Reproductive Anatomy and Physiology
Objectives
2. Discuss puberty in the developing male and female.
3. Identify the female external reproductive organs.
4. Describe the female internal reproductive organs.
5. Describe the influence of hormones on the female reproductive process.
6. Explain the menstrual and ovarian cycles.
7. Discuss the functions of the uterus.
8. Identify the bones that make up the pelvis.
9. Identify the male organs of reproduction.
10. Review the functions of the male hormone testosterone.
11. Explain the physiology of the sex act in the male and female.
Key Terms
diagonal conjugate (DĪ-ăg-ĕn-ŭl KŎN-jŭ-gĭt, p. 21)
 , p. 20)
, p. 20)follicle-stimulating hormone (FSH) (FŎL-lĭ-kŭl STĬ-mū-lā-tĭng HŌR-mōn, p. 26)
luteinizing hormone (LH) (LŪ-tĕ-nī-zĭng HŌR-mōn, p. 26)
ovulation (ŏv-ū-LĀ-shŭn, p. 20)
oxytocin (ŏks-ē-TŌ-sĭn, p. 22)
prostate gland (PRŎS-tāt glănd, p. 26)
testosterone (tĕs-TŎS-tĕ-rōn, p. 25)
 http://evolve.elsevier.com/Leifer/maternity
http://evolve.elsevier.com/Leifer/maternity
Human reproduction is a complex and fascinating process. The male and female reproductive systems functioning together produce a new life. For an understanding of how human reproduction is possible, knowledge of the structural features and functions of various organs is needed.
Puberty
Before puberty, male and female children appear very much alike except for their genitalia. Puberty involves changes in the whole body and the psyche as well as in the expectations of society toward the individual.
Puberty is a period of rapid change in the lives of boys and girls during which the reproductive systems mature and become capable of reproduction. Puberty begins when the secondary sex characteristics appear (e.g., pubic hair). Puberty ends when mature sperm are formed or when regular menstrual cycles occur. This transition from childhood to adulthood has been identified and often celebrated by various rites of passage. Some cultures have required demonstrations of bravery, such as hunting wild animals or displays of self-defense. Ritual circumcision is another rite of passage in some cultures and religions. In the United States today, some adolescents participate in religious ceremonies such as bar or bat mitzvah or confirmation, but for others, these ceremonies are unfamiliar. The lack of a “universal rite of passage” to identify adulthood has led to confusion for some contemporary adolescents in many industrialized nations.
The Male
Male hormonal changes normally begin between 10 and 16 years of age. Outward changes become apparent when the size of the penis and testes increases and there is a general growth spurt. Testosterone, the primary male hormone, causes the boy to grow taller, become more muscular, and develop secondary sex characteristics such as pubic hair, facial hair, and a deep voice. The voice deepens but is often characterized by squeaks or cracks before reaching its final pitch. Testosterone levels are constant, not cyclic like female hormones, although levels may decrease with age to 50% of peak levels by age 80 years. Nocturnal emissions (“wet dreams”) may occur without sexual stimulation. These emissions usually do not contain sperm.
The Female
The first outward change of puberty in females is the development of breasts. The first menstrual period (menarche) occurs 2 to 2½ years later (ages 11 to 15 years). Female reproductive organs mature to prepare for sexual activity and childbearing. The female experiences a growth spurt, but hers ends earlier than the male’s. Her hips broaden as her pelvis assumes the wide basin shape needed for birth. Pubic and axillary hair appears. The quantity varies, as it does in males.
Female Reproductive System
External Genitalia: Vulva
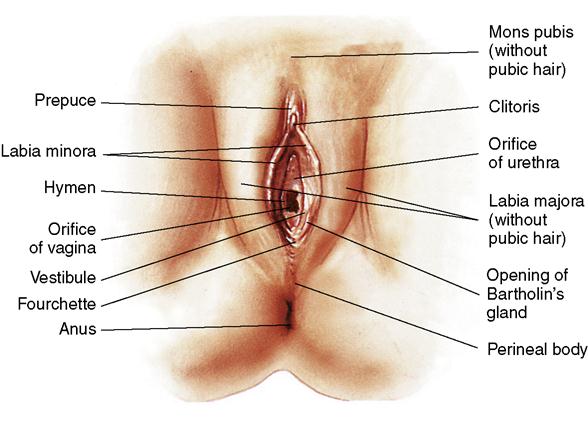
The female external reproductive organs consist of the mons pubis, which is covered with pubic hair; two paired folds of tissue, called the labia majora and labia minora, which surround a space called the vestibule; the vaginal opening; the fourchette; the perineum; the  clitoris; and glandular structures (Figure 2-1). Collectively these structures are known as the vulva.
clitoris; and glandular structures (Figure 2-1). Collectively these structures are known as the vulva.
Mons Pubis
The mons pubis is formed at the upper margin of the symphysis pubis and is shaped like an inverted triangle. It is located over the two pubic bones of the pelvis. This structure is composed of fatty tissue lying beneath the skin and, from puberty on, is covered with varying amounts of pubic hair. The mons pubis surrounds delicate tissue and protects it from injury.
Labia Majora and Labia Minora
The labia majora are two folds of fatty tissue that form the lateral boundaries of the vulva. They are covered with coarse skin and pubic hair on the outer aspect and are smooth and moist on the inner aspect, where the openings of numerous small glands are found. The labia are analogous to the scrotum in the male. Just inside the labia majora are two smaller folds of skin called the labia minora that meet at the fourchette above the anus. This area is also known as the obstetric perineum. It is often the site of lacerations during childbirth.
When the labia majora are separated, the labia minora are exposed. The labia minora are soft folds of skin that are rich in sebaceous glands. The labia minora are moist and are composed of erectile tissue containing loose connective tissue, blood vessels, and involuntary muscles. The functions of the labia minora are to lubricate and waterproof the vulvar skin and to provide bactericidal secretions that help prevent infections.
Clitoris
The clitoris is a small, sensitive structure that, like the penis, is composed of erectile tissue, nerves, and blood vessels; it is covered at its tip with very sensitive tissue. It exists primarily for female sexual enjoyment. Partially hidden at the upper end of the labia, the clitoris may seem to be the opening to an orifice and may be mistaken for the opening to the urethra. In addition, the clitoris secretes a cheese-like substance from the sebaceous glands, which is called smegma. The odor of smegma may be sexually stimulating to the male.
Vaginal Vestibule
The vaginal vestibule is a boat-shaped depression enclosed by the labia minora and is visible when the labia minora are separated. The vestibule contains the vaginal opening, or introitus, which is located between the external and internal genitalia. At the vaginal introitus, there is a thin, elastic, mucous membrane called the hymen. The hymen may be broken by the use of tampons, strenuous physical activity, or sexual intercourse. A broken hymen does not prove the loss of virginity.
The vestibule contains the openings of five structures that drain into it: the urethral meatus, Skene’s ducts, and the ducts from Bartholin’s glands that are located on each side of the vagina. These glands secrete yellowish mucus that lubricates the vagina, particularly during sexual arousal. Skene’s glands are located just inside the urethra and are part of the vestibule. The vestibule ends with the formation of the fourchette. When the nurse is preparing to do a urinary catheterization, he or she cleanses this area of the vestibule.
Perineum
The perineum is the region of the genital area that lies between the vagina and the anus. Because of its location, it plays an important role in the birth process. It is composed of the levator ani muscles, the deep perineal muscles, and the external genitalia muscles. These muscles function as supports to the pelvic organs. The pudendal arteries, veins, and nerves supply the muscles, fascia, and skin of the perineum.
The perineum is supported during the delivery of the infant’s head and shoulders because it stretches significantly during the infant’s birth and may tear. An episiotomy (incision) in the perineal area may be performed to prevent tears in the underlying muscles or tissues; the episiotomy is repaired (sutured) immediately after delivery. Pelvic weakness or painful intercourse (dyspareunia) may result if this tissue does not heal properly.
Internal Reproductive Organs
The internal female organs of reproduction are the ovaries, fallopian (uterine) tubes, uterus, and vagina (Figure 2-2).

Vagina
The vagina is a curved tube leading from the uterus to the external opening at the vestibule. It lies between the urinary bladder and the rectum. Because it meets at a right angle with the cervix, the anterior wall is about 2.5 cm (1 inch) shorter than the posterior wall, which varies from 7 to 10 cm (approximately 2.8 to 4 inches). It consists of muscle and connective tissue and is lined with epithelial tissue, which contains folds called rugae. These folds allow the vagina to stretch considerably during childbirth. The epithelial cells lining the vagina show cyclic changes related to circulating estrogens, progestins, and androgens. Doderlein’s bacilli, which are normally present in the vagina, act on glycogen from the epithelial cells to produce lactic acid. This maintains the acidity of the vagina and is the reason that the vagina is resistant to most infections. A change in the pH of the vagina, which can be caused by frequent douching, antimicrobial therapy, or deodorant tampons, can increase the vagina’s susceptibility to invading pathogens. The cyclic changes in the vagina related to age and changing pH are shown in Figure 2-3. The vagina functions as:
1. A passageway of the uterus through which the uterine secretions and menstrual flow escape
2. A female organ of copulation (sexual intercourse), allowing sperm to enter the uterus
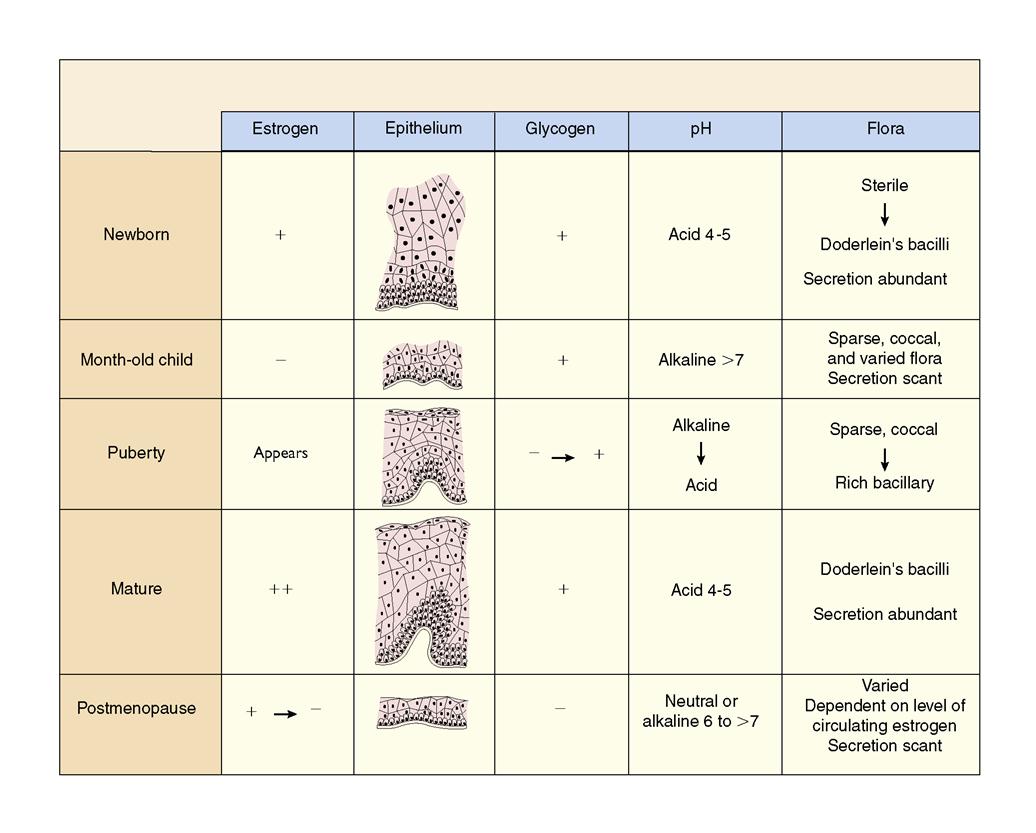
Vulvovaginal glands, called Bartholin’s glands, provide lubrication to the vaginal introitus during sexual arousal but are typically not visible. After puberty, the vagina maintains a normal acidic pH of 4 to 5. Excessive use of vaginal sprays, douches, or deodorant tampons can alter the pH of the vagina and its self-cleansing properties, thus increasing the risk of infection.
Uterus
The uterus (womb) is a hollow, pear-shaped, muscular organ. It is approximately 2.5 cm (1 inch) thick, 5 cm (2 inches) wide, and 7.5 cm (3 inches) long. During pregnancy, the uterus can stretch and enlarge considerably. The weight of the nonpregnant uterus is approximately 75 g (2.5 oz); it increases to approximately 907 g (2 lbs) during pregnancy. During pregnancy, the uterus increases in vascularity, which allows sufficient blood supply for its growth, and can stretch and enlarge to a considerable size. After pregnancy, it returns almost entirely to its former weight, size, and shape. The uterus lies between the bladder and the rectum. It is supported by two important pairs of ligaments, the round and broad ligaments. During pregnancy, these ligaments become stretched, frequently causing discomfort.
The uterus is divided into three parts: (1) the fundus, the upper rounder portion; (2) the corpus (body), the middle portion, which plays an important role in menstruation and pregnancy; and (3) the cervix, the lower portion, which is a tubular structure that projects into the vagina and provides an outlet for menstrual blood and a passageway for the delivery of a fetus.
The fundus and corpus of the uterus are made up of three layers: (1) the perimetrium, the outer layer that envelops the uterus; (2) the myometrium, the middle layer, which is a thick muscular layer; and (3) the endometrium, the inner mucous membrane layer. The endometrium is functional during menstruation and implantation of the fertilized ovum. During menstruation and after delivery, the cells of the endometrium are sloughed off. The myometrium contains muscle fibers that are arranged in the longitudinal, transverse, and oblique directions—a network that offers extreme strength to the organ. It is able to thin out, pull up, and open the cervix so that the fetus can be pushed out of the uterus. The cervix consists of a cervical canal with an internal opening near the uterine corpus, called the internal os, and an opening into the vagina, called the external os. The cervix is known for its elasticity. The mucosal lining of the cervix has four functions: (1) providing lubrication for the vagina, (2) acting as a bacteriostatic agent, (3) providing an alkaline environment to shelter the sperm from the acidic vagina, and (4) producing a mucous plug in the cervical canal during pregnancy.
Fallopian Tubes
The fallopian tubes (uterine tubes or oviducts) extend laterally from the uterus, one to each ovary. They are small, narrow, and approximately 10 cm (4 inches) long. The tubes carry the ovum from the ovary to the uterus by the peristaltic action (contractions) of cilia, or hairlike projections found in the lining of the tubes. Extending from the ends of the fallopian tubes are small, fingerlike projections called fimbriae. Their movements sweep the ovum into the tube, after which the ovum travels to the uterus. It takes approximately 5 days for the ovum to travel the 10 cm from the ovary to the uterus. Fertilization of an ovum with sperm normally takes place in the outer third of the fallopian tube.
Ovaries
The ovaries in the female and the testes in the male are similar in embryologic origin. The ovaries are two small, almond-shaped organs located on each side of the uterus. They are the female gonads, or sex glands. Approximately 2 million ova (eggs) are present at birth. Many ova degenerate until puberty, when a few thousand remain. During the course of a woman’s reproductive life, only about 400 ova mature enough to be fertilized.
During the reproductive years, the ovaries act in concert with the uterus. Saclike structures are in various stages of maturity; as they mature, they are called follicles. During each menstrual cycle, one follicle matures into what is called a graafian follicle, which contains the ovum that is released each month during ovulation.
Estrogen, secreted by the ovary, stimulates the development of secondary sexual characteristics, such as the breasts. Progesterone is responsible for preparing and maintaining the lining of the uterus for implantation of the ovum. Any remaining ova after the climacteric (menopause) will not respond to hormonal stimulation to mature.
Pelvis
The female bony pelvis has the unique functions of supporting and protecting the pelvic contents, as well as forming a relatively fixed passage through which the fetus travels during the birth process. Therefore, its size and shape are important factors in the mechanisms of labor and birth.
The pelvis is made up of four bones: the two innominate bones (hip bones), the sacrum, and the coccyx. The pelvis resembles a basin or bowl; its two sides are the innominate bones, and its back is composed of the sacrum and coccyx. The four bones are lined with fibrocartilage and held tightly together by ligaments. These bones are joined in the front by the symphysis pubis and in the back by the sacroiliac joints and the sacrococcygeal joint (Figure 2-4).
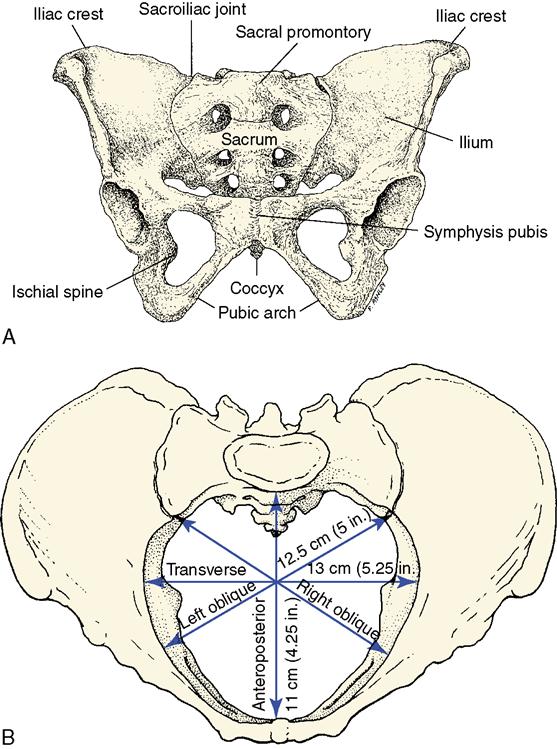
The innominate bones result from the fusion of the ilium, the ischium, and the pubis. The two ilia form the upper part of the pelvis, known as the false pelvis. The ischial spines, sharp projections that form the posterior border of the ischium, are important landmarks and represent the shortest distance (diameter) of the pelvic cavity. The spines can be palpated during a vaginal examination and are used to determine how far the fetal head has descended into the birth canal. The ischium is a heavy bone below the ilium that forms the lower part of the innominate bone. Its protuberance, the ischial tuberosity, is the part on which the body rests while in a sitting position. The pubis is the part of the innominate bone that forms the front of the pelvis. It consists of two pubic bones that unite to form a joint, called the symphysis pubis, a rounded arch under which the fetal head must pass as it emerges from the birth canal.
Pelvic Divisions
The pelvic cavity is divided into two sections, the false pelvis and true pelvis. The linea terminalis is an imaginary line that separates the pelvis into the true pelvis and false pelvis. The false pelvis is the portion above the pelvic brim (upper portion) and has little obstetric significance. However, it does support the growing uterus during pregnancy and directs the presenting fetal part (usually the head) into the true pelvis near the end of pregnancy. The true pelvis (the lower part) consists of the inlet, pelvic cavity, and outlet and is most important during birth.
Pelvic Measurements
The bony circumference of the true pelvis is made up of the sacrum, the coccyx, and the lower part of the innominate bones. This area determines the size and shape of the pelvis, which must be adequate for passage of the baby during labor and birth. For convenience, three imaginary flat surfaces crossing the pelvis have traditionally been described: the plane of the pelvic inlet, the plane of the (shortest dimensions) midpelvis, and the plane of the outlet. The diameter of the midpelvis (bordered posteriorly by the sacrum, laterally by the ischial spines, and anteriorly by the symphysis pubis) can be most accurately measured by an x-ray examination. Because x-rays are potentially hazardous to the fetus, their use is all but obsolete. An evaluation of adequacy may be based on the prominence of the ischial spines and the degree of convergence of the sidewalls. The outlet is a clinical measurement made by palpating the distance between the ischial tuberosities. This diameter is shortened when the pubic arch is narrow; therefore, the pubic arch is assessed for curvature or for the type of pelvis. A magnetic resonance imaging (MRI) pelvimetry may be indicated when there is high suspicion for labor dystocia.
A clinical measurement used to predict pelvic size is the diagonal conjugate. The diagonal conjugate is the distance from the lower margin of the symphysis pubis to the sacral promontory (Figure 2-5). The examiner measures this diameter by placing two fingers in the woman’s vagina and touching the sacral promontory. The optimal distance for most women is 11.5 cm (4.5 inches). This procedure may be part of the prenatal examination and may be uncomfortable for the patient. The woman should be prepared for the pelvic examination by being instructed to empty her bladder beforehand and to take deep breaths during the examination.

Pelvic Types
The four basic pelvic types are (1) gynecoid, or normal female-type pelvis, which is round; (2) android, or male-type pelvis, which has a heart-shaped outlet; (3) anthropoid, which has a long anteroposterior outlet; and (4) platypelloid, which has a wide transverse outlet and is not favorable to a vaginal delivery (Figure 2-6). The gynecoid pelvis is adapted for childbirth. Its inlet, cavity, and outlet are in better proportion; the pubic arch is wide; and the coccyx is more movable than in the android pelvis.

Endocrine System and Female Reproduction
The Normal Menstrual Cycle
A woman’s reproductive life has a definite beginning and ending; it begins at puberty and ends at menopause, or climacteric. Puberty is when reproduction becomes possible and other events such as breast development, growth of pubic and axillary hair, and menstruation occur. During the female reproductive years, cyclic changes occur in the ovaries and in the uterus. These changes can be considered as two interrelated cycles: the menstrual cycle and the ovarian cycle (Table 2-1).
Table 2-1
| Phase | Characteristics |
| Menstrual Cycle (Occurs When Ovum is Not Fertilized, Approximately 14 Days After Ovulation) | |
| Menstrual phase (days 1-5) | Endometrium is shed. Estrogen levels are low. Cervical mucus is scanty, viscous, and opaque. |
| Proliferative phase (days 6-14) | Endometrium thickness increases. Estrogen levels increase. Cervical mucus increases in elasticity, is called spinnbarkeit, and shows ferning pattern (indicates ovulation). Cervical mucus is more favorable to sperm. |
| Secretory phase (days 15-26) | Estrogen levels decrease and progesterone dominates. Endometrial cells become thicker, dilated, and tortuous. Glycogen is secreted by endometrial glands in preparation for the fertilized ovum. |
| Ischemic phase (days 27-28) | Both estrogen and progesterone levels fall as the corpus luteum degenerates. Spiral arteries undergo vasoconstriction, causing a deficiency of blood necessary for the endometrium. Blood pools and escapes through the endometrial surfaces (beginning of next menstrual phase). |
| Ovarian Cycle | |
| Follicular phase (days 1-14) | Ovarian follicle (ovum) matures under the influence of two hormones: FSH and LH. Follicle secretes estrogen, which accelerates maturation, and moves toward surface of ovary and is called graafian follicle. Estrogen produced affects the uterine lining (endometrium). Graafian follicle ruptures, and ovulation occurs with a surge of LH. |
| Luteal phase (days 15-28) | After the rupture of the follicle, the ovum enters the fallopian tube and travels to the uterus; corpus luteum develops under LH influence and produces high levels of estrogen and progesterone. Increased estrogen and progesterone levels suppress the growth of other follicles. If fertilization does not occur, the corpus luteum atrophies, LH levels fall, and estrogen and progesterone levels decrease. |
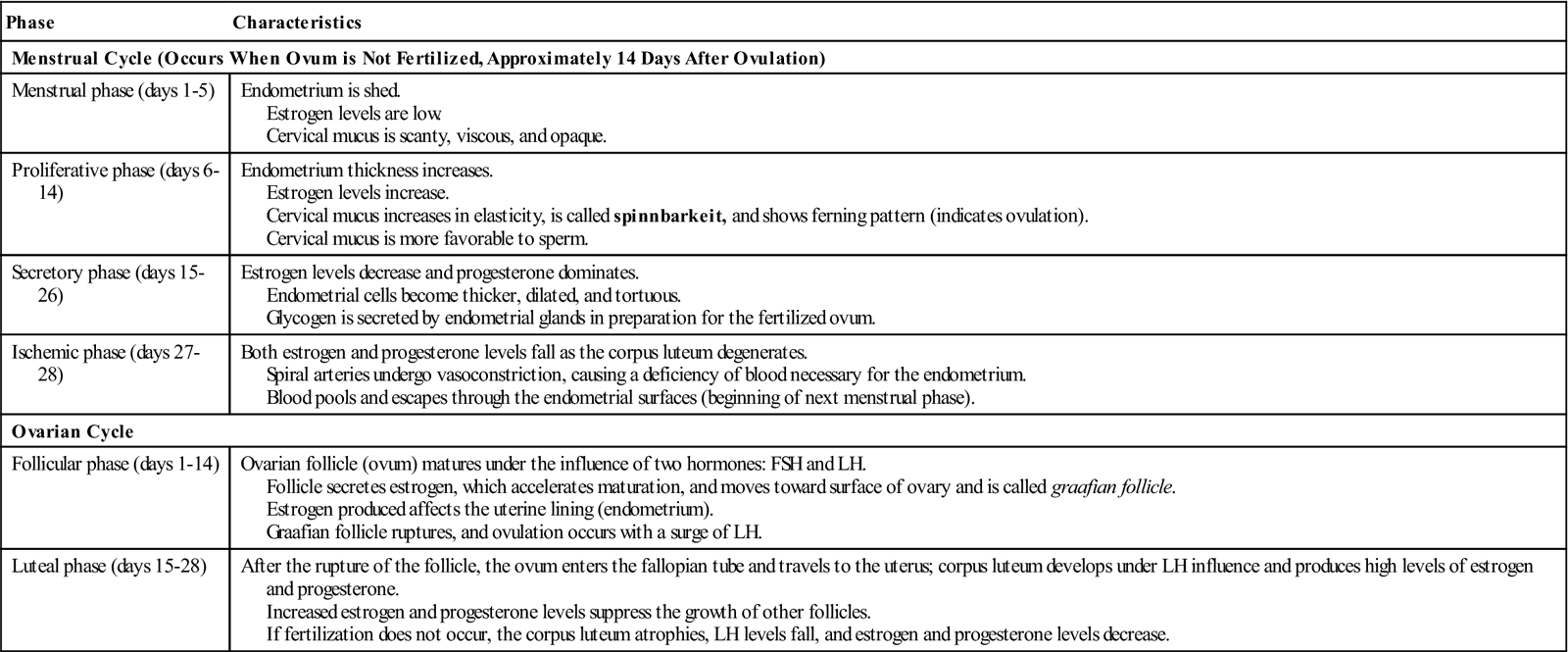
The menstrual cycle is a predictable event that normally occurs monthly. The typical monthly menstrual cycle is influenced by ovarian follicle maturation, ovulation, and corpus luteum formation and ends with menstrual bleeding (Figure 2-7). The changes that occur in the uterus depend on the changes occurring simultaneously in the ovaries. In this unique pattern of events, the development of the endometrium occurs at the precise time of the month that the release of a mature ovum occurs.
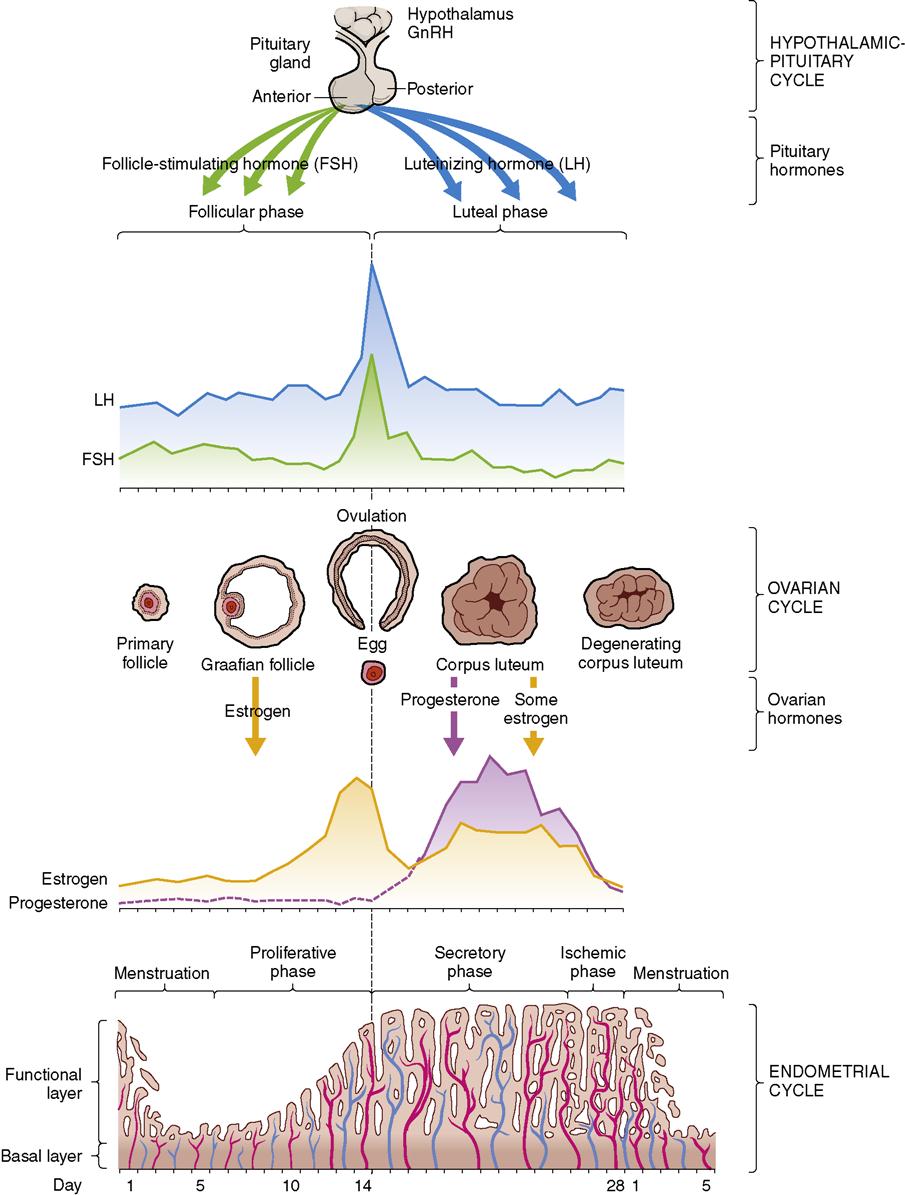
Ovulation occurs 14 days before the beginning of the next menstrual cycle, and the ovum remains fertile for approximately 24 hours. The sperm can survive up to 5 days. Fertilization most often occurs in the first few hours after ovulation.
Breasts
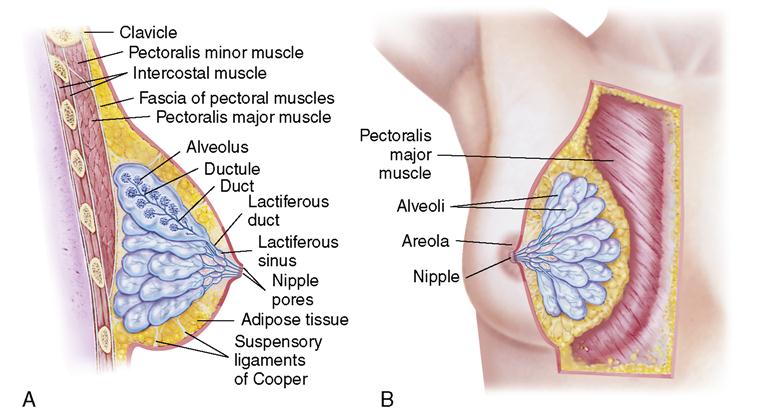
The breasts, or mammary glands, are considered accessory organs of reproduction because of their functional role in producing milk to feed and nourish the infant (Figure 2-8). The process is called lactation. The nipple, in the center of the breasts, is surrounded by a pigmented areola, which darkens during pregnancy. Montgomery’s glands (also known as Montgomery’s tubercles) are small sebaceous glands in the areola that secrete a substance that lubricates and protects the breasts during lactation (when the infant sucks). Beginning at the nipple, each breast is divided into 10 to 20 branchlike structures called lobes, which can be visualized as a treelike structure. They are separated by adipose (fatty) and fibrous tissue. Branching off from each lobe are 20 to 40 lobules; each lobule branches further, dividing into 20 to 80 saclike structures, called alveoli. These saclike structures have a lining that contains tiny secretory cells, called acini, which secrete milk. Surrounding the alveolar cells are contractile cells, called myoepithelial cells, which contract the alveolus and eject milk into the reservoir, called the lactiferous ducts. It is from these ducts that the infant, by sucking, gets milk through the nipple.
During pregnancy, high levels of estrogen and progesterone produced by the placenta inhibit milk secretion. After the expulsion of the placenta, there is an abrupt change in estrogen and progesterone levels. This allows a hormone, called prolactin, to be released from the anterior pituitary gland when the infant sucks. Prolactin stimulates the acini cells to produce milk. Infant suckling also stimulates the release of the hormone oxytocin from the posterior pituitary gland. Oxytocin stimulates the contraction of the myoepithelial cells, which causes the ejection of milk from the alveoli into the ductal system (see Chapter 11).
The size of the breasts depends on the amount of fatty tissue deposited in the breasts. Breast size does not indicate the amount of milk the breasts will produce.
Male Reproductive System
The male reproductive system includes the testes, glands, and ducts, which are internal structures, and the penis and scrotum, which are external structures (Figure 2-9).

External Male Genitalia
Penis
The penis is the male organ of copulation (sexual intercourse) and is part of the urinary system. The penis is made up of three columns of erectile tissue covered by thick skin that is freely movable. Two of the columns, the cavernous bodies, contain blood spaces, which when empty cause the penis to be limp (flaccid). When emotional or sexual stimulation occurs, these spaces fill with blood and the penis becomes engorged (swollen), considerably enlarged, and erect. The third column of erectile tissue, the spongy layer, lies beneath the cavernous bodies. Through it passes the urethra from the urinary bladder. The head of the penis is composed of an enlarged portion of spongy tissue, which forms a cap called the glans penis. Covering the glans is the loosely fitting skin, called the prepuce, or foreskin. The foreskin is sometimes removed by circumcision for hygienic, religious, or cultural reasons. The penis has the following functions:
Scrotum
The scrotum is the wrinkled, pigmented pouch of skin, muscle, and fascia that lies beneath the penis and outside of the abdominal cavity. It is divided into two sacs, with each sac containing one testis (testicle), the epididymis, and a portion of the spermatic cord. Because the sperm require a temperature slightly lower than normal body temperature for development and maintenance, when the body temperature is high, the muscles of the scrotum relax, dropping the testes away from the body. Conversely, when exposed to low temperatures, the muscles of the scrotum are stimulated to contract and bring the testes close to the body for warmth.
Internal Male Structures
Testes
The testes are two oval-shaped glands approximately 5 cm (2 inches) long and 2.5 cm (1 inch) wide, located within the scrotal sac. They correspond to the ovaries of the female. Each testis contains specialized tissue arranged in coiled tubes, called seminiferous tubules, where the spermatozoa (sperm) are produced. Between the small tubes is a small group of interstitial (Leydig’s) cells that produce the male sex hormone testosterone. This hormone is responsible for the masculine characteristics of the male body. Some of the seminal fluid, or semen, in which the spermatozoa are transported, is also produced in the tubules in the testes. The two principal functions of the testes are to manufacture sperm cells (spermatogenesis) and to secrete male hormones (androgens).
Within the testes is an elaborate ductal system. The tubelike path in each testis includes the epididymis, the vas deferens, and the seminal vesicles.
Epididymis
The testes open into the epididymis, a small coiled tube that, if stretched to its full extent, is approximately 6 m (20 feet) long. It becomes the vas deferens and is the excretory duct of each testis that provides a reservoir for the sperm. Sperm may be maintained within the epididymis for up to 3 weeks as they mature and become motile.
Vas Deferens
The vas deferens, a tube approximately 45 cm (18 inches) long, is a continuation of the epididymis. It ends by joining the duct of the seminal vesicle to form the ejaculatory duct. It carries the sperm from each testis to the urethra. The peristaltic activity of the muscles is responsible for the passage of the sperm along the vas deferens to the ejaculatory duct. A vasectomy, or severing of the vas deferens, is a means of male birth control.
Ejaculatory Duct
The ejaculatory duct is found at the base of the prostate gland and opens into the prostate portion of the urethra. It ejects sperm and seminal fluid into the urethra.
Accessory Glands
The accessory glands produce secretions for the following purposes:
Seminal Vesicles
The seminal vesicles are two saclike structures at the base of the urinary bladder. Their glandular lining produces a thick, milky secretion that forms much of the ejaculated semen. This secretion is thought to provide nourishment and protection for the sperm. The ducts of the seminal vesicles join the vas deferens to form the ejaculatory ducts, which empty into the urethra.
Prostate Gland
The prostate gland is a chestnut-sized structure that surrounds the urethra, just below the urinary bladder. During ejaculation, it contracts along with the vas deferens and seminal vesicles. It adds a thin, milky, alkaline fluid to the semen. The alkalinity of the fluid contributes to fertilization of an ovum. It helps neutralize the relatively acidic fluid of the vas deferens and the acidic environment of vaginal secretions, thereby enhancing sperm motility and life span.
Bulbourethral Glands (Cowper’s Glands)
The bulbourethral glands are approximately the size of a pea and are situated by the prostate gland on each side of the urethra. These glands secrete mucus into the urethra to serve as a lubricant and to supply alkaline fluid to the semen.
Endocrine System and Male Reproduction
As in the female, many changes occur in the male at puberty. At roughly 10 years of age, the testes, prostate gland, seminal vesicles, and penis begin to enlarge as part of the general adolescent growth spurt. Pubic and axillary hair and hair on the upper lip and chin appear, and the larynx enlarges. By age 15 years (range, 9 to 17 years), boys are physically able to produce and ejaculate sperm.
During puberty, the pituitary gland begins to release follicle-stimulating hormone (FSH) and luteinizing hormone (LH) (interstitial cell-stimulating hormones). FSH helps in the production of spermatozoa. LH acts on the interstitial Leydig’s cells of the testes to release androgens, the most significant of which is testosterone.
Spermatogenesis
The formation of sperm (spermatogenesis) begins at puberty and continues throughout a male’s life. A sperm’s fertile life is estimated to be up to 5 days after ejaculation. Sperm are much smaller than ova. Sperm cells resemble tadpoles in shape, with oval heads and long tails. During each ejaculation, approximately 300 million sperm are deposited into the vagina. Only a few sperm achieve proximity to the ovum. Typically, only one sperm penetrates and fertilizes the ovum released at ovulation. Immediately after one sperm enters the ovum, a physiologic change takes place in the outer surface of the ovum that prevents entry of additional sperm. Presumably, this change occurs in response to a substance released from the cytoplasm of the ovum.
Physiology of the Sex Act
The sexual response occurs in the following phases:
Excitement: Heart rate and blood pressure increase; nipples become erect.
Plateau: Skin flushes, erection occurs, and semen in the male appears on head of penis.
Orgasm: Involuntary muscle spasms of rectum, vagina, and uterus occur in the female; ejaculation occurs in the male.
Resolution: Engorgement resolves; vital signs return to normal.
Physiology of the Male Sex Act
The male psyche can initiate or inhibit the sexual response. The massaging action of intercourse on the glans penis stimulates sensitive nerves that send impulses to the sacral area of the spinal cord and to the brain. The parasympathetic nerve fibers cause the relaxation of penile arteries, which fill the cavernous sinuses in the shaft of the penis so that the penis becomes firm and elongated (erection). The same nerve impulses cause the urethral glands to secrete mucus to aid in lubrication for sperm motility. The sympathetic nervous system then stimulates the spinal nerves to contract the vas deferens and cause expulsion of the sperm into the urethra (emission). Contraction of the muscle of the prostate gland and seminal vesicles also expels prostatic and seminal fluid into the urethra, contributing to the flow and motility of the sperm. The nerves in the sacral region of the spinal cord aid in expelling semen from the urethra (ejaculation). The period of emission and ejaculation is called male orgasm.
Within minutes, erection ceases (resolution), the cavernous sinuses empty, penile arteries contract, and the penis becomes flaccid. Sperm can reach the woman’s fallopian tube within 5 minutes and can remain viable in the female reproductive tract for 4 or 5 days. Of the millions of sperm contained in the ejaculate, a few thousand reach each fallopian tube but only one typically fertilizes the ovum. The sphincter in the base of the bladder closes during ejaculation so that sperm does not enter the bladder and urine cannot be expelled.
Physiology of the Female Sex Act
The female psyche can initiate or inhibit the sexual response. Local stimulation by massage to the breasts, vulva, vagina, and perineum creates sexual sensations. The sensitive nerves in the glans of the clitoris send signals to the sacral areas of the spinal cord, and these signals are transmitted to the brain. Parasympathetic nerves from the sacral plexus return signals to the erectile tissue around the vaginal introitus, dilating and filling the arteries and resulting in a tightening of the vagina around the penis. These signals stimulate the Bartholin’s glands at the vaginal introitus to secrete mucus that aids in vaginal lubrication. The parasympathetic nervous system causes the perineal muscles and other muscles in the body to contract. The posterior pituitary gland secretes oxytocin, which stimulates the contraction of the uterus and dilation of the cervical canal. This process (orgasm) is believed to aid in the transport of the sperm to the fallopian tubes. (This process is also the reason why sexual abstinence is advised when there is a high risk for miscarriage or preterm labor.)
After orgasm, the muscles relax (resolution). The egg lives for only 24 hours after ovulation; therefore, sperm must be available during that time if fertilization is to occur.
Get Ready for the NCLEX® Examination!
Key Points
• Human reproduction requires an interaction between the reproductive organs, the central nervous system, and the endocrine system (pituitary, hypothalamus, ovaries, and testes).
• The female reproductive system consists of external and internal organs. The ovaries are where the female sex cells (ova) are formed. The fallopian tubes capture the ovum (egg) and transport it to the uterus, which provides an implantation site for the fertilized ovum (blastocyst). The lowest part of the uterus, the cervix, provides an opening into the vagina, which is a passageway from the cervix to the external genitalia. The vagina provides a passage for the discharge of menstrual blood and, during birth, a way for the fetus to be delivered outside of the body.
• The myometrium (middle muscular uterine layer) is functional in pregnancy and labor. The endometrium (inner uterine layer) is functional in menstruation and in the implantation of a fertilized ovum.
• There are four basic pelvis shapes, but women often have a combination of characteristics. The gynecoid pelvis is the most favorable for vaginal birth.
• The female reproductive system maintains a complex cycle known as the menstrual cycle. This cycle involves the ovaries and the uterus in the process of preparing for conception, making changes in the uterine lining to support the embryo if conception occurs, and shedding the uterine (endometrial) lining through the process of menstruation if pregnancy does not occur.
• The breasts, or mammary glands, are generally considered part of reproduction because of their functional relation, that is, secreting milk (lactation).
• The male reproductive system consists of external and internal organs. The testes are where the male sex cells and male sex hormones are formed. There is a series of continuous ducts through which spermatozoa are transported outside of the male’s body. Secretions are produced for sperm nutrition, survival, and movement. The penis serves as the male reproductive organ for sexual intercourse.
• Testosterone is the principal male hormone. Estrogen and progesterone are the principal female hormones. Testosterone secretion continues throughout a man’s life, but estrogen and progesterone secretions are very low after a woman reaches the climacteric.
• The formation of sperm (spermatogenesis) begins at puberty and continues throughout life. A sperm is smaller than an ovum. Usually, only one sperm fertilizes a single ovum (egg) released at ovulation.
Additional Learning Resources
 Go to your Study Guide on page 475 for additional Review Questions for the NCLEX® Examination, Critical Thinking Clinical Situations, and other learning activities to help you master this chapter content.
Go to your Study Guide on page 475 for additional Review Questions for the NCLEX® Examination, Critical Thinking Clinical Situations, and other learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer/maternity) for the following FREE learning resources:
 Online Resources
Online ResourcesReview Questions for the NCLEX® Examination
1. The first outward change of puberty in females is:
1. Appearance of pubic and axillary hair
2. The acidic pH of the vagina is maintained by:
4. Circulating estrogens, progestins, and androgens
4. During the excitement phase of the male sexual response
4. During what phase of the male sex act does flushing of the skin occur?
5. Sperm can remain viable in the female reproductive tract for approximately:
6. The vaginal vestibule contains what structure(s)? (Select all that apply.)
7. Fallopian tubes provide what function(s)? (Select all that apply.)
1. Site of implantation for the fertilized ovum
2. Passageway in which sperm meet the ovum
4. Site for development and maturation of the ovum
5. Means of transporting the ovum to the corpus of the uterus
8. Indicate the order in which the typical monthly menstrual cycle occurs by numbering the following 1 (first) to 4 (last).