Blood Vessels
The physical examination of the venous and arterial structures of the vascular system is a critical component of the patient's evaluation. You can gain great insight into his or her overall cardiovascular status, specifically the detection of peripheral artery disease (PAD) of the lower extremities, which is associated with an increased risk of stroke and cardiovascular events.
 http://evolve.elsevier.com/Seidel
http://evolve.elsevier.com/SeidelPhysical Examination Preview
Here is a preview of the steps involved in conducting a physical examination of the blood vessels.  These procedures are explained in detail in this chapter and are available on Evolve in printable formats.
These procedures are explained in detail in this chapter and are available on Evolve in printable formats.
Blood Vessels
1. Palpate the arterial pulses in distal extremities, comparing characteristics bilaterally for the following (p. 338):
2. Auscultate the carotid, abdominal aorta, and renal, iliac, and femoral arteries for bruits (p. 340).
3. With the patient reclining at a 45-degree angle, inspect for jugular venous pulsations and distention; differentiate jugular and carotid pulse waves, and measure jugular venous pressure (p. 342).
4. Inspect the extremities for sufficiency of arteries and veins through the following (p. 343):
• Color, skin texture, and nail changes
5. Palpate the extremities for the following (p. 344):
Anatomy and Physiology
The great vessels, the arteries leading from and the veins leading to the heart, are located in close proximity at the base of the heart. They include the aorta, superior and inferior venae cavae, pulmonary arteries, and pulmonary veins (Fig. 15-1). The aorta carries oxygenated blood out of the left ventricle to the body. The pulmonary artery, which leaves the right ventricle and divides almost immediately into right and left branches, carries deoxygenated blood to the lungs. The superior and inferior venae cavae carry deoxygenated blood from the upper and lower body, respectively, to the right atrium. The pulmonary veins return oxygenated blood from the lungs to the left atrium.

Blood Circulation
Once it leaves the heart, blood flows through two circulatory systems, the pulmonary and the systemic (Fig. 15-2). The pulmonary circulation routes blood through the lungs, where it is oxygenated before returning to the left atrium and ventricle of the heart. Venous blood arrives at the right atrium via the superior and inferior vena cavae and moves through the tricuspid valve to the right ventricle. During systole, deoxygenated blood is ejected through the pulmonic valve into the pulmonary artery; it travels through the pulmonary arteries, arterioles, and capillaries until it reaches the alveoli, where gas exchange occurs.

Oxygenated blood of the systemic circulation returns to the heart and enters the systemic circulation through the pulmonary veins into the left atrium and then through the mitral valve into the left ventricle. The left ventricle contracts, forcing a volume of blood with each beat (stroke volume) through the aortic valve into the aorta where it is distributed systemically through the arteries and capillaries. In the capillary bed, oxygen is provided to the tissues of the body; the now deoxygenated blood is carbon dioxide-rich and passes into the venous system and returns to the heart via the superior and inferior vena cavae and into the right atrium (Fig. 15-3).


 Animation: Mitral and Aortic Valve Function
Animation: Mitral and Aortic Valve Function
The structure of the arteries and veins reflects their function. The arteries are thicker with a greater smooth muscle layer and less ability to stretch and expand (distension) from internal pressure. They are subjected to much more pressure than are the veins. The veins are less sturdy and more distensible than the arteries (Fig. 15-4). Venous return is less forceful than blood flow through the arteries, and veins contain valves to keep blood flowing in one direction. If blood volume increases significantly, the veins can expand and act as a repository for extra blood. This compensatory mechanism helps diminish stress on the heart.

Arterial Pulse and Pressure
The palpable and sometimes visible arterial pulses are the result of ventricular systole, which produces a pressure wave throughout the arterial system (arterial pulse). It takes barely 0.2 second for the impact of this wave to be felt in the dorsalis pedis artery within the foot and considerably more than 2 seconds for a red blood cell to travel the same distance. The arterial blood pressure is the force exerted by the blood against the wall of an artery as a result of a bolus of blood exiting the left ventricle of the heart as it contracts.
The pulse usually is felt as a forceful wave that is smooth and more rapid on the ascending part of the wave; it becomes domed, less steep, and slower on the descending part (Fig. 15-5). Because the carotid arteries are the most accessible of the arteries closest to the heart, they have the most definitive pulse for evaluation of cardiac function.

The following variables contribute to the characteristics of the pulses:
Jugular Venous Pulse and Pressure
The jugular veins, which empty directly into the superior vena cava, reflect the activity of the right side of the heart and offer clues to its competency. The level at which the jugular venous pulse is visible gives an indication of right atrial pressure.
The external jugular veins are more superficial and more visible bilaterally above the clavicle, close to the insertion of the sternocleidomastoid muscles. The larger internal jugular veins run deep to the sternocleidomastoids, near the carotid arteries, and are less accessible to inspection (Fig. 15-6).

The activity of the right side of the heart is transmitted back through the jugular veins as a pulse* that has five identifiable components—three peaks and two descending slopes (Fig. 15-7):
| a wave | The a wave, the first and most prominent component, is the result of a brief backflow of blood to the vena cava during right atrial contraction. |
| c wave | The c wave is a transmitted impulse from the vigorous backward push produced by closure of the tricuspid valve during ventricular systole. |
| v wave | The v wave is caused by the increasing volume and concomitant increasing pressure in the right atrium. It occurs after the c wave, late in ventricular systole. |
| x slope | The downward x slope is caused by passive atrial filling. |
| y slope | The y slope following the v wave reflects the open tricuspid valve and the rapid filling of the ventricle. |

 Infants and Children
Infants and Children
At birth the cutting of the umbilical cord, through which oxygen has been provided in utero, requires the infant to begin breathing. The onset of respiration expands the lungs and carries air to the alveoli. Pulmonary vascular resistance drops, allowing blood to flow more freely to the lungs. Systemic vascular resistance increases. The ductus arteriosus closes, usually within the first 12 to 14 hours of life. Once pulmonary vascular resistance is lower than systemic resistance, blood flows into the pulmonary arteries rather than across the interatrial foramen ovale. The interatrial foramen ovale is functionally closed by the shifting pressures between the right and left sides of the heart.
Pregnant Women
During pregnancy, the systemic vascular resistance decreases and peripheral vasodilation occurs, often resulting in palmar erythema and spider telangiectasias. The systolic blood pressure decreases slightly. There is a greater decrease in the diastolic pressure. The lowest levels occur in the second trimester and then rise but still remain below prepregnancy levels. Maternal position affects blood pressure. Lower blood pressure can be noted when the patient is supine during the third trimester. This lower pressure is secondary to venous compression of the vena cava and impaired venous return. Blood in the lower extremities tends to pool in later pregnancy—except when the woman is in the lateral recumbent position—as a result of compression of the pelvic veins and inferior vena cava from pressure created by the enlarged uterus. The compression may result in an increase in dependent edema, varicosities of the legs and vulva, and hemorrhoids.
Older Adults
Calcification and plaque buildup in the walls of the arteries can cause stiffness as well as dilation of the aorta, aortic branches, and carotid arteries. The arterial walls lose elasticity and vasomotor tone and are less distensible. The resulting increased peripheral vascular resistance may lead to elevated blood pressure, especially systolic.
Review of Related History
For each of the symptoms or conditions discussed in this section, targeted topics to include in the history of the present illness are listed. Responses to questions about these topics provide clues for focusing the physical examination and the development of an appropriate diagnostic evaluation. Questions regarding medication use (prescription and over the counter preparations) as well as complementary or alternative therapies are relevant for each.
History of Present Illness
• Onset and duration: with activity or rest, recent injury or immobilization
• Continuous burning in toes, pain in thighs or buttocks, pain over specific location, induced by activity
• Skin changes: cold skin, pallor, sores, redness or warmth over vein, visible veins, darkened or ischemic skin
• Limping: pain in buttock or calf with walking (claudication)
• Waking at night with leg pain
• Onset and duration: present in the morning, appearing as the day progresses, sudden onset, insidious onset
• Related circumstances: recent and long airplane travel, recent travel to high elevations
• Associated symptoms: onset of nocturia, increased frequency of urination, increasing shortness of breath
• Treatment attempted (including rest, massage, heat, elevation)
• Medications: heparin, warfarin, diuretics, antihypertensive medications
Past Medical History
• Cardiac surgery or hospitalization for cardiac evaluation or disorder, congenital heart defect, surgical or interventional vascular catheterization procedures
• Chronic illness: hypertension and studies to define its cause, bleeding disorder, hyperlipidemia, diabetes, thyroid dysfunction, stroke, vasculitis, thrombosis, transient ischemic attacks, coronary artery disease, atrial fibrillation or other type of dysrhythmia,
Family History
Family members with risk factors, morbidity, and mortality related to cardiovascular system; hypertension, dyslipidemia, diabetes, heart disease, thrombosis, peripheral vascular disease, abdominal aortic aneurysms, ages at time of illness or death
Personal and Social History
• Employment: physical demands; environmental hazards such as heat, chemicals, dust; sources of emotional stress
• Tobacco: type (cigarettes, cigars, pipe, chewing tobacco, snuff); duration of use; amount; efforts to quit and methods used; age started and, perhaps, stopped; pack-years (Number of years smoking × Number of packs per day)
• Usual diet: proportion of fat, food preferences, history of dieting
• Weight: loss or gain, amount and rate
• Exercise: type, amount, frequency, intensity
• Use of alcohol: amount consumed, frequency, duration of current intake
Infants and Children
Pregnant Women
• Blood pressure: prepregnancy levels, elevation during pregnancy; evidence of preeclampsia with associated symptoms and signs such as headaches, visual changes, nausea and vomiting, epigastric pain, right upper quadrant pain, oliguria, rapid onset of edema (facial, abdominal, or peripheral), hyperreflexia, proteinuria, unusual bruising or bleeding
Older Adults
• Leg edema: pattern, frequency, time of day most pronounced
• Interference with activities of daily living
• Ability of the patient and family to cope with the condition
• Claudication: area involved, unilateral or bilateral, distance one can walk before its onset, sensation, length of time required for relief
Examination and Findings
Equipment
Peripheral Arteries
Video: Vessels: Palpating the Carotid Arteries
Palpation
The pulses are best palpated over arteries that are close to the surface of the body and lie over bones. These include the carotid, brachial, radial, femoral, popliteal, dorsalis pedis, and posterior tibial arteries (Fig. 15-8).

A, Carotid. B, Brachial. C, Radial. D, Femoral. E, Popliteal. F, Dorsalis pedis. G, Posterior tibial.
An arterial pulsation is essentially a bounding wave of blood that diminishes with increasing distance from the heart. The carotid pulses are most easily accessible and closest to the cardiac source, making them most useful in evaluating heart function. Examine the arterial pulses in the extremities to determine the sufficiency of the entire arterial circulation. Palpate at least one pulse point in each extremity, usually at the most distal point (see Clinical Pearl, “Carotid Palpation”).
When examining the arterial pulses, the thumb may be used, especially if vessels have a tendency to move when probed by fingers. In this setting the thumb is particularly useful in “fixing” the brachial and even the femoral pulses. Palpate firmly but not so hard as to occlude the artery. The exception to this is when doing the Allen test to ensure ulnar artery patency prior to radial artery puncture (Box 15-1).
Box 15-1
The Allen Test
This test assesses the patency of the ulnar artery. Perform this test prior to radial artery puncture for arterial blood gas sampling or the insertion of a radial arterial catheter.
1. With the patient's palm facing upward, compress the radial and ulnar artery with your fingers (A).
2. Have the patient close and open the fist five times and then leave the blanched palm open.
3. Release pressure on the ulnar artery alone and watch for palmar reperfusion within 4 to 5 seconds.
4. If palmar reperfusion does not occur, suspect ulnar artery insufficiency and do not puncture the radial artery (B).

Video: Blood Vessels: Assessing Arterial Pulses
Palpate the arterial pulses (most often the radial) to assess the heart rate and rhythm, pulse contour (waveform), amplitude (force), symmetry, and sometimes obstructions to blood flow. Variations from the expected findings are described in Figure 15-9.
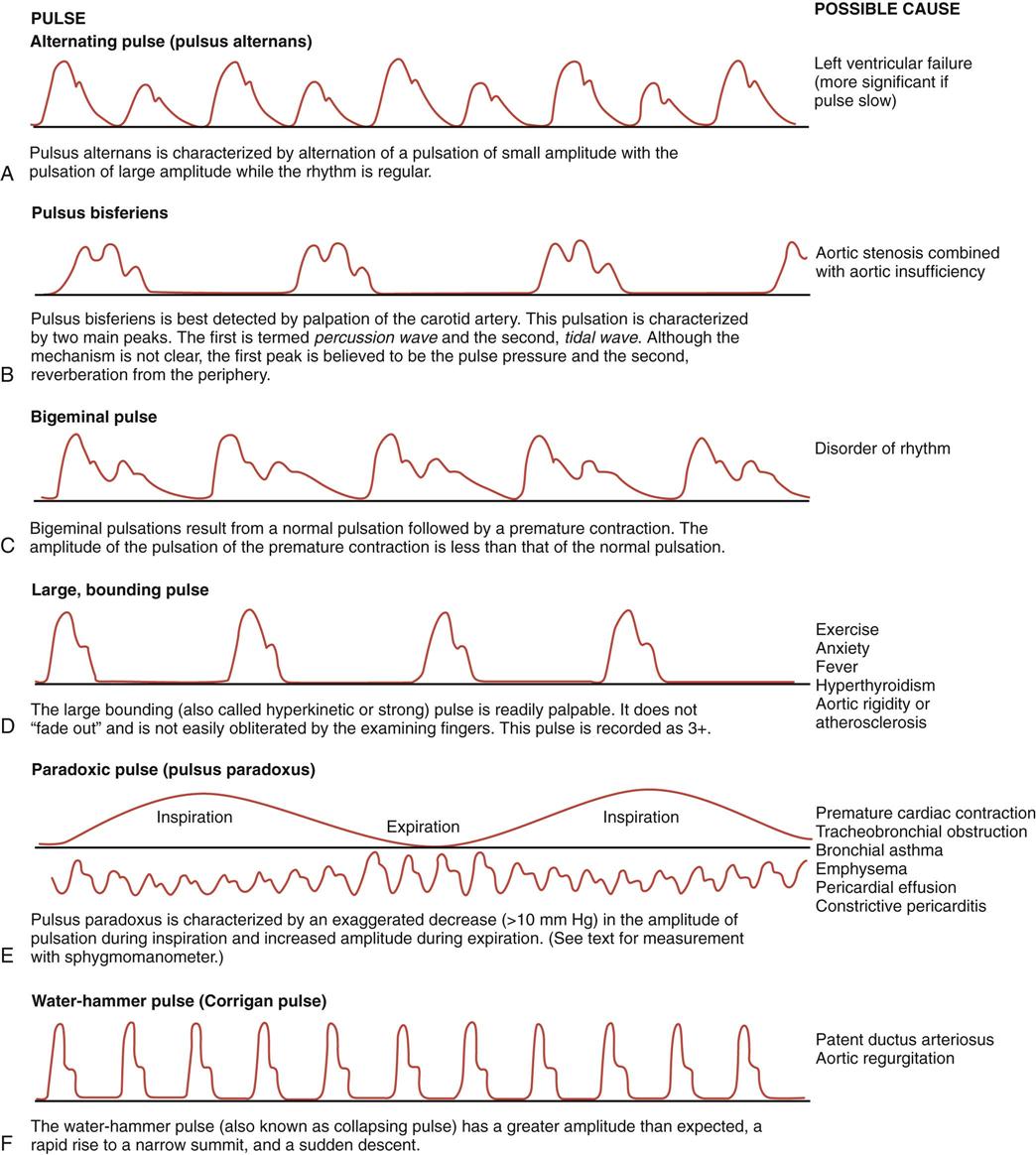
The contour of the pulse wave is pliable. Healthy arteries have a smooth, rounded, or dome shape. Pay attention to the ascending portion, the peak, and the descending portion. Compare each wave crest with the next to detect cyclic differences.
The amplitude of the pulse is described on a scale of 0 to 4:
| 4 | Bounding, aneurysmal |
| 3 | Full, increased |
| 2 | Expected |
| 1 | Diminished, barely palpable |
| 0 | Absent, not palpable |
Determine the regularity of the heart rhythm. If it is irregular, determine whether there is a consistent pattern. An irregular heart rate that occurs in a repeated pattern may indicate sinus arrhythmia, a cyclic variation of the heart rate characterized by an increasing rate on inspiration and decreasing rate on expiration. A patternless, unpredictable, irregular rate may indicate heart disease or an impaired conduction system such as atrial fibrillation. If you note an irregular rate, record the beats per minute and compare it with the rate heard when auscultating the heart (see Chapter 14). Note the strength of the pulse.
Lack of symmetry (in pulse contour or strength) between the left and right extremities suggests impaired circulation. Compare the strength of the upper extremity pulses with those of the lower extremities and the left with the right. Ordinarily, the femoral is as strong as or stronger than the radial pulse. If the femoral pulsation is absent or diminished, proximal obstruction should be suspected, which may be due to such conditions as coarctation of the aorta, atherosclerotic peripheral arterial disease, or vasculitis.
Auscultation
Auscultate over an artery for a bruit (i.e., a murmur or unexpected sound) if you are following the radiation of murmurs first noted during the cardiac examination or looking for evidence of local obstruction. These sounds are usually low-pitched and relatively hard to hear. Place the bell of the stethoscope directly over the artery. Sites to auscultate for a bruit are over the carotid, subclavian, abdominal aorta, renal, iliac, and femoral arteries. See Chapter 17 for auscultation of abdominal bruits. When listening over the carotid vessels, ask the patient to suspend his or her breathing for a few heartbeats so that respiratory sounds will not interfere with auscultation (Fig. 15-10). Sounds heard over the neck include venous hums and carotid bruits (Box 15-2).

Assessment for Peripheral Arterial Disease
Arteries in any location can become narrowed, leading to decreased blood flow. The reduced circulation to the tissues will lead to signs and symptoms that are related to the following:
The first symptom is pain that results from muscle ischemia, referred to as claudication. This pain can be characterized as a dull ache with accompanying muscle fatigue and cramps. It usually appears during sustained exercise, such as walking a distance or climbing several flights of stairs. Just a few minutes of rest will ordinarily relieve it. It recurs again with the same amount of activity. Continued activity causes worsening pain.
The site of pain is distal to the narrowing. After determining the distinguishing characteristics of the pain, note the following:
• Pulses (strong, weak or possibly absent)
• Possible systolic bruits over the arteries that may extend through diastole
• Loss of expected body warmth in the affected area
• Localized pallor and cyanosis
• Collapsed superficial veins, with delay in venous filling
• Thin, atrophied skin; muscle atrophy (particularly with long-term insufficiency)
To judge the degree of narrowing and the potential severity of the arterial insufficiency, perform the following steps:
• Have the patient lie supine.
• Note the degree of blanching.
• Have the patient sit on the edge of the bed or examining table in order to lower the extremity.
• Note the time for maximal return of color after the extremity has been elevated. Slight pallor on elevation and a return to full color as soon as the leg becomes dependent are the expected findings. A delay of many seconds or even minutes before the extremity regains full color indicates arterial insufficiency. When return to full color takes as long as 2 minutes, the problem is severe.
A measurement of the capillary refill time provides another method of assessing severity (Box 15-3).
The following list provides a general guideline for assessment of possible causes of pain:
| Pain Location | Probable Obstructed Artery |
| Calf muscles | Superficial femoral artery |
| Thigh | Common femoral artery or external iliac artery |
| Buttock | Common iliac artery or distal aorta (erectile dysfunction may accompany stenosis of distal aorta) |
If the pain is constant, the narrowing is critical and probably acute; if it is excruciating, a major artery has probably been severely compromised.
Peripheral Veins
Jugular Venous Pressure
Careful measurement of the jugular venous pressure (JVP) is an important and, in some cases, critical portion of the physical examination. Several techniques may be used. The simplest, most reproducible and reliable method requires two pocket rulers at least 15 cm long. Place the patient in the supine position using a bed or examining table with an adjustable back support. Use a light to supply tangential illumination across the right side of the patient's neck to accentuate the appearance of the jugular venous pulsations (Fig. 15-11).

Video: Blood Vessels: Assessing the Jugular Veins
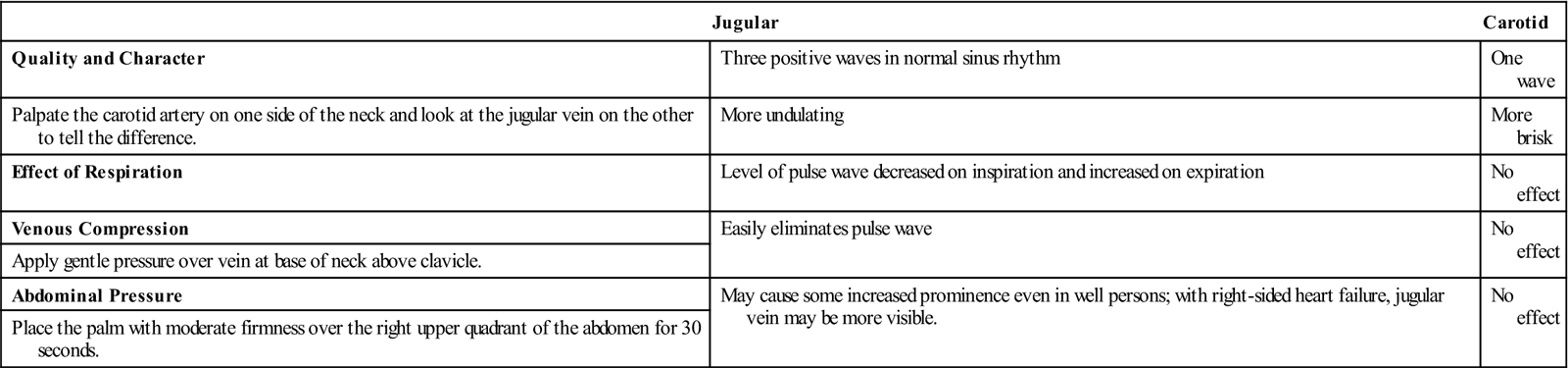
When the supine patient is initially placed flat, note the engorgement of the jugular veins. Gradually raise the head of the bed until the jugular venous pulsations become evident between the angle of the jaw and the clavicle (see Fig. 15-6). Palpating the carotid pulse helps identify the venous pulsations and distinguish them from the carotid pulsations. Table 15-1 provides instructions on differentiating between jugular and carotid pulses. The jugular pulse can only be visualized; it cannot be palpated.
Table 15-1
Comparison of the Jugular and Carotid Pulse Waves
| Jugular | Carotid | |
| Quality and Character | Three positive waves in normal sinus rhythm | One wave |
| Palpate the carotid artery on one side of the neck and look at the jugular vein on the other to tell the difference. | More undulating | More brisk |
| Effect of Respiration | Level of pulse wave decreased on inspiration and increased on expiration | No effect |
| Venous Compression | Easily eliminates pulse wave | No effect |
| Apply gentle pressure over vein at base of neck above clavicle. | ||
| Abdominal Pressure | May cause some increased prominence even in well persons; with right-sided heart failure, jugular vein may be more visible. | No effect |
| Place the palm with moderate firmness over the right upper quadrant of the abdomen for 30 seconds. |
Several conditions may make the JVP examination more difficult: (1) severe right heart failure, tricuspid insufficiency, constrictive pericarditis, and cardiac tamponade may each cause extreme elevation of the JVP so that it is not apparent until the patient is sitting upright; (2) severe volume depletion makes the JVP difficult to detect even when the patient is flat; and (3) in extreme obesity, overlying adipose tissue obscures the jugular venous pulsations.
Place a ruler with its tip at the midaxillary line (the position of the heart within the chest) at the level of the nipple and extended vertically. Place the second ruler at the level of the meniscus of the JVP, extended horizontally to where it intersects the vertical ruler. The vertical distance above the level of the heart is noted as the mean JVP in centimeters of water (see Fig. 15-11). A value of less than 9 cm H2O is the expected value.
Maneuvers useful for confirming the JVP measurement include hepatojugular reflux and evaluation of the venous engorgement of the hands at various levels of elevation above the heart.
Hepatojugular Reflux
The hepatojugular reflux is exaggerated when right heart failure is present, and its measurement is used to evaluate that condition. To assess the hepatojugular reflux maneuver, use your hand to apply firm and sustained pressure to the abdomen in the midepigastric region and instruct the patient to breathe regularly. Observe the neck for an elevation in JVP followed by an abrupt fall in JVP as the hand pressure is released. The JVP quickly equilibrates to its true level between the positions it achieved with and immediately after removal of the abdominal hand pressure.
If the JVP is not obvious with this maneuver, the pressure is either much higher or much lower. Repeat the maneuver with the patient more supine if you suspect the pressure to be lower. Position the patient more upright if you suspect the JVP to be higher.
Evaluation of Hand Veins
The veins of the hand can be used as an “auxiliary manometer” of the right heart pressure when the patient does not have thrombosis or arteriovenous fistula in that arm or superior vena cava syndrome. With the patient semirecumbent, place the hand on the examination table or mattress. Palpate the hand veins, which should be engorged, to make sure they are compressible. Slowly raise the hand until the hand veins collapse (Fig. 15-12). Use a ruler to note the vertical distance between the midaxillary line at the nipple level (level of the heart) and the level of collapse of the hand veins. Confirm this level by lowering the hand slowly until the veins distend again and raise it back until they once again collapse. This distance should be identical to the mean JVP.
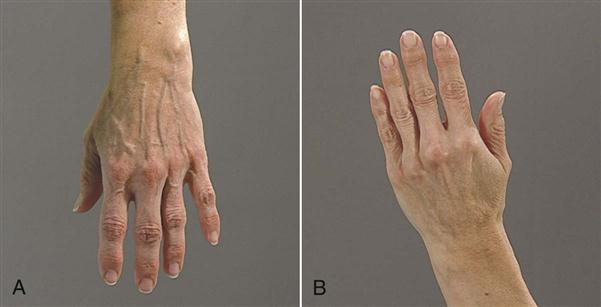
A, Engorged veins in dependent hand. B, Collapsed veins in elevated hand.
The hand vein measurement is particularly helpful to evaluate severe right heart failure when the pressure may be 20 to 30 cm H2O (i.e., JVP is not evident with the patient sitting upright) or with volume depletion (i.e., JVP not visible with the patient supine).
Assessment for Venous Obstruction and Insufficiency
Obstruction of the venous system and a consequent insufficiency results in signs and symptoms that vary depending on how rapidly the obstruction develops and on the degree of localization. An acute obstruction may result from injury, external compression, or thrombosis. In the affected area, constant pain occurs simultaneously with the following:
Inspect the extremities for signs of venous insufficiency (e.g., thrombosis, varicose veins, or edema). Examine the patient in both the standing and supine positions, particularly in the case of a suspected chronic venous occlusion. Ultrasound studies can confirm the presence of venous occlusion. See Clinical Pearl, “Calf Pain.”
Thrombosis.
Note any redness, thickening, and tenderness along a superficial vein, suggesting thrombophlebitis of a superficial vein. Suspect a deep vein thrombosis if swelling, pain, and tenderness occur over a vein. It cannot be confirmed on physical examination alone.
Homan Sign.
Flex the patient's knee slightly with one hand and, with the other, dorsiflex the foot. The description of calf pain with this procedure is a positive sign and may indicate venous thrombosis. Absence of the Homan sign does not preclude venous thrombosis.
Animation: Venous Thrombosis
Edema.
Inspect the extremities for edema, manifested as a change in the usual contour of the leg. Press your index finger over the bony prominence of the tibia or medial malleolus for several seconds. A depression that does not rapidly refill and resume its original contour indicates orthostatic (pitting) edema. This finding is not usually accompanied by thickening or pigmentation of the overlying skin. Right-sided heart failure leads to an increased fluid volume, which in turn elevates the hydrostatic pressure in the vascular space, causing edema in dependent parts of the body.
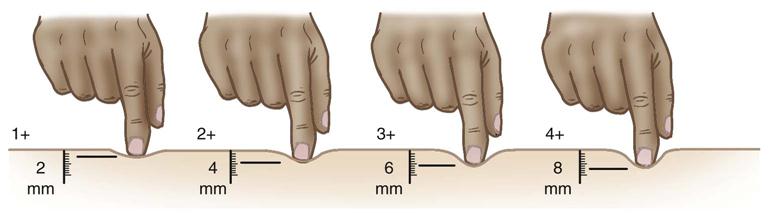
The severity of edema may be characterized by grading 1+ through 4+ (Fig. 15-13). Any concomitant pitting can be mild or severe, as evidenced by the following:
| 1+ | Slight pitting, no visible distortion, disappears rapidly |
| 2+ | A somewhat deeper pit than in 1+, but again no readily detectable distortion; disappears in 10 to 15 seconds |
| 3+ | Noticeably deep pit that may last more than a minute; dependent extremity looks fuller and swollen |
| 4+ | Very deep pit that lasts as long as 2 to 5 minutes; dependent extremity is grossly distorted |
Edema accompanied by some thickening and ulceration of the skin is frequently associated with deep venous obstruction or venous valvular incompetence (see Clinical Pearl, “Edema”). Edema related to valvular incompetence or an obstruction of a deep vein (usually in the legs) is caused by the mechanical pressure of increased blood volume in the area served by the affected vein. Circulatory disorders that cause edema so tense that it does not pit must be distinguished from lymphedema (see Chapter 9).
Varicose Veins.
Varicose veins are dilated and swollen, with a diminished rate of blood flow and an increased intravenous pressure. These characteristics result from incompetence of the vessel wall or venous valves or an obstruction in a more proximal vein.
Inspect the legs for superficial varicosities when the patient is standing. With varicosities, the veins appear dilated and often tortuous. If varicose veins are suspected, have the patient stand on the toes 10 times in succession. Palpate the legs to feel the venous distention. When the venous system is competent, the distention of the veins disappears in a few seconds. If the distention of the veins is sustained for a longer time then venous insufficiency is suspected.
To evaluate the direction of blood flow and the competency of the valves in the venous system, distend visible veins by putting the limb in a dependent position. Compress the vein with the finger or thumb of one hand and strip the vein of blood by compressing the vein and moving the fingers of the second hand proximally. If the compressed vessel fills before either compressing finger is released, collateral circulation exists. If the compressing finger nearest the heart is released, the vessel should fill backward to the first valve only. If the entire venous column fills, the valves in that vessel are incompetent.
Infants
The brachial, radial, and femoral pulses of the newborn are easily palpated. When the pulse is weaker than expected, cardiac output may be diminished or peripheral vasoconstriction may be present. A bounding pulse is associated with a large left-to-right shunt produced by a patent ductus arteriosus. In coarctation of the aorta, a difference is noted in pulse amplitude between the upper extremities or between the femoral and radial pulses, or the femoral pulses are absent.
Capillary refill times in infants and children younger than 2 years of age are rapid, less than 1 second. A prolonged capillary refill time, longer than 2 seconds, indicates dehydration or hypovolemic shock.
Children
A venous hum, common in children, usually has no pathologic significance (see Box 15-2). It is caused by the turbulence of blood flow in the internal jugular veins. To detect a venous hum, ask the child to sit with the head turned away from you and tilted slightly upward. Auscultate over the supraclavicular space at the medial end of the clavicle and along the anterior border of the sternocleidomastoid muscle (Fig. 15-14). The intensity of the hum is increased when the patient is sitting with the head turned away from the area of auscultation, and it is diminished with a Valsalva maneuver. When present, the hum is a continuous, low-pitched sound that is louder during diastole. It may be interrupted by gentle pressure over the vein in the space between the trachea and the sternocleidomastoid muscle at about the level of the thyroid cartilage. The venous hum can be confused with patent ductus arteriosus, aortic regurgitation, and the murmur of valvular aortic stenosis transmitted into the carotid arteries.

Venous thrombosis occurs less commonly in children than in adults and is most often associated with placement of venous access devices. They can occur in any peripheral vessel and cause swollen, painful extremities.
Pregnant Women
With increasing cardiac output beginning in the first trimester, the pulse may be more easily palpated, with an abrupt rise and rapid fall. With increasing blood volume in the second trimester jugular a and v waves may be easier to see. JVP should remain normal. Peripheral edema is a common finding as the pregnancy progresses. Varicose veins can develop during pregnancy and in the postpartum period.
Older Adults
The dorsalis pedis and posterior tibial pulses may be more difficult to find, and the superficial vessels are more apt to appear tortuous and distended.
Abnormalities
Blood Vessels
Vessel Disorders
Temporal Arteritis (Giant Cell Arteritis)
An inflammatory disease of the branches of the aortic arch, including the temporal arteries

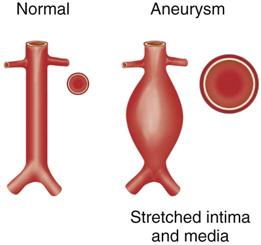
Arterial Aneurysm
An aneurysm is a localized dilation, generally defined as 1.5 times the diameter of the normal artery, caused by a weakness in the arterial wall (Fig. 15-15).

Arteriovenous Fistula
An arteriovenous fistula is a pathologic communication between an artery and a vein.

Peripheral Arterial Disease
Stenosis of the blood supply to the extremities by atherosclerotic plaques

Raynaud Phenomenon
An exaggerated spasm of the digital arterioles (occasionally in the nose and ears) usually in response to cold exposure (Fig. 15-16)


Arterial Embolic Disease
Atrial fibrillation can lead to clot formation within the atrium; if the clot is unstable, emboli may be dispersed throughout the arterial system (Fig. 15-17).


Venous Thrombosis
Thrombosis can occur suddenly or gradually and with varying severity of symptoms; it can be the result of trauma or prolonged immobilization.

Animation: Venous Thrombosis
Jugular Venous Pressure Disorder
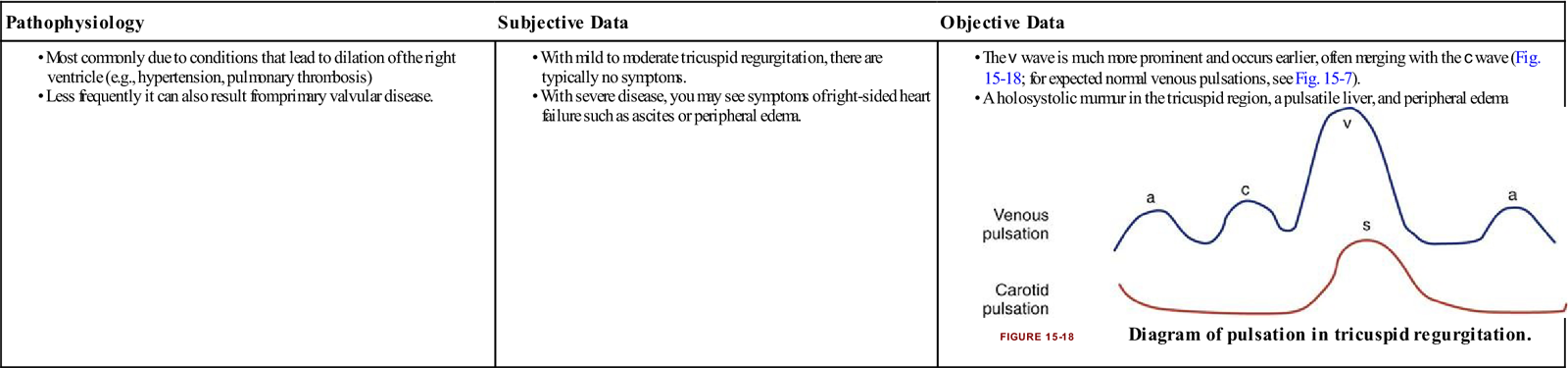
Tricuspid Regurgitation
The backflow of blood into the right atrium during systole; a mild degree of tricuspid regurgitation can be seen in up to 75% of the normal adult population.
| Pathophysiology | Subjective Data | Objective Data |
• The v wave is much more prominent and occurs earlier, often merging with the c wave (Fig. 15-18; for expected normal venous pulsations, see Fig. 15-7).
|

Children
Coarctation of the Aorta
Coarctation of the aorta is a stenosis seen most commonly in the descending aortic arch near the origin of the left subclavian artery and ligamentum arteriosum (Fig. 15-19).


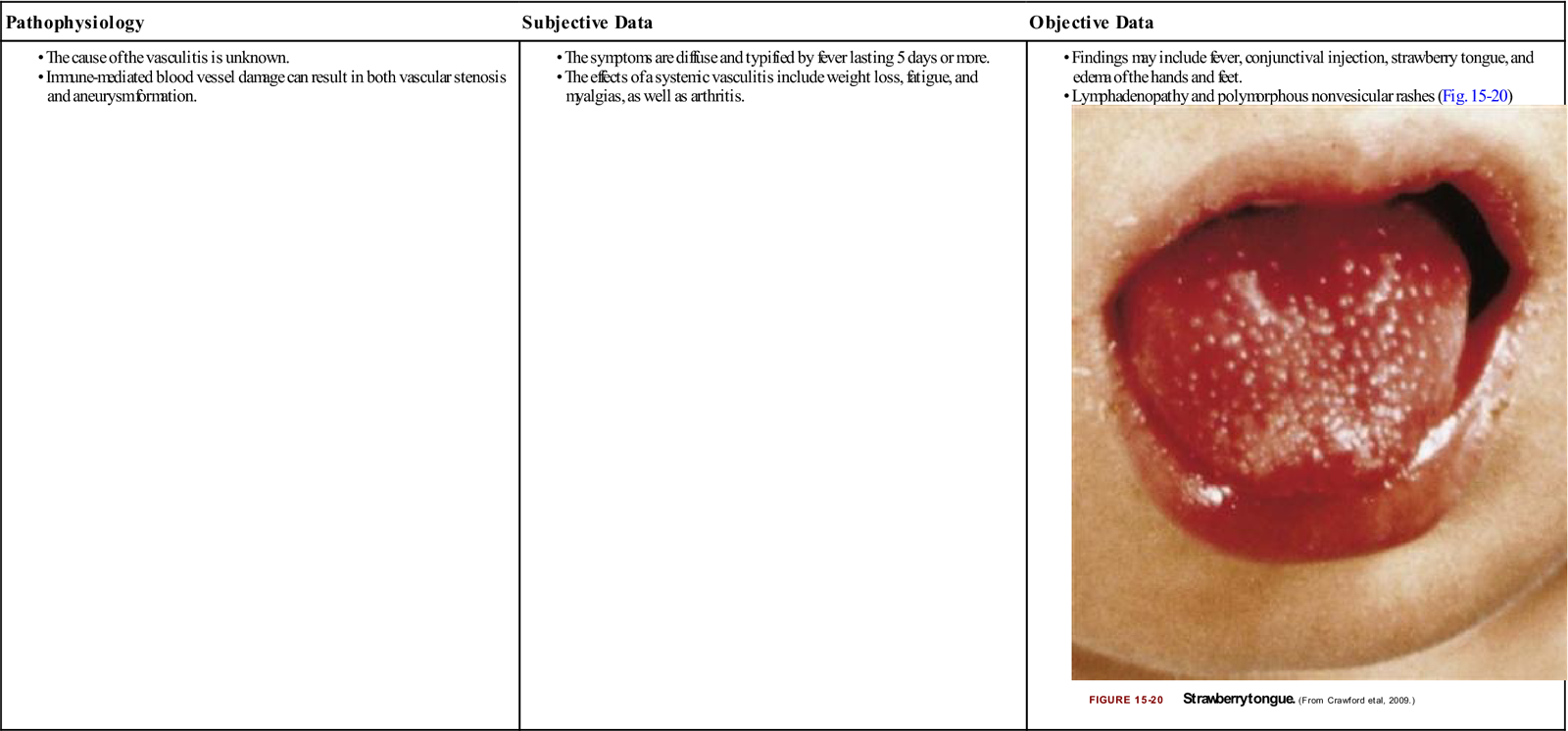
Kawasaki Disease
An acute small vessel vasculitic illness of uncertain cause affecting young males more often than females; the critical concern is cardiac involvement in which coronary artery aneurysms may develop.
| Pathophysiology | Subjective Data | Objective Data |
• Findings may include fever, conjunctival injection, strawberry tongue, and edema of the hands and feet.
• Lymphadenopathy and polymorphous nonvesicular rashes (Fig. 15-20) |

Pregnant Women
Preeclampsia-Eclampsia
Preeclampsia-eclampsia defines a syndrome specific to pregnancy; it is determined by hypertension that occurs after the 20th week of pregnancy and the presence of proteinuria; eclampsia is preeclampsia with seizures when no other cause for the seizures can be found.

Older Adults
Venous Ulcers
This results from chronic venous insufficiency in which lack of venous flow leads to lower extremity venous hypertension (Fig. 15-21).

