Chapter 143 Rehabilitation of the Injured Hand
1 What are the physiologic effects of early motion programs after tendon repair?
Experimental studies have demonstrated that early motion favors intrinsic versus extrinsic healing. Positive results of early motion after tendon repair include improved tendon excursion, increased tensile strength, and decreased edema and joint stiffness.
2 Describe early passive mobilization after flexor tendon repair in the hand
This technique mobilizes the repaired tendon using passive flexion and limited active or passive extension. The repair is immobilized using a forearm-based dorsal block splint, which limits extension of the wrist and metacarpophalangeal (MCP) joints. Current therapy protocols are based on one or both of the following approaches:
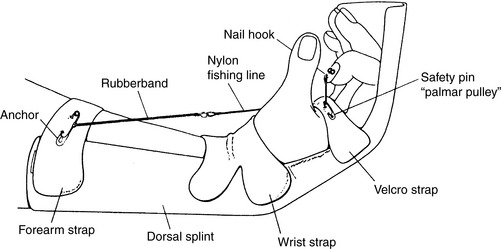
Figure 143-1 Modification of Kleinert dynamic traction splint using palmar pulley.
(From Chow JA, Thomes LJ, Dovelle S, et al: Controlled motion rehabilitation after flexor tendon repair and grafting. J Bone Joint Surg 70B:591–595, 1988, with permission.)
Active motion is generally started by 3 to 6 weeks. Progression of treatment for individual patients varies with the level of scar formation and demonstrated active motion.
3 When are early active mobilization protocols used after flexor tendon repair?
Early active mobilization may be used if the repair is sufficiently strong to withstand early motion, if the patient is reliable, and if the protocol is guided by an experienced therapist. The repaired tendon still is protected using splinting, and elements of passive mobilization are generally incorporated into the rehabilitation program. The active part of the program may involve gentle active muscle contraction in a limited range or use of a “place-and-hold” technique. A method popularized by Strickland and Cannon includes use of a tenodesis splint (hinged wrist splint limiting wrist extension and MP extension) combined with “place-and-hold” exercises.
4 Describe early passive mobilization protocols used for extensor tendons in zones V, VI, and VII
Early passive mobilization protocols use a reverse Kleinert approach. The splint maintains the wrist in approximately 45° of extension, with dynamic traction positioning the MCP (and interphalangeal [IP]) joints in 0° of extension. Active flexion in the splint is allowed to a predetermined level, depending on the protocol and the quality of the repair. Evans recommends splinting initially to provide MCP flexion equal to approximately 30° for the index and middle fingers and 40° for the ring and little fingers to achieve 5 mm of passive tendon glide for adhesion prevention.
5 What is the short arc motion protocol for zone III and IV extensor tendon repairs?
The short arc motion (SAM) protocol, developed by Evans, is an example of an early active motion protocol for zone III and IV extensor tendon repairs. Early active motion is initiated for the repaired tendon, using volar static splints as templates. The patient flexes and extends the joints, using minimal active muscle tendon tension (MAMTT). During exercise, the wrist is positioned in 30° of flexion and the MCP joint at neutral to slight flexion. The IP joints are maintained in an extension splint between exercises.
6 What are flexor tendon gliding exercises?
Tendon gliding exercises are used to obtain maximal total and differential flexor tendon glide: flexor digitorum superficialis (FDS), straight fist; flexor digitorum profundus (FDP), full fist; and hook (or claw) position, maximal differential glide.
7 Describe splinting after MCP implant arthroplasty
The patient is splinted with the MCP joints in the position of extension and neutral to slight radial deviation. Two splints are commonly used:
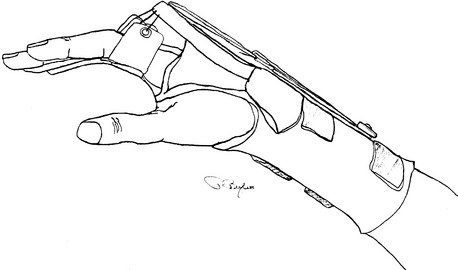
Figure 143-2 Dynamic thermoplastic splint used to position the metacarpophalangeal joints in extension and provide controlled active flexion after metacarpophalangeal implant arthroplasty.
Additional splinting for flexion may be required, including splints to block IP flexion during MCP flexion exercise and dynamic splinting, most commonly for the little finger.
8 Name three possible long-term postoperative complications of MCP implant arthroplasty
9 Describe examples of joint protection techniques for patients with arthritis
These techniques minimize stress to joints during daily activities and are appropriate for patients with arthritis in general as well as for patients who have undergone surgery such as implant arthroplasty. Examples include (1) use of larger, stronger joints; (2) three-point pinch (preferable to lateral pinch); (3) avoidance of deforming forces, such as twisting and ulnar deviation; and (4) balance of work and rest.
10 What factors must be evaluated to determine the cause of limited passive motion?
Restricted motion may be due to soft tissue and/or joint restrictions. In evaluating limited flexion at the PIP joint, for example, the following factors should be considered:
11 When is it appropriate to initiate active motion after an intraarticular fracture of the PIP joint?
The initiation of active motion depends on the stability of the fracture. Early active motion is possible if rigid fixation is achieved, with protective splinting between exercise sessions. If less rigid fixation is used, active motion generally can be started at 3 weeks and passive motion at 6 weeks.
12 What important principles must be followed in planning a treatment program after limited wrist arthrodesis to correct wrist instability?
Rehabilitation must be guided by the need for a stable, pain-free wrist with functional mobility. Keys to successful management after surgery include adequate immobilization, early active motion of uninvolved joints, a focus on regaining finger and thumb motion as soon as possible, and allowing the wrist to adapt gradually to its new kinematics through active exercise and use.
13 Why should a patient be referred for hand therapy after a nerve injury?
Before regeneration it is important to prevent deformity and improve function through the use of splinting and to educate the patient about methods of compensation for loss of sensibility and autonomic function.
During regeneration goals of therapy may include sensory desensitization and reeducation, muscle reeducation and strengthening, and restoration of functional patterns of use.
14 What are the potential deformities and splinting needs for radial nerve injuries?
The major problem is wrist drop from loss of wrist extensors (radial wrist extensors are spared with posterior interosseous nerve injury). Finger extension and thumb extension/radial abduction also are affected. Splinting options include wrist extension (dynamic or static), with or without finger and thumb outriggers to provide dynamic extension force, and the tenodesis splint, as described by Colditz (static outrigger from forearm-based splint to proximal phalanges reproduces tenodesis effect).
15 What are the potential deformities and splinting needs for ulnar nerve injuries?
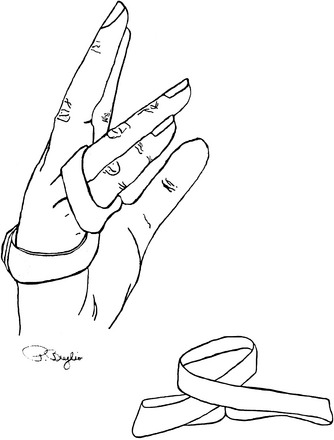
Ulnar nerve injuries may be high (affecting half of FDP, flexor carpi ulnaris [FCU], and ulnar intrinsics) or low (affecting adductor pollicis, half of flexor pollicis brevis [FPB], interossei, half of the lumbricals, abductor digiti minimi [ADM], flexor digiti minimi [FDM], and opponens digiti minimi [ODM]). The major deformity at both levels is claw deformity, caused by loss of all intrinsics to the ring and little fingers. The claw worsens as high ulnar palsy improves (increased flexion by FDP). A splint that prevents MCP hyperextension allows substitution by the long extensors to extend the IP joints. The simplest design is a figure-of-eight splint molded to the patient with thermoplastic material, which allows full flexion and permits functional use (Fig. 143-3).
16 What are the potential deformities and splinting needs for median nerve injuries?
Median nerve injuries may be high (affecting all forearm flexor/pronator muscles except half of FDP and FCU) or low (affecting half of the lumbricals, opponens pollicis [OP], abductor pollicis brevis [APB], and half of FPB). The major deformity requiring splinting at both levels is “ape hand” or loss of opposition. An opposition splint places the thumb in the corrected position to prevent deformity and improve function.
17 What readily available tests are used for determining early changes in sensibility due to nerve compression?
Semmes-Weinstein monofilaments and vibrometry (threshold tests) have been shown to be more sensitive than innervation density tests such as two-point testing in identifying early changes due to nerve compression.
18 What are the most common postural faults noted in patients with thoracic outlet syndrome that can be improved with therapy?
Rounded shoulders with a forward head posture; tight pectoral muscles (major and minor), with weak middle and lower trapezius muscles secondary to the slumped position; and tight neck flexors and scalenes with overstretched levator scapulae and upper trapezius muscles, which cause the forward head position.
19 Describe the benefits of hand therapy for patients with carpal tunnel syndrome or other forms of cumulative trauma
Splinting is appropriate for relative rest. Splints should be used judiciously to avoid problems such as disuse or development of abnormal compensatory patterns. Night splinting is recommended for carpal tunnel syndrome to prevent wrist flexion during sleep and median nerve compression. Exercises include active nerve and tendon gliding, stretching of overused tight muscles, and strengthening of opposing weak muscles, as indicated from evaluation. Postural assessment and training focus on the areas of malalignment, muscle tightness, or weakness. Work-related evaluation and modification address factors related to repetition, force, and posture, including the work station, work style assessment, and work requirements (e.g., production incentives and breaks). Finally, biofeedback training and relaxation can be used to relax muscle groups typically used in a state of sustained contraction.
20 What are the key issues in conservative treatment of cubital tunnel syndrome?
Patients with cubital tunnel syndrome need to avoid compression or stretching of the ulnar nerve at the elbow. The two key elements are to avoid direct pressure (leaning on elbows) and flexion greater than 90°. “Relative rest” can be achieved through the use of cushioned elbow sleeves or splints that prevent flexion. Ulnar nerve gliding exercises should be done only in a symptom-free range. As with other forms of cumulative trauma, work/activity modification is critical to long-term success.
21 What are upper limb tension tests?
Upper limb tension tests assess neural tension in the upper extremity by bringing the patient through sequential motions designed to place the neural tissues on stretch. A positive test reproduces the patient’s symptoms and/or demonstrates resistance or limitations in movement. Test results are assessed in reference to expected normal responses. Butler describes four basic tests for the upper extremity, with different movement patterns for the median, radial, and ulnar nerves.
22 What general principle can be used to activate a muscle after tendon transfer?
The patient is instructed to perform the original function of the transferred muscle or to combine the original function with the new function. For example, after an opponensplasty using the ring FDS, the thumb is opposed to the tip of the ring finger.
23 What are some conservative interventions specific to treating musicians with cumulative trauma?
Conservative interventions for musicians may include postural retraining, minimalist splinting, manual techniques, and instrument modifications to avoid interference with instrument mechanics or fingering requirements. Air playing, visual review of musical scores, and a gradual increase in duration and intensity of practice/performing times may assist in reducing symptoms.
24 What are some common problems that require treatment after a crush injury?
Soft tissue injury, with associated edema and scarring, may result in restriction of the intrinsic muscles of the hand, leading to intrinsic tightness. Exercise and splinting focuses on stretching the intrinsics (IP flexion with MCP extension). Another common problem secondary to edema is decreased MCP flexion. Serial splinting (thermoplastic or plaster) is an effective way to correct this problem.
25 During the first 48 to 72 hours status post burn, what is the appropriate position for splinting the hand with dorsal thermal injuries?
The wrist should be positioned in 15° to 20° of extension, the MCP joints should be flexed to 60° to 70°, the IP joints should be fully extended, and the thumb should be positioned with slight IP flexion and palmar abduction. This position discourages edema-induced MCP hyperextension and IP flexion posturing.
26 Name three methods for preventing hypertrophic scarring after a burn to the hand
27 Describe examples of splints used after surgery for Dupuytren’s contracture
Splinting to maintain extension is critical after surgery. Depending on the extent of involvement, options include the following:
Serial casting can be used to increase extension at the PIP joint if it remains unresponsive to other forms of splinting.
28 What are tests of maximal voluntary effort?
As part of functional testing or formal functional capacities evaluation, a battery of tests is used to determine whether a patient is giving maximal effort. Such testing may be necessary to help validate findings in patients who have the potential for secondary gain from their disability. Static strength tests are performed using the Jamar dynamometer and Baltimore Therapeutic Equipment (BTE) work simulator (passing scores based on coefficients of variation of 10% to 15% or less as well as correlation of grip test results), position of dynamometer handle test (skewed bell-shaped curve is anticipated with maximal effort), and the rapid exchange test using the dynamometer (increased speed of performance results in decreased ability to control force at submaximal level). No single individual test has been conclusively shown to be an adequate measure of maximum voluntary effort. Professional judgment must be used in interpreting the results of multiple tests and observations.
29 What are some of the advantages and disadvantages of whirlpool treatment versus direct application of heat, such as a hot pack or paraffin bath?
The whirlpool can be a modality of heat or neutrality because of the adjustability of temperature, thus not compromising vascularity or damaging insensitive parts. In addition, it can be used with chemical additives to decrease bacterial count in a small open wound, and the turbulence may assist in tissue débridement. The buoyancy of the water allows the patient to exercise during treatment. The primary disadvantage of whirlpool treatments is that the extremity is placed in a position of dependency, potentially increasing edema. Paraffin and hot packs have the advantage of being able to position the hand in elevation and place the hand in a position of stretch. In addition, the oil in the paraffin provides lubrication to dry tissues. When used for treatment of the hand, paraffin and hot packs can provide vigorous heating, which increases tissue extensibility, and are useful adjuncts before exercise or splinting of the stiff hand. Ultasound can be an effective and more direct heating agent for tissues with high protein and collagen content, requiring less heating time than more superficial applications of heat.
30 How can edema in the hand be measured?
Edema can be evaluated using circumferential measurements and/or a volumeter (measures total volume of the hand using water displacement). Values are compared with the values from the unaffected side as well as sequentially over time for the involved hand.
31 How should the edematous hand be treated?
The answer depends on the stage of wound healing. If seen acutely, the standard treatment is rest, ice, compression, and elevation. However, approximately 48 hours after injury or surgery, the best way to control edema is through active exercise and functional activity. Manual techniques to reduce edema can be used in preparation for exercise.
32 Define categories of splints used to gain joint motion
33 Why is it important to start therapy early, even while still casted, for example?
Patients benefit from early exercise of uninvolved joints to prevent stiffness and decrease edema and pain. The therapist can assist the patient in the use of adaptive devices or with modifications of the environment or of a task to increase functional independence. Examples of adaptive principles include increasing the diameter and/or friction of the item to be grasped to decrease the required force.
CONTROVERSY
34 Describe a course of treatment of reflex sympathetic dystrophy (complex regional pain syndrome type I)
There is lack of consensus about almost everything related to reflex sympathetic dystrophy (RSD; also known as complex regional pain syndrome type I [CRPS I]), including its definition, etiology, and most effective treatment approach. Our approach focuses on use of specific active loading exercises. Other approaches use gentle exercise as well as a wide array of other modalities, with or without sympathetic blocks.
Stress loading is defined as active, sustained exercise requiring forceful use of the entire extremity with minimal motion of painful joints. Clinically, two simple exercises actively load the affected arm—scrubbing and carrying. The stress-loading program follows basic principles of exercise physiology. The body adapts in response to demand. Exercise places a demand on the neural, vascular, and sensorimotor systems, all of which may play a role in initiating and/or perpetuating RSD. An overload is needed to achieve a training effect. Exercise must be of sufficient intensity, duration, and frequency to achieve this training effect. Theoretically, training may be due to the effect of stress-loading exercise on central processing abnormalities and neurovascular control mechanisms.
Keys to the success of the program include maximal load, compliance, structure, and emotional support, and separation of treatment of RSD from that of fibrosis. Passive exercise, splinting, and other forms of therapy are used only after RSD is under control. During the acute stage, symptoms generally resolve within days or weeks. If the patient is first seen during the dystrophic stage, the time required for resolution of RSD is generally longer, and treatment of fibrosis inevitably will be required through conservative measures. If treatment begins in the atrophic stage, motion gains with stress loading may be minimal, although improvement in function and a decrease in pain still can be achieved. Surgical intervention may include capsuloplasty of the MCP joints, check rein release (PIP joints), and intrinsic release.
Bell-Krotoski J.A., Figarola J.H. Biomechanics of soft-tissue growth and remodeling with plaster casting. J Hand Ther. 1995;8:131-137.
Butler D.S. Mobilisation of the Nervous System. New York: Churchill Livingstone, 1991.
Carlson L., Stannard J. Therapeutic management of the wrist. In: Watson H.K., Weinzweig J., editors. The Wrist. Philadelphia: Lippincott Williams & Wilkins, 2000.
Carlson L.K., Watson H.K. Treatment of reflex sympathetic dystrophy using the stress loading program. J Hand Ther. 1988;1:l49-l54.
Chow J.A., Thomes L.J., Dovelle S., et al. Controlled motion rehabilitation after flexor tendon repair and grafting. J Bone Joint Surg. 1988;70B:591-595.
Colditz J.C. Splinting for radial nerve palsy. J Hand Ther. 1987;1:18-23.
Evans R.B. Immediate active short arc motion following extensor tendon repair. Hand Clin. 1995;11:483-512.
Hunter J.M., Mackin E.J., Callahan A.D., editors. Rehabilitation of the Hand: Surgery and Therapy. St. Louis: Mosby, 1995.
King J.W., Berryhill B.H. Assessing maximum effort in upper-extremity functional testing. Work. 1991;1:65-76.
Mackin E.J., Callahan A.D., Skirven T.M., Schneider L.H., Osterman A.L. Rehabilitation of the Hand and Upper Extremity. St. Louis: Mosby, 2002.
Michlovitz S.L., editor. Thermal Agents in Rehabilitation. Philadelphia: FA Davis, 1996.
Pettengill K.M. The evolution of early mobilization of the repaired flexor tendon. J Hand Ther. 2005;18:157-168.
Sanders M.J. Management of Cumulative Trauma Disorders. Butterworth-Heinemann: Boston, 1997.
Wehbe M.A., editor, Early motion in hand and wrist surgery, 12, 1996, Hand Clin, 1-184.