Chapter 31 Learning the language of clinical reasoning
In this chapter we argue the case for a discursive view of clinical reasoning. We contend that becoming proficient at clinical reasoning is in large part a process of mastering, in particular, the language of a health profession and more broadly the language of healthcare systems. In learning to become competent in clinical reasoning, new practitioners must master a number of aspects of language; these include terminology, category systems, metaphors, heuristics, rituals, narrative, rhetoric and hermeneutics (Loftus 2006, Loftus & Higgs 2006). This interpretive view of clinical reasoning is in contrast to the current and more widespread view that clinical reasoning is, or should be, regarded as a phenomenon of computational logic and symbolic processing, combined with probability mathematics and statistics. The latter view is based within a more empirico-analytical paradigm and, we argue, is less useful as a conceptual model of clinical reasoning and how people come to learn this specialized skill. We draw both on the literature and on recent research (Loftus 2006) that utilized hermeneutic phenomenology to explore the nature of clinical decision making and how it is learned.
THE CENTRALITY OF LANGUAGE
Perhaps the most distinguishing feature of human beings is their use of language. A major problem with discussing language and its role in clinical reasoning is that for too many people language is mistakenly viewed as nothing more than a passive conduit by which meaning is transferred from the mind of one person to another. This is open to challenge. It can be argued that it is language that makes us human (Gadamer 1989). Language is central to human nature and to being human. Being immersed in a world of language allows us to construct meaning intersubjectively through the dialogue and interaction we have with others (Bakhtin 1986). The implication is that to understand reasoning of any kind, including clinical reasoning, we need to study the ways in which practitioners employ language and interaction to address clinical problems, rather than assuming that practitioners use objective mathematical methods to cope with tasks such as diagnosis.
In arguing for exclusively mathematical methods, Descartes (trans. Clarke 1999) made the error of rejecting Aristotle’s notion that different fields of knowledge require different methods and different means of proof. Aristotle (trans. Lawson-Tancred 1991) asserted that mathematical proofs normally have no place in a speech meant to persuade others. It can be argued that clinical reasoning is largely a matter of persuading oneself and others that a particular diagnosis and management plan is correct. Clinical reasoning is therefore a discursive construction of meaning, negotiated with patients, their carers, other health professionals, but above all with oneself. To become proficient at clinical reasoning, health professionals must therefore become proficient in the language skills required to persuade people.
LANGUAGE SKILLS OF CLINICAL REASONING
In recent doctoral research Loftus (Loftus 2006, Loftus & Higgs 2006) sought to gain a deeper understanding of the place of language in clinical reasoning. He studied settings where health professionals and medical students engaged in clinical decision making in groups, including problem-based learning (PBL) tutorials and a multidisciplinary clinic.
The research showed that clinical reasoning can be visualized as a quest for meaning, using the language tools that are part of the interpretive repertoire provided by the community of practice called a health profession. That is, communities of practice provide both the interpretive frames of reference and the language tools for meaning-making by their members. When working in these communities, health professionals need to learn a range of language skills to be used for clinical reasoning. These are represented in Figure 31.1. The skills include knowledge of, and ability to use, appropriate terminology, categories and category systems, metaphors, heuristics and mnemonics, ritual, narrative, rhetoric and hermeneutics. All these skills need to be coordinated, both in constructing a diagnosis and management plan and in communicating clinical decisions to other people, in a manner that can be judged intelligible, legitimate, persuasive, and as carrying the moral authority for subsequent action.
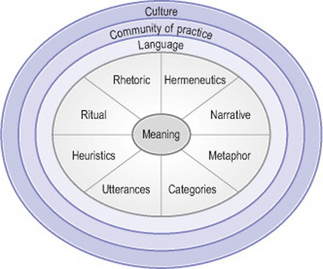
Figure. 31.1 A model for conceptualizing language in clinical decision making and communicating it. These are all embedded within a community of practice and the larger culture. This model emphasizes the construction of meaning through language. It applies to clinical decision making if we see clinical reports as a construction of meaning
TERMINOLOGY/KEY WORDS
Mastering the terminology of a health profession is a basic skill in clinical reasoning, which forms the foundation for the other skills required. This is a matter not just of knowing particular words and phrases, but more importantly, of knowing how and when to use them appropriately. For example, one medical student spoke of acquiring basic skills in psychiatry:
it [psychiatry] has its own little language for speaking to itself and you don’t pick up on that unless you’re using it every day in a group talking to someone … we’d see patients together and we’d discuss the patients and run through it using our little list of jargon terms. … So you got used to using the language and when it came time to sit your exam you felt quite comfortable. (Loftus 2006, p. 140)
Key words can also have profound effects on patients and the ways in which they interpret their illness experience. To a health professional, the expression ‘degenerative changes’ might be interpreted as a normal part of growing older and as something not to be taken too seriously. To patients, the phrase can sound disastrous and could encourage some patients to take on a ‘sick role’. For example, in the multidisciplinary pain clinic studied in the current research, health professionals dealt with patients in chronic pain, and a large part of the clinical reasoning involved seeking out the beliefs that patients built up around such key terms, and the degree to which these beliefs then led into a spiral of deterioration. There was a need to be sensitive to this aspect of language in the world of patients, and the ways in which the narratives that patients lived out could be directed in self-destructive behaviours (or, with help, redirected into self-constructive lifestyles and health behaviours) based on the interpretation of key terms such as degenerative changes. To this extent it is clear that the meanings of these key words can be multilayered and contingent on context. Health professionals need awareness of these issues if they are to help and not hinder their patients’ well-being.
CATEGORIES
Terminology, in turn, forms the basis for the various category systems that health professionals use to conceptualize clinical problems and their solutions. A large part of establishing a diagnosis is deciding upon a category for a patient’s health complaint or need. The biomedical model provides a category system that is in widespread use. Within this model categories can provide a framework that can be successively refined. Basic frameworks that medical students learn to use might include:
Many student participants in Loftus’s (2006) study found that a practice-based method of learning such as PBL gave them familiarity with a clinico-pathological category system that lent itself naturally to clinical practice. As one student observed, ‘This year I’ve realized how helpful they [PBL tutorials] are because it gives you that approach to thinking about things in categories’ (p. 143).
Many novice health professionals begin their clinical education already having learned the category systems of the basic medical sciences, and they find that these scientific categories can be quite different from the more practical categories of the real world of health professional practice. One student spoke of having to reorganize his knowledge in a case-based manner so that it was more fitting for the practice of medicine: ‘I’ve gone through my old notes and progressively thrown them out as I’ve rewritten them into a different format … now I approach learning the diseases in the same way that I would … a patient’ (Loftus 2006, p. 145). In other words, his biomedical knowledge was being reframed around patient narratives he had come across in clinical practice. The category systems used in clinical reasoning need to be appropriate for the practice situation. For example, typical diagnostic categories used by a doctor in chronic pain management were described thus: ‘I think in three components. One is nociceptive … and a neuropathic component … [and thirdly] … psychosocial contributors’ (p. 146). A clinical psychologist, working in the same setting, spoke of three different categories: thought, feelings and behaviour. Categories provide a foundation for metaphors used in clinical reasoning.
METAPHOR
Lakoff & Johnson (1980) argued that thought and language are fundamentally metaphorical. Metaphor is not simply an embellishment of language exploited by writers and poets. It can be argued that language and thought are intensely and inherently metaphorical and, because of this, metaphor use goes largely unnoticed as it is so completely natural to us (Ortony 1993). In recent years there has been a growing recognition of the extent to which metaphor underlies scientific and medical practice and shapes the ways in which both health professionals and their patients conceptualize their health problems and what can be done about them (e.g. Draaisma 2001, Reisfield & Wilson 2004).
A key metaphor underlying the biomedical model is ‘The body is a machine’. This is also the underlying metaphor through which patients in Western societies tend to conceptualize their bodily problems (Hodgkin 1985). The implication of this metaphor is that we can always, in principle at least, repair a broken machine. In acute care this metaphor could be appropriate. However, the metaphor frequently falls down in the chronic situation where repeated attempts at repair fail, resulting in frustration and disappointment for both patients and health professionals. Often such patients are ‘discarded’ by the system as ‘failed’ patients (Alder 2003).
In the Loftus (2006) study the ways in which the staff of the multidisciplinary pain centre described their work indicated that the metaphors at work were more in keeping with caring for chronic patients. For example, one metaphor that suggested itself repeatedly was ‘Life is a journey’. Rather than trying to cure patients, the staff provided interventions, from dorsal column stimulators to cognitive behavioural therapy, to help patients adjust their lives so that they could continue living a relatively normal life despite pain.
HEURISTICS/MNEMONICS
Heuristics and mnemonics are language tools that enable health professionals to manage an enormously complex and growing body of knowledge in ways that best suit the clinical reasoning required when dealing with patients in the real world. Student participants in the Loftus (2006) study who made maximum use of mnenonic and heuristic tools claimed that assessing complex cases became relatively straightforward. Typical mnemonics include the well-known VITAMIN D memory aid used to assist novices in remembering the various disease categories. This particular mnemonic stands for Vascular, Infectious, Traumatic, Autoimmune, Metabolic, Inflammatory/Idiopathic, Neoplastic and Drug-related. Another mnemonic is Dressed In A Surgeon’s Gown, Most Physicians Invent Diagnoses. This translates to: definition, incidence, aetiology, sex, geography, macroscopic/microscopic changes, presentation, investigation, drug treatment. For students, the PBL format itself can provide a heuristic for assessing patients. Medical students in the programme studied reported that by the third year they were entirely familiar with the PBL format. Most reported using the PBL format when assessing real patients, as they believed it was both a rigorous and a comprehensive approach to clinical reasoning. One student reflected: ‘I think it’s a really good idea. It’s how you think clinically’, and she was also persuaded of its normative nature: ‘it’s how you should think clinically’ (p. 166).
Health professionals assessing complex chronic pain cases certainly found that they needed some format to guide assessment. As one physiotherapist said about teaching students: ‘I encourage them [the students] to have a format to start with, because you can get lost with these patients because they can go off on many tangents’ (Loftus 2006, p. 170). Heuristics and mnemonics also tend to be used in a ritualistic manner.
RITUAL
Ritual is closely related to heuristics and mnemonics and plays a part in at least two important aspects of clinical reasoning. The first is the ritual of assessment and the second is the performative aspect of presenting information to others. All health professionals are used to following protocols as frameworks for gathering information. Following a ritual allows the process of gathering relevant information, using the various heuristics and mnemonic devices, to become habitual and routine. Health professionals can then concentrate on diagnosing the patient’s problem and planning treatment without having to be distracted with thoughts about what should be asked for next. In a sense, the ritual guarantees that information gathering will happen appropriately and expeditiously; both are important factors in the busy world of practice accountability. Rituals are closely related to the category systems in use, together with the heuristics and mnemonics built on the categories. Medical students gradually come to realize that the ritualistic nature of PBL, for example, has real-world application in the clinical setting. As one student participant in the study observed:
If someone was to come in with abdominal pain and they’ll [senior doctors] ask you the causes of it … you can sometimes get a bit intimidated by it I suppose. There are so many structures in the abdomen. And you’ll tell them the causes and they’ll ask, ‘What questions do you want to ask them [the patient] to eliminate those?’ So you start asking questions, and then it’s the PBL process. ‘What investigations do you want to do?’ And you realize you did know all the things you needed to know, but you forgot how to approach them. (Loftus 2006, p. 173)
In other words, the ritual of assessment is a means of coping with the complexity of practice. In presenting this observation, however, we emphasize two key matters. Firstly, routines should be tools and guides, not ends in themselves; they serve the needs of data collection, for example. Secondly, no matter how habitual a protocol becomes, it should not be implemented without critical attention to purpose, process and outcomes. Part of assessment, for example, is comparing anticipated to actual assessment findings and reflecting upon any discrepancies. Rituals should serve to decrease the chaotic or highly complex aspects of regular practices without reducing such input to ‘white noise’ within which errors or highly important information can go unnoticed.
Health professionals in multidisciplinary settings routinely have clinical meetings to compare assessment findings and negotiate management plans. These meetings tend to follow simple rituals of procedure that provide for smooth and rapid negotiation. For example, in the multidisciplinary pain clinic in the current study the doctor always presented a report first, followed by the physiotherapist and then a clinical psychologist, culminating in open discussion (Loftus & Higgs 2006). Atkinson (1995) and Hunter (1991) have also described the ritualistic nature, in medical practice, of delivering information to others. Mastering these discursive rituals is part of the process of socialization into a profession. The ritualistic delivery both helps the reporting health professionals to organize their information and, just as importantly, suggests to listeners (or readers of written reports) the systematic and thorough assessment that underlies the report. The ritualistic aspect thus reassures the recipients that the report is both legitimate and sound. As one medical student participant in the study remarked, mastering the rituals of clinical reporting began to make this complex experience seem easy: ‘I gave a very templated response … I would go in and I would say “I spoke to Mr name, age and occupation” … and just have this template of rehearsed framework’ (Loftus 2006, p. 176).
The same medical student echoed the words of Schön (1983, 1987) when he related that it was only the practical experience of following the rituals of assessment that eventually brought true understanding of what the students and clinicians were doing and why it was important to do it that way. Schön claimed that it was not possible for beginners in any profession to fully appreciate what the work involved until they had been completely immersed in the routines of that work for some time. Appreciating the power of routine and ritual in one’s profession is an aspect of growing competence and expertise. Ritual establishes what the business at hand is to be about. As Perelman (1982, p. 10) wrote: ‘Ritual … and rules of procedure fix, with more or less precision, the matters which are the objects of communication.’ It can be argued that much more attention should be paid to the explicit teaching of thoughtful ritual to newcomers within health professions than occurs at present. Although ritual procedures are taught, the fact that they are rituals is often glossed over, and the value of clinical reasoning ritual as a tool to manage complex, disparate and changeable clinical data is underappreciated. If students were made aware of why rituals are so important they might appreciate their value more quickly.
NARRATIVE
A large part of clinical reasoning is the construction of a narrative about a patient within the conceptual framework of a health profession and the specific context of the patient and the workplace. There is a growing realization of the importance of narrative in therapeutic encounters (e.g. Charon & Montello 2002, Greenhalgh 1999). The construction of a clinical narrative is done in a manner that not only takes account of the past and present but also suggests the narrative trajectory that the patient’s story might follow in the future, predisposing towards particular decisions about management. Such narratives can be diagnostic, prognostic and therapeutic. In multidisciplinary settings, patient narratives are best constructed jointly by the clinical team members. All the health professionals in the chronic pain clinic in the Loftus (2006) study needed to rapidly acquire the skill of reducing the findings of an hour’s intensive assessment to a summary that could be delivered verbally in 2 minutes or less. This is a narrative skill requiring more than the ability to simply summarize findings. Health professionals in these settings realized that such a summary must be coherent with their colleagues’ reports to create one comprehensive narrative, providing information that would permit the team to make complex decisions about patient management.
In addition, the physiotherapists and psychologists in that clinic had to acquire the skill of dynamically adjusting their summaries as they listened to their predecessors deliver reports about the same patient. They found that without such dynamic adjustment there would be three overlapping reports with much needless repetition and little cohesion. To prevent this from occurring, the health professionals would frequently dynamically adjust their own reports so that they delivered findings that constructively added to the collective narrative. If there was repetition then it would be deliberate, in order to emphasize an important point or to clarify any confusion. As one physiotherapist observed, ‘your contribution is valid if you add 20 lines rather than repeat 40’ (Loftus 2006, p. 184). Another physiotherapist reported that she had needed to learn ‘what bit of information was it that they wanted from me … you don’t need to go into all the nitty gritty specific stuff that the doctor has already talked about. You’re just basically covering ground that he hasn’t covered’ (p. 184).
Of particular interest is the extent to which this multidisciplinary pain clinic adopted a biopsychosocial approach in order to deal with patients in whom there was a complex interaction between medical, social and more existential issues. Most health professionals find such patients difficult to cope with, as they have such a bewildering array of problems, many of which are beyond the practitioner’s expertise to solve because of their complexity or chronicity. The intense 3-hour multidisciplinary assessments in this particular clinic gave many patients the sense that they had been properly heard for the first time. There was time for Kleinman’s (1988) ‘empathic witnessing’, which many patients found therapeutic in itself. It is encouraging that there is now a growing awareness of the importance of narrative in pain management (Carr et al 2005) and chronic conditions in general (Frank 1995). We hope that this will continue and lead to more attention being paid in practice and education to this aspect of health care, with the goal of a consequent improvement in practice.
RHETORIC
Rhetoric is the art of persuasive speaking or writing. A great deal of clinical reasoning is concerned with persuasion. Health professionals need to persuade other people, patients and their families, and other clinicians that a particular assessment and proposed course of action is both legitimate and sound. One medical student participant in the Loftus (2006) study realized the importance of this issue when reflecting on having to cope with an inadequate clinical report from a colleague: ‘It’s just being able to say what you find, and be able to say that … this person is in very dire straits. It’s not making up stuff, but it’s being able to present it in a convincing and competent manner that they [senior doctors] can say, “All right, this requires my attention”’ (p. 190).
Two factors in the neglect of the role of language and the acts of persuasion and negotiation in clinical practice are the unchallenged rules of science and the equally unchallenged (although in a different frame of reference) rules of economics. In the biomedical sciences and the empirico-analytical paradigm there is a search for the truth, for justification of practice through the use of quantitative research evidence and for credible evidence in a science dominated field and a litigious society. Rather than persuasion, science talks of justification. In the healthcare marketplace ‘the bottom line’ drives much decision making; for example, how many treatments are allowed rather than optimal for the patient? Rather than persuasion, economics talks of financial or cost accountability. So where does the language of persuasion and negotiation fit into health care? Perhaps we need to listen to patients who want to be treated as individuals rather than cases. Perhaps we need to re-ground the acknowledged strengths of the biomedical sciences and technological advancement back into the intrinsic purpose of health services, to enhance the health of people.
Rhetoric, used appropriately, is something that senior practitioners expect from novices and learners. Part of demonstrating their learning, for instance, involves novices and students in persuading their teachers that they understand the clinical situation and the patient’s needs sufficiently to have made a credible decision that goes beyond guesswork or practised answers. Senior doctors have to make decisions about patients based on clinical reports they receive from their juniors. In order to do this, the senior doctors must be persuaded that such reports are reliable and trustworthy. The reliability and trustworthiness come from a combination of the credibility of reported findings and the ritualistic, professional and persuasive manner of the reporting (Hunter 1991).
Atkinson (1995) claimed that rhetorical forms establish authority and attitudes to knowledge and uncertainty. After a ‘long case’ presentation in the Loftus (2006) study, one medical student was told by his examiners, ‘you’ve got to get to the point now where you can lead us to where you want to go’ (p. 192). It seemed that the student’s clinical report needed to be more persuasive, even though the examiners were entirely satisfied that the diagnosis and treatment plan were correct. It is interesting to observe the varied attention that may be paid to students’ decision making prior to graduation and prior to autonomous clinical practice, with all the responsibility for clinical decision making that the latter entails. Is it enough to have reached what the clinical educator sees as ‘the right answer’? Does the student’s management strategy for the patient or the intervention plan match the expectations of the educator, using familiar words and adopting compatible strategies? Beyond these matchings, does the student actually understand the rationale, the consequences and the justification of the chosen approach in comparison to others for this patient’s or client’s unique needs? We argue here that the skill of rhetoric, of presenting a sound argument, not just a solution, is required to examine each of these issues, along with the skill of critical appraisal by both learner and teacher.
In the multidisciplinary pain clinic reported in the Loftus (2006) study, one senior doctor spoke of the need for junior doctors to master the art of producing reports that were persuasive narratives that in turn permitted decisions to be made. ‘The trainees [junior doctors] need to learn that [they have to] cut down the amount of information to a manageable summary for your colleagues … and for yourself because … at the end of the day … you have to be able to isolate them [important findings] and make a decision on them’ (p. 193). This ability is both a narrative and a rhetorical skill. In constructing a clinical report, a health professional is justifying a claim about a patient. The justification is supported by arguments that depend on the context of that patient, and that will stand up to reasonable criticism. As Perelman (1982, p. 162) argued: ‘As soon as a communication tries to influence one or more persons, to orient thinking … to guide their actions, it belongs to the realm of rhetoric.’
There is frequently uncertainty in clinical reasoning, uncertainty that is associated not with self-doubt or the inability to make sound decisions but rather with the ‘greyness’ or complexity of practice situations, the variability of patient’s or client’s needs and the presence in many situations of various acceptable solutions (e.g. management strategies). And, when there is uncertainty, judgements must be made in light of all the information available for that case. This is not done mathematically or statistically but persuasively and argumentatively. This is the essence of rhetoric and of pragmatism; not the abandonment of logic or professional judgement but the incorporation of these into the intensely practical and human world of health care.
HERMENEUTICS
Hermeneutics is the art and study of interpretation. Hunter (1991) argued a strong case that the practice of medicine is a hermeneutic art. Not only must health professionals master the art of constructing persuasive narratives for themselves and others, they must also master the ability of interpreting the reports of other people, whether these reports come from patients or other health professionals. A clinical encounter is a reinterpretation of the patient’s narrative in professional terms. Svenaeus (2000) argued that the philosophical hermeneutics of Gadamer (1989) provides a powerful theoretical framework for conceptualizing clinical encounters. The assessment of a patient is not merely the gathering of objective data. Data have to be selected and interpretively synthesized into a coherent narrative. For example, a clinical psychologist in the Loftus (2006) study spoke of the need to interpret psychometric questionnaire data in the light of a clinical interview: ‘You’ve just met with them, and spoken to them, and had an hour’s discussion with them where they stayed on track, and yet, according to this questionnaire they should be lying in a vegetative state, catatonic. So it’s expressions of need for help that come out of these things’ (p. 203). Despite the claims of the validity and objective measurement of psychometric questionnaires, this health professional realized the need for the interpretation and integration of all findings into a narrative whole. This is a hermeneutic skill that builds upon all the language skills described and discussed so far.
Hermeneutics can also have an ontological aspect. The way we interpret the world can become an integral part of who and what we are. Schön (1983, 1987) recognized that being a professional is not simply knowing a body of knowledge and how to apply it, it is also a way of being in the world. Students have some sense of this when they realize that they can sometimes recognize clinical signs without having to ask certain questions. One student participant spoke of seeing ‘glaring cardiac signs’ (Loftus 2006, p. 199) in a patient. In other words, she did not need to ask herself if the patient had signs of heart disease. She could not stop herself from recognizing that the patient had heart disease. Seeing and recognizing these signs had now become a part of who and what she was. It was a part of her ontology. Mol (2002) discussed this issue at length in her examination of atherosclerosis. A patient’s experience of atherosclerosis is different from that of the vascular surgeon who operates to remove atheromatous plaques. The surgeon’s experience is different again from that of the pathologist who examines a pathological specimen in a laboratory. These people all coordinate their different perspectives and interpretations to produce the phenomenon we know as atherosclerosis.
IMPLICATIONS FOR LEARNING AND DEVELOPING CLINICAL REASONING ABILITIES
Acquiring the art of clinical reasoning is, to a large extent, acquiring mastery of the language of a health profession. Clinical reasoning is learned within the communities of practice (Lave & Wenger 1991) called health professions. A particularly powerful way of conceptualizing how clinical reasoning is learned is the ‘zone of proximal development’ (ZPD) first articulated by Vygotsky (1978). In the ZPD, with the aid of more competent members of the community of practice, students are helped to perform tasks at a level of competence above what they can achieve unassisted. Gradually, as students begin to acquire mastery, the assistance and scaffolding provided by the more competent people are withdrawn until the students are proficient on their own. A key aspect of the ZPD is that tasks are performed socially first. Mastery involves the gradual internalization of skills until students can perform alone. Intellectual tasks are performed inter-psychologically (with others) first and then increasingly intra-psychologically (self-directed). From this viewpoint, clinical reasoning is primarily a social skill.
Hutchins (1995) argued that there can be tasks that are so complex that no one individual is ever expected to master all the skills required and where a team approach is always necessary. Multidisciplinary clinics could be examples of such settings, where patients have such complex problems that a team of health professionals is needed to provide comprehensive assessment and management. Such settings could be said to form a permanent ZPD where team members are always scaffolding and supporting the work of others. This enables the team to perform at an expert level that none of its individual members could hope to emulate.
Many have argued, following Aristotle, that thinking is the internalization of talk we have with others, and that in learning to think we learn to have conversations with ourselves (Bakhtin 1984, 1986; Gergen 1999; Toulmin 1979; Vygotsky 1978, 1986). According to this argument we do not first have thoughts, which are then ‘dressed up’ in language. As Vygotsky (1986, p. 218) explained, ‘Thought is not merely expressed in words: it comes into existence through them’. Wittgenstein (1921/1974, no. 5.6) was of the same opinion: ‘The limits of my language mean the limits of my world.’ Language serves as a means of controlling what we think and how we communicate. To speak a particular language is to inhabit a particular ‘way of being’ (Wittgenstein 1958). Language both shapes and limits how we construct our social realities (Higgs et al 2004).
From this viewpoint, language is of primary importance for understanding the nature of thought. According to Vygotsky, we learn at an early age to perceive the world as much through our language as through our eyes. Clinical reasoning is no exception. It is clear from Vygotsky’s writing that language performs an integrative function. Other symbol systems and cognitive tools can have meaning because they are imbued with language and integrated within it. In the realm of clinical reasoning there are many symbol systems. These can include ECG traces, manual therapy symbols, dental notation, radiographs and MRI scans. Language, in Vygotsky’s view, is the ‘tool of tools’ (Cole & Wertsch 1996) that allows us to bring other symbol systems together into a meaningful whole.
When health professionals assess patients they have a dialogue with the patient and an internal dialogue with themselves. Diagnoses and treatment plans are not statistically calculated, they are arrived at persuasively. This does not deny the importance of evidence-based practice. Rather, the information from the evidence base, like all relevant information about a patient, has to be integrated into the narratives we construct about our patients, and this is done persuasively with the linguistic skills outlined above. Clinical reasoning is a search for the meaning of a patient’s complaint or healthcare need that can be expressed within a narrative form which integrates all the findings about the patient and persuasively suggests the future course. Similarly, for health professionals working with well populations or client groups, professional reasoning is a search for meaning, to produce with or for the client a health promotion strategy that persuasively addresses the client’s needs.
In this view of clinical reasoning, its essence is the acquisition and integration of the various linguistic and discursive skills. If we wish to study how clinical reasoning works and how it is learned we need to look at the dynamics of language use as outlined above. Although all reasoning requires active thinking, we argue that analytic priority should go to the functioning of language, rather than being focused on cognitive mechanisms. Clinical reasoning is a social and linguistic phenomenon that may occur collectively, in conversation and negotiation, but may also be performed in silence by health professionals when working alone.
Alder S. Beyond the restitution narrative. Sydney: University of Western Sydney, 2003. Unpublished PhD thesis
Aristotle. Lawson-Tancred HC, editor. The art of rhetoric. London: Penguin Books. 1991.
Atkinson P. Medical talk and medical work: the liturgy of the clinic. London: Sage Publications, 1995.
Bakhtin M. Problems of Dostoevsky’s poetics. Minneapolis: University of Minnesota Press, 1984.
Bakhtin M. McGee VW, editor. Speech genres and other late essays. Austin, TX: University of Texas Press. 1986.
Carr DB, Loeser J, Morris DB, editors. Narrative, pain, and suffering. Seattle: IASP Press. 2005.
Charon R, Montello M, editors. Stories matter: the role of narrative in medical ethics. London: Routledge. 2002.
Cole M, Wertsch JV. Beyond the social-individual antimony in discussions of Piaget and Vygotsky. Human Development. 1996;39(5):250-256.
Descartes R. Clarke DM, editor. Discourse on method and related writings. London: Penguin Books. 1641/1999.
Draaisma D. The tracks of thought. Nature. 2001;414(6860):153.
Frank AW. The wounded storyteller: body, illness, and ethics. London: University of Chicago Press, 1995.
Gadamer H-G. Truth and method, 2nd edn. New York: Continuum, 1989.
Gergen KJ. An invitation to social construction. London: Sage Publications, 1999.
Greenhalgh T. Narrative based medicine: narrative based medicine in an evidence based world. British Medical Journal. 1999;318(7179):323-325.
Higgs J, Andresen L, Fish D. Practice knowledge – its nature, sources and contexts. In: Higgs J, Richardson B, Abrandt Dahlgren M, editors. Developing practice knowledge for health professionals. Edinburgh: Butterworth-Heinemann; 2004:51-69.
Hodgkin P. Medicine is war: and other medical metaphors. British Medical Journal. 1985;291(6511):1820-1821.
Hunter KM. Doctors’ stories: the narrative structure of medical knowledge. Princeton, NJ: Princeton University Press, 1991.
Hutchins E. Cognition in the wild. Cambridge, MA: MIT Press, 1995.
Kleinman A. The illness narratives: suffering, healing and the human condition. New York: Basic Books, 1988.
Lakoff G, Johnson M. Metaphors we live by. Chicago: University of Chicago Press, 1980.
Lave J, Wenger E. Situated learning: legitimate peripheral participation. Cambridge: Cambridge University Press, 1991.
Loftus S. Unpublished PhD thesis,. Language in clinical reasoning: learning and using the language of collective clinical decision making. Australia: University of Sydney. 2006. Online. Available http://ses.library.usyd.edu.au/handle/2123/1165 9 July 2007
Loftus S, Higgs J. Clinical decision making in multidisciplinary clinics. H Flor, E Kalso, JO Dostrovsky. Proceedings of the 11th World Congress on Pain. International Association for the Study of Pain, IASP Press, Seattle. 2006:755-760.
Mol A. The body multiple: ontology in medical practice. Durham, NC: Duke University Press, 2002.
Ortony A, editor. Metaphor and thought, 2nd edn., Cambridge: Cambridge University Press, 1993.
Perelman C. Kluback W, editor. The realm of rhetoric. Notre Dame, IN: Notre Dame University Press. 1982.
Reisfield GM, Wilson GR. Use of metaphor in the discourse on cancer. Journal of Clinical Oncology. 2004;22(19):4024-4027.
Schön DA. The reflective practitioner: how professionals think in action. New York: Basic Books, 1983.
Schön DA. Educating the reflective practitioner. San Francisco: Jossey-Bass, 1987.
Svenaeus F. The hermeneutics of medicine and the phenomenology of health: steps towards a philosophy of medical practice. Dordrecht: Kluwer Academic, 2000.
Toulmin S. The inwardness of mental life. Critical Inquiry. 1979;6:1-16.
Vygotsky LS. Mind in society: the development of higher psychological processes. Cambridge, MA: Harvard University Press, 1978.
Vygotsky LS. Kozulin A, editor. Thought and language. Cambridge, MA: MIT Press. 1986.
Wittgenstein L, 3rd edn. Anscombe GEM, editor. Philosophical investigations. . Upper Saddle River, NJ:Prentice Hall. 1958.
Wittgenstein L. Pears DF, McGuinness BF, editors. Tractatus logico-philosophicus. London: Routledge & Kegan-Paul. 1921/1974.