Postpartum Assessment and Nursing Care
Objectives
2. Describe the postpartum period.
3. Explain the involution of the uterus, and describe changes in the fundal position.
4. Explain the cause of afterpains.
5. Distinguish between the characteristics of lochia rubra, lochia serosa, and lochia alba.
6. Explain how to assess the postpartum woman’s perineum.
7. Describe two ways in which the fluid accumulated during pregnancy is eliminated during the postpartum period.
8. Explain the importance of monitoring the vital signs during the first 24 hours postpartum.
9. List three factors that influence urinary retention after delivery.
10. Discuss three factors that contribute to postpartum constipation.
11. List two significant events that occur as a result of changes in the endocrine system.
12. Explain the factors involved in the woman’s weight loss after birth.
13. Interpret Rubin’s taking-in and taking-hold phases.
14. Explain the psychological alteration called postpartum blues.
15. Demonstrate three ways to prepare the sibling for the new family member.
16. Present two ways to encourage parent-newborn attachment.
17. Explain why early ambulation is encouraged.
18. Review the importance of Kegel (perineal tightening) exercises.
19. Describe five danger signs that the woman should report after discharge from the hospital.
Key Terms
diaphoresis (d -ă-fŏ-RĒ-ss, p. 231)
-ă-fŏ-RĒ-ss, p. 231)
diastasis recti (d -
- S-tā-ss RĔK-t, p. 230)
S-tā-ss RĔK-t, p. 230)
episiotomy (ĕ-pēz-ē-ŎT-ō-mē, p. 229)
exfoliation (ĕks-fō-lē-Ā-shŭn, p. 226)
involution (n-vō-LOO-shŭn, p. 226)
lochia alba (LŌ-kē-ă L-bă, p. 228)
lochia rubra (ROO-bră, p. 228)
lochia serosa (sĕr-Ō-să, p. 228)
puerperium (pū-ĕr-PĒ-rē-ŭm, p. 224)
subinvolution (sŭb-n-vō-LOO-shŭn, p. 227)
 http://evolve.elsevier.com/Leifer/maternity
http://evolve.elsevier.com/Leifer/maternity
The postpartum period, or puerperium, is the 6-week interval from childbirth to the return of the uterus and other organs to a prepregnant state. An arbitrary time frame divides the period into the immediate postpartum (first 24 hours), early postpartum (first week), and late postpartum (second to sixth weeks). Care during this time presents a challenge to nurses. With the short hospital stay, the time must be well planned to assist in maternal recovery, newborn care, family preparation, and intensive patient teaching. Many hospitals offer extended postpartum care by home visits, hospital outpatient clinic visits, and telephone communication to assist the woman and family during the postpartum recovery period (Clinical Pathway 12-1).
Goals of Postpartum Care
The main goals in postpartum care are to assist and support the woman’s recovery to the prepregnant state and identify deviations from the norm; educate the mother about her own self-care, newborn feeding, and newborn care; and promote bonding between the newborn and family. During the first 1 to 2 postpartum hours (i.e., the fourth stage of
Clinical Pathway 12-1
| Assessment | 1-8 Hours | 8-24 Hours | 24-48 Hours |
| Assessment | Assess q15 minute 1st hour; q30 minute 2nd hour then q4h: Fundus for firmness, level Lochia for color, amount, clots Bladder for voiding Perineum for sutures, bruising, hemorrhoids Breasts for softness, colostrum Vital signs (compare to baseline) Pain | Assess q4h: Fundus Breasts, nipples Newborn latch-on Colostrum Feeding technique for breast or bottle Vital signs (compare to baseline) Pain Homans’ sign Bonding Perineal healing Lochia | Assess: Breasts for softness, nipples, latch-on of newborn Feeding techniques and positioning Newborn care Hand hygiene Fundus q8h Perineal state Lochia Vital signs Family interaction |
| Teaching | Teach fundal massage, application of perineal pads, breastfeeding techniques. Discuss afterpains and pain management. Request assistance for first ambulation. Discuss orthostatic hypotension. | Explain cord care, bulb suctioning, circumcision care, newborn feeding techniques. Advise on maternal diet. Stress need for periods of rest. | Discuss: Maternal role Perineal care Newborn feeding Maternal diet Home setting and problems Support systems Plans to resume outside work Newborn care options Family planning Return of normal bowel function and the influence of medication on constipation |
| Medical and nursing interventions | Administer: Straight catheterization if unable to void Medications as ordered Stool softener if ordered Hep-Lock IV when taking oral fluids | Provide as needed: RhoGAM Hematocrit test Stool softener if no bowel movement Topical analgesics for sutures Medicine for pain Lactation nurse assistance | Provide shower and assistance with ambulation. Explain information and screening tests. Give return clinic appointments for mother and newborn. Assess bowel movements and diet. Provide discharge medication for pain, stool softener, lanolin for nipples. Provide community referral to WIC program if qualified. |
| Discharge and follow-up plan | Discuss understanding of postpartum care and newborn care. Identify support person and culturally specific needs. | Check that birth certificate is completed. Provide referral for birth records. Discuss home care. Discuss need for follow-up care for mother and newborn. Assess bonding. Discuss role of siblings and husband or partner. Administer immunizations if needed (e.g., Rubella). | Review discharge instructions for breast care, perineal care, family planning, newborn feeding, resumption of sexual activity, postpartum exercises, diet. Provide telephone resources. Review family and support system. Provide prescriptions as needed. Give appropriate gift pack and picture of newborn, as available. |
IV, intravenous; RhoGAM, Rho(D) immune globulin; WIC, Women, Infants, and Children.
labor), the woman is closely observed and assessed because it is a critical time to prevent the dangers of hemorrhage and hypovolemic shock. When her condition is stabilized, the woman may be moved to a postpartum unit.
To provide high-quality care, the nurse must be knowledgeable about the physical and emotional physiology of postpartum adaptation. After the initial dangers of hemorrhage and shock have passed, the primary postpartum danger is infection. The uterine cavity is easily accessible to microorganisms from the exterior. Also, the site where the placenta was attached is an open wound and can be easily infected.
The clinical pathway includes nursing assessments, teaching, medical and nursing interventions, discharge, and follow-up care for the postpartum woman. By indicating specific care and progress of the woman and newborn within a specified timeline that is related to a planned outcome, the nurse can clearly identify deviations from normal so they can be treated. The nurse documents the care and reports variation in progress during the postpartum period.

Confirm That the Patient Understands
To verify that the woman (or family) understands what the nurse has told her, have the woman repeat the teaching in her own words. A nod may indicate courtesy, not understanding, when the primary language and culture of the nurse and family are different.
Physiologic Changes and Nursing Interventions
Changes in the Reproductive System
Involution of the Uterus
Involution refers to the changes that the reproductive organs (particularly the uterus) undergo after birth of the newborn to return to the pre-pregnant size and condition. The process begins after the expulsion of the placenta with uterine muscle contractions. Immediately after birth, the placental site contracts to a size less than half its original diameter. During contractions, the uterine muscles act like living ligatures and compress the blood vessels, which control and reduce the amount of blood loss (Figure 12-1). A unique healing process, called exfoliation, enables the placental site to heal without scarring. In exfoliation, necrotic tissue is sloughed off of the superficial tissues, leaving a smooth surface of endometrial tissue. This unique reparative process ensures that future fertilized ova will implant in an unscarred uterus. Endometrial regeneration is completed within 16 days (Oats & Abraham, 2010), except for the placental site, where regeneration is not complete until 6 weeks postpartum.

The uterus undergoes a rapid reduction in size and weight. The uterus weighs approximately 1000 g (2.2 lb) immediately after birth. It decreases to 500 g (1.1 lb) during the first week and 340 g (12 oz) by 2 weeks postpartum. The rate of decrease varies with the size of the newborn and the number of previous pregnancies. The primary cause of involution is the sudden withdrawal of estrogen and progesterone, which triggers the release of proteolytic enzymes into the endometrium. This release causes the protein material within the endometrial cells to be broken down into substances that can be excreted in the urine. The number of muscle cells does not change during involution, but the size of each cell is markedly reduced.
Factors that can slow uterine involution include (1) prolonged labor, (2) incomplete expulsion of placenta and membranes, (3) anesthesia, (4) previous labors, and (5) a distended (full) bladder. Factors that can enhance involution include (1) uncomplicated labor and birth, (2) breastfeeding, and (3) early, frequent ambulation.
The cervix after birth is soft. By 18 hours, it has regained its form. The cervical os (dilated to 10 cm during labor) gradually closes within 2 weeks. The external os never regains its original appearance; after childbirth, it appears as a slit instead of a circle.
Descent of the Uterine Fundus
Fundal height is measured in centimeters (or fingerbreadths) in relation to the umbilicus (Skill 12-1). It is used to assess the rate of uterine involution. The usual progression of uterine descent into the pelvis is 1 cm (about one fingerbreadth) a day. After delivery (especially when an oxytocin drug is
 Skill 12-1
Skill 12-1
Assessing and Massaging the Uterine Fundus
Purpose
To prevent excessive postpartum bleeding.
Steps
1. Ask the woman to empty her bladder if she has not voided recently. (A full bladder contributes to uterine relaxation and subinvolution.)
2. Have the woman assume supine position with knees slightly flexed (relaxes abdominal muscles).
3. Apply a lower perineal pad, and observe lochia as fundus is palpated.
4. Determine uterine firmness. Cup one hand above the symphysis pubis to support the lower uterine segment; with the other hand, palpate abdomen until top of fundus is located. Determine whether firm (if not, massage lightly until firm).
5. Determine height of fundus. Measure height of top of fundus in fingerbreadths above, below, or at umbilicus.
6. Determine whether fundus is in midline (deviation typically indicates full bladder). Observe for firmness of fundus.
7. If the fundus is not firm, massage the fundus in a circular motion with the flat surface of the fingers of the dominant hand.
8. Document the consistency and location of fundus. Consistency is recorded as “fundus firm with massage” or “fundus boggy.” Record fundal height (e.g., U2 or U2 fingerbreadths below or above umbilicus).

administered after the expulsion of the placenta), the fundus of the uterus is firm and may be approximately at the level of the umbilicus or just below. Breastfeeding enhances involution because sucking stimulates the release of oxytocin from the posterior pituitary gland. The uterus is contracted to the size of a large grapefruit. By 10 days’ postpartum, it should not be abdominally palpable. A full (distended) bladder can push the uterus up and cause it to deviate to one side (usually the right side) and interfere with involution. If blood clots collect within the uterus, contractions stop, and the fundus of the uterus may rise and feel soft or boggy. This atony results in increased bleeding. Massage may be needed. A uterus deviating from the midline usually requires emptying of the bladder in order for involution to continue.

At 6 weeks after delivery, the uterus is approximately pre-pregnant size. Subinvolution is the failure of the uterus to return to the pre-pregnant state and is most commonly caused by retained placental fragments.
Afterpains
Intermittent uterine contractions, which represent relaxation and contraction of the muscle fibers, cause uterine cramping and are called afterpains. Afterpains occur for the first 2 or 3 days’ postpartum. The hormone oxytocin, released by the posterior pituitary gland, strengthens uterine contractions, compressing blood vessels and preventing excessive blood loss. If the mother breastfeeds, infant suckling stimulates oxytocin release. Therefore, the mother often notices the afterpains when she breastfeeds her newborn. Women who have had previous pregnancies often have stronger afterpains because the contraction of the uterine muscles is not sustained because of decreased muscle tone. Nonsteroidal antiinflammatory medications such as ibuprofen are more effective than acetaminophen or propoxyphene in relieving afterpains for most women (Gabbe, Niebyl, & Simpson, 2007). Ibuprofen is safe for nursing mothers (Gabbe, Niebyl, & Simpson, 2007).
Lochia
Lochia is postpartum vaginal discharge. It contains blood from the placental site, particles of necrotic decidua, and mucus. Lochia normally has a fleshy odor similar to that of menstrual flow. The quantity of lochia rapidly diminishes and becomes moderate and then scant. Lochia is the heaviest during the first 1 or 2 hours after birth. Initial lochia is bright red and commonly called lochia rubra (lasts 1 to 3 days); it may contain small clots. The vaginal flow then pales and becomes pink to brown after approximately 3 days; this is called lochia serosa. Lochia serosa should not contain clots and can last up to 27 days in some women (Gabbe, Niebyl, & Simpson, 2007). Typically, by 10 days’ postpartum, the vaginal discharge often becomes yellow to white and is called lochia alba. Lochia alba may continue, on average, to the sixth week postpartum (Table 12-1).
Table 12-1
Normal and Abnormal Characteristics of Lochia
| Lochia Type | Time | Normal Lochia | Abnormal Lochia |
| Lochia rubra | Days 1-3 | Bright red, bloody consistency; fleshy odor; temporary increase during breastfeeding and on rising | Numerous large clots; foul smell; saturation of perineal pad in 1 hour or less |
| Lochia serosa | Usually days 4-9 (can last to 27 days) | Pinkish brown; serosanguineous consistency | Foul smell; saturation of perineal pad in 1 hour or less |
| Lochia alba | Day 10 to approximately sixth week | Creamy white; fleshy odor | Foul smell; persistent lochial discharge over 3 weeks; return to pink or red discharge |

Estimating the amount of lochial flow by observation is difficult. Many facilities use perineal pads that have cold or warm packs in them. These pads absorb less lochia, which must be considered when estimating the amount of blood loss. If a mother has excessive lochia, a clean pad should be applied and checked within 15 minutes. The number of perineal pads applied during a given period should be counted or the pads weighed to help determine the amount of vaginal discharge. One gram of weight equals 1 mL of blood. In addition, the woman’s fundus should be checked for firmness. Nurses often estimate the amount of lochia in terms of the approximate size of the area soiled in 1 hour (Skill 12-2).
The amount of lochia is less after a cesarean birth. Breastfeeding or the use of oral contraceptives does not affect lochial flow. Lochia is briefly heavier when the mother ambulates because blood that has pooled in her vagina is discharged when she assumes an upright position. The gush of blood can be anxiety provoking to the woman and should not be confused with a postpartum hemorrhage. Excessive lochia rubra early in the postpartum period may suggest bleeding as a result of retained fragments of the placenta or membranes. Recurrence of bleeding in 7 to 10 days after birth suggests bleeding from the placenta site but may be the result of normal sloughing (Gabbe, Niebyl, & Simpson, 2007). After 3 to 4 weeks, late bleeding may also be caused by infection or subinvolution. Continued lochia serosa or alba suggests infection (endometritis) and is often accompanied by fever, pain, or abdominal tenderness and an offensive, foul odor to the lochia. Any abnormal lochia pattern should be documented and reported. Ultrasound is one of the diagnostic methods that can be used to confirm the cause of postpartum bleeding.
Assessment of uterine firmness, location, and position in relation to the midline (see Skill 12-1) is performed at routine intervals. A poorly contracted (soft, boggy) uterus should be massaged until firm to prevent hemorrhage. It is essential not to push down on an uncontracted uterus to avoid inverting it.
Vagina
The vagina usually appears edematous and bruised, and the opening in the vagina often gapes when intraabdominal pressure is increased, such as by
Skill 12-2
Purpose
To determine normal progress of the postpartum period.
Steps
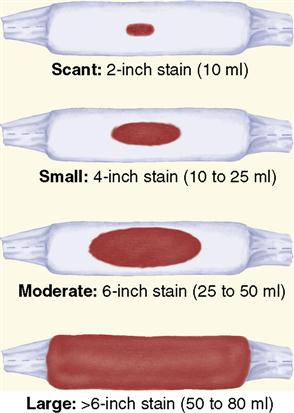
1. Assess lochia for quantity. A guideline to estimate and document the amount of flow on the menstrual pad in 1 hour is as follows (see illustration):
a. Scant: less than a 2-inch (5-cm) stain
b. Light: less than a 4-inch (10-cm) stain
c. Moderate: less than a 6-inch (15-cm) stain
d. Large or heavy: larger than a 6-inch stain or one pad saturated within 2 hours
e. Excessive: saturation of a perineal pad within 15 minutes
2. Assess lochia for type and characteristics. In first 3 days, normal lochia has fleshy odor with small clots with red or reddish brown color. Abnormal lochia has foul odor, large clots, and saturated pad with bright red color.
coughing. By the third postpartum week, the vagina resumes the appearance of the pre-pregnant state, with some relaxation of tissue. The rugae, or vaginal folds, disappear during pregnancy, and the walls of the vagina become smooth. The rugae reappear within 3 weeks postpartum. Within 6 weeks, the vagina has almost regained its pre-pregnancy form. Breastfeeding mothers, in particular, may have vaginal dryness and discomfort during sexual intercourse. A water-soluble vaginal lubricant such as K-Y Jelly makes intercourse more comfortable. Dryness usually disappears when ovulation and menstruation return.
Perineum
The perineum has been stretched and thinned to accommodate the size of the newborn. The pelvic floor muscles are overstretched and weak. The appearance of the perineum varies greatly, depending on the type and extent of the laceration(s) or episiotomy (cut in the perineum). The soft tissues of the perineum are often edematous and bruised.
The nurse puts on clean gloves before assessing the perineum to prevent contact with vaginal blood flow. The perineum is assessed for the type and amount of vaginal discharge, unusual swelling, discoloration, healing of the tissues, and discomfort (Skill 12-3). If an episiotomy was performed, the state of healing is assessed by the REEDA scale, a mnemonic for Redness, Edema, Ecchymosis (bruising), Discharge, and Approximation of the wound. Foul odor accompanied by drainage indicates infection; further examination of the incision and area of warmth and tenderness should be performed. Hemorrhoids, if present, are assessed for size, number, and discomfort. During the assessment, the nurse asks the woman about relief obtained from comfort measures (sitz bath, warm or cold applications, and medications). The nurse should record his or her findings.
Studies have shown a positive response to cold sitz baths (Gabbe, Niebyl, & Simpson, 2007). Occasionally, the cause of perineal pain is prolapsed hemorrhoids. Witch-hazel pads, astringent pads, suppositories, or local anesthetic sprays are helpful. Healing usually takes place within 6 weeks. Daily perineal care is described in Skill 12-4.
Changes in the Musculoskeletal System
Muscles and Joints
During the first few days, levels of the hormone relaxin decrease and ligaments and cartilage of the pelvis begin to return to the pre-pregnancy state. With the delivery of the placenta, the effect of progesterone on muscle tone is removed. Therefore, muscle tone begins to be restored throughout the body. In particular, the
Skill 12-3
Purpose
To observe perineal trauma, hemorrhoids, and status of healing.
Steps
1. Ask the mother to turn on side and flex upper leg, lower perineal pad, and lift up upper buttock; if necessary, use flashlight to inspect perineum.
2. Observe for edema, bruising, and hematoma.
3. Examine episiotomy or laceration for REEDA (Redness, Edema, Ecchymosis, Discharge, and Approximation).
4. Observe hemorrhoids for extent of edema (can interfere with bowel elimination).
6. Dispose of soiled contents in appropriate waste container and wash hands.
Skill 12-4
Purpose
To promote healing and prevent infection.
Steps
1. Gather supplies needed, such as bottle with warm water, peripad, and prescribed ointments.
2. Help the woman to bathroom.
3. Instruct the woman to wash her hands before and after perineal care.
4. Remove soiled pad from front to back; discard in waste container.
5. Squeeze peri bottle or pour warm water or cleansing solution over perineum without opening labia.
6. Pat dry with tissue. Use each tissue one time; pat from front to back, then discard tissue.
7. Apply medicated spray, ointment, or pad, as directed. Do not apply perineal pad for 1 to 2 minutes (otherwise, medication will be absorbed in pad).
8. Apply clean perineal pad from front to back, touching only sides and outside of pad to lessen risk of infection.
9. Do not flush toilet until the woman is standing upright; otherwise, the flushing water can spray on perineum.
10. Always perform perineal care after each voiding or stool, or at least every 4 hours during puerperium.
11. Report clots, increase in lochia flow, or excessive abdominal cramping.
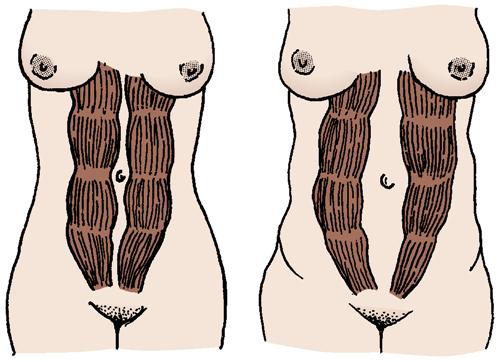
tone in the rectus abdominis muscles and the pubococcygeal muscle is restored. The abdominal muscles, including the rectus abdominis muscles, may be separated, and diastasis recti can occur (Figure 12-2). Special exercises can strengthen the abdominal wall. Women need to be advised that with proper diet, exercise, and rest, the abdominal muscle tone is usually regained more rapidly. Good body mechanics and correct posture are important to help relieve low back pain. Kegel exercises help the pubococcygeal muscle (muscle that aids bowel and bladder control) to regain normal function (see Chapter 5).
A generalized decrease in bone mineralization occurs after birth. This bone loss is not affected by calcium intake or exercise but returns to normal within 18 months (Gabbe, Niebyl, & Simpson, 2007).
Lower Extremities
Venous stasis, particularly during the later part of pregnancy, contributes to the risk of blood clots (thrombosis) forming in the lower extremities. By passively dorsiflexing the woman’s feet, the nurse determines whether there is pain in the calf (a positive Homans’ sign) (Figure 12-3). This may be an early sign of venous thrombosis and should be reported. In addition, the nurse inspects the legs for redness, swelling, and warmth.

Changes in the Cardiovascular System
Dramatic changes to the maternal cardiovascular system occur in the postpartum period. During pregnancy, an approximately 50% increase in circulating blood volume occurs (hypervolemia), which allows the woman to tolerate considerable blood loss at birth without adverse effects. Many women lose at least 200 to 500 mL of blood during vaginal births and approximately twice as much during cesarean births. Readjustments in the maternal vasculature after childbirth are rapid. During postpartum adaptation, dramatic and immediate changes take place in the circulating blood volume that prevent hypovolemia from normal blood loss during delivery. These changes include (1) elimination of the placenta, which diverts 500 to 750 mL of blood flow into the maternal systemic circulation; (2) rapid reduction of the size of the uterus, which puts more blood in the systemic circulation; (3) increase of blood flow to the vena cava from elimination of compression by the gravid uterus; and (4) mobilization of body fluids accumulated during pregnancy. Cardiac output may remain increased for 1 year or more (Gabbe, Niebyl, & Simpson, 2007). A healthy woman’s body can make these changes, but a woman with a heart disorder can encounter problems.
Excess blood volume, which is necessary during pregnancy, is removed to help the woman’s body return to the pre-pregnant state. This excess is disposed of in two ways: (1) diuresis (increased excretion of urine), in which a daily urinary output can be as much as 3000 mL; and (2) diaphoresis (profuse perspiration).
Blood Values
During the first 72 hours after childbirth, the loss in plasma volume is greater than that in the number of red blood cells (RBCs). This results in a temporary rise in the hematocrit and hemoglobin levels. Any excess will gradually disappear in accordance with the RBC life span. The normal levels are achieved within 2 to 4 weeks’ postpartum. The excess body fluids are excreted by the kidneys, which cause a marked increase in daily urinary output. Leukocytosis, an increase in the white blood cell count to 15,000/mm3 or more, occurs immediately after birth in women without infection; the levels return to normal within 10 days.
Blood Coagulation
Blood clotting factors that increased during pregnancy tend to remain elevated during the initial postpartum period. Fibrinogen levels may return to normal within 2 weeks of delivery. This fact, along with trauma, immobility, and infection, predisposes the woman to the development of a thromboembolism (one of the leading causes of maternal death is an embolus or thrombus). To decrease this risk, early and frequent ambulation is essential. Dyspnea (difficulty breathing) and tachypnea (rapid breathing) are hallmark signs of pulmonary embolus and require immediate medical intervention.
Varicose veins that have developed during pregnancy usually diminish during the puerperium because the venous stasis that was caused by the gravid uterine compression (pressure of the uterus on pelvic blood vessels) decreases. In addition, progesterone level is decreased, which during pregnancy is largely responsible for a decrease in smooth muscle tone.
Orthostatic Hypotension
Resistance to the blood flow in the vessels of the pelvis decreases after birth. As a result, the woman’s blood pressure falls when she sits upright or stands, and she may complain of feeling dizzy, lightheaded, or faint. Guidance and assistance are needed during early ambulation to prevent injury.
Postpartum Diaphoresis
Diaphoresis (perspiration) is the elimination of excess fluid through the skin. It is the body’s way of getting rid of excess fluid accumulated during pregnancy. Profuse diaphoresis (excessive sweating) often occurs at night. This adjustment has implications for nursing care. Showers, frequent changes of clothing, and adequate fluid intake are important for the woman’s comfort.
Vital Signs
Temperature
The woman’s temperature during the first 24 hours after delivery may rise to 38° C (100.4° F) as a result of the dehydration and exertion of labor. After the first 24 hours, the woman should be afebrile, and any temperature greater than 38° C suggests infection. An elevated temperature that persists longer than 24 hours or that exceeds 38° C should be reported to the physician or nurse-midwife. A short-term elevation on the second or third postpartum day can occur as a result of breast engorgement.
Pulse
The heart rate often decreases to a rate of 50 to 60 beats/min (bradycardia, or slow pulse) for the first 6 to 8 days’ postpartum. An elevated heart rate may indicate undue blood loss, infection, pain, anxiety, or cardiac disease.
Blood Pressure
Blood pressure readings should remain stable after birth. A decrease in blood pressure may be related to excessive blood loss. Blood pressure elevation—especially when accompanied by a headache—suggests gestational hypertension and indicates the need for further evaluation (see Chapter 13).
Changes in the Urinary System
The bladder of the postpartum woman has increased in capacity and has lost some of its muscle tone. In addition, during the birth, the urethra, bladder, and tissue around the urinary meatus may become edematous and traumatized. Urination is also impeded by anesthetic drugs. The diminished awareness of the need to urinate may result in decreased sensitivity to fluid pressure, and the woman may not feel an urge to void. This is important to remember because the bladder fills rapidly as a result of intravenous fluids administered during labor and after birth. With bladder distention, the uterus is displaced (often over to one side, usually the right) and has a reduced ability to contract. When the uterus fails to contract, blood vessels are free to bleed. Therefore, it is important that the nurse monitor the woman for voiding. The urinary output in the early postpartum period can be great (diuresis). Tenderness over the costovertebral angle, fever, urinary retention, and dysuria with urinary frequency signify potential urinary infection, and further evaluation is necessary. Glomerular filtration may remain elevated for up to 8 weeks postpartum.

Mild proteinuria may occur as a result of the breakdown of uterine cells. The urine may also test positive for acetone or ketones from dehydration during a prolonged labor. Lactosuria may occur in breastfeeding women as a result of the lactation process. Normal status returns by 4 weeks’ postpartum. The following measures may help a woman urinate:
Changes in the Gastrointestinal System
The woman is frequently hungry and thirsty after the birth of her newborn because of energy expended and the long period of fluid or food restriction during labor. The woman is typically offered solid food after she has shown she can tolerate liquids. Constipation may occur during the postpartum period for the following reasons: (1) decreased peristalsis caused by the lingering relaxing effects of progesterone; (2) stretched abdominal muscles, making it more difficult to bear down to expel the stool; (3) limited food and fluid intake; (4) soreness and swelling of the perineum and hemorrhoids; and (5) fear of pain. If an episiotomy were performed, a stool softener such as Docusate sodium or a gentle laxative such as MiraLAX would be prescribed to avoid the discomfort of straining. A bowel movement is expected within 3 days after delivery.
Nutrition is important for the woman’s gastrointestinal tract to function properly. The woman should be encouraged to eat three well-balanced meals and maintain adequate calcium and phosphorus intake if she is breastfeeding. A high-fluid and high-fiber intake is recommended to reduce constipation. While breastfeeding, she is advised to increase her caloric intake by 500 calories per day above the pre-pregnancy requirements. In addition, she is encouraged to increase her daily fluid intake to increase her milk supply.
The hospital’s dietitian is consulted to manage cultural aspects of postpartum nutrition. Laboratory values are often determined at the 2- or 6-week postpartum examination to detect whether anemia has persisted or developed.
Changes in the Nervous System
Neurologic changes during the postpartum period result from a reversal of maternal adaptations to pregnancy and trauma from the birth process.
Elimination of physiologic edema through diuresis that follows childbirth relieves carpal tunnel syndrome by easing the compression on the median nerves in the wrists. Headaches require careful assessment because gestational hypertension can continue to cause headaches in the postpartum period.
Changes in the Integumentary System
During pregnancy, many skin changes occur as a result of an increase in hormones. After childbirth, the skin gradually reverts to the pre-pregnancy state. The melanocyte-stimulating hormone (MSH) levels, which cause hyperpigmentation during pregnancy, decrease rapidly after childbirth. This is particularly noticeable when the mask of pregnancy (chloasma) and linea nigra disappear. Also, spider nevi and palmar erythema that develop as the result of increased estrogen levels gradually disappear. Striae gravidarum (stretch marks), which develop on the abdomen, thighs, and breasts, gradually fade to become less noticeable silvery lines but do not disappear completely. Hair growth slows, and some hair loss may be experienced in the first months after delivery, but it typically returns to normal without intervention.
Changes in the Endocrine System
After the expulsion of the placenta, estrogen and progesterone levels decrease. If the mother is bottle feeding, estrogen levels begin to rise to follicular levels approximately 3 weeks after delivery, which allow the return of menses. Often the first menses is anovulatory. Return to pre-pregnancy levels of estrogen and progesterone is slower in breastfeeding women. Lactation is initiated as levels of prolactin increase, and, with increased breastfeeding, the prolactin level rises further. In nonlactating women, the prolactin level declines and reaches the pre-pregnancy level by 14 days’ postpartum. The dramatic change (drastic drop in hormones) in the endocrine system allows two significant events to occur: lactation (milk secretion) begins with the newborn suckling, and the menstrual cycle function returns.
Lactation (the secretion of milk) is the end result of many interacting factors (see Chapter 11). After delivery, estrogen, progesterone, and human placental lactogen (hPL) (all prolactin-inhibiting agents) decrease rapidly, causing a brisk increase in prolactin secretion. Once lactation has been established, suckling is the most important stimulus for the maintenance of milk production and ejection. Prolactin, secreted by the anterior pituitary gland, promotes milk production by stimulating the alveolar cells of the breast, and oxytocin, secreted by the posterior pituitary, triggers the ejection of milk as the newborn sucks. Oxytocin also stimulates uterine contractions (afterpains) felt by the mother.
By the third day after delivery, the prolactin effect on the breast tissue is evident, and the hormone is present in sufficient quantity to cause breast engorgement. The breasts become distended, firm, tender, and warm. At this time, milk, which is thin and bluish, begins to replace the colostrum (premilk).
If the woman does not wish to breastfeed her newborn, she should avoid any breast stimulation, including newborn suckling, pumping the breasts, or allowing warm water to flow on the breasts during showers. Prolactin levels drop rapidly. Palpation of the breast on the second or third day will likely reveal engorgement. The breasts become distended (swollen), firm, tender, and warm to touch (due to vasocongestion). Breast engorgement is primarily caused by the temporary congestion of veins and lymphatics rather than by an accumulation of milk. Engorgement spontaneously resolves, and discomfort usually decreases within 24 to 36 hours. A snug, supportive bra worn for 72 hours, ice packs, and mild analgesics may be used to relieve breast discomfort. If suckling has never begun and nipple stimulation is avoided, lactation ceases within a few days to a week. Breastfeeding is discussed in detail in Chapter 11.
Resumption of Ovulation and Menstruation
Most nonlactating mothers resume menstruation within 3 months after childbirth. Breastfeeding delays the return of ovulation and menstruation. Ovulation may return within 1 month in nonlactating women and up to 6 months in lactating women. Many lactating women resume menstruation within 6 months, although some do not menstruate as long as they nurse their newborns at least 10 to 12 times in a 24-hour period. The first menstrual flow is often greater than normal for both nursing and non-nursing mothers. The woman should be advised that it is possible to ovulate and become pregnant before her menstrual periods are established. In other words, breastfeeding is not an effective contraception method. The woman should be encouraged to discuss family planning with her health care provider.
Weight Loss
Immediately after delivery, the woman’s weight decreases by approximately 4.5 to 5.8 kg (10 to 13 lbs). This weight loss is accounted for by the removal of the fetus, placenta, and amniotic fluid. An additional 2.3 to 3.6 kg (5 to 8 lbs) are lost during the early postpartum period as a result of diuresis and diaphoresis. An additional 0.9 to 1.4 kg (2 to 3 lbs) is lost via lochia and involution in the first week postpartum (Blackburn, 2007).
During pregnancy, the woman’s body stores 2.3 to 3.2 kg (5 to 7 lbs) of fat for lactation needs. The breastfeeding mother gradually uses this fat store over the first 6 months, and she often returns to her approximate pre-pregnancy weight. Some women tend to retain some of the excess weight gained during pregnancy. Therefore, women are encouraged to perform postpartum exercises to lose the excess weight gained during pregnancy and to increase the strength and tone of various muscles in their bodies. Aerobic exercise has no adverse effects on breastfeeding (Gabbe, Niebyl, & Simpson, 2007).
Psychological Changes and Nursing Interventions
Mood swings are common during the postpartum period. The rapid decline of hormones such as progesterone and estrogen is believed to contribute to the emotional upset. Other factors related to emotional reactions are conflict about the maternal role and personal insecurity. Women who have economic or family problems usually demonstrate more stress in response to motherhood. In addition, past fetal losses or pregnancy failures contribute to postpartum emotional problems. Physical discomforts such as a painful perineum, afterpains, breast engorgement, and fatigue all contribute to negative postpartum reactions and should be promptly managed to promote comfort in the postpartum phase.
Phases of Maternal Adaptation
Maternal adaptation has been described by Rubin (1984) as a series of three phases (Box 12-1). The taking-in phase begins immediately after birth and lasts for a few hours to approximately 2 days’ postpartum. This phase is characterized by passive, dependent behavior. The woman focuses on her own needs and is concerned about the overall health of her newborn. The mother often repeatedly reviews her labor and birth experience.
The taking-hold phase is the second maternal phase, when the woman is ready to assert her independence. She becomes the initiator and is ready to participate independently in newborn care. She often becomes exhausted in her new role and verbalizes anxiety about it.
The third stage is the letting-go phase. In this stage, the woman assumes her position in the home and her new maternal role. Sometimes, demands placed on her may lead to feelings of mild depression ).
Attainment of the Maternal Role
Maternal role attainment is the process by which the woman learns mothering behaviors and becomes comfortable with her identity as a mother. As the bond between the newborn and mother forms, the mother and newborn grow to know each other.
Maternal role attainment occurs in four stages. These four stages correspond to those identified by Rubin (1984). In the anticipatory stage, which occurs during pregnancy, the woman looks to role models of how to be a mother. In the formal stage, which begins when the newborn is born, the mother is still influenced by the guidance of others. The informal stage begins when the mother starts to make her own choices about mothering, and she begins to find her own style. In the personal stage, the mother does what she is comfortable with in the role of mother. This stage occurs from 3 to 10 months after delivery. Social support, the mother’s age, her personality traits, and her socioeconomic status all influence her success in assuming the mothering role.
The transition to motherhood is a complex behavioral process. Today’s new mothers tend to be less dependent and are better able to assume the self-care responsibilities because of factors such as the reduced amount of medications received during labor, early ambulation, rooming-in, and increased support from the father, significant other, or family.
Parents who are ill-prepared for the changes in relationships, lifestyle, and roles associated with the integration of the newborn in the family have more difficulty making the necessary transition. The woman’s immaturity, minimum exposure of the mother to the baby in the days after birth, lack of a support system, or ill health also can interfere with maternal role attainment.
Postpartum Blues
Postpartum blues occur in approximately 70% of women during the first few days after birth and generally last up to 10 days. This state is characterized by tearfulness, insomnia, lack of appetite, and a feeling of being disappointed. Psychological adjustments and hormonal factors are thought to contribute, and discomfort, anxiety, anger, and fatigue seem to play a part. There is no obstetric, social, personality, or economic factor that predisposes a woman to developing postpartum blues. It is possible that altered function of central neurotransmitters and hypothalamic-pituitary-thyroid interaction may be involved. However, rapid role changes and new responsibilities play a major role (Gabbe, Niebyl, & Simpson, 2007). Rest, empathy, and supportive care are the primary management strategies (Table 12-2). Teaching relaxation techniques, increasing confidence in self-care and newborn care, and promoting communication between the woman and her partner are essential nursing responsibilities. Postpartum support groups may be available in the community. Postpartum depression is discussed in Chapter 17.
Table 12-2
How to Develop an Individualized Postpartum Blues and Depression Care Map
| Findings | Interventions |
| Physiologic Factors | |
| Hormonal changes (T) | Teach that hormonal changes can result in negative feelings. |
| Fatigue from long labor and newborn feeding schedule (I) | Provide rest periods; use nursery at night and as needed. |
| Alteration in comfort (I) | Provide comfort measures: analgesics, positioning, ice packs, etc. |
| Vital signs within normal limits (A) Moderate lochia rubra with firm fundus at umbilicus at midline (A) Voiding without difficulty (A) |
|
| Breastfeeding ineffective because of poor latch-on (I, T) | Teach proper breastfeeding techniques, assist with breastfeeding as needed, and refer to lactation consultant. |
| Individual Sociocultural Factors | |
| No extended family close by (I) Decreased social support because of recent relocation (I) Supportive husband or partner Economically stable |
Encourage frequent contact with family by phone and e-mail. Provide information on community programs, parenting classes, and support groups. |
| Individual Spiritual Factors | |
| States “If I had faith in God, I wouldn’t feel this way” (I) | Make a referral to have hospital chaplain visit. |
| States she believes in God but feels disconnected from fellow believers because of not deciding on a church to join since move (I) | Provide a list of local places of worship. |
| Nursing Diagnosis: Ineffective individual coping related to effects of postpartum blues or depression | |
| Developmental Factors | |
| Assuming new role of mother (I) | Encourage positive bonding behaviors through teaching and positive reinforcement |
| Identifying newborn as separate being (I) | Demonstrate normal newborn care. Encourage patient to verbalize feelings and concerns regarding new role. Encourage patient to ask questions. Let patient know that bonding occurs over time and may not be immediate. Encourage active participation in caring for newborn and provide positive reinforcement |
| Individual Psychological Factors | |
| Expressing feelings of being “down” (A) Frequent crying (A) |
At each contact, determine and document mood (facial expressions, actions, verbal statements). |
| Verbalizes guilt about not being “happy” (A) | Encourage patient to share feelings regarding parenting role and newborn by using active listening techniques. |
| Flat affect (A) | Encourage patient to describe how she is feeling and how long she has had these feelings to rule out long-term depression that may need more immediate and more intense interventions.* If symptoms of depression are present, report to charge nurse or physician. |
| Withdrawn (A, T, I) | Encourage patient to share concerns, correct any misconceptions, and provide interventions needed to alleviate said concerns. |
| Expresses feelings of inadequacy (A, I) | Teach patient that new mothers often have feelings of inadequacy when adapting to new role. |
| Methodically cares for newborn without signs of positive bonding behaviors (A, I) | At each contact, assess and document bonding behaviors. |
| Anxiety from ineffective breastfeeding and feelings of not being able to care for newborn (A, T, I) | Teach patient that postpartum blues affects up to 80% of new mothers. Teach patient that postpartum blues is a self-limiting condition and should resolve within 2 weeks. Teach patient that if postpartum blues lasts longer than 2 weeks or if she has feelings of wanting to harm herself or others, she should contact her physician immediately.* Explore coping mechanisms that have been helpful to the patient in the past, and encourage her to use these. Explain what postpartum blues is to husband or partner and ways to be supportive during this time. Teach signs and symptoms of depression. Refer to support group or obtain social service consult. |
*Long-term depression and postpartum depression may require psychotherapy, antidepressants, or inpatient psychological treatment.
Providing support, anticipatory guidance, and reassurance that her feelings are experienced by many mothers is helpful. If the woman continues to feel depressed or has intense mood swings, further evaluation by the health care provider is necessary.
Care Management After Delivery
Nursing assessment during the first 1- to 2-hour recovery period requires close monitoring every 15 minutes for vital signs (blood pressure, pulse, and respirations), fundal location and consistency, and amount of bleeding. If the woman’s status is stable, these assessments are made less frequently, usually every 30 minutes for 1 hour and then hourly for at least 2 hours. The infant may be put to the breast, and the initial parent-infant bonding process begins. After the initial 1- to 2-hour assessments, the woman who is going to the traditional postpartum unit is transferred by wheelchair or gurney to her room. In hospitals that have a labor, delivery, recovery, and postpartum (LDRP) unit, the woman remains in the same room for the entire experience. With dyad or couplet care (the nurse cares for mother and newborn), the report is given to that nurse. In the traditional setting, an applicable report is given to a nursery nurse and a postpartum nurse. A physical assessment, including the measurement of vital signs, is performed on admission to the postpartum unit. Also at this time, the woman’s knowledge level about self-care and newborn care is determined.
The care plan incorporates nursing strategies to assist the mother and family in learning about self-care and care of the newborn. The family and siblings can visit the mother and newborn while in the facility. The basics of postpartum care (e.g., perineal care) are explained. The mother is encouraged to ask questions about her and the baby’s care. Nursing efforts during postpartum are directed toward the parents’ knowledge, expectations, anticipatory guidance, and teaching. Discharge planning is begun by using every contact with the mother to fulfill the teaching and learning goals.
The routine physical assessment focuses on the woman’s general appearance, breasts, reproductive tract, bladder and bowel elimination, and any specific physical or psychological problems.
Cultural Considerations
The nurse needs to explore cultural differences and practices concerning postpartum recovery. Cultural rituals, taboos, and traditions need to be respected. It is not uncommon for the woman to receive special foods and herbs that are believed to promote recovery. For some women, the time after childbirth (postpartum period) is a special time when others attend to their needs. For example, some groups of women from China and Southeast Asia view the first month after birth as a period for relative confinement and rest. Female family members perform the household duties and participate in the newborn’s care. Rooming-in after birth may not be compatible with some cultural beliefs. In contrast, in the American culture, women often perform light tasks soon after their discharge from the hospital.
One of the most common non-Western beliefs is the humoral theory of maintaining a balance between hot and cold. Because blood is considered “hot,” loss of blood during labor and delivery leaves the woman in a “cold” state, thus requiring “warm” items to restore balance, such as hot baths and warm water. In even the hottest weather, drinking ice water and staying in an air-conditioned room are rejected after birth by some cultures. In other cultures, such as Mexican American, bathing and hair washing are contraindicated for 40 days after delivery. Therefore, the new mother may refuse to shower the day after giving birth. This 40-day period corresponds somewhat to the modified activity recommended in traditional Western medicine. Non-Western health care practices may also have rituals related to the disposal of the umbilical cord and placenta.
Birth control practices vary among cultures and must be considered when discussing family planning. The nurse must be sensitive to the various practices and recognize that some women may feel distressed when they are told to ambulate early and participate in newborn and self-care activities. The nurse should incorporate cultural practices of the patient in the care plan (Nursing Care Plan 12-1).
 Nursing Care Plan 12-1
Nursing Care Plan 12-1
Cultural Considerations for Postpartum Care
Scenario
A mother is 1 day postpartum. She does not speak English well and appears anxious. When encouraged by the nurse to ambulate and shower, the woman cries.
Selected Nursing Diagnosis
Decisional conflict related to desire to please health care workers and desire to engage in cultural rituals and practice
| Expected Outcomes | Nursing Interventions | Rationales |
| Patient will participate with nurse in developing a culturally congruent individualized plan for obstetric care. | Assess cultural rituals and practices that are important to the patient by interview, with an interpreter if necessary or with a birth plan questionnaire. | Information obtained aids in the development of a culturally congruent individualized care plan. |
| Provide a warm, friendly environment. | Relieves anxiety and conveys a message of acceptance. | |
| Patient will freely verbalize her desires when asked to participate in culturally incongruent practices. | Explain to patient that she has the right to verbalize any disagreement with the way care is being delivered and to request that the care include culturally specific rituals and practices. | Patient and support persons are more likely to disagree and make requests when they are informed it is acceptable to do so. |
| Allow patient to engage in cultural rituals or practices whenever it is medically safe to do so. | Allowing patient to engage in activities can be comforting and can enhance coping abilities. | |
| Patient will express satisfaction with the care received during her hospitalization. | Whenever possible, provide choices to patient (e.g., “Would you like to take a shower now or would you prefer to wait?”). | Allows patient to choose culturally acceptable ways of doing things without feeling like she is being disrespectful to health care providers. |

Selected Nursing Diagnosis
Impaired verbal communication related to effects of language barrier
| Expected Outcomes | Nursing Interventions | Rationales |
| Patient and support persons will have all essential information communicated to them in a manner they can understand. | Whenever possible, assign a nurse who speaks the same language as the patient. | Allows direct communication between nurse and patient. |
| Obtain an interpreter or use a support person. If patient feels uncomfortable answering questions when using an interpreter who knows her, provide a hospital interpreter and inform the patient that all information will be kept confidential. | Ensures that correct information is obtained and conveyed. | |
| Ask permission to use the support person or family member to interpret. Inform patient that she has the right to refuse to answer any question when she does not want the interpreter to know the answer. | Patients have a right to privacy regarding health care matters, so they need to give permission for information to be shared with someone they know. Persons in some cultures believe they must answer all questions to maintain respect, so they need to be told it is acceptable to keep information confidential. | |
| Ask permission before using children to interpret and use only if another interpreter is not available. | In some cultures, it is not acceptable for children to know more than their parents. | |
| Obtain hospital interpreters as needed (preferably a woman); inform patient that all information will remain confidential. | When patients feel uncomfortable discussing health care information with support persons, or when support persons do not speak the dominant language, a hospital interpreter is needed to translate information. Most women prefer to discuss intimate matters with other women. | |
| In the absence of an interpreter, provide a questionnaire in the patient’s native language to be given on admission that includes essential assessment information that can be answered with numbers, yes/no answers, or multiple choice answers. | This can be compared with an identical questionnaire that is written in English and the dominant language of the patient to provide important assessment data that can be charted in English on the medical record. | |
| Patient and support person will have all of their questions answered. | Assess for patient’s and support person’s nonverbal signs of needs or concerns. | Facial expressions or tone of voice used as the patient and support person interact can be clues that they have questions or concerns. |
| Write down or memorize short yes/no questions and simple commands you can use to communicate with the patient and support person. | Allows for quick assessments to be made in the absence of an interpreter. It is important to remember that some patients may respond “yes” even when they do not understand the question; therefore, it is important to look for congruence between the verbal response and nonverbal responses or behaviors. | |
| Health care providers will become aware of all needs of patient and support person as they arise. | Assess ability to read and provide literature to patient in her native language if appropriate. | If patient can read written information, it can be an effective way of communicating when verbal communication is impaired. |
| Use pictures, diagrams, or body signals to communicate. | Can be an effective way to convey information or directions in the absence of an interpreter. |

Selected Nursing Diagnosis
Fear related to unfamiliarity of the dominant culture’s environment and childbirth practices
| Expected Outcomes | Nursing Interventions | Rationales |
| Patient will freely express her feelings and concerns. | Orient patient to the environment, equipment, procedures, routines, and anticipatory guidance of what she can expect. Use interpreter as needed. | Knowledge reduces fears and can clear up misconceptions that may be contributing to fear. |
| Patient will verbalize and use coping strategies to alleviate fears. | Use events to identify or estimate when things will occur (e.g., before sunset, after lunch). | Many cultures rely on events rather than a clock to determine time. When patients can anticipate approximate time frames, fear and anxiety can be reduced. |
| Encourage family members to visit and stay with patient. | Provides support to the patient. | |
| Patient will state she is less afraid. | Encourage patient to express fears and concerns. | Provides the opportunity to correct misconceptions or misunderstandings. |
| Expected Outcomes | Nursing Interventions | Rationales |
| Assess childbirth and newborn cultural practices and rituals that are important to patient. Unless these practices are contraindicated or unsafe, allow patient to participate in those that are important to her. | Provides insight into cultural belief system, which can be used to individualize a care plan. Participating in cultural practices can provide feelings of security, which help alleviate fear. | |
| Maintain a nonjudgmental attitude toward cultural practices that are safe to implement. | Conveys feelings of acceptance and decreases patient’s fears of not acting in expected manner. | |
| Provide scientific rationale for practices that are contraindicated or unsafe. | Knowledge allows patients to make informed decisions about adopting safer practices. | |
| Develop mutually acceptable compromises when cultural practices are contraindicated or unsafe. | Can increase compliance with adopting safer practices. | |
| Patient will have relaxed facial expressions. | Provide patient and support person with frequent encouragement. | Increases patient’s feelings of well-being and self-worth. |

Critical Thinking Questions
1. A mother tells you that she refused to give her newborn to the technician, who wanted to bring the infant to the nursery for routine screening tests, because the technician was not wearing a name badge. How should you respond?
2. You are assigned to care for a woman who gave birth yesterday. She refuses to get out of bed or take a shower. How should you respond?
Postpartum Check
The postpartum check, which can be remembered by the mnemonic BUBBLE-HE, includes assessment of the Breasts, Uterus, Bladder, Bowel, Lochia, Episiotomy (perineum), Homans’ sign, and Emotions (psyche) (Table 12-3). The Homans’ sign checks for the development of blood clots in the lower extremities. The emotional status includes bonding between parents and infant.
Table 12-3
| Assessment | Recording |
| Breasts and nipples | Signs of engorgement, tenderness, lactation |
| Uterus | Fundal height, location, and consistency |
| Bladder | Output amount, frequency, and discomfort |
| Bowel | If or when patient had bowel movement |
| Lochia | Amount, color, presence of clots, and odor |
| Episiotomy | Edema, hematoma, signs of episiotomy or laceration healing, or signs of inflammation (REEDA scale) |
| Homans’ sign | Edema, redness, tenderness, warmth of legs, and Homans’ sign (positive or negative) |
| Emotional status | General attitude, sense of satisfaction, level of fatigue |
| Hydration | Amount of fluid intake, tissue turgor |
| Ambulation | If patient was dizzy or faint when up and about; frequency of ambulation |
| Vital signs | Temperature, pulse rate, respirations, and blood pressure |
| General condition | Color of skin and mucous membranes, coping ability |
| Pain or discomfort | Location and degree of discomfort, pain management strategies |
| Parenting | Mother’s reaction to newborn |
In addition to these specific assessments, observation and recording of vital signs, pain, hydration status, the woman’s ability to ambulate, and the ability to care for her newborn should also be included. When performing the postpartum check, the nurse explains that the reason for the assessment is to rule out any deviation from normal. In addition, the nurse teaches the woman how to assess the height and firmness of the uterus (Table 12-4). Because of early discharge, the woman is encouraged to continue this assessment when at home. If the uterus appears relaxed or boggy during the assessment, the uterus should be massaged until it is firm and remains firm. When the uterus is massaged, it is important not to be too vigorous because this may cause overstimulation, which can result in uterine atony (loss of muscular tone of the uterus) and hemorrhage.
Table 12-4
Assessment of the Uterine Fundus
| Finding | Characteristic | Nursing Intervention |
| Fundus is firmly contracted and at level of umbilicus. | Fundus feels like a hard grapefruit. | Instruct woman how to massage fundus. |
| Fundus is soft and boggy. | Fundus is difficult to locate and soft. | Support lower uterine. Segment and massage fundus until firm. Apply slight pressure to expel clots. Notify health care provider if fundus remains soft or if a trickle of bright red blood continues after fundus is firm. |
| Fundus is displaced from midline or above level of umbilicus. | Fundus may be firm but above level of umbilicus and not in midline. | Assess bladder for distention. Assist mother to void or catheterize and recheck fundus. Document findings. |
On completion of the postpartum check, the nurse documents the findings and promptly reports any abnormal findings. In addition to the usual postpartum assessments, the post-cesarean mother must also be assessed as a postoperative patient. Care of the woman after a cesarean birth is discussed in Chapter 14. Breast care and breastfeeding are discussed in Chapter 11.
Ambulation
Early and frequent ambulation is essential to reduce the risk of infection or thrombosis (clot formation). Early ambulation also reduces the chance that respiratory, circulatory, gastrointestinal, or urinary problems will develop and promotes the rapid return of strength. The woman is advised to ask the nurse to be with her when she gets out of bed for the first time. Women who have lost a large amount of blood are more apt to feel faint because of the decrease in blood volume.
Postpartum Chill
Women often experience a shaking, uncontrollable chill immediately after birth. The exact cause is unknown, but it may be related to a nervous response or to vasomotor changes rather than the coldness of the delivery or recovery room. If the chill is not followed by an elevated temperature, it is of no clinical significance. The woman should be covered with a warm blanket or have a hot drink and be reassured that the chill is a common experience after birth. After the first 24 hours, chill and fever may indicate infection, and the woman should have further evaluation.
Promoting Comfort
Most women have some degree of discomfort during the first few postpartum days. Common causes of discomfort include episiotomy, hemorrhoids, afterpains, and breast engorgement. Nursing interventions are intended to reduce the discomfort and allow the woman to take care of herself and her baby. Nonpharmacologic measures are used, either alone or in combination with pharmacologic interventions.
Nursing Interventions
Simple interventions that can decrease the discomfort associated with perineal trauma and hemorrhoids include encouraging the woman to lie on her side whenever possible and to use a pillow when sitting. Other interventions include applying an ice pack, moist or dry heat, or topical applications (if ordered); cleansing the perineum with a squeeze bottle (see Skill 12-4); and taking a warm shower or a sitz bath (Skill 12-5).
Application of Cold to the Perineum
An ice pack is often intermittently applied to the episiotomy in the first few hours after birth to reduce edema and numb the tissues, which can promote comfort. Commercial chemical ice packs are commonly used. Inexpensive ice bags can be made by filling a disposable glove with ice and then taping or securing the glove at the wrist opening to prevent water leakage as the ice melts. An ice pack is most effective during the first 24 hours after delivery.
The nurse should teach the woman about the purpose of the ice pack and its preparation at home if swelling is present. The woman is advised to cover the ice pack with a towel to prevent damage to skin integrity.
Application of Heat to the Perineum
Heat can also be used to decrease the woman’s discomfort. Heat increases circulation to the perineal area and relaxes the tissues. Either moist or dry heat can be applied after the first 24 hours.
Skill 12-5
Purpose
To aid healing of perineum through application of moist heat or cold.*
Steps
2. Assess the woman’s condition and analyze appropriateness of procedure.
3. Assemble equipment: sitz bath, clean towel, and clean perineal pad.
4. Place sitz bath on toilet seat; turn on flow of water.
5. Help the woman remove pad and sit in flow of water for 20 minutes.
6. When completed, help woman pat perineum dry; apply clean perineal pad (front to back).
7. Assist woman in returning to the room (then to the chair or bed).
8. Document that sitz bath was taken, condition of woman, and condition of perineum.

Sitz Bath
A sitz bath is an effective method of applying moist heat or cold to the perineum. It provides comfort, promotes healing, and reduces the incidence of infection. It is supplied as a plastic, disposable basin that fits inside the toilet. The sitz bath should not last longer than 20 minutes. Because of the soothing effect of the warm water and the sitting position, the woman may feel extremely tired and unsteady on her feet afterward and may need help getting into bed.
The nurse encourages the woman to clean a portable sitz bath basin or the tub before using it when she is home and to have the temperature of the water at approximately 38° C to 40.5° C (100° F to 105° F) when warm water is used. Cold moisture numbs nerve endings and causes vasoconstriction, which can reduce edema and hematoma. The use of a sitz bath is described in Skill 12-5.
Topical Anesthetic Application
Topical anesthetics (e.g., benzocaine [Americaine] or benzocaine and menthol [Dermoplast]) are given to relieve perineal discomfort. Sprays, dibucaine ointment, or witch hazel pads are commonly used to relieve hemorrhoidal discomfort. The woman is advised to apply the topical medication after a sitz bath or after using a heat lamp and to wait 1 to 2 minutes before applying the perineal pad, or much of the medication will be absorbed into the pad rather than stay on the perineal tissues.
Family Adjustment and Development of Attachment
Partner Bonding
The advancement from a generally farming society to a high-technology industrial economy has changed family and social interactions. Extended families often live far apart. Two-career families result in both partners working and both contributing to the nurturing of the family. The nurse should be sensitive to the roles of each parent, which may be nontraditional.
Responsibilities are often negotiated. The partner should be included in all teaching sessions involving newborn care and feeding. Partners often attend prenatal classes with the mother, are present at delivery as a primary coach, and must be included in follow-up care. Adaptation of the partner parallels that of the mother. Bonding actually begins prenatally when the father or partner feels the fetus move or hears the heartbeat.
Engrossment is the keen awareness and interest in the newborn, characterized by holding the newborn en face; studying and touching features; accepting and expressing unique resemblances of the newborn to family or themselves; and feeling pride, elation, and increased self-esteem (Figure 12-4). The reality is established when the partner participates in newborn care. A stage of conflict may follow when the partner may resent the time the mother spends focused on the newborn; the partner may seek recognition or feel excluded. Adjustment and transition occur when the partner is able to increase interaction with the newborn and understand that there will be time set aside for partner interaction as well. Family crises can be prevented by helping the parents incorporate the newborn into their modified lifestyle and helping them communicate personal and family issues and needs. The role of siblings and grandparents may need to be reestablished. The availability of social support and community resources should be explored and telephone numbers for support and advice given to parents.

Sibling Adjustment
Sibling response to the birth of a new sister or brother depends on their age and development. Younger siblings may consider the newborn to be competition and may fear that they will be replaced in the parents’ affections. Experts believe that children benefit from seeing the mother and newborn in the hospital setting (Figure 12-5). Early involvement can help reduce the older child’s anxiety, jealousy, and rivalry toward the newborn (Box 12-2). Behaviors that may surface include regression to more infantile behaviors such as thumb sucking. Some may show jealousy and frustration when they see the mother holding or feeding the newborn and miss how it feels to be the baby. Special time must be taken by both parents and grandparents to give attention to older siblings.

Grandparent Involvement
The involvement of grandparents with grandchildren depends on many factors. One of the most significant factors is proximity. Grandparents who live nearby often develop a strong attachment that involves sharing love, which adds security for the grandchildren (Figure 12-6). However, parenting practices change from one generation to the next, and this may bring conflict in child rearing. Attending classes, especially for grandparents, should be encouraged. In some cultures, the grandparents are expected to be with the new mother for the first 1 to 3 months to both help with the household duties and care for the new baby.

Promoting Parent-Newborn Bonding
Bonding and attachment are processes that produce an affectionate and emotional commitment between two individuals. This process is intense during the early post-birth period. The newborn, when alert, is able to elicit a strong positive response from the mother by making eye contact with her. Touch is important and elicits a positive response from the mother and stimulates the newborn. Mothers are observed using a high-pitched voice as they comfort the newborn, which causes newborns to become more alert and turn toward the mother. The attachment process is usually progressive over time. It is made easier with positive newborn behaviors, such as sucking, smiling, clinging by the grasp reflex, and eye-to-eye contact. During the postpartum stay, the nurse is responsible for monitoring that attachment is developing between family members and the newborn. Promoting and facilitating parental attachment are important. The nurse must recognize that the attachment process is strengthened through the use of sensual responses between the parents and newborn. Every positive interaction between parent and newborn intensifies the attachment (Box 12-3).

Signs of Positive Parent-Newborn Attachment
• Holds newborn close while feeding
• Makes eye contact with newborn
• Identifies physical characteristics to admire about newborn
• Assigns meaning to newborn’s actions such as grasp reflex (“The baby is holding my finger.”)
• Not upset with newborn stooling
• Strokes and massages newborn as newborn becomes quiet and relaxed
Early Discharge Planning and Health Promotion
Discharge planning is especially important with the current length of hospital stay. The woman’s greatest need is education to prepare her to care for herself and her newborn (Table 12-5). The woman must know how to prevent introducing infection to the still-unhealed uterus and episiotomy before discharge. She must be made aware of the danger signs and, if they occur, know to call the physician, nurse-midwife, or clinic.

Postpartum Danger Signs
After discharge, the woman should contact her physician or nurse-midwife if any of the following develops:
• Sudden persistent or spiking fever
• Change in vaginal discharge: increased amount, change to earlier color (bright red bleeding), offensive odor
• Pain or tenderness in abdomen or pelvic area
• Localized pain, redness, swelling, or warm area in calf
• Localized area of pain, redness, or swelling in breast
• Frequency, urgency, or burning on urination
Table 12-5
Postpartum Discharge Instructions
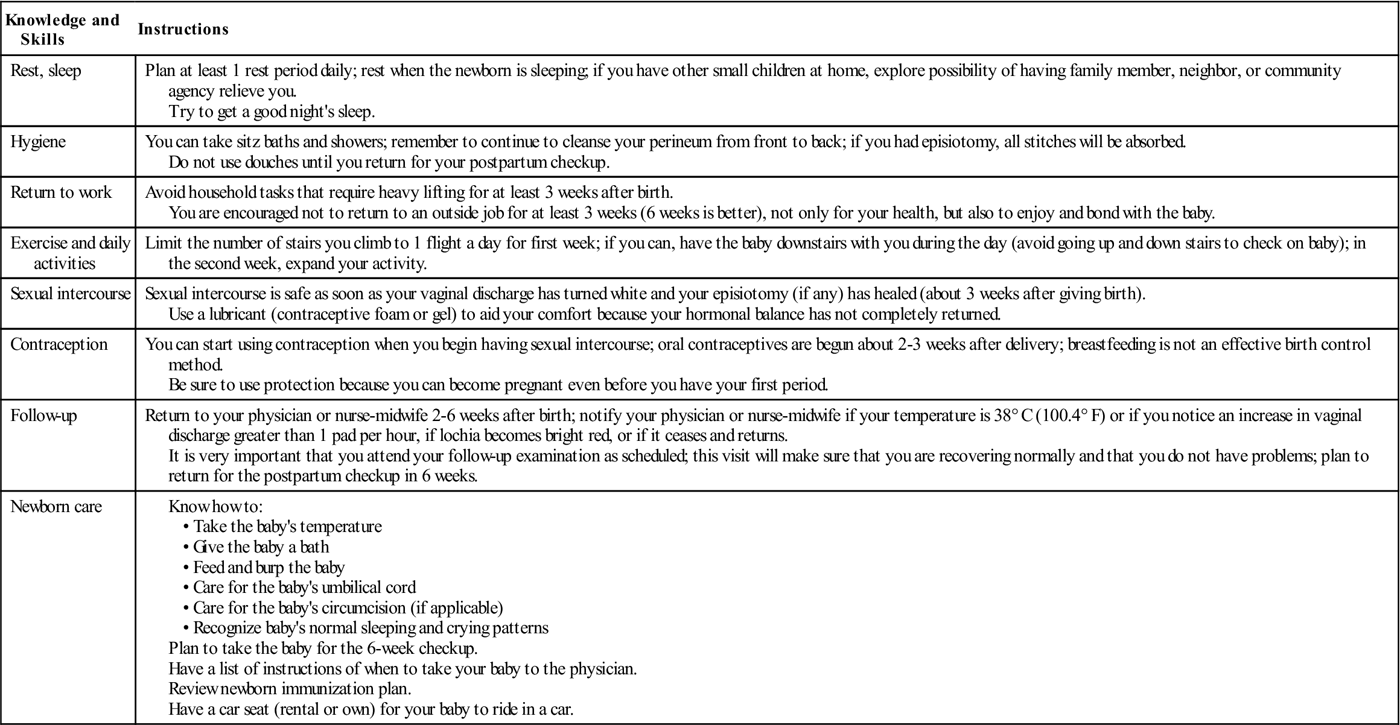
Nursing efforts are directed toward assessing the couple’s knowledge and expectations. The nurse should provide the parents with the opportunity to engage in newborn care while in the hospital to build confidence, allay fears, and ask questions. Referral for postpartum home visits or hotline resources may be indicated. Parents need to discuss relationships, their return to work schedules, and their roles in transition to parenthood. The nurse should guide the parents in understanding newborn behavior and growth and development patterns. Before actual discharge, the nurse spends time with the woman or couple to teach them and determine whether they have any last-minute questions (see Nursing Care Plan 12-1). This may be done by the primary nurse, case manager, or, in some facilities, a perinatal educator. The use of a clinical path for timelines and a maternal-newborn teaching checklist can serve as a documentation tool and ensures that all mothers are provided similar key information. The nurse often reviews the pamphlet or hospital-prepared discharge literature that explains what women are encouraged to do and not do for the stated period. The woman is informed whether videos on newborn bathing, cord and circumcision care, breast or formula feeding, and cardiopulmonary resuscitation (CPR) are available on loan or for purchase in the hospital gift shop. She also receives information about local agencies or support groups that can help them in parenting. When possible, literature should be provided in the patient’s language of preference.
The woman should have a scheduled appointment for her 2- or 6-week postpartum examination and her newborn’s first well-baby examination. Follow-up telephone calls and home visits allow for clarification and an opportunity to answer any questions. Many postpartum hospital units provide the woman with the telephone number, and she is encouraged to call if she has any questions, no matter how simple. The woman should be alerted to danger signs to report.
Resumption of Normal Activities
Women often ask what they may or may not do once they are home. They are advised to increase their activities gradually and avoid fatigue. They are instructed to avoid heavy lifting and excessive stair climbing for the 6-week recovery period. Most women resume practically all activities by 4 to 5 weeks’ postpartum. Current maternity leave provisions may enable the mother to delay returning to work outside of the home until after the 6-week postpartum period. When the woman can assume the duties of her previous position will vary, depending on the type of work and the normalcy of the postpartum recovery. Cultural factors also influence when normal activities are resumed.
Resumption of Sexual Intercourse
Sexual intercourse can safely be resumed when lochia has ceased, the episiotomy incision has healed, and the woman feels ready. The time varies from 2 to 6 weeks’ postpartum. If the woman had an extensive episiotomy or a laceration, she may want to wait for the perineum to heal. The first postpartum intercourse may be somewhat uncomfortable. This is partly attributable to dryness and diminished vaginal lubrication. Women are advised to use a water-soluble vaginal lubricant. Patience and gentleness by the partner are important factors for the woman and should be discussed with both before discharge. A position that puts less strain on the woman’s perineum is helpful (woman on top or woman on her side). Couples may be frustrated if there is decreased libido because of hormonal changes that may persist for a few months. Breastfeeding mothers should be forewarned that during orgasm, milk may spurt from the nipples because of the release of oxytocin. Nursing the newborn before lovemaking may reduce the chance of milk release. Other factors that may inhibit satisfactory sexual experience include the baby’s crying and sleep deprivation.
Postpartum Fatigue
Postpartum assessment should include evaluation for fatigue. In today’s modern lifestyle, the woman often works throughout her pregnancy, rooms in with the newborn, and returns home in 48 hours or less to take on full household responsibilities. There may be little opportunity to rest and adapt to the postpartum phase.
Postpartum fatigue is defined as an overwhelming, sustained sense of exhaustion and decreased capacity for physical and mental work. Most women start to experience fatigue during pregnancy, and it sometimes persists for more than a year after delivery. After delivery, most people inquire and comment about the baby; in the United States, few inquire about the mother’s fatigue. The stresses of labor and hormonal changes, wound healing, and establishment of breastfeeding contribute to the development of fatigue in the early postpartum days. Continuing sleep difficulties, child care responsibilities, and lack of assistance contribute to longer term fatigue that can interfere with the return to full pre-pregnancy functioning. Nursing intervention is challenged by the short hospital stay of postpartum women.
Some anticipatory counseling concerning preventive techniques should be given to all new mothers before discharge. Plans to minimize fatigue could include using the side-lying position for breastfeeding, avoiding telephone interruptions with use of an answering machine, and using Internet resources for stress management techniques. Assessment for fatigue should continue during all postpartum mother and baby clinic visits.
Family Planning
Although the decision is the couple’s, they are encouraged to discuss the use of various contraceptives during their hospital stay. The nurse can provide information about options for family planning (see Chapter 19) before the woman’s discharge from the hospital. The nurse should stress that ovulation often resumes before the first menses, and pregnancy can occur. Mothers who breastfeed exclusively may ovulate and menstruate later than women who breastfeed less frequently, but contraception should resume by 6 months’ postpartum. Oral contraceptives can be started 2 to 3 weeks after delivery in nonlactating women and as soon as lactation is well established in breastfeeding women. Progestin-only contraceptives have been used for contraception after birth and have shown to enhance the quality and duration of lactation. However, progestin-only contraceptives may be contraindicated in Hispanic women who have gestational diabetes because of the risk of developing type 2 diabetes (Gabbe, Niebyl, & Simpson, 2007).
Postpartum Exercises
Persistent maternal musculoskeletal and cardiovascular changes can present potential problems for the woman who exercises. The hormonal effects on connective tissue are not reversed until approximately 6 weeks’ postpartum. Until that time, the risk of injury is still present. For the woman with an uneventful birth, deep breathing, abdominal exercise for diastasis recti muscles, Kegel exercises, and pelvic tilts can be started on the first or second postpartum day.
Walking is an ideal exercise. The woman’s return to more vigorous fitness activities should be monitored according to individual responses and past fitness activities. Many hospitals and other facilities sponsor exercise classes for the postpartum woman.
Kegel Exercises
Kegel (perineal tightening) exercises are advised for the prenatal and the postpartum period. These exercises are encouraged to strengthen and tone the muscles of the pelvic floor. It is commonly believed that these exercises decrease stress incontinence, speed recovery, and increase sexual response. After a vaginal delivery, these muscles are often weaker than before birth, but tone can be regained with Kegel exercises. In performing these exercises, the woman contracts the pelvic floor muscles. The woman pulls up her entire pelvic floor, as if trying to suck up water with her vagina. She then bears down, as if trying to push the imaginary water out. In doing this, she is also using abdominal muscles. The woman should feel a tightening of the muscles around the anal sphincter, vagina, and urethra. This is done to promote healing of perineal tissues, increase the strength of the muscles, and increase urinary control. The woman is advised that doing perineal tightening exercises is beneficial throughout her life.
Pelvic Tilt
The pelvic tilt is helpful for good postural alignment and relief of strain on the lower back. It can be done in a sitting or standing position. With her arms stretched out, the woman tightens her abdominal and buttock muscles, arches her back, and then flattens her back against the wall (if standing) or chair (if sitting). This exercise strengthens back muscles and lessens back discomfort (see Chapter 5). This exercise is helpful beyond the postpartum period.
Special Immunizations
Most immunizations are not contraindicated during the postpartum phase, even if the mother is breastfeeding (Centers for Disease Control and Prevention, 2008).
Rubella Vaccine
Women who have a rubella titer of less than 1:10 are given the rubella vaccine during the postpartum period to protect their next fetus from fetal malformations. The nurse must make certain that these women understand the purpose of the rubella vaccine and that they must not get pregnant for the next 3 months.
Rho(D) Immune Globulin
Women who are Rh negative and meet specific criteria (see Chapter 13) should receive Rho(D) immune globulin (RhoGAM) within 72 hours’ postpartum. RhoGAM prevents the development of antibodies that would destroy fetal RBCs in subsequent pregnancies. In 2004, Rhophylac was approved by the FDA and is used in many hospitals to replace RhoGAM. It is derived from human plasma and never contained thimerosal (mercury). Rhophylac can be given IM or IV but cannot be given at the same time as other vaccines.
Get Ready for the NCLEX® Examination!
Key Points
• The postpartum period (puerperium) is the 6-week period after childbirth. During the early postpartum period, dramatic physiologic changes are made that result in the return of the body systems to the pre-pregnant state.
• Partners should be included in teaching newborn care and feeding.
• After childbirth, the woman is at great risk for hemorrhage; therefore, the woman is monitored very closely during the first few hours. These assessments are critical; however, the overall observations and interventions are focused on wellness.
• Uterine involution is the process by which the uterus returns to its pre-pregnant state.
• Postpartum assessment (postpartum checks) is made frequently to determine the woman’s response to recovery. The checks include the assessment of the level and firmness of the uterine fundus; the amount, color, and odor of the lochia; condition of the perineum, episiotomy, and hemorrhoids; hydration; adequate bladder emptying; and psychological responses.
• Lochia is the name given to vaginal flow after childbirth. The flow is lochia rubra (red) for the first 1 to 3 days, lochia serosa (pink to brown) during days 4 to 9, and lochia alba (yellow to white) until approximately 6 weeks’ postpartum.
• A hypercoagulable state exists during the puerperium, increasing the risk of venous thromboembolism.
• Postpartum blues is a common occurrence during the first 10 days after delivery. Nurses can offer supportive care and management strategies.
• Various comfort measures are used to alleviate pain from tissue trauma that occurs during birth, episiotomy, afterpains, and breast tenderness. Nursing interventions include ice packs and administration of analgesics as necessary.
• Ways to prevent infection during the postpartum period include adequate perineal care: cleansing the perineum after each voiding and defecation and always wiping from front to back (urinary meatus toward anus).
• Counseling and guidance that help new mothers and their families make adjustments to the newborn, deal with sibling responses, and react positively with grandparents are important nursing interventions.
• Self-care teaching is an integral part of postpartum nursing. With the brief hospital stay, follow-up by telephone and home visits are a welcome trend. All women are advised to return for their 2- or 6-week visit to be sure their recovery is uneventful.
• Discharge planning includes the assessment of the woman’s knowledge of self-care and newborn care. In addition, she is taught to report excessive vaginal bleeding, lochia with a foul odor, or increase in discharge; pain in the calf of the leg, which may be accompanied by redness, swelling, or warmth; pain, redness, or warmth of breasts in breastfeeding mothers; fever; pain, burning, or difficulty in urination; and abdominal or pelvic tenderness. Resumption of sexual intercourse and family planning are discussed with the couple.
• Anticipatory counseling to minimize postpartum fatigue should be offered to all new mothers.
• Information concerning support groups and telephone lines for questions or concerns should be given before discharge.
Additional Learning Resources
 Go to your Study Guide on pages 495-496 for additional Review Questions for the NCLEX® Examination, Critical Thinking Clinical Situations, and other learning activities to help you master this chapter content.
Go to your Study Guide on pages 495-496 for additional Review Questions for the NCLEX® Examination, Critical Thinking Clinical Situations, and other learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer/maternity) for the following FREE learning resources:
 Online Resources
Online ResourcesReview Questions for the NCLEX® Examination
1. The correct order for the phases of lochia during the postpartum period is:
1. Lochia rubra, lochia alba, lochia serosa
2. Lochia serosa, lochia rubra, lochia alba
3. Lochia rubra, lochia serosa, lochia alba
4. Lochia alba, lochia rubra, lochia serosa
2. Which changes are expected to occur during the initial postpartum period (Select all that Apply.)
2. Decrease in daily urinary output
3. Increase in white blood cell count to 15,000/mm3
4. Increased fibrinogen levels
3. The nurse is caring for a postpartum patient 24 hours following delivery. Which assessment made by the nurse requires immediate attention?
1. Heart rate of 50 beats/minute
4. Decrease in blood pressure to 80/56
4. According to Rubin (1984), the taking hold phase is the second maternal phase and is characterized by:
1. The woman’s readiness to assert independence
2. Passive, dependent behavior
3. The woman focusing on her own needs
4. The woman’s concern about the overall health of the newborn
5. When assessing the amount of lochia present on the perineal pad of a postpartum woman, after it has been applied for 1 hour, the nurse notes a 5-inch stain. Documentation should indicate quantity as a:
6. Postpartum blues occur in approximately 70% of women during the first few days after birth and generally lasts up to 10 days. This state is characterized by which trait(s)? (Select all that apply.)
7. Put the stages of maternal role attainment in the correct order from first to last.