The lower limb examination and peripheral vascular disease
Examination anatomy
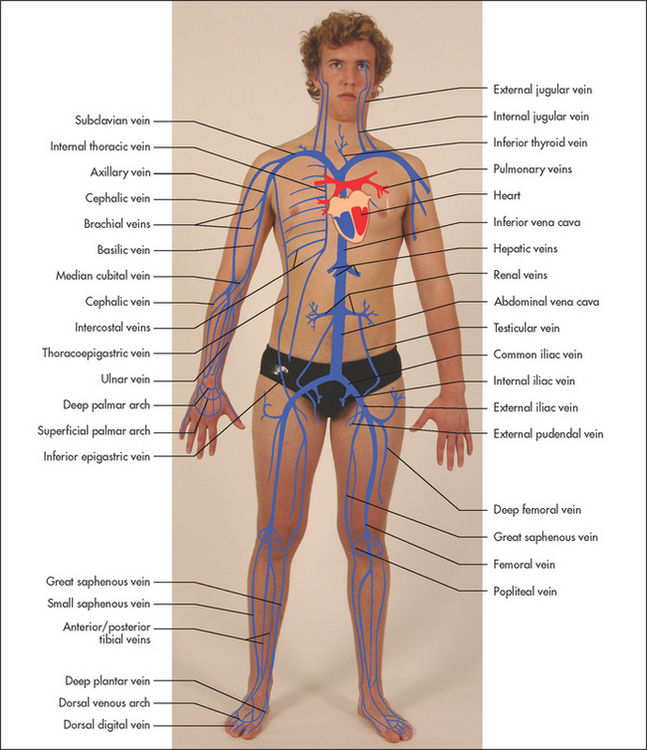
The arteries are normally palpable where they run close to the surface. Figures 5.2 and 6.1 shows their basic anatomy.
ARMS
Most of the blood supply of the arm is provided by the axillary artery which, after giving off some small branches in the upper arm, becomes the brachial artery. This divides into the radial and ulnar arteries, which run down the forearm following their bones. Both continue to the wrist where they go on to supply the hands and fingers. The radial artery is very superficial at the wrist and easily palpable. The veins of the arm include the digital veins of the hands, the cephalic and median vein of the forearm and the basilica vein, which runs the whole length of the arm. In the upper arm the brachial and cephalic veins run to the shoulder. These veins drain via the axillary vein into the superior vena cava.
LEGS
The main blood supply to the leg is from the external iliac artery, which becomes the femoral artery in the groin. Its main branches are the profunda femoris (deep femoral) artery in the thigh and the anterior and posterior tibial arteries in the lower leg. The posterior tibial artery is usually palpable behind the medial malleolus and the continuation of the anterior tibial—the dorsalis pedis is palpable over the dorsum of the foot. The veins of the leg include the longest vein in the body, the great saphenous vein. This superficial vein drains via perforating veins to the deep veins, which contain valves to assist return of blood to the heart. Damage to these valves, for example by venous thromboses, can lead to venous varicosities. The leg veins drain into the external iliac veins and then into the inferior vena cava.
LOWER LIMBS
See List 6.1. Palpate behind the medial malleolus of the tibia and the distal shaft of the tibia for oedema by compressing the area for at least 15 seconds with the thumb. This latter area is often tender in normal people, and gentleness is necessary. Oedema may be pitting (the skin is indented and only slowly refills—Figure 6.2) or non-pitting. Oedema due to hypoalbuminaemia often refills more quickly.
LIST 6.1 Lower limb examination
1. Inspection—anterior and lateral surfaces, sole of foot, between toes:
• Discolouration (e.g. venous staining; see Figure 6.3)

• Temperature: run the dorsum of the hand from the hips to the foot on each side. Note any reduction in temperature peripherally and compare left and right.
• Test capillary refill: press on the great toenail and release. The blanched nail bed should turn pink within 3 seconds.
• Test venous filling: occlude the dorsal venous arch of each foot in turn using two fingers; release the distal finger and look for venous refilling. Absence of venous refilling suggests poor arterial supply to the foot
• Pulses: feel for an abdominal aortic aneurysm, feel for a femoral pulse, the popliteal pulses (flex the patient’s leg), then feel the posterior tibial and dorsalis pedis pulses.
4. Perform Buerger’s test (see text).
5. Measure the ankle–brachial index.
6. Test lower limb sensation. Diabetes may cause sensory loss in a ‘stocking’ distribution.

Pitting oedema occurs in cardiac failure unless the condition has been present for a long time and secondary changes in the lymphatic vessels have occurred. If oedema is present, note its upper level (e.g. ‘pitting oedema to mid-calf’ or ‘pitting oedema to mid-thigh’). Severe oedema can involve the skin of the abdominal wall and the scrotum as well as the lower limbs. Causes and differential diagnosis of oedema are listed in Lists 6.2 and 6.3.
Non-pitting oedema suggests chronic lymphoedema that is due to lymphatic obstruction (see Figure 6.4). Lipoedema is a term used to describe fat deposition in the ankles. It typically spares the feet and affects obese women.

Figure 6.4 Lymphoedema (elephantiasis) (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
Look for evidence of Achillesa tendon xanthomata due to hyperlipidaemia. Also look for cyanosis and clubbing of the toes (this may occur without finger clubbing in a patient with a patent ductus arteriosus, because a rise in pulmonary artery pressures, sufficient to reverse the direction of flow in the shunt, has occurred).
Peripheral vascular disease
Examine both femoral arteries by palpating and then auscultating them. A bruit may be heard if the artery is narrowed. Next palpate the following pulses: popliteal (behind the knee—see Figure 6.5(a): if this is difficult to feel when the patient is supine, try the method shown in Figure 6.5(b)), posterior tibial (under the medial malleolus, see Figure 6.6(a)) and dorsalis pedis (on the forefoot, Figure 6.6(b)) on both sides.1

Figure 6.5 Palpating the popliteal artery: (a) patient supine; (b) patient prone (Courtesy of Glenn McCulloch)

Figure 6.6 Feeling (a) the posterior tibial artery and (b) the dorsalis pedis artery (Courtesy of Glenn McCulloch)
Patients with exertional calf pain (intermittent claudication) are likely to have disease of the peripheral arteries. More severe disease can lead to pain even at rest and to ischaemic changes in the legs and feet (see Good signs guide 6.1). Look for atrophic skin and loss of hair, colour changes of the feet (blue or red) and ulcers at the lower end of the tibia.2 Venous and diabetic ulcers can be distinguished from arterial ulcers (see Figures 6.7–6.9).

Figure 6.7 Venous ulcer This venous ulcer has an irregular margin, pale surrounding neo-epithelium (new skin) and a pink base of granulation tissue. There is often a history of deep venous thrombosis. The skin is warm and oedema is often present. (See List 6.4.) (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)

Figure 6.8 Arterial ulcer This arterial ulcer has a regular margin and ‘punched out’ appearance. The surrounding skin is cold. The peripheral pulses are absent. (See List 6.4.) (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)

Figure 6.9 Diabetic (neuropathic) ulcer. Neuropathic ulcers are painless and are associated with reduced sensation in the surrounding skin. (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)
Look for reduced capillary return (compress the toenails—the return of the normal red colour is slow).3 In such cases, perform Buerger’sb test to help confirm your diagnosis: elevate the legs to 45° (pallor is rapid if there is a poor arterial supply), then place them dependent at 90° over the edge of the bed (cyanosis occurs if the arterial supply is impaired). Normally there is no change in colour in either position.
The ankle–brachial index (ABI) is a measure of arterial supply to the lower limbs; an abnormal index indicates increased cardiovascular risk. The systolic blood pressure in the dorsalis pedis or posterior tibial artery is measured using a Doppler probe and a blood pressure cuff over the calf. This is divided by the systolic blood pressure measured in the normal way at the brachial artery. An ABI of less than 0.9 indicates significant arterial disease and an ABI of between 0.4 and 0.9 is associated with claudication. An ABI of less than 0.4 is associated with critical limb ischaemia. An ABI greater than 1.3 occurs with a calcified (non-compressible) artery. A reduced ABI is also considered a risk factor for arterial disease elsewhere.
Acute arterial occlusion
Acute arterial occlusion of a major peripheral limb artery results in a painful, pulseless, pale, ‘paralysed’ limb that is perishingly cold and has paraesthesias (the six Ps). It can be the result of embolism, thrombosis or injury. Peripheral arterial embolism usually arises from thrombus in the heart, where it is often secondary to (1) myocardial infarction, (2) dilated cardiomyopathy, (3) atrial fibrillation or (4) infective endocarditis.4
Deep venous thrombosis
Deep venous thrombosis (DVT) is a difficult clinical diagnosis.5 The patient may complain of calf pain. On examination, the clinician should look for swelling of the calf and the thigh, and dilated superficial veins. Feel then for increased warmth and squeeze the calf (gently) to determine if the area is tender. Homans’c sign (pain in the calf when the foot is sharply dorsiflexed) is of limited diagnostic value and is theoretically dangerous because of the possibility of dislodgement of loose thrombus.
The causes of thrombosis were described by Virchowd in 1856 under three broad headings (the famous Virchow’s triad): (1) changes in the vessel wall, (2) changes in blood flow and (3) changes in the constitution of the blood. Deep venous thrombosis is usually caused by prolonged immobilisation, cardiac failure (stasis) or trauma (vessel wall damage), but may also result from occult neoplasm, disseminated intravascular coagulation, the contraceptive pill, pregnancy and a number of inherited defects of coagulation (the thrombophilias: e.g. Factor V Leiden, anti-thrombin III deficiency).
Varicose veins
If a patient complains of ‘varicose veins’, ask him or her to stand with the legs fully exposed.6 Inspect the front of the whole leg for tortuous, dilated branches of the long saphenous vein (below the femoral vein in the groin to the medial side of the lower leg). Then inspect the back of the calf for varicosities of the short saphenous vein (from the popliteal fossa to the back of the calf and lateral malleolus). Look to see whether the leg is inflamed, swollen or pigmented (subcutaneous haemosiderin deposition secondary to venous stasis).
Palpate the veins. Hard leg veins suggest thrombosis, while tenderness indicates thrombophlebitis. Perform the cough impulse test. Put the fingers over the long saphenous vein opening in the groin, medial to the femoral vein. (Do not forget the anatomy—femoral vein [medial], artery [your landmark], nerve [lateral].) Ask the patient to cough: a fluid thrill is felt if the saphenofemoral valve is incompetent.
The following supplementary tests are occasionally helpful (and surgeons like to quiz students on them in examinations):
• Trendelenburge test: with the patient lying down, the leg is elevated. Firm pressure is placed on the saphenous opening in the groin, and the patient is instructed to stand. The sign is positive if the veins stay empty until the groin pressure is released (incompetence at the saphenofemoral valve). If the veins fill despite groin pressure, the incompetent valves are in the thigh or calf, and Perthes’f test is performed.
• Perthes’ test: repeat the Trendelenburg test, but when the patient stands, allow some blood to be released and then get him or her to stand up and down on the toes a few times. The veins will become less tense if the perforating calf veins are patent and have competent valves (the muscle pump is functioning).
If the pattern of affected veins is unusual (e.g. pubic varices), try to exclude secondary varicose veins. These may be due to an intrapelvic neoplasm that has obstructed deep venous return. Rectal and pelvic examinations should then be performed.
Finally, chronic venous stasis is one cause of ulceration of the lower leg. This is often associated with pigmentation and eczema, which are due to venous stasis.
The differential diagnosis of leg ulcers is summarised in List 6.4 overleaf.
References
1. Magee, TR, Stanley, P, Mufti, R, et al. Should we palpate foot pulses. Ann Roy Coll Surg Eng. 1992; 74:166–168. [Elderly patients who do not have a palpable dorsalis pedis pulse will often have adequate perfusion (unless there is clinical evidence of claudication or foot ulcers). Palpation of the dorsalis pedis is more helpful than the posterior tibial.].
2. Khan, NA, Rahim, SA, Avand, SS, et al. Does the clinical examination predict lower extremity peripheral arterial disease. JAMA. 2006; 295(5):536–546.
3. McGee, SR, Boyko, EJ. Physical examination and chronic lower-extremity ischemia: a critical review. Arch Intern Med. 1998; 158:1357–1364. [The presence of peripheral arterial disease is positively predicted by abnormal pedal pulses, a unilaterally cool extremity, prolonged venous filling time and a femoral bruit.].
4. O’Keefe, ST, Woods, BO, Breslin, DJ, Tsapatsaris, NP. Blue toe syndrome. Causes and management. Arch Intern Med. 1992; 152:2197–2202. [Explains how to identify the cause by clinical methods and directed investigations.].
5. Anand, SS, Wells, PS, Hunt, D, et al. Does this patient have deep venous thrombosis. JAMA. 1998; 279:1094–1099. [The sensitivity of individual symptoms and signs is 60%–96% and the specificity 20%–72%. Patients can be subdivided into those with a low, intermediate or high pretest probability, based on risk factors and clinical features.].
6. Butie, A. Clinical examination of varicose veins. Dermat Surg. 1995; 21:52–56. [Techniques are outlined and compared with Doppler ultrasound assessment.].
aAchilles, mythical Greek hero, whose body was invulnerable except for his heels, by which he was held when dipped in the River Styx as a baby to make him immortal. He was killed by Paris, who shot an arrow into his heel.
bLeo Buerger (1879–1943), New York physician, born in Vienna, who described thromboangiitis obliterans. He was obsessed with expensive cars.
cJohn Homans (1877–1954), professor of surgery, Harvard University, Boston. He described his sign in 1941, originally in cases of thrombophlebitis. He later became disenchanted with the sign and is reputed to have asked why if a sign were to be named after him it couldn’t be a useful one.
dRudolph Virchow (1821–1902), brilliant German pathologist, regarded as the founder of modern pathology, professor of pathological anatomy in Berlin. He provided the first description of leukaemia. He died at 81 after fracturing his femur jumping from a moving tram.
eFriedrich Trendelenburg (1844–1924), professor of surgery, Leipzig.
fGeorg Clemens Perthes (1869–1927), German surgeon, professor of surgery at Tübingen. He was the first to use radiotherapy for the treatment of cancer (in 1903).