FIGURE 3-1 European conceptual framework for occupational therapy. Reprinted from Creek J (2010) The core concepts of occupational therapy: a dynamic framework for practice. Reproduced by permission of Jessica Kingsley Publishers.
CHAPTER CONTENTS
PHILOSOPHICAL DEVELOPMENT OF THE PROFESSION
The Influence of Service Settings
Epistemological Underpinnings of a Two-Body Practice
Terms Used When Talking About Theory
Organizing Framework for Occupational Therapy Theory
There are two main parts in this chapter. The first section describes philosophical assumptions and beliefs that underpin the theory and practice of occupational therapy. This includes a brief discussion of the origins of occupational therapy philosophy, an account of how it has changed over the past 100 years and an outline of the main beliefs and assumptions held by occupational therapists today.
The second part describes the breadth of theory used by occupational therapists. It begins with an explanation of what we mean by theory and goes on to consider the different types of theory needed to support occupational therapy practice. Key occupational therapy concepts are identified and defined, including core concepts and emerging concepts. Definitions are given of the terms used when talking about theory for practice, such as frame of reference and model. The chapter finishes with an explanation of how knowledge is organized for use in practice, illustrated with an example of an occupational therapy theory: the European conceptual framework for occupational therapy (Creek 2010).
The modern profession of occupational therapy dates from about 1917. Since then, the profession has undergone, and is still undergoing, changes in its outlook and philosophy. Philosophy is a ‘system of ideas, opinions, beliefs, or principles of behaviour based on an overall understanding of existence and the universe’ (Shorter Oxford English Dictionary 2002). The philosophy of occupational therapy includes ideas and beliefs about the nature of human beings, society, health, ill health and the relationships between these various elements. Occupational therapy philosophy also includes principles of professional behaviour, and these are discussed in Chapter 7.
Initially, occupational therapy operated with a pragmatic and humanistic view of human beings and their relationship with occupation. Some of the main proponents of this philosophy of pragmatism worked in Chicago, where the first occupational therapy course was started in 1908. Pragmatism stresses the relationship between theory and action (Audi 1999): it has been described as ‘the philosophy of “common sense”, problem solving, activity, and adaptation’ (Breines 1986, p. 56). Pragmatism ‘recognizes the inextricable influences on each other of the mental and physical aspects of human beings, their artifacts, their environments, and the societies and times in which they live’ (Breines 1995, p. 16).
Adolph Meyer, one of the founder members of the National Society for the Promotion of Occupational Therapy in the USA, was a friend of the two most famous pragmatic philosophers of his day, John Dewey and William James, sharing their perspective (Serrett 1985). From 1913 to 1914, Meyer worked with Eleanor Clarke Slagle to develop a method of treatment called habit training, based on the work of James. This has been described as the oldest model of occupational therapy practice (Reed and Sanderson 1999).
Meyer wrote a paper on The philosophy of occupation therapy, which shows clearly the influence of pragmatism (Meyer 1922/1977, pp. 640–641).
Direct experience and performance [are] everywhere acknowledged as the fullest type of life. Thought, reason and fancy [are] more and more recognised as merely a step to action, and the mental life in general as the integrator of time, giving us the fullest sense of past, present and future … performance is its own judge and regulator and therefore the most dependable and influential part of life … Our conception of man is that of an organism that maintains and balances itself in the world of reality and actuality by being in active life and active use, i.e., using and living and acting its time in harmony with its own nature and the nature about it. It is the use that we make of ourselves that gives the ultimate stamp to our every organ.
The humanistic perspective taken by occupational therapists grew from the profession’s connection with the arts and crafts movement in the UK (Mattingly 1994b). The first occupational therapists believed ‘that unleashing people’s creativity might help them transcend the stultifying effects of incapacity, hospitalization and industrial labour’ (Hocking 2007, p. 23). Humanism views people as ‘growing, developing, creating being(s), with the ability to take full self-responsibility’ (Cracknell 1984, p. 73). This includes taking responsibility for maintaining their own health and for making choices that determine what they become.
Several of the early influences on occupational therapy came from outside health and social care services, for example, the arts and crafts movement and pragmatism (Paterson 2010). Nonetheless, the first occupational therapists worked in hospitals for people with mental and physical illness or disability and their actions were constrained by the ethos and expectations of these settings.
During the 1950s and 1960s, the reductionist model of science was being adopted by all the life sciences. Reductionism is based on the belief that the structure and function of the whole can best be understood from a detailed study of the parts by observation and experiment (Smith 1983). Western medicine is based on a reductionist medical model, with a ‘focus on pathology … and on the minute and measurable’ (Shannon 1977, p. 231). Scientific advances in medicine in the second half of the twentieth century led to an increasing use of technological interventions and an accompanying need for specialization, so that the focus of health services moved from health to illness and the responsibility for wellness moved from the individual to the medical profession.
In the first half of the twentieth century, the profession of occupational therapy did not have its own knowledge base with which to justify a pragmatic approach to intervention; occupational therapists worked under the direction of doctors. This left them vulnerable to pressure to adopt reductionist theories into the educational curriculum:
early occupational therapists had a moral imperative to train more practitioners but no knowledge base of their own with which to educate them or much of any status or expertise with which to argue for particular educational practices. This vacuum was largely filled by deference to medical authorities … under the strong influence of physicians, basic medical sciences and applied medical lectures occupied more of the field’s core curricula over ensuing decades.
(Hooper and Wood 2002, p. 46)
By adopting a reductionist paradigm, occupational therapists were able to develop a great depth of expertise in various fields of practice – for example, many therapists became highly skilled in the use of projective media in analytic group psychotherapy – but the profession as a whole suffered from role diffusion and loss of identity (Kielhofner and Burke 1977). The broad, humanistic perspective was lost and occupational therapists’ concern gradually shifted from people with complex, long-term needs to those who could be cured, while their goals changed from adaptation to the reduction of symptoms.
In the 1980s, there was a general move away from a mechanistic view of man and health to a systems view that is more congruent with the pragmatic and humanistic perspective of occupational therapy. Occupational therapists saw the possibility that ‘health care of the future will consist of restoring and maintaining the dynamic balance of individuals, families and social groups, and it will mean people taking care of their own health individually, as a society, and with the help of therapists’ (West 1984, p. 21). This prompted them to reassess the original philosophy of occupational therapy, which had become obscured during the 1950s and 1960s.
More recently, the profession attempted to reassert the validity of occupational therapy traditions and values without losing the very real advances in theory and practice made during the reductionist era. The areas of belief that are still relevant to occupational therapy practice in mental health are summarized here and will be explored in more detail later in the chapter:
■ concern with the person as a physical, thinking, emotional, spiritual and social being, who has a past, present and future, and who functions within physical and social environments
■ belief in intrinsic motivation, which is an innate predisposition to explore and act on the environment and to use one’s capacities
■ recognition of each person’s need for a balanced range of occupations in their life in order to facilitate development, give meaning to life, satisfy inherent needs, realize personal and biological potentials, adapt to changing circumstances and maintain health
■ acceptance of the social nature of people and of the importance of social interaction in shaping what we become
■ recognition that what we do influences what we become – the primacy of function over structure
■ view of health as a subjective experience of wellbeing that results from being able to achieve and maintain a sense of meaning and balance in life
■ belief in the capability and responsibility of people to find healthy ways of adapting to changing circumstances through what they do
■ acceptance of the role of occupational therapy in serving the occupational needs of people in order to help them restore meaning and balance to their lives
■ belief in occupation as the central organizing concept of the profession and in the use of activity as our main treatment medium.
Professional philosophy is the system of beliefs and values shared by members of a profession. Philosophical assumptions are the basic beliefs which make up this system and show how members of a particular profession view the world and their own goals and function within it (Mosey 1986). In occupational therapy, we accept as true certain beliefs about the nature of people, for example that; ‘All people experience the need to engage in occupational behaviour because of their species common combination of anatomical features and physiological mechanisms. Such engagement in occupation is an integral part of complex health maintenance systems’ (Wilcock 1995, p. 69). Without this belief, we would not be convinced of the value of occupation as therapy. It is healthy for us to question and challenge our basic assumptions, which are inevitably modified over time, but the sharing of a set of fundamental beliefs contributes to our sense of identity as a profession.
The three areas of belief central to occupational therapy are concerned with:
■ The nature of health and illness
■ The goals and function of occupational therapy.
Occupational therapy is essentially client-centred, which means that: ‘the occupational therapist does not force his value system upon the client. But rather, through using his skills and knowledge, exposes the client to a range of possibilities which constitute his external reality. The client is the one who makes the choice.’ (Yerxa 1967, p. 8).
This belief in the right of people to make their own choices is made up of three separate beliefs:
■ A concern with the whole person within their environment
■ A belief in intrinsic motivation to be active
■ An understanding of the social nature of people.
Occupational therapists see each person as a unique individual, whose body, mind and spirit function together and cannot be understood as separate entities. People change, according to this view, if they are separated from the environmental influences that shape who they are. These influences include the physical environment, the cultural environment, societal factors and social support (Christiansen 1997).
This whole-person approach assumes that people can only be understood by seeing the relationships between body, mind, spirit and environment over time because the unique feature of humanity is the ‘capacity of imagination and the use of time with foresight based on a corresponding appreciation of the past and the present’ (Meyer 1922/1977). Occupational therapists are concerned with the person as they are now, at this moment, and with how they function at different times and in different environments. We are concerned with the balance of occupations in the course of the individual’s lifetime, not just with single activities.
Western medical science is founded on the principle that human life should be preserved if possible. Occupational therapy takes the principle that human function should be preserved or restored where possible. It is the basic premise of our profession that being able to function and participate in a range of occupations is a desirable condition (Reilly 1962).
Indeed, it can be argued that human life and human function are the same thing. People have an intrinsic motivation to act on the environment in order to discover their own potential and to develop their capacities. We do not wait for the environment to impinge on us and then respond; we are able to visualize the ends we wish to achieve and act to realize them. West (1984, p. 13–14) summarized writings on occupational therapy philosophy as follows:
Activity is the essence of living and is significantly interrelated with high morale … to some degree life itself is seen as purposeful occupation – that is to say, as activity, as task, as challenge … it is the purposefulness of behaviour and activity that gives human life order … the basic philosophy of occupational therapy speaks to Man as an active being and to the use of purposeful activity as Man’s interaction with and manipulation of his environment.
People do not act in isolation: we are essentially social animals who develop and live in the context of groups. Human interaction stimulates biological, psychological, emotional and social development, and people deprived of human company do not thrive. There is a long period of physical and emotional dependency in childhood, and it is both normal and healthy to retain some emotional dependence on others once physical maturity is reached.
Social groupings take different forms in different cultures but a small and stable social group is considered most desirable within all cultures. People do not cope well with living in groups that are too large for us to have meaningful contact with everyone else. This means that we have had to devise coping strategies for living in larger groups, for example in cities.
Occupational therapists view health as not merely the absence of disease but ‘a dynamic, functional state which enables the individual to perform her/his daily occupations to a satisfying and effective level and to respond positively to change by adapting activities to meet changing needs’ (Creek 2003, p. 54). The individual is seen as healthy, or functional, when they have learned the skills necessary for successful participation in their expected range of roles throughout their life.
Not only do occupational therapists believe that health can be defined by what we are able to do, we also believe that what we do makes us healthy or unhealthy. What people do creates functional demands that drive neuroplastic changes and organization, and therefore occupations shape what we become: physically, mentally, socially and spiritually. This belief was expressed in a much quoted phrase: ‘that man, through the use of his hands as they are energized by mind and will, can influence the state of his own health’ (Reilly 1962, p. 2). An even stronger expression of this belief is that ‘engagement in occupation is a central, evolutionary mechanism for the maintenance and promotion of health’ (Wilcock 1998a, p. 1). An inability to achieve a desired state of function is called dysfunction but the two states can be seen as a continuum: ‘there is essentially no break or line of demarcation between that which is considered function and that which is considered dysfunction’ (Mosey 1986, p. 13).
Dysfunction is ‘a temporary or chronic inability to meet performance demands adaptively and competently and to engage in the repertoire of roles, relationships and occupations expected or required in daily life’ (Creek 2003, p. 52). Dysfunction occurs when people are unable to maintain themselves within their environment because they do not have the skills necessary for coping with the current situation. It is therefore very individual: for a pilot, fear of flying could be a major disability while, for an occupational therapist, the same phobia may be only a minor inconvenience.
Causes of dysfunction fall into four main groups:
■ Failure to develop and mature normally due to physical abnormality or environmental deprivation, for example chromosomal abnormality or emotional abuse
■ Environmental or personal changes that the individual cannot cope with, such as war or bereavement
■ New physiological or psychological demands that cannot be met using existing skills, such as parenthood
■ Pathology or trauma causing loss of skills.
When the individual encounters a new situation, they use their existing skills to try to master it. If these fail, they try to learn effective new skills. Eventually, if the situation still remains outside their control, they experience disequilibrium or crisis. The pace at which change occurs is important for maintaining equilibrium; too fast a pace means that new skills are not learned quickly enough, adaptation is disturbed and a state of dysfunction may occur (Mosey 1968). The degree and pace of change that a person can manage without losing equilibrium are dependent on both internal factors (e.g. the ability to learn new skills quickly) and external factors (e.g. the amount of support available in the social environment).
The occupational therapist’s perspective on health and dysfunction is similar to that described in the International Classification of Functioning, Disability and Health (ICF). The ICF defines functioning as ‘an umbrella term encompassing all body functions, activities and participation’, while disability is ‘an umbrella terms for impairments, activity limitations or participation restrictions’ (WHO 2001, p, 3). Diseases and disorders are called health conditions. The word illness is sometimes used synonymously with disease but is more often used to refer to a person’s subjective experience of having a health condition.
The uniqueness of the occupational therapy approach to mental health difficulties lies in the assumption that human beings have the ability to influence their own health through what they do. If people can maintain or improve their health by engaging in occupation, it follows that occupation can be used as a treatment medium to ‘remediate disability, encourage adaptive behaviour, teach skills and build individual and group identity’ (Creek 2007, p. 127).
Occupational therapy has been described as a ‘two-body practice’ because it encompasses both a disease perspective, focusing on problem identification and treatment, and an illness experience perspective, which is concerned with the ways that disease affects a person’s life (Mattingly 1994a, p. 37). Occupational therapy addresses the consequences of disease or injury, as they affect a person’s ability to function, rather than the primary pathology. For example, the occupational therapist tries to teach a person how to manage their anxiety so that it does not interfere with their activities and occupations, rather than working directly on the anxiety. However, reduction in anxiety often follows as the individual’s quality of life improves through this approach.
The core skills of occupational therapy are activity analysis, adaptation, synthesis and application. The outcome of intervention should be that the client is able to enact a satisfying range of occupations ‘that will support recovery, health, wellbeing, satisfaction and sense of achievement’ (Creek 2003, p. 32). The main aim of intervention is to develop each person’s potentials to the highest possible level, to enhance their quality of life and sense of wellbeing, to increase their satisfaction in daily living and to improve access to opportunities for participation in life situations through occupation.
Occupational therapy is concerned with the things that people do in their daily lives, the meanings that people give to what they do and the impact that doing has on their health and wellbeing. This broad focus on ‘the ordinary and extraordinary things that people do every day’ (Watson 2004, p. 3) means that occupational therapy not only contributes to the restoration of health and function but also meets people’s needs within broader occupational and social contexts. Occupational therapy contributes to building people’s occupational identities as much as to restoring physical and mental function, and to building healthy communities that can include all their members, whatever disadvantages or disabilities they may experience.
The unique goal of occupational therapy is to help people with performance deficits of any kind make and express meaning through occupation, or intentional, organized performance … Occupations are applied to promote, achieve and maintain human functioning and a quality of life that gives meaning and purpose to living. The primary aim is to address issues of occupational dysfunction, disruption, deprivation, alienation, and unfulfilled potential.
(Watson and Fourie 2004, p. 26)
Occupational therapy is often concerned with multiple and complex needs and problems but can also be of benefit to people who have minor coping difficulties or for those who wish to maintain and promote their wellbeing (Creek 2003). Intervention may be at an early stage of the person’s difficulties, in order to mitigate or prevent any ongoing adverse effects, or may be appropriate at any stage of a long-term health condition.
Occupational therapists work with people of all ages who have problems with carrying out the activities and occupations that they expect or need to do, or with carers or care staff who support people’s daily activities and occupations. Occupational therapy can be focused on individuals and groups, such as a family, or an organization, such as a school.
Occupational therapists recognize that their interventions are most effective when the person is involved and engaged in the process of setting and working towards goals. It is a requirement of the Code of Ethics and Professional Conduct (College of Occupational Therapists 2010, p. 16) that the therapist ‘should work in partnership with the service user and their carer(s), throughout the care process, respecting their choices and wishes and acting in the service user’s best interests at all times’.
In the traditional professional–client relationship, the therapist is the expert and the client is the passive recipient of that expertise. When the therapeutic relationship is seen as a partnership, the professional is the expert in managing disease or illness while the person is the expert in their own life. Client-centred occupational therapy intervention is a collaborative process in which everyone involved aims to negotiate and share choice and control. This can be at two levels:
■ The level of the intervention: throughout the occupational therapy process, the focus is on the person’s needs, wishes and goals rather than on the requirements of the health or social care system. This includes determining the need for occupational therapy, assessing, gathering data, setting goals, working in partnership to attain goals and evaluating the outcomes of intervention (Sumsion 1999)
■ The level of service planning, delivery and evaluation: service users are represented and take an active role in those committees and working groups responsible for the design, delivery and evaluation of services.
There is a third model for the professional–client relationship and this is full self-management, in which the professional is only one of the resources that the person draws on in managing their own health condition (Van Olmen et al. 2011). Choice and control are not shared but are located with the person.
When a person is too ill or disabled to take control or to participate fully in the intervention process, the therapist may have to take responsibility for making decisions, remaining aware of the risk of imposing their own goals and values and actively trying to avoid this. One of the goals of intervention will be ‘to work towards increasing client understanding, autonomy and choice’ (Creek 2003, p. 30).
The understandings that occupational therapists have of people, occupation and health, and of the relationships between them, determine what they see as their professional purpose. In order to fulfil that purpose, the profession builds a knowledge base to explain, support and justify the practice of occupational therapy. The current knowledge base is outlined in the next section.
Theories are conceptual systems or frameworks used to organize knowledge in order to understand or shape reality: they give the mind a conceptual grasp on reality (Dickoff et al. 1968). Theories are constructed for particular purposes and a good theory will fulfil the purpose for which it was designed. For example, the ICF is a theory that was developed to promote international communication about health at every level (WHO 2001).
Theory in a practice discipline must provide ways of conceptualizing reality that can guide action towards fulfilling the profession’s professional goals (Dickoff and James 1968). For occupational therapists, theory must enable individualized, responsive, client-centred practice. Occupational therapists use theory:
■ as a guide to practice, to encourage coherent and systematic treatment
■ to suggest alternative treatment strategies
■ to enable effective communication
■ to provide a rationale for practice
■ to provide a basis for researching practice (Creek 2003, p. 35).
It has been suggested that occupational therapy theory is not something we learn and then apply in practice.
In occupational therapy, theorising is an integral aspect of practice. We do not contribute to theory by first understanding what theory is and then developing a theory of our own. We do theory by developing collaborative models of thoughtful practice that challenge assumptions and suggest new lines of inquiry; we do theory by learning how to align thoughtfulness and practice within specific contexts that require constant negotiation across complex professional, cultural and social boundaries.
(Nixon and Creek 2006, p. 77)
This view describes a practitioner who is continually thinking about what they are doing, reasoning about the most appropriate course of action, reflecting on the effects of their interventions and negotiating with everyone involved to reach agreement on the best way forward. Formal theories, learned from lectures and books, are only one part of theorizing in complex, client-centred interventions.
As described above, occupational therapists work with both a disease perspective that focuses on the identification and treatment of disease-related problems and an illness perspective that considers the ways a health condition affects a person’s life (Mattingly 1994a). These two perspectives represent different ways of knowing, or epistemologies. An American occupational therapist, Hooper (2006), claimed that our chosen epistemology ‘functions as a screen through which we filter the experiences we consider important from those we do not’ (p. 16). It is important to understand not just what we know but also how we know, that is, how we take in and make sense of experience.
The two epistemologies espoused by occupational therapy enable us to move, without losing sight of the complexity of occupation, from the ‘minute and measurable’ (Shannon 1977, p. 231) consequences of disease, such as short-term memory loss or sleep disturbance, to the wider aspects of illness experience and its impact on performance. Mattingly (1994a, p. 37), called this a ‘two-body practice’. The capacity to support a two-body practice, by moving between two epistemologies, is one of the strengths and unique features of occupational therapy.
Occupational therapists have bridged two contradictory value systems for more than 75 years. The ability to combine the biomedical aspects of patient illnesses with the humanistic values of the Arts and Crafts Movement requires complex patterns of integrative treatment planning. This skill is an asset in today’s healthcare arena where the limitations of scientific medicine encourage practitioners to emphasize the art of patient care. Occupational therapists who have struggled with ways to balance the scientific and artful aspects of practice can guide other professionals to develop more integrative health services.
(Schemm 1994, p. 1086–1087)
A good theory for practice is predictive, in that it helps the therapist to understand cause and effect and to make predictions about the likely outcomes of intervention, so that the most appropriate and effective course of action can be undertaken (Dickoff et al. 1968). Predictive theory is underpinned by more basic types of theory: naming and descriptive. Naming theory involves isolating and categorizing concepts, such as objects, ideas and feelings. Different names may be given to the same phenomenon, for example a person who does not want to attend occupational therapy groups may be called non-compliant, antisocial, independent or unmotivated. Each of these words represents a different way of understanding the person’s behaviour. The names that a discipline selects for its core concepts indicate how its members view the world.
Descriptive theory depicts the relationships between concepts. The ICF is an example of a descriptive theory. Concepts that represent functioning and disability associated with health conditions are first named and defined, including body functions, body structures, impairments, activity and participation (WHO 2001). These concepts are then organized into a framework that depicts how they interact with each other.
The next section defines the concepts that have been identified as core to occupational therapy theory and discusses some of the newer concepts that are emerging to support more recent theoretical and practical developments.
A concept is a mental representation of an object or idea (Creek 2003). Giving a name to a concept enables us ‘to point out, denote, or attend to conceptually a factor within the mind’s consciousness’ (Dickoff et al. 1968, p. 420). For example, the word activity represents a concept that can be differentiated from other concepts that are not called activity. In a sense, until something is given a name it does not exist.
All disciplines identify the key concepts that underpin their subject area and the names of these concepts form the vocabulary of the field. Concepts are the building blocks of theory, just as words are the building blocks of language. In order to build theories that support the practice of occupational therapy, it is necessary to identify key concepts, agree on their precise meanings and find words to name them. Clearly defined and named concepts allow us to think and communicate about occupational therapy, to describe what we see and what we are doing, and to explain why certain situations or actions lead to change in one direction or another.
Most occupational therapists are able to agree on the names that represent core concepts underpinning the profession’s knowledge base, such as occupation, activity and function. However, there are many different ways of defining these concepts, leading to confusion and a weak foundation for building higher levels of theory. If we cannot agree on the precise meaning of activity and on how it differs from occupation, it is not possible to describe clearly the relationship between the two concepts or to predict how change in the way a person performs an activity will impact on their occupations.
The definitions presented in this section were developed by the terminology working group of the European Network of Occupational Therapy in Higher Education (ENOTHE) from 2002 to 2008 (Creek 2010). This terminology project was a collaboration between occupational therapists from six countries, representing six European languages. The ENOTHE definitions are based on a review of existing definitions in the occupational therapy literature worldwide. The terms that refer to aspects of the performer’s perspective on occupation, and their definitions, are given in Box 3-1.
The words activity and occupation are often used synonymously by occupational therapists but it is important to clarify the differences, for the reasons given above. Traditionally, occupational therapists have classified these two terms in a hierarchical relationship, with occupation at a higher level so that activities are seen to contribute to occupations (Hagedorn 2000). A hierarchical taxonomy of occupational therapy terms, developed in Canada, described seven levels of occupation, from occupational grouping at the highest level to voluntary movement at the lowest (Polatajko et al. 2004). In this classification, occupations are made up of activities, which are made up of tasks, which are made up of actions.
A different approach to understanding the relationships between occupation, activity and task was suggested by the ENOTHE terminology group, who described the concepts as a network rather than a hierarchy. In this conceptualization, a piece of performance can be experienced as an occupation, an activity or a task, depending on the context and the perspective of the person performing the action: ‘the terms do not refer to the action itself but to how the performer conceptualizes it’ (Creek 2010, p. 80). For example, cooking might be an occupation for a chef, an activity for a housewife and a task for a person undergoing rehabilitation. But each person’s perspective can change so that there may be times when the chef experiences cooking as a leisure activity or, within rehabilitation, cooking becomes a purposeful activity, contributing to recovery.
The purpose of an activity is its goal and an intrinsic part of the activity (Creek 2010); for example, when I am making a cup of tea, my goal is to make a cup of tea. A single activity can have more than one goal; for example, walking to work may be for the dual purpose of getting to work and keeping fit. When an activity is used as a therapeutic medium, it has both an intrinsic goal (make a cup of tea) and a therapeutic goal or goals (complete a simple activity, without prompting, by planning and executing the appropriate sequence of tasks).
The meaning of an activity is its significance for the person performing it; therefore meaning is located in the person, not in the activity (Creek 2010). Much of the meaning of an activity comes from the context in which it is performed and can change each time it is performed, or even during the performance. For example, I make a cup of tea mid-morning to give myself a short break from working at the computer. The meaning of this activity comes from my liking tea and needing to move around. However, making tea takes on a more formal and social meaning if a friend arrives as I put the kettle on.
A person receiving occupational therapy intervention may perceive a different meaning in the activity from that intended by the therapist. For example, in order to assess sequencing ability the therapist asks someone to make a cup of tea, but the person perceives this task as a test to be passed before being allowed to leave hospital.
Occupations are frequently classified into different categories, such as self-care, productivity and leisure, which are sometimes called occupational performance areas (ENOTHE 2006). These are artificial differentiations, since an occupation can move from one category to another or belong in more than one category at the same time. For example, cooking a meal may be self-care if it is to satisfy an individual’s hunger, it may be productive work if it is to feed a family, it may be leisure if it is a dinner party for friends, or it may serve more than one purpose.
Self-care activities and tasks enable the individual to survive and to promote and maintain health. They include:
■ basic physical functions such as eating, sleeping, excreting, keeping clean and keeping warm
■ survival functions such as cooking, dressing, shopping, maintaining one’s living environment and keeping fit.
Work is any productive activity, whether paid or unpaid, that contributes to the maintenance or advancement of society, as well as to the individual’s own survival or development. Work may help to maintain society (e.g. housework) or contribute to its advancement (e.g. theoretical physics).
The work in which a person spends most of their time usually becomes an important part of their personal identity and a major social role, giving them their position in society and a sense of their own value as a contributing member. Different jobs are given different social values so that people in certain jobs are considered to be more important than others, irrespective of how necessary their work is to the continuation of society. For example, the work of a doctor is more highly valued in Western society than that of a housewife.
Man is a very adaptable species and this adaptability has been achieved by developing flexible behaviour rather than specialized behaviour (Kielhofner 1980). Play is the medium through which children are able to learn and rehearse a wide range of skills that will enable them to respond appropriately and adaptively in different situations. Even in adult life, new skills are learned more thoroughly and integrated more successfully into the pattern of daily life if the individual approaches learning in a playful and explorative manner.
In adult life, play is usually called leisure and is often used to satisfy individual needs that are not met by either self-care or work occupations. For example, amateur dramatics can improve the physical wellbeing of a person who has an otherwise sedentary lifestyle, provide intellectual stimulation for a full-time mother of small children, create social contacts for an unemployed person or enhance the social status and self-esteem of someone who has a low-level position at work.
The word occupation is used to refer both to the pre-existing format that guides or structures how someone performs an activity and to the performance itself (Nelson 1988). For example, there is an established format of rules, procedures, equipment and environment for playing football. This is the occupational form, which is socially constructed and exists independently of performance. Football has a physical environment that includes materials, location, human context and temporal context. It also has a sociocultural reality that depends on a social or cultural consensus and allows the occupational form to be interpreted differently in different social contexts, such as the differences between a game of football for schoolchildren and a professional championship match.
Playing football, the doing, is performance. Depending on how a person feels about playing football on a particular occasion, this may be experienced as occupational performance, activity performance or task performance. The way in which we perform an occupation, activity or task depends not only on the given occupational form but also on our level of competence and the meanings that we give to it. For example, a professional goalkeeper may deliberately allow the ball into the net if they are trying to encourage a young child to learn the game, or they may do their best to keep it out when their team is playing an international match.
The intrinsic factors that enable or support occupational performance are called occupational performance components (ENOTHE 2006), performance enablers (Christiansen 1997) or personal requisites for action (ENOTHE 2006). These factors include:
■ abilities, such as the ability to sing in tune
■ skills, including motor, sensory, cognitive, intrapersonal and interpersonal skills
■ functions, such as grasping a bat or using it to hit a cricket ball.
It should be noted that the word function has two related meanings for occupational therapists and this can lead to misunderstandings. In the phrase upper limb function it is being used in the sense of ‘the underlying physical and psychological components that support occupational performance’ (Creek 2010). In the phrase function in personal activities of daily living it is being used in the sense of ‘the ability to perform competently the roles and occupations required in the course of daily life’ (Creek 2010).
Each person organizes their occupations, activities and tasks over time into patterns that meet their needs and satisfy the demands of their environment. The organization of time in this way is known as temporal adaptation. The healthy individual has their daily life activities organized into a satisfying and flexible pattern of habits and routines that meets their needs and is socially acceptable.
A habit is a way of structuring the performance of tasks, activities and occupations (Creek 2010). Habits enable efficient function because they are practised sequences of action that do not require conscious attention, such as changing gears when driving a car. When most of the actions involved in driving are habitual, the driver’s mind is free to concentrate on the route, on safety or on other matters.
The terms habit and routine are sometimes used synonymously by occupational therapists but it is useful to think of them as two distinct concepts. A routine is an established and predictable way of doing something, for example following the same route to work every day, even when there are alternatives. Some routines are repeated until they become habitual and so do not require conscious thought. Habits and routines create stability and security for both individuals and communities.
Independence has sometimes been described as the goal of occupational therapy interventions but, in recent years, the concept of interdependence has been gaining ground. Baum and Christiansen (1997) pointed out that no person who lives in a community is truly independent because we all collaborate and cooperate with each other. They suggested that:.
The concept of interdependence is embodied within the idea of occupational therapy as a helping profession. That is, by working with our clients and their families, we can achieve goals that we could not achieve working independently.
(p. 35)
The occupational therapist may work towards increasing independence or interdependence – the goal will be determined by what the person wishes. When a person is not able to make decisions, it may be because their autonomy is compromised. The ability to make and enact choices rests on three types of autonomy (Gillon 1985/1986):
■ Autonomy of thought: being able to think for oneself, to have preferences and to make decisions
■ Autonomy of will: having the freedom to decide to do things on the basis of one’s deliberations
■ Autonomy of action: the capacity to act on the basis of reasoning.
It is possible to make autonomous decisions without compromising healthy interdependence. For example, an individual with severe physical disabilities may take the decision to be dependent on others for their self-care so that they can put their time and energy into pursuing an interesting career.
Another term that is used when referring to people’s ability to make their own decisions is mental capacity. This is a legal term that denotes competence. Competence is a ‘skilled and adequately successful completion of a piece of performance, task or activity’ or being adequately qualified to perform a task (Hagedorn 2000, p. 308).
The 2005 Mental Capacity Act makes provision for people who are identified as lacking the capacity to make their own decisions in the areas of finance, social care, medical treatment, research and so on. Each decision is treated separately, so that someone can be deemed to have mental capacity in some areas of life but not in others.
Occupational performance always takes place within environments, contexts and settings that influence why and how the person performs. Occupational therapists sometimes use these three terms interchangeably but we can think more clearly, and communicate more precisely about the influences on performance, if we understand their subtle differences in meaning.
Environment is a broad concept that includes physical, social, cultural, temporal, economic and political influences. Environment influences occupational performance by making demands on the individual or group: these demands shape when and how people perform while performance, in turn, shapes the environment. For example, a person with a large garden has to make decisions about how to care for it, including the layout, what to plant and what standard they want to achieve. The garden demands some type and level of action, however minimal, and that action changes the garden. Hagedorn (2000) described three levels of environment, recognizing familiar, possible and inaccessible elements.
The context for action refers to the relationships between environment, personal factors and events. For example, the way a person cares for their garden is influenced not only by where they live, and the appearance of other neighbouring gardens, but also by their own tastes and skills, the amount of money they can afford to spend, any help available and many other contextual factors. An event, such as a violent storm, will also influence what they do in the garden.
The reason why context influences performance is that it shapes the meaning of a task, activity or occupation for the individual or community. The meaning of an action changes depending on the context; for example, preparing the garden for an open garden day, in which people raise money for charity by allowing the public into their gardens, has a different meaning from organizing the garden as a setting for children’s games and sports.
The setting for action is the immediate environment in which the person or group is performing, such as the treatment setting, work setting or community setting. The setting influences how a task, activity or occupation is performed; for example, a person cooking a meal in the setting of their own kitchen is likely to perform differently from when they cook with an occupational therapy group in the hospital setting.
Three concepts associated with the social context in which a person performs are task, participation and role, as defined in Box 3-1. It should be noted that occupational therapists use the word task with two distinct meanings. A task can be a step taken in the performance of an activity, as described in the earlier section on occupation and activity. It can also be a piece of work that the individual is expected to do; for example an occupational therapy tutor might set a group of students the task of critically appraising a research paper.
Participation is defined in the ICF as ‘involvement in a life situation’ (WHO 2001, p. 10). The ENOTHE terminology group added two elements to this definition: activity and social context (ENOTHE 2006). For occupational therapists, the key features of participation are that it involves action by the individual and that it always has a social context, even when the person is acting alone. Voting in a local election is an example of participation: it requires the person to take action, either by sending a postal vote or going to the polling station. Whether postal or personal, casting a vote is a solitary activity but it takes place in a social context and has a social impact.
The process of creating opportunities ‘to participate in life’s tasks and occupations irrespective of physical or mental impairment or environmental challenges’ has been called enablement (Christiansen and Townsend 2004, p. 276) and is a key part of the occupational therapist’s role.
Roles are allocated by society and adopted by the individual, so that a role is both a social position and a set of tasks performed by the individual. Each person will interpret a role in a unique way. For example, the role of mother carries expectations about the care and nurturing of children. Women in the UK normally play a major part in bringing up their own children because that is the expectation in Western society. However, different women interpret the role in different ways, perhaps delegating some aspects to a relative or a paid childminder. If society feels that a woman is not fulfilling her role adequately, then it may be taken away from her and her children given into the care of others. Or a woman may choose not to accept the role of mother and may give her children into some form of care.
An occupation and a social role may share the same name, although a role is more likely to be described by a noun and an occupation by a verb. For example, mother is a role, while mothering is an occupation. The concept of occupation is mainly concerned with the actions that a person takes to achieve their purposes, while the concept of role is mainly concerned with social expectations and the mechanisms by which society shapes the actions of individuals.
Social role is linked to social status, which refers to the position of the individual within the social structure. The status we achieve through our major social roles influences both the way that other people in our social group treat us and our expectations of how we will be treated. For example, if we have a high social status, we are more likely to expect to be treated with respect and consideration.
Roles carry both rights within society and obligations to that society. For example, a university student has the obligation to attend a certain number of teaching sessions, behave in an acceptable way during those sessions, make an effort to learn the topics presented and complete a prescribed number of assignments within a given timescale. In return, the student is provided with money, a valued position in society and the possibility of paid employment at the end of the programme of study.
Person-centred practice requires a person’s active involvement in the process of therapy, and three terms are used to refer to this involvement: motivation, volition and engagement.
Motivation is the energy source for action, the ‘drive that directs a person’s actions towards meeting needs’ (ENOTHE 2006). The term is sometimes used synonymously with volition and there are similarities in meaning between the two words.
However, the concepts can be differentiated by thinking of motivation as the drive to act and volition as an ability to make choices about action. Exercising volition becomes easier with practice so it can also be thought of as a skill.
Engagement in activity suggests attention and commitment to what is being done, not simply being present in body. When someone is engaged in an activity, their attention is focused on a goal and/or on the experience, not on the skills and effort required. They are absorbed in the activity and pay minimal attention to extraneous thoughts and feelings or to their physical state (Creek 2007). Engagement is not an absolute condition; rather, there are degrees of engagement. Occupational therapists sometimes use the word flow to refer to total absorption in an activity, when performance becomes unconscious and spontaneous (McNulty 2009).
As occupational therapy theory develops, new concepts are identified and new terms coined to refer to them. Many of these terms are prefixed with the word occupational, such as occupational justice (Townsend and Wilcock 2004), occupational balance (Wilcock 2006) and occupational alienation (Wilcock 1998b). This usage highlights the centrality of occupation in all aspects of human life.
People have an occupational nature. This means that we seek to be occupied and that occupation fulfils many functions for us as individuals, including promoting survival and health. However, occupation also has a social dimension. Societies determine how occupations should be performed, which occupations are socially useful or acceptable and what occupations are available to particular groups of people.
Ideally, a wide range of occupations would be available to each person throughout the lifespan, so that an individual occupational profile can be developed through the choices made. However, individual and social factors sometimes combine to block access to an adequate number of occupations, so that the person may experience occupational imbalance, occupational deprivation or occupational alienation (Wilcock 1998b). These concepts draw attention to inequalities between those people who have access to a satisfying, personally enriching range of occupations and those who do not.
Each person engages in many occupations in the course of their life. These fit together in what has been called ‘the framework of a life’ (Bateson 1997, p. 7). Self-care, play and work exist in a balance that is not static but changes at different stages of the life course. People are not pre-programmed to follow a daily routine of activities; they continually make choices about what to do with their time and how to structure their daily routines.
Occupational therapists understand occupational balance as ‘managing [occupation] in a way that is personally fulfilling … and meets role demands (Reed and Sanderson 1999, p. 99). The balance of occupations in a person’s life is determined by personal interests and abilities, social expectations, age, environment and personal circumstances. For example, a professional woman with no children may find that she enjoys a variety of social and sporting activities that keep her fit, relieve the stress of working and enable her to meet people. On the other hand, a single mother with four children and a low-paid job may not have the resources of time, energy or money to engage in a range of leisure activities.
A healthy balance includes a variety of physical, mental and social activities, so that the individual is able to develop and exercise their capacities in all these areas. The balance may also be ‘between chosen and obligatory occupations; between strenuous and restful occupations; or between doing and being’ (Wilcock 2006, p. 343). Each person seeks a balance that is comfortable for them and that promotes health and wellbeing. For occupational therapists, the balanced use of time in daily living activities both influences health and is an indicator of health (Creek 2003).
Occupational balance may be disrupted if a person focuses too much time and energy on one occupational area to the detriment of others, or if they do not have access to enough occupations, so that there are empty times in the day when there is nothing worthwhile to do. The inability to manage occupations in a way that is personally fulfilling and meets role demands is called occupational imbalance and can lead to health and quality of life being compromised (Reed and Sanderson 1999; Christiansen and Townsend 2004). One cause of occupational imbalance is occupational deprivation.
Occupational deprivation is ‘a state of prolonged preclusion from engagement in occupations of necessity or meaning due to factors outside the control of an individual, such as through geographic isolation, incarceration or disability’ (Christiansen and Townsend 2004, p. 278).
Wilcock (2006, p. 164) identified some of the social factors that can lead to people being deprived of access to a broad range of occupations, including ‘technology, the division of labor, lack of employment opportunities, poverty or affluence, cultural values, local regulations, and limitations imposed by social services and education systems, as well as the social consequences of illness and disability’. A recent example of this is the reduction in numbers of public sector jobs in the UK, leading to a massive loss of paid employment in some areas. Compulsory detention in hospital under the Mental Health Act can also lead to occupational deprivation when there is little or no access to activity on the wards.
Whiteford (2004) suggested that when occupational deprivation is a temporary phenomenon, such as during a period of mourning, and when it is due to personal factors, such as a broken leg, it should be called disruption rather than deprivation. Occupational disruption is ‘a transient or temporary condition of being restricted from participation in necessary or meaningful occupations, such as that caused by illness, temporary relocation, or temporary unemployment’ (Christiansen and Townsend 2004, p. 278).
Some occupations are experienced as spiritually and mentally enriching, in addition to having more practical functions. These occupations provide opportunities for choice and individual expression, and often have an element of creativity. Other occupations may be experienced as confining, regimented and lacking in meaning, leading to boredom and alienation. When people experience daily life as lacking meaning or purpose, either because they cannot find anything important to do or because they have to spend all their time and energy on tasks that they do not value, the outcome is occupational alienation (Townsend and Wilcock 2004).
Occupational alienation refers to ‘a sense that one’s occupations are meaningless and unfulfilling, typically associated with feelings of powerlessness to alter the situation’ (Hagedorn 2001, p. 166). Having to spend a lot of time performing occupations that do not enhance, or that diminish, a person’s sense of self can damage personal identity (Townsend and Wilcock 2004).
In its most general meaning, justice is ‘each getting what he or she is due’ (Audi 1999, p. 456). However, several aspects of justice can be differentiated, including:
■ formal justice: the maintenance of legal, social or moral principles by the exercise of authority or power (Shorter Oxford English Dictionary 2002)
■ retributive justice: when and why punishment is justified
■ substantive justice: the rights that people can legitimately claim in relation to each other or what they can demand of their government
■ distributive justice: the fairness of the distribution of resources (Audi 1999).
The term occupational justice mainly refers to substantive and distributive justice because it is based on the belief that people have rights in relation to occupation and that it is unfair to block access to occupation for particular groups of people. The rights underpinning the concept of occupational justice can be summarized as (Townsend and Wilcock 2004):
■ The right to experience occupation as meaningful and enriching
■ The right to participate in occupations for health and social inclusion
■ The right to exert autonomy through choice of occupations
■ The right to benefit from diverse participation in occupations.
Occupational injustice is a social condition that offers unequal access to occupation for different groups in society. Occupational injustice creates societies in which some people have too much to do, while others do not have enough to occupy them (Townsend and Wilcock 2004), often in the area of work, where some sectors of the population are overemployed while other sectors are either underemployed or unemployed. Both over- and under-occupation are examples of occupational imbalance.
The concept of occupational injustice draws attention to the many ways in which participation in occupations can be ‘barred, confined, restricted, segregated, prohibited, undeveloped, disrupted, alienated, marginalized, exploited, excluded or otherwise restricted’ (Townsend and Wilcock 2004, p. 77).
The related concept of occupational apartheid refers to the ‘more or less chronic established environmental (systemic) conditions that deny marginalized people rightful access to participation in occupations that they value as meaningful and useful to them’ (Kronenberg and Pollard 2005, p. 65). This state results from ‘political constraints which may extend to encompass all aspects of daily living and human occupation through legal, economic, social, and religious restrictions, and can be found as a consequence of chronic poverty and inequality’ (Kronenberg and Pollard 2005, p. 66).
Although occupational therapy was founded on a set of beliefs about the occupational nature of people, it is only relatively recently that the profession has begun to formulate its own theories about occupation. Occupational science is the academic discipline that studies people as occupational beings (Yerxa 2000). It brings together knowledge from different fields with the intention of providing a knowledge base in occupation for the practice of occupational therapy.
Occupational science was established in the last decade of the 20th century to promote the study of occupation, develop theories to explain why people choose certain activities over others and explore the complexity of factors that influence why, where and how people decide to live their lives in relation to work, rest and play (Clark et al. 1991). Elizabeth Yerxa, the founder of the first doctoral programme in occupational science at the University of Southern California, claimed that occupational science would ‘address some of the major dilemmas of occupational therapy practice’ (Yerxa 1993, p. 3).
In a relatively short time, occupational science has contributed to the knowledge base of occupational therapy at all levels, from elucidating key concepts, such as occupational alienation (Townsend and Wilcock 2004), through building theories to explain why people choose particular occupations, such as theories of meaning (Primeau 1996), to developing appropriate research methodologies (Carlson and Clark 1991) and carrying out research into the effects of occupation on health (Iwarsson et al. 1997).
The next section discusses some of the ways in which occupational therapy theory is organized for use in practice.
Occupational therapists use theories from a variety of disciplines as well as their own theories of occupation. The breadth of this theoretical base and the complexity of some of the theories used could seem overwhelming. However, not all occupational therapists need to know all the theories that make up the total body of knowledge of the profession. Different theories are used depending on the area of work, the kind of problems encountered most often by the therapist and their own knowledge, skills and preferences.
In this section, we look first at the vocabulary used when talking about theories for practice: frame of reference, approach, model and paradigm. We then look at how the different concepts relate to each other in a theoretical framework.
Theory acts as a guide to practice by offering explanations of what the therapist observes and making it possible to predict the outcomes of interventions. In order to use theory to support clinical and professional reasoning, the therapist has to select appropriate theories and organize them into useful frameworks. Theories that work well together and can be applied within a particular field of practice are organized as frames of reference that, in turn, are translated into practice through various approaches and models.
A frame of reference is an individual’s ‘personal notion of reality, their cultural, social, and psychological biases, their values and beliefs, and how these factors influence the practice of occupational therapy’ (Krefting 1985, p. 175). So, in its widest sense, a frame of reference is the way a person sees the world. Creek (2003, p. 53) offered a narrower definition for occupational therapists: ‘a collection of ideas or theories that provide a coherent conceptual foundation for practice’. Bruce and Borg (1993) wrote that a frame of reference refers to the principles behind practice with different issues. Examples from occupational therapy include the psychodynamic, human developmental and occupational performance frames of reference.
An approach is ‘the methods by which theories are put into practice and treatment is administered’ (Creek 2003), for example, the rehabilitation approach. The terms frame of reference and approach are sometimes used synonymously.
Within occupational therapy, there are many frames of reference and approaches, some of which are appropriate to more than one field and some of which are used for very specific purposes. The choice of a frame of reference or approach is influenced by the presenting problems of the individual, the ethos of the unit where the intervention takes place and the knowledge of the therapist (Hurff 1985).
Frames of reference and approaches describe the principles of practice, enabling therapists to be consistent in their way of working. Models for practice give more guidance to the inexperienced therapist as they suggest a more structured procedure and tools for intervention.
A model is ‘a simplified representation of the structure and content of a phenomenon or system that describes or explains certain data or relationships and integrates elements of theory and practice’ (Creek 2003, p. 55). A model for practice acts as a guide for the practitioner, providing ‘an explanation of clinical phenomena and [suggesting] the type of intervention the therapist should make’ (Feaver and Creek 1993, p. 59). During the 1980s and 1990s, a large body of literature was developed on models for practice in occupational therapy.
The therapist’s methods of intervention, that is, the tools and processes of therapy, are determined by the frame of reference, approach or model being used. For example, projective techniques are tools used for assessment and treatment within a psychodynamic frame of reference.
Another term sometimes heard in connection with the knowledge base of occupational therapy is paradigm, which is used to refer to the particular way in which a profession perceives itself, its relationship to other professions, and its association with the society to which it is responsible. Creek and Feaver (1993) suggested that a paradigm is ‘the profession’s world view that encompasses philosophies, theories, frames of reference and models for practice’.
The profession of occupational therapy began to develop its own theory base during the second half of the twentieth century. The building blocks of theory are concepts, which give us an understanding of a situation through how they relate to each other. For example, when we use a hierarchical system of classification to describe the relationships between occupations, activities and tasks, we understand that occupations are made up of activities, which are made up of tasks, which are made up of actions (Polatajko et al. 2004). Most of the occupational therapy models developed during the past 50 years employed a hierarchical system, called general systems theory, for classifying the relationships between core concepts.
Over the last 20 years, there has been an emerging recognition that organic systems are complex and cannot be fully described and understood through hierarchical systems of classification. One of the key features of a complex system is that the interactions between its components change how the system works. This means that the relationships and interactions between components in the system are more important than their properties. Think about the multidisciplinary healthcare team. Each member of the team is a skilled specialist but the effectiveness of interventions comes from the way that team members work together, not from the skills of individual staff. My role as an occupational therapist changes depending on the skills of other members of the team and on how we negotiate and share out tasks among us.
Complexity is manifested at the level of the system but it results from interactions between adjacent components of the system (Cilliers 1998). Complexity cannot emerge in a system if the interactions between components are preset or prescribed from outside: it occurs because interactions within the system change as circumstances and needs change. In other words, complex systems are adaptive. This feature allows complex systems to learn from experience and to develop new ways of working in response to external demands.
Occupational therapists in Europe have developed a theory of occupational performance that uses complexity theory to explain the relationships between key concepts: the European conceptual framework for occupational therapy (Creek 2010).
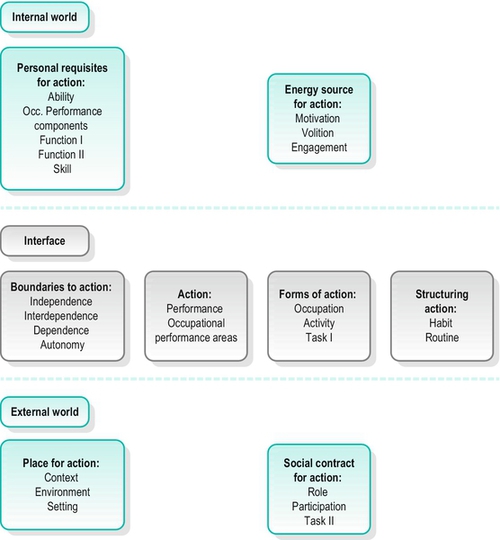
The purpose of the framework is to help the occupational therapist to understand occupation and performance from the service user’s perspective. A conceptual framework is a structure made up of concepts displayed together in a way that shows how they relate to each other and that supports thinking. The European conceptual framework for occupational therapy consists of 25 terms representing 27 concepts (task and function each have two definitions). These terms refer to aspects of occupation, such as engagement and routine (Fig. 3-1).
FIGURE 3-1 European conceptual framework for occupational therapy. Reprinted from Creek J (2010) The core concepts of occupational therapy: a dynamic framework for practice. Reproduced by permission of Jessica Kingsley Publishers.
The terms in the framework are organized into eight clusters, each of which relates to a particular aspect of action. All the terms within a cluster share some of their meanings; for example, setting, environment and context are all terms that refer to aspects of the physical, social and temporal place for action.
The clusters are grouped into three categories: the internal world of the performer; the external world of the performer; and the interface between the internal and external worlds.
■ The internal world of the performer consists of two clusters: the energy source for action, which is the individual’s emotional energy, and the personal requisites for action, which are the personal factors necessary for performance
■ The interface between the internal and external worlds consists of four clusters: the action cluster, which is action by the individual; forms of action, which is how the performer perceives the action; structuring action, which is the ways that actions are organized, and boundaries to action, which are the individual factors that set limits to action
■ The external world of the performer consists of two clusters: the place for action, which is the place where a task, activity or occupation is performed, and the social contract for action, which includes social supports and constraints on performance.
The internal and external worlds of the performer influence what a person does and shape how they perform. We can say that interaction between the internal and external worlds leads to action by the individual.
For the purposes of print, the European conceptual framework for occupational therapy is presented as a static diagram. However, relationships between terms in the framework are not fixed but change depending on the context in which the framework is being used. For example, I worked for 10 years as a freelance occupational therapist. The decisions I made about what jobs to take were strongly influenced by factors such as my role as a single parent and the context of being self-employed, so there were strong relationships between my volition and a range of contextual and social influences in my external world. Since retirement, my decisions about whether to work and what jobs to take are more strongly influenced by such factors as whether I have the up-to-date skills for the job and the extent to which my interest is stimulated: my volition is most strongly linked with other aspects of my internal world.
For more information about how to use the conceptual framework, the reader is recommended to look at the ENOTHE (2006) website or one of the books written by members of the terminology working group (e.g. Creek 2010).
This chapter presented the knowledge base of occupational therapy, including the philosophical assumptions and beliefs held by occupational therapists and the theories that support practice. Emphasis was placed on occupational therapy as a two-body practice that is concerned both with disorders of the body and with the experience of the person. The nature of theory was explored and the content of the occupational therapy theory base outlined. The chapter finished with a description of key occupational therapy theories and how they are organized.
The next chapter looks in more detail at how philosophy and theory are used to inform practice.
Audi R. The Cambridge Dictionary of Philosophy. second ed. Cambridge: Cambridge University Press; 1999.
Bateson MC. Enfolded activity and the concept of occupation. In: Zemke R, Clark F, eds. Occupational Science: The Evolving Discipline. Philadelphia: FA Davis; 1997.
Baum C, Christiansen C. The occupational therapy context: philosophy – principles – practice. In: Christiansen C, Baum C, eds. Occupational Therapy: Enabling Function and Well-Being. second ed. Thorofare, NJ: Slack; 1997.
Breines EB. Occupational Therapy Activities from Clay to Computers: Theory and Practice. Philadelphia: FA Davis; 1995.
Breines E. Origins and Adaptations: A Philosophy of Practice. Lebanon, NJ: Geri-Rehab Inc; 1986.
Bruce MA, Borg B. Psychosocial Occupational Therapy: Frames of Reference for Intervention. second ed. Thorofare, NJ: Slack; 1993.
Carlson ME, Clark FA. The search for useful methodologies in occupational science. Am. J. Occup. Ther. 1991;45(3):235–241.
Christiansen C. Person–environment occupational performance. In: Christiansen C, Baum C, eds. Enabling Function and Well-Being. Thorofare, NJ: Slack; 1997.
Christiansen CH, Townsend EA. An introduction to occupation. In: Christiansen CH, Townsend EA, eds. Introduction to Occupation: The art and Science of Living. Upper Saddle River, NJ: Prentice Hall; 2004:1–27.
Cilliers P. Complexity and Postmodernism: Understanding Complex Systems. London: Routledge; 1998.
Clark FA, Parham D, Carlson ME, et al. Occupational science: academic innovation in the service of occupational therapy’s future. Am. J. Occup. Ther. 1991;45(4):300–310.
College of Occupational Therapists. Code of Ethics and Professional Conduct. London: COT; 2010.
Cracknell E. Humanistic psychology. In: Willson M, ed. Occupational Therapy in Short-Term Psychiatry. Edinburgh: Churchill Livingstone; 1984:73–88.
Creek J. The Core Concepts of Occupational Therapy: A Dynamic Framework for Practice. London: Jessica Kingsley; 2010.
Creek J. Engaging the reluctant client. In: Creek J, ed. Contemporary Issues in Occupational Therapy: Reasoning and Reflection. Chichester: Wiley; 2007.
Creek J. Occupational therapy defined as a complex intervention. London: College of Occupational Therapists; 2003.
Creek J, Feaver S. Models for practice in occupational therapy, part 1: defining terms. Br. J. Occup. Ther. 1993;56(1):4–6.
Dickoff J, James P. A theory of theories: a position paper. Nurs. Res. 1968;17(1):197–203.
Dickoff J, James P, Wiedenbach E. Theory in a practice discipline: part 1. Practice oriented theory. Nurs. Res. 1968;17(5):415–435.
ENOTHE, 2006. Available at: www.enothe.hva.nl.
Feaver S, Creek J. Models for practice in occupational therapy: part 2, what use are they? Br. J. Occup. Ther. 1993;56(2):59–62.
Gillon R. Philosophical Medical Ethics. Chichester: Wiley; 1985/1986.
Hagedorn R. Foundations for Practice in Occupational Therapy. third ed. Edinburgh: Churchill Livingstone; 2001.
Hagedorn R. Tools for Practice in Occupational Therapy: A Structured Approach to Core Skills and Processes. Edinburgh: Churchill Livingstone; 2000.
Hocking C. The romance of occupational therapy. In: Creek J, Lawson-Porter A, eds. Contemporary Issues in Occupational Therapy: Reasoning and Reflection. Chichester: Wiley; 2007:23–40.
Hooper B. Epistemological transformation in occupational therapy: educational implications and challenges. OTJR: Occup., Particip. Health. 2006;26(1):15–24.
Hooper B, Wood W. Pragmatism and structuralism in occupational therapy: the long conversation. Am. J. Occup. Ther. 2002;56(1):40–50.
Hurff JM. Visualization: a decision-making tool for assessment and treatment planning. Occup. Ther. Health Care. 1985;1(2):5–12.
Iwarsson S, Isacsson Å., Persson D, Scherstén B. Occupation and survival: a 25-year follow-up study of an aging population. Am. J. Occup. Ther. 1997;52(1):65–70.
Kielhofner G. A model of human occupation, part 2: ontogenesis from the perspective of temporal adaptation. Am. J. Occup. Ther. 1980;34(10):657–663.
Kielhofner G, Burke JP. Occupational therapy after 60 years: an account of changing identity and knowledge. Am. J. Occup. Ther. 1977;31(10):675–689.
Krefting LH. The use of conceptual models in clinical practice. Can. J. Occup. Ther. 1985;52(4):173–178.
Kronenberg F, Pollard N. Overcoming occupational apartheid: a preliminary exploration of the political nature of occupational therapy. In: Kronenberg F, Algado SS, Pollard N, eds. Occupational Therapy Without Borders: Learning from the Spirit of Survivors. Edinburgh: Churchill Livingstone/Elsevier; 2005:58–86.
McNulty C. The Sleaford MACA group. In: Pollard N, Sakellariou D, Kronenberg F, eds. A Political Practice of Occupational Therapy. Edinburgh: Churchill Livingstone/Elsevier; 2009:171–174.
Mattingly C. Occupational therapy as a two-body practice: the body as machine. In: Mattingly C, Fleming MH, eds. Clinical Reasoning: Forms of Inquiry in a Therapeutic Practice. Philadelphia: FA Davis; 1994a:37–63.
Mattingly C. Occupational therapy as a two-body practice: the lived body. In: Mattingly C, Fleming MH, eds. Clinical Reasoning: Forms of Inquiry in a Therapeutic Practice. Philadelphia: FA Davis; 1994b:64–93.
Meyer, A. 1922/1977. The philosophy of occupation therapy. Arch. Occup. Ther. 1, 1–10. Reprinted in: American Journal of Occupational Therapy 1977; 31(10):639–642.
Mosey AC. Psychological Components of Occupational Therapy. New York: Raven Press; 1986.
Mosey AC. Recapitulation of ontogenesis: a theory for the practice of occupational therapy. Am. J. Occup. Ther. 1968;22(5):426–438.
Nelson DL. Occupation: form and performance. Am. J. Occup. Ther. 1988;42(10):633–641.
Nixon J, Creek J. Towards a theory of practice. Br. J. Occup. Ther. 2006;69(2):77–80.
Paterson CF. Opportunities not prescriptions: the development of occupational therapy in Scotland 1900–1960. Aberdeen: Aberdeen History of Medicine Publications; 2010.
Polatajko H, Davis J, Hobson SJG, et al. Meeting the responsibility that comes with the privilege: introducing a taxonomic code for understanding occupation. Can. J. Occup. Ther. 2004;71(5):261–264.
Primeau LA. Running as an occupation: multiple meanings and purposes. In: Zemke R, Clark F, eds. Occupational Science: The Evolving Discipline. Philadelphia: FA Davis; 1996.
Reed KL, Sanderson SR. Concepts of Occupational Therapy. Philadelphia: Lippincott, Williams & Wilkins; 1999.
Reilly M. Occupational therapy can be one of the great ideas of 20th century medicine. Am. J. Occup. Ther. 1962;16(1):1–9.
Schemm RL. Bridging conflicting ideologies: the origins of American and British occupational therapy. Am. J. Occup. Ther. 1994;48(11):1082–1088.
Serrett KD. Another look at occupational therapy’s history: paradigm or pair of hands? In: Serrett KD, ed. Philosophical and Historical Roots of Occupational Therapy. New York: Haworth; 1985:1–31.
Shannon PD. The derailment of occupational therapy. Am. J. Occup. Ther. 1977;31(4):229–234.
Shorter Oxford English Dictionary. fifth ed. Oxford: Oxford University Press; 2002.
Smith AG. Holistic philosophy and general systems theory: an overview for occupational therapy. J. NZ Assoc. Occup. Ther. 1983;34(1):13–18.
Sumsion T. The client-centred approach. In: Sumsion T, ed. Client-Centred Practice in Occupational Therapy: A Guide to Implementation. Edinburgh: Churchill Livingstone; 1999.
Townsend E, Wilcock A. Occupational justice and client-centred practice: a dialogue in progress. Can. J. Occup. Ther. 2004;71(2):75–87.
Van Olmen J, Ku GM, Bermejo R, et al. The growing caseload of chronic life-long conditions calls for a move towards full self-management in low-income countries. Global. Health. 2011;7:38. Available at: www.globalizationandhealth.com/content/7/1/38.
Watson R. New horizons in occupational therapy. In: Watson R, Swartz L, eds. Transformation Through Occupation. London: Whurr; 2004:3–18.
Watson R, Fourie M. Occupation and occupational therapy. In: Watson R, Swartz L, eds. Transformation Through Occupation. London: Whurr; 2004:19–32.
West WL. A reaffirmed philosophy and practice of occupational therapy for the 1980s. Am. J. Occup. Ther. 1984;38(1):15–23.
Whiteford G. When people cannot participate: occupational deprivation. In: Christiansen CH, Townsend EA, eds. Introduction to Occupation: The Art and Science of Living. Upper Saddle River, NJ: Prentice Hall; 2004:221–242.
Wilcock AA. An Occupational Perspective of Health. second ed. Thorofare, NJ: Slack; 2006.
Wilcock AA. A theory of occupation and health. In: Creek J, ed. Occupational Therapy: New Perspectives. London: Whurr; 1998a.
Wilcock AA. An Occupational Perspective of Health. Thorofare, NJ: Slack; 1998b.
Wilcock AA. The occupational brain: a theory of human nature. J. Occup. Sci. 1995;2(1):68–73.
WHO. International Classification of Functioning, Disability and Health. Geneva: World Health Organization; 2001.
Yerxa EJ. Confessions of an occupational therapist who became a detective. Br. J. Occup. Ther. 2000;63(5):192–199.
Yerxa EJ. Occupational science: a new source of power for participants in occupational therapy. Occup. Sci. 1993;1(1):3–10.
Yerxa EJ. Authentic occupational therapy. Am. J. Occup. Ther. 1967;21(1):1–9.