MP angle, increased lower anterior heights and larger gonial angle.28,29 Most patients exhibit shorter ramus heights leading to decreased PFHs. Mandibular dentoalveolar heights generally tend to be excessive. The glenoid fossa is often positioned more superior relative to sella turcica. All these features combine to produce overall proportional increase in lower facial height to upper and total AFHs.
It is clear from these findings that the vertical discrepancies are often associated with problems in sagittal and transverse dimension. Therefore, a well-designed treatment strategy must address the three-dimensional problems pertaining to the dental, alveolar and skeletal structures of both the jaws. Hyperdivergent Class III open bite cases are less frequently observed and are more difficult to treat non-surgically than hyperdivergent Class II patients. Control of vertical dimension is considered to be the most important factor in successfully treating patients with hyperdivergency.
Treatment goals for hyperdivergent Class II patients are as follows:
1. Reductions in maxillary and mandibular dentoalveolar heights
3. Increase in palatal plane angulations
5. Mandibular autorotation to decrease lower facial height and reposition the chin forward
Orthopaedic and orthodontic treatment options to manage hyperdivergent patients include the use of high-pull headgear, posterior bite-blocks, vertical-pull chin cup, extractions etc.
Mixed dentition treatment
Overall growth potential of an individual and the ability of certain morphological features to change are greater during childhood than adolescence. This potential combined with psychosocial benefits best justifies early intervention of skeletal open bite problems. Early treatment holds the key to nonsurgical correction of these complex malocclusions. It is based on the premises that this condition can be diagnosed at an early stage of development; potential for mandibular autorotation is maximum during childhood, and certain components of these discrepancies require long periods of growth for maximum correction. These problems do not self-correct; psychosocial benefits of correction and various treatment options are available to address associated discrepancies in transverse and sagittal dimensions.
Therefore, early diagnosis and interceptive treatment are of utmost importance since the prognosis becomes progressively poor longer the open bite persists. Certain early signs of subtle structural changes in the craniofacial complex should be carefully observed by the clinician. Elimination of all possible aetiological factors as soon as the case is diagnosed is important. Since these patients are difficult to treat and often challenge the experience and skills of the best orthodontist, early mistakes in the treatment may compound the existing problem.
High-pull headgear has been the appliance of choice in the management of hyperdivergent open bite patients (Figs 4.11–4.14). This appliance system has good control over maxillary sutural growth and vertical dentoalveolar development.30,31 Author prefers high-pull or occipital-pull headgear attached to the maxillary acrylic splint to prevent unfavourable tipping of molars. This appliance has good vertical control over the maxillary molars and produces superior and distal displacement of the maxilla, clockwise rotation of the palatal plane, reductions in SNA angle and relative intrusion of the maxillary molars.32 As the maxillary molars are intruded, the mandible hinges upward, closes the open bite, displaces the chin forward and reduces the lower AFH (Figs 4.13 and 4.14). It is critical to be aware of the associated molar extrusion in this type of situation unless appropriate mechanics has been designed to control their eruption. The addition of a vertical-pull chin cup to this appliance system helps to prevent the eruption of mandibular molars.33
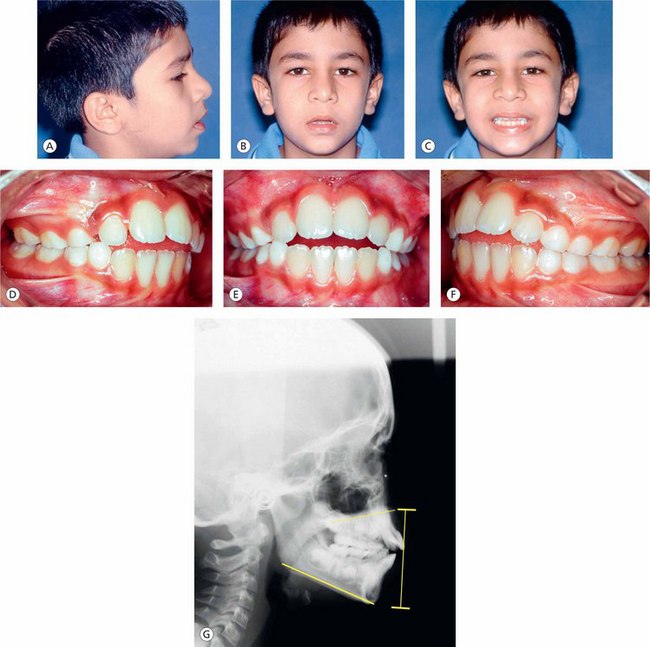
Figure 4.11 (A–C) Extraoral photographs of a growing male patient having increased lower facial height, convex profile and incompetent lips. (D–F) Intraoral photographs show mixed dentition stage, anterior open bite and tongue-thrust habit. (G) Pretreatment lateral cephalogram shows high mandibular plane angle, increased lower anterior facial height and superiorly tipped palatal plane in the anterior region.
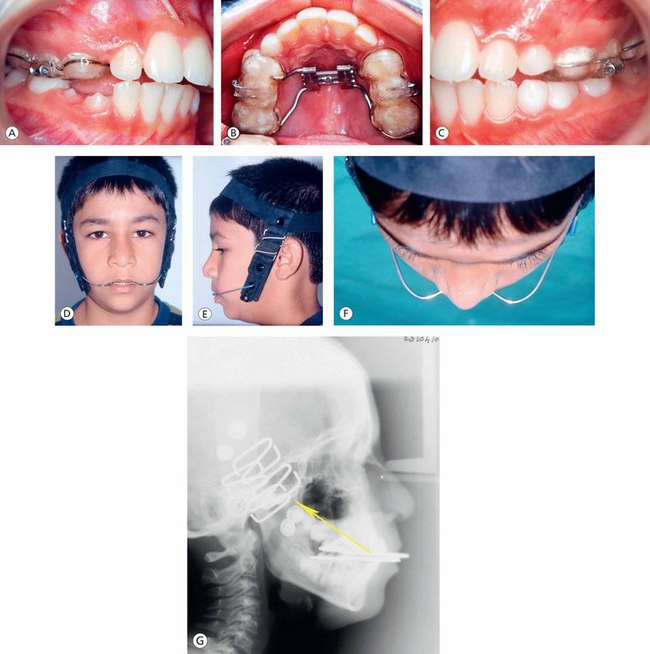
Figure 4.12 (A–C) Full occlusal coverage maxillary splint with rapid expansion device and headgear tubes. (D–F) Patient using high-pull headgear. (G) Extraoral orthopaedic force passing through the centre of resistance of the maxilla.
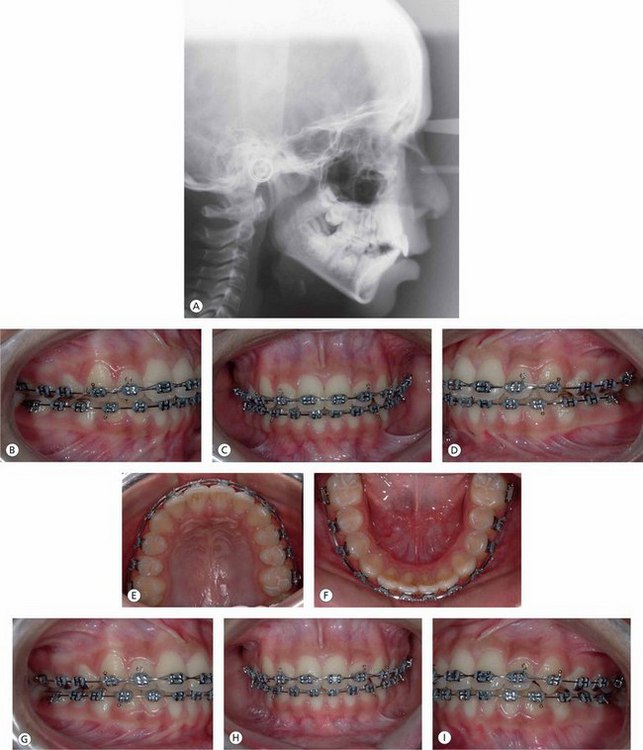
Figure 4.13 (A) Postorthopaedic treatment lateral cephalogram showing closure of the mandibular plane angle, positive incisor overlap and favourable orientation of the palatal plane. (B–I) Postorthopaedic treatment fixed appliance therapy to establish a well-coordinated maxillary and mandibular archforms, alignment, levelling and torque control of anterior and posterior teeth.
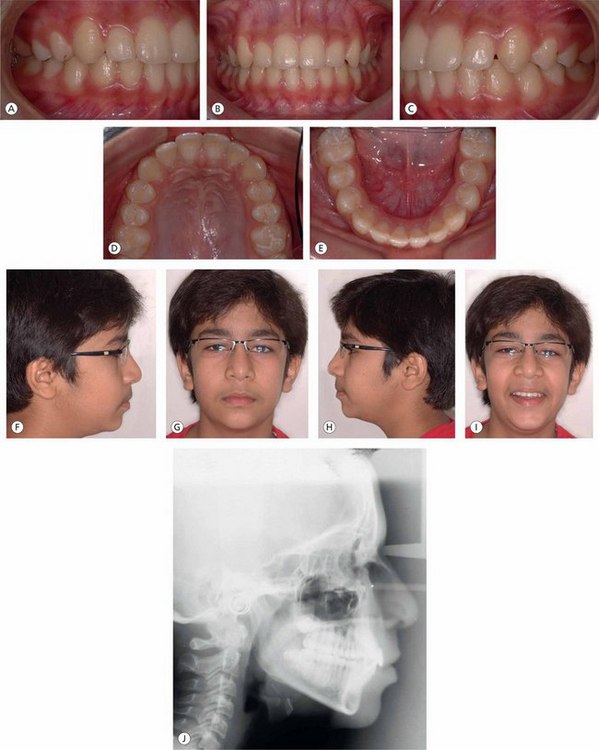
Figure 4.14 (A–E) Posttreatment intraoral photographs showing good occlusion and archforms. (F–I) Posttreatment extraoral photographs show normal facial features and a pleasing smile. (J) Posttreatment lateral cephalogram showing normal orientation of the palatal plane, good interincisal relationship and reduction in the lower anterior face height.
As stated earlier, vertical discrepancies are often associated with abnormalities in other two planes of space. Skeletal open bite malocclusions occasionally exhibit constricted maxillary arch leading to unilateral or bilateral posterior crossbites. The best way to approach maxillary transverse discrepancy is to use rapid palatal expansion device along with full posterior occlusal coverage appliance for better vertical molar control (Figs 4.15–4.18).
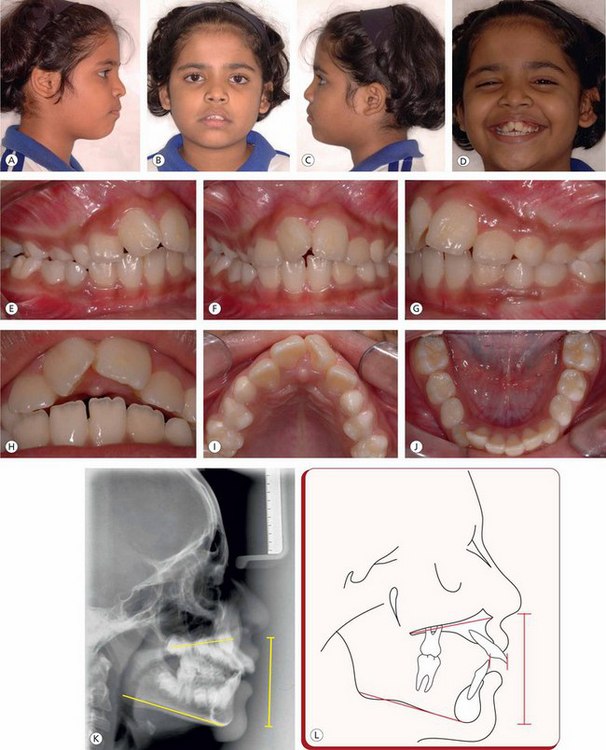
Figure 4.15 (A–D) Pretreatment extraoral photographs of a growing female patient showing convex profile and incompetent lips. (E–J) Intraoral photographs show mixed dentition stage with unilateral crossbite on the right side, anterior open bite, constricted maxillary arch and upper and lower arch anterior crowding. (K and L) Pretreatment lateral cephalogram shows tipped-up palatal plane in the anterior region, anterior open bite, increased lower anterior face height, incompetent lips and upper lip line high on the maxillary alveolar process.

Figure 4.16 (A–D) Bonded rapid palatal expansion device given to split the maxillary suture and achieve desired orthopaedic expansion. (E–H) Postorthopaedic expansion intraoral photographs show the correction of posterior crossbite and the closure of anterior open bite.
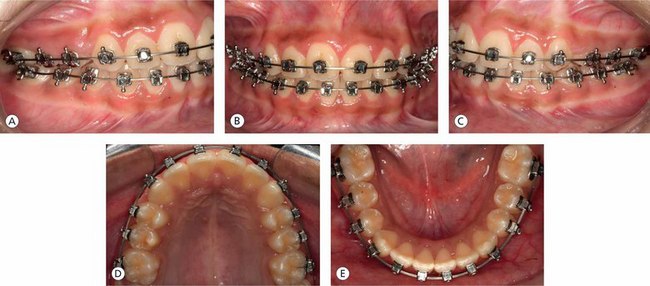
Figure 4.17 (A–E) Fixed appliance therapy to improve individual tooth positioning and achieve normal occlusal relationships.
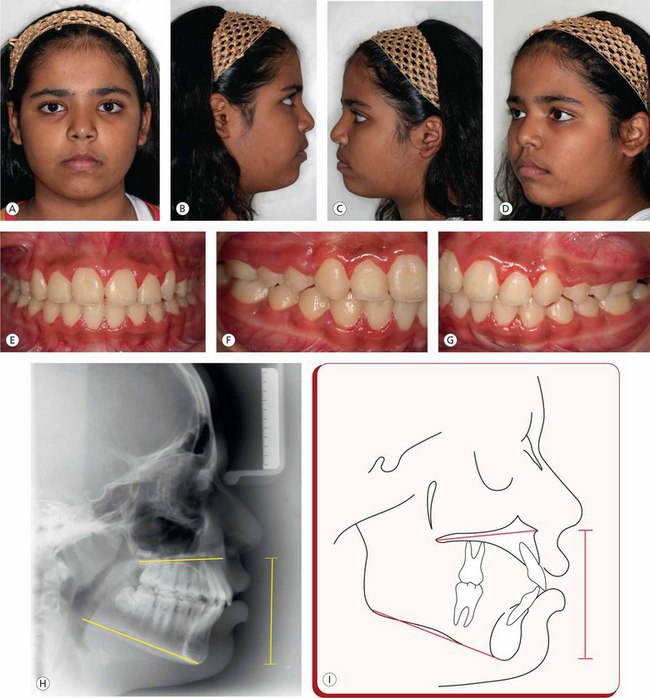
Figure 4.18 (A–D) Posttreatment extraoral photographs show improved facial aesthetics. (E–G) Posttreatment intraoral photographs show good individual teeth position and interarch relationship. (H and I) Posttreatment lateral cephalogram and tracing demonstrate normal orientation of palatal plane, reduction in lower anterior facial height, closure of mandibular plane angle and normal interincisal relationship.
This also prevents undesirable buccal tipping of the posterior teeth and concomitant overhanging of palatal cusps that further accentuates mandibular backward rotation. After the desired amount of maxillary orthopaedic expansion, the appliance is removed prior to fixed appliance therapy; however, continued vertical control of the posterior teeth is maintained by giving mandibular posterior bite blocks. This is frequently combined with vertical-pull chin cup to maximize the result, along with the prevention of mandibular molar eruption.
The significance of the role of certain environmental factors like tongue posture and tongue thrust has been evaluated by many with regard to their contribution as a causative factor in the development of a vertical problem. The management of patients with such problems is illustrated in Figures 4.19–4.22.
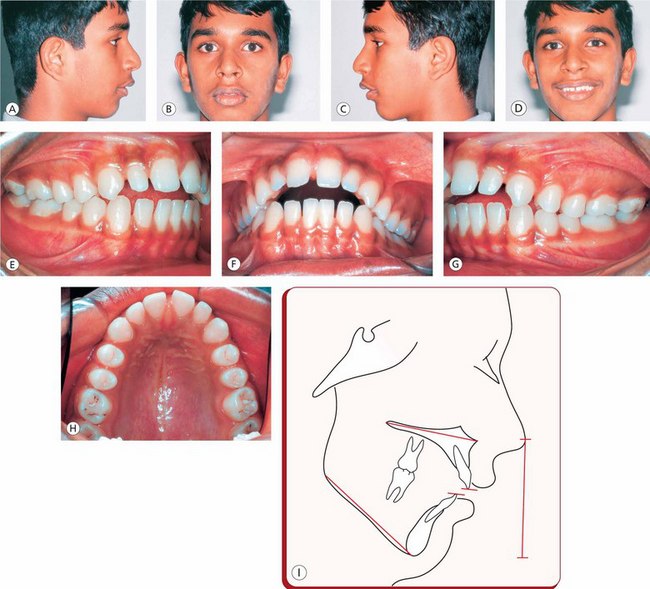
Figure 4.19 (A–D) Pretreatment extraoral photographs showing convex profile, posterior chin position and incompetent lips. (E–H) Intraoral photographs showing early permanent dentition with anterior open bite, interproximal spacing and Class I molar and Class II canine relationships. (I) Pretreatment lateral cephalometric tracing showing downward and backward rotation of the mandible, anterior open bite and increased lower anterior facial height.
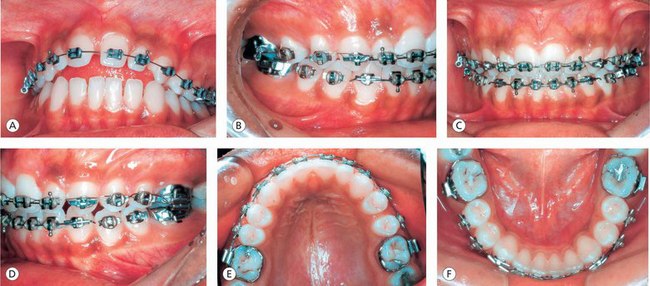
Figure 4.20 (A–F) Fixed appliance therapy was initiated along with the use of a molar-inserted high-pull headgear to intrude maxillary posterior teeth to achieve closure of interproximal spaces and open bite, normal interincisal relationship and well-coordinated and compatible maxillary and mandibular archforms.
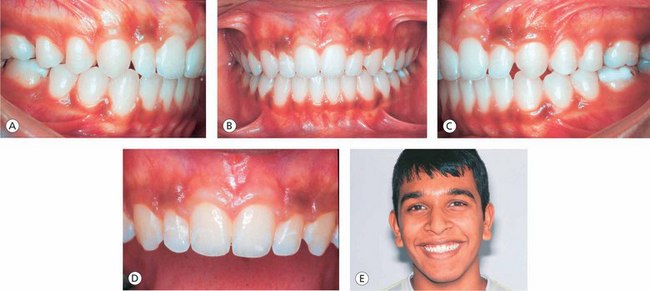
Figure 4.21 (A–D) Posttreatment intraoral photographs showing normal overjet and overbite and progressive buccal root torque of the posterior teeth. Note: the maxillary and mandibular midlines are not coinciding with each other due to disproportionate widths of maxillary lateral incisors. (E) Posttreatment pleasing smile.
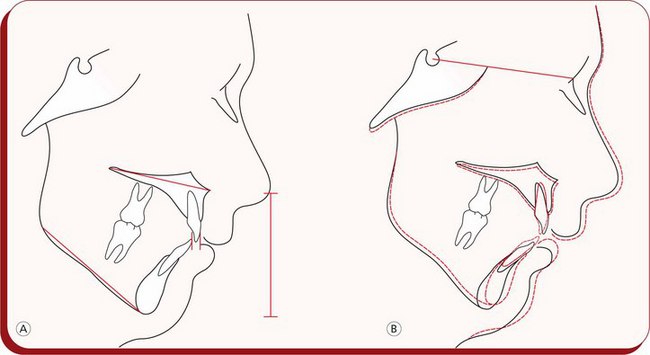
Figure 4.22 (A) Posttreatment lateral cephalometric tracing shows significant reduction in the lower anterior face height and improved vertical incisor and lip relationship. (B) Pretreatment and posttreatment cephalometric tracing superimpositions showing favourable dental, skeletal and soft tissue changes.
Extraction treatment approach
Extractions of teeth in the management of high-angle patients is considered to be useful; it is based on the belief that molars tend to move mesially out of the occlusal wedge promoting mandibular autorotation, decrease in lower anterior face height and closure of open bite relationship (Figs 4.23–4.26). Following extractions, Class II patients demonstrate decrease in ANB angle, supraeruption of the mandibular molars and increase in MP angle.44 Patients with steep MP angles and treated with extractions and occipital headgears have also demonstrated significant amount of vertical movement of mandibular molars.35 Following extractions in a patient with an increased vertical dimension, the treatment mechanics of extraction space closure must be carefully planned to prevent eruption of posterior teeth. A common mistake by most clinicians in dealing with the closure of extraction space is to use heavy forces with either horizontal chains or coil springs while the teeth are engaged on a relatively light archwire. This approach typically promotes tipping of both the anterior and posterior teeth into the extraction space. After the resolution of anterior discrepancy in a high-angle patient, the residual extraction space to a large extent is closed by controlled protraction of the posterior teeth into the extraction sites. Extraction treatment approach when compared with nonextraction treatment has shown no significant differences in changes of MP angle, AFH or vertical position of maxillary and mandibular molars.36 Vertical movement of upper molars is better controlled with a combination of high-pull headgear and extraction treatment; however, mandibular molars show even greater compensatory vertical movement34,35 It has been shown that the combined treatment of extractions and vertical-pull chin cup produces significant decrease in AFH and gonial angle.37
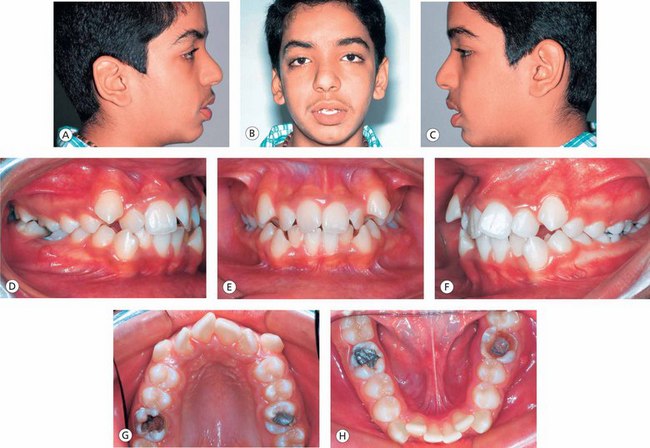
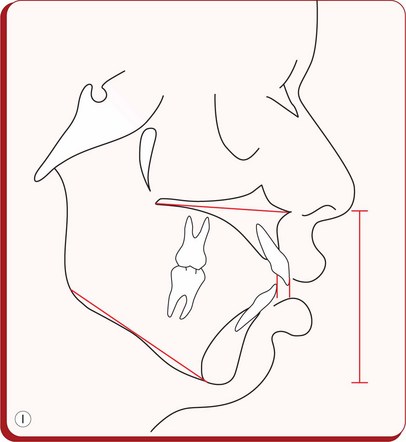
Figure 4.23 (A–C) Pretreatment extraoral photographs show acute nasiolabial angle and incompetent lips. (D–H) Pretreatment intraoral photographs show severe maxillary and mandibular crowding, labially placed maxillary and mandibular cuspids and badly decayed and filled maxillary and mandibular permanent first molars. (I) Pretreatment lateral cephalometric tracing shows increased mandibular plane angle, incompetent lips, acute nasiolabial angle and significantly increased lower anterior facial height.
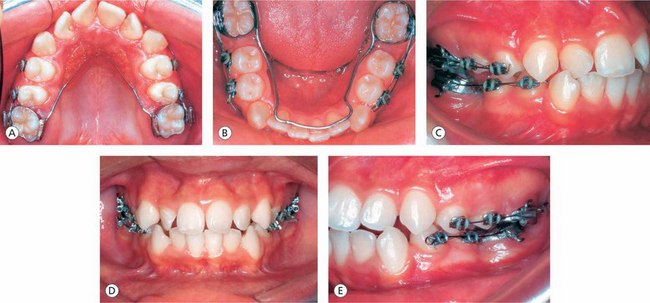
Figure 4.24 The treatment plan included the extraction of all permanent first molars to resolve the discrepancy. (A and B) Modified Nance palatal button cemented on the maxillary second molars, and the lingual arch cemented on the mandibular second molars. (C–E) Posterior segmental arch mechanics to retract the bicuspids to create space anteriorly to allow decrowding of the anterior teeth.
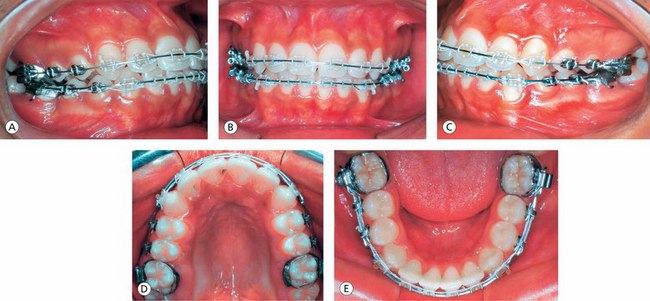
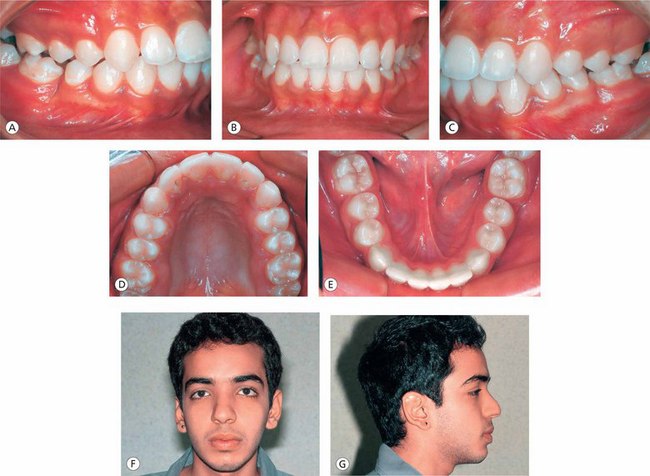
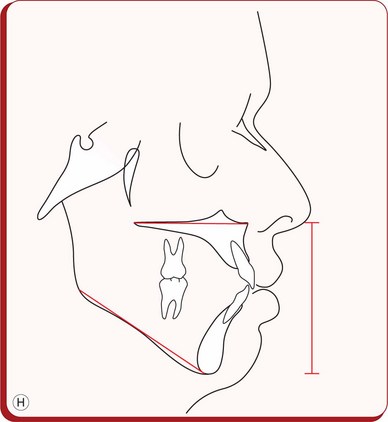
Figure 4.26 (A–E) Posttreatment intraoral photographs show good alignment and levelling of teeth, normal overjet and overbite relationships and good archforms. (F and G) Posttreatment extraoral photographs showing a good facial balance exhibiting normal nasiolabial angle, lip competency and chin position. (H) Posttreatment lateral cephalometric tracing showing significantly improved dental, skeletal and soft tissue relationships.
Mandibular bite blocks and vertical-pull chin cup
Another method used in the management of high-angle cases is the use of mandibular bite blocks combined with vertical-pull chin cup.38 Mandibular bite block along with vertical chin cup therapy intrudes posterior teeth, brings about counterclockwise rotation of the mandible, promotes favourable vertical height control throughout the growth period and facilitates closure of anterior open bite.39 However, the positive effects of extraction treatment combined with the use of a high-pull headgear are confined mainly to the maxillary dentoalveolar region.
Vertical-pull chin cup, used in association with a Kloehn cervical headgear, produces significant favourable skeletal and dental alterations by inhibiting maxillary molar eruption and descent of the maxilla and redirecting mandibular growth in a more horizontal direction.40 An increase in PFH has been the main contributing factor in the success of this approach. It is evident from the above discussion that the vertical-pull chin cup is the only appliance that effectively alters mandibular shape by decreasing gonial angle, redirecting condylar growth and increasing posterior heights. This modality seems to be favourable in achieving the main goal of hyperdivergent skeletal open bite treatment to improve the orientation, position and shape of the mandible.
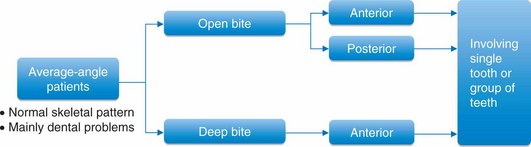
Management of vertical problems in average-angle patients
Vertical dentoalveolar discrepancies like open bite, deep bite etc are often associated with individuals with normal vertical dimension (Fig 4.27). Vertical problems in patients having average or normal MP angle are mainly dentoalveolar in nature involving single or group of teeth. Treatment of such patients is aimed at improving vertical abnormalities of teeth while simultaneously maintaining the vertical dimension.
Dentoalveolar open bite
Patients with anterior open bite due to displacement of the teeth should be carefully analyzed to design a treatment plan. Tongue posture, tongue function and eruption problems should be primarily considered in such cases. It is important to correlate the findings of the functional assessment and cephalometric analysis to establish an accurate diagnosis. In dentoalveolar open bite, the severity of the condition depends on the extent of the eruption of the teeth – infraocclusion of the incisors or supraocclusion of the molars. The dentoalveolar profile of a patient with a vertical growth pattern consists of upper anterior protrusion combined with lingual inclination of the lower incisors. The proclination of both upper and lower incisors due to tongue posture and thrust is usually present in patients with horizontal growth pattern.
The proper treatment time and type depend on the aetiology and the localization of the problem. There are various treatment modalities possible during the various developmental periods of the dentition. The resolution of anterior open bite in the deciduous dentition should involve the control of the abnormal habits and the elimination of dysfunctions. If the anterior open bite is not associated with crowding of the maxillary anterior teeth or crossbite, one can expect spontaneous improvement once the deforming muscle activity is eliminated. In the early mixed dentition stage, screening therapy to eliminate abnormal muscle forces on the dentition is effective. This approach may not be useful in the late mixed dentition stage, wherein fixed appliance therapy along with swallowing exercises is the treatment modality of choice. Following the fixed appliance therapy, patient usually requires a long-term posttreatment retention until the abnormal muscle function is eliminated. Swallowing exercises like asking the patient to put the tip of the tongue behind the upper and lower incisors promote the transition from the infantile to a mature deglutitional and functional pattern of the tongue.
If the dentoalveolar anterior open bite is because of supraeruption of posterior teeth, it is advisable either to intrude posterior teeth or to prevent further eruption of these by using posterior bite blocks with or without the headgear.
Dentoalveolar deep overbite
The deep overbite is the amount and percentage of vertical overlap of the lower incisors by the upper incisors. The overbite varies from childhood to adulthood; between 9 and 12 years of age, it increases, whereas between the age 12 and adulthood, it decreases.41 In the management of the deep overbite, it is important to consider the sagittal relationship and the direction and amount of growth to be expected for a particular patient. The dentoalveolar deep overbite could be either due to infraocclusion of posterior teeth or due to supraeruption of incisors. An accurate diagnosis should be established before planning the treatment. The dentoalveolar deep bite due to infraocclusion of molars is characterized by partially erupted molars, large interocclusal space and short distances between the maxillary basal plane, occlusal plane and mandibular basal plane. The deep overbite caused by supraeruption of incisors is characterized by fully erupted molars, normal interocclusal space, excessive curve of Spee and incisal edges of incisors extending beyond the functional occlusal plane (Figs 4.28–4.31). Therefore, the correction of dental deep overbite can be achieved by intrusion of incisors, extrusion of molars or combination of incisor intrusion and molar extrusion.
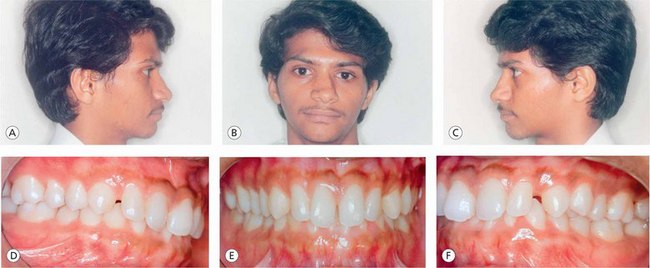
Figure 4.28 (A–C) Pretreatment extraoral photographs of a patient with normal vertical facial relationships. (D–F) Pretreatment intraoral photographs showing Class I molar relationship, rotated maxillary central incisors with median diastema and deep overbite.

Figure 4.29 Since vertical skeletal relationships are normal, the treatment plan included the alignment and intrusion of maxillary incisors while simultaneously maintaining the lower anterior facial height. (A–C) The initial treatment mechanics involved the use of maxillary intrusion arch tied to the segmental archwire on the incisors between central and lateral incisors, along with rigid posterior segmental archwires to reinforce the anchorage.
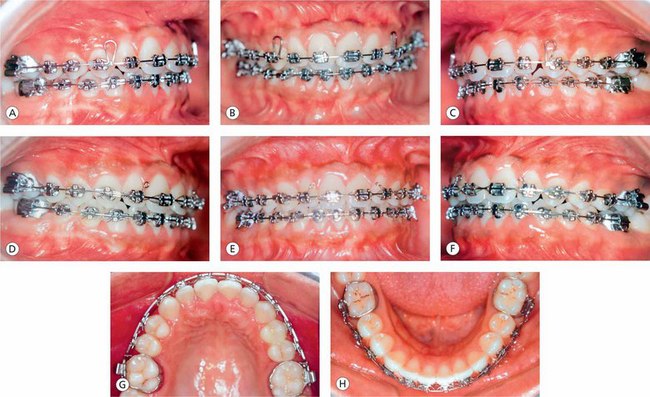
Figure 4.30 (A–C) Postintrusion treatment mechanics involved the use of teardrop looped archwire in the maxillary arch to close the residual space distal to the lateral incisors and the alignment, levelling and torque control in the mandibular arch. (D–F) Continuous finishing archwires in the maxillary and mandibular arches. (G and H) Well-coordinated and compatible maxillary and mandibular archforms.

Figure 4.31 (A) Posttreatment intraoral photographs showing normal overbite and overjet relationships, levelling, alignment and interproximal space closure. (B) Posttreatment use of a gnathological tooth positioner.
In patients with deep overbite caused by the supraeruption of maxillary incisors, intrusion of incisors is the treatment of choice. Before implementing the intrusion mechanics, it is essential to assess the inclination of incisors and the position of the incisor root apex with respect to the nasal floor (NF). The vertical space within the alveolar process, between the root apex and the NF, should permit the desired amount of incisor intrusion.
Burstone42 has outlined six principles that must be considered in incisor or canine intrusion mechanics.
1. Force levels – optimal magnitude, constant delivery and low-load deflections
2. Selection of the point of force application with respect to the centre of resistance of the teeth to be intruded
3. Use of the single-point contact in the anterior region
4. Selective intrusion based on anterior tooth geometry
5. Posterior anchorage to control over the reactive unit
6. Control over the undesirable extrusive effects on the posterior teeth
One of the primary goals of deep overbite correction in Class II malocclusion, especially in Class II division 2 cases, is to achieve long-term stability of the corrected overbite. The proclination of the incisors during orthodontic therapy may cause relapse of the corrected deep overbite in the postretention period.43 The relapse of corrected deep overbite is mainly due to continued lower incisor eruption, retroclination of incisors and forward rotation of the mandible with continued growth.44 The relapse potential of treated overbite is also associated with the interincisal angle and the lower AFH.45
The correction of deep overbite is considered to be stable in patients with a posttreatment interincisal angle between 125° and 135°, showing more relapse potential in brachycephalic patients than others. Therefore, the primary goal of deep overbite correction is to achieve proper torque of incisors and proper interincisal angle to prevent their continued eruption, with a special attention to the lower anterior face height and forward rotation of the mandible with continued growth (Figs 4.32–4.35).
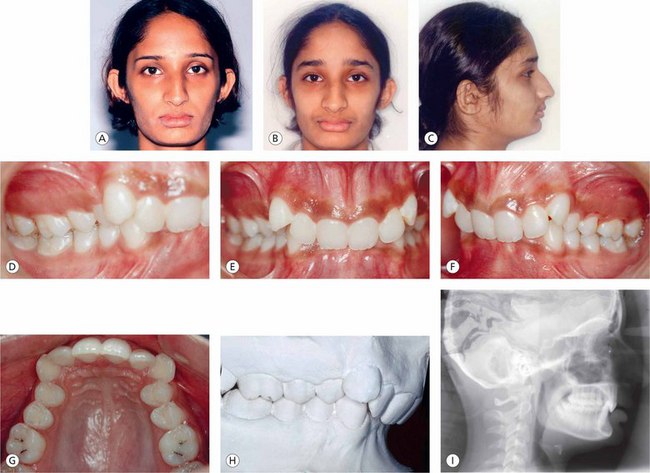
Figure 4.32 (A–C) Pretreatment extraoral photographs exhibiting severe decrease in lower facial height and deep mentolabial groove. (D–G) Pretreatment intraoral photographs demonstrate severe deep bite, retroclined maxillary incisors, high labially placed upper cuspids, square maxillary archform and Class II molar relationship. (H) Pretreatment study model demonstrates severe discrepancy between the posterior and anterior occlusal planes. (I) Pretreatment lateral cephalogram exhibits decreased lower anterior facial height, nearly parallel mandibular and palatal planes and retroclined and supraerupted maxillary incisors.
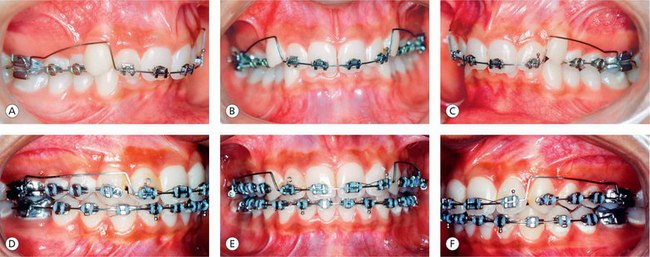

Figure 4.33 Since severely compromised lower anterior facial height and severe deep bite are the main components contributing to the development of a problem, the primary treatment goal is to intrude maxillary incisors and encourage vertical movement of posterior dentoalveolar segments to increase the lower anterior facial height. (A–G) Maxillary intrusion arch is in place to intrude and establish proper incisor torque.
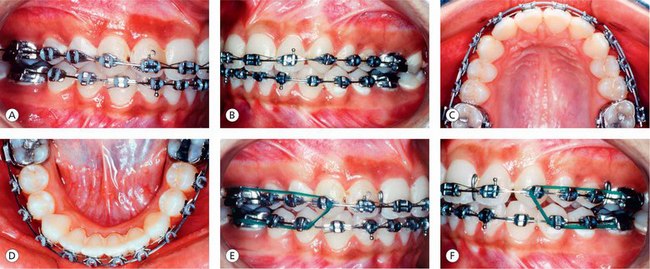
Figure 4.34 (A–D) Post intrusion treatment mechanics to resolve upper and lower anterior arch discrepancy, establish proper archforms and detailing of dentition. (E and F) Patient wearing anterior bite plate and posterior box elastics to encourage vertical eruption of posterior dentoalveolar units.
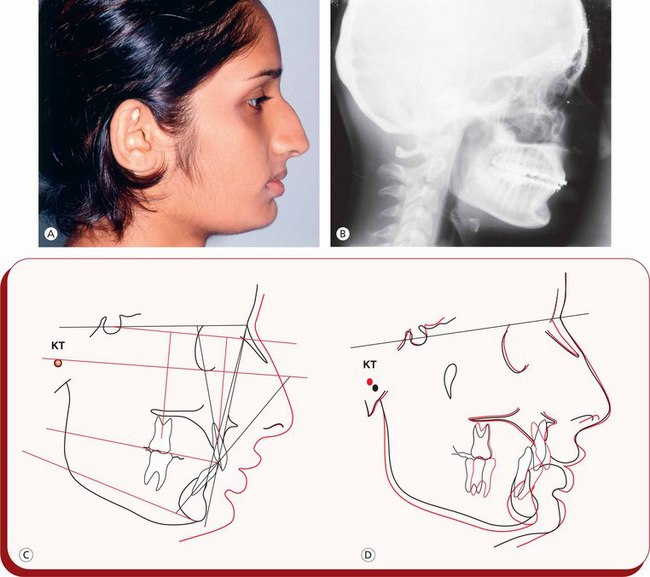
Figure 4.35 (A) Posttreatment extraoral photograph exhibiting improved facial features and vertical facial relationships. (B) Posttreatment lateral cephalogram. (C) Posttreatment cephalometric tracing. (D) Pretreatment and posttreatment cephalometric superimpositions.
Intrusion of incisors: It is challenging for the orthodontists to correct deep overbite in patients with flared incisors by using conventional continuous archwires without producing any untoward movements. In such patients, uprighting flared incisors to their better axial inclinations is often associated with lengthening their crowns, leading to the deepening of the overbite. In order to prevent further flaring of incisors during treatment, the simultaneous overbite correction and space closure is the treatment mechanics of choice in dealing with such cases. It has been observed that the possibility of flaring out of the maxillary incisors is more in Class II division 1 than in Class II division 2 malocclusions.46,47 When using a utility arch to intrude incisors, the mechanics should be based on sound biomechanical principles for efficient tooth movement. An application of force should be directed through the centre of resistance of a tooth to be intruded to ensure translation without any tipping. It is, therefore, important to determine the centre of resistance of a particular tooth to design biomechanically sound force system. The intrusion arch should be attached to a sectional archwire in the four upper incisors distal to the lateral incisors as the centre of resistance of the upper front teeth is supposed to be situated at this point anteroposteriorly.46,48
The reaction forces exerted by the intrusion arches during the intrusion mechanics should be controlled and neutralized by the posterior units. When the posterior units consist of only the first molars on either side, the reaction forces will cause extrusion, distal tipping and, occasionally, the palatal tipping of these teeth. Therefore, the posterior anchorage units must be reinforced to control these reaction forces, especially in patients with increased lower facial height, to prevent clockwise rotation of the mandible and further lengthening of the face. The use of a transpalatal arch along with the rigid rectangular posterior sectional archwires, headgear and bite plate covering the occlusal surfaces of premolars and molars are some of the methods to stabilize the posterior units. Also, apical root resorption is found in patients with isolated incisor intrusion; however, there was no correlation between the amount of root resorption and the tooth type – central or lateral incisor49 – and between the position of the apex in relation to the NF50 and the amount of intrusion.51
Orthodontic camouflage: A treatment alternative for skeletal discrepancy
Orthodontic camouflage consists of the repositioning of the dentition in order to obtain proper molar and incisor relationships in patients with underlying skeletal discrepancies with a favourable effect on facial aesthetics. For some reason, if the patient does not accept the orthosurgical treatment approach for the correction of a dentofacial deformity, camouflage proves to be quite useful. The goal is to achieve certain degree of dentofacial aesthetics and is to establish proper occlusion, accepting the limitations in skeletal relationships. The success of camouflage treatment approach depends on the severity of underlying skeletal discrepancy. In mild to moderate skeletal malocclusions, movement of teeth to achieve dentoalveolar changes and aesthetic results are much better than those in severe skeletal problems. In severe Class II patients, the need for greater displacement of teeth relative to their bony bases, either by extraction or by nonextraction approach, is possible due to improvements in orthodontic treatment mechanics but only at considerable expense to facial aesthetics. Therefore, the clinician should assess the case carefully for the underlying skeletal discrepancy to plan treatment mechanics and strike a balance between occlusal and facial aesthetic goals using camouflage approach.
Management of short-face patients
As there is a strong correlation between the vertical and sagittal dimension, any discrepancy in the vertical dimension contributing to the development of a problem can influence the anteroposterior dental and skeletal relationships (Fig 4.36). An increased overbite relationship may be associated with average lower facial height; however, when it is related to the overclosure of the mandible through an excessive freeway space, it results in a decreased lower anterior face height. It has been observed that the mandibular rest position remains unchanged as growth progresses, and neither the presence nor the absence of teeth affects this position.52 The excess interocclusal clearance or the freeway space as seen in the patients with mandibular overclosure may be due to a lack of vertical development in the buccal alveolar segments.53 This could be the result of defects in tooth eruption or interference with normal tooth eruption.
The primary goal of treatment in the management of patients with diminished lower face height should be to improve vertical facial proportions. This can be accomplished in growing patients by encouraging vertical growth of the maxillary complex with headgears and by growth of the posterior alveolar processes along with the use of functional appliances, in adolescent patients by allowing posterior teeth eruption, and in adult population by surgical correction.
In growing patients with decreased lower AFH, orthopaedic repositioning of the maxilla and the mandible should be considered. Most patients can benefit from maxillary expansion due to desired downward movement associated with this procedure54,55 The use of cervical-pull headgear plays an important role in increasing the lower facial height through encouragement of vertical growth of maxillary complex and dental eruption. This vertical movement promotes downward and backward rotation of the mandible with a resultant increase in lower facial height and a change in the interarch relationship in a Class II direction. This unfavourable Class II relationship should be minimized by the distal component of the cervical-pull headgear force and mandibular growth. Treatment mechanics to achieve desired tooth movements depends on the age of the patient and whether the Class II correction is being carried out with the functional appliance (Figs 4.37–4.39). In the early correction of dental deep overbite, if the patient is undergoing sagittal correction with the functional appliance like activator and twin-block appliance, the desired posterior teeth extrusion can be achieved by prescribed occlusal relieving of molars and premolars to encourage orthodontic tooth guidance while simultaneously exerting an intrusive force on the anterior teeth. This also promotes the levelling of curve of Spee. In growing patients with lateral tongue thrust and posture, the abnormal tongue function prevents the full eruption of posterior teeth. This can be controlled by a removable plate-type appliance with lateral tongue crips and buccinator loop extensions of the labial bow to permit extrusion and elongation of bicuspids and molars. Therefore, functional appliance therapy may be the treatment modality of choice to correct the sagittal relationships and to allow for vertical development of the lower face in growing patients exhibiting Class II dental relationships.

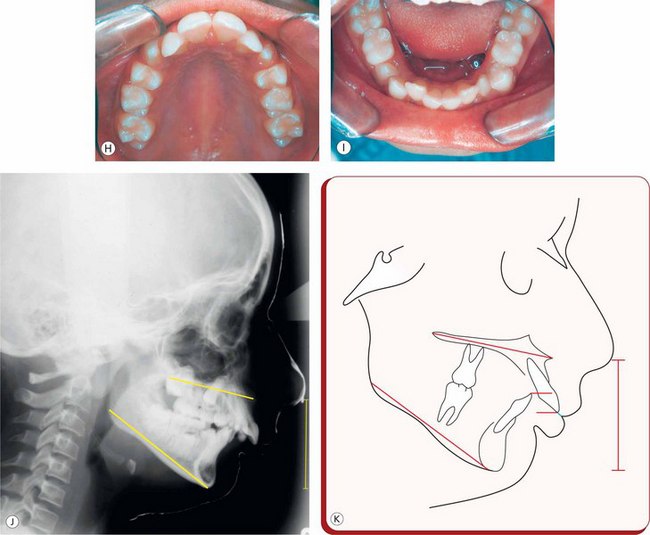
Figure 4.37 (A–D) Pretreatment extraoral photographs of a growing female patient showing convex profile, decreased lower facial height, incompetent lips, deep mentolabial groove, receding chin and lower lip trap. (E–I) Pretreatment intraoral photographs showing typical features of a severe Class II division 1 malocclusion in a late mixed dentition stage. Patient also exhibits moderate crowding in the upper and lower arches. (J and K) Pretreatment lateral cephalogram and tracing.
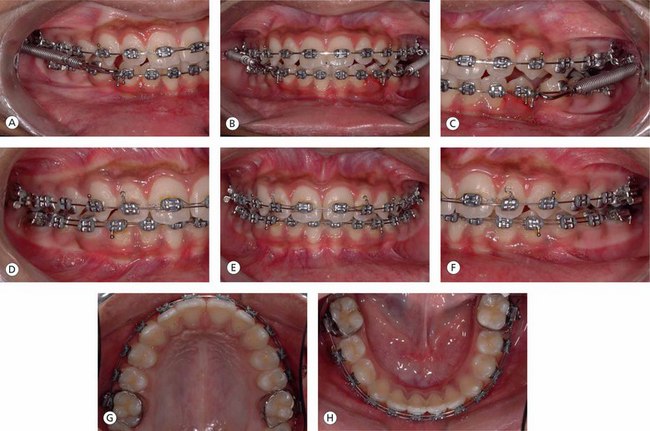
Figure 4.38 Since the patient's problem is characterized by receding chin and decreased lower anterior facial height, the primary focus of treatment is on advancing the mandible downward and forward and promoting posterior vertical dentoalveolar growth. (A–C) Fixed functional appliance in place to advance the mandible. (D–H) Settling of occlusion and coordination of upper and lower archforms during the postfixed functional therapy.

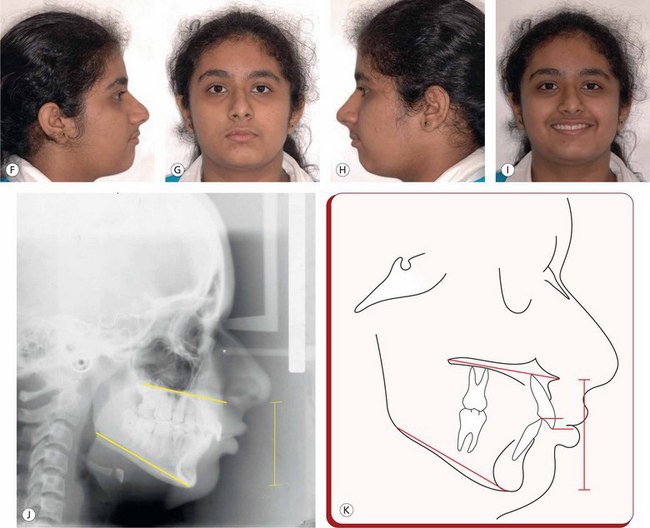
Figure 4.39 (A–E) Posttreatment Class I molar and cuspid relationships, normal overjet and overbite and well-coordinated and compatible archforms. (F–I) Posttreatment extraoral photographs demonstrate orthognathic profile exhibiting improved vertical dimension of lower face. (J and K) Posttreatment lateral cephalogram and tracing.
The orthopaedic face mask commonly used in the treatment of Class III malocclusions in growing patients consists of bilateral forces emanating from a face mask and applied to the intraoral appliance to the first molar or canine regions (Figs 4.40–4.42). The line of the protraction forces as determined sagittally by the commissure of the lips and the intraoral points of attachment influences the type of dentomaxillary complex movement. For true protraction to occur, the direction of protraction forces must pass through the centres of resistance of the dentomaxillary complex and parallel to the occlusal plane. It is therefore essential to locate the centres of resistance of the dentomaxillary complex. The centre of resistance of the dentomaxillary complex, as seen on a lateral cephalogram, is located on a line drawn perpendicular to the functional occlusal plane through the distal aspect of the maxillary first molar.56 It is identified on this perpendicular line at one half the distance from the functional occlusal plane to a line through the inferior border of the orbit (parallel to the functional occlusal plane). It is recognized that the protraction forces of the face mask cause dentomaxillary rotation (counterclockwise) that results in an increase in the lower facial height and a decrease in the upper facial height.57
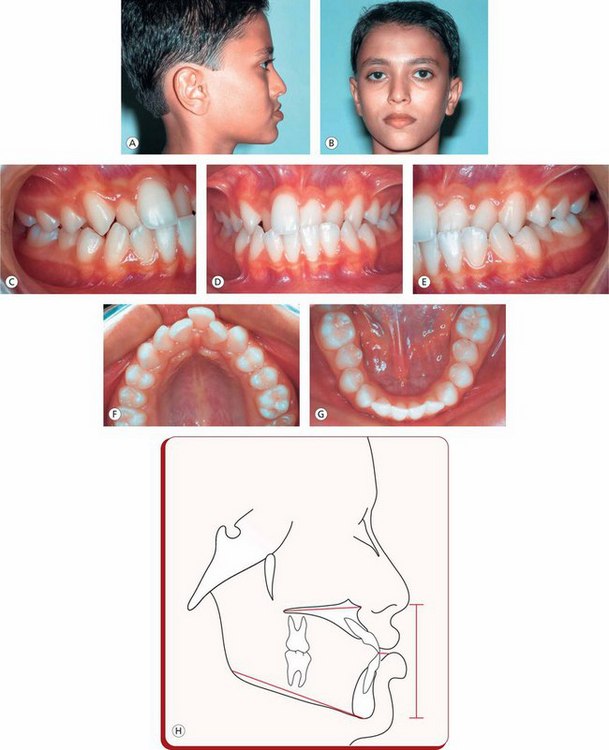
Figure 4.40 (A and B) Pretreatment extraoral photographs demonstrating decreased lower facial height, concave profile, malar insufficiency and prominence of the lower lip and chin. (C–G) Pretreatment intraoral photographs show a Class III molar relationship, anterior crossbite and crowding in the upper and lower anterior segments. (H) Pretreatment lateral cephalometric tracing exhibits the typical features of Class III malocclusion characterized by a combination of maxillary deficiency and mandibular prognathism.

Figure 4.41 Since decreased lower facial height, deficient premaxilla and prognathic mandible are the main components contributing to the development of patient's problem, the treatment goal is to protract the maxilla and increase the lower anterior facial height. It was therefore decided to initiate the treatment with the orthopaedic facial mask followed by a fixed appliance therapy. (A–C) Maxillary bonded splint with a rapid palatal expansion device in place. (D and E) The use of orthopaedic facial mask. Note: the force exerted on the maxilla is downward and forward that will displace the maxilla anteriorly and inferiorly with a resultant downward and backward rotation of the mandible leading to increase in the lower anterior facial height.
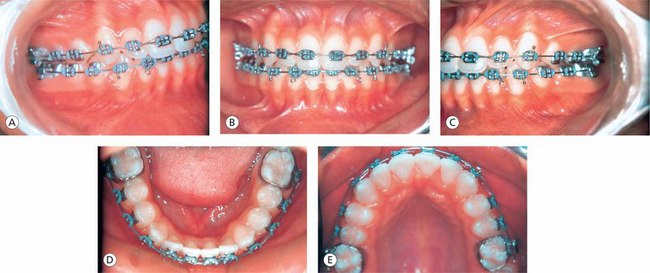
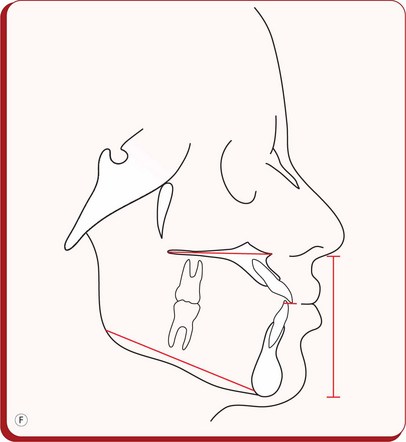
Figure 4.42 (A–E) Postorthopaedic treatment fixed appliance therapy to finetune the dentition. (F) Posttreatment lateral cephalometric tracing exhibiting an improvement in dental, skeletal and soft tissue relationships with an emphasis on improved vertical dimension of lower face.
In a growing patient undergoing fixed appliance therapy where a clockwise rotation of the mandible is desirable, extrusion of molars may prove to be useful. There are many methods to bring about this change, e.g. anterior bite plate, leaving molars free to erupt, cervical-pull headgear, Class II elastics and anchorage bends or tip-back bends in the upper and lower arches. It is the author's experience that to achieve this result, the use of anterior bite plate, leaving the molars free to erupt, along with the use of posterior box elastics works very well. In a growing individual, the use of reverse curve of Spee mechanics produces supraeruption of the mandibular posterior teeth leading to downward and backward rotation of the mandible. This results in a reduction of a deep overbite and in an increase in the MP angle, the AFH and facial convexity. The use of intermaxillary elastics over a period of time in a Class II clinical situation leads to the eruption of mandibular molars and in Class III traction leads to the eruption of the maxillary posterior teeth. These changes are often associated with the rotation of the occlusal plane.
The use of a reverse curve of Spee in archwire in the edgewise brackets produces undesirable changes in the axial inclinations of the posterior teeth and flaring of the incisors.48
Conclusion
Vertical discrepancies consist of various components of the craniofacial complex. The clinician must establish differential diagnosis of vertical problem as it forms an integral part of designing a successful treatment strategy. While dealing with the patients with vertical problems, it must be recognized that all cases cannot be treated in a similar manner due to extreme variation in facial pattern and morphological characteristics. Therefore, in patients with compromised AFHs, various treatment methods of mandibular rotation – opening versus closure – as a part of orthodontic treatment should be recognized as either desirable or undesirable. Control of vertical dimension is considered to be the most important factor in successfully treating patients with vertical discrepancies. The primary treatment goal in patients with hyperdivergent malocclusions is to autorotate the mandible to decrease the lower facial height; in patients with average facial height, the goal is to correct vertical dental problems while simultaneously maintaining the vertical dimension; and in low-angle patients, various treatment procedures should contribute to the downward and backward rotation of the mandible resulting into an increased lower facial height.
References
1. Brodie, A.G. On the growth pattern of the human head from the third month to the eighth year of life. Am J Anat. 1941;68:209–262.
2. Schudy, F.F. Vertical growth versus antero-posterior growth as related to function and treatment. Angle Orthod. 1964;34(2):75–93.
3. Coben, S.E. Growth and Class II treatment. Am J Orthod. 1966;52(1):5–26.
4. Pederson, R.A. Cranial base growth. Individual variation studied roentgenographically, MS Thesis. Philadelphia, USA: Temple University, 1962.
5. Powell, T.V., Brodie, A.G. Closure of the spheno-occipital synchon-drosis. Anat Rec. 1963;147:15–23.
6. Coben, S.E. The integration of facial skeletal variants. Am J Orthod. 1955;41:407–434.
7. Björk, A. Facial growth in man, studied with the aid of metallic implants. Acta Odontol Scand. 1955;13:9–34.
8. Björk, A. Variations in the growth pattern of the human mandible: longitudinal cephalometric study by the implant method. J Dent Res. 1963;42(1):400–411.
9. Björk, A. Sutural growth of the upper face studied by the implant method. Acta Odontol Scand. 1966;24:109–129.
10. Björk, A. The use of metallic implants in the study of facial growth in children: method and application. Am J Phys Anthropol. 1968;29:243–254.
11. Björk, A. Prediction of mandibular growth rotation. Am J Orthod. 1969;55:585–599.
12. Björk, A., Skieller, V. Facial growth and development. An implant study at the age of puberty. Am J Orthod. 1972;48:61–74.
13. Björk, A., Skieller, V. Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983;5:1–46.
14. Isaacson, R.J., Zapfel, R.J., Worms, F.W., et al. Effects of rotational jaw growth on the occlusion and profile. Am J Orthod. 1977;72(3):276–286.
15. Issacson, J.R., Issacson, R.J., Speidel, T.M., et al. Extreme variation in vertical facial growth and associated variation in skeletal and dental relationships. Angle Orthod. 1971;41:219–228.
16. Janson, G., Metaxas, A., Woodside, D. Variation in maxillary and mandibular molar and incisor vertical dimension in 12 years old subjects with excess, normal, and short lower anterior face height. Am J Orthod Dentofacial Orthop. 1994;106:409–418.
17. Linder-Aronson, S. Effects of adenoidectomy on the dentition and facial skeleton over a period of five years. In: Cook J.T., ed. Transactions of the third International orthodontic congress. St. Louis: Mosby; 1975:85–100.
18. Woodside, D.G., Linder-Aronson, S., Lundstrom, A., et al. Mandibular and maxillary growth after changed mode of breathing. Am J Orthod Dentofacial Orthop. 1991;100:1–18.
19. Sassouni, V., Nanda, S. Analysis of dentofacial vertical proportions. Am J Orthod. 1964;50:801–823.
20. Ingervall, B., Thilander, B. Relationship between facial morphology and activity of the masticatory muscles. J Oral Rehabil. 1974;1:131–147.
21. Jarabak, J.R., Fizzell, J.A. Technique and treatment with light wire edgewise appliances, 2nd, St. Louis: CV Mosby, 1972.
22. Björk, A. The face in profile: an anthropological X-ray investigation on Swedish children and conscripts. Sven Tandlak Tidskr. 40(suppl), 1947.
23. Björk, A. Prediction of mandibular growth rotation. Am J Orthod. 1969;55:585–599.
24. Skieller, V., Björk, A., Linde-Hansen, T. Prediction of mandibular growth rotation evaluated from a longitudinal implant sample. Am J Orthod. 1984;86:359–370.
25. Moyers, R.E., Guire, K.E., Riolo, M. Differential diagnosis of Class II malocclusion. Am J Orthod. 1980;78:477–494.
26. Profitt, W.R., Fields, H.W., Nixon, N.L. Occlusal forces in normal and long-face adults. J Dent Res. 1983;62:566–570.
27. Björk, A. The relationship of the jaws to the cranium. In: Lundstrom A., ed. Introduction to orthodontics. London: McGraw-Hill; 1961:104–140.
28. Subtelny, J.D., Sakuda, M. Open-bite: diagnosis and treatment. Am J Orthod. 1964;50:337–358.
29. Nahoum, H.I., Horowitz, S.L., Benedicto, E.A. Varieties of anterior open-bite. Am J Orthod. 1972;61:486–492.
30. Armstrong, M.M. Controlling the magnitude, direction and duration of extraoral force. Am J Orthod. 1971;59:217–243.
31. Firouz, M., Zernik, J., Nanda, R. Dental and orthopaedic effects of high-pull headgear in treatment of Class II division 1 malocclusion. Am J Orthod. 1992;102:197–205.
32. Caldwell, S.F., Hymas, T.A., Timm, T.A. Mxillary traction splint: a cephalometric evaluation. Am J Orthod. 1984;85:376–384.
33. Pearson, L.E. Vertical control in treatment of patients having backward rotational growth tendencies. Angle Orthod. 1978;48(2):132–140.
34. Dougherty, H.L. The effect of mechanical forces upon the mandibular buccal segments during orthodontic treatment. Am J Orthod. 1968;54:29–49.
35. Pearson, L.E. Vertical control through use of mandibular posterior intrusive forces. Angle Orthod. 1973;43:194–200.
36. Staggers, J.A. Vertical changes following first premolar extractions. Am J Orthod Dentofacial Orthop. 1994;105:19–24.
37. DiPalma, D. A morphometric study of orthopaedic and functional therapy for the hyperdivergent skeletal pattern, Master's thesis. Celveland, Ohio: Case Western Reserve University, 1982. [May].
38. Progressive increase in lower anterior face height and the use of posterior occlusal bite-block in its management. In: Woodside D., Linder-Aronson S., Graber L.W., eds. Orthodontics: state of the art, essence of the science. St. Louis: Mosby; 1986:200–221.
39. Pearson, L.E. Case report KP. Treatment of a severe open-bite excessive vertical pattern with an eclectic nonsurgical approach. Angle Orthod. 1991;61:71–76.
40. Haas, A.J. A biological approach to diagnosis, mechanics and treatment of vertical dysplasia. Angle Orthod. 1980;50:279–300.
41. Flemming, H.B. Investigation of the vertical overbite during the eruption of the permanent dentition. Angle Orthod. 1961;31:53–62.
42. Burstone, C.R. Deep overbite correction by intrusion. Am J Orthod. 1977;72(1):1–22.
43. Simons, M.E., Joondeph, D.R. Change in overbite: a ten year postretention study. Am J Orthod. 1973;64(4):349–367.
44. Ball, J.V., Hunt, N.P. The effect of Andresen, Harvold and Begg treatment on overbite and molar eruption. Eur J Orthod. 1991;13:53–58.
45. McAlpine, J.E. A comparison of overbite relapse to age, interincisal angle and lower face height in Class II deep bite cases, Master's thesis. USA: Loma Linda University, 1976.
46. Melsen, B., Agerbaek, N., Eriksen, J., et al. New attachment through periodontal treatment and orthodontic intrusion. Am J Orthod. 1988;94(2):104–116.
47. Demange, C. Equilibrium situations in bend force systems. Am J Orthod. 1990;98:333–339.
48. Nanda, R. The differential diagnosis and treatment of excessive overbite. Dent Clin North Am. 1981;25(1):69–84.
49. Dermaut, L.R., DeMunck, A. Apical root resorption of upper incisors caused by intrusive tooth movement: a radiographic study. Am J Orthod. 1986;90(4):321–326.
50. Linge, B.O., Ling, J. Apical root resorption in upper anterior teeth. Eur J Orthod. 1983;5:173–183.
51. Costopoulous, G., Nanda, R. An evaluation of root resorption incident to orthodontic intrusion. Am J Orthod. 1996;109(5):543–548.
52. Thompson, J.R., Brodie, A.G. Factors in the position of the mandible. J Am Dent Assoc. 1942;29:925–942.
53. Linder-Aronson, S., Woodside, D.G. Some craniofacial variables related to small or diminishing lower anterior face height. Swed Dent J Suppl. 1982;15:131–146.
54. Da Silva, O.G., Boas, M.C.V., Capelozza, L. Rapid maxillary expansion in the primary and mixed dentitions: a cepahlometric evaluation. Am J Orthod Dentofacial Orthop. 1991;100:171–181.
55. Davis, W.M., Kronman, J.H. Anatomical changes induced by splitting of the midpalatal suture. Angle Orthod. 1969;39:126–132.
56. Lee, K., Young, K.R., Young, C.P., et al. A study of holographic inter-ferometry on the initial reaction of the maxillofacial complex during protraction. Am J Orthod Dentofacial Orthop. 1997;111:623–632.
57. Nanda, R., Bruce, G. Biomechanical approaches to the study of alterations of facial morphology. Am J Orthod. 1980;78:213–226.