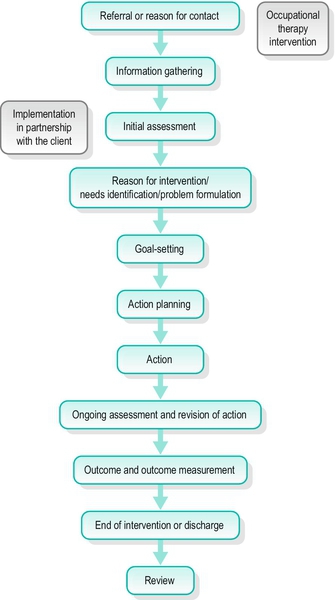
FIGURE 4-1 The occupational therapy process.
CHAPTER CONTENTS
THE OCCUPATIONAL THERAPY PROCESS
On-Going Assessment and Revision of Action
Psychodynamic Frame of Reference
Basic Assumptions About People
Human Developmental Frame of Reference
Basic Assumptions About People
Occupational Performance Frame of Reference
Chapter 3 delineated the knowledge base of occupational therapy, including philosophical beliefs and theories, and introduced the structures that are used to organize that knowledge for practical application: frames of reference, approaches and models for practice. This chapter looks in more detail at how the occupational therapy knowledge base informs and supports practice. The chapter is in three parts. The first part outlines the content of occupational therapy practice, including the goals of intervention, people who might benefit from occupational therapy, legitimate tools for practice, the skills of the occupational therapist and the art of occupational therapy. The second part describes the process by which occupational therapy is delivered. There are a number of stages in this process but it should not be seen as finite or linear: occupational therapy is individualized, iterative and complex. The third part gives examples of occupational therapy frames of reference used in the field of mental health: the psychodynamic, human developmental and occupational performance frames of reference.
Practice can be described as the actions taken by the therapist to serve the needs of the people they work with (Agyris and Schon 1974). A definition of the structure and scope of occupational therapy practice should derive from the philosophical and theoretical base of the profession, not from the constraints and demands of the service setting, although the way an intervention is carried out will be influenced by such external factors. Only if practice is based on a coherent philosophical and theoretical framework can the therapist make skilled predictions about the outcomes of intervention.
We will look at the content of practice under five headings:
■ Populations served
■ Legitimate tools
■ Core skills
■ Professional artistry.
The word outcome refers to two different things: the changes that are expected to occur as a result of intervention, the intended outcomes, and the results of intervention, the actual outcomes. Goals are specific and positive results to be attained by an individual from planned therapeutic interventions. Process goals are the conditions to be achieved during an intervention, such as an individual arriving on time for their sessions. Outcome goals are statements of measurable changes that the intervention is designed to bring about.
Desired outcomes are discussed with those involved before beginning the intervention, often following a baseline assessment to determine the current level of performance and set goals. After an agreed period of intervention, the assessment is repeated. By comparing the assessment results before and after intervention it is possible to see what changes have taken place, that is, to measure the outcomes of intervention. (See Ch. 5 for a detailed discussion of assessment and outcome measurement.) The focus of the intervention is usually agreed jointly, to produce a set of individualized outcome goals. If the overall goal of intervention is likely to take some time to achieve, it can be broken down into a sequence of short-term goals that represent steps to be taken towards reaching the long-term goal. For example, an individual’s long-term goal may be to find full-time, paid employment. If the person has not worked for a long time, a short-term goal on the way to achieving this might be to establish a regular pattern of sleeping at night and waking at the same time every morning.
The occupational therapy premise, that people influence their health by what they do, can be applied to a wide range of problems once the appropriate specialist knowledge and skills to support it have been acquired. Anyone who has problems of doing, whatever the person’s age, gender or diagnosis, could potentially work with an occupational therapist. In practice, occupational therapists work in two main settings: statutory services and the social field.
The occupational therapist traditionally worked with people in a medical setting, which predetermined, to some extent, the range of problems seen, the degree of dysfunction people were experiencing and the amount of time the therapist could spend on intervention. As the profession continued to expand into new areas, people have also been encountered in other settings, such as social services departments, educational settings, health centres, community centres, day hospitals, day centres, prisons, the workplace and people’s own homes. Occupational therapists increasingly work across service boundaries, in partnership with other agencies and other professionals, to provide integrated services (College of Occupational Therapists 2006).
Referrals often come from a doctor or other professional who makes the initial decision about who would benefit from occupational therapy. The occupational therapist accepts referrals on the basis of information gained from the referral and an initial assessment with the person referred. In some settings, such as continuing care units, occupational therapists select people to work with from the unit’s population. In the multidisciplinary team, the decision about which professional should work with a particular individual is usually made by all the team members. An increasing number of people are referring themselves for occupational therapy, in part due to an increase in private practice.
In recent years, occupational therapists have extended their practice into a range of new areas outside mainstream health and social services. A Brazilian occupational therapist, Sandra Galheigo (2005, p. 87), called this ‘the social field’ because occupational therapy, with its humanistic principles and practices, has a significant contribution to make to social affairs.
The movement towards a more socially embedded way of working has been supported by two parallel developments: increased awareness of the contribution that occupational therapy can make to addressing occupational needs not met by hospital-based models of healthcare, and theoretical developments within the profession (Lorenzo 2004; Watson 2004; Galheigo 2005; Wilcock 2006; Crouch 2010; see also Chs 12, 13 and 29).
Galheigo (2005) highlighted the need for an occupational therapy vocabulary ‘to refer to those in need … excluded, marginalized, vulnerable survivors, deviant, under apartheid, disadvantaged, disaffiliated’ (p. 87) that would leave no room for misinterpretations of ‘the phenomenon of inequality’ (p. 88). As described in the last chapter, occupational therapists are developing a new vocabulary, using such terms as occupational imbalance, occupational deprivation (Wilcock 2006) and occupational injustice (Townsend and Wilcock 2004), to describe their professional purpose and goals in terms of occupational needs. This enables them to identify the occupational needs of people who do not necessarily have a medical diagnosis, including those living in chronic poverty, refugees, homeless people or those displaced by natural disasters. Occupational therapists working in these areas take a public health, health promotion and/or community development role, focusing on communities and populations rather than individuals or small groups.
The social field of occupational therapy is discussed further in Ch. 29.
The occupational therapist may use a variety of techniques and media during an intervention. Mosey (1986) described the permissible means of carrying out occupational therapy as the profession’s legitimate tools. These tools are: the self, activities and the environment.
The relationship between the therapist and the client is an important part of the therapeutic process, from first meeting a person who has been newly referred, through coping together with the successes and setbacks of the intervention process, to ending the relationship on a positive note.
Ideally, the therapeutic relationship is a partnership or collaboration between therapist and the client, in which the goals and methods of intervention are negotiated throughout the process. If an individual is unable to take a full part in negotiating the process, because of illness or disability, the therapist has a responsibility to facilitate their involvement as far as possible and to protect their interests to the best of the occupational therapist’s ability (see also Ch. 22).
Mosey (1986) identified 11 elements that contribute to the therapist’s ability to relate effectively to the people they work with:
■ a perception of individuality – recognition of each person as a unique whole
■ respect for the dignity and rights of each individual
■ empathy – ability to enter into the experience of another person without losing objectivity
■ compassion or sympathy – willingness to engage with another person’s suffering
■ humility – recognition of the limits of one’s own knowledge and skill
■ unconditional positive regard – concern for the individual without moral judgements on their thoughts and actions
■ honesty – telling the truth to the people they work with; this is an aspect of being respectful
■ a relaxed manner
■ flexibility – ability to modify own actions to meet the demands of a situation
■ self-awareness – ability to reflect on one’s own reactions to the world and on the effect one is having on the world in any given situation
■ humour – a lightness of approach which, used appropriately, can facilitate the therapeutic process.
Peloquin (1998) described the occupational therapist being with an individual by doing with them, and identified empathy as the most important element of the therapeutic relationship. Empathy involves the therapist turning to an individual in a genuine attempt to make a positive relationship, recognizing both what they have in common and what is unique about the person, entering into their experience, connecting with their feelings and being able to recover from that connection so that the therapist is not damaged by the therapeutic encounter.
The therapist uses interpersonal skills to deal with a whole range of needs, such as engaging the initial interest of someone with a volitional disorder, supporting a bereaved person through the grieving process, helping someone to express difficult feelings appropriately, valuing a person with chronic low self-esteem and helping carers to work out how best to balance their own needs with their caring role. These interpersonal skills can be the most valuable resource in an intervention.
Activities are the means by which each person interacts with the world and the main therapeutic tools used by occupational therapists to bring about changes in an individual’s function and performance. Activity is a flexible and adaptable intervention that can be used with all people in many different contexts to achieve diverse outcomes. The use of activity as a therapeutic tool requires that the therapist has a range of skills for manipulating activity, including analysis, synthesis, adaptation, grading and sequencing.
Activity analysis is the process of ‘breaking up an activity into the components that influence how it is chosen, organized and carried out in interaction with the environment’ (ENOTHE 2006). Activity analysis enables the therapist to evaluate the therapeutic potential of activities and select or design the most appropriate ones for each situation. For example, activity analysis of football reveals that it is socially valued by many young people, so that they are keen to play, and that it makes variable physical and social demands on the players, depending on the position they play. Analysis also shows that five-a-side football uses a smaller pitch and makes less physical demands on the players, making it a more suitable activity for people who are not fully fit.
The therapist selects activities that have the greatest potential to meet the person’s needs, develop their skills and engage their interest. Alternatively, activity components may be combined into new activities (activity synthesis) that will better achieve these goals. For example, a craft activity could be done in a group so that interpersonal demands are added to the other skills required for the performance of the activity.
Activity adaptation means adjusting or modifying the activity to suit the individual’s needs, skills, values and interests. For example, a traditional craft such as macramé could be done with modern materials to produce a modern piece of jewellery that an individual finds attractive.
Activity grading means adapting an activity so that it becomes progressively more demanding as a person’s skills improve, or less demanding if their function deteriorates. For example, walking can be done for longer or over more difficult terrain to increase stamina.
Activity sequencing means ‘finding or designing a sequence of different but related activities that will incrementally increase the demands made on the individual as her/his performance improves or decrease them as her/his performance deteriorates. It is used as an adjunct or alternative to activity grading’ (Creek 2003, p. 38).
These techniques are described more fully in Ch. 6.
People function within human and non-human environments that influence both what they do and how they do it, by providing supports and barriers to occupational performance. For example, living in a town centre provides easy access to shops and other community facilities (support) but means that a person has to travel a long way to their allotment, located on the edge of town (barrier).
A person’s activities are shaped by environmental factors and those activities also change the environment. For example, washing the floor changes the physical environment and visiting a friend changes the human environment. A third aspect that may be changed by activity is the person performing it, who develops skills and abilities as they adapt their performance to suit the environment.
A person’s environment consists of two main elements (Hagedorn 1995):
■ Content – the physical and human elements in the environment
■ Demands – the effect the environment has on behaviour.
For the occupational therapist, a third element is the potential for adaptation of the content and demands of the environment. The goal of intervention may be to enable adaptation to the environment, to adapt the environment to suit the person’s needs and abilities, or to organize a move to a different environment.
When planning and implementing an intervention with an individual, the therapist considers many aspects of the environment: home; working environment; local area and resources; wider living environment, such as the town or geographical location; transport infrastructure; and potential new environments, such as a care home.
The therapeutic encounter always takes place within an environment that can be adapted or manipulated to change its demands and achieve the desired outcomes, whether it is a specialized intervention setting or the home or workplace.
Occupational therapists are characteristically flexible, innovative and responsive to the people with whom they are working and the context within which intervention is taking place. In order to achieve this flexibility, the occupational therapist requires a wide range of skills. Some skills are common to all therapists, whatever field they are working in, for example analysing and adapting activities. Other skills are developed for a specific field of practice. An example of a specific skill is integrated memory training, which is not requisite for every area of mental health practice (see Ch. 19 which is about older people and refers to memory clinics).
Skills that are required by all occupational therapists are called core skills. The College of Occupational Therapists in the UK defined core skills as ‘the expert knowledge and abilities that are shared by all occupational therapists, irrespective of their field or level of practice’ (College of Occupational Therapists 2009, p. 4). These core skills were identified as:
■ Collaboration involves building a relationship with the client in which decisions are shared and actions negotiated. The aim of a collaborative relationship is to promote autonomy and engage the client in the therapeutic process.
■ Assessment is a collaborative process through which the therapist and the client are able to identify and explore functional potential, limitations, needs and environmental conditions.
■ Enablement is the process of helping clients to take more control of their lives, by identifying what is important, setting goals and working towards them.
■ Problem-solving is a process involving a set of cognitive strategies that are used to identify occupational performance problems, resolve difficulties and decide on an appropriate course of action.
■ Using activity as a therapeutic tool involves using activity analysis, synthesis, adaptation, grading and sequencing to transform everyday activities into interventions.
■ Group work involves planning, organizing, leading and evaluating activity groups.
■ Environmental adaptation involves assessing, analysing and modifying physical and social environments to increase function and social participation.
The occupational therapist’s skills are made up of three elements (Creek 2007):
1. Techniques: such as communication, interpersonal and team-working skills, skills and techniques for assessment and therapy, time management and self-management skills. These practical skills are discussed in Chs. 4–8.
2. Knowledge and understanding: including concepts, theories, frames of reference, approaches and models (see Ch. 3).
3. Thinking: including clinical reasoning, decision-making, reflection, analysis and ethical reasoning. These skills are discussed in the next section.
Thinking means using the mind and includes such mental actions as applying rules, choosing, conceptualizing, evaluating, judging, justifying, knowing, perceiving and understanding (Creek 2007). Client-centred practice requires that the occupational therapist is able to process large amounts of information in order to select the most appropriate course of action with an individual, within a specific intervention context, to achieve the best possible outcome. Collecting information and incorporating it into the decision-making process demands a range of thinking styles that the therapist can employ for thinking about different aspects of the intervention.
Sinclair (2007) identified five distinct types of reasoning used by occupational therapists:
■ Evidence discovery is used when the therapist and an individual are trying to frame the individual’s problems and identify what they need to work on. It includes problem sensing, problem formulation and problem definition.
■ Theory application means using both formal theory and personal theory. Task analysis and activity analysis are core skills of theory application, and are described in Ch. 6.
■ Decision-making involves using clinical reasoning (Mattingly and Fleming 1994) to assess, plan, set priorities, predict, evaluate and determine the best approach to use in a particular context.
■ Judgement is reflection by therapists on their practice, leading to recognition of strengths, weaknesses and biases, and of how the views of others might differ from their own. Reflection takes place both during an intervention and afterwards.
■ Ethical reasoning is the process of thinking through ethical issues. It includes recognizing the ethical dimension of intervention, being sensitive to the differing views of others and maintaining personal integrity.
Occupational therapy has been defined as ‘the art and science of directing man’s participation in selected tasks to restore, reinforce and enhance performance’ (AOTA 1972, p. 204). Art is ‘skill as the result of knowledge and practice’ or ‘the application of skill according to aesthetic principles’ and science is ‘a particular branch of knowledge or study’ (Shorter Oxford English Dictionary 2002). This definition identifies occupational therapy as the skilled application (art) of a particular branch of knowledge (science); therefore it is both an art and a science. The skilled application of knowledge to practice requires the occupational therapist to think about what is being done, not just follow rules, guidelines or protocols.
The science of occupational therapy includes theoretical knowledge, research evidence, proven techniques and procedures. Universal theories identify the ‘general systems in which people act, general structures common to all people, and general internal systems of all people’ (Hooper and Wood 2002, p. 43). They can be learned from textbooks and lectures and serve several important functions for the occupational therapist:
■ They set out what constitutes a normal range and performance of occupations for a person from a particular cultural and social background at each stage of life
■ They explain how a health condition can affect an individual’s function and impair their ability to engage in activities and occupations
■ They offer ways of understanding of how an imbalance of occupations can adversely affect the health of individuals and communities.
The art of occupational therapy consists of principles, values, contextual knowledge, thinking skills, interpersonal skills and practical skills. Contextual knowledge is not universal but is specific to particular people, at particular times, in particular settings. It includes the individual’s social circumstances, educational experiences, employment, cultural background, personal beliefs and values, relationships, skills, abilities, habits, interests, needs, aspirations and social roles, and how all of these influence their occupations and activities. Contextual knowledge also includes the living environment, family, neighbourhood, workplace, financial situation, social networks and support systems, and how these support or inhibit occupations and activities. Contextual knowledge cannot be found in books but is gained through working with people in their own life world contexts.
The occupational therapist applies formal theories, research evidence, techniques, skills and contextual knowledge when working out the best way forward for an individual at a particular time and place. The science of occupational therapy enables an occupational therapist to think about the implications of the individual’s health condition, the extent to which their occupational performance meets their own and society’s standards, what frame of reference or approach might be most helpful and what actions the occupational therapist could take to bring about positive change. The art of occupational therapy lies in how this understanding is translated into action.
Through experience, the therapist gains both contextual knowledge about the worlds of the people they work with and practical knowledge of how occupational therapy works. Theoretical and contextual knowledge involve knowing that something is so; practical knowledge means knowing how to do something (Dreyfus and Dreyfus 1986). Knowing how is part of the art of occupational therapy. Artful practitioners know how to:
■ talk appropriately to colleagues and clients, put nervous people at ease and match the moods of others by adjusting their tone of voice
■ engage people in activities that will help them to develop skills to support their occupational performance
■ provide aids or other forms of support and adapt environments to enable occupation
■ manage their time and avoid unhealthy levels of stress.
Occupational therapy is a process in the sense that change takes place over time. Life itself is more usually experienced as a process rather than as a series of steps or goals to be achieved. In many cases, going through the therapeutic process can be more important than reaching the original goal of an intervention.
Occupational therapy is also a process in that the therapist’s actions follow a recognisable sequence. Mosey (1986, p. 9) said that ‘Principles for sequencing various aspects of practice refer to the way in which a profession goes about the process of problem identification and proceeds through to problem solution relative to assisting the client’. There is an accepted first step to occupational therapy intervention, followed by a logical second step, and so on.
There is general agreement on the steps that make up the occupational therapy process, although not all the steps are carried out in every case. For example, in some settings the occupational therapist does not go through the whole process but merely assesses an individual and passes the results to others to carry out the rest of the intervention. For the novice therapist, the occupational therapy process may appear to be linear but the experienced practitioner uses it in a flexible and iterative way to suit the individual and the context of the intervention.
The 11 steps of the occupational therapy process are shown in Figure 4-1. Two of these steps may be carried out by the therapist alone, often before meeting the person they are working with, and nine of them take place in collaboration with the individual. The occupational therapy process is outlined here but more details can be found in Chs. 5 and 6.
FIGURE 4-1 The occupational therapy process.
Occupational therapists come into contact with the people they work with through various routes. In some settings, the therapist sees only those people who are referred to the service or identifies potential people to work with during team meetings. Many therapists usually see everyone who is admitted to the service and make their own decisions about whom to work with. Some therapists work in drop-in centres or other settings where there is no formal system of referral.
Depending on the setting, the therapist may or may not receive useful information about an individual before meeting them. Whether or not there is a formal referral, the therapist will want to know certain things about an individual before making a decision about whether or not to intervene.
Certain information is necessary for the therapist to determine whether the referral is appropriate or if someone will benefit from occupational therapy intervention. If it is decided that the referral is not appropriate, the referring agent is informed of the decision and the reasons for it.
The type of information sought includes the person’s medical history and presenting problem, social history and present social situation, educational and work history, current work status, reason for referral to occupational therapy, other services involved and any risk factors. This information may be gleaned from case notes, other staff, the referring agent, family, carers and the person concerned.
If the referral seems appropriate and the therapist judges that the person or people might benefit from occupational therapy intervention, an initial assessment is carried out.
Assessment is the basis for all intervention and must be both thorough and valid in order to ensure that intervention is appropriate. Assessment is in two stages, the initial screening assessment and more focused assessment.
Assessment begins from the moment a referral is received or the therapist starts to identify those people who could benefit from occupational therapy. The initial assessment is a screening process to determine the main areas of needs of the individual and whether or not occupational therapy can be of any value at this time. Factors influencing whether or not a referral is accepted include:
■ the individual’s goals, expectations and views about occupational therapy
■ the resources available, including manpower and expertise
■ the individual’s personal support systems and social networks
■ the reason for referral
■ the intervention contract.
Once a referral is accepted, a more focused assessment is carried out to determine the person’s needs, strengths, interests and goals. Effective assessment leads directly to setting measurable goals or defining expected outcomes of intervention and to choice of intervention methods. It also establishes a baseline from which change can be measured.
There may be no clear division between assessment and intervention in occupational therapy, where people are often assessed through observation of their participation in activities, which also have therapeutic value. (This is explained in more detail in the Chapter 5.) However, at some stage the therapist and the person they are working with begin to formulate problems, establish goals and agree on a plan of action.
People are complex and it is usually possible to formulate their problems or needs in different ways, each of which will indicate an alternative approach to intervention. For example, a woman with a diagnosis of severe depression may be experiencing low mood, suicidal ideation, fatigue, poor self-esteem, delusions about her body, loss of appetite, insomnia and agitation. If her problem is formulated as a biochemical imbalance, the main focus of intervention will be to remediate this with antidepressant medication. If her problem is seen as the result of faulty thinking, the object of intervention will be to provide her with cognitive strategies for managing her condition. The occupational therapist is more likely to formulate her problem in terms of activity limitation and restricted participation, so that intervention will focus on achieving a more healthy range and balance of activities.
The occupational therapist formulates the desired outcomes of intervention as goals (the individual will return to work), problems (the individual is too tired to get up in time for work) or needs (the individual needs to re-establish a normal sleep pattern). The way that problems are formulated influences the actions that are taken to achieve desired outcomes.
In person-centred practice, the therapist and the person they are working with negotiate and agree the goals of intervention. Goals are the desired outcomes of the intervention. An actual outcome is the extent to which goals have been met following the intervention. Outcome goals can be expressed on different levels (Creek 2003):
■ Adapting to fixed deficits, for example, the goal for a person who has developed a serious hearing impairment might be to read a newspaper every morning instead of listening to the news on the radio
■ Developing skills, such as learning to read
■ Carrying out tasks, such as putting aside the money to buy a newspaper every day
■ Engaging in activities, for example, walking to the shop to buy a newspaper every morning
■ Performing occupations, for example, keeping abreast of current affairs by reading the newspaper every day
■ Participating in life situations, for example, reading the newspaper every morning and discussing the news with a group of friends.
A review date is set at the time when the goals of intervention are set. This is the date when measurement occurs. The more precisely a goal is defined the easier it will be to measure when it has been reached.
An individual may want to achieve several outcomes, in which case it will be necessary to decide which ones to work on first. When an individual is too unwell to express a view about what the priority should be, the therapist has to make a decision about initial goals. If possible, this should be discussed with colleagues, family and carers.
Once problems have been identified and priorities agreed, it is necessary to plan what approach to use and what actions are needed to achieve the desired outcomes. The preliminary action plan should be formulated by the therapist and the individual together, depending on the person’s capacity for contributing to the process at this stage. Other significant people, such as carers, may also be involved.
The action plan includes the goals of intervention or desired outcomes, methods to be used, an individual programme and a list of the people who need to be informed about the programme. Occupational therapy interventions are usually designed to meet several goals or achieve several outcomes.
In person-centred practice, each programme of intervention is highly individualized. Factors taken into account in drawing up the intervention plan include:
■ the person’s needs, values and preferences
■ the person’s circumstances and environments, including social circumstances
■ the therapist’s style of working and preferences
■ the quality of the relationship between the therapist and the person they are working with
■ the intervention setting, including resources available and what is expected of the therapist
■ the evidence base for intervention
■ local and national policies and standards.
Most occupational therapy interventions involve partnership working with other professionals, carers, community workers or volunteers. As far as possible, the therapist negotiates what action to take and how the results can be interpreted so that the person involved in occupational therapy shares control over the process (Creek 2003).
Occupational therapy intervention usually involves engaging individuals in activity. The therapist may engage in activity with them or they may discuss activities that individuals carry out elsewhere. For example, a person may attend a cookery group run by the therapist or decide to join a cookery class at their local college.
There is an element of risk in all occupational therapy interventions and respecting an individual’s choices can seem particularly alarming, especially for the inexperienced therapist. Assessing and managing risk is an essential aspect of intervention (see Ch. 5 for further discussion of risk assessment).
The occupational therapist remains responsible for the people they work with when they delegate interventions to others, such as students or support workers. This includes ensuring that they only delegate tasks to those who are competent to carry out the procedures and provide sufficient direction or supervision (Creek 2003).
An individual’s progress is continually monitored, both during intervention sessions and over time, in order to measure progress towards agreed goals and ensure that the intervention is being effective. Collaboratively, the therapist discusses and agrees modifications to the programme in response to assessment findings. Minor changes can be agreed without having to organize a full review or alter the action plan.
Throughout the process of intervention, a close liaison is maintained with other disciplines involved so that any changes or problems can be shared. If the setting allows for a long period of intervention, regular reviews are held to evaluate the need for more radical programme changes. Clear and regular records of intervention sessions are kept to assist in the review process (see Ch. 7). Review meetings serve several purposes:
■ They give the therapist and the team an opportunity to review what progress has been made and to judge the success or otherwise of the intervention programme
■ They give everyone involved in intervention an update on the person’s progress. Review meetings may be multidisciplinary, in which case everyone has a chance to discuss the person’s progress, they may be within the occupational therapy team, or they may be between a single therapist and the individual
■ They provide opportunities to set new short-term goals and to adjust intermediate and long-term goals in the light of new information or changes in the individual’s circumstances.
Change is measured by comparing the results of assessment following intervention with the baseline assessment. There are four possible results of intervention:
■ the expected outcome is achieved
■ the outcome falls short of what was expected
■ the outcome is better than expected
■ the individual’s performance is worse than before the intervention.
If the expected outcome has been achieved, the therapist and the individual involved may set new goals or, if they feel that enough has been done, the discharge procedure may be started. If goals have been partially met, then the intervention programme may be upgraded. If goals have not been met or the individual’s performance has deteriorated, then goal setting and action planning may have to be revisited.
Planning for the end of an occupational therapy intervention should take place from the moment a referral is received or the therapist first starts working with an individual. If a person has been in hospital, or other place of residential care, discharge is planned so that their resettlement takes place as smoothly as possible.
Ideally, everyone involved recognizes when goals have been reached or outcomes achieved, and agrees on the best time for the intervention to end. However, it is not always possible to reach agreement between an individual, the multidisciplinary team and any care-givers, so compromises have to be made. This may involve some form of follow-up so that an individual does not experience the termination as too abrupt.
Reviewing and evaluating interventions and services is a way of safeguarding standards and ensuring that services are fit for purpose. Evaluation is essential to demonstrate the effectiveness of intervention for the person involved, the therapist, the referring agent and other interested parties. Evaluation should be a part of the whole occupational therapy process, through self-appraisal, professional supervision, peer review and feedback from service users. Formal evaluation of a particular aspect of the service, such as a group, or of the service as a whole may be carried out at intervals in the form of an audit. Clinical audit is discussed in more detail in Ch. 7.
Evaluation of services should be carried out by occupational therapists themselves against their own standards of performance. Such evaluation may lead to: changes in skill mix in a service; a request for improved resources; restructuring the service, or a complete change of focus, such as relocating staff from specialist community teams to primary care.
In Ch. 3, a frame of reference was defined as: ‘a collection of ideas or theories that provide a coherent conceptual foundation for practice’ (Creek 2003, p. 53). As the knowledge base of occupational therapy has expanded, theories have been organized into an increasing number of frames of reference, approaches and models.
In 1946, a textbook on the theory of occupational therapy (Haworth and MacDonald 1946) described one approach to therapy (rehabilitation) and offered one chapter on occupational therapy in the treatment of mental disorders, which focused on engaging patients in activities to improve or maintain health. In 2008, the 4th edition of this book referred to eight frames of reference used in occupational therapy for mental health: psychodynamic; human developmental; cognitive behavioural; occupational behaviour; health promotion; cognitive; rehabilitative and occupational performance (Creek 2008). New developments in theory and practice may result in further frames of reference being developed in the future, such as a community development frame of reference.
A frame of reference delineates the field and the theoretical base for practice while a model gives more precise directions for putting theory into practice. Some models for practice are associated with more than one frame of reference. For example, Cole’s seven steps, which are a model for group leadership, draw on elements of the person-centred, the cognitive behavioural and the developmental frames of reference (Cole 2012). Other models draw their theory from a single frame of reference: for example, adaptation through occupation (Reed and Sanderson 1992) developed within the occupational behaviour frame of reference. Table 4-1 shows eight frames of reference and examples of models that are associated with them.
TABLE 4-1
Frames of Reference Used in Mental Health Occupational Therapy
| Frame of Reference | Example of a Model for Practice | Reference |
| Psychodynamic | Occupational therapy as a communication process | Fidler and Fidler 1963 |
| Human developmental | Recapitulation of ontogenesis | Mosey 1968 |
| Cognitive behavioural | Cognitive therapy | Beck 1976 |
| Occupational behaviour | Model of human occupation (MOHO) | Kielhofner and Burke 1980 |
| Health promotion | Transtheoretical model | Prochaska and DiClemente 1983 |
| Cognitive | Functional information-processing model (cognitive disability) | Allen 1985 |
| Rehabilitative | Recovery | Deegan 1988 |
| Occupational performance | Canadian model of occupational performance and engagement (CMOP-E) | Townsend and Polatajko 2007 |
Note: Original references have been given to highlight the sequence of development of the models for practice. There have been more recent developments and publications on all these models because they are still in use by occupational therapists.
Three frames of reference are introduced here: psychodynamic, human developmental and occupational performance. Each frame of reference is described in terms of seven characteristics:
■ basic assumptions about the nature of people
■ the knowledge base
■ how function and dysfunction are conceptualized
■ how change occurs
■ the client group
■ goals of intervention
■ techniques for assessment and intervention.
In the 1950s, a psychiatrist and a psychologist at McGill University carried out a partial survey of psychiatric occupational therapy in Canada (Azima and Wittkower 1957). They concluded that ‘too much emphasis has been put upon the diversional and occupational aspects of activities to the neglect of psychodynamic problems of the individual receiving occupational therapy’ (p. 1). Two years later, one of them published a paper outlining a theory of occupational therapy based on object relations theory (Azima and Azima 1959). This work was taken up and expanded by Fidler and Fidler (1963) in their book Occupational Therapy: A Communication Process in Psychiatry. These publications represented the first systematic attempts by occupational therapists to develop their own knowledge base for practice in the field of mental health.
Since the 1980s, psychodynamic theory has almost disappeared from the occupational therapy curriculum in many countries, although it is still included in some textbooks (Atkinson and Wells 2000; Blair and Daniel 2006) and a new textbook was published in 2013, discussing the place of psychoanalysis as a theory and method within occupational therapy (Nicholls et al. 2013). It is important to keep psychodynamic theory in the occupational therapy knowledge base because ‘psychodynamic theory is one of the few occupational therapy (OT) approaches that deals effectively with emotional issues’ (Cole and Tufano 2008, p. 255).
Psychodynamic theory and approaches developed from the work of Sigmund Freud and his followers. Freudian thinking views people as having both a conscious and an unconscious mind. Behaviour is largely influenced by material in the unconscious mind, therefore people are usually not aware of why they act in particular ways and their actions are not always under conscious control. Actions are taken to gratify needs, but not necessarily those needs of which the individual is consciously aware.
People have an innate drive to be active that is directed towards gratifying needs and making satisfactory relationships. Action is used to express and communicate feelings and thoughts. Action arises from mental images, and feedback about the results of action allows these images to be modified to match external reality.
The infant strives for competence in actions that will both meet the infant’s needs and increase their sense of personal identity and integrity. A sense of self-worth comes from intrinsic satisfaction in doing well in the areas of life that the infant values. The more situations and actions the child is able to experience, the greater will be their knowledge of their own potential and limitations, leading to greater adaptability. Knowledge of what patterns of action are most useful and acceptable in the individual’s culture is learned through interaction with the social environment.
A number of different psychodynamic theories evolved, as many of Freud’s followers developed their own approaches to psychotherapy. The occupational therapist working within a psychodynamic frame of reference will have knowledge and understanding of:
■ Psychoanalytic theory
■ Psychopathology
■ Group dynamics
■ The symbolic meaning and potential of activities and materials
■ Object relations theory.
A recent edition of a standard text on group dynamics in occupational therapy (Cole 2012, p. 129) suggested that the psychodynamic frame of reference also encompasses ‘concepts from ego psychology, humanism, and human spirituality’.
The psychodynamic approach is concerned with both intrapersonal aspects of the person, that is how the individual relates to him/herself, and interpersonal aspects, how individuals relate to other people (Atkinson and Wells 2000). For the occupational therapist, a third dimension is how the individual relates to activity, using activity to create her/himself, express him/herself and interact with objects in the world.
The term ‘object relations’ refers to the investment of emotions and psychic energy in objects for the purpose of satisfying needs …. Objects are any human being (including the self), abstract concept, or non-human thing which has the potential for satisfying needs or interfering with need satisfaction.
(Mosey 1986, p. 55)
Objects have both actual meanings and symbolic meanings. For example, a woman wraps a woollen shawl over her coat in winter when she is using public transport, because it keeps her warm. This is the real and practical meaning of the shawl. But it also creates a symbolic barrier between her and the distracting environment of public transport. This is part of the shawl’s symbolic meaning and value for her.
Symbols play a part in ‘connecting the inner life and the consciousness of the individual with the collective belief systems of his or her culture’ (Fine 1999, p. 13). Hence, symbolism can be used by the therapist as a route to understanding the meaning that activities have for individuals and how they use them to relate to their human and non-human environments.
People may use activity, without being consciously aware that they are doing so, as a way of managing the turmoil caused by ‘their connection to (reliance on) others’ (Nicholls 2007, p. 60). Engaging in activity can be an effective coping mechanism but, without self-awareness, we ‘may work too hard, spend too much time in the gym or in the bar, become obsessively interested in our weight or use our hobbies as the main source of pleasure in our lives’ (Blair and Daniel 2006, p. 244). This can lead to occupational imbalance.
There are several ways of conceptualizing dysfunction, depending on which theory is being used. For example, in Freudian theory, the ego has to balance the conflicting demands of reality, the id and the superego. Conflicts that are not dealt with as the individual grows and develops may be retained in the unconscious mind and surface as anxiety. The ego defends against anxiety by employing ego defence mechanisms. These use psychic energy so that it is not available for other uses. Dysfunction occurs when the individual is unable to contain the anxiety, because the conflicts are too great or ego defence mechanisms are not working effectively, and material from the unconscious interferes with function.
In object relations theory, as applied to occupational therapy, a functioning individual is one who has an integrated self-identity and a realistic concept of others, who continues to grow and develop throughout their life, who is able to satisfy their own basic needs and who contributes to the welfare of others. A well-organized personality has a positive and realistic sense of self and good object concepts. Dysfunction is characterized by immature object relationships which may be the result of a failure to develop healthy object-concepts or may be due to psychopathology and regression (Fidler and Fidler 1963). For example, people experiencing psychological disorganization in severe psychosis may have difficulty recognizing themselves as separate from others.
If dysfunction arises from unresolved conflicts located in the unconscious mind, change can be initiated by bringing these conflicts into the conscious mind to be verbalized and shared. Once the difficult or painful material has been accessed, the therapist can help the client to find alternative ways of coming to terms with the feelings it arouses or dealing with it in a more adaptive way. Alternatively, the therapist may decide not to engage in exploration of the unconscious mind but deal with anxiety by supporting the client’s existing coping mechanisms or finding alternative ways of gratifying needs.
Mosey (1986) pointed out that resolution of conflicts does not necessarily lead to a person spontaneously learning the skills needed for successful functioning. A psychodynamic approach may have to be used in conjunction with, or followed by, a more pragmatic approach to facilitate the acquisition of these skills.
The psychodynamic approach is appropriate for use with people of all ages and for treating a wide range of psychosocial disorders. It has perhaps been most widely used with adults and adolescents with acute disorders but is also appropriate in child and family work, palliative care and substance abuse (Blair and Daniel 2006). Traditional forms of psychotherapy require good verbal skills but occupational therapists can use non-verbal media, such as paint or music, to facilitate expression and communication in people who lack verbal ability.
There are two main approaches associated with this frame of reference, each of which is associated with different goals. An explorative approach assumes that the content of the unconscious can best be dealt with by bringing it into the conscious mind where it can be shared and examined. The client then has the opportunity to find more adaptive ways of resolving conflicts and accepting difficult or painful feelings.
A supportive approach aims to keep unresolved conflicts and painful feelings hidden in the unconscious mind and to strengthen the client’s ego defence mechanisms so that material does not leak into the conscious mind and cause problems.
Whichever approach is used, the goals of intervention may be to:
■ assist in finding ways to gratify frustrated basic needs
■ reverse psychopathology
■ provide conditions for normal psychosexual and psychosocial development
■ facilitate the development of a more realistic view of the self in relation to action and to others
■ help to build a more healthy and integrated ego.
Within a psychodynamic frame of reference there may be no clear distinction between assessment and intervention. The activities that help to bring unconscious material into the conscious mind allow for a clearer understanding of underlying conflicts while at the same time beginning the process of resolving those conflicts. The client’s progress is apparent in the way they respond to the activities provided as interventions.
Examples of assessment tools used within this frame of reference include the meaning of objects interview (Fidler 1999a), the Azima battery (Azima 1982) and observation of relationships in groups (Finlay 2002).
In both supportive and explorative approaches, the therapeutic elements of occupational therapy include: actions of the client; objects used in, or resulting from, action; human and non-human environments, and interpersonal relationships. Activities are selected for their symbolic potential as well as their potential to provide an appropriate level and type of social interaction. Activity analysis is in terms of the psychodynamics of activity, the symbolic potential of materials and actions, interpersonal aspects and sociocultural significance (Fidler 1999b). The choice of activities may be made by the therapist or client, depending upon their needs. However, the client has to be an active participant in the therapeutic process if it is to be of value to them.
During intervention, close liaison with other team members is essential and supervision is always part of the process (Blair and Daniel 2006). Intervention planning takes account of the amount of support and structure available to the therapist, as well as the support available to the client outside of intervention sessions.
Intervention may be individual or in groups but the group should always be small enough to allow the clients to relate closely to everyone in it: 8–10 members is usually considered to be the optimum size.
A supportive psychotherapy group would aim to:
■ provide opportunities for mutual support
■ provide a forum for exchanging information about resources
■ provide a place to air problems
■ help to relieve anxiety
■ give opportunities to consider new ways of dealing with problems.
Explorative psychotherapy was traditionally a talking therapy, either one-to-one or in small groups. Occupational therapy has contributed activity to the process, with the use of the creative arts as ego-explorative activities (Blair and Daniel 2006). This involves:
■ the presentation of stimuli to which participants can respond with feelings or thoughts (e.g. a piece of music or a poem), or
■ the creation of a piece of work through which participants can express feelings or thoughts (e.g. a painting or a piece of free clay modelling).
At the beginning of the 21st century, few occupational therapists are working solely within a psychodynamic frame of reference. However, knowledge of psychodynamic theories and processes can deepen the therapist’s understanding of how people relate to activity, and to the world through activity, and so enhance any therapeutic approach.
The human developmental frame of reference, also known as the lifespan development frame of reference (Bruce and Borg 1993; Cole and Tufano 2008), fits comfortably with the temporal perspective taken by occupational therapists. The two names mostclosely associated with this approach in occupational therapy are Anne Cronin Mosey and Lela A. Llorens.
Mosey’s (1968) paper Recapitulation of ontogenesis: a theory for the practice of occupational therapy outlined a developmental model that can be used in the field of mental health. She subsequently expanded and developed the model, drawing out general principles of a human developmental frame of reference.
Llorens (1970) gave the 1969 Eleanor Clarke Slagle lecture, entitled Facilitating growth and development: the promise of occupational therapy. In this lecture, she outlined a framework for intervention based on developmental theory, which had grown out of her work in the fields of psychiatry, paediatrics and community health. This was followed by a series of publications expanding and clarifying the frame of reference and exploring aspects of its application.
This outline of the human developmental frame of reference draws on the work of both Mosey and Llorens, as well as on the work of more recent occupational therapy theorists such as Fortmeier and Thanning.
People are dynamic, developing organisms whose lives go through predictable stages of growth and decline that necessitate adaptation by the individual. Development can be thought of as a process in which the key elements are the individual, society and the person’s own activity (Fortmeier and Thanning 2002). It takes place in a sequence that is common to everyone, although the pace may vary widely. Developmental achievements are not necessarily permanent: regression to an earlier level can occur.
Although it is possible to identify the average age at which someone might reach a particular developmental stage, there is a wide variation between individuals and across cultures. People develop at different rates, they encounter different environmental opportunities and barriers and their ‘development can be understood only in light of the cultural practices and circumstances of their communities’ (author’s emphasis, Rogoff 2003, pp. 3–4). Age ranges can be suggested for particular skills to be mastered but these are not absolute and are mainly useful for checking whether development in all skill areas is proceeding at the same pace.
Each stage of development can only proceed normally if the preceding stages have been completed successfully and the conditions for further development are in place. Incomplete development in one area of skill, or in one life stage, will influence subsequent development. Early patterns of development influence the personality structure of the adult but growth and development continue into adulthood and middle age. Maladaptive or incomplete development can be remediated at any age by recapitulating earlier developmental stages (Mosey 1968).
Llorens (1970) based her model of human growth and development on 10 premises:
1. A person develops in parallel the areas of neurophysiological, physical, psychosocial and psychodynamic growth, social language, daily living and sociocultural skills
2. All these areas continue to develop throughout the person’s life
3. Mastery of skills to an age-appropriate level in all areas of development is necessary to the achievement of satisfactory coping behaviour and adaptive relationships
4. Such mastery is usually achieved naturally in the course of development
5. Intrinsic factors and external stimulation received within the family environment interact to promote early growth and development
6. The later influences of the extended family, community and social groups assist in the growth process
7. Physical or psychological trauma can interrupt the growth and development process
8. Such interruption will cause a gap in the developmental cycle resulting in a disparity between expected coping behaviour and the skills necessary to achieve it
9. Occupational therapy can provide growth and developmental links to assist in closing the gap between expectation and ability through the skilled application of activities and relationships
10. Occupational therapy can provide growth experiences to prevent the development of maladaptive behaviour and skills related to insufficient nurturance.
The developmental frame of reference is based on theories of human development covering all skill areas: physical, sensorimotor, intellectual, language, psychosocial, psychosexual, moral and spiritual development. The knowledge base draws on the work of such developmental theorists as Piaget, Erikson, Kohlberg, Levison, Havighurst and Gesell (Bruce and Borg 1993; Cole and Tufano 2008).
Activity theory contributes an understanding of how people develop skills through four levels, in interaction with the environment (Fortmeier and Thanning 2002):
■ Functions are the motor and sensory requisites for action, such as muscle tone, perception and sensory-motor coordination.
■ Operations are the procedures through which functions are translated into action; for example, putting on a shirt is an operation. The more operations a person can perform, the greater will be their range of occupational choices.
■ Activity includes: general abilities, such as setting goals; theoretical abilities, such as having knowledge and skills in a particular subject, and social abilities, such as collaborating with others.
■ Consciousness of the world and of one’s own place in it enables people to develop a sense of identity and gives them the capacity to assume responsibility for their own lives.
Different aspects of developmental theory may be used with different client groups. For example, the occupational therapist working with children with learning difficulties may draw on knowledge of language, cognitive, emotional, psychosexual, social and sociocultural development. If the child has multiple impairments, the therapist may also draw on knowledge of sensorimotor and perceptual development. The therapist working with adults in an acute psychiatric setting may use theories of personality, emotional, moral, psychosexual, psychosocial, social and sociocultural development.
Function and dysfunction exist on a continuum. A functioning individual is one who achieves satisfactory coping behaviour and adaptive relationships by developing appropriate skills, abilities and relationships throughout the lifespan. These adaptive behaviours allow the individual to adjust to both internal needs and external demands.
Growth and development can be disrupted or delayed by congenital or acquired disease or injury, or if the conditions for normal growth and development are absent. Dysfunction occurs when the developmental level of the individual, in any area, is unequal to the age-related demands made on them. Some of these expectations are for skills common to all people, such as walking by a certain age, while others are culturally determined, such as social skills. Dysfunction can also occur when the person fails ‘to resolve the dilemmas, conflicts, or polarities appropriate for one’s stage of life’ (Cole and Tufano 2008).
Trauma at any age can interrupt the developmental process and inhibit the development of adaptive skills or cause regression to an earlier developmental level. A major disruption in any one skill area affects all other areas, and the longer the disruption continues the more gaps there will be in the developmental process. However, people may complete a delayed developmental stage at a later time, when the conditions are right, or may compensate for developmental delay by learning certain higher-level skills without the underpinning of more basic ones (Mosey 1986).
Change occurs through learning new skills (Cole and Tufano 2008). As the individual’s physical and psychological needs change, and new environmental demands are encountered, the person experiences disequilibrium. This motivates them to learn the skills needed to re-establish a state of equilibrium. When internal or external change happens unexpectedly, or proceeds too quickly, disequilibrium can be experienced as stressful; however, change is not in itself a problem and disequilibrium is a necessary aspect of adaptation (Bruce and Borg 1993).
New skills are acquired through practice in a facilitating environment until competence is achieved. Once a basic skill has been learned, the individual refines and elaborates it through use. During normal development, skills are learned in parallel so that higher-level skills are integrated with lower-level skills in the same area and with other skills areas developing at the same time. If higher-level skills are not integrated with more basic ones, they may be lost when the individual is under stress, causing regression to an earlier level of development.
Occupational therapists are concerned with promoting development at all ages; therefore this frame of reference is applicable throughout the lifespan. It can be used with people experiencing any kind of mental health problem, as well as those with delay in physical, emotional or cognitive development.
The occupational therapist uses activities and relationships to facilitate growth and development. The overall goal of intervention is to increase skills in all areas, with emphasis being placed on the main area of deficit so that the gap is narrowed or closed between expected coping behaviour for the individual’s chronological age and actual adaptive ability. Short-term goals are to learn the skills needed for the next stage of development.
Occupational therapy is also concerned with maintaining health and preventing maladaptation through early detection of problems and early intervention. This allows the individual to continue the growth process with a minimum of disruption or maladaptation. Intervention may be particularly effective in helping people adapt to change at times of transition, such as starting a family or retiring (Cole and Tufano 2008).
The individual’s developmental level in the different skill areas is assessed to find where normal development has been disrupted or has ceased. Appropriate assessment methods include interviews, observation, review of records, projective techniques, tests and collaboration with care givers.
It is necessary to meet an individual’s needs at their present developmental level if further development is to take place, so intervention takes the person’s present level of development as the starting point (Llorens 1970). However, it is also possible to continue development in some skill areas when the development of other areas is blocked. For example, a person with a learning disability may develop good interpersonal skills despite having limited intellectual ability.
Activity theory (Fortmeier and Thanning 2002) tells us that each person has an actual developmental level, which determines what can be performed independently, and a potential developmental level, which is the area in which further learning can take place. The distance between the actual and potential developmental levels is called the zone of proximal development (ZDP). A person can perform tasks in the ZDP with support from others.
Skills are developed most effectively through performing activities (Fortmeier and Thanning 2002) so that basic functions, such as attention and listening, become integrated in performance. It is important for the occupational therapist to take the individual’s ZDP as the starting point for selecting therapeutic activities in order to present demands that slightly exceed the person’s abilities. If the demands of the activity are too easy, the individual will not learn new skills and will lose interest. If the demands are beyond the individual’s ZDP, she or he will become discouraged and defensive.
If development has proceeded unevenly so that one or more skill areas lag behind the others, then intervention usually starts with the area where development is most delayed. When that area has caught up, attention is transferred to the next most delayed area so that development across the skill areas proceeds relatively evenly. Intervention continues until the individual has attained an age-appropriate level of adaptive skill in all areas, or has attained sufficient skill to be able to function adequately in their expected environment, or has reached what seems to be their highest possible level of achievement.
Intervention techniques include activities, relationships and environments. Activities are analysed and selected for their potential to facilitate the development of particular skills and combined with a suitable type and level of interpersonal interaction to achieve the maximum benefit. The person’s human and non-human environments are organized, as far as possible, to provide the appropriate stimulation and support for learning.
The development of a frame of reference focusing on occupation was initiated by Mary Reilly who, early in her career, became interested in the relevance of the central nervous system to human performance. She began to construct a frame of reference that combined knowledge of the neurosciences with theories of intrinsic motivation and social psychology, and with the ideas of Meyer, one of the founders of the occupational therapy profession. This was the occupational behaviour frame of reference, which had a major influence on occupational therapy theory and practice throughout the latter half of the 20th century and was a forerunner of the occupational performance frame of reference.
Following on from Reilly, several occupational therapy theorists began to develop conceptual frameworks to support occupation-focused practice (e.g. Kielhofner and Burke 1980; Reed and Sanderson 1980; Christiansen and Baum 1997). One of the most influential of these has been the Canadian Model of Occupational Performance and Engagement (CMOP-E) (Townsend and Polatajko 2007).
Most occupational therapists today would acknowledge the influence of the occupational performance frame of reference on their practice, even if it is not the only approach they use.
People are occupational beings who have evolved to be flexible enough to engage in a wide range of occupations that enable survival in almost any environment on Earth. Wilcock (2006) introduced the idea that the primary role of the human brain is healthy survival, describing it as both an occupational brain and a healing brain. Survival is the primary drive of all animals, and health is necessary for survival. Each person has an intrinsic drive to explore the environment, interact with it and learn how to live successfully within it.
There is an interdependent relationship between people and the environments in which they develop and live (Law et al. 1996). Occupational performance results from the interactions between people, their occupations and their environments. Achieving competent occupational performance is a lifelong process of adaptation to the internal and external demands that occur naturally within the context of person–environment–occupation interactions (Schkade and Schultz 1998). Adaptation is the process through which people are able to use their own resources, and environmental resources, to cope with the challenges of daily living (Cole and Tufano 2008).
People live and occupy themselves in communities that include both human and non-human environments. Five groups of intrinsic factors influence how a person interacts with these environments: neurobehavioural, physiological, cognitive, psychological and spiritual (Cole and Tufano 2008). People are able to adapt to their environments through what they do but environments also shape what people do and who they become, in a two-way process.
The discipline of occupational science has contributed much to the occupational performance theory base, from clarifying basic concepts to carrying out research into the relationships between occupations, environments and health. Some of the knowledge base is also drawn from established disciplines, such as biology, sociology, social psychology, neurology and anthropology. Specific areas of knowledge include:
■ Adaptation
■ The components of occupational performance
■ Motivation
■ Meaning and values
■ Volition and engagement
■ Occupational choice
■ Occupational balance and temporal adaptation
■ Environment
■ Role and identity
■ Social and cultural structures.
The three main components of the occupational performance frame of reference are person, occupation (or occupational performance) and environment. These components interact with each other across time and space as the person attempts to adapt to ever-changing environments through occupation (Law et al. 1996).
This frame of reference integrates an understanding of the structure and functions of the body with awareness of the person. We talk about the health of the body but we use the term wellbeing to refer to the state of the person. People are thinking, feeling, spiritual and social beings, who express themselves, transform themselves and relate to the world through occupation.
The occupations that people perform at any stage of their lives are shaped by their own abilities and preferences but also by their environments and opportunities. Occupations develop throughout the lifespan and shape people as much as people shape their occupations.
The environments in which occupations are performed include objects, spaces, people, events, cultural influences, social norms and attitudes (Creek 2003). Cultural influences include values, beliefs, customs and behaviours (Christiansen and Baum 1997). The social environment also includes politics, economy and law.
Wilcock (2006) spoke of being, doing and becoming. Being refers to who the person is, their essential nature, which shapes and is shaped by their occupations. Doing refers to occupational performance, to the engagement of the person in all the occupations that make up the framework of their everyday life. Becoming refers to growth and development, which take place through occupational performance.
People have the capacity to influence the state of their own health through what they do, and a balance of rest, play and work in daily life is necessary to maintain physical and mental health. People are in a state of function when they have the range of skills and level of competence necessary to cope with their environments and perform a balanced variety of occupations that satisfy their needs and support their health and wellbeing.
Dysfunction occurs when people are unable to perform the occupations they need to do, want to do or are expected to do due to disease, injury or environmental conditions (Law et al. 1994).
Human beings have a very large and complex brain that gives them highly developed capacities for abstraction, insight, learning, curiosity and exploratory behaviour (Wilcock 2006). These capacities make people very adaptable and, although much adaptation to specific environments takes place in childhood, people retain the ability to change in response to changing circumstances throughout their lives. Change occurs through various processes:
■ learning or re-learning skills to support the performance of a desired range of occupations
■ putting in place support to enable the performance of those occupations
■ finding alternative occupations to meet personal needs so as to maintain health and life satisfaction.
The occupational performance frame of reference has a very wide applicability because it is concerned with what people do in their daily lives, at any age, in any circumstances and in any environment. It can be used in traditional health and social care settings, in other institutions, such as prisons, and in health promotion or community development projects.
The task of the occupational therapist is to reduce the incapacities resulting from illness and enable occupational performance in the presence of impairment, disability or any other barrier (Reilly 1969). The main process goal of occupational therapy is for the individual to become the agent of therapeutic change (Schkade and Schultz 1998), therefore it is important to elicit the person’s perception of needs and desired level of performance. The outcome goals of intervention are to increase competence in occupational performance and develop skills to support health, wellbeing and life satisfaction.
The occupational therapist begins by helping the people they are working with to identify the occupations that they expect to do in daily life and the areas of performance with which they are having problems. Examples of assessment techniques include: interviewing, the Canadian Occupational Performance Measure (Law et al. 1994), environmental analysis (Hagedorn 2000), observation, checklists and self-assessment.
When problem areas have been identified, the therapist and the person together identify barriers to and enablers of occupational performance. These may be personal and/or environmental. Intervention is targeted at removing or overcoming barriers or putting in place more effective enablers. This may involve developing skills to a level of competence that supports occupational performance, solving occupational performance problems or adapting environments to facilitate performance.
Within the occupational performance frame of reference, interventions are usually individualized because each person has a unique range of occupations and environments. Effective intervention depends on matching people’s performance to the demands of their physical and social environments and their occupations.
Intervention techniques can be categorized as:
■ activity used as a therapeutic medium, for example, developing self-confidence and self-esteem through creative activities
■ education and training strategies, for example, teaching social skills
■ modification of the physical environment, for example, buying a microwave oven to make cooking easier
■ modification of the human environment, for example, joining a course at the local college in order to meet people.
This chapter began by exploring the content of occupational therapy practice under five headings: goals and outcomes; populations served; legitimate tools; core skills; and professional artistry. Occupational therapists work both in statutory health and social care services and in the social field so the content of practice has to reflect this broad scope. The process of intervention was then described, emphasizing that in a person-centred practice it is essentially a complex and iterative process. The chapter ended with descriptions of three frames of reference, chosen to reflect the breadth of knowledge and skills used by occupational therapists in the field of mental health.
Many of the themes introduced in this chapter are discussed in more detail in subsequent chapters.
Agyris C, Schon DA. Theory in Practice: Increasing Professional Effectiveness. San Francisco: Jossey-Bass; 1974.
Allen CK. Occupational Therapy for Psychiatric Diseases: Measurement and Management of Cognitive Disabilities. Boston: Little Brown; 1985.
American Occupational Therapy Association Council on Standards (AOTA). Occupational therapy: its definition and functions. Am. J. Occup. Ther. 1972;26:204–205.
Atkinson K, Wells C. Creative Therapies: A Psychodynamic Approach Within Occupational Therapy. Cheltenham: Stanley Thornes; 2000.
Azima FJ. The Azima battery: an overview. In: Hemphill B, ed. The Evaluation Process in Psychiatric Occupational Therapy. Thorofare, NJ: Slack; 1982:57–67.
Azima H, Azima FJ. Outline of a dynamic theory of occupational therapy. Am. J. Occup. Ther. 1959;13(5):215–221.
Azima H, Wittkower ED. A partial field survey of psychiatric occupational therapy. Am. J. Occup. Ther. 1957;11(1):1–7.
Beck AT. Cognitive therapy and the emotional disorders. New York: International Universities Press; 1976.
Blair S, Daniel MA. An introduction to the psychodynamic frame of reference. In: Duncan EAS, ed. Foundations for Practice in Occupational Therapy. fourth ed. Edinburgh: Elsevier/Churchill Livingstone; 2006:233–253.
Bruce MA, Borg B. Psychosocial Occupational Therapy: Frames of Reference for Intervention. second ed. Thorofare, NJ: Slack; 1993.
Christiansen C, Baum C. Person-environment occupational performance: a conceptual model for practice. In: Christiansen C, Baum C, eds. Occupational Therapy: Enabling Function and Well-Being. Thorofare, NJ: Slack; 1997:47–70.
Cole MB. Group Dynamics in Occupational Therapy: The Theoretical Basis and Practice Application of Group Intervention. fourth ed. Thorofare, NJ: Slack; 2012.
Cole MB, Tufano R. Applied Theories in Occupational Therapy: A Practical Approach. Thorofare, NJ: Slack; 2008.
College of Occupational Therapists. Recovering Ordinary Lives: The Strategy for Occupational Therapy in Mental Health Services 2007–2017. London: College of Occupational Therapists; 2006.
College of Occupational Therapists. Definitions and Core Skills for Occupational Therapy. London: College of Occupational Therapists; 2009.
Creek J. Occupational Therapy Defined as a Complex Intervention. London: College of Occupational Therapists; 2003.
Creek J. The thinking therapist. In: Creek J, Lawson-Porter A, eds. Contemporary Issues in Occupational Therapy: Reasoning and Reflection. Chichester: Wiley; 2007:1–21.
Creek J. Approaches to practice. In: Creek J, Lougher L, eds. Occupational Therapy and Mental Health. fourth ed. Edinburgh: Churchill Livingstone/Elsevier; 2008:59–79.
Crouch R. The impact of poverty on the service delivery of occupational therapy in Africa. In: Alers V, Crouch R, eds. Occupational Therapy: An African Perspective. Johannesburg: Sarah Shorten; 2010:98–110.
Deegan PE. Recovery: the lived experience of rehabilitation. Psychosoc. Rehabil. J. 1988;11(4):11–19.
Dreyfus HL, Dreyfus SE. Mind Over Machine: The Power of Human Intuition and Expertise in the era of the Computer. New York: The Free Press; 1986.
European Network of Occupational Therapy in Higher Education (ENOTHE). 2006. Available at: www.enothe.hva.nl.
Fidler CG. The language of objects. In: Fidler GS, Velde BP, eds. Activities: Reality and Symbol. Thorofare, NJ: Slack; 1999a:37–45.
Fidler CG. Deciphering the message: the activity analysis. In: Fidler GS, Velde BP, eds. Activities: Reality and Symbol. Thorofare, NJ: Slack; 1999b:47–58.
Fidler GS, Fidler JW. Occupational Therapy: A Communication Process in Psychiatry. New York: MacMillan; 1963.
Fine SB. Symbolization: making meaning for self and society. In: Fidler GS, Velde BP, eds. Activities: Reality and Symbol. Thorofare, NJ: Slack; 1999:11–25.
Finlay L. Groupwork. In: Creek J, ed. Occupational Therapy and Mental Health. third ed. Edinburgh: Churchill Livingstone; 2002:245–264.
Fortmeier S, Thanning G. From the Patient’s Point of View: An Activity Theory Approach to Occupational Therapy. Copenhagen: Ergoterapeutforeningen; 2002.
Galheigo SM. Occupational therapy and the social field: clarifying concepts and ideas. In: Kronenberg F, Algado SS, Pollard N, eds. Occupational Therapy Without Borders: Learning from the Spirit of Survivors. Edinburgh: Elsevier/Churchill Livingstone; 2005:87–98.
Hagedorn R. Occupational Therapy: Perspectives and Processes. Edinburgh: Churchill Livingstone; 1995.
Hagedorn R. Tools for Practice in Occupational Therapy: A Structured Approach to Core Skills and Processes. Edinburgh: Churchill Livingstone; 2000.
Haworth NA, MacDonald EM. Theory of Occupational Therapy. third ed. London: Ballière, Tindall and Cox; 1946.
Hooper B, Wood W. Pragmatism and structuralism in occupational therapy: the long conversation. Am. J. Occup. Ther. 2002;56(1):40–50.
Kielhofner G, Burke JP. A model of human occupation, part 1. Conceptual framework and content. Am. J. Occup. Ther. 1980;34(9):572–581.
Law M, Baptiste S, Carswell A, et al. Canadian Occupational Performance Measure. Canada: Canadian Association of Occupational Therapists; 1994.
Law M, Cooper B, Strong S, et al. The person-environment-occupation model: a transactive approach to occupational performance. Can. J. Occup. Ther. 1996;63(1):9–23.
Llorens LA. Facilitating growth and development: the promise of occupational therapy. Am. J. Occup. Ther. 1970;24(2):93–101.
Lorenzo T. Equalizing opportunities for occupational engagement: disabled women’s stories. In: Watson R, Swartz L, eds. Transformation Through Occupation. London: Whurr; 2004:85–102.
Mattingly C, Fleming MH. Clinical Reasoning: Forms of Inquiry in a Therapeutic Practice. Philadelphia: FA Davis; 1994.
Mosey AC. Recapitulation of ontogenesis: a theory for the practice of occupational therapy. Am. J. Occup. Ther. 1968;22(5):426–438.
Mosey AC. Psychosocial Components of Occupational Therapy. New York: Raven; 1986.
Nicholls L. A psychoanalytic discourse in occupational therapy. In: Creek J, Lawson-Porter A, eds. Contemporary Issues in Occupational Therapy: Reasoning and Reflection. Chichester: Wiley; 2007:55–85.
Nicholls L, Piergrossi JC, Gibertoni C de S, et al. Psychoanalytic Thinking in Occupational Therapy. Chichester: Wiley-Blackwell; 2013.
Peloquin SM. The therapeutic relationship. In: Neistadt ME, Crepeau EB, eds. Willard and Spackman’s Occupational Therapy. nineth ed. Philadelphia: Lippincott; 1998:105–119.
Prochaska JO, DiClemente CC. Stages and processes of self-change in smoking: towards an integrative model of change. J. Consult. Clin. Psychol. 1983;51(3):390–395.
Reed KL, Sanderson SN. Concepts of Occupational Therapy. Baltimore: Williams and Wilkins; 1980.
Reed KL, Sanderson SN. Concepts of Occupational Therapy. third ed. Baltimore: Williams and Wilkins; 1992.
Reilly M. The educational process. Am. J. Occup. Ther. 1969;23(4):299–307.
Rogoff B. The Cultural Nature of Human Development. Oxford: Oxford University Press; 2003.
Schkade JK, Schultz S. Occupational adaptation: an integrative frame of reference. In: Neistadt ME, Crepeau EB, eds. Willard and Spackman’s Occupational Therapy. nineth ed. Philadelphia: Lippincott; 1998:529–535.
Shorter Oxford English Dictionary on Historical Principles. fifth ed. Oxford: Oxford University Press; 2002.
Sinclair K. Exploring the facets of clinical reasoning. In: Creek J, Lawson-Porter A, eds. Contemporary Issues in Occupational Therapy: Reasoning and Reflection. Chichester: Wiley; 2007:143–160.
Townsend E, Polatajko HJ. Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-Being and Justice Through Occupation. CAOT Publications ACE. Ontario: Ottawa; 2007.
Townsend E, Wilcock A. Occupational justice and client-centred practice: a dialogue in progress. Can. J. Occup. Ther. 2004;71(2):75–87.
Watson R. A population approach to transformation. In: Watson R, Swartz L, eds. Transformation Through Occupation. London: Whurr; 2004:51–65.
Wilcock AA. An Occupational Perspective of Health. second ed. Thorofare, NJ: Slack; 2006.