Chapter 16 Professional practice judgement artistry
INTRODUCTION
A reflective revolution is occurring in professional practice which requires knowledge beyond science to best provide quality client-centred professional services (Edwards et al 2004; Fulford et al 1996; Higgs & Titchen 2001a, b). In this revolution there is an increasing interest among various professions in challenging the hegemony of biomedical science and the medical model. There is growing support for a wellness orientation in care, and recognition of the unique blend of reasoning approaches which characterize and enrich health care (e.g. Edwards et al 2004, Mattingly & Fleming 1994). If we are to incorporate in practice the breadth of evidence that serves the interests of client/patient-centred care as well as evidence-based practice (which need not be mutually exclusive) then we need to address one of the greatest challenges facing the health professions today; that is, the need to make visible and credible the many invisible, tacit and as yet unexplored aspects of professional practice that are vital to the success of the professions.
This chapter reports on recent research (Paterson 2003, Paterson & Higgs 2001) that addressed this topic by focusing on the fusion of two such invisible and tacit aspects of advanced and expert practice: professional judgement and practice artistry. The construct professional practice judgement artistry (PPJA) was developed to name this merged skill.
PROFESSIONAL ARTISTRY IN PRACTICE
In client-centred health care we are seeing a significant trend to explore and embrace emerging literature (Eraut 1994, Fish 1998, Higgs & Titchen 2001c, Scott 1990, Titchen 2000) that acknowledges the value of artistry within professional practice, alongside science and humanism. Professional artistry is a uniquely individual view of practice within a shared tradition involving a blend of practitioner qualities, practice skills and creative imagination processes (Higgs & Titchen 2001c). It is concerned with ‘practical knowledge, skilful performance or knowing as doing’ (Fish 1998, p. 87) and is developed through the acquisition of a deep and relevant knowledge base and extensive experience (Beeston & Higgs 2001). Importantly, professional artistry does not negate research and theoretical knowledge or scientific evidence for practice; rather the professional artist practitioner uses such knowledge as a significant part of the range of knowledge (including experience-based knowledge) that serves as tools, input and a framework for clinical decision making.
PROFESSIONAL JUDGEMENT
Professional judgement refers to the ways in which practitioners interpret patients’ problems and issues and demonstrate saliency and concern in responding to these matters. It involves deliberate, conscious decision making and is associated with professional competence and judgements that reflect holistic discrimination, intuition and responsiveness reflective of proficient and expert performance (Dreyfus & Dreyfus 1986, p. 2). Judgement is both an action, the process of making evaluative decisions, and the product of these decisions. Health professionals constantly make judgements within, about and as a result of practice. We speak of making a judgement in much the same way as making a clinical decision, but with perhaps a greater emphasis, in judgement making, on the importance of higher level awareness, discrimination and evaluation in the face of the greyness (complexity) of professional practice due to its complexity, humanity, uncertainty and indeterminacy. If decision making in professional practice were entirely procedural and logical it could potentially be reduced to the realm of rules and manuals. However, from the viewpoint of PPJA, to be a professional and to provide professional services means that the client is receiving the benefit of extensive education and the capacity of the professional to make complex, situationally relevant judgements, utilizing a deep and broad store of professional knowledge. Skilled professionals are expected to have both propositional knowledge of the field and also experience-derived knowledge. Clients seek this blend of knowledge in the same way that they want technical competence as well as a depth of experience and artistry in refining these skills to address their unique needs.
OVERVIEW OF THE PPJA RESEARCH
A hermeneutic study (Paterson 2003) was conducted to investigate the question ‘How can the term judgement artistry be understood in relation to occupational therapy (OT) practice?’ The hermeneutic strategy, derived from the work of Gadamer and colleagues (Gadamer 1976, 1981; Gadamer et al 1988), was implemented as a hermeneutic spiral incorporating three hermeneutic strategies:
The text interpretation process involved repeated engagement with the texts, using these three strategies in the hermeneutic spiral. The researchers became deeply immersed in the texts, examining the parts or segments of the texts and then spiralling out to answer questions posed and reflect on the emerging whole or bigger picture of the phenomenon of PPJA being interpreted. Further details of the research strategy are presented in Paterson & Higgs (2005).
PPJA RESEARCH FINDINGS
A) PARTICIPANTS’ Understanding Of Judgement Artistry
The artistry of the judgements, being individually tailored and perceived, is impossible to represent as a single image. However, many of the participants in this research used various metaphors of professional artists at work to portray the special characteristics of judgement artistry. Examples included the artisan (artistry in painters, sculptors and jewellers), the athlete (in dance and sports), the cook/chef and the musician/conductor. In all cases the intention of these metaphors was to illuminate participants’ understanding of PPJA from the viewpoint of either an educator or a practitioner, elicited in a focus group or an individual interview. The unattributed quotations in this chapter are from participants in these different contexts.
An example of describing the therapist with PPJA as a cook came from one participant:
You need proportions of technical skill, philosophy, life experience and you need equal proportions. It is like baking a cake – to be successful you need the right proportions – you’ve got to get the temperature right, the ingredients right.
An educator said that a practitioner with PPJA is similar to:
The notion of an artisan … I think it is like a jeweller: somebody who, for instance, knows the science of the materials they work with, has a vision about what they want to produce, and has some skills and techniques in terms of being able to take the raw materials to the end product … There’s a big difference between a jeweller who has an inert material, which is gold, and working with another human being who is very much not inert. When we look at people who have genius, like Leonardo da Vinci … what they’ve actually done if you look carefully, they’ve actually taken more than one body of knowledge and combined them.
In the tasks of processing and unravelling the highly complex problems that arise in professional practice, PPJA utilizes the unique knowledge base, frame of reference and reasoning capacity of individual practitioners, along with the skilled valuing and inclusion of the client’s knowledge, capabilities and frame of reference. Such problems can involve demanding moral and ethical issues, questions of values, beliefs and assumptions, and the intricacies of health issues as they impact on people’s lives.
B) DIMENSIONS OF PPJA
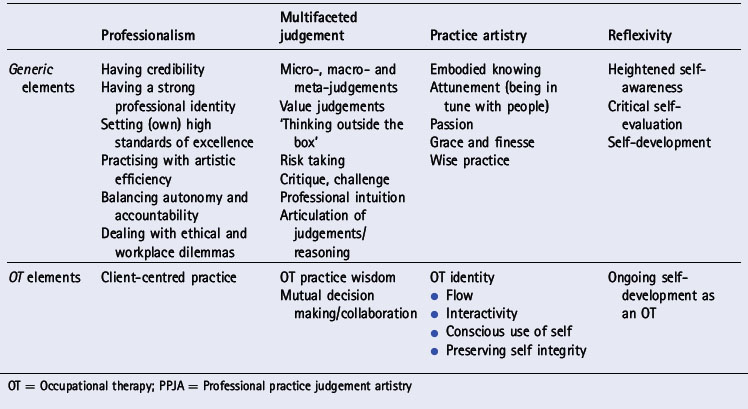
Four key dimensions of PPJA were identified: professionalism, multifaceted judgements, practice artistry and reflexivity (Table 16.1). Within these dimensions were a range of generic elements, some relevant across different professions and some specific to OT. In Table 16.1 the generic elements are so called because as researchers we found authenticity in these labels for many professions, in keeping with literature beyond OT that portrays professional artistry and practice wisdom (Scott 1990), and at multidisciplinary workshops and conferences where we received feedback on the applicability of these elements in other disciplines. More research in other disciplinary areas is required to investigate this question further and to develop other discipline-specific elements.
Professionalism
Professionalism is seen as an integral aspect of PPJA, as well as being the broader context for making high level/artistic professional/clinical judgements. That is, professionalism is a key ingredient of making sound judgements and demonstrating judgement artistry as well as being the overall framework within which professional practice occurs. Professionalism is portrayed by Eraut (1994) as an ideology, characterized by the traits and features of an ‘ideal type’ profession. Professionals are expected to practise with integrity and personal tolerance, to communicate effectively across language, cultural and situational barriers (Josebury et al 1990) and to demonstrate social responsibility (Prosser 1995), accountability and recognition of their limitations (Sultz et al 1984).
During interviews and focus groups the research participants clearly identified the professional nature of practice judgements. For them, practitioners with judgement artistry constantly go beyond required levels of competence in ‘furthering their professional knowledge; keeping up to date with journals; making the theory and practice link; processing and integrating highly complex information’. They blend technical efficiency and evidence with humanity. On an individual client level they weigh ‘the evidence versus the everyday, “what’s important”, the priorities for the person’. The connection with efficiency was identified:
Multifaceted judgement
This is a major feature of PPJA (as opposed to standard decision making), and involves a deep understanding of professional judgement, along with the capacity to artistically, credibly and effectively juggle the many human, technical and contextual facets of judgement at micro, macro and meta levels. Recognition of these different levels and facets of judgement was an important finding of this research (Table 16.2). Judgements can occur at micro (within process), macro (in outcomes and conclusions), and meta (monitoring) levels. Micro-judgements are made constantly in clinical practice. They deal with such questions as: Are these data reliable? How does this joint feel? What instruments and equipment do I need for this procedure? References to macro-judgements occur frequently in the extensive literature on clinical reasoning with a particular focus on making decisions about diagnosis, treatment, and prognosis. The meta-judgement level involves employing metacognition within reasoning and decision making, to refine, question and monitor the reasoning process and challenge the decisions being made. This requires a heightened level of awareness of one’s actions and thinking, and the capacity critically to reflect upon and modify thinking in response to self-evaluation. Meta-judgement is also employed in coming to understand one’s reasoning and learning how to use and choose strategies for making, critiquing and refining judgements.
Table 16.2 Types of professional judgement
| Type of judgement | Definition | Example |
|---|---|---|
| Micro- | Process decisions, or decisions within decisions | Reliability of data, choice of next action/test/question |
| Macro- | Output decisions or conclusions | Diagnosis, prognosis, management plan, agreement with client on healthcare goals |
| Meta- | Reflective evaluative decisions | Awareness of change in client’s responses to intervention, self-monitoring, recognition of communication difficulties |
An example of micro-judgement is recognizing ‘a change in response to different cues’. The larger, macro-judgements are ‘being able to make the right decision at the right time or [within] the bigger picture, bringing together a whole lot of different things’. Meta-judgements involve metacognition and ‘being able to kind of conceive of a big picture and bring a whole lot of pieces together, as distinct from making your actual decision about what your actual intervention’s going to be today’.
Different levels and purposes of judgement were described by one participant as follows:
You see there are different sorts of judgements, aren’t there? … If you have a judgement in the sense of a skilled medical clinical judgement, then there is a collection of data [that leads the practitioner] to make a professional judgement that this is going to be this choice rather than that, and therefore the judgement is critical to deciding on the nature of the treatment. … And then there is the [sort of] judgement that says what should I do now and why; and you make one judgement, and then 30 seconds later you are making another judgement and 30 seconds later you are making another judgement because what you are doing is making decisions about how to handle and support or process this evolving thing that is happening between you and another person or a situation at a particular time. That is a judgement but it is very different from the other two sorts of judgements … It is about the irretrievability of the decision-making: that moment in time has gone and nobody can say whether your decision was right or wrong. … So there is something about the … ephemeral [nature of] professional judgements. … They vanish. They go. They are not there. They are lost in time. You cannot get them back.
Practice artistry
Practice artistry is the embodiment of knowing in practice whereby practitioners bring all of their knowledge and judgement to realization in their practice acts and being.
Embodied knowing was mentioned by various participants as:
something in the eyes [of the practitioner] – the aliveness, the alertness, the constantly watching to see what is going on … that way of connecting, spiritual level, subconscious level – you hear patterns;
Reflexivity
Reflexivity is linked both to the outcome of judgement artistry (i.e. growth and enhanced capability of the practitioner) and an inherent process within it. Judgement artistry by its very nature is reflexive. Within the making of judgements, practitioners are constantly reflecting on their judgements, their capacity for judgement and their practice actions, and learning from these reflections. This is a process of self-critique and self-development. As stated by one educator, you need ‘to be open to growth and development’. Participants believed that ongoing self-development was an important aspect of judgement artistry. For example:
[in] some areas of my practice I’m probably getting towards the top, but I’ve always got lots of reading to do and I always find a client who has got a new problem or a different situation. So I don’t think I will ever be an expert … when you’re more experienced you get through faster. You still consider huge amounts of things.
Overlap of dimensions. In looking at the dimensions listed, the overlap evident between attributes of practice as a whole and judgement which is a part of practice is both remarkable and ‘right’. For the practitioner who is a professional artist, there can be no practice without advanced judgement (PPJA), and for judgement to be demonstrated as advanced artistry it must be embedded within and congruent with the overall practice artistry approach. Just as the professional artist practitioner embodies grace and humanity in interpersonal relationships and finesse in implementing the technical skills of his/her profession, so too, PPJA must be the embodiment of such finesse, grace and humanity in thinking and decision making.
C) Defining PPJA
In drawing the dimensions together we generated the following definition: PPJA refers to ‘the capacity of professional artist practitioners to make highly skilled micro-, macro- and meta-judgements that are optimal for the circumstances of the client and the context’ (Paterson & Higgs 2001).
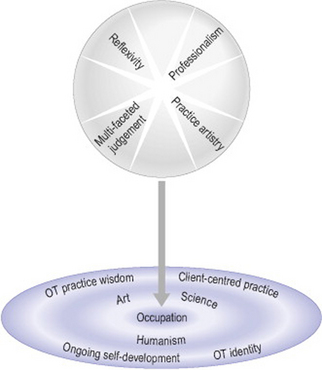
D) A model of PPJA
The research findings were formulated into a model of PPJA (Figure 16.1) which reflects the four dimensions of professional practice judgement artistry (upper section) and PPJA in occupational therapy (lower section). The image created is one of a dynamic whole (PPJA) entering the arena of OT and drawing out elements of PPJA that are consistent with and characteristic of OT. The OT section illustrates the way that PPJA has a deep connection with the philosophical underpinnings of OT in art, science and humanism. In OT the place of occupation is central and the four elements derived from the research participants’ words and text interpretation reflect the essence of OT: client-centred practice, OT practice wisdom, OT identity and ongoing self-development. (For further discussion of PPJA in OT see: Paterson 2003; Paterson et al 2005, 2006.)
WHAT DOES IT MEAN TO PRACTISE USING PPJA?
Firstly, it means understanding professionalism as a means of engaging with people rather than distancing oneself from them. It means knowing one’s professional identity and engaging in self-critique, being able to set high standards for one’s practice and learning to blend artistry and efficiency.
In clinical reasoning education and literature, much attention is given to knowledge and practical skills, with a growing emphasis on clinical decision making. However, even in the latter the focus is on making decisions, the reasoning processes, decision outcomes, novice–expert differences and reasoning in relation to evidence-based practice. This is the approach of science and education; it gives little attention to the subtleties of judgement. Advanced skills and capacity for judgement were identified by the participants in this study as moving beyond mere accuracy and defensibility. Instead, this PPJA mode of making judgements was highly reflexive, requiring heightened levels of self-awareness and critique and resulting in continual self-development. Practitioners evidencing PPJA continued to learn and deepen their professional craft knowledge and understanding of self and others.
In addition, PPJA was recognized in this study as being multifaceted. For such practitioners, judgements were made at multiple levels about multiple aspects of practice, ranging from the evaluation of a single piece of data to being aware of their own values and the values of others and seeking to accommodate diversity in cultural, personal and system values. Judgement involves risk taking rather than rule following. It is the key tool and challenge of the skilled practitioner and is used in making difficult decisions in the majority of clinical situations where the clarity and comfort of black and white decisions are absent and complexity, variability and ‘shades of greyness’ are the order of the day. Making these judgements requires practitioners to draw heavily on all their professional learning, their professional craft knowledge and their professional intuition (that is, a heightened level of awareness and perceptiveness with a greater capacity to make insightful judgments relevant to the unique situation). Articulating the judgements made and the judgements within judgements (why and how the judgement was made) requires practitioners to understand and bring to awareness, through reflection and dialogue, the nature of judgements and judgement making. One participant described a practitioner with PPJA as:
a very good trainer, she’s a very good supervisor and she’s a very good manager; and she’s very adaptable, she’s very reflective in her practice. She was very open to change and was constantly re-evaluating her practice and the practice of the service. [Especially when she is] compared with other colleagues, who might be very resistant to change, be resistant to evaluation. And she wasn’t evangelical to me, but you wouldn’t really know that she was striving to improve things. She did this quite quietly really, but it was in her nature to be a good practitioner. And being a reflective practitioner, you can learn an awful lot more from those people, because they include you in that question, they include you in that problem-solving.
To practise using PPJA demands more than producing legally-, professionally- or evidence-based decisions and outcomes. Those issues and reasoning strategies are not negated by practitioners engaging in PPJA but are subsumed into a holistic approach that places the patient firmly at the centre of practice and recognizes that practice artistry requires more. It demands of the practitioner passion for wise implementation of practice, caring for others, and an understanding and embodiment of all that practice can be beyond technology and efficiency, to achieve an artistry of practice characterized by grace, attunement and finesse. As stated by an educator:
I was talking about grace … something outside ourselves even that allows us to become master clinicians or experts in the area. Some of it is environmental that I went from job to job, always a different area and then [I was] able to put those pieces together, and some people might not be able to do that, but I do think about [it] and I suppose I use grace instead of luck because I think of it some way more deliberate or more thoughtful a word than luck that allows some of us to be able to have that [grace]. … John Dewey talks about intellectual grace. He talks about the idea that there is a moment when the teacher and the learner are transformed to the experience, which to me is the same thing as what I would call the therapeutic grace. There is the moment (and I mean it goes on to be a lifelong moment for some of the clients) where the client and I are transformed or transcend or whatever, so I really like that idea of his [Dewey]. … There is something in the interaction that becomes bigger than all of us.
Some participants spoke about the difference between expertise and judgement artistry. For example:
You can have someone who is technically expert. For instance if you have a hand therapist, who is marvellous at what she does, or he does, and gets the [client’s] hands back and is absolutely wonderful, but doesn’t have the humanism and the ability to nurture the whole person within that injury. The trauma of the injury, the hand injury. … they are an expert, they are marvellous, but they haven’t got that judgment artistry.
WHY IS PPJA RELEVANT TO HEALTH PROFESSIONAL PRACTICE AND HEALTH CARE TODAY?
Within the context of the growing dissatisfaction with the biomedical model as a complete framework for practice today, and the concurrent support for models of wellness and patient-centred care, a common element in healthcare rhetoric is the recognition of the importance of the human world and personal relevance of health care. In part, this is being addressed by a greater valuing and focus on the human sciences in concert with the physical and biomedical sciences. Such an argument is built around the recognition that the value of scientific study is not limited to the physical world, and the status that science accords and receives in the public arena can be shared across both the human and physical worlds.
Secondly, there is the recent trend towards models of collaborative reasoning (Edwards et al 2004). This collaborative trend is a reflection of an increasing societal movement toward greater self-management and prevention (Higgs & Hunt 1999, Richardson 1999), a higher level of accessibility of web-based healthcare information, changing views of health care as empowerment (Mattsson et al 2000, Trede et al 2003), changing healthcare funding strategies with increasing expectations of ‘user pays’ and community care (Lorig et al 1999), and demographic changes (including population ageing, increase in numbers of chronically ill people).
Thirdly, there is recognition of the value of interpretive and critical paradigm research (often jointly called qualitative research) for investigating human and social aspects of health and health care, alongside quantitative or empirico-analytical research with its emphasis on empirical measurement for description, testing and prediction.
Next there is an ongoing debate about what constitutes evidence (Higgs et al 2001). And finally, there is a need to look beyond science to the world of artistry in an endeavour to explore those aspects of care that are reflected in artistry, embodied knowing and the more ephemeral, person-centred and situationally-relevant aspects of caring.
Beeston S, Higgs J. Professional practice: artistry and connoisseurship. In: Higgs J, Titchen A, editors. Practice knowledge and expertise in the health professions. Oxford: Butterworth-Heinemann; 2001:108-117.
Dreyfus HL, Dreyfus SE. Mind over machine: the power of human intuition and expertise in the era of the computer. New York: The Free Press, 1986.
Edwards I, Jones M, Higgs J, et al. What is collaborative reasoning? Advances in Physiotherapy. 2004;6:70-83.
Eraut M. Developing professional knowledge and competence. London: Falmer Press, 1994.
Fish D. Appreciating practice in the caring professions: refocusing professional development and practitioner research. Oxford: Butterworth-Heinemann, 1998.
Fulford KW M, Ersser S, Hope T. Essential practice in patient-centred care. Oxford: Blackwell Science, 1996.
Gadamer HG. Lange D, editor. Philosophical hermeneutics. Berkeley, CA: University of California Press. 1976.
Gadamer H. Reason in the age of science. Cambridge, MA: MIT Press, 1981.
Gadamer HG, Specht EK, Stegmuller W. Hermeneutics vs. science. Notre Dame, IN: University of Notre Dame Press, 1988.
Higgs J, Hunt A. rethinking the beginning practitioner: introducing the ‘interactional professional’. In: Higgs J, Edwards H, editors. Educating beginning practitioners: challenges for health professional education. Oxford: Butterworth-Heinemann; 1999:10-18.
Higgs J, Titchen A, editors. Practice knowledge and expertise. Oxford: Butterworth-Heinemann. 2001.
Higgs J, Titchen A, editors. Professional practice in health, education and the creative arts. Oxford: Blackwell Science. 2001.
Higgs J, Titchen A. Rethinking the practice-knowledge interface in an uncertain world: a model for practice development. British Journal of Occupational Therapy. 2001;64(11):526-533.
Higgs J, Burn A, Jones M. Integrating clinical reasoning and evidence-based practice. AACN Clinical Issues: Advanced Practice in Acute and Critical Care. 2001;12(4):482-490.
Josebury HE, Bax ND S, Hannay DR. Communication skills and clinical methods: a new introductory course. Medical Education. 1990;24:433-437.
Koch T. Implementation of a hermeneutic inquiry in nursing: philosophy, rigour and representation. Journal of Advanced Nursing. 1996;24:174-184.
Koch T. An interpretive research process: revisiting phenomenological and hermeneutical approaches. Nurse Researcher. 1999;6(3):20-34.
Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing utilization and costs: a randomized trial. Medical Care. 1999;37:5-14.
Mattingly C, Fleming MH. Clinical reasoning: forms of inquiry in a therapeutic practice. Philadelphia: F A Davis, 1994.
Mattsson M, Wikman M, Dahlgren L, et al. Physiotherapy as empowerment – treating women with chronic pelvic pain. Advances in Physiotherapy. 2000;2:125-143.
Paterson M. Professional practice judgement artistry in occupational therapy practice. Australia: The University of Sydney, 2003. Unpublished PhD thesis,
Paterson M, Higgs J. Professional practice judgement artistry. Australia: Centre for Professional Education Advancement, The University of Sydney, 2001. CPEA Occasional paper 3,
Paterson M, Higgs J. Using hermeneutics as a qualitative research approach in professional practice. Qualitative Report. 2005;10(2):339-357. Online. Available: http://www.nova.edu/ssss/QR/QR10-2/paterson.pdf 20 Jul 2006
Paterson M, Higgs J, Wilcox S. The artistry of judgement: a model for occupational therapy practice. British Journal of Occupational Therapy. 2005;68(9):409-417.
Paterson M, Higgs J, Wilcox S. Developing expertise in judgement artistry in OT practice. The British Journal of Occupational Therapy. 2006;69(3):115-123.
Prosser A. Teaching and learning social responsibility. Canberra: Higher Education Research and Development Society of Australasia, 1995.
Richardson B. Professional development: 2. professional knowledge and situated learning in the workplace. Physiotherapy. 1999;85(9):467-474.
Scott D. Practice wisdom: the neglected source of practice research. Social Work. 1990;35:564-568.
Sultz HA, Sawner KA, Sherwin FS. Determining and maintaining competence: An obligation of allied health education. Journal of Allied Health. 1984;13(4):272-279.
Titchen A. Professional craft knowledge in patient centred nursing and the facilitation of its development. Oxford: Ashdale Press, 2000.
Trede F, Higgs J, Jones M, et al. Emancipatory practice: a model for physiotherapy practice? Focus on Health Professional Education: A Multidisciplinary Journal. 2003;5(2):1-13.