The female pelvis and the reproductive organs
Ranee Thakar, Abdul H Sultan
Female external genital organs
The female external genitalia (the vulva) include the mons pubis, labia majora, labia minora, clitoris, vestibule, the greater vestibular glands (Bartholin's glands) and bulbs of the vestibule (Fig. 3.1).
• The mons pubis is a rounded pad of fat lying anterior to the symphysis pubis. It is covered with pubic hair from the time of puberty.
• The labia majora (‘greater lips’) are two folds of fat and areolar tissue which are covered with skin and pubic hair on the outer surface and have a pink, smooth inner surface.
• The labia minora (‘lesser lips’) are two small subcutaneous folds, devoid of fat, that lie between the labia majora. Anteriorly, each labium minus divides into two parts: the upper layer passes above the clitoris to form along with its fellow a fold, the prepuce, which overhangs the clitoris. The prepuce is a retractable piece of skin which surrounds and protects the clitoris. The lower layer passes below the clitoris to form with its fellow the frenulum of the clitoris.
• The clitoris is a small rudimentary sexual organ corresponding to the male penis. The visible knob-like portion is located near the anterior junction of the labia minora, above the opening of the urethra and vagina. Unlike the penis, the clitoris does not contain the distal portion of the urethra and functions solely to induce the orgasm during sexual intercourse.
• The vestibule is the area enclosed by the labia minora in which the openings of the urethra and the vagina are situated.
• The urethral orifice lies 2.5 cm posterior to the clitoris and immediately in front of the vaginal orifice. On either side lie the openings of the Skene's ducts, two small blind-ended tubules 0.5 cm long running within the urethral wall.
• The vaginal orifice, also known as the introitus of the vagina, occupies the posterior two-thirds of the vestibule. The orifice is partially closed by the hymen, a thin membrane that tears during sexual intercourse. The remaining tags of hymen are known as the ‘carunculae myrtiformes’ because they are thought to resemble myrtle berries.
• The greater vestibular glands (Bartholin's glands) are two small glands that open on either side of the vaginal orifice and lie in the posterior part of the labia majora. They secrete mucus, which lubricates the vaginal opening. The duct may occasionally become blocked, which can cause the secretions from the gland to accommodate within it and form a cyst.
• The bulbs of the vestibule are two elongated erectile masses flanking the vaginal orifice.

Blood supply
The blood supply comes from the internal and the external pudendal arteries. The blood drains through corresponding veins.
Lymphatic drainage
Lymphatic drainage is mainly via the inguinal glands.
Innervation
The nerve supply is derived from branches of the pudendal nerve.
The perineum
The perineum corresponds to the outlet of the pelvis and is somewhat lozenge-shaped. Anteriorly, it is bound by the pubic arch, posteriorly by the coccyx, and laterally by the ischiopubic rami, ischial tuberosities and sacrotuberous ligaments. The perineum can be divided into two triangular parts by drawing an arbitrary line transversely between the ischial tuberosities. The anterior triangle, which contains the external urogenital organs, is known as the urogenital triangle and the posterior triangle, which contains the termination of the anal canal, is known as the anal triangle.
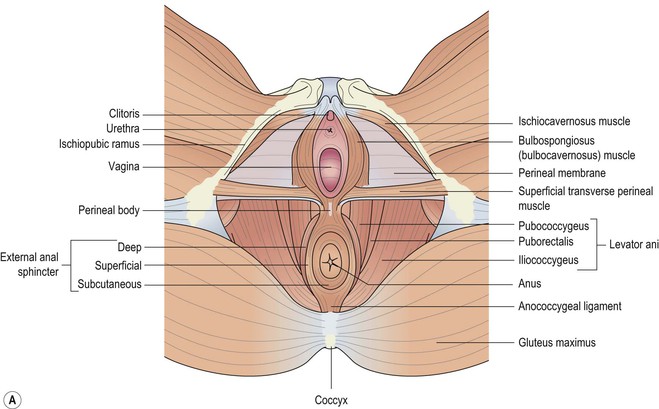
The urogenital triangle
The urogenital triangle (Fig. 3.2a) is bound anteriorly and laterally by the pubic symphysis and the ischiopubic rami. The urogenital triangle has been divided into two compartments: the superficial and deep perineal spaces, separated by the perineal membrane which spans the space between the ischiopubic rami. The levator ani muscles are attached to the cranial surface of the perineal membrane. The vestibular bulb and clitoral crus lie on the caudal surface of the membrane and are fused with it. These erectile tissues are covered by the bulbospongiosus and the ischiocavernosus muscles.
Superficial muscles of the perineum
Superficial transverse perineal muscle
The superficial transverse muscle is a narrow slip of a muscle that arises from the inner and forepart of the ischial tuberosity and is inserted into the central tendinous part of the perineal body (Fig. 3.2a). The muscle from the opposite side, the external anal sphincter (EAS) from behind, and the bulbospongiosus in the front, all attach to the central tendon of the perineal body.
Bulbospongiosus muscle
The bulbospongiosus (previously known as bulbocavernosus) muscle runs on either side of the vaginal orifice, covering the lateral aspects of the vestibular bulb anteriorly and the Bartholin's gland posteriorly (Fig. 3.2b). Some fibres merge posteriorly with the superficial transverse perineal muscle and the EAS in the central fibromuscular perineal body. Anteriorly, its fibres pass forward on either side of the vagina and insert into the corpora cavernosa clitoridis, a fasciculus crossing over the body of the organ so as to compress the deep dorsal vein. This muscle diminishes the orifice of the vagina and contributes to the erection of the clitoris.

Ischiocavernosus muscle
The ischiocavernosus muscle is elongated, broader at the middle than at either end and is situated on the side of the lateral boundary of the perineum (Fig. 3.2a). It arises by tendinous and fleshy fibres from the inner surface of the ischial tuberosity, behind the crus clitoridis, from the surface of the crus and from the adjacent portions of the ischial ramus.
Innervation
The nerve supply is derived from branches of the pudendal nerve.
The anal triangle
This area includes the anal canal, the anal sphincters and the ischioanal fossae.
Anal canal
The rectum terminates in the anal canal (Fig. 3.3). The anal canal is attached posteriorly to the coccyx by the anococcygeal ligament, a midline fibromuscular structure that runs between the posterior aspect of the EAS and the coccyx. The anus is surrounded laterally and posteriorly by loose adipose tissue within the ischioanal fossae, which is a potential pathway for spread of perianal sepsis from one side to the other. The pudendal nerves pass over the ischial spines at this point and can be accessed for injection of local anaesthetic into the pudenal nerve at this site. Anteriorly, the perineal body separates the anal canal from the vagina.

The anal canal is surrounded by an inner epithelial lining, a vascular subepithelium, the internal anal sphincter (IAS), the EAS and fibromuscular supporting tissue. The lining of the anal canal varies along its length due to its embryologic derivation. The proximal anal canal is lined with rectal mucosa (columnar epithelium) and is arranged in vertical mucosal folds called the columns of Morgagni (Fig. 3.3). Each column contains a terminal radical of the superior rectal artery and vein. The vessels are largest in the left-lateral, right-posterior and right-anterior quadrants of the wall of the anal canal where the subepithelial tissues expand into three anal cushions. These cushions seal the anal canal and help maintain continence of flatus and liquid stools. The columns are joined together at their inferior margin by crescentic folds called anal valves. About 2 cm from the anal verge, the anal valves create a demarcation called the dentate line. Anoderm covers the last 1–1.5 cm of the distal canal below the dentate line and consists of modified squamous epithelium that lack skin adnexal tissues such as hair follicles and glands, but contains numerous somatic nerve endings. Since the epithelium in the lower canal is well supplied with sensory nerve endings, acute distension or invasive treatment of haemorrhoids in this area causes profuse discomfort, whereas treatment can be carried out with relatively few symptoms in the upper canal lined by insensate columnar epithelium. As a result of tonic circumferential contraction of the sphincter, the skin is arranged in radiating folds around the anus and is called the anal margin. These folds appear to be flat or ironed out when there is underlying sphincter damage. The junction between the columnar and squamous epithelia is referred to as the anal transitional zone, which is variable in height and position and often contains islands of squamous epithelium extending into columnar epithelium. This zone probably has a role to play in continence by providing a highly specialized sampling mechanism.
Anal sphincter complex
The anal sphincter complex consists of the EAS and IAS separated by the conjoint longitudinal coat (Fig. 3.3). Although they form a single unit, they are distinct in structure and function.
External anal sphincter
The EAS comprises of striated muscle and appears red in colour (similar to raw red meat) (Fig. 3.4). As the EAS is normally under tonic contraction, it tends to retract when completely torn. A defect of the EAS can lead to urge faecal incontinence.

Internal anal sphincter
The IAS is a thickened continuation of the circular smooth muscle of the bowel and ends with a well-defined rounded edge 6–8 mm above the anal margin at the junction of the superficial and subcutaneous part of the EAS. In contrast to the EAS, the IAS has a pale appearance to the naked eye (Fig. 3.5). Defect of the IAS can lead to passive soiling of stools and flatus incontinence.

The longitudinal layer and the conjoint longitudinal coat
The longitudinal layer is situated between the EAS and IAS and consists of a fibromuscular layer, the conjoint longitudinal coat and the intersphincteric space with its connective tissue components (see Fig. 3.3).
Innervation of the anal sphincter complex
The nerve supply is derived from branches of the pudendal nerve.
Vascular supply
The anorectum receives its major blood supply from the superior haemorrhoidal (terminal branch of the inferior mesenteric artery) and inferior haemorrhoidal (branch of the pudendal artery) arteries, and to a lesser degree, from the middle haemorrhoidal artery (branch of the internal iliac), forming a wide intramural network of collaterals. The venous drainage of the upper anal canal mucosa, IAS and conjoint longitudinal coat passes via the terminal branches of the superior rectal vein into the inferior mesenteric vein. The lower anal canal and the EAS drain via the inferior rectal branch of the pudendal vein into the internal iliac vein.
Lymphatic drainage
The anorectum has a rich network of lymphatic plexuses. The dentate line represents the interface between the two different systems of lymphatic drainage. Above the dentate line (the upper anal canal), the IAS and the conjoint longitudinal coat drain into the inferior mesenteric and internal iliac nodes. Lymphatic drainage below the dentate line, which consists of the lower anal canal epithelium and the EAS, proceeds to the external inguinal lymph nodes.
The ischioanal fossa
The ischioanal fossa (previously known as the ‘ischiorectal fossa’) extends around the anal canal and is bound anteriorly by the perineal membrane, superiorly by the fascia of the levator ani muscle and medially by the EAS complex at the level of the anal canal. The ischioanal fossa contains fat and neurovascular structures, including the pudendal nerve and the internal pudendal vessels.
The perineal body
The perineal body is the central point between the urogenital and the anal triangles of the perineum (see Fig. 3.2a). Within the perineal body there are interlacing muscle fibres from the bulbospongiosus, superficial transverse perineal and EAS muscles. Above this level there is a contribution from the conjoint longitudinal coat and the medial fibres of the puborectalis muscle. Therefore, the support of the pelvic structures, and to some extent the hiatus urogenitalis between the levator ani muscles, depends upon the integrity of the perineal body.
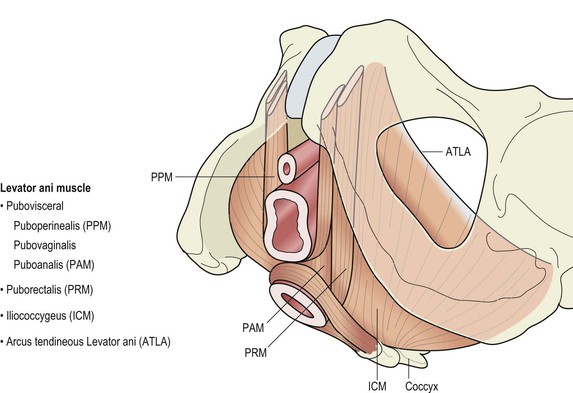
The pelvic floor
The pelvic floor is a musculotendinous sheet that spans the pelvic outlet and consists mainly of the symmetrically paired levator ani muscle (LAM) (Fig. 3.6), which is a broad muscular sheet of variable thickness attached to the internal surface of the true pelvis. Although there is controversy regarding the subdivisions of the muscle, it is broadly accepted that it is subdivided into parts according to their attachments, namely the pubovisceral (also known as pubococcygeus), puborectal and iliococcygeus. The pubovisceral part is further subdivided according to its relationship to the viscera, i.e. puboperinealis, pubovaginalis and puboanalis. The puborectalis muscle is located lateral to the pubovisceral muscle, cephalad to the deep component of the EAS, from which it is inseparable posteriorly.
The muscles of the levator ani differ from most other skeletal muscles in that they:
• maintain constant tone, except during voiding, defaecation and the Valsalva manoeuvre;
• have the ability to contract quickly at the time of acute stress (such as a cough or sneeze) to maintain continence;
• distend considerably during parturition to allow the passage of the term infant and then contract after birth to resume normal functioning.
Until recently, the concept of pelvic floor trauma was attributed largely to perineal, vaginal and anal sphincter injuries. However, in recent years, with advances in magnetic resonance imaging and three-dimensional ultrasound, it has become evident that LAM injuries form an important component of pelvic floor trauma. LAM injuries occur in 13–36% of women who have a vaginal birth. Injury to the LAM is attributed to vaginal birth resulting in reduced pelvic floor muscle strength, enlargement of the vaginal hiatus and pelvic organ prolapse. There is inconclusive evidence to support an association between LAM injuries and stress urinary incontinence and there seems to be a trend towards the development of faecal incontinence.
Innervation of the levator ani
The levator ani is supplied on its superior surface by the sacral nerve roots (S2–S4) and on its inferior surface by the perineal branch of the pudendal nerve.
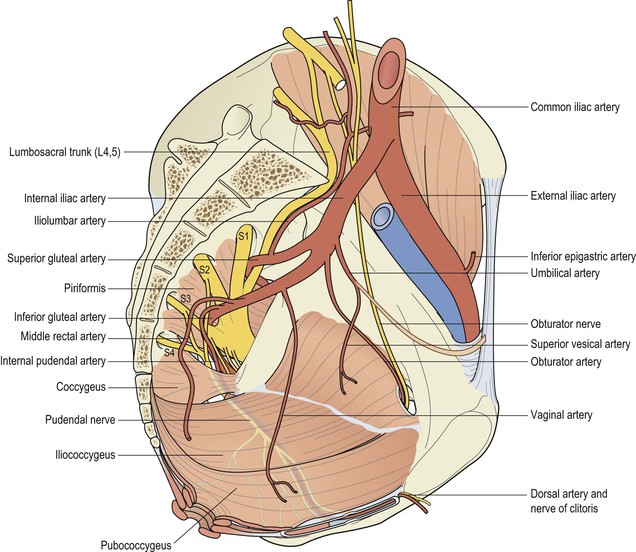
Vascular supply
The levator ani is supplied by branches of the inferior gluteal artery, the inferior vesical artery and the pudendal artery.
The pudendal nerve
The pudendal nerve is a mixed motor and sensory nerve and derives its fibres from the ventral branches of the second, third and fourth sacral nerves and leaves the pelvis through the lower part of the greater sciatic foramen. It then crosses the ischial spine and re-enters the pelvis through the lesser sciatic foramen. It accompanies the internal pudendal vessels upward and forward along the lateral wall of the ischioanal fossa, contained in a sheath of the obturator fascia termed Alcock's canal (Fig. 3.7). It is presumed that during a prolonged second stage of labour, the pudendal nerve is vulnerable to stretch injury due to its relative immobility at this site.
The inferior haemorrhoidal (rectal) nerve then branches off posteriorly from the pudendal nerve to innervate the EAS. The pudendal nerve then divides into two terminal branches: the perineal nerve and the dorsal nerve of the clitoris. The perineal nerve divides into posterior labial and muscular branches. The posterior labial branches supply the labium majora. The muscular branches are distributed to the superficial transverse perineal, bulbospongiosus, ischiocavernosus and constrictor urethræ muscles. The dorsal nerve of the clitoris, which innervates the clitoris, is the deepest division of the pudendal nerve (Fig. 3.8).

The pelvis
Knowledge of anatomy of a normal female pelvis is key to midwifery and obstetrics practice, as one of the ways to estimate a woman's progress in labour is by assessing the relationship of the fetus to certain bony landmarks of the pelvis. Understanding the normal pelvic anatomy helps to detect deviations from normal and facilitate appropriate care.
The pelvic girdle
The pelvic girdle is a basin-shaped cavity and consists of two innominate bones (hip bones), the sacrum and the coccyx. It is virtually incapable of independent movement except during childbirth as it provides the skeletal framework of the birth canal. It contains and protects the bladder, rectum and internal reproductive organs. In addition it provides an attachment for trunk and limb muscles. Some women experience pelvic girdle pain in pregnancy and need referral to a physiotherapist (see Chapter 12).
Innominate bones
Each innominate bone or hip bone is made up of three bones that have fused together: the ilium, the ischium and the pubis (Fig. 3.9). On its lateral aspect is a large, cup shaped acetabulum articulating with the femoral head, which is composed of the three fused bones in the following proportions: two-fifths ilium, two-fifths ischium and one-fifth pubis (Fig. 3.9). Anteroinferior to this is the large oval or triangular obturator foramen. The bone is articulated with its fellow to form the pelvic girdle.
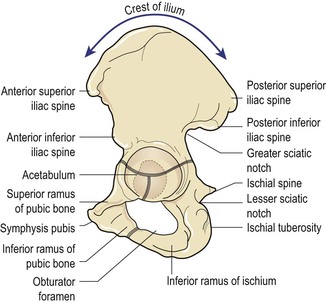
The ilium has an upper and lower part. The smaller lower part forms part of the acetabulum and the upper part is the large flared-out part. When the hand is placed on the hip, it rests on the iliac crest, which is the upper border. A bony prominence felt in front of the iliac crest is known as the anterior superior iliac spine. A short distance below it is the anterior inferior iliac spine. There are two similar points at the other end of the iliac crest, namely the posterior superior and the posterior inferior iliac spines. The internal concave anterior surface of the ilium is known as the iliac fossa.
The ischium is the inferoposterior part of the innominate bone and consists of a body and a ramus. Above it forms part of the acetabulum. Below its ramus ascends anteromedially at an acute angle to meet the descending pubic ramus and complete the obturator foramen. It has a large prominence known as the ischial tuberosity, on which the body rests when sitting. Behind and a little above the tuberosity is an inward projection, the ischial spine. This is an important landmark in midwifery and obstetric practice, as in labour, the station of the fetal head is estimated in relation to the ischial spines allowing assessment of progress of labour.
The pubis forms the anterior part. It has a body and two oar-like projections, the superior ramus and the inferior ramus. The two pubic bones meet at the symphysis pubis and the two inferior rami form the pubic arch, merging into a similar ramus on the ischium. The space enclosed by the body of the pubic bone, the rami and the ischium is called the obturator foramen.
The sacrum
The sacrum is a wedge-shaped bone consisting of five fused vertebrae, and forms the posterior wall of the pelvic cavity as it is wedged between the innominate bones. The caudal apex articulates with the coccyx and the upper border of the first sacral vertebra (sacral promontory) articulates with the first lumbar vertebra. The anterior surface of the sacrum is concave and is referred to as the hollow of the sacrum. Laterally the sacrum extends into a wing or ala. Four pairs of holes or foramina pierce the sacrum and, through these, nerves from the cauda equina emerge to innervate the pelvic organs. The posterior surface is roughened to receive attachments of muscles.
The coccyx
The coccyx is a vestigial tail. It consists of four fused vertebrae, forming a small triangular bone, which articulates with the fifth sacral segment.
Pelvic joints
There are four pelvic joints: one symphysis pubis, two sacroiliac joints and one sacrococcygeal joint.
The symphysis pubis is the midline cartilaginous joint uniting the rami of the left and right pubic bones.
The sacroiliac joints are strong, weight-bearing synovial joints with irregular elevations and depressions that produce interlocking of the bones. They join the sacrum to the ilium and as a result connect the spine to the pelvis. The joints allow a limited backward and forward movement of the tip and promontory of the sacrum, sometimes known as ‘nodding’ of the sacrum.
The sacrococcygeal joint is formed where the base of the coccyx articulates with the tip of the sacrum. It permits the coccyx to be deflected backwards during the birth of the fetal head.
Pelvic ligaments
The pelvic joints are held together by very strong ligaments that are designed not to allow movement. However, during pregnancy the hormone relaxin gradually loosens all the pelvic ligaments allowing slight pelvic movement providing more room for the fetal head as it passes through the pelvis. A widening of 2–3 mm at the symphysis pubis during pregnancy above the normal gap of 4–5 mm is normal but if it widens significantly, the degree of movement permitted may give rise to pain on walking.
The ligaments connecting the bones of the pelvis with each other can be divided into four groups:
• those connecting the sacrum and ilium – the sacroiliac ligaments;
• those passing between the sacrum and ischium – the sacrotuberous ligaments and the sacrospinous ligaments (Fig. 3.10);

• those uniting the sacrum and coccyx – the sacrococcygeal ligaments;
• those between the two pubic bones – the inter-pubic ligaments.
The pelvis in relation to pregnancy and childbirth
The term pelvis is applied to the skeletal ring formed by the innominate bones and the sacrum, the cavity within and even the entire region where the trunk and the lower limbs meet. The pelvis is divided by an oblique plane which passes through the prominence of the sacrum, the arcuate line (the smooth rounded border on the internal surface of the ilium), the pectineal line (a ridge on the superior ramus of the pubic bone) and the upper margin of the symphysis pubis, into the true and the false pelves.
The true pelvis
The true pelvis is the bony canal through which the fetus must pass during birth. It is divided into a brim, a cavity and an outlet.
The pelvic brim
The superior circumference forms the brim of the true pelvis, the included space being called the inlet. The brim is round except where the sacral promontory projects into it.
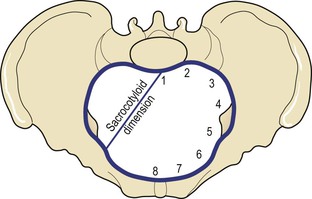
Midwives need to be familiar with the fixed points on the pelvic brim that are known as its landmarks. Commencing posteriorly, these are (Fig. 3.11):
The pelvic cavity
The cavity of the true pelvis extends from the brim superiorly to the outlet inferiorly. The anterior wall is formed by the pubic bones and symphysis pubis and its depth is 4 cm. The posterior wall is formed by the curve of the sacrum, which is 12 cm in length. Because there is such a difference in these measurements, the cavity forms a curved canal. With the woman upright, the upper portion of the pelvic canal is directed downward and backward, and its lower course curves and becomes directed downward and forward. Its lateral walls are the sides of the pelvis, which are mainly covered by the obturator internus muscle.
The cavity contains the pelvic colon, rectum, bladder and some of the reproductive organs. The rectum is placed posteriorly, in the curve of the sacrum and coccyx; the bladder is anterior behind the symphysis pubis.
The pelvic outlet
The lower circumference of the true pelvis is very irregular; the space enclosed by it is called the outlet. Two outlets are described: the anatomical and the obstetrical. The anatomical outlet is formed by the lower borders of each of the bones together with the sacrotuberous ligament. The obstetrical outlet is of greater practical significance because it includes the narrow pelvic strait through which the fetus must pass. The narrow pelvic strait lies between the sacrococcygeal joint, the two ischial spines and the lower border of the symphysis pubis. The obstetrical outlet is the space between the narrow pelvic strait and the anatomical outlet. This outlet is diamond-shaped.
The false pelvis
It is bounded posteriorly by the lumbar vertebrae and laterally by the iliac fossae, and in front by the lower portion of the anterior abdominal wall. The false pelvis varies considerably in size according to the flare of the iliac bones. However, the false pelvis has no significance in midwifery.
Pelvic diameters
Knowledge of the diameters of the normal female pelvis is essential in the practice of midwifery because contraction of any of them can result in malposition or malpresentation of the presenting part of the fetus.
Diameters of the pelvic inlet
The brim has four principal diameters: the anteroposterior diameter, the transverse diameter and the two oblique diameters (Figs 3.12, 3.13).


The anteroposterior or conjugate diameter extends from the midpoint of the sacral promontory to the upper border of the symphysis pubis. Three conjugate diameters can be measured: the anatomical (true) conjugate, the obstetrical conjugate and the internal or diagonal conjugate (Fig. 3.14).

The anatomical conjugate, which averages 12 cm, is measured from the sacral promontory to the uppermost point of the symphysis pubis. The obstetrical conjugate, which averages 11 cm, is measured from the sacral promontory to the posterior border of the upper surface of the symphysis pubis. This represents the shortest anteroposterior diameter through which the fetus must pass and is hence of clinical significance to midwives (Fig. 3.15). The obstetrical conjugate cannot be measured with the examining fingers or any other technique.

The diagonal conjugate is measured anteroposteriorly from the lower border of the symphysis to the sacral promontory.
The transverse diameter is constructed at right-angles to the obstetric conjugate and extends across the greatest width of the brim; its average measurement is about 13 cm.
Each oblique diameter extends from the iliopectineal eminence of one side to the sacroiliac articulation of the opposite side; its average measurement is about 12 cm. Each takes its name from the sacroiliac joint from which it arises, so the left oblique diameter arises from the left sacroiliac joint and the right oblique from the right sacroiliac joint.
Another dimension, the sacrocotyloid (see Fig. 3.11), passes from the sacral promontory to the iliopectineal eminence on each side and measures 9–9.5 cm. Its importance is concerned with posterior positions of the occiput when the parietal eminences of the fetal head may become caught (see Chapter 20).
Diameters of the cavity
The cavity is circular in shape and although it is not possible to measure its diameters exactly, they are all considered to be 12 cm (see Fig. 3.13).
Diameters of the outlet
The outlet, which is diamond-shaped, has three diameters: the anteroposterior diameter, the oblique diameter and the transverse diameter (see Fig. 3.13).
The anteroposterior diameter extends from the lower border of the symphysis pubis to the sacrococcygeal joint. It measures 13 cm; as the coccyx may be deflected backwards during labour, this diameter indicates the space available during birth.
The oblique diameter, although there are no fixed points, is said to be between the obturator foramen and the sacrospinous ligament. The measurement is taken as being 12 cm.
The transverse diameter extends between the two ischial spines and measures 10–11 cm. It is the narrowest diameter in the pelvis. The plane of least pelvic dimensions is said to be at the level of the ischial spines.
Orientation of the pelvis
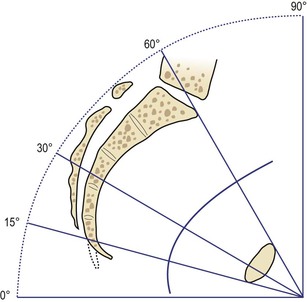
In the standing position, the pelvis is placed such that the anterior superior iliac spine and the front edge of the symphysis pubis are in the same vertical plane, perpendicular to the floor. If the line joining the sacral promontory and the top of the symphysis pubis were to be extended, it would form an angle of 60° with the horizontal floor. Similarly, if a line joining the centre of the sacrum and the centre of the symphysis pubis were to be extended, the resultant angle with the floor would be 30°. The angle of inclination of the outlet is 15° (Fig. 3.16). When in the recumbent position, the same angles are made as in the vertical position; this fact should be kept in mind when carrying out an abdominal examination.
Pelvic planes
Pelvic planes are imaginary flat surfaces at the brim, cavity and outlet of the pelvic canal at the levels of the lines described above (Fig. 3.17).

Axis of the pelvic canal
A line drawn exactly half-way between the anterior wall and the posterior wall of the pelvic canal would trace a curve known as the curve of Carus. The midwife needs to become familiar with this concept in order to make accurate observations on vaginal examination and to facilitate the birth of the baby.
The four types of pelvis
The size of the pelvis varies not only in the two sexes, but also in different members of the same sex. The height of the individual does not appear to influence the size of the pelvis in any way, as women of short stature, in general, have a broad pelvis. Nevertheless, the pelvis is occasionally equally contracted in all its dimensions, so much so that all its diameters can measure 1.25 cm less than the average. This type of pelvis, known as a justo minor pelvis, can result in normal labour and birth if the fetal size is consistent with the size of the maternal pelvis. However, if the fetus is large, a degree of cephalopelvic disproportion will result. The same is true when a malpresentation or malposition of the fetus exists.
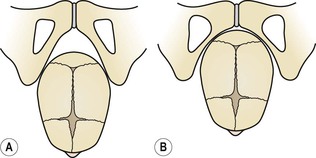
The principal divergences, however, are found at the brim (Fig. 3.18) and affect the relation of the anteroposterior to the transverse diameter. If one of the measurements is reduced by 1 cm or more from the normal, the pelvis is said to be contracted and may give rise to difficulty in labour or necessitate caesarean section.
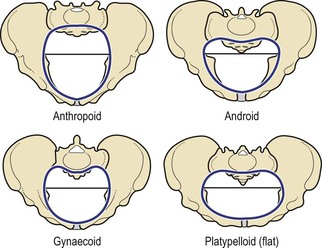
Classically, pelves have been described as falling into four categories: the gynaecoid pelvis, the android pelvis, the anthropoid pelvis and the platypelloid pelvis (Table 3.1).
Table 3.1
Features of the four types of pelvis
| Features | Gynaecoid | Android | Anthropoid | Platypelloid |
| Brim | Rounded | Heart-shaped | Long oval | Kidney-shaped |
| Forepelvis | Generous | Narrow | Narrowed | Wide |
| Side walls | Straight | Convergent | Divergent | Divergent |
| Ischial spines | Blunt | Prominent | Blunt | Blunt |
| Sciatic notch | Rounded | Narrow | Wide | Wide |
| Sub-pubic angle | 90° | <90° | >90° | >90° |
| Incidence | 50% | 20% | 25% (50% in non-Caucasian) | 5% |

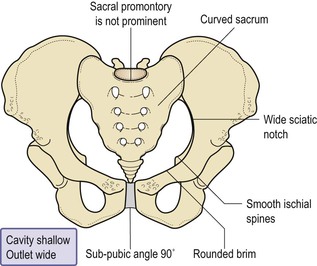
The gynaecoid pelvis (Fig. 3.19)
This is the best type for childbearing as it has a rounded brim, generous forepelvis, straight side walls, a shallow cavity with a well-curved sacrum and a sub-pubic arch of 90°.
The android pelvis
The android pelvis is so called because it resembles the male pelvis. Its brim is heart-shaped, it has a narrow forepelvis and its transverse diameter is situated towards the back. The side walls converge, making it funnel-shaped, and it has a deep cavity and a straight sacrum. The ischial spines are prominent and the sciatic notch is narrow. The sub-pubic angle is less than 90°. It is found in short and heavily built women, who have a tendency to be hirsute.
Because of the narrow forepelvis and the fact that the greater space lies in the hindpelvis the heart-shaped brim favours an occipitoposterior position. Furthermore, funnelling in the cavity may hinder progress in labour. At the pelvic outlet, the prominent ischial spines sometimes prevent complete internal rotation of the head and the anteroposterior diameter becomes caught on them, causing a deep transverse arrest. The narrowed sub-pubic angle cannot easily accommodate the biparietal diameter (Fig. 3.20) and this displaces the head backwards. Because of these factors, this type of pelvis is the least suited to childbearing.
The anthropoid pelvis
The anthropoid pelvis has a long, oval brim in which the anteroposterior diameter is longer than the transverse diameter. The side walls diverge and the sacrum is long and deeply concave. The ischial spines are not prominent and the sciatic notch and the sub-pubic angle are very wide. Women with this type of pelvis tend to be tall, with narrow shoulders. Labour does not usually present any difficulties, but a direct occipitoanterior or direct occipitoposterior position is often a feature and the position adopted for engagement may persist to birth.
The platypelloid pelvis
The platypelloid (flat) pelvis has a kidney-shaped brim in which the anteroposterior diameter is reduced and the transverse diameter increased. The sacrum is flat and the cavity shallow. The ischial spines are blunt, and the sciatic notch and the sub-pubic angle are both wide. The head must engage with the sagittal suture in the transverse diameter, but usually descends through the cavity without difficulty. Engagement may necessitate lateral tilting of the head, known as asynclitism, in order to allow the biparietal diameter to pass the narrowest anteroposterior diameter of the brim (Box 3.1).
Other pelvic variations
High assimilation pelvis occurs when the 5th lumbar vertebra is fused to the sacrum and the angle of inclination of the pelvic brim is increased. Engagement of the head is difficult but, once achieved, labour progresses normally.
Deformed pelvis may result from a developmental anomaly, dietary deficiency, injury or disease (Box 3.2).
Box 3.2
Deformed pelves
Developmental anomalies
The Naegele's and Robert's pelves are rare malformations caused by a failure in development. In the Naegele's pelvis, one sacral ala is missing and the sacrum is fused to the ilium causing a grossly asymmetric brim. The Robert's pelvis has similar malformations which are bilateral. In both instances, the abnormal brim prevents engagement of the fetal head.
Dietary deficiency
Deficiency of vitamins and minerals necessary for the formation of healthy bones is less frequently seen today than in the past but might still complicate pregnancy and labour to some extent.
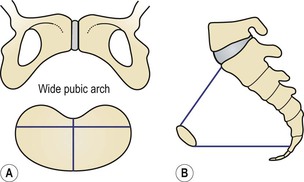
A rachitic pelvis is a pelvis deformed by rickets in early childhood, as a consequence of malnutrition. The weight of the upper body presses downwards on to the softened pelvic bones, the sacral promontory is pushed downwards and forwards and the ilium and ischium are drawn outwards resulting in a flat pelvic brim similar to that of the platypelloid pelvis (Fig. 3.21). The sacrum tends to be straight, with the coccyx bending acutely forward. Because the tuberosities are wide apart, the pubic arch is wide. The clinical signs of rickets are bow legs and spinal deformity.
If severe contraction is present, caesarean section is required to deliver the baby. The fetal head will attempt to enter the pelvis by asynclitism.
Osteomalacic pelvis. The disease osteomalacia is rarely encountered in the United Kingdom. It is due to an acquired deficiency of calcium and occurs in adults. All bones of the skeleton soften because of gross calcium deficiency. The pelvic canal is squashed together until the brim becomes a Y-shaped slit. Labour is impossible. In early pregnancy, incarceration of the gravid uterus may occur because of the gross deformity.
Injury and disease
Trauma. A pelvis that has been fractured will develop callus formation or may fail to unite correctly. This may lead to reduced measurements and therefore to some degree of contraction. Conditions sustained in childhood such as fractures of the pelvis or lower limbs, congenital dislocation of the hip and poliomyelitis may lead to unequal weight-bearing, which will also cause deformity.
Spinal deformity. If kyphosis (forward angulation) or scoliosis (lateral curvature) is evident, or is suggested by a limp or deformity, the midwife must refer the woman to a doctor. Pelvic contraction is likely in these cases.
The female reproductive system
The female reproductive system consists of the external genitalia, known collectively as the vulva, and the internal reproductive organs: the vagina, the uterus, two uterine tubes and two ovaries. In the non-pregnant state, the internal reproductive organs are situated within the true pelvis.
The vagina
The vagina is a hollow, distensible fibromuscular tube that extends from the vestibule to the cervix. It is approximately 10 cm in length and 2.5 cm in diameter (although there is wide anatomical variation). During sexual intercourse and when a woman gives birth, the vagina temporarily widens and lengthens.
The vaginal canal passes upwards and backwards into the pelvis with the anterior and posterior walls in close contact along a line approximately parallel to the plane of the pelvic brim. When the woman stands upright, the vaginal canal points in an upward-backward direction and forms an angle of slightly more than 45° with the uterus.
Function
The vagina allows the escape of the menstrual fluids, receives the penis and the ejected sperm during sexual intercourse, and provides an exit for the fetus during birth.
Relations
Knowledge of the relations of the vagina to other pelvic organs is essential for the accurate examination of the pregnant woman and the safe birth of the baby (Figs 3.22, 3.23).
• Anterior to the vagina lie the bladder and the urethra, which are closely connected to the anterior vaginal wall.
• Posterior to the vagina lie the pouch of Douglas, the rectum and the perineal body, which separates the vagina from the anal canal.
• Laterally on the upper two-thirds are the pelvic fascia and the ureters, which pass beside the cervix; on either side of the lower third are the muscles of the pelvic floor.


Structure
The posterior wall of the vagina is 10 cm long whereas the anterior wall is only 7.5 cm in length; this is because the cervix projects into its upper part at a right-angle.
The upper end of the vagina is known as the vault. Where the cervix projects into it, the vault forms a circular recess that is described as four arches or fornices. The posterior fornix is the largest of these because the vagina is attached to the uterus at a higher level behind than in front. The anterior fornix lies in front of the cervix and the lateral fornices lie on either side.
Layers
The vaginal wall is composed of three layers: mucosa, muscle and fascia. The mucosa is the most superficial layer and consists of stratified, squamous non-keratinized epithelium, thrown in transverse folds called rugae. These allow the vaginal walls to stretch during intercourse and childbirth. Beneath the epithelium lies a layer of vascular connective tissue. The muscle layer is divided into a weak inner coat of circular fibres and a stronger outer coat of longitudinal fibres. Pelvic fascia surrounds the vagina and adjacent pelvic organs and allows for their independent expansion and contraction.
There are no glands in the vagina; however, it is moistened by mucus from the cervix and a transudate that seeps out from the blood vessels of the vaginal wall.
In spite of the alkaline mucus, the vaginal fluid is strongly acid (pH 4.5) owing to the presence of lactic acid formed by the action of Doderlein's bacilli on glycogen found in the squamous epithelium of the lining. These lactobacilli are normal inhabitants of the vagina. The acid deters the growth of pathogenic bacteria.
Blood supply
The blood supply comes from branches of the internal iliac artery and includes the vaginal artery and a descending branch of the uterine artery. The blood drains through corresponding veins.
Lymphatic drainage
Lymphatic drainage is via the inguinal, the internal iliac and the sacral glands.
Nerve supply
The nerve supply is derived from the pelvic plexus. The vaginal nerves follow the vaginal arteries to supply the vaginal walls and the erectile tissue of the vulva.
The uterus
The uterus is a hollow, pear-shaped muscular organ located in the true pelvis between the bladder and the rectum. The position of the uterus within the true pelvis is one of anteversion and anteflexion. Anteversion means that the uterus leans forward and anteflexion means that it bends forwards upon itself. When the woman is standing, the uterus is in an almost horizontal position with the fundus resting on the bladder if the uterus is anteverted (see Fig. 3.23).
Function
The main function of the uterus is to nourish the developing fetus prior to birth. It prepares for pregnancy each month and following pregnancy expels the products of conception.
Relations
Knowledge of the relations of the uterus to other pelvic organs (Figs 3.24, 3.25) is desirable, particularly when giving women advice about bladder and bowel care during pregnancy and childbirth.


Supports
The uterus is supported by the pelvic floor and maintained in position by several ligaments, of which those at the level of the cervix (Fig. 3.24) are the most important.
• The transverse cervical ligaments fan out from the sides of the cervix to the side walls of the pelvis. They are sometimes known as the ‘cardinal ligaments’ or ‘Mackenrodt’s ligaments’.
• The uterosacral ligaments pass backwards from the cervix to the sacrum.
• The pubocervical ligaments pass forwards from the cervix, under the bladder, to the pubic bones.
• The broad ligaments are formed from the folds of peritoneum, which are draped over the uterine tubes. They hang down like a curtain and spread from the sides of the uterus to the side walls of the pelvis.
• The round ligaments have little value as a support but tend to maintain the anteverted position of the uterus; they arise from the cornua of the uterus, in front of and below the insertion of each uterine tube, and pass between the folds of the broad ligament, through the inguinal canal, to be inserted into each labium majus.
• The ovarian ligaments also begin at the cornua of the uterus but behind the uterine tubes and pass down between the folds of the broad ligament to the ovaries.
It is helpful to note that the round ligament, the uterine tube and the ovarian ligament are very similar in appearance and arise from the same area of the uterus. This makes careful identification important when tubal surgery is undertaken.
Structure
The non-pregnant uterus is 7.5 cm long, 5 cm wide and 2.5 cm in depth, each wall being 1.25 cm thick (see Fig. 3.25). The cervix forms the lower third of the uterus and measures 2.5 cm in each direction. The uterus consists of the following parts:
• The cornua are the upper outer angles of the uterus where the uterine tubes join.
• The fundus is the domed upper wall between the insertions of the uterine tubes.
• The body or corpus makes up the upper two-thirds of the uterus and is the greater part.
• The cavity is a potential space between the anterior and posterior walls. It is triangular in shape, the base of the triangle being uppermost.
• The isthmus is a narrow area between the cavity and the cervix, which is 7 mm long. It enlarges during pregnancy to form the lower uterine segment.
• The cervix or neck protrudes into the vagina. The upper half, being above the vagina, is known as the supravaginal portion while the lower half is the infravaginal portion.
• The internal os (mouth) is the narrow opening between the isthmus and the cervix.
• The external os is a small round opening at the lower end of the cervix. After childbirth, it becomes a transverse slit.
• The cervical canal lies between these two ostia and is a continuation of the uterine cavity. This canal is shaped like a spindle, narrow at each end and wider in the middle.
Layers
The uterus has three layers: the endometrium, the myometrium and the perimetrium, of which the myometrium, the middle muscle layer, is by far the thickest.
The endometrium forms a lining of ciliated epithelium (mucous membrane) on a base of connective tissue or stroma. In the uterine cavity, this endometrium is constantly changing in thickness throughout the menstrual cycle (see Chapter 5). The basal layer does not alter, but provides the foundation from which the upper layers regenerate. The epithelial cells are cubical in shape and dip down to form glands that secrete an alkaline mucus.
The cervical endometrium does not respond to the hormonal stimuli of the menstrual cycle to the same extent. Here the epithelial cells are tall and columnar in shape and the mucus-secreting glands are branching racemose glands. The cervical endometrium is thinner than that of the body and is folded into a pattern known as the ‘arbor vitae’ (tree of life). This is thought to assist the passage of the sperm. The portion of the cervix that protrudes into the vagina is covered with squamous epithelium similar to that lining the vagina. The point where the epithelium changes, at the external os, is termed the squamo-columnar junction.
The myometrium is thick in the upper part of the uterus and is sparser in the isthmus and cervix. Its fibres run in all directions and interlace to surround the blood vessels and lymphatics that pass to and from the endometrium. The outer layer is formed of longitudinal fibres that are continuous with those of the uterine tube, the uterine ligaments and the vagina.
In the cervix, the muscle fibres are embedded in collagen fibres, which enable it to stretch in labour.
The perimetrium is a double serous membrane, an extension of the peritoneum, which is draped over the fundus and the anterior surface of the uterus to the level of the internal os. It is then reflected onto the bladder forming a small pouch between the uterus and the bladder called the uterovesical pouch. The posterior surface is covered to where the cervix protrudes into the vagina and is then reflected onto the rectum forming the recto-uterine pouch. Laterally the perimetrium extends over the uterine tubes forming a double fold, the broad ligament, leaving the lateral borders of the body uncovered.
Blood supply
The uterine artery arrives at the level of the cervix and is a branch of the internal iliac artery. It sends a small branch to the upper vagina, and then runs upwards in a twisted fashion to meet the ovarian artery and form an anastomosis with it near the cornu. The ovarian artery is a branch of the abdominal aorta, leaving near the renal artery. It supplies the ovary and uterine tube before joining the uterine artery. The blood drains through corresponding veins (Fig. 3.26).

Lymphatic drainage
Lymph is drained from the uterine body to the internal iliac glands and from the cervical area to many other pelvic lymph glands. This provides an effective defence against uterine infection.
Nerve supply
The nerve supply is mainly from the autonomic nervous system, sympathetic and parasympathetic, via the inferior hypogastric or pelvic plexus.
Uterine malformations
The prevalence of uterine malformation is estimated to be 6.7% in the general population. The female genital tract is formed in early embryonic life when a pair of ducts develops. These paramesonephric or Müllerian ducts come together in the midline and fuse into a Y-shaped canal. The open upper ends of this structure lead into the peritoneal cavity and the unfused portions become the uterine tubes. The fused lower portion forms the uterovaginal area, which further develops into the uterus and vagina. Abnormal development of the Müllerian duct(s) during embryogenesis can lead to uterine abnormalities (Box 3.3) (Fig. 3.27).
Box 3.3
Uterine malformations
Types of uterine malformation
Various types of structural abnormality can result from failure of fusion of the Müllerian ducts. Three of these abnormalities can be seen in Fig. 3.27. A double uterus with an associated double vagina will develop where there has been complete failure of fusion. Partial fusion results in various degrees of duplication. A single vagina with a double uterus is the result of fusion at the lower end of the ducts only. A bicornuate uterus (one with two horns) is the result of incomplete fusion at the upper portion of the uterovaginal area. In rare cases, one Müllerian duct regresses and the result is a uterus with one horn – termed a unicornuate uterus.

Structural abnormality of the uterus can lead to various problems during pregnancy and childbirth. The outcome depends on the ability of the uterus to accommodate the growing fetus. A problem exists only if the tissue is insufficient to allow the uterus to enlarge for a full-term fetus lying longitudinally. If there is insufficient hypertrophy, the possible difficulties are miscarriage, premature labour and abnormal lie of the fetus. In labour, poor uterine function may be experienced. Minor defects of structure cause little problem and might pass unnoticed, with the woman having a normal outcome to her pregnancy. Occasionally problems arise when a fetus is accommodated in one horn of a double uterus and the empty horn has filled the pelvic cavity. In this situation, the empty horn has grown owing to the hormonal influences of the pregnancy, and its size and position will cause obstruction during labour. Caesarean section would be the method of delivery.
The fallopian tubes
The uterine tubes, also known as fallopian tubes, oviducts and salpinges, are two very fine tubes leading from the ovaries into the uterus.
Function
The uterine tube propels the ovum towards the uterus, receives the spermatozoa as they travel upwards and provides a site for fertilization. It supplies the fertilized ovum with nutrition during its continued journey to the uterus.
Position
The uterine tubes extend laterally from the cornua of the uterus towards the side walls of the pelvis. They arch over the ovaries, the fringed ends hovering near the ovaries in order to receive the ovum.
Supports
The uterine tubes are held in place by their attachment to the uterus. The peritoneum folds over them, draping down below as the broad ligaments and extending at the sides to form the infundibulopelvic ligaments.
Structure
Each tube is 10 cm long. The lumen of the tube provides an open pathway from the outside to the peritoneal cavity. The uterine tube has four portions (Fig. 3.28):
• The interstitial portion is 1.25 cm long and lies within the wall of the uterus. Its lumen is 1 mm wide.
• The isthmus is another narrow part that extends for 2.5 cm from the uterus.
• The ampulla is the wider portion, where fertilization usually occurs. It is 5 cm long.
• The infundibulum is the funnel-shaped fringed end that is composed of many processes known as fimbriae. One fimbria is elongated to form the ovarian fimbria, which is attached to the ovary.

Layers (Fig. 3.29)
The lining of the uterine tubes is a mucous membrane of ciliated cubical epithelium that is thrown into complicated folds known as plicae. These folds slow the ovum down on its way to the uterus. In this lining are goblet cells that produce a secretion containing glycogen to nourish the oocyte.

Beneath the lining is a layer of vascular connective tissue.
The muscle coat consists of two layers: an inner circular layer and an outer longitudinal layer, both of smooth muscle. The peristaltic movement of the uterine tube is due to the action of these muscles.
The tube is covered with peritoneum but the infundibulum passes through it to open into the peritoneal cavity.
Blood supply
The blood supply is via the uterine and ovarian arteries, returning by the corresponding veins.
Lymphatic drainage
Lymph is drained to the lumbar glands.
Nerve supply
The nerve supply is from the ovarian plexus.
The ovaries
The ovaries are components of the female reproductive system and the endocrine system.
Function
The ovaries produce oocytes and the hormones, oestrogen and progesterone.
Position
The ovaries are attached to the back of the broad ligaments within the peritoneal cavity.
Relations
• Anterior to the ovaries are the broad ligaments.
• Posterior to the ovaries are the intestines.
• Lateral to the ovaries are the infundibulopelvic ligaments and the side walls of the pelvis.
• Superior to the ovaries lie the uterine tubes.
• Medial to the ovaries lie the ovarian ligaments and the uterus.
Supports
The ovary is attached to the broad ligament but is supported from above by the ovarian ligament medially and the infundibulopelvic ligament laterally.
Structure
The ovary is composed of a medulla and cortex, covered with germinal epithelium.
The medulla is the supporting framework, which is made of fibrous tissue; the ovarian blood vessels, lymphatics and nerves travel through it. The hilum where these vessels enter lies just where the ovary is attached to the broad ligament and this area is called the mesovarium (see Fig. 3.29).
The cortex is the functioning part of the ovary. It contains the ovarian follicles in different stages of development, surrounded by stroma. The outer layer is formed of fibrous tissue known as the tunica albuginea. Over this lies the germinal epithelium, which is a modification of the peritoneum.
The cycle of the ovary is described in Chapter 5.
Blood supply
Blood is supplied to the ovaries from the ovarian arteries and drains via the ovarian veins. The right ovarian vein joins the inferior vena cava, but the left returns its blood to the left renal vein.
Lymphatic drainage
Lymphatic drainage is to the lumbar glands.
Nerve supply
The nerve supply is from the ovarian plexus.
The male reproductive system
The male reproductive system (Fig. 3.30) consists of a set of organs that are partly visible and partly hidden within the body. The visible parts are the scrotum and the penis. Inside the body are the prostate gland and tubes that link the system together. The male organs produce and transfer sperm to the female for fertilization. The organs are the scrotum, testis, rete and epididymis, ductus deferens, seminal vesicles prostate gland, bulbourethral glands and penis with the urethra.

The scrotum
The scrotum is part of the external genitalia. Also called the scrotal sac, the scrotum is a thin-walled, soft, muscular pouch located below the symphysis pubis, between the upper parts of the thighs behind the penis.
Function
The scrotum forms a pouch in which the testes are suspended outside the body, keeping them at a temperature slightly lower than that of the rest of the body. A temperature around 34.4 °C enables the production of viable sperm, whereas a temperature of or above 36.7 °C can be damaging to sperm count.
Structure
The scrotum is formed of pigmented skin and has two compartments, one for each testis.
The testes
Like the ovaries, to which they are homologous, the testes (also known as testicles) are components of both the reproductive system and the endocrine system. Each testis weighs about 25 g.
Function
The testes produce and store spermatozoa, and are the body's main source of the male hormone testosterone. Testosterone is responsible for the development of secondary sex characteristics.
Position
In the embryo, the testes develop high up in the lumbar region of the abdominal cavity. In the last few months of fetal life they descend through the abdomen, over the pelvic brim and down the inguinal canal into the scrotum outside the body. The testes are contained within the scrotum.
Structure
Each testis is an oval structure about 5 cm long and 3 cm in diameter.
Layers
There are three layers to the testis:
The tunica vasculosa is an inner layer of connective tissue containing a fine network of capillaries.
The tunica albuginea is a fibrous covering, ingrowths of which divide the testis into 200–300 lobules.
The tunica vaginalis is the outer layer, which is made of peritoneum brought down with the descending testis when it migrated from the lumbar region in fetal life.
The duct system within the testes is highly intricate:
The seminiferous (‘seed-carrying’) tubules are where spermatogenesis, or production of sperm, takes place. There are up to three of them in each lobule. Between the tubules are interstitial cells that secrete testosterone. The tubules join to form a system of channels that lead to the epididymis.
The epididymis is a comma-shaped, coiled tube that lies on the superior surface and travels down the posterior aspect to the lower pole of the testis, where it leads into the deferent duct or vas deferens.
The spermatic cord
The spermatic cord is the name given to the cord-like structure consisting of the vas deferens and its accompanying arteries, veins, nerves and lymphatic vessels.
Function
The function of the deferent duct is to carry the sperm to the ejaculatory duct.
Position
The cord passes upwards through the inguinal canal, where the different structures diverge. The deferent duct then continues upwards over the symphysis pubis and arches backwards beside the bladder. Behind the bladder, it merges with the duct from the seminal vesicle and passes through the prostate gland as the ejaculatory duct to join the urethra.
Blood supply
The testicular artery, a branch of the abdominal aorta, supplies the testes, scrotum and attachments. The testicular veins drain in the same manner as the ovarian veins.
Lymphatic drainage
Lymphatic drainage is to the lymph nodes round the aorta.
Nerve supply
The nerve supply to the spermatic cord is from the 10th and 11th thoracic nerves.
The seminal vesicles
The seminal vesicles are a pair of simple tubular glands.
Function
The function of the seminal vesicles is production of a viscous secretion to keep the sperm alive and motile. This secretion ultimately becomes semen.
Position
The seminal vesicles are situated posterior to the bladder and superior to the prostate gland.
Structure
The seminal vesicles are 5 cm long and pyramid-shaped. They are composed of columnar epithelium, muscle tissue and fibrous tissue.
The ejaculatory ducts
These small muscular ducts carry the spermatozoa and the seminal fluid to the urethra.
The prostate gland
The prostate is an exocrine gland of the male reproductive system.
Function
The prostate gland produces a thin lubricating fluid that enters the urethra through ducts.
Position
The prostate gland surrounds the urethra at the base of the bladder, lying between the rectum and the symphysis pubis.
Structure
The prostate gland measures 4 × 3 × 2 cm. It is composed of columnar epithelium, a muscle layer and an outer fibrous layer.
The bulbourethral glands
The bulbourethral glands are two very small glands, which produce yet another lubricating fluid that passes into the urethra just below the prostate gland.
The penis
The penis is the male reproductive organ and additionally serves as the external male organ of urination.
Functions
The penis carries the urethra, which is a passage for both urine and semen. During sexual excitement it stiffens (an erection) in order to be able to penetrate the vagina and deposit the semen near the woman's cervix.
Position
The root of the penis lies in the perineum, from where it passes forward below the symphysis pubis. The lower two-thirds are outside the body in front of the scrotum.
Structure
The penis has three columns of erectile tissue:
The corpora cavernosa are two lateral columns that lie one on either side in front of the urethra.
The corpus spongiosum is the posterior column that contains the urethra. The tip is expanded to form the glans penis.
The lower two-thirds of the penis are covered in skin. At the end, the skin is folded back on itself above the glans penis to form the prepuce or foreskin, which is a movable double fold. The penis is extremely vascular and during an erection the blood spaces fill and become distended.
The male hormones
The control of the male gonads is similar to that in the female, but it is not cyclical. The hypothalamus produces gonadotrophin-releasing factors. These stimulate the anterior pituitary gland to produce follicle stimulating hormone (FSH) and luteinizing hormone (LH). FSH acts on the seminiferous tubules to bring about the production of sperm, whereas LH acts on the interstitial cells that produce testosterone.
Testosterone is responsible for the secondary sex characteristics: deepening of the voice, growth of the genitalia and growth of hair on the chest, pubis, axilla and face.
Formation of the spermatozoa
Production of sperm begins at puberty and continues throughout adult life. Spermatogenesis takes place in the seminiferous tubules under the influence of FSH and testosterone. The process of maturation is a lengthy one and takes some weeks. The mature sperm are stored in the epididymis and the deferent duct until ejaculation. If this does not happen, they degenerate and are reabsorbed. At each ejaculation, 2–4 ml of semen is deposited in the vagina. The seminal fluid contains about 100 million sperm/ml, of which 20–25% are likely to be abnormal. The remainder move at a speed of 2–3 mm/min. The individual spermatozoon has a head, a body and a long, mobile tail that lashes to propel the sperm along (Fig. 3.31). The tip of the head is covered by an acrosome; this contains enzymes to dissolve the covering of the oocyte in order to penetrate it.
