Chapter 3 Short-answer questions
Learning is finding out what you already know.
Richard Bach
The short-answer question (SAQ) section is regarded as one of the more challenging components of the exam. While it examines general knowledge of emergency medicine topics and scenarios, the format in which it is presented tests candidates’ ability to link multiple concepts as well as provide detailed knowledge for individual areas. Since it is difficult to judge the balance between the breadth and depth of information required to score good marks, the SAQ section can be quite draining. Well-structured answers showing a logical, systematic approach will be more successful than simply writing to exhaustion in an overelaborate manner.
Purpose
The aim of this section is to test both theoretical and practical knowledge covering a broad range of topics related to the practice of emergency medicine.
Format
There are eight questions to be answered over a period of two hours, giving approximately 15 minutes to answer each question. In addition, 10 minutes of reading time is allocated at the beginning of the exam during which no writing is permitted. It is normal at the end of the SAQs not to be able to control your cramped writing arm!
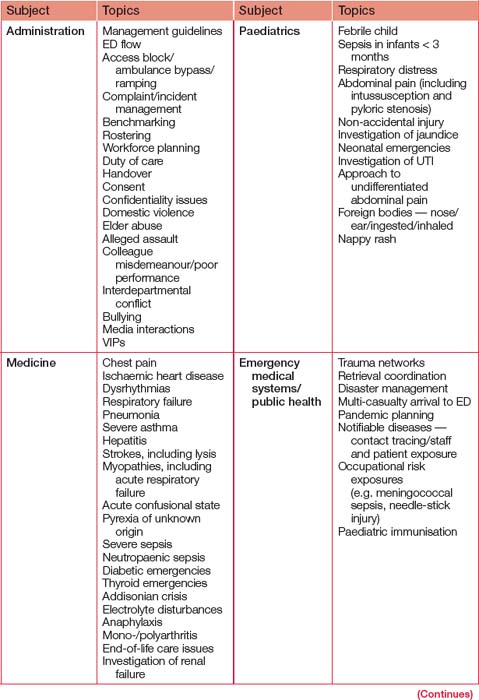
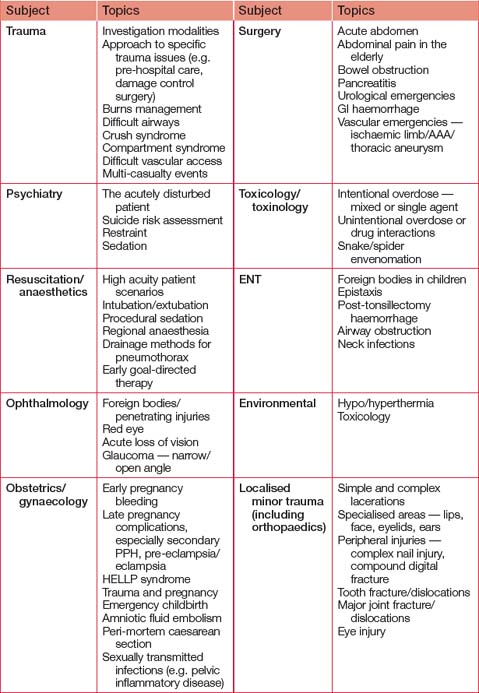
Six questions cover the ‘core’ topics: administration, medicine, trauma, paediatrics, resuscitation/anaes thetics and surgery. Others may be sourced from the following topics: emergency medical systems/public health, ENT/eyes, environmental, obstetrics/gynaecology, psychiatry, toxicology and minor trauma (including orthopaedics). As with all sections of the exam, individual questions may cover more than one topic.
Questions can be posed in a number of different ways. The majority will involve a clinical scenario: remember that every word in the scenario has been specifically chosen for a reason and is important in answering the question. The remainder of questions ask you to write about a certain subject or how you would approach a particular situation.
Questions may comprise up to three parts, and each part will be given a specified percentage value of the total mark for that question. You need to reflect this percentage breakdown in your answer.
The College has produced a glossary of terms used in the fellowship exam, which is available for use in the exam room (see the glossary at the back of this book). Utilise this list when answering the questions: answering about treatment when investigations have been requested will not score marks.
Preparation
Questions can be taken from almost anywhere in the curriculum. Thus, general preparation in learning the curriculum goes without saying. In addition, most of the questions will address issues that present in your day-to-day practice. Working in an ED setting will greatly enhance your ability to answer these questions.
Although the range of topics that may be covered is almost endless, there are a number of recurring themes, many of which overlap. Practice questions can be sourced from your DEMT and other consultants, or you and your colleagues can write them for each other. Table 3.1 outlines the major topics that should be practised or at least considered. There is a significant overlap with lists of likely VAQ and SCE topics. This reflects the fact that certain core topics are consistently tested in one format or another during the examination process.
As with much of your exam preparation, practice in answering SAQs is vital. Every time you answer an SAQ, complete it in the required time frame (15 minutes) and ask someone (preferably a FACEM) to mark it. Over time, you can progress to ‘half ’ (four-question) and full-practice exams. Do them under exam conditions where possible, including a proportional amount of reading time.
During your preparation, it can be useful to develop some standard templates for answering certain types of question. Tables, flow charts and diagrams are acceptable as part or all of an answer and are particularly relevant for certain types of question. Table 3.2 provides some examples of answer templates for certain types of questions. The table is arranged as per the College’s glossary of terms for the fellowship examination. Some of these templates will be relevant for answering other question types, such as VAQs and SCEs, in a more structured manner.
TABLE 3.2 Sample SAQ answer templates
| Question type |
Possible templates |
| Assessment |
Stable patient: presenting complaints and details, past history (medical, surgical, obstetric, birth and development, psychiatric), social history, allergies, medications (prescribed, over the counter, alternative therapies), immunisations, systems enquiry including focus on conditions to consider/exclude.
Emergent setting: AMPLE history (allergies, medications, past history, last oral intake, events).
Stable patient: general appearance, vital signs, each organ system (cardiovascular, respiratory, hepatic, gastrointestinal, renal, neurological (central and peripheral), musculoskeletal, haematological, endocrine, dermatological).
Emergent setting: primary survey (ABCDE), then focused secondary survey (head-to-toe examination). Full examination if/when able.
Bedside: e.g. dipstick urine, BSL, ECG, blood gas, focused ultrasound.
Laboratory: haematology, biochemistry, microbiology, other.
Radiology: plain imaging, ultrasound, CT, MRI, angiography.
Investigations can be listed either in the order above if the differential diagnosis is broad or as specific investigations to confirm/exclude individual diagnosis where the list is smaller (e.g. in stroke, CT scan of brain to exclude haemorrhage, followed by chest X-ray to exclude aspiration and then U&E for biochemical derangements associated with dehydration if unable to drink). |
| Discuss |
Tables are often useful (e.g. simple grid with pros and consoradvantages and disadvantages for each alternative under discussion).
Specifically consider controversies/unanswered questions — quote key papers if possible. |
| Disposition |
In-patient: ED observation ward, hospital ward, HDU, ICU, inter-hospital transfer.
Outpatient: home, GP referral, specialist referral, community or at-home assessment and interventions.
|
| Interpret |
Provide the most likely diagnosis then a differential diagnosis. For differential diagnosis templates, see ’list’ section below. |
| Investigations |
See ’assessment’ section above. |
| List |
Use a logical, relevant order. If referring to a differential diagnosis, the most important or most likely diagnosis should be presented first and given maximal emphasis. Some subjects may have pre-prepared lists. In the absence of an existing list, construct one by considering a generic list of possible causes. For example: Pathophysiological classification
1. Congenital or acquired. 2. For acquired, use a mnemonic such as VINTMEDATI:
Inflammatory/infectious (bacterial/viral/fungal/protozoal/other)
Neoplastic (benign/malignant — primary/secondary)
Traumatic (including non-accidental, especially paediatric and elderly)
Idiopathic (always leave to last) including drug-related.
Other classifications
• Organic versus psychiatric (e.g. causes of abnormal behaviour). • Pragmatic classification — most common, most potentially lethal, most forgotten causes (e.g. causes of chest pain). • Anatomic classifications (e.g. causes of desaturation in a ventilated patient — consider possibilities from the gas source to the circuit and tube to the patient’s airway, lungs and chest wall; jaundice — obstructive versus non-obstructive; bowel obstruction — small versus large bowel; luminal, intraluminal or extraluminal pathologic lesions; renal failure — pre-renal, renal and post-renal causes). • Infective versus non-infective causes (e.g. causes of lymphadenopathy); infective causes can be bacterial (Gram +ve, -ve, anaerobes, mycobacteria, atypicals), viral, protozoal, fungal. • Malignant versus non-malignant causes (e.g. causes of coin lesions on a chest X-ray).
|
| Management |
The College definition is specific treatment, supportive care and disposition. Investigation, however, may be an essential part of patient management (e.g. in febrile or trauma patients), but if the diagnosis is already clear, investigation would not attract marks in a management question. For an emergent setting one approach is to simultaneously:
• resuscitate — identify and treat immediate threats to life (ABCDE/ATLS approach) • investigate — determine a probable diagnosis and differential diagnosis through assessment (see ’assessment’ section above) • definitively treat — divide into supportive versus specific treatment (medical/surgical/other interventions) • plan disposition — appropriately for condition and response to treatment |
| Outline |
This is similar to ‘describe’ (which is self-explanatory) but can be structured for specific conditions, procedures and practice guidelines. If referring to a specific condition, divide into:
• background — provide a brief overview; set the context • size of problem — incidence/prevalence (common/rare), morbidity/mortality, risk factors/causes, medicolegal relevance • presenting features — history, examination, investigation findings • differential diagnosis (see ’list’ section above) • treatment — supportive versus specific (usually medical/surgical/other interventions) • outcomes and follow-up. If referring to a procedure or practice guideline:
• preparation (staff, equipment, setting, patient e.g. fasting) • process of procedure in detail • possible complications (and treatment) • discharge criteria (or disposition if not discharged) • notes/variations for subgroups e.g. paediatrics • references/evidence base. |
| Protocol |
Protocols are useful to ensure consistency of practice against agreed best practice. General headings to consider:
• rationale (for needing a protocol) • background knowledge (the evidence base for the protocol, including performance and predictive characteristics of the protocol) • target (which patients and what criteria to identify/exclude them) • recommendations (a flow chart ’algorithm’ can be helpful) • special considerations (e.g. costs, special equipment/training) • governance issues (process and time line for audit, responsible staff signing off on the protocol, date of introduction and review) • notes/variations for subgroups e.g. paediatrics • references/evidence base • authorising person/body and date • review date and history. |
| Treatment |
See ’management’ section above. |
| Other |
For administration questions consider all stakeholders that may be relevant to a complex issue: patients, relatives/carers, nursing staff, medical staff (junior and senior), ED, GPs and other specialists, allied health workers, pre-hospital care workers, hospital administrators, health department, medical board, training authorities (e.g. ACEM), medical defence organisations, media/general public, the law/police When discussing transport options consider road, fixed wing, rotary. When discussing analgesia options consider routes of administration (oral, intravenous, subcutaneous, intramuscular, inhalational, nasal, sublingual, rectal), classes of agents to be used and other therapeutic options. When discussing anaesthetic techniques consider general anaesthesia and blocks (local infiltration, peripheral nerve blocks, regional blocks). Any answer about paediatrics must have considered consent issues, immunisation status, development, non-accidental injury, communication with child or family. |
The answer book for the SAQs is similar to that used for the primary examination. A sample is avail able on the College website (www.acem.org.au). Practise writing your answers in these answer books and using the templates given in Table 3.2. It is worth trying to write your answers on every second line, since this not only facilitates legibility but also gives you space to insert new material should you recall more information later.
We recommend writing a brief outline or ‘plan’ at the start of each answer. It is helpful if you can consider what this will be during the reading time. A good outline provides a structured, logical, sequential response and helps trigger recall of relevant material. If you run out of time to provide a full answer and provide only an annotated plan, at least the examiner will see your intentions and may reward you with marks you would not otherwise have obtained. Avoid writing excessively long plans, as this detracts from their purpose.
Th e aim of the SAQ is to impart as much knowledge as possible in a brief, logically structured and concise format. Point-form answers using standard abbreviations are preferred. ‘Essay-style’ answers can be a less efficient method of communicating information and are discouraged.
Using a template immediately gives your answers subheadings. This makes it easier for the examiners to read and mark your work, particularly if you lay out the sections in a controlled, legible fashion. A well-structured introduction and a concluding statement can link together the material for maximal impact.
For ‘treatment’ and ‘management’ questions in particular, it is oft en useful to consider the 3Cs (condition, cause and complications) and not just the condition when formulating answers. Try to tailor the template to the question by providing examples of the key relevant history, and what you would be looking for or expecting to find on examination or from specific investigations. A few examples for each subpoint are expected (e.g. in suspected renal colic, ward test urine for haematuria to support diagnosis and examine abdomen to exclude AAA if elderly).
On the day
Use your 10 minutes of reading time wisely. Read through the whole paper and decide which questions you are more likely to be able to answer well. Use this time to plan the format in which you will answer the questions and the order in which you will tackle them. Some people prefer to answer the questions in order, whereas others prefer to start with the question(s) they feel more confident with. The latter option has the advantage of your writing being at its best when you have the most information to impart.
Maintain your focus on what each question is asking using the definitions supplied by the College. Do not transcribe the question onto the answer book let before answering it as this wastes valuable time and is not necessary.
Be aware that by the end of the two hours, you will be both physically and mentally fatigued and can easily lose track of time. Have a reliable method of timekeeping and keep to your self-allocated time frame for each question. It may be worthwhile writing down the number of minutes you have to spend on the sections within each question (or the start/finish times) proportionate to the percentage value designated.
Ensure you answer all questions. The marking system rewards consistency above high scores on individual questions. Failing to provide an answer to a question will substantially reduce your overall mark. If you have time remaining at the end of the exam, you can go back and ‘fill in the gaps’ for those questions where you have additional relevant information.
Worked sample SAQs
The following worked examples show the types of questions that may be encountered in the exam.
SAQ 1: resuscitation/toxicology
A 20-year-old male presents to ED one hour after being bitten by a snake. He collapsed 20 minutes after being bitten and since then has been vomiting bloodstained fluid.
(a) Outline your initial assessment of this patient. (50%)
(b) Outline your immediate treatment. (50%)
Sample answer
Plan
•
Initial assessment — history, examination, investigations
•
Immediate treatment — supportive, specific, disposition
Overview
This young man has life-threatening envenomation, most likely from a brown snake (Pseudonaja spp.) bite. He requires simultaneous resuscitation, investigations and definitive therapies.
(a) Initial assessment
History
•
How the bite occurred
•
known snake? (e.g. snake handler)
•
Symptoms in addition to above
•
bleeding from bite site or other sites?
•
Past medical history
•
pre-existing bleeding disorder?
•
past history of bite and/or administration of antivenom?
Examination
•
General appearance
•
presence and adequacy of first aid
•
evidence of bleeding from bite site
•
evidence of covert bleeding (e.g. haematemesis/melaena)
•
Airway compromise, especially if progressive bulbar palsy or airway bleeding
•
Breathing
•
rate/work of breathing/effectiveness
•
Disability
•
eye movements — looking for ptosis and extraocular palsies
•
other localised or generalised weakness
Investigations
•
Bedside
•
bite site swab and urine for venom detection kit (VDK) to guide selection of antivenom
•
urinalysis (for blood/myoglobin)
•
blood for whole blood clotting screen (in plain tube)
•
Laboratory — serial tests
•
pCO
2 (venous gas or expired air) for progressive respiratory failure
•
full blood profile (low platelets with DIC, acute anaemia from bleeding)
•
U&Es (signs of renal failure, rhabdomyolysis)
•
CK and LDH (for rhabdomyolysis)
•
coagulation profile (DIC with prolonged PT, aPTT and low fibrinogen)
•
d-dimer/FDP (expect gross elevations)
•
Radiology
•
none essential immediately
•
consider mobile chest X-ray if at risk of aspiration
•
consider CT scan of head if suspicious of spontaneous intracranial
(b) Immediate treatment
•
Patient is showing signs of envenomation, most likely from the brown snake group (
Pseudonaja spp.), which would explain his collapse and bleeding.
Supportive
•
Move to a resuscitation bay and institute supportive care of ABCs.
Specific
•
If compression and immobilisation first aid is not in place or is ineffective, this should be (re)applied.
•
Treatment to proceed in conjunction with early consultation of toxicology service.
•
Use of antivenom will be determined by clinical status:
•
If clinical examination is consistent with severe envenomation, immediate treatment with polyvalent antivenom may be required.
•
If clinical examination and/or whole blood clotting time are consistent with envenomation, but time is available to perform VDK, wait and use targeted monovalent antivenom.
•
If no clinical evidence of envenomation (unlikely), await formal bloods or development of clinical signs to indicate the need for monovalent antivenom.
•
Administration of antivenom:
–
antivenom (diluted in 1 L normal saline) given by infusion over 30 minutes.
•
Adrenaline available in case of anaphylactic reaction.
•
Give corticosteroid cover if polyvalent or multiple doses of monovalent antivenom are given to reduce the risk of serum sickness.
•
Consider use of replacement products of coagulation — FFP, platelets, cryoprecipitate etc. (recent evidence suggests that doing this in addition to supplying one dose of antivenom is adequate for most cases) — in consultation with local toxicology service.
Disposition
•
Admit to HDU/ICU for ongoing care.
SAQ 2: resuscitation/surgery
A 45-year-old alcoholic man presents to ED with a two-day history of severe upper abdominal pain. Observations taken at triage are:
| T |
38°C |
| HR |
120/min |
| BP |
100/80 mmHg |
| RR |
28/min |
| SaO2 |
91% on air |
(a) List your differential diagnosis. (50%)
(b) Outline your immediate management. (50%)
Sample answer
Plan
•
Differential diagnosis — classify anatomically into abdominal versus extra-abdominal causes and rank in order of likelihood
•
Immediate management — simultaneous resuscitation (ABCs), investigations, definitive therapies (supportive/specific), disposition
Overview
This is a critically ill alcoholic patient with undifferentiated shock. A broad differential diagnosis must be considered and simultaneous resuscitation, investigations and definitive therapies instituted.
(a) Differential diagnosis
Abdominal causes
•
Perforated viscus (e.g. duodenal or gastric ulcer)
•
Hepatitis (e.g. alcoholic, infective)
•
Pyelonephritis +/– infected obstructed kidney
•
Primary peritonitis (e.g. setting of ascites complicating chronic liver disease)
•
Acute appendicitis (e.g. retrocaecal location)
•
Ruptured spleen (splenomegaly associated with spontaneous or traumatic rupture)
Extra-abdominal causes
•
Oesophageal perforation (i.e. Boerhaave’s syndrome)
•
Pneumonia (consider aspiration, as well as typical community acquired pathogens; consider associated lung abscess and empyema)
•
Myocardial ischaemia +/– pulmonary oedema
•
Pulmonary thromboembolism
•
Congestive cardiac failure with hepatic engorgement
•
Traumatic pneumothorax (e.g. if a recent fall)
•
Cardiomyopathy (e.g. alcoholic, thiamine deficiency-related, ischaemic, hypertensive)
(b) Immediate management
Resuscitate
•
Triage
•
ATS 2 to a resuscitation area and commence non-invasive monitoring (NIBP, SaO
2, ECG)
•
Airway
•
ensure intact; if not may require definitive airway management
•
Breathing
•
exclude immediate life threats (e.g. hypoglycaemia, tension pneumothorax, pericardial tamponade)
•
apply oxygen at 15 L/min via non-rebreather mask
•
consider intubation (e.g. severe type 1 or 2 respiratory failure)
•
Circulation
•
large bore IV access × 2 (14/16 G)
•
characterise likely cause(s) of shock clinically (e.g. perfusion of peripheries, JVP)
•
administer IV fluids (e.g. initial bolus of 500 ml normal saline then reassess using endpoint of tissue perfusion — brain, urine, peripheries, as well as HR, BP and JVP)
•
look for evidence of overt/concealed blood loss (e.g. haematemesis/melaena) and treat as appropriate
Investigate
•
Perform a history and examination to help produce a likely provisional and differential diagnosis; examine medical record for additional information
•
Perform high yield tests
•
Bedside
–
urine dipstick (urinary ketones in alcoholic ketoacidosis; white cells, nitrites, blood in infection)
–
ECG for acute coronary syndrome or pericarditis
–
ABG to ascertain degree of respiratory and metabolic failure
•
Laboratory
–
full blood profile (high/low white cells in sepsis, low platelets from hypersplenism or sepsis, anaemia from blood loss; pancytopaenia from alcohol-related marrow suppression)
–
coagulation profile (liver dysfunction)
–
LFTs (hepatic or obstructive picture)
–
amylase/lipase (pancreatitis)
–
blood, urine, sputum culture
–
serum lactate (correlates with severity of shock, allows progress evaluation)
•
Radiology
–
mobile erect chest X-ray (pneumonia, abscess, subphrenic collection, pleural effusions/empyema, cardiogenic/non-cardiogenic pulmonary oedema, mediastinal air, free gas under diaphragm)
–
CT abdomen +/– chest likely to be helpful (once stabilised)
Definitive therapies
•
Supportive
•
analgesia (titrated doses of IV morphine)
•
correct severe coagulation disturbances
•
empiric thiamine (prevention of Wernicke’s encephalopathy)
•
management of alcohol withdrawal (e.g. diazepam) — commence now to prevent withdrawal on day 2 to 3
•
consider invasive monitoring (CVL/arterial line)
•
sepsis bundle for early goal-directed therapy if severe sepsis (as per Surviving Sepsis Campaign 2008)
•
communicate with patient/family
•
Specific — will depend on diagnosis, e.g.
•
pneumonia — antibiotics
•
pancreatitis — supportive initially
•
cholecystitis — antibiotics initially; possible surgery
•
perforated viscus/abdominal collection/appendicitis — operative, then supportive
•
Boerhaave’s syndrome — antibiotics then stenting or surgery
•
myocardial ischaemia — treat as per local acute coronary syndrome guideline
•
upper GI variceal bleeding— octreotide infusion and endoscopic therapy
•
upper GI non-variceal bleeding — high dose PPI then endoscopic therapy
Disposition
•
Will require admission under appropriate specialist team
•
Will likely require admission to HDU depending on progress
•
Social work/alcohol and drugs dependency support if agreeable when improves
SAQ 3: medicine/resuscitation
A 34-year-old man presents to ED 10 days following his second course of chemotherapy for metastatic seminoma. He has been vomiting at home for the past eight hours. At triage his observations are:
| T |
39.5°C |
| HR |
110/min |
| BP |
65/35 mmHg |
Outline your assessment of this man. (100%)
Sample answer
Plan
•
Assessment
•
history — AMPLE, then more comprehensive when possible
•
examination — ABCs, then head-to-toe examination with assessment of each organ system
Overview
This young man has neutropaenic septic shock until proven otherwise and requires aggressive resuscitation and management. Assessment will occur in concert with these efforts. While he has metastatic disease, long-term remission from this disease process is not uncommon and he is young, so maximal resuscitative attempts should be made in the initial phase, unless/until information is available to the contrary.
Assessment
History
•
AMPLE initially, then more comprehensive when possible
•
History of presenting complaint
•
vomiting — frequency; haematemesis or coffee grounds
•
recent pattern of oral intake and urine output (assess accumulated volume deficit)
•
fever history — onset, duration, pattern
•
Associated symptoms
•
diarrhoea/melaena/abdominal pain (colitis, gastroenteritis, GI bleeding)
•
URTI symptoms/cough/dyspnoea (respiratory infection, sinusitis)
•
frequency/dysuria/haematuria (UTI)
•
headache/confusion (meningitis/encephalitis)
•
toothache (dental abscess)
•
shoulder tip pain (referred from diaphragmatic irritation)
•
rash (cellulitis, bacteraemia, fungaemia)
•
Cancer history
•
previous therapy/timing — surgery, radiotherapy, chemotherapy regimens
–
recent cell counts and neutropaenia prophylaxis (e.g. G-CSF)
–
steroid use (likelihood of deficiency state)
–
bleomycin exposure (need for cautious O
2 therapy)
–
vascular access (e.g. Hickman/Portocath)
•
extent of metastatic disease (e.g. adrenal/pericardial involvement)
•
current aims of therapy — palliative/curative
•
advanced health directive — has DNR been considered/documented?
•
patient’s (and relatives’) level of understanding about short- and long-term prognosis
•
Additional history
•
past medical and surgical history (e.g. rheumatic fever increases risk of endocarditis)
•
social history (clarify current supports, smoking, illicit drug and alcohol use)
•
full list of current medications
•
allergies (particularly to antibiotics)
Examination
•
General appearance (distress, effort of breathing, conscious state, nutritional status)
•
Identify immediate life threats to airway, breathing, circulation
•
Vital signs (continuous monitoring of HR/rhythm, BP, RR, SaO
2, T)
•
Head-to-toe, looking for a source of sepsis particularly:
•
colitis (including neutropaenic enteritis or typhlitis)
•
central venous access sites/lines
•
Features suggestive of additional causes of shock — peripheral perfusion (warm versus cold) and JVP/neck veins
•
more likely:
–
hypovolaemia from vomiting or haemorrhage (low platelets)
–
Addisonian crisis from steroid withdrawal (history)
–
pericardial tamponade from metastatic disease (assess neck veins, heart sounds)
–
pulmonary thromboembolism (look for a limb DVT)
•
less likely:
–
tension pneumothorax (e.g. from recent central line insertion)
–
cardiomyopathy (chemotherapy-induced)
–
toxicological causes (although depression may have predisposed to an overdose)
Investigations
•
Bedside
•
ECG (look for signs of ischaemia/arrhythmia/electrolyte abnormalities)
•
blood gas (type 1 or 2 respiratory failure, acid-base status/Na/K/Cl changes from vomiting, hypoadrenalism, hypoperfusion from shock, renal failure)
•
urine dipstick (signs of infection)
•
Laboratory
•
full blood profile (look for neutropaenia, check Hb and platelets)
•
U&Es (look for electrolyte abnormalities including hypercalcaemia and renal impairment, serum glucose)
•
septic screen — blood (peripheral stab and from lines), sputum, urine, skin lesion culture
•
serum lactate correlates with degree of shock
•
consider lumbar puncture (if coagulation and platelets appropriate)
•
Radiology
•
chest X-ray (respiratory infection and pattern that may suggest the aetiology)
•
consider CT head if GCS abnormal
•
consider CT abdomen if intra-abdominal pathology suspected
SAQ 4: administration/medical systems
You are the director of a regional ED, and have 10 other district hospitals within a 250 km radius in your region. The CEO of your district has asked you to implement a retrieval service for the surrounding region. You are 400 km from the nearest metropolitan hospital.
Outline your response. (100%)
Sample answer
Plan
•
Information gathering and stakeholder assessment
Overview
The prospect of implementing a new retrieval service is exciting; however, extreme caution must be exercised before committing to an undertaking that has major ramifications for many individuals as well as major resource implications. It is prudent to defer immediate decision making in order to undertake a feasibility study and stakeholder analysis. Only then can an appropriate response be provided to the CEO.
Information gathering
•
Motivation/triggering events for district CEO — consider personal, medical and political possibilities; explore who else is driving/supporting the proposal
•
Need for service
•
patient numbers and predicted acuity/resource utilisation
•
Availability of alternatives, including the nature and efficacy of existing processes
•
Adequacy of current ED staffing
•
Projected number of FTEs required for a retrieval service
•
road-based transport staff
•
coordination by senior clinician
•
Internal resources available/service expansion capacity for retrieved patients
Response
A formal report should be prepared that encompasses the relevant information above and also:
•
Projected costs
•
equipment
–
communication — phones, radios
•
Choice of transport method(s) — procurement and maintenance
•
air — fixed, rotary wing
•
Flow-on effects — resources at receiving centre
•
Proposed clinical governance, business and management model
•
Proposed audit protocols and metrics
•
key performance indicators (KPIs)
•
critical incidents such as prolonged scene time, deaths during transfer
•
Proposed staffing model
•
Proposed implementation time line and key milestones
•
Analysis of possible external funding streams
•
local agencies/organisations (e.g. Rotary/Lions clubs)
•
Analysis of external links with services elsewhere (e.g. RFDS, Careflight)
•
Summary and recommendations
SAQ 5: paediatrics/anaesthetics
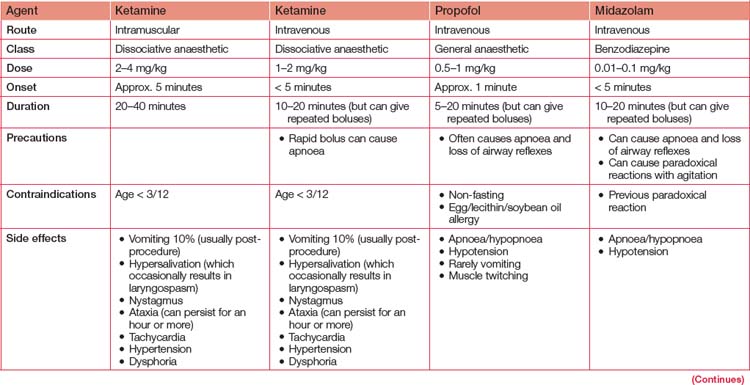
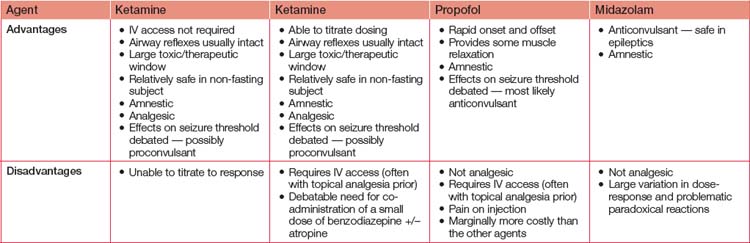
Discuss the use of parenteral agents for procedural sedation of children in ED. (100%)
Sample answer
Plan
•
Table 3.3 to assist coverage of pros and cons pertaining to the principal agents — ketamine, propofol, midazolam
•
Concluding brief summary of key positive and negative aspects of each drug
SAQ 6: psychiatry/medicine
A 37-year-old male presents to ED with a two-day history of bizarre behaviour including talking to himself, pacing and not sleeping. His wife is distressed because ‘he has never behaved like this before’. He is normally well and works as a computer programmer.
Describe your assessment. (100%)
Sample answer
Plan
•
Differential diagnosis based on what is known — organic and psychiatric conditions
•
Assessment — to differentiate between diagnostic possibilities
•
examination — ABC, then head-to-toe examination with assessment of each organ system
Overview
This patient has the potential for a life-threatening illness. An organic cause is more likely given his age, but a psychiatric disorder is also possible. Assessing him will involve searching for treatable causes while also managing him (and his wife) in a way that does not compromise one or the other’s safety.
Differential diagnosis
•
Organic
•
systemic disorder (e.g. hypoxia, acidosis, uraemic or hepatic encephalopathy, sepsis)
•
encephalitis (e.g. HSV, HIV, syphilis)
•
epilepsy (e.g. temporal lobe seizures)
•
drug intoxication, withdrawal or side effect (illicit or prescribed)
•
poisoning (e.g. heavy metals)
•
autoimmune disorder (e.g. SLE)
•
vitamin deficiency (e.g. B
6/B
12)
•
normal pressure hydrocephalus
•
Psychiatric
•
brief psychotic disorder
•
schizoaffective disorder
•
schizophreniform disorder
Assessment
History
•
Sources
•
previous health professionals/medical records
•
mental health teams where he has lived
•
History of presenting complaint
•
onset of symptoms — gradual, sudden
•
course of symptoms — fluctuating (? delirium); progressive (evolving disease)
•
any previous similar episodes
•
associated symptoms — full systems review
–
e.g. fever and infective symptoms such as cough, pain, headache, urinary frequency/dysuria, vomiting/diarrhoea, rash, recent oral or genital HSV infection/contacts (infection)
–
e.g. headache, numbness, weakness, head trauma (suggestive of intracranial lesions)
–
e.g. auditory hallucinations (psychiatric problem) versus visual hallucinations (suggestive of organic cause)
•
Past medical, surgical, psychiatric history (looking for predisposing factors to the conditions in the differential diagnosis list)
•
Medications
•
treatments suggesting a predisposing condition (e.g. steroids, mood stabilisers, anticonvulsants)
•
Social history
•
detailed drug and alcohol history; access to intoxicating agent
•
recent personal/work stressors
Examination
•
Mental state examination
•
concentrating particularly on safety issues, including violence and suicide risk
•
consider need for/use of restraint (verbal, physical and/or pharmacological) under ‘duty of care’ until cause clear and appropriate management determined
•
evaluate for mood derangements and perceptual disturbances
•
Vital signs (derangements may suggest an organic cause (e.g. fever, hypoxia))
•
Full head-to-toe examination (note this may require pharmacological restraint) looking particularly for:
•
asterixis (suggesting hepatic failure/hypercarbia)
•
skin lesions — rash, cellulitis, track marks
•
nuchal rigidity/meningism
•
localising neurological signs
•
ocular nerve palsy and/or nystagmus (suggestive of Wernicke’s encephalopathy)
•
evidence of pneumonia or intra-abdominal sepsis
•
toxidromes (mydriasis/miosis, tachy-/bradycardia, sweating/dry skin, increased secretions)
Investigations
•
Bedside
•
ECG — looking for ischaemia/arrhythmia/evidence of toxidrome
•
urinalysis — looking for infection
•
consider urine drug screen (a positive result should not dissuade from other potential diagnoses)
•
Laboratory
•
full blood profile
–
white cell count (potentially raised in infection; low in malignancy)
–
platelets (low associated with intracranial bleed and contraindicates LP; may be high with inflammation)
•
U&Es — hypo-/hypernatraemia; renal failure
•
Ca
2+ — elevated level more likely cause than low
•
LFTs — with hepatic failure
•
coagulation profile — abnormal with hepatic failure; associated with intracranial bleeding
•
urine culture — for infection
•
consider if indicated:
–
formal urine drug screen depending on history
–
blood alcohol — only to confirm what has been offered by history
–
lumbar puncture (if any evidence suggesting meningitis/encephalitis)
–
serum vitamin B
6, B
12, red cell transketolase (B
1/thiamine deficiency)
–
serum copper and caeruloplasmin (Wilson’s disease)
•
Radiology
•
chest X-ray — for infection/other causes of hypoxia if present, heart failure
•
CT brain — looking for space-occupying lesion, infarct, obvious encephalitis (e.g. HSV involving temporal lobes) — prior to LP
•
MRI — if focal signs and CT non-diagnostic or MS considered
–
likely to be difficult with restless patient
•
Other
•
EEG — looking for evidence of seizure activity
SAQ 7: surgery/administration
Write a guideline for the management of patients with suspected renal colic in the Department of Emergency Medicine. (100%)
Sample answer
Plan
Guidelines should be written on DEM letterhead using the standard department format.
Rationale
Suspected renal colic is a common presentation to ED. This protocol aims to improve the flow of patients through the department and serves as a guide for new staff members.
Background knowledge
CT KUB has replaced IVP as the investigation of choice to confirm the presence and precise location of calculi, exclude complications and guide management decisions. Spontaneous passage of a stone depends on the stone’s size (e.g. if 4 mm or less, 90% chance; if 5–7 mm, 50% chance; and if > 7 mm, intervention is usually required). Abnormal anatomy will also reduce passage (e.g. ureteral strictures).
Target
All adult patients presenting to ED with a diagnosis of suspected renal colic — a typical history includes unilateral flank pain that may radiate to the groin and genital region, nausea and vomiting, agitation and microscopic haematuria.
Recommendations
Analgesia
•
All patients should be given rectal indomethacin unless there is a contraindication. Dose: 100 mg once or twice daily. Patients who weigh less than 60 kg and are older than 60 years should not generally be given more than 100 mg daily.
•
Intravenous narcotics can be given at the same time (e.g. morphine titrated to effect).
•
Hyoscine-n-butyl bromide helps some patients, but not enough to reliably treat severe pain. Should not be used as sole analgesic agent.
Fluids
Hydration is necessary only for imaging and for the rare patient unable to tolerate oral fluids. Over-aggressive hydration is associated with increased pain from renal distension and urinomas and does not facilitate the passage of stones.
Investigations
First presentation
Perform the following investigations:
•
full blood profile, U&Es, calcium, phosphate and urate, urine microscopy and culture
•
non-contrast CT KUB
•
patients need a fluid load for optimal imaging and should be sent for imaging with a full bladder. Younger patients can be admitted to DEM overnight for CT in the morning. If CT shows an opaque stone, plain film KUBs can be useful to follow progress.
•
CT is
urgent in:
–
older patients with a first presentation as a ruptured or rapidly expanding abdominal aortic aneurysm — this is the most serious disorder to rule out; diverticulitis is also common in this group
–
patients with a single kidney
–
patients with infection and suspected obstruction (fever, leukocytosis, pyuria)
•
bedside ultrasound may be useful if skilled staff available. Renal distension confirms diagnosis and AAA may be excluded. However, inadequate and/or incomplete imaging limits bedside ultrasound to a quick screening test on first presentations prior to definite CT.
Subsequent presentations
•
Repeat blood tests only if indicated (e.g. fever, known or suspected renal impairment).
•
All patients should have a urine test sent for m/c/s to exclude pyuria and infection.
•
If the presentation is a continuation of a documented episode, there is rarely any need for CT.
•
Plain films can assess migration if the stone is radio-opaque.
•
Consider ultrasound if a change in the quality or intensity of pain suggests obstruction. This is
not urgent in the absence of infection.
•
Investigation depends on patient-specific factors. A young person should not be subjected to repeat CT scans due to radiation load. Conversely, renal colic cannot be assumed to be the cause of pain in an older patient with a distant history of stones.
Medical expulsive therapy
This term refers to the use of calcium channel blockers, alpha-blockers and steroids that have been shown to increase the rate of spontaneous passage and decrease the duration of pain. All patients should be started on this therapy unless there is a contraindication. It is best to give initial doses in hospital — even for patients going home — because of the incidence of symptomatic palpitations (nifedipine) and hypotension (alpha-blockers, nifedipine).
Disposition
•
Admit
if
•
diagnosis is uncertain — usually to DEM
•
patient requires ongoing parenteral analgesia — once diagnosis is certain, admission should be to urology rather than to DEM
•
infection with obstruction
— this means urgent urological referral, intravenous antibiotics and drainage
•
patient has a single kidney with a stone
— urgent urological referral Strain urine and send stone for analysis.
•
Discharge with follow-up
•
uncomplicated renal colic — refer to GP
•
Refer to urology as an outpatient if repeated presentations or stones > 5 mm.
•
Ensure patient is discharged with adequate analgesia and their imaging is organised.
•
Ask patient to strain urine with a tea-strainer at home so the stone can be sent for analysis.
Governance issues
These guidelines were prepared by the DEM Clinical Guidelines Committee <date>.
An audit of compliance with the guidelines will be performed after six months.
References
<list references>
Authorised by <DEM Medical Director>
Review date <typically 2–3 years>
SAQ 8: trauma
A 30-year-old electrician weighing approximately 100 kg presents to ED after a power-board explosion. He has 30% burns to his hands, face, chest and arms. He is awake and alert but in severe pain. He has an area of encircling full-thickness burn to his right arm.
Describe your management. (100%)
Sample answer
Plan
•
Management — simultaneous resuscitation (ABCDE), investigations and definitive therapies (supportive/specific)
Overview
There is potential for both life and limb threats in this setting. Much will depend on specific history (e.g. an associated fall, loss of consciousness), and assessment and management will occur in parallel. A trauma team should be involved and an EMST/EMSB approach utilised.
Management
Resuscitation
•
Primary survey
•
airway
–
intact at present, but potential for deterioration
–
consider early intubation if evidence of airway burns:
•
oedema/carbon-staining of pharynx
–
maintain spinal precautions
•
breathing
–
supplemental high-flow oxygen
–
treat tension pneumothorax/haemothorax if present
–
consider supporting ventilation +/– chest wall escharotomy if chest burns are causing respiratory compromise
•
circulation
–
large bore IV access × 2 — preferably through intact skin
•
disability
–
no obvious issues at present
•
exposure
–
keep covered following examination to prevent hypothermia
•
Secondary survey
•
head-to-toe examination including back and flanks for obscured burns
•
documentation of burns — area and estimate of depths
Investigations
•
Bedside
•
ECG (e.g. hyperkalaemia from deep burns/crush injury, myocardial contusion)
•
ABG (e.g. hypoxia/hypercapnoea from chest injuries, metabolic acidosis suggesting under-resuscitation, high carboxy Hb if accident in enclosed space)
•
dipstick urine (e.g. haematuria +ve in myoglobinuria — will be –ve on microscopy)
•
Laboratory
•
full blood profile (e.g. anaemia from blood loss)
•
E/LFTs (e.g. baseline renal function, hyperkalaemia with low Ca
2+ and high phosphate and CK/LDH in rhabdomyolysis)
•
coagulation profile (baseline)
•
Radiology
•
trauma series X-rays (C-spine, chest and pelvis)
•
CT chest/abdomen as clinically indicated
Definitive therapies
•
Supportive
•
if not already done, cool burned areas with room-temperature water for 20–30 minutes only (longer can cause/exacerbate hypothermia)
•
administer IV fluids (using Parkland formula)
–
4 × 30% × body weight (kg) = mL to be infused over 24 h
–
weight = 100 kg = 12,000 mL in first 24 h (half in first 8 h since the burn)
–
+ approximately 3 L maintenance fluid
•
monitor progress clinically as well as with urine output (aiming for 1 mL/kg/hr to avoid complications associated with myoglobinuria)
•
pain may be severe — analgesia options include inhaled methoxyflurane/nitrous oxide, titrated IV narcotic, low-dose ketamine as an adjunct
•
Specific
•
burns dressing guided by the burns team; cover in clear film initially
•
escharotomy of right upper limb — incisions for this should run through the burned tissue on the medial and lateral borders of the forearm and arm and continue to a depth where the underlying tissue is bleeding (as this indicates living unburned tissue)
•
may require circulatory or other support depending on organs involved
•
may require tissue debridement (e.g. electrical burns with deep necrosis)
•
may require specific management of other traumatic injuries
•
Disposition
•
will require admission +/– transfer to a specialised burns unit
•
high likelihood of requiring intensive care management
Key points
•
Practise answering SAQs early in your preparation and continue to do so throughout.
•
Be acutely aware of time — attempting an answer for
every question is the key to success.
•
Start each answer with a plan. If you are short on time, you may still score marks for this.
•
Remember this is a ‘short-answer’ question. Consider using lists, tables and diagrams where appropriate. Do
not write an essay.