Chapter 91 Abdominal Wall Reconstruction
1 What is the functional role of the abdominal wall?
The abdominal wall consists of vertically, obliquely, and transversely oriented muscles that play a key role in posture maintenance, standing, walking, bending, and lifting. The abdominal wall muscles also protect the abdominal viscera and increase intraabdominal pressure to aid in coughing, vomiting, defecation, micturition, and parturition. The muscles also serve an important role in respiration.
2 What are the layers of the abdominal wall?
3 What are the origins and insertions of the abdominal wall muscles?
The external oblique muscle is the most superficial and largest of the three muscles in the lateral aspect of the abdominal wall. It arises from the lower eight ribs and interdigitates with the serratus anterior and latissimus dorsi muscles. It inserts on the anterior half of the iliac crest; inferiorly its aponeurosis forms the inguinal ligament (Poupart’s ligament), which extends from the anterosuperior iliac spine to the pubic spine. Its fascicles are directed in a superolateral to inferomedial direction. Its aponeurosis passes anterior to the rectus abdominis muscle.
The internal oblique muscle lies beneath the external oblique and its fibers course in an opposite direction. Originates from lumbodorsal fascia, anterior two thirds of iliac crest, and lateral two thirds of the inguinal ligament. The lower fibers join those of the transverses abdominis muscle to form the conjoined tendon, which inserts on the pubic crest and spine and on the iliopectineal line. The superior fibers insert as a broad aponeurosis into the linea alba and cartilages of the seventh to ninth ribs. Its aponeurosis splits above the arcuate line to envelope the rectus abdominis. Below the arcuate line it passes anterior to the rectus abdominis.
The transversus abdominis muscle is located deep to the internal oblique muscle. It is the deepest and smallest of the muscles of the lateral abdominal wall. It originates from the lower six ribs, lumbodorsal fascia, anterior two thirds of the iliac crest, and lateral third of the inguinal ligament. It inserts on the linea alba and contributes to the conjoined tendon that inserts on the pubic spine and iliopectineal line.
The rectus abdominis muscle is a longitudinal muscle located in the medial aspect of the abdominal wall. It arises from the front of the symphysis and pubic crest and inserts on the xiphoid process and cartilages of the fifth through seventh ribs.
The pyramidalis muscle is present in 80% to 90% of patients. It is a small triangular muscle that lies superficial to the rectus muscle. It arises from the front of the pubis and inserts on the linea alba halfway between the symphysis and umbilicus.
4 What are the functions of the abdominal wall muscles?
The rectus muscles flex the body anteriorly and are important in climbing into and out of bed. The external and internal oblique muscles are important in rotating the upper body against the lower body. Trunk rotation results from the joint contraction of one external oblique and the contralateral internal oblique. The vertical component of the oblique musculature can substitute for the rectus muscles if they are absent.
5 What fascial layer lines the entire abdominal wall?
The transversalis fascia is an internal investing fascia that lines the entire abdominal wall. It exists on the deep surface of the transversus abdominis fascia and is continuous from side to side deep to the linea alba. It extends into the thigh to form the femoral sheath. In the inguinal canal it forms the internal spermatic fascia. Internal to this layer is the peritoneum.
6 What is the arterial supply to the abdominal wall?
7 Describe the three vascular zones of the abdominal wall
The midabdomen is supplied by the deep epigastric arcade (zone I), the lower abdomen by the external iliac artery (zone II), and the lateral abdomen by the intercostal, subcostal, and lumbar arteries (zone III; Fig. 91-1). After an abdominoplasty, the majority of the abdominal wall skin is supplied by intercostal lumbar perforating arteries of zone III.
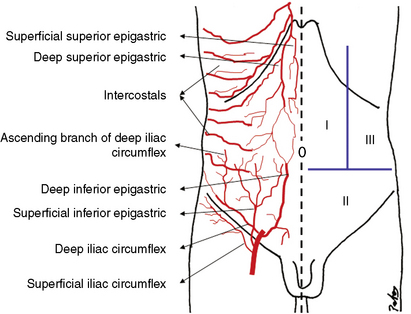
Figure 91-1 Vascular zones of the abdominal wall. Zone I, deep epigastric arcade; zone II, external iliac branches; zone III, intercostal, subcostal, and lumbar arteries.
(Courtesy Patricio Andrades, MD, Clinical and Research Fellow, Division of Plastic Surgery and Transplant Immunology, Division of Plastic Surgery, University of Alabama at Birmingham, Birmingham, Alabama.)
8 What are the venous and lymphatic drainages of the abdominal wall?
The venous drainage parallels the arterial supply to the abdominal wall. The upper abdomen is drained by the superior epigastric, intercostal, and axillary veins. The lower abdomen is drained by the superficial inferior epigastric, superficial circumflex iliac, and deep inferior epigastric veins.
The lymphatic drainage is divided by the umbilicus. Above the umbilicus, the superficial and deep lymphatics drain into the ipsilateral axillary and internal mammary lymph nodes, respectively.
Below the umbilicus, superficial and deep lymphatics flow into the ipsilateral inguinal and deep iliac lymph nodes, respectively.
9 What is the motor and sensory innervation to the abdominal wall?
The nerve supply to the abdominal wall is predominantly from intercostal nerves. A neurovascular plane exists between the internal oblique and transversus abdominis muscles. Through this plane pass the nerves as well as intercostal blood vessels that supply the abdominal wall. The main trunks of the anterior cutaneous rami nerves are found in this neurovascular plane as they pass anteriorly to provide sensation to the overlying skin. There is slight overlap of the sensory dermatomes. Motor innervation of the abdominal obliques and transversalis muscles are from the lower thoracic and lumbar dorsal rami. Motor innervation to the rectus abdominis is from the fifth through twelfth intercostal nerves. The ilioinguinal and iliohypogastric nerves pass between the internal oblique and transversus abdominis muscles as they extend from the lateral costal margin to the pubic region. Although they do not supply innervation to the abdomen, their course can be disrupted with dissection in the lateral abdomen. Loss of function results in sensory defects in the medial thigh and groin.
10 Describe the mechanism by which an adynamic abdominal wall contributes to lumbosacral pain
Patients with an adynamic segment of the abdominal wall as a result of ventral hernia or adynamic reconstruction and those with a decreased efficiency of the abdominal wall musculature from diastasis are prone to development of lumbodorsal back pain. The internal oblique–transversus abdominis complex fuses to the anterior and middle layers of the lumbodorsal fascia. Gracovetsky et al. demonstrated that contraction of these muscles tightens the lumbodorsal fascia, adding ligamentous support to the fixed spine and reducing the need for back muscle action with a resultant increase in lumbosacral disc pressure. When an adynamic or “stretched out” segment exists, the internal oblique and transversus abdominis are not stretched to physiologic length. This laxity prevents maximum force generation with contraction and weakens support by means of the lumbodorsal fascia. Toranto et al. demonstrated complete relief of back pain in 24 of 25 patients treated with wide rectus placation.
12 What are important considerations in the evaluation of abdominal wall defects?
13 What studies aid in the evaluation of abdominal wall defects?
Computed tomographic scans and magnetic resonance imaging studies may be helpful in evaluating the extent of tumor invasion and the integrity of potential muscle or musculocutaneous flaps to be used in reconstruction. The vascular status of these flaps can be determined by color flow duplex Doppler study that combines Doppler ultrasound and B-mode ultrasound to produce images of blood vessels and their surroundings. A fistulogram or intestinal contrast study may be needed to evaluate for the presence of gastrointestinal fistulas.
14 How are acquired abdominal wall defects managed?
Acute Traumatic Wounds: Temporizing measures such as a wound vacuum-assisted closure (VAC), Vicryl mesh, x-ray cassette cover, vacuum pack, and Velcro mesh (Whitman patch) provide coverage while the acute problems are addressed. Varying rates of secondary fascial closure have been reported, but no randomized, comparative data support one method of temporary closure over another.
Tumor Resection: Primary tumors of the abdominal wall include desmoid tumors, sarcomas, and their malignant variants. There also may be primary skin malignancies, malignant degeneration of chronic scars, fistulas, and radiation injury. Secondary tumors result from extensions of carcinomas of the colon, bladder, gallbladder, and other visceral malignancies. The primary goal of treatment is definitive resection. Once the wound margins are free of tumor, definitive reconstruction can be performed.
Radiation Wounds: These wounds involve an area of skin prone to ulceration or infection that does not heal. Treatment is wide resection and examination of the specimen for recurrence. Once the wound margins are tumor free, definitive reconstruction can be performed while the wound is temporarily covered with dressings or mesh.
Postoperative Defects: Abdominal wall defects after surgery include incisional hernias, parastomal hernias, planned ventral hernias after trauma, and those resulting from mesh-related complications. Definitive reconstruction is performed when the initial problem and associated complications are resolved.
15 What are the reconstructive options?
16 What is the “components separation” technique? What size defect can be closed using this technique?
A significant contribution to the repair of incisional hernias was the description by Ramirez et al. of the components separation technique. The evolution of the components separation technique is based on early descriptions by Vasconez et al. of transverse rectus abdominis myocutaneous (TRAM) closure that involves separation of external and internal oblique musculature and release of the posterior rectus sheath. Ramirez et al. noted that the abdominal wall is formed by overlapping muscle layers that may be separated while preserving their innervation and blood supply, specifically, elevation of the external oblique off of the internal oblique while maintaining the neurovascular supply to the rectus, which travels in segmental fashion between the internal oblique and transversus abdominis. The rectus can then be released from the posterior rectus sheath. Once this is accomplished, medial advancement of a compound flap of rectus muscle and attached internal oblique–transversus abdominis complex. Unilateral advancement of 5 cm in the epigastric region, 10 cm at the umbilicus, and 3 cm in the suprapubic region were described.
The efficacy of this particular technique and modifications of the anatomic principles described by it have been substantiated in multiple series. Fabian et al. described a modification involving division of the internal oblique component of the anterior rectus sheath, which allowed for unilateral advancement of 8 to 10 cm in the epigastric area, 10 to 15 cm in the midabdomen, and 6 to 8 cm in the suprapubic region.
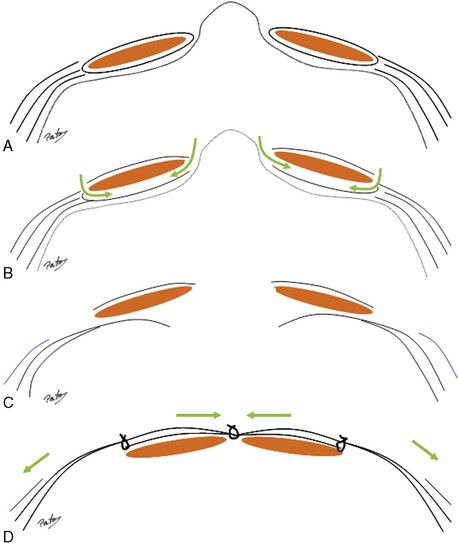
A lower hernia recurrence rate, avoidance of prosthetic material, restoration of dynamic abdominal wall function, and improvement in back pain and postural abnormalities have been cited in the literature. Wound-related complications have been problematic with this technique and are related to the wide undermining required. Studies have demonstrated a reduction in wound-related complications with the preservation of periumbilical perforators (Figs. 91-2 and 91-3).
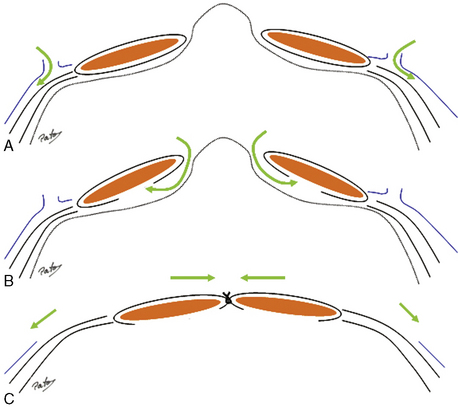
Figure 91-2 Component separation technique. A, External oblique release with separation of external oblique and internal oblique in an avascular plane. B, Incision and release of the posterior rectus sheath. C, Midline myofascial approximation of compound flaps composed of rectus abdominis with attached internal oblique/transverses abdominis.
(Courtesy Patricio Andrades, MD, Clinical and Research Fellow, Division of Plastic Surgery and Transplant Immunology, Division of Plastic Surgery, University of Alabama at Birmingham, Birmingham, Alabama.)
17 Describe the concept of staged abdominal reconstruction
When an abdominal wound is unstable as a result of contamination or if primary fascial approximation is not possible due to visceral edema, then temporary abdominal closure with a wound VAC, vacuum pack, or absorbable Vicryl mesh is indicated. Failure to perform secondary fascial approximation in a timely fashion is an indication for staged abdominal reconstruction. Fabian et al. described a technique that is divided into three stages. In stage I, Vicryl mesh is applied for visceral coverage. If fascial approximation is not able to be obtained by 2 weeks, the mesh is removed and a split-thickness skin graft (STSG) is placed over the viscera (stage II). Six to twelve months later the skin graft is removed, and definitive reconstruction is performed using a modification of the component separation technique (stage III). They found the risk of fistula formation correlated with the duration of mesh, with a statistically significant increase in risk after 18 days. They also found that delay in definitive reconstruction beyond 1 year leads to loss of abdominal domain and difficulty obtaining a tension-free repair.
18 What is the incidence of incisional hernia formation after laparotomy? What are commonly associated risk factors?
More than two million laparotomies are performed annually in the United States, with a reported 2% to 11% incidence of incisional hernia formation. It is the most common complication after laparotomy by 2:1 over bowel obstruction and is the most common indication for reoperation by 3:1 over adhesive small bowel obstruction. In a review of 1000 midline laparotomies by Condon et al., no single factor was associated with the development of incisional hernia on univariate analysis. On multivariate analysis, the combination of reopening and reclosure of previous incisions combined with wound infection influenced the development of incisional hernia.
Postoperative wound infection has been found in other studies to be associated with the development of incisional hernias. Obesity, aneurysmal disease, smoking, male gender, chronic obstructive pulmonary disease, malnourishment, malignancy, corticosteroid dependency, and prostatism are other risk factors reported in the literature.
19 What suture material and technique are associated with the lowest rate of incisional hernia formation?
A meta-analysis of randomized trials comparing suture material and technique found that abdominal fascial closure with nonabsorbable, monofilament suture in continuous fashion had a significantly lower incisional hernia rate. In work that has been reinforced by others, Jenkins et al. found that a suture length to wound length ratio of 4:1 was optimal for fascial closure. To use this length of suture, bites should encompass 1 cm of tissue at 1-cm intervals with attention to simply approximate the fascia. They also found nonabsorbable suture used in continuous fashion to be the material and technique of choice.
20 What is the natural history of incisional hernia formation?
The presence of an incisional hernia is an indication for repair. The linea alba serves as the midline anchor for the aponeurotic insertions of the rectus sheath and oblique musculature. Disruption results in gradual enlargement of the hernia defect due to the unopposed lateral contractions of the oblique musculature. As the defect widens, task-dependent functions of the abdominal wall musculature are interfered with and significant physiologic derangements occur.
21 What are the primary goals in abdominal hernia repair?
DiBello et al. defined several goals that the surgeon should accomplish when repairing abdominal wall hernias: Prevention of visceral eventration
The application of these principles with an emphasis on restoration of midline myofascial continuity has led to a reduction in hernia recurrence rates and improved functional and cosmetic outcomes in abdominal wall reconstruction.
22 What are the criteria for use of synthetic mesh?
Prosthetic material is used for structural support of the abdominal wall in a stable wound or as a temporizing measure in an open acute or infected wound. Mesh should meet certain criteria prior to its use. Mesh should be resistant to mechanical stress; it should be strong, durable, and of significant tensile strength so that it will not fragment with usage. It should be chemically inert; it should not be modified by tissue fluids or induce an inflammatory response. It should be capable of host tissue incorporation. Mesh should be tolerant to infection and capable of being reentered in the presence of infection or in the need for further exploratory surgery. Mesh should be easy to handle and capable of being fabricated into a desired shape.
23 How has the application of mesh affected the surgical approach and outcomes in abdominal hernia repair?
Use of synthetic mesh in the repair of incisional hernias increased from 34% in 1987 to 65% in 1999. The American Hernia Society has declared that the use of mesh now represents the standard of care in incisional hernia repair. A multicenter, prospective randomized trial by Luijendijk et al. comparing mesh and primary suture repair of incisional hernias 6 cm in greatest dimension found a 46% recurrence rate in the suture repair group compared with 23% in the mesh repair group at 3-year follow-up. A long-term 10-year follow-up of this study by Burger et al. revealed a cumulative recurrence rate of 63% for the primary suture repair group compared with 32% for the mesh repair group. An expert panel meeting on incisional herniorrhaphy concluded that primary suture repair should be used only for small hernias, less than 5 cm in greatest dimension, and if the repair is oriented horizontally with nonresorbable, monofilament suture with a suture to wound length ratio of 4:1.
24 Describe the experience with prosthetic materials
The two most commonly used prosthetic materials are polypropylene and expanded polytetrafluoroethylene (ePTFE). Polypropylene was first introduced in the 1950s by Usher. The large pore size of polypropylene mesh allows for macrophage and neutrophil infiltration providing for greater resistance to infection. Its porosity allows for better fibrovascular ingrowth and a reduced incidence of seroma formation.
Expanded polytetrafluoroethylene (Gore-Tex, W.L. Gore and Associates, Flagstaff, Arizona) has a microporous structure that minimizes cellular infiltration and tissue incorporation. Studies have shown ePTFE prosthesis to be equivalent to polypropylene in terms of suture retention strength. As a result of its flexibility, conforming nature, and minimal tissue ingrowth, ePTFE can be placed directly on bowel. The disadvantages are related to its microporous structure. The material is virtually impenetrable, preventing host tissue ingrowth and leading to seroma formation. Once infected, ePTFE requires explantation. The micropores range from 3 to 41 microns in size, which are large enough for bacteria (1micron) but too small for macrophages (>50 microns).
In an effort to reduce mesh-related complications and more closely duplicate abdominal wall physiology, research has focused on the development of composite materials that combine absorbable and nonabsorbable or barrier materials. Well-designed comparative studies with long-term follow-up are needed.
25 What is the clinical course of prosthetic materials capable of incorporation?
Within 18 to 24 hours, a fibrous exudate seals the viscera from the mesh. At 5 to 10 days, there is ingrowth of granulation tissue into the interstices of the mesh. At 14 to 21 days, the granulation tissue is ready for skin grafting or flap coverage. Fabian et al. demonstrated a statistically significant reduction in enteroatmospheric fistula formation with skin grafting of open abdominal wounds prior to 18 days after mesh placement.
26 Describe the technique for prosthetic material placement during abdominal wall reconstruction
Several methods of securing the mesh to the fascia have been described; the most common are mesh onlay, mesh inlay, retrorectus placement, and intraperitoneal underlay. The retrorectus technique popularized by Rives and Stoppa and the intraperitoneal underlay technique have become popular and are associated with the lowest recurrence rates. Recurrence after mesh repair is rarely due to an intrinsic failure in the prosthetic material. Failure to identify healthy fascia and technical error in securing the mesh to the fascia commonly lead to recurrence at the mesh–fascia interface.
Retrorectus and intraperitoneal underlay techniques involve placement of the mesh beneath the abdominal wall. When possible, omentum should be interposed between the mesh and the viscera. It is generally recommended to place the mesh with at least 4 cm of contact between the mesh and the fascia. This allows for a distribution of pressure over a wider area (Pascal’s principle), and the pressure-induced apposition promotes fibrous ingrowth at the mesh–fascial interface. It has also been experimentally demonstrated that polypropylene (Prolene) may shrink up to 30% after implantation. By placing the mesh beneath the abdominal wall, the repair is bolstered by the anterior abdominal wall, providing for a more secure and physiologic repair. Recurrence rates of less than 5% have been reported with these techniques (Fig. 91-4).
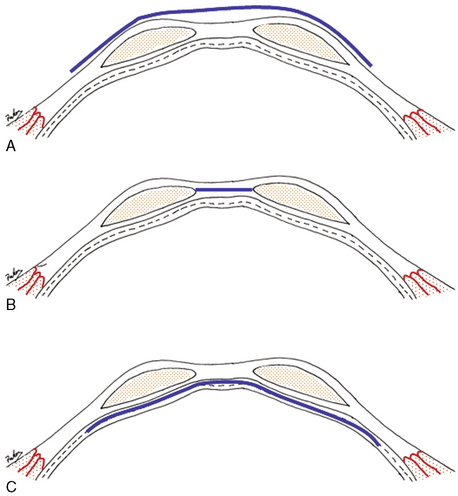
Figure 91-4 Mesh positions. A, Onlay technique. B, Inlay technique. C, Retrorectus underlay technique.
(Courtesy Patricio Andrades, MD, Clinical and Research Fellow, Division of Plastic Surgery and Transplant Immunology, Division of Plastic Surgery, University of Alabama at Birmingham, Birmingham, Alabama.)
27 What are the advantages and disadvantages of using bioprosthetics in abdominal wall reconstruction?
Concern regarding mesh-related complications, such as infection, extrusion, abdominal wall stiffness, pain, and fistula formation, has led to the search for more biocompatible prosthetic materials. Advances in tissue engineering technology have led to the development of biomaterials derived from human and animal tissues. Materials such as human acellular dermis (AlloDerm, LifeCell, Branchburg, New Jersey), porcine acellular dermis (Permacol Tissue Science Laboratories, Covington, Georgia), and porcine small intestinal submucosa (Surgisis, Cook Surgical Incorporated, Bloomington, Indiana) are the most commonly used biomaterials. These materials consist of an acellular collagen matrix that promotes host tissue remodeling while maintaining mechanical integrity. They differ in that they heal by a regenerative process rather than by scar tissue formation. They have demonstrated resistance to infection, biocompatibility, tolerance to cutaneous exposure, and mechanical stability when used in incisional hernia repair. Disadvantages are their high cost and the lack of long-term follow-up studies validating their use.
28 What is gas gangrene of the abdominal wall? How do you differentiate it from anaerobic clostridial cellulitis?
Gas gangrene, or clostridial myonecrosis, is a rare but highly lethal postoperative complication that requires early recognition and prompt surgical débridement of all involved layers of the abdominal wall. Clinical signs include wound swelling, tenderness, drainage, discoloration that changes from pink to magenta within a few hours, and usually a small amount of crepitation. The patient is toxic out of proportion to the temperature elevation, with signs of tachycardia and hypotension. The wound culture is polymicrobial with at least one species of Clostridium, usually C. oedematiens or C. septicum. The most important exotoxin is lecithinase. The main difference between anaerobic clostridial cellulitis and clostridial myonecrosis is the relationship of gas to the signs of toxicity; a small amount of gas with severe toxicity usually represents clostridial myonecrosis.
30 What is an omphalocele? What causes it?
An omphalocele is a developmental anomaly of the abdominal wall that occurs in 1: 3200 to 1:10,000 live births, often in association with sternal or diaphragmatic abnormalities, heart defects, or extrophy of the bladder. Large defects, often associated with syndromes, have a high mortality rate. An omphalocele results from failure of the four folds of the abdominal wall (endoderm, ectoderm, inner splanchnic, outer somatic mesoderm) to fuse at the umbilical ring. The sac (yolk sac) of amnion and chorion that covers the eviscerated mass commonly contains the liver and midgut. The defect develops during the extracolemic phase, between the sixth and twelfth weeks of intrauterine life, when the entire midgut passes out of the abdomen and into the yolk sac. After a period of linear growth, the bowel rotates 270° counterclockwise around the superior mesenteric vascular axis before returning to the abdomen. Defects range from those limited to the umbilicus to those extending from the xiphoid to the pubis. The umbilical cord attachment is most often at the apex of the sac.
31 What is gastroschisis?
A gastroschisis is a full-thickness defect of the abdominal wall that occurs lateral to the umbilical ring (usually to the right) with the umbilical cord attached at the normal position. A variable amount of intestine and occasionally parts of other abdominal organs are herniated outside the abdominal wall with no covering membrane or sac. It likely is the result of an abdominal wall ischemic event. Most of the morbidity is the result of in utero bowel injury.
32 Besides the physical findings of the abdominal wall, what characteristics do patients with gastroschisis have in common?
Nonrotation of the bowel, abnormally short midgut, and small peritoneal cavity.
33 How does gastroschisis differ from omphalocele?
A gastroschisis differs from an omphalocele in that it lacks a covering sac, and it is rare to see liver or other organs in the defect. The intestines usually are thickened, matted, and shortened because of prolonged contact with the amniotic fluid. Umbilical cord insertion is normal. The abdominal wall defect is lateral to the umbilicus, usually on the right side where the umbilical vein has resorbed, leaving it structurally weaker. The long-term outcome in gastroschisis is mainly related to the degree of associated intestinal injury, whereas the long-term outcome in omphalocele is primarily related to the severity of associated anomalies.
34 What is the treatment of patients with gastroschisis or omphalocele?
Primary closure, if it does not produce dangerously high intraabdominal pressure. Otherwise, staged procedures are indicated. Silon (Silastic-coated Dacron), polyethylene, or Teflon sheets are sutured to the edges of the fascial defect, and the viscera are gradually returned into the abdomen as the abdominal wall becomes more compliant and the cavity enlarges. If necessary, local or regional flaps are used.
35 What is “prune belly” syndrome?
Prune belly syndrome, also known as triad syndrome or Eagle-Barrett syndrome, consists of a triad of anomalies found almost exclusively in newborn boys: (1) absent or hypoplastic abdominal wall musculature, (2) bilateral cryptorchidism, and (3) dilation of the urinary tract. On physical examination, the muscular deficiency may be limited to one area, ranging from complete absence of muscle to the presence of all muscles as thin but recognizable structures. Complete absence of lower rectus muscles is most common. The abdomen appears as wrinkled or flabby, much like a prune, because of the weakened abdominal wall. As the child grows, the body contour resembles a pear or pot belly more than a prune. Children are often subject to respiratory complications due to impaired diaphragmatic motion and scoliosis due to the absence of the abdominal support mechanism. Reports describe the use of tensor fascia lata and rectus femoris muscle flaps to strengthen the abdominal wall.
36 What are the options for lower abdominal wall reconstruction?
38 What is commonly described as the “flap of choice” for abdominal wall reconstruction?
The tensor fascia lata is an ideal reconstructive option for abdominal wall defects. A dense, strong sheet of vascularized fascia and overlying skin can be transferred as a single unit in a single stage with minimal donor deficit. It is useful in irradiated and contaminated fields. Protective sensation can be maintained by inclusion of the lateral femoral cutaneous nerve (T12), and voluntary control is provided by the descending branch of the superior gluteal nerve. Flaps wider than 8 cm usually require skin grafting of the donor site; narrower flaps can be closed primarily. There is a tremendous disparity between the small size of the tensor muscle, originating from the greater trochanter, and the surrounding tensor fascia lata flap. The cutaneous paddle is reliable to approximately 5 to 8 cm above the knee; the distal portion is essentially a random pattern flap supplied largely by cutaneous perforators from the vastus lateralis muscle. The dominant pedicle, the lateral femoral circumflex femoral vessels arising from the profunda femoris, pierces the medial aspect of the flap 8 to 10 cm below the anterosuperior iliac spine. The arc of rotation allows the tip of the flap to reach the ipsilateral lower chest wall and xiphoid, especially in the thin patient. The flap can be used to resurface the entire suprapubic region, lower abdominal quadrants, or ipsilateral abdomen.
39 What is the role of the rectus femoris in abdominal wall reconstruction?
The rectus femoris is an excellent flap for reconstruction of the ipsilateral or lower abdominal wall. For extensive defects, a larger cutaneous paddle can be incorporated with the adjacent fascia lata in the musculocutaneous flap. The tip of the flap reaches a point midway between the umbilicus and the xiphoid. The flap is supplied by the lateral femoral circumflex vessels. It also can cover the entire suprapubic region and extend to the contralateral anterosuperior iliac spine. After transposition, the vastus lateralis and vastus medialis are approximated to prevent a functional deficit resulting in loss of the terminal 15° of knee extension.
40 What is the “mutton chop” flap?
Described by Dibbell et al., the mutton chop flap or extended rectus femoris myocutaneous flap allows for reconstruction of large full-thickness abdominal wall defects, including the epigastrium, without prosthetic material (Fig. 91-5).
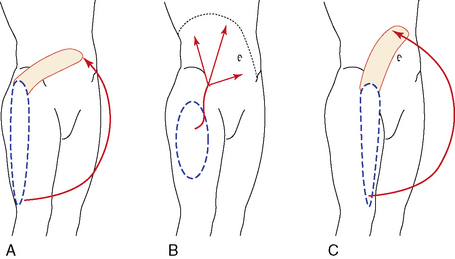
Figure 91-5 Flaps used in abdominal wall reconstruction. A, Tensor fascia lata. B, Anterior lateral thigh. C, Rectus femoris.
(Courtesy Patricio Andrades, MD, Clinical and Research Fellow, Division of Plastic Surgery and Transplant Immunology, Division of Plastic Surgery, University of Alabama at Birmingham, Birmingham, Alabama.)
41 What is the role of the omentum in abdominal wall reconstruction?
The omentum, a double layer of fused peritoneum arising from the greater curvature of the stomach, is supplied by the right and left gastroepiploic arteries. This flap can cover the entire abdominal wall and perineal areas. It can be used with mesh and provides a good bed for a skin graft.
42 What is the role of tissue expansion in abdominal wall reconstruction?
Tissue expansion is a reconstructive option that has been used in congenital abdominal wall defects for extensive soft tissue defects. Expanders can be placed between the external oblique and internal oblique muscles to create an enlarged external oblique musculocutaneous flap and to allow greater mobilization with rectus advancement techniques.
43 What is the incidence of herniation following TRAM flaps?
Kroll et al. reported using mesh in 21.4% of free TRAM flaps and in 45% of conventional TRAM flaps. The incidence of lower abdominal wall laxity following conventional TRAM flaps ranged from 0.2% to 16% and was lower in free TRAM flaps (1.0% to 5.0%). There was no difference in abdominal wall strength, based on ability to perform sit-ups, in patients who had a pedicled or free TRAM flap in age-matched controls.
Bleichrodt R.P., Simmermacher R.K.J., van der Lei B. Expanded polytetrafluoroethylene patch versus polypropylene mesh for the repair of contaminated defects of the abdominal wall. Surg Gynecol Obstet. 1993;176:18-23.
Bostwick J., Hill H.L., Nahai F. Repairs in the lower abdomen, groin, and perineum with myocutaneous flaps or omentum. Plast Reconstr Surg. 1978;63:186-194.
Boyd W.C. Use of Marlex mesh in acute loss of the abdominal wall due to infection. Surg Gynecol Obstet. 1977;144:251.
Brown G.L., Richardson J.D., Malangoni M.A. Comparison of prosthetic materials for abdominal wall reconstruction in the presence of contamination and infection. Ann Plast Surg. 1984;13:705-711.
Burger J.W., Luijendijk R.W., Hop W.C., Halm J.A., et al. Long term follow up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg. 2004;240:578-583.
Byrd H.S., Hobar P.C. Abdominal wall expansion in congenital defects. Plast Reconstr Surg. 1989;84:347-352.
Caix M., Outrequin G., Descottes B. Muscles of the abdominal wall: a new functional approach with anatoclinical deductions. Anat Clin. 1984;6:101-108.
Carlson M.A., Ludwig K.A., Condon R.E. Ventral hernia and other complications of 1,000 midline laparotomies. South Med J. 1995;88:450-453.
Caulfield W.H., Curtsinger L., Powell G., et al. Donor leg morbidity after pedicled rectus femoris muscle flap transfer for abdominal wall and pelvic reconstruction. Ann Plast Surg. 1994;32:377-382.
De Troyer A. Mechanical role of the abdominal wall muscles in relation to posture. Respir Physiol. 1983;53:341-353.
Dibbell D.G.Jr, Mixter R.C., Dibbell D.G.Sr. Abdominal wall reconstruction (the “mutton chop” flap). Plast Reconstr Surg. 1991;87:60-65.
DiBello J.N.Jr, Moore J.H.Jr. Sliding myofascial flap of rectus abdominis for the closure of recurrent ventral hernias. Plast Reconstr Surg. 1996;98:464-469.
Fabian T.C., Croce M.A., Pritchard F.E. Planned ventral hernia: Staged management for acute abdominal wall defects. Ann Surg. 1994;219:643-650.
Gracovetsky S., Farfan H.F., Helleur C. The abdominal mechanism. Spine. 1985;10:317.
Hodgson N.C., Malthaner R.A., Østbye T. The search for the ideal method of fascial closure: A meta-analysis. Ann Surg. 2000;231:436-442.
Hui K., Lineweaver W. Abdominal wall reconstruction. Adv Plast Reconstr Surg. 1997;14:213-244.
Jenkins T.P. The burst abdominal wound: A mechanical approach. Br J Surg. 1976;63:873-876.
Jernigan T.W., Fabian T.C., Croce M.A., et al. Staged management of giant abdominal wall defects: acute and long term results. Ann Surg. 2003;238:349-355.
Klein M.D., Hertzler J.H. Congenital defects of the abdominal wall. Surg Gynecol Obstet. 1981;152:805-808.
Kroll S.S., Marchi M. Comparison of strategies for preventing abdominal wall weakness after TRAM flap breast reconstruction. Plast Reconstr Surg. 1992;89:1045-1051.
Livingston D.H., Sharma P.K., Glantz A.I. Tissue expanders for abdominal wall reconstruction following severe trauma: Technical note and case reports. J Trauma. 1992;32:82-86.
Luijendijk R.W., Hop W.C., van den Tol M.P., et al. A comparison of suture and mesh repair for incisional hernia. N Engl J Med. 2000;343:392-398.
Parkas S., Ramakrishman K. A myocutaneous island flap in the treatment of a chronic radionecrotic ulcer of the abdominal wall. Br J Plast Surg. 1980;33:138-139.
Peled I.J., Kaplan H.Y., Herson M., et al. Tensor fascia lata musculocutaneous flap for abdominal wall reconstruction. Ann Plast Surg. 1983;11:141-143.
Ramirez O.M., Ruas E., Dellon A.L. Components separation” method for closure of abdominal wall defects: An anatomic and clinical study. Plast Reconstr Surg. 1990;86:519-526.
Shaw W.W., Aston S.J., Zide B.M. Reconstruction of the trunk. In: McCarthy J.G., editor. Plastic Surgery. Philadelphia: WB Saunders; 1990:3755-3796.
Stoppa R.E. Treatment of complicated groin and incisional hernias. World J Surg. 1989;13:545-554.
Suominen S., Asko-Seljavaara S., von Smitten K., et al. Sequelae of abdominal wall after pedicled or free TRAM flap surgery. Ann Plast Surg. 1996;36:629-636.
Taylor G.I., Watterson P.A., Zelt R.G. The vascular anatomy of the anterior abdominal wall: The basis for flap design. Perspect Plast Surg. 1991;5:1-30.
Toranto R.I. The relief of back pain with the WARP abdominoplasty: A preliminary report. Plast Reconstr Surg. 1990;85:545-555.
Voyles C.R., Richardson J.D., Bland K.I., et al. Emergency abdominal reconstruction with polypropylene mesh: Short term benefits versus long term complications. Ann Surg. 1981;194:219.