Chapter 34 Using decision aids to involve clients in clinical decision making
WHAT IS A DECISION AID?
As the term implies, decision aids are tools that are designed to facilitate health decision making between patient and practitioner. Probably the most widely used definition of decision aids is the following, from the Cochrane Library’s systematic review:
Decision aids are interventions designed to help people make specific and deliberative choices among options by providing information about the options and outcomes that is relevant to a person’s health status. The specific aims of decision aids and the type of decision support they provide may vary slightly, but in general they are designed to enable people to:
Although there is some variation in viewpoints, there is general consensus among international groups (IPDAS 2006) developing decision aids that, in the context of making decisions about health, such tools should be:
We propose that decision aids should also be accessible to people from a range of literacy levels, but the best mechanism for achieving this is still being determined. A more detailed list of quality criteria for decision aids is discussed later in this chapter.
Interest in clinical decision making has been increasing for some time. David Eddy wrote a significant series of essays over a decade ago in which he proposed that health decisions not only include analyses of scientific and clinical evidence but also patient preferences. He maintained that most decisions involved weighing up benefit against harm and that some judgement is involved (Eddy 1996). In the past, such a weighing up process might have been completed by the clinician on behalf of the patient. However, as this chapter will demonstrate, societal attitudes have changed substantially, and patients increasingly want to be involved in these decision-making processes. Clinicians may assume wrongly that their preferences are the same as those of their patients. There is now empiric evidence that consumers and clinicians value at least some treatment outcomes differently. For example, the value patients place on stroke prevention with anticoagulants is different from that of their physicians (Protheroe et al 2000), and families are content to discontinue antiepileptic drugs at different levels of risk than are their physicians (Gordon et al 1996). The concepts proposed by Eddy have been further developed by members of the Evidence-Based Medicine Working Group and others to suggest that research evidence should be combined with clinical expertise, the patient’s clinical state and circumstances and the patient’s preferences and actions (Haynes et al 2002, Trevena & Barratt 2003). Decision aids may be one mechanism by which this can be achieved.
A systematic review of effective strategies for communicating with patients about evidence showed that patients’ understanding of evidence was improved by most structured tools but particularly if they were tailored, personalized and/or interactive. Decision aids have the capacity to achieve tailoring and also to facilitate the elicitation of patient preferences through personalized worksheets and value clarification exercises (Trevena et al 2005).
WHAT IS THE EFFECT OF DECISION AIDS ON PATIENT INVOLVEMENT?
A Cochrane systematic review of 32 decision aids concluded that decision aids increased patient knowledge of the options compared to usual care, with gains in such knowledge ranging from 9 to 30 percentage points (weighted mean difference (WMD) 19 points, 95% CI: 13 to 24). Studies also suggested that decision aids increased realistic expectations about the benefits and harms of different healthcare options as measured by patients’ perception of the probability of outcomes. The review indicated improved patient satisfaction with the decision-making process and greater agreement between patient values and actual choice.
There is some evidence that decision aids increase the proportion of patients who are actively involved in decision making. The Cochrane systematic review included seven randomized controlled trials comparing decision aids against usual care. These trials covered a range of decisions such as prostate cancer screening, treatment of early prostate cancer, treatment of ischaemic heart disease, anticoagulation in atrial fibrillation, colorectal cancer screening and the use of hormone therapy during the menopause. The meta-analysis showed that people receiving a decision aid were 30% less likely to report having a passive (practitioner-controlled) role in their decision (RR 0.7; 95% CI: 0.5 to 0.9). The corollary of this is that decision aids were more likely to be associated with an active role in decision-making (RR 1.4, 95% CI: 1.0 to 2.3). The quality of the decision process was also significantly improved. In particular, uncertainty about decision making (decisional conflict) was significantly reduced (WMD −9.1 of 100, 95% CI: −12 to −6).
HOW CAN WE ASSESS PATIENT INVOLVEMENT?
The measurement of patient involvement in decision making has mainly used the Control Preferences Scale (Degner et al 1997). Patients usually assess their actual or preferred role from the five options shown in Box 34.1.
Box 34.1 Control Preferences Scale
Active role
A. I prefer to make the decision about which treatment I will receive.
B. I prefer to make the final decision about my treatment after seriously considering my doctor’s opinion.
Although this scale continues to be widely used in many studies to measure patient involvement, some researchers have questioned its validity (Davey et al 2004; Entwistle et al 2001, 2004). A systematic review of instruments to measure patient involvement came to a similar conclusion, suggesting that patient involvement is a complex construct that requires more qualitative assessment (Elwyn et al 2001). As a result of this, other instruments have now been used and validated in analysing recorded consultations (Elwyn et al 2005, Shields et al 2005). Both of these instruments expand the Control Preferences Scale to assess whether patients were provided with a range of options, their pros and cons, whether the patient’s preferred level of involvement was assessed, whether questions were invited and clarification offered. The effect of decision aids on patient involvement as measured by these new instruments has not yet been published.
TO WHAT EXTENT DO PATIENTS WANT TO BE INVOLVED IN HEALTH DECISIONS?
There is increasing evidence that a high proportion of people want to be actively involved in a range of health decisions. A telephone survey of 8119 randomly selected adults from eight European countries showed some inter-country variability in the proportion of people wanting to be actively involved in healthcare decisions but overall, the majority preferring such a role. This was particularly so in people under the age of 35 years, of whom 74% indicated a preference for active involvement in treatment decisions (Coulter & Jenkinson 2005). Desire for greater participation in decision making was increased in people with higher socioeconomic status but there was still a substantial proportion of people wanting participation even in the lowest socioeconomic groups (McKinstry 2000). Similarly an Australian survey of 652 women showed that 94.6% preferred to share decisions about diagnostic tests and 91.2% to share treatment decisions (Davey et al 2002). The Australian study, however, showed no difference across age groups.
A closer look shows that what ‘preference for involvement’ actually means to patients can vary not only with culture and age, but also with the decision itself. Cancer patients in one study indicated that involvement for them meant having information but not necessarily making the decision about treatment. They perceived more opportunity for participation in decisions about adjuvant therapy than about definitive surgical management. They also considered that decisions about physical therapies such as stoma care and psychological therapies such as counselling were more amenable to active roles in decision making (Beaver et al 2005). Cancer patients also appear to have different levels of preferred involvement with respect to information needs about prognosis (Leydon et al 2000).
Despite a preference for active involvement, it seems that many patients continue to value the doctor’s opinion in some circumstances. A study of 202 patients attending a general medicine clinic reported that 62.5% preferred shared, 22.5% physician-based and 15.5% patient-based decision making. More than half of respondents rated the doctor’s opinion as the most important information for decision making. These patients were considering decisions about invasive medical procedures such as endoscopy, biopsy, interventional radiology and cardiac catheterization (Mazur et al 2005).
Studies of screening decisions appear to show a higher level of patient preference for involvement. A study of women aged 40–49 considering screening mammography showed that 46% preferred shared and a further 46% preferred patient-based decision making compared with 9% preferring physician-based decision making (Nekhlyudov et al 2005).
DOES PATIENT INVOLVEMENT IMPROVE HEALTH OUTCOMES?
This question has been the source of considerable debate (Coulter 2005). Given the evidence provided about societal attitudes towards involvement in health decisions, one could argue on ethical grounds that a relationship with improved health outcomes is not important. Some have suggested that ‘effective decisions’ are those which are consistent with the patient’s values (Kennedy 2003). Yet others maintain that health care is primarily concerned with improving health and well-being, not just with the processes of decision making (Entwistle et al 1998). A direct link between patient involvement in decision making and improved health and well-being is not well documented.
McNutt (2004) succinctly argued that patient involvement in decision making is concerned with two things: (a) informing them of the consequences of the available options, including the probabilities of these where available; and (b) the opportunity to trade off the benefits and risks for them. This may not result in the patient actually making the final decision but does describe a process of involvement.
Involving patients in health decision making implies some level of choice and autonomy. In some circumstances, patient decisions may not be consistent with population level or policy recommendations. Concerns about this potential source of tension and conflict have been raised, particularly in relation to informed decisions by individuals not to immunize their children or not to participate in population screening (Entwistle 2001, Hargreaves et al 2005). Nevertheless, declining MMR (measles, mumps and rubella) vaccination rates in the UK may also be attributed to uninformed or ill-informed decisions in many cases (Coulter 2005, Parker 2001). As decision aids continue to be evaluated in these decision areas, it appears that involving patients through the use of evidence-based decision aids may facilitate informed decisions that are consistent with the evidence. For example, an online decision aid about the pros and cons of MMR vaccination improved parental attitudes towards vaccination (Wallace et al 2006) and a decision aid about prostate cancer screening reduced the proportion of men who had testing (Gattellari & Ward 2003). Similarly, a decision aid for women considering adjuvant breast cancer therapy showed a reduction in the proportion of women choosing adjuvant therapy in those with low tumour severity who would gain little or no benefit (Peele et al 2005).
WHAT MAKES A GOOD DECISION AID?
Given that decision aids can increase patient knowledge, satisfaction with decision making and involvement in healthcare decisions, and this appears to be consistent with societal attitudes and ethically desirable, we should consider criteria by which the quality of such tools can be appraised.
Internationally there has been a two-stage process to establish such criteria. Firstly, the Cochrane Review group developed the CREDIBLE criteria for evaluating decision aids included in their systematic review and inventory (Box 34.2).
Box 34.2 Cochrane Review CREDIBLE criteria
Secondly, a recent international collaboration has been establishing a more comprehensive set of criteria for judging the quality of patient decision aids. The International Patient Decision Aid Standards (IPDAS) collaboration will make available a detailed list of criteria under the following broad headings (IPDAS 2006; Box 34.3). It is anticipated that the IPDAS criteria will supersede the earlier CREDIBLE checklist.
IPDAS subheadings
Although the final and more detailed list of quality criteria is not yet available, it is worth considering briefly some of the issues that each of the 12 subheadings are concerned with, particularly to judge how these features might facilitate patient involvement in clinical decision making.
1 Using a systematic development process
Users of a decision aid should be able to view the credentials of the developers and authenticate them in some way. Since clinical decision making will involve both patients and practitioners (and sometimes family members as well), these user groups should be consulted about their information needs during development and should pilot test decision aids for acceptability. The development process should also be reviewed by expert peers.
2 Providing information about options
Unlike many traditional forms of patient information, decision aids involve patients by providing balanced information about a range of options (including what happens if you do nothing). In addition to providing background information about the disease and tests or treatments under consideration, they also explain the potential risks as well as the potential benefits of each.
3 Basing information on up-to-date scientific evidence
Decision aids should be based on high-quality evidence. The quality of the evidence and the method used to obtain it should be documented. If relevant, this should be applied to a specific population. It should report when the decision aid was last updated and references should be provided.
4 Presenting probabilities
Outcomes should be quantified (where available) using visual diagrams and presented using natural frequency formats over the same timeframe. Words should also explain the numbers. An example from a published decision aid about hormone therapy during the menopause is shown in Figure 34.1 (Sydney Health Decision Group (SHDG) 2005).
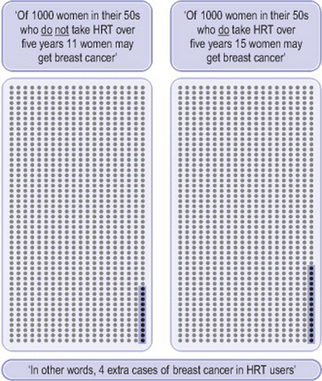
Figure 34.1 Example from decision aid for women considering hormone therapy for menopausal symptoms (SHDG 2005; copyright Commonwealth of Australia, reproduced by permission)
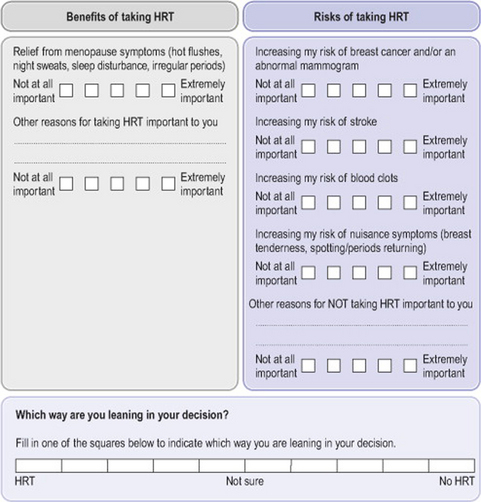
5 Clarifying and expressing values
The decision aid usually contains a personal worksheet or interactive section of a website which provides patients with the opportunity to think about the positive and negative aspects of each option and how important it is for them. This component of the decision aid is important for patient involvement, as it requires them to indicate their preferences. An example of this is given in Figure 34.2.
6 Using patient stories
Some decision aids include videos or written descriptions of patient experiences. If these are included they should represent a range of patient experiences.
7 Guiding/coaching in deliberation and communication
Many decision aids facilitate decision making through a step-by-step approach to the personal worksheet.
8 Disclosing conflicts of interest
Funding sources should be stated, as should any relationship between decision outcomes and the authors. In other words, it should be stated if the authors might gain or lose by the choices patients make using the decision aid.
9 Delivering patient decision aids on the internet
This is an emerging area but a popular one, given the ability to make decision aids more interactive and tailored online. Security of information and clear design are important.
10 Balancing the presentation of options
Presentation of benefits and harms for each option should be consistent. Field testing with patients should assess whether they felt the decision aid was balanced.
11 Using plain language
Readability scores should be no higher than grade 8 and the decision aid should be written at a level that can be understood by at least half the target audience.
12 Establishing effectiveness
Evaluation of the decision aid is important. This should establish that patients understand the available options, are aware of their values associated with the possible outcomes, and appreciate that the decision aid helps them to become more involved in decision-making.
WHERE CAN DECISION AIDS BE FOUND?
The Cochrane systematic review group has established an inventory of decision aids within the Cochrane Library. Some of these can be accessed freely online. The poor accessibility of many decision aids is an issue that needs to be addressed. A number of research groups have links to their decision aids on their website and some of these are listed in Table 34.1.
Table 34.1 Decision aid sources
| Group sources | URL |
|---|---|
| Cochrane Inventory Ottawa Health Research Institute Sydney Health Decision Group |
www.cochrane.org
http://204.187.39.28/decaids.html www.health.usyd.edu.au/shdg/ |
| Specific examples | |
| MMR decision aid HRT decision aid PSA for prostate cancer screen |
http://www.ncirs.usyd.edu.au/decisionaid/index.html
http://www.nhmrc.gov.au/publications/_files/wh37.pdf http://www.prosdex.com/index_content.htm |
DECISION AIDS: WHAT LIES AHEAD?
One of the main issues for future research into decision aids is how they can best be implemented within clinical practice to promote patient involvement in healthcare decisions. As this chapter has shown, there is evidence that decision aids increase patient involvement in clinical decision making by presenting options and helping patients to weigh up what is important for them. We have also highlighted that access to decision aids is not easy, although a highly motivated patient or practitioner could find some using standard search engines on the internet.
It is quite likely that decision aid use will vary depending on the patient and also the clinical decision. Decision aids about surgical treatment options for early breast cancer have included interactive desktop aids that breast surgeon and patient can discuss during the consultation (Whelan et al 2004). Other decisions may be considered by the patient at home before or after visiting a healthcare provider (SHDG 2005). There is probably also a need for information that independent consumers can access in response to concerns they may have, such as regarding the safety of childhood vaccinations (Wallace et al 2006).
Further research is also needed on the effect of decision aids on clinical consultation processes and duration. It is unclear whether patient involvement in this way is a cost-effective use of healthcare resources, albeit ethically desirable.
Nevertheless, the future of clinical decision making in health care is likely to be increasingly concerned with patient involvement. Decision aids appear to be one tool that can facilitate this process. Quality criteria will be important in maintaining the best possible outcomes, but strategies for facilitating access to decision aids and assessing their implementation in clinical practice remain an area of research activity.
The potential role for decision aids in clinical decision making of the 21st century is well described by Muir Gray & Rutter (2003):
The fundamental contract between patient and clinician in the 21st century should start with the assumption that the patient is competent and responsible, providing they are given the resources to exercise that responsibility. There is a need to recognize that some patients would want to ask the clinician to take responsibility for, among other things, managing their records, arranging all aspects of their care, and taking the lead in decision-making. However, many patients would like to be more involved and to take more responsibility themselves. For those patients who wish to use the resources there will, however, be expectations: they will be expected to prepare for the consultation and, if necessary, do homework after it. (Muir Gray & Rutter 2003)
Beaver K, Jones D, Mazur MD, et al. Exploring the decision-making preferences of people with colorectal cancer. Health Expectations. 2005;8(2):103-113.
Coulter A. Shared decision-making: the debate continues. Health Expectations. 2005;8:95-96.
Coulter A, Jenkinson C. European patients’ views on the responsiveness of health systems and healthcare providers. European Journal of Public Health. 2005;15(4):355-360.
Davey H, Barratt A, Davey E, et al. Medical tests: women’s reported and preferred decision-making roles and preferences for information on benefits, side-effects and false results. Health Expectations. 2002;5(4):330-340.
Davey H, Lim J, Barratt A, et al. Women’s preferences for and views on decision-making for diagnostic tests. Social Science and Medicine. 2004;58:1699-1707.
Degner LF, Sloan JA, Venkatesh P. The Control Preferences Scale. Canadian Journal of Nursing Research. 1997;29(3):21-43.
Eddy D. Clinical decision making: from theory to practice. In A collection of essays from the Journal of the American Medical Association. Boston: Jones and Bartlett; 1996.
Elwyn G, Edwards A, Mowle S, et al. Measuring the involvement of patients in shared decision-making: a systematic review of instruments. Patient Education and Counseling. 2001;43(1):5-22.
Elwyn G, Hutchings H, Edwards A, et al. The OPTION scale: measuring the extent that clinicians involve patients in decision-making tasks. Health Expectations. 2005;8:34-42.
Entwistle V. Participation in screening programmes. Health Expectations. 2001;4:79-80.
Entwistle VA, Sowden AJ, Watt IS. Evaluating interventions to promote patient involvement in decision making: by what criteria should effectiveness be judged? Journal of Health Service Research and Policy. 1998;3(2):100-107.
Entwistle V, Skea Z, O’Donnell M. Decisions about treatment: interpretations of two measures of control by women having a hysterectomy. Social Science and Medicine. 2001;53:721-732.
Entwistle VA, Watt IS, Gilhooly K, et al. Assessing patients’ participation and quality of decision-making: insights from a study of routine practice in diverse settings. Patient Education and Counseling. 2004;55(1):105-113.
Gattellari M, Ward J. Does evidence-based information about screening for prostate cancer enhance consumer decision-making? A randomised controlled trial. Journal of Medical Screening. 2003;10(1):27-39.
Gordon K, MacSween J, Dooley J, et al. Families are content to discontinue antiepileptic drugs at different risks than their physicians. Epilepsia. 1996;37(6):557-562.
Hargreaves KM, Stewart RJ, Oliver SR. Informed choice and public health screening for children: the case of blood spot screening. Health Expectations. 2005;8:161-171.
Haynes RB, Devereaux PJ, Guyatt GH. Physicians’ and patients’ choices in evidence based practice. British Medical Journal. 2002;324(7350):1350.
IPDAS. International patient decision aid standards. 2006. Online. Available http://ipdas.ohri.ca/ 20 Sep 2006
Kennedy A. On what basis should the effectiveness of decision aids be judged? Health Expectations. 2003;6:255-268.
Leydon GM, Boulton M, Moynihan C, et al. Cancer patients’ information needs and information seeking behaviour: in depth interview study. British Medical Journal. 2000;320(7239):909-913.
McKinstry B. Do patients wish to be involved in decision making in the consultation? A cross sectional survey with video vignettes. British Medical Journal. 2000;321:867-871.
McNutt R. Shared medical decision making: problems, process, progress. JAMA. 2004;292(20):2516-2518.
Mazur DJ, Hickam DH, Mazur MD, et al. The role of doctor’s opinion in shared decision making: what does shared decision making really mean when considering invasive medical procedures? Health Expectations. 2005;8:97-102.
Muir Gray J, Rutter H. The resourceful patient: 21st century healthcare. 2003. Online. Available http://www.resourcefulpatient.org/ 13 Jul 2005
Nekhlyudov L, Li R, Fletcher SW. Information and involvement preferences of women in their 40s before their first screening mammogram. Archives of Internal Medicine. 2005;165(12):1370-1374.
O’Connor AM, Stacey D, Entwistle V, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database of Systematic Reviews 2006. (3):2006. Online. Available http://www.cochrane.org/reviews/en/ab001431.html 16 Oct 2006
Parker M. The ethics of evidence-based patient choice. Health Expectations. 2001;4:87-91.
Peele PB, Siminoff LA, Xu Y, et al. Decreased use of adjuvant breast cancer therapy in a randomised controlled trial of a decision aid with individualised risk information. Medical Decision Making. 2005;25(3):301-307.
Protheroe J, Fahey T, Montgomery AA, et al. The impact of patients’ preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis. British Medical Journal. 2000;320(7246):1380-1384.
Shields CG, Franks P, Fiscella K, et al. Rochester Participatory Decision-Making Scale (RPAD): reliability and validity. Annals of Family Medicine. 2005;3:436-442.
Sydney Health Decision Group (SHDG). Making decisions: should I use hormone replacement therapy?. 2005. Online. Available http://www.nhmrc.gov.au/publications/synopses/wh35syn.htm 19 Sep 2006
Trevena L, Barratt A. Integrated decision making: definitions for a new discipline. Patient Education and Counseling. 2003;50(3):265-268.
Trevena L, Davey H, Barratt A, et al. A systematic review on communicating with patients about evidence. Journal of Evaluation in Clinical Practice. 2005;12(1):13-23.
Wallace C, Leask J, Trevena LJ. A web-based decision aid pilot improves parental attitudes to MMR vaccination. British Medical Journal. 2006;332(7534):146-149.
Whelan T, Levine M, Willan A, et al. Effect of a decision aid on knowledge and treatment decision-making for breast cancer surgery: a randomized trial. JAMA. 2004;292(4):435-441.