Digestion, Absorption, and Metabolism
State of dynamic equilibrium within the body’s internal environment; a balance achieved through the operation of many interrelated physiologic mechanisms.
The process of breaking down food to release its nutrients for absorption and transport to the cells for use in body functions.
Outer surface layer of the intestines interfacing with the blood vessels of the portal system going to the liver.
The mucous membrane forming the inner surface of the gastrointestinal tract with extensive nutrient absorption and transport functions.
A wavelike progression of alternate contraction and relaxation of the muscle fibers of the gastrointestinal tract.
Semifluid food mass in the gastrointestinal tract after gastric digestion.
On-going low-level muscle contraction and relaxation.
Network of nerves in the walls of the intestine that make up the intramural nervous system, controlling muscle action and secretions for digestion and absorption.
Red, swollen, bleeding gums, most often caused by accumulation of bacterial plaque on the teeth.
Throat.
Rounded mass of food formed in the mouth and ready to be swallowed.
Away from the point of origin.
The first section of the small intestine entered by food passing through the pyloric valve from the stomach.
Sticky.
Lower section of the stomach.
Hormone secreted by mucosal cells in the antrum of the stomach that stimulates the parietal cells to produce hydrochloric acid. Gastrin is released into the stomach in response to various stimulants, especially caffeine, alcohol, and meat extracts. When the gastric pH falls below 3, a feedback mechanism cuts off gastrin secretion to prevent excess acid formation.
Hormone produced in the mucous membrane of the duodenum that inhibits gastric acid secretion and motility.
Number of millimoles of liquid or solid in a liter of solution.
Viscous fluid secreted by mucous membranes and glands, consisting mainly of mucin (a glycoprotein), inorganic salts, and water. Mucus lubricates and protects the gastrointestinal mucosa and helps move the food mass along the digestive tract.
Hormone produced in the mucous membrane of the duodenum in response to the entrance of acid contents from the stomach. Secretin in turn stimulates the flow of pancreatic juices, providing needed enzymes and the proper alkalinity for their action.
A peptide hormone secreted by the mucosa of the duodenum in response to the presence of fat. Cholecystokinin causes the gallbladder to contract and propel bile into the duodenum, where it is needed to emulsify the fat and prepare it for digestion and absorption.
Transport of nutrients from the lumen of the intestine across the intestinal wall into the blood (glucose and amino acids) or the lymph (fatty acids).
Small protrusions from the surface of a membrane; fingerlike projections covering mucosal surfaces of the small intestine.
Minute vascular structures protruding from the villi covering the inner surface of the small intestine and forming a “brush border” that facilitates absorption of nutrients.
Means of nutrient absorption by which the molecule is engulfed by the cytoplasm of the receiving cell.
Noncovalent complexes of fat with protein. The lipoproteins function as major carriers of lipids in the plasma; this combination of fat surrounded by protein makes possible the transport of fatty substances in a water medium such as plasma.
Cistern or receptacle of the chyle; a dilated sac at the origin of the thoracic duct, which is the common trunk that receives all the lymphatic vessels. The cisterna chyli lies in the abdomen between the second lumbar vertebra and the aorta. It receives the lymph from the intestinal trunk, the right and left lumbar lymphatic trunks, and two descending lymphatic trunks. The chyle, after passing through the cisterna chyli, is carried upward into the chest through the thoracic duct and empties into the venous blood at the point where the left subclavian vein joins the left internal jugular vein. This is the way absorbed fats enter the general circulation.
The large intestine extending from the cecum to the rectum.
The distal section of the small intestine that connects with the colon.
A reddish bile pigment resulting from the degradation of heme by reticuloendothelial cells in the liver; a high level in the blood produces the yellow skin symptomatic of jaundice.
Chain of 8 to 10 glucose units.
Gastric distress or indigestion involving nausea, pain, burning sensations, or excessive gas.
Production of glucose from keto acid carbon skeletons from deaminated amino acids and the glycerol portion of fatty acids.
Specific term for conversion of glycogen into glucose in the liver; chemical process of enzymatic hydrolysis or breakdown by which this conversion is accomplished.
Removal of an amino group (NH2) from an amino acid.
Amino acid residue after deamination. The glycogenic keto acids are used to form carbohydrates.

We continue our study of nutrition by looking at what happens to food as it follows its path through the digestive system and is broken down into forms that the body can use to perform its work. We will review all the steps that must occur to convert the tuna sandwich we had at lunch into the energy-yielding nutrients—glucose, amino acids, and fatty acids. These steps are accomplished by an integrated system that receives the foods we take in and transforms them for our use.
The physiologic and biochemical process that turns the food we eat into energy and body tissue has three parts: digestion, absorption, and metabolism. We begin with a review of the gastrointestinal tract and then follow the path of the nutrients to the cells, where they nourish and protect us. We will see how all parts work together to accomplish this task.
Human body: The role of nutrition
Food: Change and transformation
The foods we eat contain the nutrients necessary for our survival, but these life-sustaining materials must first be released from other food components and transformed into units the body can use. Through a successive interrelated system, foods are broken down into simpler substances and then still simpler substances that can enter the metabolic pathways in cells. Each section of the gastrointestinal tract has a unique function, but together they form a continuous whole. A problem in one organ has clinical consequences for the entire system.
Importance for health and nutrition
Gastrointestinal function is a partner in nutritional well-being.1 Food, as it occurs in nature and as we eat it, is not a single substance but a mixture of nutrients and other chemical matter. These substances must be separated so the body can handle each one as an individual unit. Nutrients released from food remain unavailable to the body until they cross the intestinal wall and enter the circulatory system for transport to tissues. Diseases affecting the organs of the gastrointestinal tract or the absorbing surface of the intestinal wall have adverse effects on nutritional status because nutrients are not made available in the amounts needed. At the same time, moderate to severe malnutrition lowers secretion of digestive enzymes and blunts the absorbing structures, further limiting digestion and nutrient passage. This vicious cycle results in rapid and progressive deterioration of nutritional status.1
The gastrointestinal tract is one of the many body systems with an output that is essential to the chemical work taking place in tissues and cells. The recognition of the human body as an integrated physiochemical organism is basic to understanding human nutrition in both health and disease. The internal control responsible for maintaining a constant chemical environment and keeping the many functional systems operating in harmony with one another is called homeostasis.2
The gastrointestinal tract
Component Parts
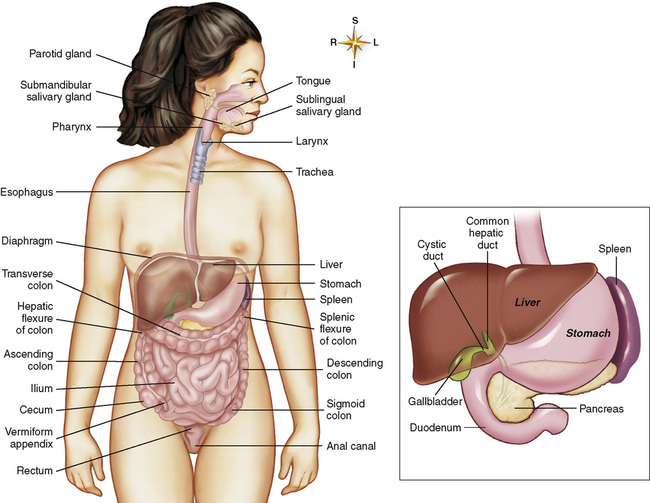
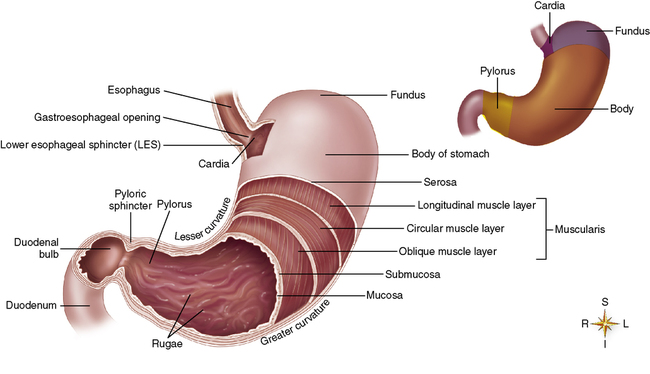
The gastrointestinal tract, also called the alimentary canal, is a long hollow tube that begins at the mouth and ends at the anus. The specific parts that make up the tract are the mouth, esophagus, stomach, small intestine, large intestine or colon, and rectum. Other organs that lie outside the tract but support its work by secretion of important enzymes and digestive fluids are the pancreas, gallbladder, and liver. Look at the respective components of the gastrointestinal tract and their relative position to one another, as shown in Figure 2-1. These organs, working as a team, can break down and/or absorb several kilograms of carbohydrate, one half kilogram of fat, one half kilogram of protein, and 20 or more liters of water daily.2 We will follow these food components as they travel together through the successive parts of the gastrointestinal tract.
General Functions
The gastrointestinal tract has the following four major functions:
1. Receives food: The mouth is the entrance to the gastrointestinal tract. From here the food is moved on to the stomach and other organs for digestion and absorption.
2. Releases nutrients from food: Digestion and the separation of nutrients from other food components take place in the stomach and small intestine.
3. Delivers nutrients into the blood: Absorbing structures called microvilli located in the small intestine transfer the nutrients into the portal blood (glucose and amino acids) or lymph (fatty acids). Water is absorbed later in the colon.
4. Excretes nondigestible waste: The fecal mass moves from the colon into the rectum, where it is stored until excreted.
Both physical and chemical actions accomplish these tasks.
Sensory Stimulation and Gastrointestinal Function
Both physiologic and psychologic stimuli influence the gastrointestinal tract. The physical presence of food in the mouth, stomach, or small intestine initiates a variety of responses that coordinate the muscular movements and chemical secretions necessary for digestion and absorption. Sensory stimuli—the sight, smell, or proximity to food—brings about the secretion of digestive juices and muscle motility.2 Smelling cookies baking, hearing foods sizzle on an outdoor grill, or picking a fresh berry can evoke the physiologic process of digestion. Seeing a sign advertising your favorite food or even thinking about food stimulates the gastrointestinal tract. On the other hand, dread of an unpleasant-tasting medication or recalling the nausea brought on by chemotherapy can repress the desire for food. Positive associations with food and mealtime promote efficient digestion and absorption of nutrients.
Principles of digestion
Digestion is the first step in preparing food for use by the body. It includes two types of actions: muscular and chemical.
Gastrointestinal Motility: Muscles and Movement
Digestion involves mechanical mixing and propulsive movements controlled by neuromuscular, self-regulating systems. These actions work together to move the food mass along the alimentary canal at the best rate for digestion and absorption.
Types of Muscles
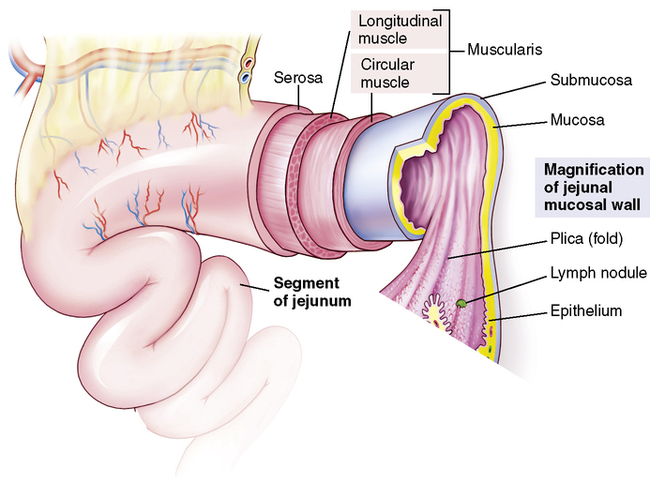
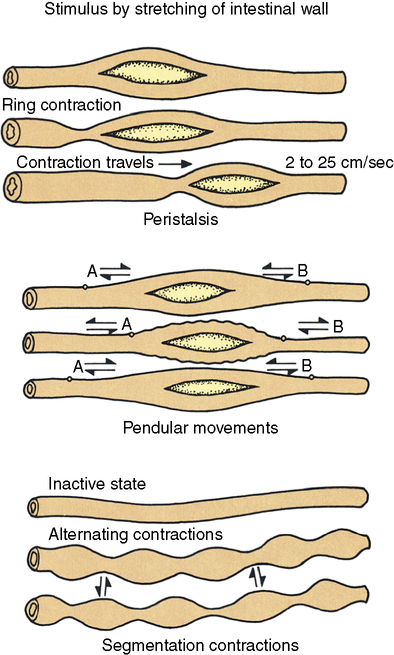
Organized muscle layers in the gastrointestinal wall provide the motility needed for digestion (Figure 2-2). From the outer surface inward the layers are (1) the serosa, (2) a longitudinal muscle layer, (3) a circular muscle layer, (4) the submucosa, and (5) the mucosa. Embedded in the deeper layers of the mucosa are thin bundles of smooth-muscle fibers called the muscularis mucosae. The coordinated interaction of the following four smooth-muscle layers makes possible four different types of movement (Figure 2-3).
1. Longitudinal muscles: These long, smooth muscles arranged in fiber bundles extend lengthwise along the gastrointestinal tract and help propel the food mass forward.
2. Circular contractile muscles: The circular smooth-muscle fibers extend around the hollow tube forming the alimentary canal. These contractile rings initiate rhythmic sweeping waves along the digestive tract, pushing the food mass forward. These regularly occurring propulsive movements are called peristalsis.
3. Sphincter muscles: At strategic points, muscle sphincters act as valves—pyloric, ileocecal, and anal—to prevent reflux or backflow and keep the food mass moving in a forward direction.
4. Mucosal muscles: This thin embedded layer of smooth muscle produces local constrictive contractions every few centimeters. These contractions mix and chop the food mass, effectively churning and mixing it with secretions to form a semiliquid called chyme that is ready for absorption.
In summary, the muscles lining the gastrointestinal tract produce the following two types of action:
1. Tonic contractions that ensure continuous passage of the food mass and valve control
2. Periodic rhythmic contractions that mix and propel the food mass forward
Alternating contraction and relaxation of these muscles moves the food contents along the tract and facilitates digestion and absorption.
Nervous System Control
Throughout the gastrointestinal tract, specific nerves regulate muscle action. An interrelated network of nerves within the gastrointestinal wall called the intramural nerve plexus (Figure 2-4) extends from the esophagus to the anus. This network of approximately 100 million nerve fibers regulates the rate and intensity of muscle contractions, controls the speed at which the food mass moves along the tract, and coordinates the digestive process, including the secretion of enzymes and digestive juices.3

Gastrointestinal Secretions
Food is digested chemically through the combined action of several secretions. These secretions are of the following four types.
1. Enzymes: Certain enzymes attack designated chemical bonds within the structure of nutrient compounds, freeing their component parts.
2. Hydrochloric acid and buffer ions: These secretions produce the pH necessary for the activity of certain enzymes.
3. Mucus: This sticky, slippery fluid lubricates and protects the inner lining of the gastrointestinal tract and eases the passage of the food mass.
4. Water and electrolytes: These agents provide appropriate solutions in the amounts needed to circulate the substances released in the digestive process.
These secretions are produced by special cells in the mucosal lining of the gastrointestinal tract and in adjacent accessory organs, especially the pancreas. Their release is stimulated by (1) the presence of food in the gastrointestinal tract, (2) the sensory nerve network activated by the sight, taste, or smell of food, and (3) hormones specific to certain nutrients.
Mouth and esophagus: Preparation and delivery
Eating begins the physiologic process by which food is broken down into individual nutrients. The first step takes place in the mouth, where food is prepared for digestion and delivered to the stomach by way of the esophagus.
Taste and Smell
Much of our enjoyment of food comes from its unique flavors and aromas. Taste buds located on the tongue, roof of the mouth, and throat contain chemical receptors that respond to food and produce the four sensations of taste: salty, sweet, sour, and bitter. Some individuals have a stronger perception of one taste over another, and certain medications produce a bitter taste or loss of taste. Genetic-related differences in taste affecting our preference for one type of food over another (e.g., fatty foods, sweets, or vegetables) can influence what we eat and our risk for developing a particular disease or condition.4 Patients on chemotherapy often have distorted taste (dysgeusia). Zinc deficiency causes a loss of taste (hypogeusia), and older people sometimes experience changes in taste as the number of taste buds decreases.5
Foods contain volatile components that move from the back of the mouth up into the nasal cavity, where they act on olfactory receptors to produce the pleasant odors we associate with particular foods. In fact, much of what we perceive as a food taste may actually be its odor. Radiation therapy of the head or neck, Parkinson’s disease, and senile dementia of the Alzheimer type often lead to olfactory losses and reduced joy in eating.
Mastication
Biting and chewing break food into smaller particles. The incisors cut; the molars grind. Jaw muscles provide tremendous force: 55 lb of muscular pressure is applied through the incisors, and 200 lb is applied through the molars.2 Digestive enzymes act only on the surface of food particles; therefore chewing to enlarge the surface area available for enzyme action is an important step in preparing food for digestion. Chewing produces fine particles that ease the passage of the food mass down the esophagus and into the stomach. Chewing is necessary to prepare fiber-containing foods—fruits, vegetables, and whole grains—for digestion. Decayed teeth, loss of teeth, or poorly fitting dentures make eating difficult. Gingivitis and other diseases of the gums and supporting structures of the teeth resulting in mouth pain, infection, or further loss of teeth restrict food intake and contribute to malnutrition.
Swallowing
Swallowing involves both the mouth and the pharynx. It is intricately controlled by the swallowing center in the brainstem,2 and damage to these nerves through radiation therapy, aging, or disease makes swallowing difficult. The tongue initiates a swallow by pressing the food upward and backward against the palate. From this point on, swallowing proceeds as an involuntary reflex and, once begun, cannot be interrupted. Swallowing occurs rapidly, taking less than 1 second, but in that time (1) the larynx must close to prevent food from entering the trachea and moving into the lungs, and (2) the soft palate must rise to prevent food from entering the nasal cavity (Figure 2-5). Patients must never be fed in a supine position because it increases the risk of aspirating food into the lungs.

Esophagus
The esophagus is a muscular tube that connects the mouth and throat with the stomach and serves as a channel to carry the food mass into the body. Functionally, it has the following three parts2:
1. Upper esophageal sphincter (UES): The UES controls the entry of the food bolus into the esophagus. Between intakes the UES muscle is closed. Within 0.2 to 0.3 second after a swallow, nerve stimuli open the sphincter to receive the food mass.
2. Esophageal body: The mixed bolus of food passes immediately down the esophagus, moved along by peristaltic waves controlled by nerve reflexes. Changes in the muscles or nerves lower the intensity and frequency of the peristaltic waves, slowing passage down the channel. Diabetic neuropathy is one cause of such problems.6 Pain and discomfort associated with these changes can add to anorexia and weight loss in older persons. Gravity aids the passage of food down the esophagus when the person eats in an upright position.
3. Lower esophageal sphincter (LES): The LES controls the movement of the food bolus from the esophagus into the stomach. When the LES muscles maintain excessively high muscle tone, they fail to open after a swallow, preventing the passage of food into the stomach. This condition is called achalasia, meaning unrelaxed muscle. (See Chapter 20 for a discussion of this condition.)
Entry into the Stomach
At the point of entry into the stomach the gastroesophageal constrictor muscle relaxes to allow the food to pass and then contracts quickly to prevent regurgitation or reflux of the acidic stomach contents back into the esophagus. When this mechanism fails and regurgitation occurs, one feels what is often called heartburn. The medical name for this condition is gastroesophageal reflux disease (GERD), and an estimated 25% of the population experience GERD on an occasional or chronic basis.7 GERD damages the tissues of the esophagus which are unprotected against the destructive effects of gastric acid. (Mucus secreted by cells in the stomach wall protects those tissues against the harsh effects of gastric acid.) Obesity, overeating, physical inactivity, smoking, and certain medications contribute to this condition.8–9 Increasing severity of GERD affects quality of life.9
Chemical Digestion
In the mouth, three pairs of salivary glands—(1) parotid, (2) submaxillary, and (3) sublingual—produce a watery fluid containing salivary amylase. This enzyme is specific for starch. The salivary glands also secrete mucus to lubricate and bind the food particles together. Sensory stimuli—and even thoughts of favorite or disliked foods—influence these secretions. As described in Table 2-1, large amounts of digestive fluids are secreted throughout the gastrointestinal tract. Saliva secretion ranges from 800 to 1500 mL a day, with a pH range of 6.0 to 7.4 (approximately neutral). Food remains in the mouth for only a short time, thus starch digestion here is brief. However, when salivary amylase binds to starch molecules, it becomes resistant to inactivation by gastric acid, thus breakdown of starch continues in the stomach.3 A second digestive enzyme released in saliva is lingual lipase, which begins the digestion of fat. Cigarette smoke alters the composition of saliva even in passive smokers,10 and this effect may contribute to the loss of taste associated with smoking, as well as the increased risk of oral cancer.11
TABLE 2-1
Comparative pH Values and Approximate Daily Volumes of Gastrointestinal Secretions
| Secretion | pH | Daily Volume (in mL) |
| Salivary | 6.0-7.4 | 1000 |
| Gastric | 1.0-3.5 | 1500 |
| Pancreatic | 8.0-8.3 | 1000 |
| Small intestinal | 7.5-8.0 | 1800 |
| Brunner gland (bicarbonate) | 8.0-8.9 | 200 |
| Bile | 7.5-7.8 | 1000 |
| Large intestinal | 7.5-8.0 | 200 |
| Total | 6700 |
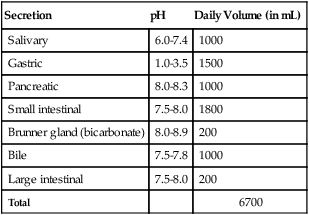
Modified from Guyton AC, Hall JE: Textbook of medical physiology, ed 10, Philadelphia, 2000, Saunders.
Salivary secretions have other important functions in addition to initiating digestion. They (1) moisten the food particles so they bind together to form a bolus that moves easily down the esophagus, and (2) they lubricate and cleanse the teeth and tissues of the mouth, destroying harmful bacteria and neutralizing toxic substances entering the mouth. Inadequate secretion leads to the condition known as dry mouth. Everyone experiences dry mouth now and then when nervous, upset, or under stress. However, when saliva production is drastically reduced and prolonged, it leads to swallowing problems because individual particles of food get separated in the esophagus. Infections and ulcers in the mouth along with tooth decay are other outcomes of extreme dry mouth, usually known as xerostomia. Radiation therapy causing damage to the salivary glands and diseases such as diabetes, Parkinson’s disease, and autoimmune deficiency disease can lead to xerostomia. Various medications for the management of cardiac failure, hypertension, depression, or chronic pain contribute to dry mouth and are often associated with this condition in elderly adults.12
Stomach: Storage and initial digestion
Motility
The major parts of the stomach are shown in Figure 2-6. Muscles in the stomach wall have three motor functions: (1) storage, (2) mixing, and (3) controlled emptying. As the food mass enters the stomach it rests against the stomach walls, which stretch to store as much as 1 L of food and fluid. Local tonic muscle waves increase their kneading and mixing action to move the mass of food and secretions toward the pyloric valve at the distal end of the stomach. Waves of peristaltic contractions reduce the food mass to the semifluid chyme. Finally, with each wave, small amounts of chyme pass through the pyloric valve into the duodenum. The pyloric sphincter periodically constricts and relaxes to control the rate of emptying of the stomach contents. The highly acid chyme must be released slowly enough to allow it to be buffered by the alkaline secretions of the duodenum.
The caloric density of a meal, along with its volume and composition, influences the rate of stomach emptying. The speed at which food moves from the gastroesophageal sphincter to the distal end of the stomach and into the small intestine influences food intake, as messages to the brain signaling the arrival of food in the small intestine induce feelings of satiety.
Chemical Digestion
Types of Secretions
Secretions produced in the stomach include acid, mucus, and enzymes, as follows:
• Acid: Hydrochloric acid creates the acidic environment necessary for certain digestive enzymes to work. For example, a pH of 1.8 to 3.5 is needed for the enzyme pepsin to act on protein; at a pH of 5.0 or above, little or no pepsin activity occurs.
• Mucus: This viscous secretion protects the stomach lining from the eroding effect of the acid. Mucus also binds and mixes the food mass and helps move it along.
• Enzymes: The major enzyme in the stomach is pepsin, which begins the breakdown of protein. Pepsin is secreted in the form of pepsinogen and activated by hydrochloric acid. The stomach also produces a small amount of gastric lipase (tributyrinase) that acts only on butterfat and has a relatively minor role in overall digestion. Children have a gastric enzyme called rennin (not to be confused with the renal enzyme renin) that aids in the coagulation of milk. Coagulation of the proteins in milk, changing them from a liquid to a semisolid (as occurs when egg white is heated), slows the rate of stomach emptying, ensuring gradual passage of material to the small intestine. Rennin is absent in adults.
Control of Secretions
Stimuli for the release of gastric secretions come from the following two sources:
1. Nerve stimuli are produced in response to the visual and chemical senses, the presence of food in the gastrointestinal tract, and emotional distress. Anger and hostility increase gastric secretions; fear and depression lower secretions and inhibit both blood flow to the region and gastric motility.
2. Hormonal stimuli are produced when food enters the stomach. Certain food components, especially caffeine, alcohol, and meat extracts, cause the mucosal cells of the antrum to release the local gastrointestinal hormone gastrin. Gastrin, in turn, stimulates the secretion of hydrochloric acid. When the pH falls below 3, a feedback mechanism halts the release of gastrin, preventing accumulation of excess acid.3 A second gastrointestinal hormone, enterogastrone, produced in the mucosa of the duodenum, prevents excessive gastric activity by inhibiting secretion of hydrochloric acid and pepsin and slowing gastric motility. (See the Evidence-Based Practice box, “Why Are Many Older Adults Deficient in Vitamin B12?” for an example of a problem related to inadequate secretion of gastric acid.)
Small intestine: Major digestion, absorption, and transport
Motility
Intestinal Muscle Layers
Review the complex structure of the intestinal wall pictured in Figure 2-2. Coordination of intestinal motility is accomplished by three layers of muscle: (1) the thin layer of smooth muscle embedded in the mucosa (the muscularis mucosae) with fibers extending up into the villi, (2) the circular muscle layer, and (3) the longitudinal muscle lying next to the outer serosa.
Types of Intestinal Muscle Action
Under the control of the intramural nerve plexus, wall-stretch pressure from food or hormonal stimuli produces muscle action of the following two types:
1. Propulsive movements: Peristaltic waves from contractions of the deep circular muscles propel the food mass slowly forward. The presence of food or irritants brings about long sweeping waves over the entire intestine. A series of local segmental contractions also support the forward movement of the food bolus. Fiber and other indigestible materials from plant foods aid this process, providing bulk for the action of these muscles.
2. Mixing movements: Local constrictive contractions occurring every few centimeters mix and chop the food particles to form the semiliquid chyme.
The interaction of the muscles in the small intestine producing (1) general tonic contractions that ensure continuous passage and valve control and (2) periodic, rhythmic contractions that mix and propel the food mass forward facilitates ongoing digestion and future absorption.
Chemical Digestion
Major Role of the Small Intestine
In comparison to other sections of the gastrointestinal tract, the small intestine carries the major burden of chemical digestion. It secretes various enzymes, each specific for carbohydrate, fat, or protein, and is assisted by other enzymes entering from the pancreas. The small intestine acts as a regulatory center sensing the nutrient content, pH, and osmolarity of its contents and controls enzyme secretion accordingly.3
Types of Secretions
The following four types of digestive secretions complete this final stage of chemical breakdown:
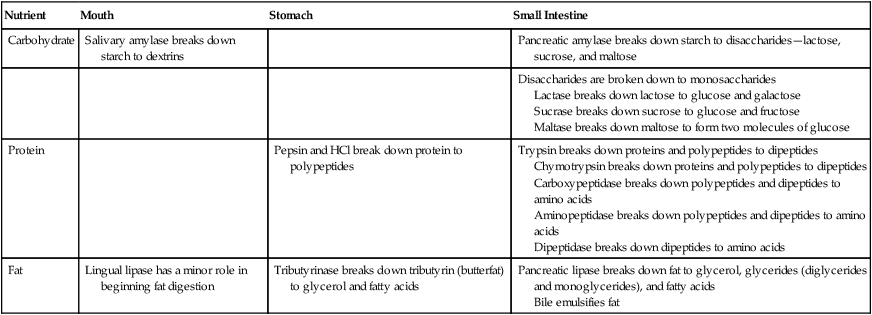
1. Enzymes: Specific enzymes act on specific macronutrients to bring about their final breakdown to forms the body can absorb and use (review Table 2-2).
TABLE 2-2
Summary of Digestive Processes
| Nutrient | Mouth | Stomach | Small Intestine |
| Carbohydrate | Salivary amylase breaks down starch to dextrins | Pancreatic amylase breaks down starch to disaccharides—lactose, sucrose, and maltose | |
| Disaccharides are broken down to monosaccharides Lactase breaks down lactose to glucose and galactose Sucrase breaks down sucrose to glucose and fructose Maltase breaks down maltose to form two molecules of glucose |
|||
| Protein | Pepsin and HCl break down protein to polypeptides | Trypsin breaks down proteins and polypeptides to dipeptides Chymotrypsin breaks down proteins and polypeptides to dipeptides Carboxypeptidase breaks down polypeptides and dipeptides to amino acids Aminopeptidase breaks down polypeptides and dipeptides to amino acids Dipeptidase breaks down dipeptides to amino acids |
|
| Fat | Lingual lipase has a minor role in beginning fat digestion | Tributyrinase breaks down tributyrin (butterfat) to glycerol and fatty acids | Pancreatic lipase breaks down fat to glycerol, glycerides (diglycerides and monoglycerides), and fatty acids Bile emulsifies fat |
2. Mucus: Glands located at the entrance to the duodenum secrete large amounts of mucus. As in the stomach, mucus protects the intestinal mucosa from irritation and digestion by the highly acid chyme entering from the stomach. Other cells along the length of the inner intestinal wall secrete mucus when touched by the moving food mass, lubricating and protecting the mucosal tissues from abrasion.
3. Hormones: When signaled by the presence of acid in the food mass entering from the stomach, mucosal cells in the upper part of the small intestine produce the local gastrointestinal hormone secretin.3 Secretin, in turn, stimulates the pancreas to send alkaline pancreatic juices into the duodenum to buffer the acidic chyme. The intestinal mucosa in the upper duodenum cannot withstand the high acid of the entering chyme without the neutralizing action of the bicarbonate-containing pancreatic juice.
4. Bile: Bile emulsifies fat and facilitates its digestion. Bile is produced in the liver as a dilute watery solution and then is concentrated and stored by the gallbladder. When fat enters the duodenum, the local gastrointestinal hormone cholecystokinin (CCK) is secreted by glands in the intestinal mucosa and stimulates the gallbladder to contract and release bile. By means of the enterohepatic circulation (Figure 2-7), molecules of bile are reabsorbed and returned to the liver and gallbladder to be used over and over again. CCK also acts on the pancreas to stimulate the release of enzymes that break down fats, proteins, and carbohydrates.3

End Products of Digestion
When digestion of the macronutrients is complete, the simplified end products, summarized in Table 2-3, are ready for absorption. At times, undigested nutrients remain in the small intestine,6 with accompanying discomfort or distress. When persons lack the digestive enzyme lactase, the disaccharide lactose remains in the small intestine, attracting large amounts of fluid and resulting in abdominal pain and diarrhea, nausea, or flatulence.13 (This condition and its clinical management are discussed later in this chapter.)
Absorption
Surface Structures
Viewed from the outside, the small intestine appears smooth, but the inner surface is quite different. Note in Figure 2-8 the following three types of convolutions and projections that greatly expand the area of the absorbing surface:
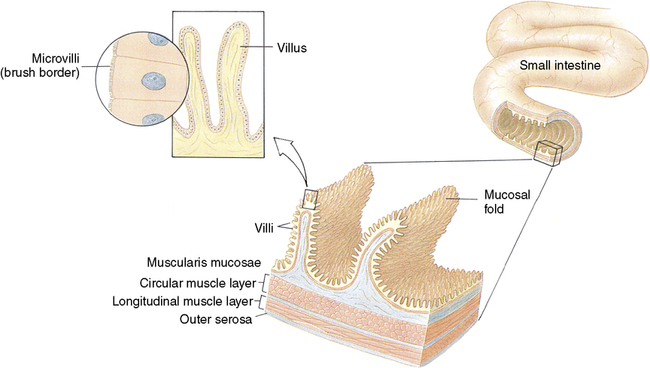
1. Mucosal folds: Large folds similar to hills and valleys in a mountain range can be easily seen with the naked eye.
2. Villi: Finger-like projections on these folds called villi can be seen through a simple compound microscope.
3. Microvilli: These extremely small projections on each villus can be seen only with an electron microscope. The array of microvilli covering the edge of each villus is called the brush border because it resembles bristles on a brush. Each villus has an ample network of blood capillaries for the absorption of monosaccharides and amino acids and a central lymph vessel called a lacteal for the absorption of fatty acids.
The mucosa, villi, and microvilli together increase the inner surface area of the small intestine approximately 1000 times over that of the outside serosa.2 These specialized structures, plus the contracted length of the small intestine—630 to 660 cm (21-22 feet)—produce a tremendously large surface area to capture and absorb nutrients. This absorbing surface, if stretched out flat, would be as large as a tennis or basketball court! The small intestine is one of the most highly developed organs in the body, making possible its tremendous absorptive capacity for food and fluid (Table 2-4).
TABLE 2-4
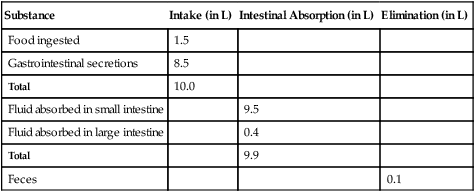
Volume of Nutrients Absorbed Daily by the Gastrointestinal System
| Substance | Intake (in L) | Intestinal Absorption (in L) | Elimination (in L) |
| Food ingested | 1.5 | ||
| Gastrointestinal secretions | 8.5 | ||
| Total | 10.0 | ||
| Fluid absorbed in small intestine | 9.5 | ||
| Fluid absorbed in large intestine | 0.4 | ||
| Total | 9.9 | ||
| Feces | 0.1 |
Mechanisms of Absorption
Absorption of the nutrients dispersed in the water-based solution entering the small intestine involves several transport mechanisms. The particular transport used depends on the nutrient and the prevailing electrochemical fluid pressure gradient, as follows:
• Passive diffusion and osmosis: When no opposing fluid pressure is present, molecules small enough to pass through the capillary membranes diffuse easily into the villi (Figure 2-9). High concentrations of nutrients waiting to move into the capillaries where nutrient concentrations are low create an electrochemical gradient and osmotic pressure that promote absorption.2

• Facilitated diffusion: Even when the pressure gradient is favorable, some molecules may be too large to pass easily through the membrane pores and need assistance. Specific proteins located in the membrane facilitate passage by carrying the nutrient across the membrane.
• Energy-dependent active transport: Nutrients must cross the intestinal membrane to reach hungry cells even when the flow pressures are against them. Such active work requires extra energy along with a pumping mechanism. A special membrane protein carrier, coupled with the active transport of sodium, assists in the process. The energy-requiring, sodium-coupled transport of glucose is an example of this action. The enzyme sodium/potassium-dependent adenosine triphosphatase (Na+/K+-ATPase), in the cell membrane, supplies the energy for the pump.
• Engulfing pinocytosis: At times, fluid and nutrient molecules are absorbed by pinocytosis. When the nutrient particle touches the absorbing cell membrane, the membrane dips inward around the nutrient, surrounds it to form a vacuole, and then engulfs it. The nutrient is then conveyed through the cell cytoplasm and discharged into the circulation. Smaller whole proteins and neutral fat droplets can be absorbed through pinocytosis (Figure 2-10).

Routes of Absorption
After their absorption, the water-soluble monosaccharides and amino acids enter directly into the portal blood and travel to the liver and other tissues. Fat, which is not water soluble, follows a different route. Fats packaged in a bile complex called a micelle (to be described in more detail in Chapter 4) are carried into the cells of the intestinal wall, where they are processed into human lipid compounds and joined with protein as a carrier. These lipoproteins, called chylomicrons, flow into the lymph, empty into the cisterna chyli (the central abdominal collecting vessel of the lymphatic system), travel upward into the chest through the thoracic duct, and finally flow into the venous blood at the left subclavian vein. The chylomicrons are rapidly cleared from the blood by a special fat enzyme—lipoprotein lipase.
Exceptions to this route of fat absorption are the short-chain fatty acids with 10 or fewer carbons. Because these short-chain fatty acids are water soluble, they can be absorbed directly into the blood, as are carbohydrate and protein breakdown products. However, most dietary fats are made of long-chain fatty acids that are not water soluble and must take the lymphatic route.
Colon (large intestine): Final absorption and waste elimination
Role in Absorption
Within a 24-hour period, approximately 1500 mL of the remaining food mass leaves the ileum, the last section of the small intestine, and enters the cecum, the pouch at the entrance to the colon. Passage is controlled by the ileocecal valve. Normally the valve remains closed, but each peristaltic wave relaxes the valve muscle, squirting a small amount of remaining chyme into the cecum. This action holds the food mass in the small intestine long enough to ensure maximal digestion and absorption. Nutrients and other materials, including electrolytes, minerals, vitamins, intestinal bacteria, and nondigestible residue, remain in the chyme delivered to the large intestine.
Water Absorption
The main task remaining for the colon is the absorption of water. The capacity of the colon to absorb water is vast, with a net daily maximum of 5 to 8 L.2 Normally, from 1.0 to 1.5 L is received from the ileum, and 95% of that is absorbed (see Table 2-4).
Much of the water in the chyme (350-400 mL) is absorbed in the first half of the colon. Only 100 to 150 mL remains to form the feces.2 Absorption of water in the colon is important in the regulation of water balance and the elimination of fecal waste. When the chyme first enters the colon, it is a semiliquid, but water absorption during passage changes it to the semisolid nature of normal feces.
The amount of water absorbed in the colon depends on motility and rate of passage. Poor motility and a slow passage rate, often related to low dietary fiber and low fecal mass, allow greater absorption of water, resulting in hard stools that are difficult to pass and constipation. Excess motility and too-rapid passage limit the absorption of water and important electrolytes, producing a high volume of loose, watery stool (diarrhea). Diarrhea can result from disease, microbial infection, as in foodborne illness, or large amounts of undigested sugar such as lactose that exert osmotic pressure and hold vast amounts of fluid. Severe or extended diarrhea leads to dehydration and serious loss of electrolytes.
Mineral Absorption
Sodium and other electrolytes are absorbed from the colon. Intestinal absorption exerts major control on body content of many minerals, and much of the dietary intake is unabsorbed and excreted in the feces. Up to 90% of the calcium and iron in the food we eat is not absorbed. The proportion of a mineral intake that is generally absorbed is an important aspect of nutrient balance and dietary evaluation.
Vitamin Absorption
Conditions in the gastrointestinal tract influence the absorption of vitamins. When gastric acid is lower than normal, vitamin B12 is not easily released from animal tissues and is lost in the feces (see the Evidence-Based Practice box). Conversely, colon bacteria synthesize vitamin K and biotin, which are actively absorbed and serve as a major source of the body’s supply.
Role of Intestinal Bacteria
At birth the colon is sterile, but intestinal bacteria soon become established. More than 500 different species of bacteria are found in the normal gastrointestinal tract, and intestinal contents may contain as many as 1 billion bacteria per gram.14 Various factors influence the composition of the microflora. Dietary intake of fiber or other nondigestible carbohydrates, immune responses favoring one group of bacteria over another, and the use of antibiotics affect the types and numbers of particular bacteria. Bacterial populations also differ along the length of the gastrointestinal tract based on differences in structure and pH.15 Many bacteria ingested with food cannot survive the extreme acid environment in the stomach.
Intestinal bacteria make up approximately one third of fecal weight2 and affect the color and odor of the stool. The customary brown color comes from bile pigments produced by colon bacteria from bilirubin. Thus, when bile flow is hindered, the feces may become clay colored or white. The characteristic odor of the stool comes from amines, especially indole and skatole, formed by the action of bacterial enzymes on amino acids.
Intestinal microflora have many roles. Particular microorganisms produce bothersome gas or increase the risk of gastrointestinal disease. Other species make positive contributions to health (Box 2-1).
Excessive Gas Production
Intestinal bacteria are the major contributors to gas production, including carbon dioxide (CO2), molecular hydrogen (H2), methane, and sometimes hydrogen sulfide. Gas formation is a normal occurrence and, though harmless, is distressful when it causes pain or embarrassment. Intestinal gas, or flatus, can be exaggerated as a result of specific foods or physiologic circumstances in the person eating them.
In general, gas is produced by the bacterial fermentation of undigested or incompletely absorbed carbohydrate. Humans lack the enzymes necessary to digest the oligosaccharides raffinose and stachyose in legumes that cause the intestinal gas associated with these foods. Certain starches and fibrous materials in whole grains, fruits, and vegetables are resistant to pancreatic amylase and are not broken down and absorbed. People should be encouraged to increase their intakes of fiber gradually to allow a more comfortable adjustment and prevent gastrointestinal distress.
Excessive gas has social implications. CO2, H2, and methane are odorless, but hydrogen sulfide carries a striking odor. Hydrogen sulfide most often arises from cruciferous vegetables (cabbage, cauliflower, or broccoli) or large amounts of beer, all high in sulfur. Various over-the-counter products claim to reduce the formation of gas or eliminate gaseous odors, but all of these products have limitations. Persons should check with their physician before using such preparations.16 (See the Complementary and Alternative Medicine [CAM] box, “Bismuth and Certain Herbs: A Dangerous Combination” for cautions.)
Waste Elimination
Fully formed and ready for elimination, normal feces contain approximately 75% water and 25% solids.2 The solids include fiber, bacteria, inorganic matter such as minerals, a small amount of fat and its derivatives, some mucus, and sloughed-off mucosal cells.
 Complementary and Alternative Medicine (CAM)
Complementary and Alternative Medicine (CAM)
Bismuth and Certain Herbs: A Dangerous Combination
Bismuth-containing medications such as Pepto-Bismol are sometimes used to ease gas and bloating. Bismuth also binds with the odor-causing sulfur compounds in intestinal gas and helps reduce embarrassment. However, when combined with ginkgo, garlic, ginger, or ginseng, bismuth can have serious side effects. Working together bismuth and these herbs act as anticoagulants.
Bonci L: American Dietetic Association guide to better digestion, Hoboken, NJ, 2003, John Wiley & Sons.
The mass of food residue now slows its passage. Approximately 4 hours after a meal is eaten, it enters the cecum, having traveled the entire length of the small intestine, 630 to 660 cm (21-22 feet). Approximately 8 hours later, it reaches the sigmoid colon, having traveled an additional 90 cm (3 feet) through the large intestine. In the sigmoid colon, the residue descends still more slowly toward its final destination, the rectum.
The rectum begins at the end of the large intestine immediately past the descending colon and ends at the anus. Feces are usually stored in the descending colon; however, when it becomes full, feces pass into the rectum, resulting in the urge to defecate. Anal sphincters under voluntary control regulate the elimination of feces from the body. As much as 25% of a meal may remain in the rectum for up to 72 hours.
Gastrointestinal function and clinical applications
Chronic Gastrointestinal Distress
Most of the time the gastrointestinal tract is a smoothly working system that allows us to enjoy the food we eat while effectively handling digestion, absorption, and the elimination of waste. However, for some people, abdominal pain, nausea, vomiting, or diarrhea is a regular occurrence, and no specific biochemical or structural explanation can be found.17–18 Mental and emotional stress, depression, various prescription medications, foods eaten, and chronic disease all influence gastrointestinal function. Some populations appear to be particularly vulnerable to chronic gastrointestinal distress (see the Focus on Culture box, “Digestive Distress in African Americans and Hispanic Americans”).
We need to listen carefully when people tell us about gastrointestinal problems that interfere with eating and their enjoyment of food.19 Health education for self-care should point to the dangers of over-the-counter supplements such as food enzymes claiming to enhance digestion, inappropriate laxatives, or ill-advised procedures such as colonic irrigation. Chronic digestive problems demand medical assessment and intervention.
 Focus on Culture
Focus on CultureDigestive Distress in African Americans and Hispanic Americans
Chronic digestive distress can influence food choices, nutrient intake, and general health. African Americans and Hispanic Americans may be at greater risk than other groups. When adults were asked to complete a questionnaire asking about abdominal pain and fullness, nausea, vomiting, or gastric reflux, almost one third of the participants indicated at least one of these problems.1 The majority reporting problems were African Americans, and on follow-up, many were found to have previously undiagnosed gastric ulcers, duodenal ulcers, or damage to their esophagus. African Americans and Hispanic Americans are more likely than other groups to be infected with Helicobacter pylori, the microorganism known to have a role in development of ulcers, as well as other digestive disorders.2–3 Infection with H. pylori relates to socioeconomic rather than genetic factors, and infection rates are higher than normal in both children and adults from families with lower incomes, reduced access to health care facilities, and living in a rural environment. This burden of infection may contribute to the increased prevalence of dyspepsia and digestive disease in these groups.
References
1. Shaib, Y., El-Serag, H. B. The prevalence and risk factors of functional dyspepsia in a multiethnic population in the United States. Am J Gastroenterol. 2004; 99:2210.
2. Kruszon-Moran, D., McQuillan, G. M.Seroprevalence of six infectious diseases among adults in the United States by race/ethnicity: data from the third National Health and Nutrition Examination Survey, 1988-94, advance data, vital and health statistics, No. 352. Hyattsville, Md: U.S. Department of Health and Human Services, 2005.
3. Malaty, H. M. Epidemiology of Helicobacter pylori infection. Best Pract Res Clin Gastroenterol. 2007; 21(2):205.
Lactose Intolerance
Lactose intolerance is a digestive problem facing 70%20 of the world’s population—as many as 22% of Caucasians, 80% of African Americans and Latinos, and almost 100% of Asians.13 Those with lactose intolerance may have symptoms after taking in as little as 6 g or as much as 12 to 18 g of lactose (1 cup of milk contains 12 g of lactose).13 This problem stems from a deficiency of lactase, the digestive enzyme in the microvilli of the small intestine that breaks lactose into its simple sugars—glucose and galactose. When undigested lactose remains in the small intestine and colon, it absorbs large amounts of water and is fermented by resident bacteria, producing diarrhea, bloating, and gas.
Congenital intolerance to lactose is rare; infants usually produce enough lactase to digest the large amounts of lactose in mother’s milk. However, loss of lactase activity beyond early childhood is the normal physiologic pattern, with relatively few adults retaining their former capacity for lactose digestion. Before the domestication of cows, lactose was not present in the diet after weaning, therefore this enzyme was no longer needed. The introduction of a dairy-based culture in particular geographic regions 10,000 years ago likely contributed to the retention of lactase activity among certain European groups.13 Most populations lose more than 70% of their lactase activity within 3 to 4 years of weaning, although Caucasians may retain high lactase activity through adolescence.20
Other conditions can cause or worsen symptoms after eating lactose-containing foods. Irritable bowel syndrome, celiac disease, cystic fibrosis, or other disorders that damages the intestinal mucosa can interfere with the digestion of lactose, and medical diagnosis is often needed to confirm the problem. Viral infections can cause temporary lactose intolerance.
Distinguishing between lactose maldigestion and lactose intolerance is important. Individuals with some degree of lactose maldigestion may not necessarily exhibit symptoms characteristic of lactose intolerance. When lactose maldigesters were given a lactose-containing beverage as compared with a similar beverage that looked and tasted the same but had the lactose removed, their responses were similar, suggesting that lactose is not a major cause of symptoms when consumed in the customary dietary portion of one cup of milk.21 Most people with problems digesting lactose do not need to follow a totally lactose-free diet, although milk may be limited in favor of other dairy foods20 or lactose-containing foods gradually added to the diet. Maldigesting lactose does not mean that you are allergic to milk or dairy foods. A true milk allergy is caused by the protein in milk, not the lactose.16
To increase their intakes of calcium and vitamin D, people with lactose maldigestion might begin to include dairy foods in their diet in the following ways16:
• Add dairy foods gradually: Begin with a small amount of one dairy food each day, one quarter cup of milk or one half ounce of cheese; include only one lactose-containing food per meal. (See Box 2-2 for food lactose content.)
BOX 2-2 Food Sources of Lactose






Images copyright 2006 JupiterImages Corporation.
Data from Bonci L: American Dietetic Association guide to better digestion, Hoboken, NJ, 2003, John Wiley & Sons.
• Include lactose-containing foods with a meal or snack: This combination slows the movement of lactose into the intestine and may reduce discomfort.
• Choose dairy foods low in lactose: Use lactose-free or lactose-reduced milk. (Acidophilus milk is not lactose free.) Add lactase enzyme drops (Lactaid or Dairy Ease) to milk to lower the lactose. Lactase tablets taken right before eating dairy foods can reduce discomfort. Aged cheeses such as cheddar or Swiss are lower in lactose than cheese spreads or other processed cheese.
Lactose is also found in nondairy foods that have milk as an ingredient. Breads and other baked products, some ready-to-eat breakfast cereals, pancake and cookie mixes, instant potatoes, cream soups, hot dogs, and luncheon meats may contain lactose. Read the Nutrition Facts label, and look for the word milk or whey. (See Chapter 7 for food sources of calcium for persons who cannot tolerate dairy foods.)
Health promotion
Prebiotics and Probiotics
Many people have the perception that all microbes are harmful, as we read reports of antibiotic-resistant virus, outbreaks of foodborne illness, or advertisements for antibacterial soap. Nonetheless, in the nineteenth century, Elie Metchnikoff speculated that Bulgarian peasants enjoyed long lives because of their use of fermented milk that supplied microbes beneficial to colonic health. Today, we recognize that certain microbes found in the gastrointestinal tract contribute to human health and provide new tools for improving gastrointestinal function (see Box 2-1). These microbes and related food components have been termed prebiotics and probiotics based on their use and intestinal effects. Prebiotics are food ingredients that selectively stimulate the growth of one or more bacteria in the colon. Probiotics are live microorganisms that when administered in adequate amounts result in a health benefit to the host.22
Prebiotics
Prebiotics are indigestible carbohydrates, mostly polysaccharides, that promote the growth of the microbes Lactobacilli and Bifidobacteria. Any dietary component that reaches the colon intact is a potential prebiotic. Prebiotics used clinically include oligosaccharides (isolated from wheat, onions, bananas, garlic, soybeans, and artichokes), various fiber derivatives, and lactulose, a synthetic disaccharide.22–23
Increases in Lactobacilli and Bifidobacteria have various favorable actions, including:
• Increase in mineral absorption: Although most minerals are absorbed in the small intestine, the lower pH in the colon resulting from bacterial fermentation stimulates the absorption of zinc, calcium, magnesium, and iron still remaining in the food residue. These microbes break down phytate, an indigestible material found in plant foods that binds minerals and prevents their absorption.23–24
• Promotion of normal laxation: The fermenting action of bacteria on lactulose relieves constipation and helps avoid dependence on laxatives. Prebiotics can be added to tube feedings to prevent the common problem of diarrhea.22–23
• Protection against colon cancer: The fermentation products of healthful bacteria destroy cancer cells and toxic enzymes produced by harmful bacteria.23
Probiotics
The benefits of probiotics depend on the particular strain of bacteria and the active substances it produces. Lactic acid–producing bacteria have been used over the centuries to acidify and preserve foods. Common fermented foods include cultured milk and yogurt, cheese, distilled mash, pickled cabbages, and tempeh. Probiotic cultures are available from pharmaceutical companies for clinical use, although lactic acid–producing bacteria that survive the passage through the gastrointestinal tract and thrive in the colon can be obtained from commercially produced yogurt.22
Clinical applications of probiotics include the following:
• Diarrhea: Species of Lactobacillus are effective in treating infectious diarrhea in children and the diarrhea induced by antibiotics.22 Loss of the normal microflora through antibiotics allows the growth of harmful bacteria, and the resulting diarrhea adds days to the usual hospital stay.23
• Infant allergies: Poi, a probiotic made from the taro plant of the Pacific Islands, can be fed to babies allergic to cereals. When given to expectant mothers with a family history of cereal allergy, only one half of their infants showed signs of potential allergy.25
• Inflammatory bowel disease: Patients with ulcerative colitis and Crohn’s disease have abnormal patterns of intestinal bacteria that foster these diseases. Probiotics may assist in prevention or treatment.22
• Inhibition of H. pylori: This pathogenic bacterium attaches to the gastric mucosa and is implicated in the development of peptic ulcer, gastric cancer, and chronic gastritis. Probiotics seem to inhibit its growth and prevent it from burrowing into the stomach lining.25
• Gastrointestinal immune response: Probiotics support the immune cells in the gastrointestinal tract that provide the first line of defense against pathogens entering the body.22
• Lactose intolerance: Probiotics in the colon help break down lactose, preventing symptoms associated with lactase deficiency.22
Although lactic acid–producing bacteria have been used successfully in food and therapeutic preparations, new strains must be determined safe before being sold as a supplement. Individuals with compromised immune function should not use probiotics without medical supervision. Contamination of the probiotic with a pathogenic strain or the passage of a probiotic microorganism across the intestinal mucosa and into the blood could lead to sepsis in an infant or adult lacking normal immune response.26 Currently, no legal definitions have been formulated for the terms prebiotic or probiotic, and as dietary supplements, their product labels are not reviewed for accuracy or efficacy by the U.S. Food and Drug Administration. Accurate information relating to the exact strain or species of bacteria, dosage required for effective intervention, safety of a particular product, or product shelf life can be difficult to obtain.22
Fermented dairy products are sources of both important nutrients and live bacteria, although the strain of microorganism and the level present may be unknown. Yogurt, cheese, and kefir (fermented milk prepared by adding kefir grains to cow’s or goat’s milk) all contain potentially beneficial live bacteria. Some yogurts currently sold in the United States contain not only starter cultures of bacteria, but also added Lactobacillus or Bifidobacterium to produce a probiotic effect, although label information as to the amount added is often limited. New commercial fermented milk and yogurt products marketed as functional foods containing known strains of bacteria at probiotic levels are also entering the market place.22
(See the Perspectives in Practice box, “Help Your Digestive System Work for You,” for ideas on maintaining optimum digestive function.)
 Perspectives in Practice
Perspectives in PracticeHelp Your Digestive System Work for You
Our personal eating habits can either support or stress the normal function of the digestive tract. Positive practices will maximize our enjoyment of food and help regulate our food intake.
• Do not gulp your food; allow time for the vapors to enter your sinus cavity and contribute to your sensation of taste.
• Wait 15 to 20 minutes before taking second helpings; when food moves from your stomach into your small intestine, it triggers feelings of satiety, and you may find that you do not need that extra spoonful.1
• Try to concentrate on pleasant thoughts or conversation while eating; emotional distress—fear, anger, worry—depresses the secretion of digestive enzymes and slows peristalsis, leading to gastrointestinal discomfort or upset.
• Enjoy the sight, smells, and anticipation of food as you prepare or serve your meals; these responses promote enzyme secretion and digestive function.
• The cells lining the gastrointestinal tract derive most of their energy from the food passing through and require a constant supply of nutrients to meet their high metabolic demands; try to eat about the same amount of food every day; do not gorge one day and fast the next.
Metabolism
After their absorption, nutrients are transported to the cells to be used for energy or to produce substances and tissues needed to sustain life. Cell metabolism encompasses the total spectrum of chemical changes associated with the final use of the individual nutrients.
Carbohydrate Metabolism
Although glucose is an immediate energy source for all body cells, it is also the preferred energy source for the brain and nervous system. Because glucose is so critical to life, its level in the blood is carefully regulated.
Sources of Blood Glucose
Both carbohydrate and noncarbohydrate molecules are sources of blood glucose, described as follows:
• Carbohydrate sources: Three carbohydrate substances can be converted to glucose: (1) dietary starches and sugars, (2) glycogen stored in the liver and muscle, and (3) products of carbohydrate metabolism such as lactic acid and pyruvic acid.
• Noncarbohydrate sources: Both protein and fat are indirect sources of glucose. Certain amino acids are called glucogenic amino acids because they can form glucose after their amino group (NH2+) is removed. Approximately 58% of the protein in a mixed diet is made of glucogenic amino acids. Thus more than one half of dietary protein might ultimately be used for energy if sufficient carbohydrate and fat were not available. After fats are broken down into fatty acids and glycerol, the glycerol portion (approximately 10% of the fat) can be converted to glycogen in the liver and then to glucose as needed. The formation of glucose from protein, glycerol, and carbohydrate metabolites is called gluconeogenesis.
Uses of Blood Glucose
Blood glucose is maintained within a normal range of 70 to 140 mg/dL (3.9-7.8 mmol/L) but is in constant flux as absorbed glucose is transported to cells for immediate use or removed from the circulation and stored as glycogen or fat. Blood glucose is used in three different ways:
• Energy production: The primary function of glucose is to supply energy to meet the body’s constant demand. An array of metabolic pathways requiring specific and successive enzymes accomplishes this task.
• Energy storage: Glucose is stored in two forms: (1) glycogen—held in limited amounts in liver and muscle, and (2) fat (adipose tissue)—the storage form for all excess glucose after energy demands have been met. Only a small supply of glycogen exists at any one time, and it turns over rapidly. Fat can be stored in unlimited amounts in adipose tissue and provides long-term energy stores.
• Glucose products: Small amounts of glucose are used to produce various carbohydrate compounds with important roles in body metabolism. Examples include deoxyribonucleic acid (DNA) and ribonucleic acid (RNA), galactose, and certain amino acids.
These sources and uses of glucose act as checks and balances to maintain normal blood glucose levels, adding or removing glucose as needed.
Hormonal Controls
Several hormones directly and indirectly influence glucose metabolism and regulate blood glucose levels.
• Blood glucose–lowering hormone. Only one hormone—insulin—lowers blood glucose. Insulin is produced by the beta cells in the pancreas. These cells are scattered in clusters, forming “islands” in the pancreas—giving rise to the name islets of Langerhans after the German scientist who first discovered them. Insulin lowers blood glucose by the following actions:
• Glycogenesis stimulates the conversion of glucose to glycogen in the liver for energy reserve.
• Lipogenesis stimulates the conversion of glucose to fat for storage in adipose tissue.
• Cell permeability increases, allowing more glucose to enter the cell and be oxidized for energy.
• Blood glucose–raising hormones. The following hormones effectively raise blood glucose levels:
• Glucagon produced by the alpha cells in the pancreas acts in opposition to insulin, increasing the breakdown of liver glycogen to glucose and maintaining blood glucose levels during fasting or sleep hours. (The hydrolysis of liver glycogen to yield glucose is called glycogenolysis.)
• Somatostatin, produced in the delta cells of the pancreas and in the hypothalamus, suppresses insulin and glucagon and acts as a general modulator of related metabolic activities.
• Steroid hormones, secreted by the adrenal cortex, release glucose-forming carbon units from protein and oppose the actions of insulin.
• Epinephrine, originating from the adrenal medulla, stimulates the breakdown of liver glycogen and quick release of glucose.
• Growth hormone (GH) and adrenocorticotropic hormone (ACTH), released from the anterior pituitary gland, oppose the actions of insulin.
• Thyroxine, originating in the thyroid gland, increases the rate of insulin breakdown, increases glucose absorption from the small intestine, and liberates epinephrine.
Lipid Metabolism
Lipid Synthesis and Breakdown
Two organ tissues—(1) liver and (2) adipose tissue—form a balanced axis of lipid metabolism. Both tissues participate in lipid synthesis and breakdown. The fatty acids released from lipids are used by body cells as concentrated fuel for energy.
Lipoproteins
Lipid-protein complexes are the transport form of lipids in the blood. An excess of blood lipoproteins produces a clinical condition called hyperlipoproteinemia. Lipoproteins are produced (1) in the intestinal wall after the initial absorption of dietary lipids and (2) in the liver for constant recirculation to and from cells.
Hormonal Controls
Because lipid and carbohydrate metabolism are interrelated, the same hormones are involved, as follows:
• GH, ACTH, and thyroid-stimulating hormone (TSH), all from the pituitary gland, increase the release of free fatty acids from stored lipids when energy demands are imposed.
• Cortisol and corticosterone, from the adrenal gland, release free fatty acids.
• Epinephrine and norepinephrine stimulate the breakdown of lipids and release of free fatty acids.
• Insulin from the pancreas promotes lipid synthesis and storage, whereas glucagon has the opposite effect of breaking down lipid stores to release free fatty acids.
• Thyroxine from the thyroid gland stimulates release of free fatty acids and lowers blood cholesterol levels.
When fatty acids from the gastrointestinal tract are delivered to the liver and muscle in larger amounts than needed for immediate energy or synthesis of important molecules, the hormone insulin promotes the formation of triglycerides for storage in the adipose tissue. In situations of prolonged physical activity, starvation, physical stress, or other circumstances requiring energy beyond what can be supplied by available glycogen, these triglycerides are broken down and their fatty acids released. Free fatty acids are delivered to the liver to be packaged in lipoproteins for transport to cells for meeting energy needs or for redeposition in adipose tissue. Muscle cells, including the heart muscle, depend on free fatty acids for their ongoing energy needs.
Protein Metabolism
Anabolism (Tissue Building)
Protein metabolism centers on the critical balance between anabolism (tissue building) and catabolism (tissue breakdown). The process of anabolism builds tissue through the synthesis of new protein. The making of new protein is governed by a definite pattern or “blueprint” provided by DNA in the cell nucleus that calls for specific amino acids. Specific enzymes and coenzymes along with certain hormones—GH, gonadotropins, and thyroxine—control and stimulate the building of tissue protein.
Catabolism (Tissue Breakdown)
Amino acids released by tissue breakdown are reused for making new proteins or, if not needed for protein synthesis, are further broken down and used for other purposes. The breakdown of these amino acids yields two parts: (1) the nitrogen-containing group and (2) the remaining nonnitrogen residue, described as follows:
1. Nitrogen group: The nitrogen portion is split off first, a process called deamination. This nitrogen can be converted to ammonia and excreted in the urine or retained for use in making other nitrogen compounds.
2. Nonnitrogen residue: The nonnitrogen residues are called keto acids. They can be used to form either carbohydrates or fats. With the addition of a nitrogen group, they can form a new amino acid.
Cell enzymes and coenzymes along with hormones control tissue breakdown. In health, a dynamic equilibrium exists between anabolism and catabolism that sustains growth and maintains sound tissue.
Metabolic Interrelationships
Each of the chemical reactions in body metabolism is purposeful, and all are interdependent. They are designed to fill two essential needs: produce energy and support growth and maintenance of healthy tissue. The controlling agents necessary for these reactions to proceed in an orderly manner are the cell enzymes, their coenzymes (that often include vitamins and minerals), and special hormones. Overall, human metabolism is an exciting biochemical process designed to develop, sustain, and protect our most precious possession—life itself.
To sum up
The process of digestion breaks down food to release and convert the nutrients to simple forms that the body can use and ensures their passage across the intestinal wall and into the circulatory system for delivery to the tissues. Digestion involves two types of activities: mechanical and chemical. Muscle action breaks down food through mixing and churning motions and moves the food mass along the gastrointestinal tract. The chemical activity of gastrointestinal secretions breaks down food into smaller and smaller components for absorption. Nutrients move across the intestinal wall by the process of diffusion, facilitated diffusion, active transport, or pinocytosis. Monosaccharides and amino acids are water soluble and pass from the mucosal cells of the small intestine into the portal blood. Long-chain fatty acids must be packaged in lipid-protein complexes that enter the lymph and then pass through the thoracic duct into the general circulation. New research is helping us learn more about the important roles of intestinal bacteria and their overall contribution to gastrointestinal health. The day-to-day function of the gastrointestinal tract, often taken for granted, represents a highly coordinated and efficient body system. The breakdown products released through digestion—glucose, amino acids, and fatty acids—participate in multiple metabolic pathways under hormonal and enzymatic control that provide energy and produce substances and tissues necessary for life and well-being.
Questions for review
1. List the muscle types and their locations in the walls of the gastrointestinal tract. What types of motions or movements do they provide in each section of the tract? What is the role of the intramural nerve plexus in controlling gastrointestinal muscle function?
2. You are working with an older adult who suffered a stroke resulting in damage to the nerves in the swallowing center of the hypothalamus. What are the implications for his food intake and nutritional well-being?
3. Make a chart describing the chemical actions of digestion that occur in each section of the gastrointestinal tract. List across the top of the page the mouth, esophagus, stomach, small intestine, and colon. What are (a) the enzymes or fluids that act on the food mass in that location, (b) the sources of those enzymes or fluids, (c) the factors that stimulate their release, and (d) the factors that inhibit their activity?
4. Describe what happens in absorption. What are the four mechanisms by which nutrients are absorbed from the small intestine?
5. You have just eaten a lunch that included a hamburger on a whole-wheat bun, a glass of low-fat milk, and a bunch of grapes. Trace the digestion and final use of each of the macronutrients present in your lunch. What are (a) the enzymes, locations, and breakdown products formed in the complete digestion of these foods; (b) the routes taken by the breakdown products after absorption; and (c) one possible body use for each breakdown product?
6. Visit a local supermarket or drug store and examine three over-the-counter medications that claim to (a) reduce stomach acid or (b) alleviate intestinal gas. Make a table that includes each product and list the active ingredients on the product label. Visit the National Library of Medicine/National Institutes of Health MedlinePlus website at www.nlm.nih.gov/medlineplus/druginformation.html or other drug index to identify the specific actions of the active ingredients. What is the mechanism by which each active ingredient is believed to bring about the desired effect? What is the relative safety of this drug based on the possible side effects or contraindications?
7. How might long-term use of an antibiotic affect the overall function of the gastrointestinal tract? Explain.
8. Describe the complementary roles of insulin and glucagon in regulating blood glucose levels. What are the effects of these hormones over the course of a day for an individual who eats breakfast at 7:00 am, lunch at 12:00 pm, and dinner at 6:00 pm with no snacks?