Chapter 3 Clinical reasoning and models of practice
INTRODUCTION
Clinical reasoning occurs within models of practice. These models can be tacit (understood and largely unquestioned), controversial (known and debated), hegemonic (dominant and widely supported) and chosen (knowingly adopted). Practice models occur at different levels: they identify the broad strategy (such as the biomedical model) which operates at the level of a system, organization or workplace; they frame the interactions of team members (such as patient-centred care); and they give meaning and direction to the actions of individual practitioners (such as a humanistic or evidence-based orientation). In each case they reflect or challenge the interests (benefits and motivations) of the people working within the systems in which these models operate. In this chapter we report on doctoral research (Trede 2006) investigating interests underlying models of practice, and the impact of these interests on the model(s) that practitioners adopt, and the behaviours, particularly clinical reasoning, that are associated with these models.
The key issue addressed in this chapter is the impact of practitioners’ interests on the construction of their practice models and thus their clinical reasoning. Of particular interest is how these interests are shaped and to what extent the practitioners are conscious of the interests that determine their decision making and behaviour. We discuss in this chapter a framework that illuminates current practice models from an interest-driven practiceperspective and present a critical practice model, considering how such a perspective could redefine clinical reasoning.
Clinical reasoning is a challenging undertaking. It is influenced by a complex interplay between different interests and priorities that can range from wanting to assert professional authority and control over healthcare situations, to wanting to negotiate common ground with patients and create meaning, to striving to learn, transform and change oneself and patients. This discussion is framed by Habermas’s (1972) theory of cognitive interests, in which he argued that ideas shape our interests and actions. In this chapter we explore the link between interests and the actions of clinical reasoning and clinical practice. Interests can be thought of as the motivation for wanting to think and act in certain ways. Such motivation can be internally driven by values, attitudes and desires, such as a humanistic perspective, valuing rationality, or the desire to be patient-centred. It can also be shaped by external interests such as pressures to adhere to the dominant healthcare practice model, system imperatives such as economic rationalism, society and peer expectations of professional behaviour, and trends or discourse in health care.
Health professionals are accountable and accept responsibility for their decisions and actions. What values, assumptions and reasons underpin and guide their thinking and decisions? Often such interests are subconscious and have been acquired through the pervasive and often osmotic process of professional socialization (Eraut 1994) rather than being consciously learned and adopted through critical self-appraisal and informed choice of a desired model of practice. Once practitioners are aware of their interests and understand what motivates these interests they are in a better position to make critically conscious choices as to how they seek to frame their clinical reasoning and consequent actions.
OVERVIEW OF THE RESEARCH
The doctoral research (Trede 2006) that informs this chapter was conducted with physiotherapy practitioners using an integrated research approach involving descriptive, critical and action-learning oriented strategies. The research methodology was guided by hermeneutic traditions including principles of question-and-answer dialogue. These dialogues were critically analysed to illuminate unreflected assumptions, professional ideology and any hidden professional authority adopted by the participants or their workplaces.
MODELS OF PRACTICE
The first phase of the research involved examination of the literature and different practice models and their underlying interests. Models of practice are abstract ideas of what practice should look like if it followed a given framework. These frameworks comprise a variety of interests, criteria, norms, practice principles and strategies and behavioural expectations that inform clinical reasoning and practice. Models can be thought of as mental maps that assist practitioners to understand their practice. They serve to structure and to fine-tune practitioners’ clinical reasoning. Whether they are learned, chosen or unconsciously acquired through professional socialization, practice models generate the principles that guide practice, create the standards practitioners strive towards and the behavioural expectations that determine performance. Participants in this research had commonly acquired a biomedical science or medical practice model, the dominant physiotherapy practice model, through their educational and practice acculturation, with limited critique or questioning of this model. In such cases practitioners are commonly unaware of their practice model since it represents the unquestioned norm, and they are consequently unaware of how this model influences the way they reason. They reason within their adopted practice model without challenging the values and interests their practice model may entail.
THE SHAPING OF PRACTICE MODELS: THE PLACE OF IDEOLOGY
Professional ideology and interests, whether consciously or unconsciously enacted, inform practicemodels and professional practice (Newman 1994). Professional ideology is made up of the values, assumptions and prejudgements that guide our thinking (Therborn 1999). The type of practice we aspire to enact, the type of knowledge and evidence we value and utilize in practice, the way we justify our way of practising, and our clinical reasoning are all informed by interests that guide our curiosity in the first place.
We tend to interpret and justify our clinical reasoning processes with theoretical knowledge and research findings without acknowledging the interests and assumptions that inform our practice. Practice is justified with theories, guidelines and professional training. The ideology behind these theories and training remains hidden. To bring the assumptions out of hiding and question our way of reasoning enhances our practice awareness and provides us with real choices to practise optimally in each given clinical context.
It would be simplistic and limiting for a profession to define its practice purely on the basis of technical knowledge and skills (Schön 1987). This would reduce practice to the aspects that can be measured with empirico-analytical evidence only. What we observe, what we do, needs to be interpreted to make sense for us and to be communicated to others. Measurements and numbers on their own are meaningless. As professions develop and mature they become more involved with questions of expertise development and knowledge growth. Higgs et al (1999) claimed that a mature profession is one that enters into dialogue about its practices, is self-reflective, and pro-actively transforms with global changes.
CATEGORIZING PRACTICE MODELS
Professional practice models can be categorized in a number of ways. One such categorization is based on the theory of knowledge and human interest (Habermas 1972). According to this theory there are three types of interest, technical, practical and critical, each of which generates a certain type of knowledge. Each interest directs the types of question that can be asked, in turn dictating the type of knowledge that is generated and the way we practise. These interests not only shape the professional practice we adopt and determine which modes of practice we see as valuable, they also influence the identity we adopt as professionals, how we see the role of patients, how we believe clinical decisions should be made, and how we justify and argue our professional roles and actions. Table 3.1 presents the illness, wellness and capacity practice models and their inherent interests, based on the three Habermasian interests.
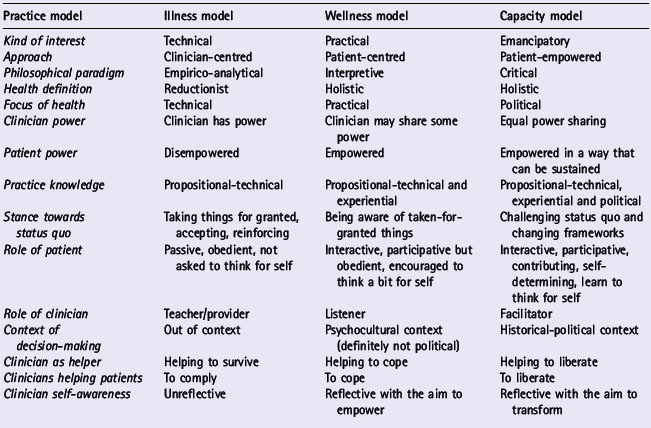
Table 3.1 illustrates how interests shape practice models, knowledge and clinical reasoning in practice. Some aspects are of particular relevance in this discussion of clinical reasoning:
CRITIQUING CURRENT PRACTICE MODELS
In the second phase of the research, the participants (physiotherapists) were asked to reflect on their way of practising, how they thought about their practice, and how they communicated with patients. The interview and discussion questions were categorized into issue questions and topical questions.
The aim was to critically understand how practitioners made sense of their practice and how they interpreted what happened in practice. There was a wide range of practice models that this participant group adopted. Participants were commonly unclear about their practice model and the values that underpinned it, and had difficulty articulatingthose factors. Most said at one stage in the interview that they found these questions difficult to answer, they had not thought about these questions, and they had to think more about them.
The interviewees’ responses revealed that practice is complex and that the practitioners in this study unknowingly adopted practice models. Much of their practice was unreflected and taken for granted. We concluded from the analysis that practice approaches are diverse and depend on context. Unsurprisingly, there was a preference for the biomedical practice model, as the hegemonic system and educational model of the participants’ workplaces and professional socialization.
All interviewees claimed that it was important to listen to patients and they stated that they were somewhat patient-centred. However, in practice, when experiencing interest clashes they reinforced their therapist-centred approach on the basis of technical interests. Felix (pseudonym), for instance, was convinced that his treatment plans were the right ones. Herein lies a fundamental contradiction: he described exercises as promoting independence but in reality his approach was actually prescriptive and fostered dependence on his power and control. Felix displayed purely instrumental, technical values that underpinned his understanding of his professional role and power. Felix critiqued his patients’ beliefs but he did not critique his own beliefs. He chose selective reasoning or professional power over negotiated clinical reasoning.
Another key finding of the research was the importance of external context factors on the preferred or existing practice model of the practitioners and the workplace. Where the environment was ‘hi-tech’ and healthcare delivery relied on advanced technology, and in acute care or emergency situations where patients were very ill or required critical care, the level of acceptability of the technical, biomedical model was high. There was an unchallenged focus on pathological diagnoses and biomedical intervention approaches, with the expectation of patient compliance. In less acute and less technology-dependent healthcare settings participants considered that there was greater opportunity for patient-centred care that involved patient participation in clinical decision making. The notion of emancipatory practice was foreign to most of the participants, and in early discussions they considered that in their workplace situations, with high workloads, time pressures, medical model frameworks, traditional approaches to professional hierarchies and an emphasis on evidence-based practice and cost efficiency, moves to treat patients on an equal footing in terms of clinical decision making were not particularly feasible, expected or needed.
DEVELOPING A CRITICAL SOCIAL SCIENCE MODEL FOR PRACTICE
The primary goal of the research (see Trede 2006, Trede & Higgs 2003) was to understand how a critical social science (CSS) perspective, with its inherent emancipatory interests, might influence and transform healthcare practice. The development of the CSS model for practice involved four cycles of critical transformative dialogues based on critique and reflexivity and the pursuit of change that led to liberation. The dialogues involved two-way conversations with self and others (including other participants, patients, colleagues) using critical reasoning. The first dialogue described the status quo of the CSS and health-related literature and developed a conceptual approximation of a CSS model for healthcare practice. The second dialogue involved critique and interpretation of the related physiotherapy literature followed by a critical dialogue with the first group of physiotherapist participants to critique the status quo of physiotherapy practice. In the third dialogue a group of practitioners trialled a CSS approach using action-learning strategies. The fourth dialogue, with another physiotherapy participant group, envisioned a CSS approach to practice.
In discussion of the status quo of practice a few participants, either through dissatisfaction with their model or prompted by further education, consciously chose to adopt an alternative model based in humanistic philosophy or, less frequently, a critical social science perspective. The more conscious the choice of practice model and the more this model differed from hegemonic practices, the more likely it was that the practitioners adopted a heightened level of awareness into their reasoning and behaviour. Instead of reasoningagainst scientific knowledge, evidence, established practice guidelines, or learned behaviour expectations set by their professions, workplaces or society at large, these practitioners sought to critically construct their own set of practice standards and ways of being in the world of practice, and they monitored their behaviour against these standards. These participants, without theoretical understanding of CSS theory, had created a critical practice model.
A critical practice model starts with the assumptions that practice is complex, outcomes are uncertain, and perceptions and interpretations of patient presentations are diverse. This means that a patient with an arthritic knee is not simply an arthritic knee – an object of treatment. Instead, practitioners need to consider patients holistically, thus including age, gender, attitude towards pain and physical activity, expectations of practitioners and themselves. Gaining a critical perspective means becoming aware of the interests that collide in practice, and questioning these interests.
A CRITICAL SOCIAL SCIENCE PERSPECTIVE
Critical social science is distinguished from the natural and social sciences in that it focuses on critique that leads to change and emancipation (Fay 1987). Critique is raising awareness about interests that have arisen in the sociocultural, historical worlds that influence clinical reasoning and practice approaches. From a CSS perspective, critical thinking means being able to take a sceptical stance towards self, culture, norms, practices, and institutions, as well as policy and regulations. CSS starts from the assumptions that all these dimensions are human-made and therefore can be changed. Before these dimensions are accepted and adopted they should be challenged and checked for their intentions and assumptions. CSS separates truth from ideology, reason from power and emancipation from oppression. The agenda of CSS is to critique, engage in dialogue and transform the status quo at an individual as well as a collective level, working towards transformation through professional development and maturity to become a self-aware and articulate professional who works with patients, policy and institutions that respect diversity and social justice. The focus is on transforming unnecessarily constraining policies and oppressive practices that restrict workforce development as well as patient empowerment.
TRIALLING A CRITICAL PRACTICE MODEL
We conducted action-learning research with a second participant group, trialling what it was like to transform their practice into (or towards) a critical practice model. This dialogue cycle included a pre-implementation workshop, an action-learning phase and a critical appraisal workshop. Participants were informed about the findings from the first phase of the research investigating the status quo of physiotherapy practice models. They were educated about the dimensions of critique, power and emancipation of CSS, and they were invited to critically discuss our critique of current practices. All participants designed an action plan that identified what aspects of their practice they were willing to change towards a more CSS-oriented approach. During the action-learning phase participants were interviewed on two or three occasions to discuss their progress and experiences of CSS practice.
The findings from this phase indicated that the practitioners had varied levels of readiness (cognitive, emotional and pragmatic) to engage in practice reflection and change, and different perceptions of the value of CSS as a basis for practice. Different levels of engagement with CSS were identified. These are discussed below, in conjunction with the findings of phase four of the research.
CRITIQUING AND VISIONING THE CRITICAL SOCIAL SCIENCE PRACTICE MODEL
In the final phase of the research we identified a group of participants who practised a patient-centred model closely related to our emerging model. The prime purpose of these discussions was to provide a ‘reality check’ of the emerging CSS model. These participants were explicitly requested as practising physiotherapists to provide critique of the draft model, as well as a self-critique of their own practice models, including their practice dilemmas.
A CRITICAL PRACTICE MODEL
This model for practice has two core dimensions:
(A) AN EMANCIPATORY DIMENSION
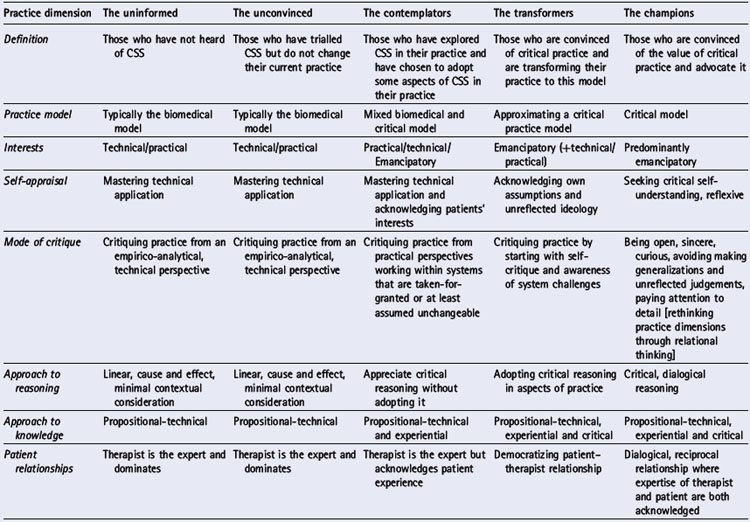
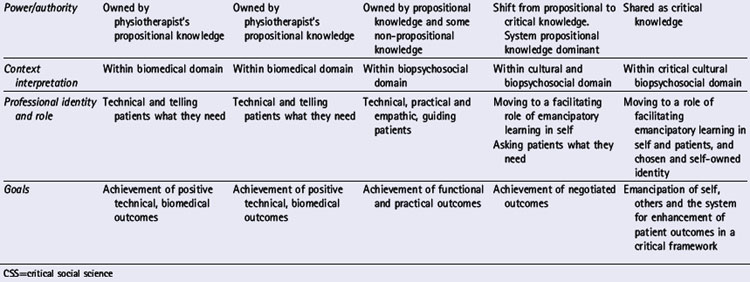
The emancipatory dimension entails recognition that to adopt a CSS or emancipatory model in a world of practice where such practice is a minority view requires a journey of emancipation for the practitioner. We have labelled this a journey of critical transformative dialogues. We recognize that to journey towards practice that is informed by CSS can start with a small degree of change. The research identified five modes of engagement with CSS as a practice model. These were labelled:
In this study the participants in this group were called impending champions, to recognise their adoption of CSS practices and their learning about CSS theory. They have come a long way from their traditional medical model backgrounds but have some way to go towards fully embodying CSS principles in their practice.
Table 3.2 details the interests, practices and characteristics of each of these modes. Of particular relevance here are the changing patterns of interaction, power use and reasoning approaches, ranging from therapist-centred and therapist-empowered decision making for patients to patient-centred and mutually empowered decision making dialogues with patients.
(B) A CRITICAL, LIVED DIMENSION
Practitioners bring their assumptions, values and prejudgements and professional experiences to the clinical situation. Practitioners with a critical perspective are aware of the interests that collide in practice, and they question these interests.
To practise within a CSS model rather than journeying towards CSS is to live or embody CSS in practice. Figure 3.1 illustrates Trede’s (2006) critical practice model. In the centre are critical transformative dialogues that enable practitioners to make practice model choices (on the lower left-hand side) and list all the requirements for critical practice (right-hand side).
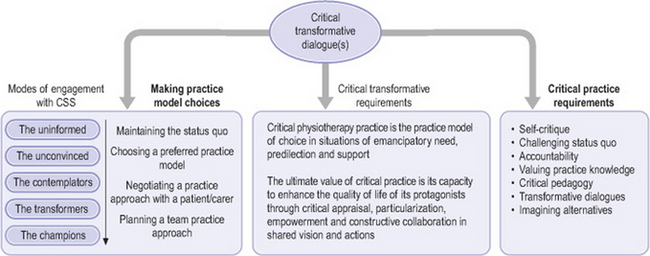
Practising within a CSS model requires practitioners to:
In advocating consideration and adoption of a CSS practice model we recognize that critical practice has variable relevance and potential across the range of practice contexts, and that other models (as discussed above) may be preferable or more feasible in certain contexts. We see critical practice as the practice model of choice in situations of emancipatory need, predilection and support. That is, critical practice is an accessible and acceptable choice when four situations coincide: (a) when there is a perceived need for patients and physiotherapists to collaborate in clinical decision making and to liberate practice; (b) when it is the preferred practice model of a practitioner (or group) who is a champion of critical practice; (c) when otherteam members are supportive of this approach and keen to embody authentic critical practice; and (d) where management and organizational systems support rather than restrict critical approaches. These four situations create a facilitative and supportive environment for embedding a critical practice perspective in the existing discourse. Critical practice would then be the practice model of choice because marginalized voices of patients and practitioners are heard and acted upon in a system-based environment that is sensitive, supportive and responsive to critique and emancipation.
The relevance of CSS for health professional practice is that such a practice model:
A critical practice model is challenging because practitioners must constantly question their clinical reasoning and maintain a critical stance to current practices. This critical stance to self and others can only be sustained within a supportive environment that facilitates such emancipatory learning. Adopting a CSS perspective requires advanced clinical reasoning skills that allow critical reflection about self, patients and the wider practice context and open yet sceptical professional relationships with patients.
CONCLUSION
Healthcare practice operates in increasingly more complex, diverse and uncertain environments. Patients are better informed, technology is advancing, and healthcare practice is constantly changing. It is important in this context to adopt an informed and critical stance to practice. Being aware of the interests that drive and frame practice and practice models, and understanding the way these models influence practice actions and clinical reasoning, are necessary aspects of being a responsible and critically competent practitioner in a demanding work environment. We have examined different practice models and have proposed advantages in relevant contexts of adopting a critical practice model. The relevance of critique in today’s challenging and dynamic healthcare environments is for practitioners to reclaim their human agency and critical self-reflective capacity. Critical thinking based on technical and practical interests is important but incomplete in meeting the challenging demands of current practice.
Eraut M. Developing professional knowledge and competence. London: Falmer Press, 1994.
Fay B. Critical social science. Ithaca: Cornell University Press, 1987.
Habermas J. (trans J J Shapiro). Knowledge and human interest. London: Heinemann. 1972.
Higgs J, Hunt A, Higgs C, et al. Physiotherapy education in the changing international healthcare and educational contexts. Advances in Physiotherapy. 1999;1:17-26.
Newman M. Defining the enemy: adult education in social action. Sydney: Stewart Victor Publishing, 1994.
Schön DA. Educating the reflective practitioner. San Francisco: Jossey-Bass, 1987.
Therborn G. The ideology of power and the power of ideology. London: Verso, 1999.
Trede FV. Unpublished PhD thesis. A critical practice for physiotherapy. Australia: University of Sydney. 2006.
Trede F, Higgs J. Re-framing the clinician’s role in collaborative clinical decision making: re-thinking practice knowledge and the notion of clinician–patient relationships. Learning in Health and Social Care. 2003;2(2):66-73.