Evidence-Based Practice
1. Differentiate between research utilization and evidence-based practice.
2. Review the nurse’s role in the implementation of evidence-based practice.
3. Identify the hierarchy of evidence.
4. Discuss the critical appraisal process in evaluating evidence.
Effects of an intervention are examined by comparing the treatment group with the nontreatment group; patients are placed in treatment or nontreatment group through random sampling
Same as a randomized clinical trial but patient placement in treatment or nontreatment group depends on study variables, with not every individual having an opportunity for selection
MEDICAL MYTHS AND TRUTHS
Two sentinel publications by the Institute of Medicine—To Err Is Human and Crossing the Quality Chasm (IOM, 2000; IOM, 2001)—drew attention to quality issues in U.S. health care (see Chapter 10). A major theme of both reports was that although the technology of health care had advanced at lightning speed, the delivery system had not advanced, causing potentially lethal situations in health care. One of the most common situations seen was the increased rate of hospital-acquired infections, and one of the proposed solutions to the improvement of care was the use of evidence-based decision making in health care.
Evidence-based practice requires a shift from the traditional paradigm of clinical practice grounded in pathophysiology and clinical experience to one of the integration of best practice and scientific evidence. This paradigm shift allows for the continuous improvement of practice and a creation of environments that stimulate innovation.
As a new nurse, there will be many times that you ask yourself, “Why do we do it this way?” Or “There must be a better way to do this.” For answers to these questions, you must look to the evidence. What does the evidence tell you? What is the best practice, or what is the best way to do this? Some of our standard practices are “sacred cows,” meaning they represent “the way it has always been done.” For instance, does every patient admitted to your unit need their temperature taken at 7 am? Perhaps not, but that is just the “way that we do it” or perhaps that was the “best practice” when the policy was implemented. But what does the evidence (scientific data) tell us today? As nurses, it is important that you remain current within your practice area, because the evidence is always changing and growing. Estabrooks (1998) and Pravikoff et al. (2005) found that knowledge sources most frequently used by nurses were school experiences and colleague experience. Assuming that this is the case, a nurse with 15 years of experience may be using “evidence” that is 15 years out of date, and this experienced nurse who is mentoring new nurses may be fostering practice in the new nurse that is 15 years out of date. A colleague of this author once said that “health care was a long history of tradition unimpeded by progress”—the move to evidence-based practice is changing this.
EXAMPLES OF SOME MEDICAL MYTHS
Myth: Patients with musculoskeletal back pain respond best to bed rest followed by a specialized back exercise program (myths from Flaherty, 2007).
• Bed rest is not an effective treatment for acute low back pain and may delay recovery. Current advice is to stay active and to continue ordinary activities, which results in a faster return to work, less chronic disability, and fewer recurrent problems (Waddell, 1997).
• Among patients with acute low back pain, continuing ordinary activities within the limits permitted by the pain leads to more rapid recovery than either bed rest or back-mobilizing exercises (Malmivaara, 1995).
Myth: “Figure-of-eight” dressings or similar appliances are the preferred treatment for clavicle fractures.
• No statistical difference was found in the speed of recovery when clavicle fractures were treated by either a figure-of-eight bandage or a broad arm sling (Stanley & Norris, 1988).
• Treatment with a simple sling caused less discomfort and perhaps fewer complications than with the figure-of-eight bandage. The functional and cosmetic results of the two methods of treatment were identical and alignment of the healed fractures was unchanged from the initial displacement (Andersen et al., 1987).
Myth: Bed rest is a useful adjunctive therapy.
Truth: A meta-analysis of 39 studies of the use of bed rest versus early mobilization for prevention and treatment of a variety of medical conditions showed bed rest to be at best not beneficial and at worst harmful (Allen, 1999).
Myth: Rectal temperature can be accurately estimated by adding 1° C to the temperature measured at the axilla.
Truth: In children and young adults, temperature measured at the axilla does not agree sufficiently with temperature measured at the rectum to be relied on in clinical situations where accurate measurement is important (Craig, 2000).
DECISION-MAKING MODEL
Evidence-based practice is a decision-making model based on the “conscientious, explicit and judicious use of current best practice in making decisions about the care of individual or groups of patients” (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). “This practice requires the integration of individual clinical expertise with the best available external clinical evidence from systematic research, available resources, and our patient’s unique values and circumstances” (Sackett et al., 1996). This definition requires nurses to carefully and thoroughly integrate evidence into their practice. But how do they do this?
This new paradigm of evidence-based practice requires the development of a clinical inquiry approach. Nurses must ask themselves the following questions and not blindly accept standard practice (Salmon, 2007):
RESEARCH UTILIZATION
Evidence-based practice differs from research utilization. Research utilization is the process of using research-generated knowledge to make an impact on or a change in existing practices (Burns and Grove, 2007). Evidence-based practice requires synthesizing research study findings to determine best research evidence. Research evidence is a synthesis of high-quality, relevant studies to form a body of empirical knowledge for the selected area of practice. The best research evidence is then integrated with clinical expertise and patient values and needs to deliver quality, cost-effective care (Sackett et al., 2000).
QUESTION FORMULATION
The first thing that you will need to do is to formulate the question. As nurses, we make numerous decisions when caring for our patients. As we make these decisions, we are influenced by a number of factors (Craig & Smyth, 2002):
Up-to-date, valid evidence needs to be integrated with these factors to maximize the likelihood of what we want to happen (the outcome). The more explicit the question, the easier it is to run searches through the multiple electronic databases available to nurses (CINAHL, MEDLINE, Cochrane Library). For example, you are interested in determining best practice for change-of-shift reports. If you enter “end-of-shift report” into the search line, you will receive 56 references. If you narrow the search to within the past 5 years, the number of references is cut to 32. A focused question makes your “search strategy” much easier. It is very helpful for any nurse working in a hospital to develop a good relationship with the hospital librarian; he or she will assist you in the gathering of research evidence.
RELIABLE EVIDENCE
Once you have focused your question, you need to select the best evidence. Just because something has been published, albeit in print or on the Internet, does not mean that it is a valid source of evidence. You must first determine the reliability of the source. Your librarian will assist you in this. A research study on urinary catheters funded by the company that makes urinary catheters may not be the most reliable source of evidence; a study supporting their catheter is in the company’s best interest. The first question in your critical appraisal of the evidence is whether this study is good enough to use the findings. You will be attempting to determine if the quality of the study that you are reading is good enough for you to use the results in the design of a nursing protocol. You would need to look at the research design, the sample, and the sample size. Obviously, results from a study directed at children may not be appropriate in the design of a protocol addressed at adults. Also, a study with a sample size of 4 will not carry as much strength as will a study with a sample size of 1000. Some research designs are more powerful than others. The fact that some studies are more powerful than others has given rise to the hierarchy of evidence (Peto, 1993). The hierarchy of evidence for questions about effectiveness of an intervention follows (Polit & Beck, 2008, p. 31):
CRITICAL APPRAISAL
The next question to ask in your critical appraisal is whether the findings are applicable to your setting. The patients used in a study will never be identical to yours but there may be similarities. The following questions can be asked to determine applicability of the study to your practice area:
• Is it clear what the study is about?
• Is the sample/context adequately described?
• Are my patients/contexts so different that the results will not apply?
• Is the intervention available, or is the change possible in my setting?
• Do the benefits of the change for my patient/context outweigh the costs?
• Are the patients’ values and preferences satisfied by change?
Part of this question will be to ask what these results mean for your patients.
POPULATION, INTERVENTION, COMPARISON INTERVENTION, OUTCOME (PICO)
A framework for formulating evidence-based questions is PICO (Population, Intervention, Comparison Intervention, Outcome). Box 4-1 describes the focus of the PICO question.
In health care organizations, there may be many triggers that initiate the need for change. They can be data driven, resulting from performance review data, risk management data, benchmarking data, and financial data. Or they can be knowledge driven, resulting from new research findings, change in regulatory guidelines and standards, or questions from practitioners.
As a nurse manager, your role will be in the promotion and implementation of evidence-based practice in your organization. The Iowa Model of Evidence-Based Practice provides direction for the development of evidence-based practice in a clinical facility (Figure 4-1).
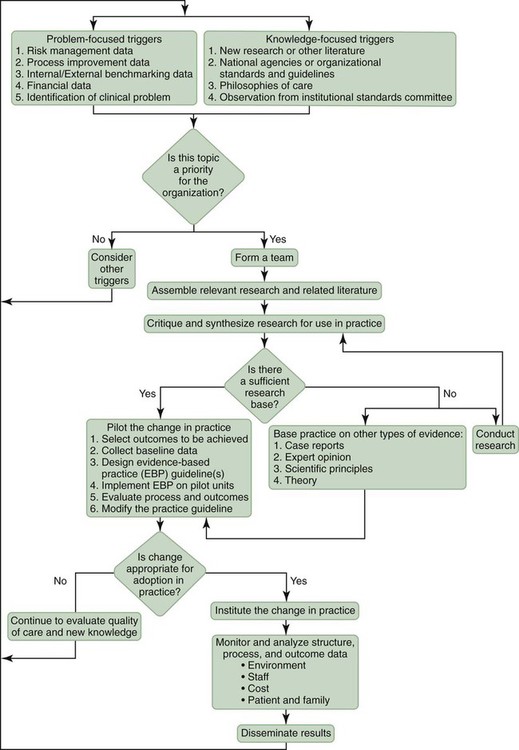
This model of evidence-based practice can be used as a guide for implementing a research-based protocol. The steps in this model are to:
SUMMARY
As a new nurse entering the profession, it is imperative that you maintain currency within your profession. Here are some strategies for using research evidence in your own practice:
• Read widely and critically—professionally accountable nurses keep abreast of their practice by reading journals relating to their practice.
• Join a professional organization related to your specialty—many innovations in practice and best practices are shared through professional organizations.
• Attend professional conferences and continuing education seminars.
 CLINICAL CORNER
CLINICAL CORNER
Evidence-Based Practice Changes
The best evidence in patient care often travels a hard, sometimes circuitous, journey before becoming embedded into the practice of nursing care and ritualized. In acknowledging this, our hospital’s Nurse Research Council attempts to provide an open forum for bringing evidence-based practice to the council membership for review and to make decisions on implementation, with the final goal of streamlining the process of adoption to dissemination within our facility.
New research and evidence-based practice guidelines issued by national organizations frequently provide triggers to question our current policy and practice. This was just the scenario in June 2008, when a Nurse Research Council member brought an article to the scheduled meeting about evidence-based guidelines for enteral feeding. It was noted in the peer-reviewed article that feeding tube placement should be confirmed only by radiography. This generated a lively discussion within the council about what was our current practice and what was being put forth as the best practice. Fueled by the substantiated findings that 1.4% to 27% of hospitalized patients have enteral tube placements inadvertently placed in the lung, we pursued a further literature search of the evidence and investigated our own standard of practice (Marderstein, Simmons, and Ochoa, 2004).
In our institution, if a certain procedure is already outlined in an approved nursing reference manual, then that manual serves as the guideline for that particular standard of care or procedure. If there is no standard of reference for a related practice, then a policy or procedure will be developed and written. We discovered that the hospital had no specific written policy for insertion and confirmation of placement of enteral feeding tubes, so we looked to our approved nursing reference manuals that we subscribed to—the Lippincott Manual of Nursing Practice, 8th Edition, and the AACN Procedure Manual for Critical Care, published in 2005. Neither approved nursing reference manual endorsed radiographic confirmation as the only reliable method to confirm enteral feeding tube placement.
The Nurse Research Council members then spent the next month searching the literature to lend strength to the evidence cited in the one peer-reviewed journal article.
In September 2008, our council met and proceeded to assemble the relevant findings from our literature search. We critiqued the literature, synopsized the findings, and weighed the evidence. Would it be sufficient to endorse a change in practice? Yes! We discovered that no other method, including air insufflation, visual inspection, or testing of aspirate for pH or capnography, proved to be a 100% reliable in confirming correct enteral feeding tube placement. Recognizing that requiring the hospital’s neonate population to have radiographic confirmation every time a feeding tube is placed would result in multiple x-ray exposures on a daily basis for an infant, our recommendation for implementing the evidence-based practice change was only for our adult patient population.
Our recommendation for radiographic confirmation would require the availability of a physician to read a radiograph 24 hours a day, 7 days a week. Being a nonteaching hospital, without residents or interns, we worked with our radiology department and director of medical administration to ensure that we had the resources to support our proposed practice change. At first, the director was not appreciative of the proposed practice change until he was duly convinced by the presentation and weight of the evidence from our literature search. At the request of the director, we commenced to poll our entire nursing staff as to how many times they inserted enteral feedings tubes to evaluate the feasibility of using the house physician’s time to provide the necessary radiographic confirmation. The information from the informal survey was that, on average, between the medical-surgical units and the critical care units, tubes were inserted two to three times a week by nursing staff, certainly not an overwhelming number that would monopolize the time of the house physician staff. With the endorsement of the director of medical administration in December 2008, we set out to develop a policy that would include evidence-based guidelines in the placement and confirmation of enteral feeding tubes in adult patients that would ensure the resource to read radiographs whenever necessary. The recommended evidence-based practice change will be finalized and approved at the necessary committee levels following our shared governance philosophy that we adopted at our hospital, which states that nursing governs its own practice and makes autonomous decisions to provide the best care to our patients.
 EVIDENCE-BASED PRACTICE
EVIDENCE-BASED PRACTICE
Saline Versus Heparin Flushes
Adapted from Building an evidence-based practice. In Burns, N., Grove, S. K. (2007). Understanding nursing research: building an evidence-based practice (4th ed.) (pp. 515-517). St. Louis, MO: Saunders Elsevier.
Research Example: Synthesis of Research
Goode and colleagues (1991) conducted a meta-analysis “to estimate the effects of heparin flush and saline flush solutions on maintaining patency, preventing phlebitis, and increasing duration of peripheral heparin locks [peripheral venous catheters]” (p. 324). The meta-analysis was conducted on 17 high-quality studies, which the investigators summarized in a table (Table 14-A). The total sample size for the 17 studies was 4153; the study settings included a variety of medical-surgical and critical care units. The small effect size values (most are less than 0.20) for clotting, phlebitis, and duration indicate that saline flush is as effective as heparin flush in maintaining peripheral venous catheters. Goode and colleagues summarized current knowledge on the use of saline versus heparin flushes:
Table 14-A
STUDIES INCLUDED IN THE META-ANALYSIS
| Study | N | Subject | Assignment | Heparin Dose (U/ml) | Clotting Effect Size (dc) | Phlebitis Effect Size (dp) | Duration Effect Size (dd) |
| Ashton et al., 1990 | 16 expc | Adult critical care | Random, double blind | 10 | 0.3590 | −0.1230 | |
| 16 conc | |||||||
| 13 expp | |||||||
| 14 conp | |||||||
| Barrett & Lester, 1990 | 59 experimental | Adult med-surg patients | Nonrandom double-blind | 10 | −0.1068 | −0.4718 | |
| 50 control | |||||||
| Craig & Anderson, 1991 | 129 exp | Adult med-surg patients | Random double-blind crossover | 10 | 0.0095 | −0.0586 | |
| 145 con | |||||||
| Cyganski et al., 1987 | 225 exp | Adult med-surg patients | Nonrandom | 10 | 0.2510 | ||
| 196 con | |||||||
| Donham & Denning, 1987 | 8 expc | Adult critical care | Random, double blind | 10 | 0.0000 | 0.0548 | |
| 4 conc | |||||||
| 7 expp | |||||||
| 5 conp | |||||||
| Dunn & Lenihan, 1987 | 61 experimental | Adult patients | Nonrandom | 50 | −0.2057 | −0.2258 | |
| 51 control | |||||||
| Epperson, 1984 | 138 exp | Adult med-surg patients | Random, double blind | 10 | −0.1176 | ||
| 120 con 100 | −0.1232 | ||||||
| 138 exp | |||||||
| 154 con | |||||||
| Garrelts et al., 1989 | 131 exp | Adult med-surg patients | Random, double blind | 10 | −0.1773 | 0.1057 | 0.2753 |
| 173 con | |||||||
| Hamilton et al., 1988 | 137 exp | Adult patients | Random, double blind | 10 | −0.0850 | −0.1819 | −0.0604 |
| 170 con | |||||||
| Holford et al., 1977 | 39 experimental | Young adult volunteers | Nonrandom, double blind | 3.3, 10, 16.5, 100, 132 | 0.6545 | ||
| 140 control | |||||||
| Kasparek et al., 1988 | 49 exp | Adult med patients | Random, double blind | 10 | 0.3670 | −0.5430 | |
| 50 con | |||||||
| Lombardi et al., 1988 | 34 experimental | Pediatric patients (4 wk to 18 yr) | Nonrandom, sequential double blind | 10 | −0.2324 | 0.0000 | |
| 40 control | |||||||
| Miracle et al., 1989 | 167 exp | Adult med-surg patients | Nonrandom | 100 | −0.0042 | ||
| 441 con | |||||||
| Shearer, 1987 | 87 exp | Med-surg patients | Nonrandom | 10 | −0.1170 | −0.0977 | |
| 73 con | |||||||
| Spann, 1988 | 15 experimental | Adult telemetry step-down | Nonrandom, double blind | 10 | −0.3163 | −0.3252 | |
| 19 control | |||||||
| Taylor et al., 1989 | 369 exp | Adult med-surg patients | Nonrandom, time series | 10 | 0.0308 | 0.0288 | −0.1472 |
| 356 con | |||||||
| Tuten & Gueldner, 1991 | 43 exp | Adult med-surg patients | Nonrandom | 100 | 0.0000 | 0.1662 | |
| 71 con |

Modified from Goode, C. J., Titler, M., Rakel, B., Ones, D. S., Kleiber, C., Small, S., & Triolo, P. K. (1991). A meta-analysis of effects of heparin flush and saline flush: quality and cost implications. Nursing Research, 40(6), 325. Copyright © 1991, The American Journal of Nursing Company. Used with permission.
• It can be concluded that saline is as effective as heparin in maintaining patency, preventing phlebitis, and increasing duration in peripheral heparin locks. Quality of care can be enhanced by using saline as the flush solution, thereby eliminating problems associated with anticoagulant effects and drug incompatibilities. In addition, an estimated yearly savings of $109,100,000 to $218,200,000 U.S. health care dollars could be attained (Goode et al., 1991, p. 324).
These investigators also provided a table (Table 14-B) to present evidence of cost savings from changing to saline.
Table 14-B
ANNUAL COST SAVINGS FROM CHANGING TO SALINE
| Study | Cost Savings | Hospital |
| Craig & Anderson, 1991 | $40,000/yr | 525-bed tertiary care hospital |
| Dunn & Lenihan, 1987 | $19,000/yr | 530-bed private hospital |
| Goode et al., 1991 (this study) | $38,000/yr | 879-bed tertiary care hospital |
| Kasparek et al., 1988 | $19,000/yr | 350-bed private hospital |
| Lombardi et al., 1988 | $20,000–$25,000/yr | 52-bed pediatric unit |
| Schustek, 1984 | $20,000/yr | 391-bed private hospital |
| Taylor et al., 1989 | $30,000–$40,000/yr | 216-bed private hospital |
From Goode, C. J., Titler, M., Rakel, B., Ones, D. S., Kleiber, C., Small, S., & Triolo, P. K. (1991). A meta-analysis of effects of heparin flush and saline flush: quality and cost implications. Nursing Research, 40(6), 325. Copyright © 1991, The American Journal of Nursing Company. Used with permission.
Based on this review of the evidence, the following patient care protocol was developed.
Evidence-Based Protocol for Irrigating Peripheral Venous Catheters in Adults*
1. Review the medical order for irrigation of the peripheral venous catheter. Order should indicate that the catheter be irrigated with saline (0.9% sodium chloride) (Goode et al., 1991: Randolph et al., 1998).
2. Obtain the saline flush for irrigation from the hospital pharmacy (ASHP, 1994).
3. Wash hands with chlorhexidine, collect equipment for irrigating the peripheral venous catheter, and put on gloves.
4. Evaluate the peripheral venous catheter site every 8 hours for complications of phlebitis. The symptoms of phlebitis include the presence of erythema, tenderness, warmth, and a tender or palpable cord (Goode et al., 1991; Randolph et al., 1998).
5. Cleanse the peripheral venous catheter prior to irrigation with alcohol.
6. Flush the peripheral venous catheter with 1 ml for normal saline every 8 hours if no other medication is being given through the site (Goode et al., 1991; Randolph et al., 1998). Check the loss of catheter patency by noting any resistance in irrigating with 1 ml of saline or by the inability to administer saline solution within 30 seconds (Geritz, 1992; Shoaf & Oliver, 1992).
7. If a patient is receiving IV medication, administer 1 ml of saline, administer the medication, and follow with 1 ml of saline (Goode et al., 1991; Shoaf & Oliver, 1992).
8. Chart the date and time of the peripheral venous catheter irrigation and the appearance and patency of the catheter site.
As can be seen by this research example, the change in practice resulted from a critical analysis of research evidence, and the patient care protocol is based on evidence.
Evidence-based practice has been emphasized since the advent of the Institute of Medicine report. Professional organizations and federal agencies have developed many evidence-based guidelines. An excellent source of research publications is the Cochrane Library Collection (available online at http://www.cochrane.org). The Agency for Healthcare Quality and Research (AHRQ) has developed many guidelines relevant to your nursing practice. Some of the practice areas with guidelines are management of acute pain in adults, infants, and children; predication and prevention of pressure ulcers in adults; treatment of depression in primary care; and availability of cardiac rehabilitation services. AHRQ has also developed many tools to assess the quality of care that is provided. Access to the numerous clinical practice guidelines is available at www.ahrq.gov.
American Society of Hospital Pharmacists (ASHP). ASHP therapeutic position statement on the institutional use of 0.9% sodium chloride injection to maintain patency of peripheral indwelling intermittent infusion devices. American Journal of Hospital Pharmacy. 1994; 51(12):1572–1574.
Geritz, M. A. Saline versus heparin in intermittent infuser patency maintenance. Western Journal of Nursing Research. 1992; 14(2):131–141.
Goode, C. J., Titler, M., Rakel, B., Ones, D. S., Kleiber, C., Small, S., et al. A meta-analysis of effects of heparin flush and saline flush: quality and cost implications. Nursing Research. 1991; 40(6):324–330.
Randolph, A. G., Cook, D. J., Gonzales, C. A., Andrew, M. Benefits of heparin in peripheral venous and arterial catheters: Systematic review and meta-analysis of randomized controlled trials. British Medical Journal. 1998; 316(7136):969–975.
Shoaf, J., Oliver, S. Efficacy of normal saline injection with and without heparin for maintaining intermittent intravenous site. Applied Nursing Research. 1992; 5(1):9–12.
*Note: All peripheral venous catheters for pediatric patients must be flushed with heparin flush unless otherwise ordered by physician (Randolph et al., 1998).