A summary of the rheumatological examination and extending the rheumatological examination
Extending the rheumatological system examination
RHEUMATOLOGY INVESTIGATIONS
Diagnosis in rheumatology relies on careful history taking and physical examination, and in many cases pattern recognition applied against accepted diagnostic criteria. Testing is undertaken to confirm the clinical diagnosis.
Laboratory testing
Know your autoimmune antibodies! Testing includes the following:
• Antinuclear antibody (ANA) is positive in high titre in a number of autoimmune diseases including systemic lupus erythematosus (SLE) (95%), drug-induced lupus, mixed connective tissue disease, scleroderma and Sjögren’s syndrome (and ANA is positive in at least 5% of healthy elderly patients). ANA is sensitive but not specific.
• If ANA is positive, testing for specific ANAs is helpful—for example, anti-double stranded DNA (specific for SLE), anti-U1-RNP (very sensitive for mixed connective tissue disease) and anti-centromere antibody (CREST).
• Anti-neutrophil cytoplasmic antibodies (ANCA) can be perinuclear in pattern (p-ANCA; e.g. Churg-Strauss syndrome) or homogeneous in the neutrophil cytoplasm (c-ANCA; e.g. Wegner’s granulomatosis).
• Complement components (C4 and C3) are reduced in SLE.
• HLA-B27 is present in 90% of patients with ankylosing spondylitis and in up to 80% with Reiter’s syndrome but is not used for diagnosis (up to 8% of the normal population are also HLA-B27 positive).
IMAGING
X-rays, CT scans and MRI scans are now a standard part of the rheumatological investigation. Students need to be familiar with some of the more common changes in these tests and how they may be useful.
Plain X-rays may show the following in soft tissues and bones in different types of arthritis:
• soft-tissue swelling (e.g. pannus)
• deformity or enlargement of bone
• narrowing of the joint spaces due to loss of cartilage—focal in inflammatory arthritis and generalised in osteoarthritis (see Figures 26.1 and 26.2)
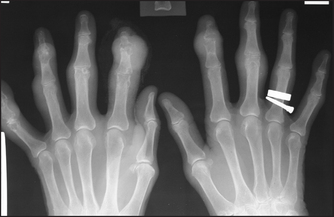
Figure 26.1 Osteoarthritis X-ray of the hands showing the typical findings of osteoarthritis with joint-space narrowing and proliferative changes in the distal joints. Also note erosive and destructive changes at multiple proximal interphalangeal joints.

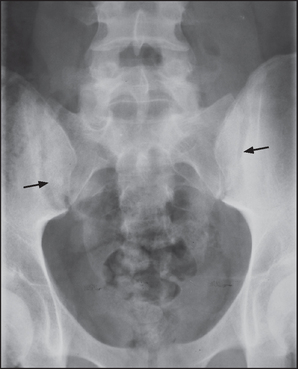
Figure 26.2 Osteoarthritis Anteroposterior X-ray of the hip showing the features of osteoarthritis. The left side is more severely affected than the right; note sclerosis, osteophyte formation and asymmetrical joint space narrowing.
• joint erosion with areas of proliferation of bone (e.g. psoriatic; see Figure 26.9 below) or without (e.g. rheumatoid arthritis; see Figure 26.3)
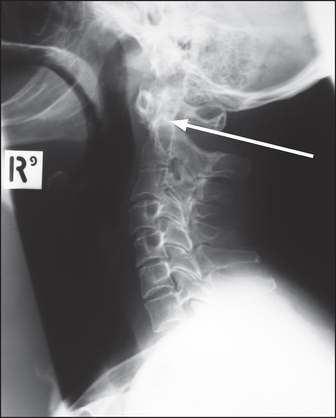
Figure 26.3 Rheumatoid arthritis Lateral X-ray of the cervical spine showing anterior subluxation of the anterior arch of the dens of the axis (C2, arrow).
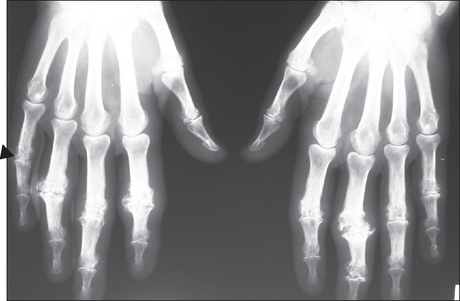
Figure 26.9 Psoriatic arthritis X-ray of the wrist of a patient with psoriatic arthritis; note the ‘pencil in cup’ deformity (tapered proximal osseous surface and expanded base) of the distal bone of the fingers, early ankylosis [arrowhead] of the proximal interphalangeal joint of the right little finger and erosions with proliferative change of the little finger). Note also the lack of osteoporosis.
• bone deformity (see Figure 26.5)
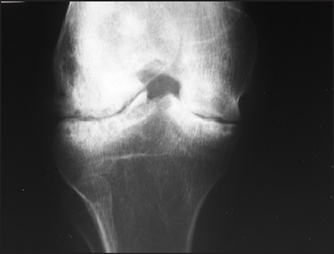
Figure 26.5 Haemophilia X-ray of the knee showing loss of joint space and some deformity of the adjacent bone. Although the tibia and femur are sclerotic adjacent to the destructive change, the bones are generally osteopenic with mild overgrowth of the epiphysis. Ask about the consequences of arthritis.
• new bone formation (e.g. syndesmophytes [see Figure 26.4], periosteal reaction, osteophytes)
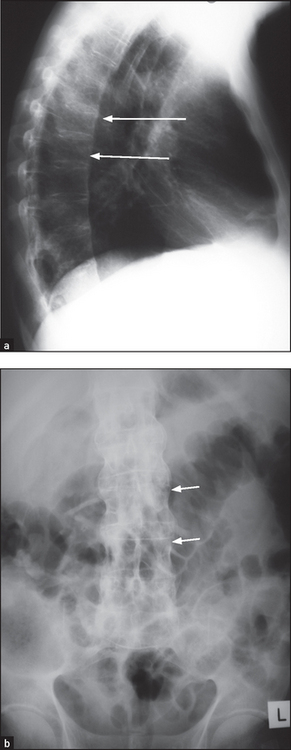
Figure 26.4 Ankylosing spondylitis Anteroposterior (a) and lateral (b) X-rays of the thoracic spine showing ankylosis of the sacroiliac joints, extensive syndesmophyte formation (short arrows) and squaring of the vertebral bodies (long arrows).
• abnormal calcification of ligaments, cartilage, tendon or within joint spaces
• changes in bone density: osteosclerosis, increased density (e.g. at joint margins in osteoporosis), osteoporosis, decreased density (e.g. septic arthritis).
It is not usually necessary to X-ray all symptomatic joints; information about joint destruction and typical changes that help make the diagnosis can be obtained from selected X-rays. For example, a clinical presentation with a polyarthritis may warrant hand and foot X-rays which, if they show erosion and a typical pattern (e.g. metatarsophalangeal and metacarpophalangeal involvement), can help make the diagnosis of rheumatoid arthritis (see Figures 26.6 and 26.7).
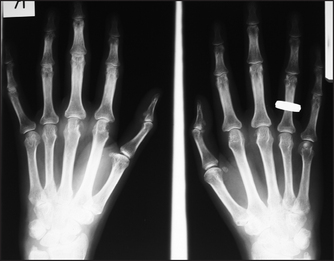
Figure 26.6 Rheumatoid arthritis, early findings X-ray of the hands of a patient with early rheumatoid arthritis. Note erosions of the heads of the metacarpophalangeal joints and of the ulnar styloid, and reduced amounts of cartilage in the joint spaces.

Figure 26.7 Rheumatoid arthritis, late findings X-ray of the hands of a patient with advanced rheumatoid arthritis. Note loss of joint space and destruction of the right carpal joints, subluxation of metacarpophalangeal and proximal interphalangeal (PIP) joints, and Z deformity of the thumb. There are erosions of the PIP joints, a sign of active disease.
X-rays of the sacroiliac joints may reveal joint involvement in patients with some symptoms of ankylosing spondylitis before these joints are clinically abnormal.
CT scans and MRI scans are increasingly used for the investigation of these patients. It must be kept in mind that CT scans expose patients to many times the radiation dose of plain X-rays, so they should be used only when they are likely to give information beyond what plain X-rays and ultrasound can show. MRI is often preferred when it is available.
CT scans and MRI scans give three-dimensional information about complicated joints and are especially useful for spinal problems. Examples of indications include:
• soft-tissue problems such as bursitis, tenosynovitis and rotator cuff tears
• suspected joint or soft-tissue infection
• intervertebral disc problems such as spinal cord compression or nerve root entrapment
• joint or associated soft-tissue or bony malignancy
• joint injury or damage such as knee problems in athletes or after trauma.
Ultrasound can be used to look for joint effusions, cysts and tendon thickening. However, it does not provide the spatial resolution of CT or MRI.
Nuclear scans using Tc-bisphosphonate can be useful for a number of specific problems, including:
X-rays in specific rheumatological conditions
Ankylosing spondylitis
X-rays of the spine and sacroiliac joints (see Figure 26.4) may show ankylosis (fusion) of the sacroiliac joints and ‘squaring’ of the vertebral bodies as a result of loss of their anterior corners and periostitis of their waists. ‘Bridging syndesmophytes’a occur as a result of ossification of the fibres of the joint annulus. Severe disease causes the changes called bamboo spine visible on X-ray.
Reiter’s syndrome
The first attack of arthritis is associated with soft-tissue changes and subsequent attacks may lead to joint-space narrowing and proliferative erosions at the joint margins that show on X-ray. Changes in the sacroiliac joints and spine resemble those of ankylosing spondylitis except that the sacroiliac joint changes and spinal syndesmophytes tend to be asymmetrical. Calcaneal spurs—a result of plantar fasciitis—are characteristic.
Psoriatic arthritis
In mild cases X-rays are normal or show only joint-space narrowing and erosive changes. Unlike the X-rays of rheumatoid joints the bone density is maintained and there may be sclerotic changes in the small bones (see Figure 26.9). Ankylosis of peripheral joints and arthritis mutilans can occur in either condition. The involvement of the spine and sacroiliac joints is asymmetrical, as in Reiter’s syndrome.
Gout
X-rays (see Figure 26.10) show multiple juxta-articular erosions, which may obliterate the joint space.
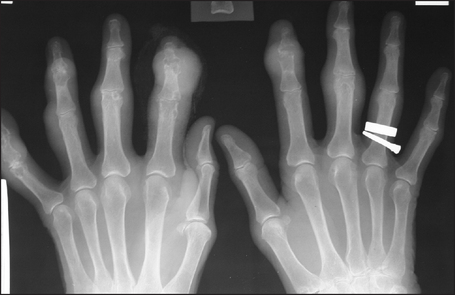
Figure 26.10 Gout X-ray of the hands of a patient with severe gouty arthritis. Note multiple juxta-articular erosions with relative preservation of the joint space, and erosions with overhanging edges. There are large soft-tissue swellings over the distal interphalangeal joints of the index fingers.
Pseudogout
X-rays show joint-space narrowing, cyst formation under the cartilage and calcification of the joint cartilage (chondrocalcinosis). Chondrocalcinosis on X-ray is typical of pseudogout but is not always present.
Scans
Figures 26.11 and 26.12 show CT scans of changes in the knee.
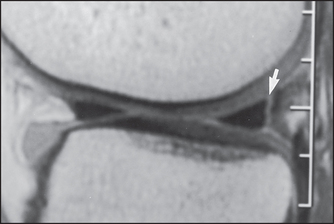
Figure 26.11 CT scan showing a meniscal tear in the knee joint (arrow) (Resnick DR et al. Internal derangement of joints, 2nd edn. Saunders, 2006.)
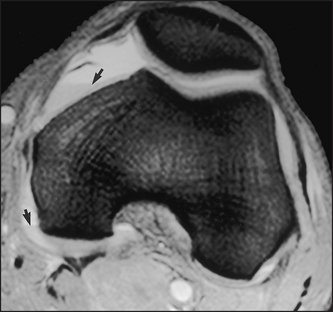
Figure 26.12 CT scan showing a haemarthrosis of the knee (Resnick DR et al. Internal derangement of joints, 2nd edn. Saunders, 2006.)
References
1. Beattie, KA, Bobba, R, Bayoumi, I, et al. Validation of the GALS musculoskeletal screening exam for use in primary care: a pilot study. BMC Musculoskelet Disord. 2008; 9:115. [GALS is a useful tool in primary care.].
2. Doherty, M, Dacre, J, Dieppe, P, Snaith, M. The ‘GALS’ locomotor screen. Ann Rheum Dis. 1992; 51:1165–1169. [Describes the GALS screen.].
aA syndesmosis is a joint where the bones are joined by fibrous ligaments or sheets.