Chapter 11 Expertise and clinical reasoning
In all professions, there are individuals who perform exceptionally well and who are held in high regard by their colleagues and their patients – in other words, experts. The simple definition of an expert is someone ‘capable of doing the right thing at the right time’ (Holyoak 1991). In research on expertise there are several variations on this definition. An expert can be defined as someone who performs at the level of an experienced professional such as a master or grandmaster in chess or a clinical specialist in medicine (Ericsson & Smith 1991, Rikers & Paas 2005). Experts can also be defined as top performers who excel in a particular field, for example elite athletes or musicians, or those clinicians who achieve the best clinical outcomes (Rothstein 1999). Experts can also be seen as those who achieve at least a moderate degree of success in their occupation (Boshuizen et al 2004).
Knowing more about the development of expertise, components of expertise and expert practice are all critical elements in expertise research. Ideally, an enhanced understanding of what distinguishes novices from experts should facilitate learning strategies for more effective education. Novice development in pursuit of expertise is an area of great interest in professional education as it lays the foundation for entry into practice (Boshuizen et al 2004). Expertise is much more of a process or continuum of development than a static state resulting from a cluster of attributes such as knowledge and problem-solving skills or high level performance (Bereiter & Scardamalia 1993). This does not mean that the process of moving toward expertise is based merely on the gathering of years of experience. Without learning mechanisms or reflection used to mediate improvement from experience there will be little acquisition of expertise (Tsui 2003).
One of the most critical and complex dimensions of expertise is clinical reasoning and decision making. A core assumption we make in this chapter is that we must not separate the critical analysis of clinical reasoning from the deliberate action that results as part of the reasoning and decision-making process. This is an interactive relationship where analysis and action each influence the other (Kennedy 1987). Clinical reasoning, then, is a process in which the healthcare professional, through interacting with the patient, family or care givers and other members of the healthcare team, structures meaning, goals and health management strategies based on clinical data, client preferences and values, knowledge and professional judgement (Higgs & Jones 2000). We begin this chapter with a ‘deconstruction of the concept of expertise’ achieved through a brief, analytical overview of key elements in traditional expertise theory and research. Next we explore the essential role of clinical reasoning and expertise in the context of everyday practice. Here we draw on predominantly qualitative research that has been carried out with practitioners in the context of practice. From this review, we generate a working list of attributes that we believe need to be considered when talking about clinical reasoning and decision making. In the final section of the chapter we engage in a discussion of strategies for facilitating learning and novice development in clinical reasoning. The goal of understanding expertise and clinical reasoning is the translation to more effective teaching and student learning and ultimately the delivery of the highest quality care.
DECONSTRUCTING THE CONCEPT OF EXPERTISE
EXPERTISE AS MENTAL PROCESSING AND PROBLEM SOLVING
Expertise is a complex multidimensional concept that has captured the interest of researchers over 50 years (Rikers & Paas 2005). Early work was in the field of cognitive psychology and accepted a tradition of basic information-processing capabilities of humans. Initial work in expertise concentrated on mental processing or, more simply, the conceptualization of problem solving. In deGroot’s well known work with chess players he began to look at differences between chess players with varying levels of expertise (deGroot 1966). He found that chess masters were able to recognize and reproduce chess patterns more quickly and accurately than novice players. Newell & Simon (1972) suggested that reasoning brought progressive expansion of knowledge of a problematic situation that continued until the problem was solved. They proposed that general methods or heuristics could be used for problem solving or information processing in all fields. An expert was someone who was particularly skilled at carrying out this heuristic search (Chase & Simon 1973, Ericsson & Smith 1991, Holyoak 1991). Investigative work required experts and novices to think aloud, or verbalize, as a way to explore thought processes and assess problem-solving skills. Subsequent studies in areas such as chess (Chase & Simon 1973) and physics (Chi et al 1981) revealed that expertise depended not only on the method of problem solving but also on the expert’s detailed knowledge in a specific area, ability to memorize, and ability to make inferences.
The well-known research by Elstein et al (1978, 1990) in medical problem solving was based on elements from early cognitive work in clinical reasoning and problem solving. They used various methods to analyse subjects’ reasoning processes, including the use of simulated patients, recall tasks and verbalization. Several major findings from this work have had a strong influence on education in medicine and other health professions (Elstein & Schwartz 2000; Elstein et al 1978, 1990; Rothstein & Echternach 1986). The hypothetico-deductive method that they identified continues to be incorporated into models that represent the clinical reasoning process in health professional education (Barrows & Pickell 1991, Elstein & Schwartz 2000, Elstein et al 1990, Jones 1992, Jones & Rivett 2004, Rothstein & Echternach 1986). In hypothetico-deductive reasoning the focus is on a process that includes cue acquisition, hypothesis generation, cue interpretation and hypothesis evaluation. The process of collecting data or cues from the patient and generating hypotheses is considered a technique for transforming an unstructured problem (e.g. a patient presenting with several complications) into a structured problem by generating a small possible set of solutions.
One of the most fundamental differences between experts and novices is that experts will bring more and better organized knowledge to bear on a problem. In medicine, the ability to determine the proper patient diagnosis was discovered to be highly dependent on the physician’s knowledge in a particular clinical specialty area, called case specificity (Elstein & Schwartz 2000, Rikers & Paas 2005). Case specificity implies that a successful reasoning strategy in one situation may not apply in a second case, because the practitioner may not know enough about the area of the patient’s problem. Identification of case specificity focused attention on the role of knowledge in expertise. Both clinician experience and the features of the case are factors that affect the problem-solving strategy that is used. Experts appear to have not only methods of problem solving but also the ability to combine these methods with knowledge and an understanding of how the knowledge necessary to solve the problem should be organized (Boshuizen et al 2004, Brandsford et al 2000, Chi et al 1988, Ericsson 1996). In a test of diagnostic reasoning, both successful and unsuccessful diagnosticians used a hypothesis-testing strategy (Rikers & Paas 2005). Research on the clinical reasoning of expert physicians demonstrated that in familiar situations experts did not display hypothesis testing but instead used rapid, automatic and often nonverbal strategies. This showed that expert reasoning in non-problematic situations is similar to pattern recognition or retrieval of a well-structured network of knowledge (Elstein & Schwartz 2000, Norman et al 1994). Experts can make connections or inferences from the data by recognizing the pattern and links between clinical findings and a highly structured knowledge base. This explains why experts tend to ask fewer, more relevant questions and perform examinations more quickly and accurately than novices. Novices and intermediate subjects tend to use hypothetico-deductive processes that involve setting up hypotheses and gathering clinical data to prove or disprove them (Elstein & Schwartz 2000). Thus, less experienced clinicians tend to ask patients more questions than do experts, and in the same order, regardless of their relevance to the case (Rivett & Higgs 1995).
EXPERTISE AS SKILL ACQUISITION
For health professions where diagnosis is not the predominant decision point, there has been perhaps no more influential work in expertise than that done by Benner (Benner 1984; Benner et al 1996, 1999). In her original work Benner applied a model of skill acquisition developed by Hubert Dreyfus, a philosopher, and Stuart Dreyfus, a mathematician and system analyst (Dreyfus & Dreyfus 1980). Their work came out of a reaction to the cognitive psychology tradition that intelligent practice is not just the application of knowledge and rules for instrumental decision making. A central premise in this work is that human understanding is a skill akin to knowing how to find one’s way about the world, rather than knowing a lot of facts and rules for relating them. ‘Our basic understanding was thus a knowing how rather than a knowing that’ (Dreyfus & Dreyfus 1980, 1996). From their research on chess players and airline pilots they put forward a five stage model for the acquisition and development of skill (novice, advanced beginner, competent, proficient and expert) (Table 11.1).
Table 11.1 The Dreyfus & Dreyfus (1980) model of skill acquisition (adapted from Benner 1984)
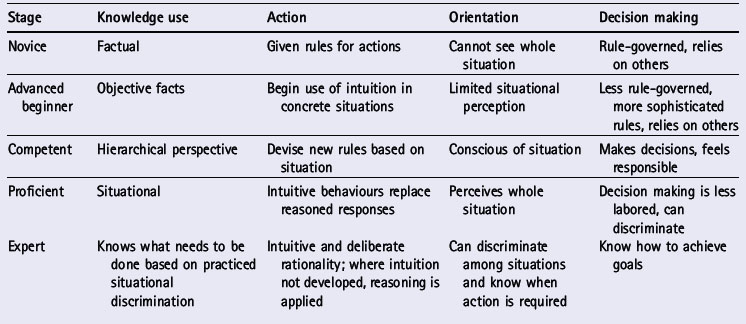
The Dreyfus & Dreyfus conception of expertise is much more focused on the context of actual practice. Several critical elements emerged from their model (Dreyfus & Dreyfus 1980, 1996): (1) expertise is more about ‘knowing how’ (procedural knowledge, knowing how to do things) rather than ‘knowing what’ (declarative knowledge, knowing information and facts); (2) expert knowledge is embedded in the action of the expert rather than from propositional knowledge; (3) experience is a critical factor in the development of expertise; (4) much of expert performance is automatic and non-reflective (but when a situation is novel, experts engage in deliberation before action); (5) intuition of experts or the knowing how to do things is both experiential and tacit.
In her analysis of nursing practice Benner found that much of expert performance in nursing emphasizes individual perceptions and decision-making abilities rather than just the performance of the skill. Skill is identified as an overall approach to professional action that includes both perception and decision making, not just what we would think of as technical skill or technique (Benner 1984; Benner et al 1996, 1999). The knowledge necessary to perform the skill is practical knowledge (i.e. knowing how to perform a skill in its real setting). Practical knowledge contrasts with knowing material in a textbook or theoretical knowledge that is learned in the classroom (Eraut 1994, Ryle 1949).
The Dreyfus model captured the complexity of nursing expertise that is acquired from deep, intuitive and holistic understanding of a situation. Benner argued that skilled know-how or practical knowledge is a form of knowledge, not just application of it. Furthermore, knowledge is not possessed by an individual in isolation, but rather is based upon the ‘shared life of a work group’, whereby clinicians learn from watching and interacting with others in collaborative and cooperative teamwork (Benner et al 1997).
Gruppen & Frohna (2002, p. 221), reviewing clinical reasoning research in medical education, wrote about the importance of context in research on clinical reasoning:
Too often studies of clinical reasoning take place in a vacuum. A case or scenario is presented to subjects … stripped of any ‘irrelevant’ noise that stems from the physician’s prior relationship with the patient …. The traditional methodology of providing clinical cases that are decontextualized and ‘clean’ may not be particularly valid means of assessing the full range of processes and behaviors present in clinical reasoning in natural settings.
KEY ELEMENTS IN EXPERTISE RESEARCH
Although there has been prolonged debate and controversy in expertise research on the acquisition of expert characteristics, there continues to be strong agreement on the characteristics of experts. In fact, that consistency is seen here in the characteristics of experts identified by Glaser & Chi (1988):
Another way to look at the key elements of expertise is to cluster them into categories. Sternberg & Horvath (1995) described three such clusters of categories for thinking about expertise in real-world settings:
In summary, experts are knowledgeable because they have extensive, accessible, well-organized knowledge. Experts continue to build their practical knowledge base through a repertoire of examples, images, illness scripts, and understanding learned through experience (Eraut 1994, Schön 1983). Experts learn from experience by using reflective inquiry or metacognitive strategies to think about what they are doing, what worked and what did not work. Although much of the expertise research has been done contrasting the performance of novices and experts, it is investigations of actual practice that provide an opportunity to explore more fully the knowledge, experience and complex human decision making embedded in expertise (Schön 1983, 1991).
EXPERTISE AND CLINICAL REASONING IN EVERYDAY PRACTICE
Qualitative research methods have been central tools in investigative work and theoretical writing done in several applied professions such as nursing (Benner 1984; Benner et al 1996, 1999), teaching (Berliner 1986, Sternberg 1998, Tsui 2003), occupational therapy (Fleming & Mattingly 2000, Mattingly & Fleming 1994), and physical therapy (Edwards et al 2004; Gwyer et al 2004; Jensen et al 1999, 2000, 2007; Resnik & Hart 2003; Shepard et al 1999). These are all professions where human interactions and care are central aspects of the work. In these studies we find that the clinical reasoning process is not as analytical, deductive or rational because the focus of care is a much larger process that extends beyond the identification of a diagnosis. The clinical reasoning process is iterative and ongoing. Knowing a patient, understanding his or her story, fitting the patient’s story with clinical knowledge and collaborating with the patient to problem-solve are the kinds of integral components of clinical reasoning that emerge from these studies. Here we discuss and compare in greater detail key findings from conceptual and theoretical work in clinical reasoning and expertise in occupational therapy, physical therapy and nursing. Each of these investigations represents important and provocative theory development for these professions, that led to sustained work exploring the context of everyday practice.
In their ethnographic study of clinical reasoning in occupational therapy, Mattingly & Fleming (1994) originally proposed three types of reasoning in their ‘theory of the three-track’ mind.
A fourth form of reasoning, narrative reasoning (Fleming & Mattingly 2000, Mattingly & Fleming 1994), is used to describe the story-telling aspect of patient cases. Often therapists use narrative thinking and telling of a kind of ‘short story’ in coming to understand or make sense of the human experience. This making sense of the illness experience is shifting the thinking and dialogue from a physiological event to a personally meaningful one for the patient. Reflecting on ethnographic research work done in occupational therapy since their original work, Mattingly & Fleming (1994) highlighted two key concepts in clinical reasoning: active judgement and narrative. Working together, these two streams of reasoning are core processes for occupational therapists.
In physical therapy, Jensen and colleagues developed a grounded theory of expert practice in physical therapy (Jensen et al 1999, 2000; Shepard et al 1999). It is proposed in this model that expertise in physical therapy is some combination of multidimensional knowledge, clinical reasoning skills, skilled movement and virtue (Figure 11.1). All four of these dimensions (knowledge, reasoning, movement and virtue) contribute to the therapist’s philosophy of practice. For novices, each of these core dimensions of expertise may exist but they do not appear to be as well integrated (Figure 11.2) (Jensen et al 2007). As novices continue to develop, each of the dimensions may become stronger, yet they may not be well integrated for proficient practice. When the expert therapist has fully integrated these dimensions of expertise, that in turn leads to an explicit philosophy of practice (Figure 11.2) (Jensen et al 2007). In this model of expertise it is difficult to highlight only one dimension such as clinical reasoning, as all dimensions could be seen as contributing to thinking and actions of expert practitioners. For example, experts’ knowledge is multidimensional and patient-centred. Therapists draw from several sources such as specialty knowledge, clinical knowledge gained through reflection on practice and listening carefully to their patients. Experts trust their tacit or craft knowledge and use it in making intuitive decisions about patient care.
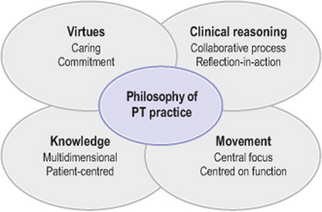
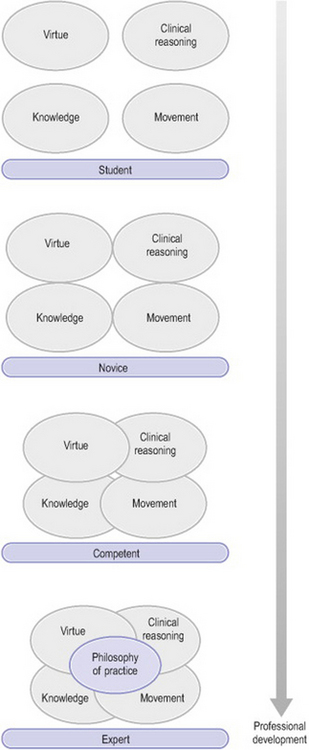
Figure 11.2 Professional development across the professional development continuum – student, novice, competent to expert (Jensen et al 2007, with permission)
The clinical reasoning dimension of the model has two core components: (1) it is a collaborative process between therapist and patient in which the patient is seen as an important source of knowledge; and (2) therapists demonstrate evidence of strong self-monitoring reflection skills in this collaborative process. Function, as defined by the patient, forms the core of a framework used in establishing patient care goals. Skilful facilitation of movement focused on function, done through data gathering, hands-on skills, assessment palpation and touch, is the central aim of therapists. One final element of the expert model is virtuous practice, seen in behaviours such as care and compassion for patients, non-judgemental approaches to patients, admitting mistakes and taking deliberate actions such as reporting unethical behaviour of colleagues or advocating for patients.
Subsequent work by Resnik & Jensen (2003) corroborated the presence of a patient-centred approach to care seen in collaborative clinical reasoning and promotion of patient empowerment. At the foundation of the patient-centred approach they identified an ethic of caring and a respect for individuality, a passion for clinical care and a desire to continually learn and improve. The primary goals of empowering patients, increasing self-efficacy beliefs and involving patients in the care process are facilitated by patient–therapist collaborative problem solving and enhanced through attentive listening, trust building and observation. The patient-centred approach is exemplified by the therapist’s emphasis on patient education and by strong beliefs about the power of education. This approach alters the therapeutic relationship and enhances patients’ abilities to make autonomous choices. Resnik & Jensen reported that these efforts not only promoted patient empowerment and self-efficacy, but also resulted in greater continuity of services, more skilful care, and more individualized plans of care and ultimately better outcomes.
Although experts in that study possessed a broad, multidimensional knowledge base, Resnik & Jensen (2003) discovered that years of clinical experience and specialty certification did not appear to be mandatory in achieving expertise. This seemed to challenge a basic assertion of the Dreyfus model, that experience is a critical factor in development of expertise. In Resnik & Jensen’s study this was not observed, and in fact, some therapists classified as experts were relatively new physical therapists. In these instances, they theorized, knowledge acquisition was facilitated by work and life experience prior to attending physical therapy school, by being in a work environment that offered access to pooled collegial knowledge, and by practitioners’ values and virtues of inquisitiveness and humility which drove their use of reflection. This combination of factors helped accelerate the acquisition and integration of knowledge. Furthermore, expert therapists used the rich knowledge base of colleagues and sought out knowledgeable mentors to assist them in challenging cases. Thus, in their theoretical model, expert therapists’ knowledge base comprised knowledge gained from personal experience and movement and rehabilitation, colleagues, patients, clinical experience, teaching experience, specialty work and entry-level education, as well as continuing education.
In-depth ethnographic work by Edwards and colleagues (2004) on expert physical therapists’ clinical reasoning strategies further revealed an interplay of different reasoning strategies in every task of clinical practice (for example interactive reasoning, diagnostic reasoning, narrative reasoning, ethical reasoning, reasoning about teaching). Rather than contrasting the cognitively-based rational models of reasoning and interactive models of reasoning, Edwards et al proposed a dialectic model of clinical reasoning that moves between the cognitive and decision-making processes required to diagnose and manage patients’ physical disabilities and the narrative or communicative reasoning and action required to understand and engage patients and caregivers. Critical reflection is required with either process.
The work of Benner and colleagues in Expertise in Nursing Practice: Caring, Clinical Judgment and Ethics (Benner et al 1996) and Clinical Wisdom and Interventions in Critical Care: A Thinking-in-action Approach (Benner et al 1999) represents the richness and the relevance of ‘learning from practice’ in order to improve understanding of expert practice. They used observations and narrative accounts of actual clinical examples as primary tools for understanding the everyday clinical and caring knowledge and practical reasoning that were used in nursing practice. Important findings from this work include these aspects of clinical judgement and skilful comportment of experienced nurses (Benner et al 1999):
What do these examples of investigative work centred on everyday practice tell us about clinical reasoning and expertise? As we look across the three health professions, we see striking similarities that emerge from understanding the context of practice (Table 11.2). It is the human or relationship side of practice that emerges as a central component of clinical reasoning and expertise. The critical analysis that is fundamental to clinical reasoning is not just a matter of matching the signs and symptoms to the practitioner’s existing knowledge base. It is a complex process where critical analysis must take place within the context of the action and interaction with the patient. That analysis and thinking must lead to wise judgement and action. It is these key attributes or habits of mind that are the focus of our discussion in the final section of this chapter.
Table 11.2 Learning from everyday practice: comparisons across professions
| Health profession theoretical elements | Key themes | Common themes shared by two or more professions |
|---|---|---|
| Occupational therapy | ||
| Procedural reasoning Interactive reasoning Conditional reasoning Narrative reasoning |
Use of hypothetico-deductive reasoning for identifying functional problems Collaboration with patient to understand patient’s perspective Integration of social and cultural processes for understanding Narrative as important tool for making sense of the illness experience |
Hypothetico-deductive reasoning used for specific procedural issues The patient is a respected and central aspect of the work Collaboration with the patient is a critical strategy in clinical reasoning and decision making Metacognitive skill (reflection) is an integral aspect of patient care Narrative is a critical tool for understanding the clinical situation including patient, caregivers as well as the clinical knowledge that is part of the story Moral agency and deliberate actions are essential elements of what it means to be ‘good’ at one’s work (it is difficult to separate clinical and ethical reasoning) |
| Physical therapy | ||
| Multidimensional knowledge base Clinical reasoning is collaborative and patient centred; reflection; self-monitoring Function central to movement Virtuous practice; deliberate action Dialectic reasoning Instrumental reasoning (hypothetico-deductive for diagnosis and management) Communicative/narrative for understanding |
Use of hypothetico-deductive reasoning for identifying diagnosis, patient management Collaboration with the patient is an important aspect of clinical reasoning Knowledge comes from many sources including the patient Reflection, self-monitoring is a critical skill Non-judgemental approach, deliberate actions Narrative/communicative reasoning and action for understanding patient or caregiver experience |
|
CLINICAL REASONING AND NOVICE DEVELOPMENT: DEVELOPING HABITS OF MIND ACROSS THE PROFESSIONAL DEVELOPMENT CONTINUUM
Understanding the context in which practice occurs is critical in the clinical reasoning and decision-making process of experts, yet challenging for novices who are often focused on technical skills. Experts do much more than ‘make a diagnosis’; they engage in a process of reasoning and decision making that includes patients as a partners in their care. Although we use patient-centred language in professional association documents and professional journals, we spend little time focusing on the development of patient-centred skills in our novices.
The university setting does well in training analytic ‘habits of mind’ but it does far less in developing practical skills and capacity for professional judgement. Sullivan (2005) argued that in professional education, the strong emphasis on formal analytic reasoning and knowledge creation leaves out perhaps one of the most important elements, the act of inquiry in the context of the relationship. ‘The clearest way to grasp the insufficiency of the positivist model of professional expertise is to notice what the positivist account of knowledge leaves out and must take for granted’ (Sullivan 2005, p. 242). While expert practitioners bring scientific evidence, analysis and problem-solving skills to the clinical situation, they also bring the skills of practical reasoning as they listen to patients, reflect on and make meaning of what they hear. It is this narrative understanding and practical reasoning that is informed by scientific knowledge but guided by concern for human well-being that is central to expertise. The challenge for professional education is how to teach this complex ensemble of analytic thinking, skilful practice and wise judgement that is required in the professions. How do we go about developing habits of mind in our students? We, along with many others (Benner et al 1996, 1999; Dewey 1910; Epstein 1999; Higgs & Tichen 2001; Kennedy 1987; Schön 1987), argue that the relationship between patient and practitioner is a critical element of skilful ethical comportment, and that it is foundational in expert work and therefore an essential foundation for novice development.
The choice of the metaphor of foundation is important in that it emphasizes the supportive nature of ethical comportment. A foundation allows something, in this case expert work, to stand on a solid base. If something is lacking in a foundation, or is shakily built, then it will not be strong enough to withstand the stresses encountered in clinical practice. Skilful ethical comportment draws on at least three basic approaches to ethics: principled reasoning, virtue and a care orientation. A solid moral foundation includes all these approaches because an expert needs to understand moral norms and theories and the use of such tools to examine moral problems and practices. However, ‘theories and principles are only starting points and general guides for the development of norms of appropriate conduct’ (Beauchamp & Childress 2001, p. 2). An expert must also possess the virtues or character to do the right thing. If a clinician knows the correct moral action but lacks the courage or compassion to act, then the knowledge is of little significance. Lastly, a solid foundation in ethics includes the ability to discern what is worth caring about in healthcare practice. A care orientation considers what values should be pursued, nurtured or sustained and, conversely, what should be disvalued. Approaches that include only abstract principles or duties often lead to conclusions that minimize the particulars of individual circumstances that are considered morally relevant to care orientation. An orientation to care allows health professionals and patients to interact on the basis of ‘receptivity, relatedness, and responsiveness’ (Noddings 1984, p. 35).
Ethical comportment requires balancing all of these approaches as well as translating a judgement into action. Moral judgements can be about abstract, distant issues or they can be about up-close and personal issues involving ‘identified lives’: ‘The more personally involved we feel, the more emotive and aesthetic elements play a role; the farther the situation is from us, the less the force of emotion or aesthetics will be’ (Loewy 2000, p. 222). Within the realm of expert practice, the emotions of compassion, sympathy and empathy have a central place in our understanding of humane and ethical treatment of patients. Beyond these basic expressions of care, patients expect a range of emotional responsiveness appropriate to context. For example, in an emergency situation most patients would prefer quick and competent action to save their lives rather than heartfelt empathy. However, it is clear that in certain cases the emotional tone matters deeply. It is the life work of health professionals to recognize those situations and adapt their emotional response to the particular needs of the patient at that time.
In addition to these central emotions that are a part of care, other emotions are evoked through interactions with patients that are not always positive. It is important that students develop emotional sensitivity and realize that emotions or felt affect are distinct from thought or action: ‘Thus, to grieve, pity, show empathy or love is to focus on an aspect of self or other and to grasp information to which purer cognition or thought may not have access’ (Sherman 1995, p. 664). One way to attend to emotions is to encourage novices to reflect on the emotional content of interactions with patients or peers as this is an often overlooked component of ethical decision making. Reflection on emotions emphasizes the relationship between behaviours or words that begin or trigger an emotional response. By openly acknowledging that different emotions are evoked in different circumstances, novices have an opportunity to reflect on their emotional repertoire in a way that is encouraging and safe.
The processes of self-reflection, reflecting together between novice and expert at the moment of a clinical encounter, or small group discussion on the identification and understanding of emotions are steps in strengthening novices’ capacity to hold on to and name their emotional experiences. Rather than novices being told what they should feel or should have felt (such as empathy and compassion) when interacting with patients or others, opportunities should be provided to let novices interact with simulated patients or real patients in clinically complex situations and then reflect on their experiences in their own words.
Although emotions are sometimes seen as a somewhat fragile platform upon which to build such heavy obligations as moral duty or care, by attending to emotions we can see that they highlight certain aspects of a situation, serve as a mode of communication, lead to deeper self-knowledge and provide insight into motivation. Grounding and naming emotions in specific examples from novices’ and experts’ experiences in clinical practice begins to create a framework that legitimizes this component of the self in one’s professional role. Novices can then examine, question and develop their skills in emotional sensitivity – an important part of ethical comportment and caring for others.
In health professional education we have certainly heard and embraced the concepts of reflection and helping students develop their skills of reflective inquiry (Harris 1993; Schön 1983, 1991). Our understanding of reflection as an important metacognitive skill is often just that, a skill to be taught and a process to be applied by the student. Yet we know from experts that there is much more to reflection than writing down or discussing insights from one’s experience. Expert clinicians have the capacity to engage in critical self-reflection. Expert clinicians are more sensitive to contextual cues, as they are aware of their own mental processes, listen more attentively, are flexible, recognise bias and judgements and therefore act with compassion based on insight (Benner et al 1999, Epstein 1999, Gwyer et al 2004, Jensen et al 1999, Shepard et al 1999).
It is essential that novices have multiple opportunities to act on ethical judgements in a safe environment and reflect not only on the reasons for a particular action or set of actions but also on the thinking and responses that led up to the action. Novices need to hear experts ‘think out loud’ after a particularly difficult exchange with a patient or colleague, so that the process of arriving at a sound decision becomes more transparent. The habit of reflecting on what is going on ethically in a situation, what should be done about it, and the meaning for the broader professional and public community can be fostered throughout professional education.
CONCLUSION
In this chapter we have argued that expertise is not a static state, congruent with a list of specific attributes or obtained through years of experience. It is much more a continuum of development and a dynamic process where critical reflection and deliberate action are central components. Experts continue to learn and build extensive, well organized practical knowledge through the use of reflective inquiry and metacognitive strategies. Clinical reasoning is a complex process where critical analysis and reflection take place in the context of the action and interaction with the patient. Experts demonstrate their patient-centred focus through a consistent commitment to knowing the patient, intense listening that leads to a rich understanding of the patient’s perspective, and character to do the right thing. It is the ability of experts to engage in reflective analysis in patient care that leads to deliberate action to do the right thing with their patients. The challenge in professional education is to teach the complex ensemble of analytic thinking, skilful practice and wise judgement that is required in the health professions. This skilful ethical comportment based on principled reasoning, virtue and a care orientation is the foundation of expertise.
Barrows HS, Pickell GC. Developing clinical problem-solving skills: a guide to more effective diagnosis and treatment. New York: Norton, 1991.
Beauchamp T, Childress J. Principles of biomedical ethics, 5th edn. Oxford: Oxford University Press, 2001.
Benner P. From novice to expert: excellence and power in clinical nursing practice. Menlo Park, CA: Addison-Wesley, 1984.
Benner P, Tanner CA, Chesla CA. Expertise in nursing practice. New York: Springer, 1996.
Benner P, Tanner CA, Chesla CA. The social fabric of nursing knowledge. American Journal of Nursing. 1997;97(6):16BBB. 16DDD
Benner P, Hooper-Kyriakidis P, Stannard D. Clinical wisdom and interventions in critical care. Philadelphia: W B Saunders, 1999.
Bereiter C, Scardamalia M. Surpassing ourselves: an inquiry into the nature and implications of expertise. Chicago: Open Court Press, 1993.
Berliner D. In pursuit of the expert pedagogue. Educational Researcher. 1986;15(7):5-13.
Boshuizen H, Bromme R, Gruber H. Professional learning: gaps and transitions on the way from novice to expert. Norwell, MA: Kluwer Academic, 2004.
Brandsford J, Brown A, Cocking R. How people learn: brain, mind, experience and school. Washington, DC: National Academy Press. 2000:31-50.
Chase WG, Simon HA. Perception in chess. Cognitive Psychology. 1973;4:55-81.
Chi MT, Feltovich PJ, Glaser R. Categorization and representation of physics problems by experts and novices. Cognitive Science. 1981;5:121-152.
Chi MT, Glaser R, Farr M. The nature of expertise. Hillsdale, NJ: Lawrence Erlbaum, 1988.
DeGroot AD. Perception and memory versus thought. In: Kleinmuntz B, editor. Problem solving research, methods, and theory. New York: Wiley; 1966:19-50.
Dewey J. How we think. Chicago: University of Chicago, 1910.
Dreyfus HL, Dreyfus SL. A five stage model of the mental activities involved in directed skill acquisition. Berkeley: University of California, 1980. Unpublished report supported by the Air Force of Scientific Research (AFSC), USAF (Contract F49620-79-C—63),
Dreyfus HL, Dreyfus SE. The relationship of theory and practice in the acquisition of skill. In: Benner P, Tanner CA, Chesla CA, editors. Expertise in nursing practice. New York: Springer; 1996:29-48.
Edwards I, Jones M, Carr J, et al. Clinical reasoning strategies in physical therapy. Physical Therapy. 2004;84(4):312-335.
Elstein AS, Schwartz A. Clinical reasoning in medicine. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:95-106.
Elstein AS, Shulman LS, Sprafka SA. Medical problem solving: an analysis of clinical reasoning. Cambridge, MA: Harvard University Press, 1978.
Elstein AS, Shulman LS, Sprafka SA. Medical problem solving: a ten year retrospective. Evaluation and the Health Professions. 1990;13:5-36.
Epstein RM. Mindful practice. Journal of the American Medical Association. 1999;282:833-839.
Eraut M. Developing professional knowledge and competence. London: Falmer Press, 1994.
Ericsson KA, editor. The road to excellence. Mahwah, NJ: Lawrence Erlbaum. 1996.
Ericsson KA, Smith J, editors. Toward a general theory of expertise. New York: Cambridge University Press. 1991.
Fleming MH, Mattingly C. Action and narrative: two dynamics of clinical reasoning. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:54-61.
Glaser R, Chi MTH. Overview. In: Chi MTH, Glaser R, Farr MJ, editors. The nature of expertise. Hillsdale, NJ: Lawrence Erlbaum; 1988:xv-xxviii.
Gruppen LD, Frohna AZ. Clinical reasoning. In: Norman GR, van der Vleuten CPM, Newble DI, editors. International handbook of research in medical education. Dordrecht: Kluwer Academic; 2002:205-230.
Gwyer J, Jensen GM, Hack L, et al. Using a multiple case-study research design to develop an understanding of clinical expertise in physical therapy. In: Hammell KW, Carpenter C, editors. Qualitative research in evidence-based rehabilitation. New York: Churchill-Livingstone; 2004:103-115.
Harris IB. New expectations for professional competence. In: Curry L, Wergin JF, et al, editors. Educating professionals: responding to new expectations for competence and accountability. San Francisco: Jossey-Bass; 1993:17-52.
Higgs J, Jones M. Clinical reasoning in the health professions, 2nd edn. Oxford: Butterworth-Heinemann, 2000.
Higgs J, Titchen A. Practice knowledge and expertise in the health professions. Oxford: Butterworth-Heinemann, 2001.
Holyoak KJ. Symbolic connectionism: toward third-generation theories of expertise. In: Ericsson KA, Smith J, editors. Toward a general theory of expertise. New York: Cambridge University Press; 1991:301-336.
Jensen GM, Gwyer J, Hack LM, et al. Expertise in physical therapy practice. Boston: Butterworth-Heinemann, 1999.
Jensen GM, Gwyer J, Shepard KF, et al. Expert practice in physical therapy. Physical Therapy. 2000;80(1):28-43.
Jensen GM, Gwyer J, Hack LM, et al. Expertise in physical therapy practice, 2nd edn. St Louis: Saunders-Elsevier, 2007.
Jones MA. Clinical reasoning in manual therapy. Physical Therapy. 1992;72:875-884.
Jones MA, Rivett DA. Clinical reasoning for manual therapists. Edinburgh: Butterworth-Heinemann, 2004.
Kennedy M. Inexact sciences: professional education and the development of expertise. Review of Research in Education. 1987;14:133-168.
Loewy EH. The role of reason, emotion, and aesthetics in making ethical judgments. In: Thomasma D, Kissell J, editors. The health care professional as friend and healer. Washington, DC: Georgetown University Press; 2000:210-226.
Mattingly C, Fleming MH. Clinical reasoning: forms of inquiry in a therapeutic practice. Philadelphia: F A Davis, 1994.
Newell A, Simon HA. Human problem solving. Englewood Cliffs, NJ: Prentice-Hall, 1972.
Noddings N. Caring: a feminine approach to ethics and moral education. Berkeley: University of California Press, 1984.
Norman GR, Trott AL, Brooks LR, et al. Cognitive differences in clinical reasoning related to postgraduate training. Teaching and Learning in Medicine. 1994;6:114-120.
Resnik L, Hart D. Using clinical outcomes to identify expert physical therapists. Physical Therapy. 2003;83:990-1002.
Resnik L, Jensen GM. Using clinical outcomes to explore the theory of expert practice in physical therapy. Physical Therapy. 2003;83(12):1090-1106.
Rikers R, Paas F. Recent advances in expertise research. Applied Cognitive Psychology. 2005;19:145-149.
Rivettt D, Higgs J. Experience and expertise in clinical reasoning. New Zealand Journal of Physiotherapy. 1995;23(1):16-21.
Rothstein J. Foreword II. In: Jensen G, Gwyer J, Hack L, et al, editors. Expertise in physical therapy practice. Boston: Butterworth-Heinemann; 1999:xviii.
Rothstein JM, Echternach JL. Hypothesis-oriented algorithm for clinicians: a method for evaluation and treatment planning. Physical Therapy. 1986;66:1388-1394.
Ryle G. The concept of the mind. Chicago: University of Chicago Press, 1949.
Schön DA. The reflective practitioner: how professionals think in action. New York: Basic Books, 1983.
Schön D. Educating the reflective practitioner. San Francisco: Jossey-Bass, 1987.
Schön DA, editor. The reflective turn: case studies in and on educational practice. New York: Teachers College Press. 1991.
Shepard K, Hack L, Gwyer J, et al. Describing expert practice. Qualitative Health Research. 1999;9:746-758.
Sherman N. Emotions. In: Reich W, editor. The encyclopedia of bioethics. 2nd edn. New York: Macmillan; 1995:664.
Sternberg R. Abilities are forms of developing expertise. Educational Researcher. 1998;28:11-20.
Sternberg RJ, Horvath JA. A prototype view of expert teaching. Educational Researcher. 1995;24:9-17.
Sullivan W. Work and integrity: the crisis and promise of professionalism in America. San Francisco: Jossey-Bass. 2005:221-256.
Tsui A. Understanding expertise in teaching. New York: Cambridge University Press, 2003.