Physiology of Micturition
 Filling of urinary bladder
Filling of urinary bladderUrinary bladder and urethra
Functional anatomy
The urinary bladder, a hollow muscular viscus, is a temporary reservoir for urine. The main body of empty bladder is pyramidal, having an apex and a base. The lowest part of the bladder is called neck, which continues as urethra.
Interior of the bladder. In an empty bladder, the greater part of the mucosa shows irregular folds due to its loose attachments to the muscular coat. The interior of the base (posterior surface) of the bladder presents a triangular area, the trigone where the mucosa is smooth due to its firm attachment.
Internal urethral orifice is located at the apex (inferior angle) of the trigone. The ureters open into the bladder at superior angles of the trigone (Fig.6.5-1). The ureters pierce the bladder wall obliquely, and this provides a valve-like action, which prevents a reverse flow of urine towards the kidneys as the bladder fills.
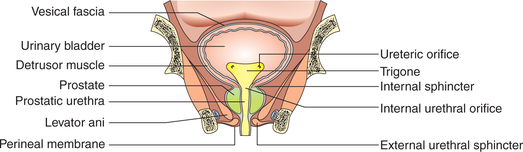
Fig. 6.5-1 Coronal section through the bladder and prostate to show the interior of the bladder, internal urethral sphincter and external urethral sphincter.
Structure of the bladder
The wall of the urinary bladder consists of three layers: an inner mucous membrane, a thick coat of smooth muscle and the outer serous layer.
Mucous membrane is lined by the transitional epithelium.
Muscular layer is formed by smooth muscle fibres, which constitute the detrusor muscle. Contraction of this muscle coat is responsible for emptying of the bladder.
Serous coat is a reflection of peritoneum and covers only superior surface.
Urethra and its sphincters
Male urethra is about 20 cm in length and is divided into three parts: prostatic urethra (3 cm), membranous urethra (1.25 cm) and penile urethra (15.75 cm). Membranous urethra is surrounded by the external sphincter.
Female urethra is about 3.8 cm long. It extends from the neck of the bladder to the external meatus. It traverses the external sphincter and lies immediately in front of the vagina.
Sphincters of the urethra
1. Internal sphincter. The circular smooth muscle fibres in the area of the neck of bladder are thickened to form the internal sphincter (sphincter vesicae). The natural tone of the internal sphincter prevents emptying of the bladder until the pressure in the body of bladder rises above a threshold level.
2. External sphincter. Beyond the bladder neck, it is encircled by a ring of voluntary (skeletal type) muscle known as external sphincter of the bladder. The external sphincter provides voluntary control over micturition.
Innervation of the urinary bladder (Fig.6.5-2)
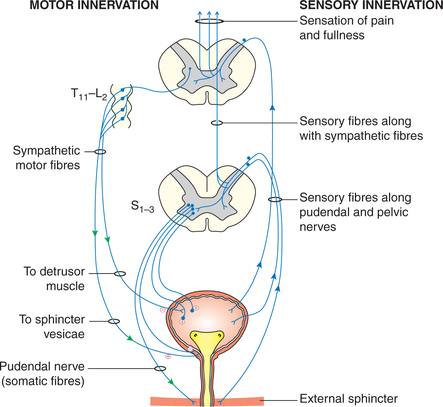
Parasympathetic innervation. The parasympathetic efferent fibres (nervi erigentes) are derived from the second, third and fourth sacral segments (mainly S2 and S3). These fibres carry motor impulses to the urinary bladder causing contraction of detrusor muscle and emptying of the bladder. These fibres are inhibitory to the internal sphincter.
Sympathetic innervation. These nerves arise in the 11th thoracic to the second lumbar segments (T11–L2). These fibres are said to be inhibitory to detrusor muscle and motor to the sphincter vesicae.
Somatic motor innervation. The somatic pudendal nerve (S2, S3 and S4) supplies the external sphincter which is voluntary.
Sensation of bladder distension. Afferents from the detrusor stretch receptors travel to the spinal cord via the pelvic splanchnic nerve (nervi erigentes). From the region of the bladder neck and trigone, the afferents travel via the hypogastric plexus to spinal cord segments T11–L2.
In the spinal cord, the fibres of awareness of bladder distension run in the posterior column (fasciculus gracilis) to reach the spinal, pontine and suprapontine micturition centres.
Sensation of bladder pain. The pain fibres are stimulated by excessive distension or spasm of the bladder wall, or by stone, inflammation or malignant disease irritating the bladder. The pain fibres run predominantly in the hypogastric plexus but are also present in the nervi erigentes.
In the spinal cord, the fibres carrying pain sensation run in the lateral spinothalamic tract.
Urethral sensations include sensation of imminent voiding associated with maximal bladder filling, and reach the spinal cord via the pudendal nerve.
In the spinal cord, fibres carrying urethral sensations travel in the dorsal column.
Physiology of micturition
Micturition is the process by which urinary bladder empties when filled. The main physiological events in the process of micturition are:
Filling of urinary bladder
Emptying of the bladder
Emptying of the bladder is basically a reflex action called the micturition reflex, which is controlled by supraspinal centres and is assisted by contraction of perineal and abdominal muscles.
Micturition reflex
Initiation. Micturition reflex is initiated by the stimulation of the stretch receptors located in the wall of urinary bladder.
Stimulus. Filling of bladder by 300–400 mL of urine in adults constitutes the adequate stimulus for the micturition reflex to occur.
Afferents. The afferents from the stretch receptors in the detrusor muscle and urethra travel along the pelvic splanchnic nerves and enter the spinal cord through dorsal roots to S2, S3 and S4 segments to reach the sacral micturition centre (Fig.6.5-3).
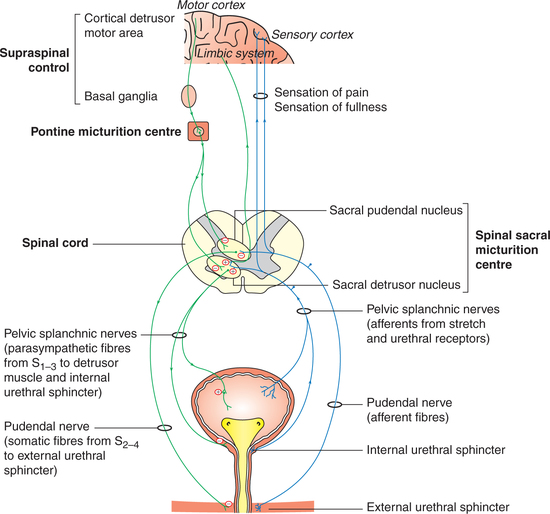
Sacral micturition centre is formed by the sacral detrusor nucleus and sacral pudendal nucleus.
Efferents. Efferents arising from the sacral detrusor nucleus are the preganglionic parasympathetic fibres, which relay in the ganglia near or within bladder and urethra (Fig.6.5-3). The postganglionic parasympathetic fibres are excitatory to the detrusor muscle and inhibitory to the internal sphincter.
Response. Once micturition reflex is initiated, it is selfregenerative, i.e. initial contraction of the bladder wall further activates the receptors to increase the sensory impulses (afferents) from the bladder and urethra, which cause further increase in the reflex contraction of detrusor muscle of the bladder. The cycle thus keeps on repeating itself again and again until the bladder has reached a strong degree of contraction.
Voluntary control of micturition
The micturition reflex is fundamentally a spinal reflex facilitated and inhibited by higher brain centres (supraspinal centres) and, like defaecation, is subjected to voluntary facilitation and inhibition. In infants and young children, micturition is purely a reflex action. Voluntary control is gradually acquired as a learned ability of the toilet training.
Supraspinal control centres which control the micturition reflex (a completely automatic cord reflex) include the pontine micturition centre (PMC) and suprapontine centres.
Role of perineal and abdominal muscles in micturition
Certain muscular movements, which aid the emptying of bladder, but are not the essential component of micturition process are:
• At the onset of micturition, the levator ani and perineal muscles are relaxed, thereby shortening the post-urethra and decreasing the urethral resistance.
• The abdominal muscles contract, accelerating the flow of urine by raising intra-abdominal pressure, which in turn secondarily increase the intravesical pressure, thereby increasing the flow of urine.