Community-oriented nursing and community-based nursing
After reading this chapter, the student should be able to:
1. Describe the goal and core functions of public health and the services generally provided by practitioners of public health.
2. Discuss the role of the public health nurse specialist and how the role influences nursing practice in the community.
3. Explain community-based nursing practice.
4. Describe community-oriented nursing practice.
5. Examine how community-based nursing practice differs from community-oriented nursing practice.
Professional nurses must actively participate in developing evidence-based, cost-effective, high-quality, innovative, and useful ways to provide care to citizens. Evidence-based practice is the norm today and simply means that a nurse’s practice is based on the use of the best available evidence to provide this care. This evidence may be research, but if research is not available, practice may be based on opinions, case studies, or professional and governmental reports, to name a few examples. Of course it is always the best if research related to a strategy, an intervention, a program, or an application of a model can be found.
Because of the growing costs of hospital care, more services are being provided in community-based settings. Increasingly, nurses will engage in what is called community-based nursing (CBN). In CBN, the nurse focuses on “illness care” of individuals and families across the life span. The aim is to manage acute and chronic health conditions in the community, and the practice is family-centered illness care. While providing health care to individuals and families, the nurse maintains an appreciation for the values of the community. CBN is not a specialty in nursing but rather a philosophy that guides care from all nursing specialties when applied in the community.
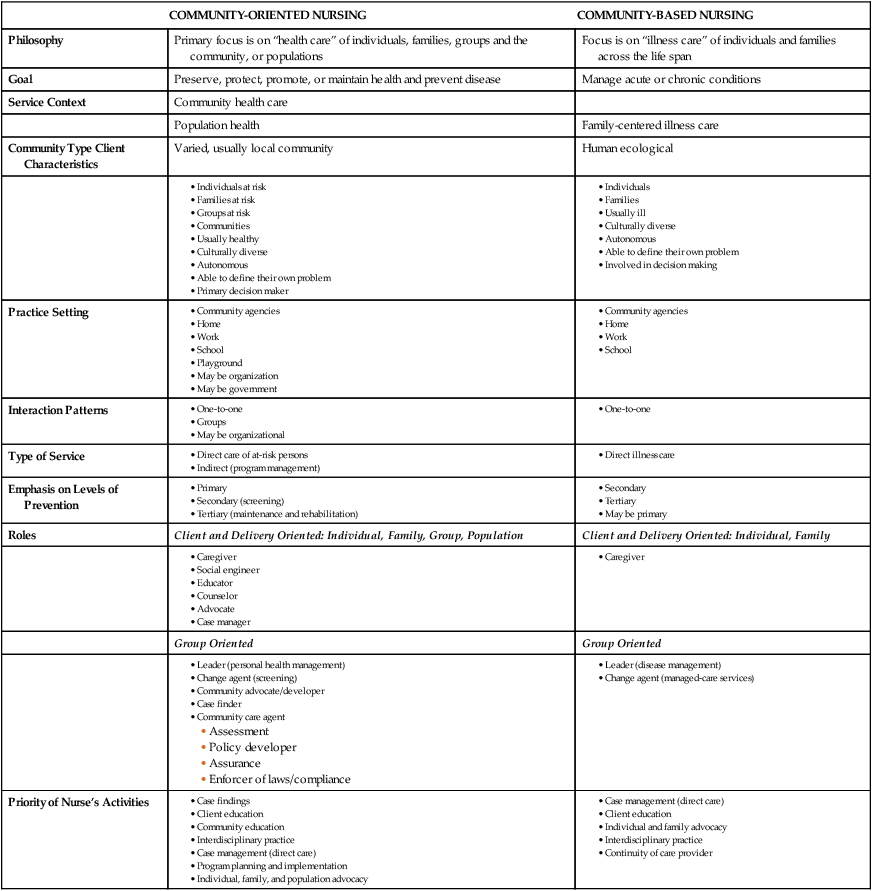
In contrast, community-oriented nursing has as its primary focus the health care of either the community or populations, as in public health nursing (PHN) or of individuals, families, and groups in a community. In the past, and by some today, care of individuals, families, and groups has been called community health nursing. In community-oriented nursing the goal is to preserve, protect, promote, or maintain health. The key difference between CBN and community-oriented nursing is that community-based nurses deal primarily with illness-oriented care, whereas community-oriented nurses provide health care to promote quality of life. They both deal with individuals and families, and the community-oriented nurse also typically deals with groups in the community. Table 1-1 lists the similarities and differences between community-oriented nursing and CBN.
TABLE 1-1
SELECT EXAMPLES OF SIMILARITIES AND DIFFERENCES BETWEEN COMMUNITY-ORIENTED AND COMMUNITY-BASED NURSING
| COMMUNITY-ORIENTED NURSING | COMMUNITY-BASED NURSING | |
| Philosophy | Primary focus is on “health care” of individuals, families, groups and the community, or populations | Focus is on “illness care” of individuals and families across the life span |
| Goal | Preserve, protect, promote, or maintain health and prevent disease | Manage acute or chronic conditions |
| Service Context | Community health care | |
| Population health | Family-centered illness care | |
| Community Type Client Characteristics | Varied, usually local community | Human ecological |
| Practice Setting | ||
| Interaction Patterns | ||
| Type of Service | ||
| Emphasis on Levels of Prevention | ||
| Roles | Client and Delivery Oriented: Individual, Family, Group, Population | Client and Delivery Oriented: Individual, Family |
| Group Oriented | Group Oriented | |
| Priority of Nurse’s Activities |
As mentioned, community-oriented nursing includes PHN. This is a specialty area whose primary focus is on the health care of communities and populations rather than on individuals, groups, and families. The goal of this specialty is to prevent disease and preserve, promote, restore, and protect health for the community and the population within it. The focus is on the public health ethic of “the greatest good for the greatest number.” This specialty is built on the blending of nursing and the discipline of public health (American Nurses Association, 2007).
This chapter examines both CBN and community-oriented nursing. It describes the similarities and differences between these two areas of nursing and also discusses public health and the core functions and services included in public health practice. In addition, the essential services of public health nurses are discussed, because nurses working from both a CBN and a community-oriented community health nursing framework may use some of these skills. To work effectively in the community, regardless of the focus, it is useful to know exactly what public health is and how the functions of that discipline work to improve the health of people in their communities.
What is public health?
Public health is a scientific discipline that includes the study of epidemiology, statistics, and assessment—including attention to behavioral, cultural, and economic factors—as well as program planning and policy development. In recent years, efforts in the United States to change the way in which health care is delivered have focused heavily on looking at ways to change the delivery of medical care and on health insurance. Limited attention has been focused on looking at the health of the population. Although people are excited when a new drug is discovered that cures a disease or when a new way to transplant organs is perfected, it is important to know about the significant gains in the health of populations that have come largely from public health accomplishments. For example, public health has influenced the safety and adequacy of food and water, sewage disposal, public safety from biological threats, and changes in personal behaviors such as smoking. The dramatic increase in life expectancy for Americans during the 1900s, from less than 50 years in 1900 to 77.9 years in 2007, is credited primarily to improvements in sanitation, the control of infectious diseases through immunizations, and other public health activities (U.S. Department of Health and Human Services [USDHHS], 2010a). Population-based preventive programs launched in the 1970s were also largely responsible for the more recent changes in tobacco use, blood pressure control, dietary patterns (except obesity), automobile safety restraint, and injury control measures that have fostered declines in adult death rates. A more than 50% decline in stroke and coronary heart disease deaths has occurred. Overall death rates for children have declined by about 40% (USDHHS, 2010a).
Another way of looking at the benefits of public health practice is to look at how early deaths can be prevented. The U.S. Public Health Service estimates that medical treatment can prevent only about 10% of all early deaths in the United States, whereas population-focused public health approaches could help prevent about 70% of early deaths in America through measures targeted to the factors that contribute to those deaths. Many of these contributing factors are behavioral, such as tobacco use, diet, and sedentary lifestyle. Other factors that affect health are the environment, social conditions, education, culture, economics, working conditions, and housing (Healthy People 2020, USDHHS, 2010b).
The passage of the Affordable Care Act of 2010 created and charged the National Prevention, Health Promotion and Public Health Council with developing the National Prevention and Health Promotion strategy to focus on community-oriented approaches to prevention and wellness to “reduce the incidence and burden of the leading causes of death and disability.” The strategy identifies the five leading causes of death as heart disease, cancers, stroke, chronic lower respiratory disease, and unintentional injuries. Other priorities named are behavioral and mental health, substance use, and domestic violence screenings. In addition, the four health-promoting behaviors associated with the underlying causes of death that will be targeted through prevention measures are tobacco use, nutrition, physical activity, and underage and excessive alcohol use (USDHHS, 2010c).
Public health practice is of great value. The Centers for Medicare and Medicaid Services (CMS) (2012) reported that only 3% (up from 1.5% in 1960) of all national health expenditures supported population-focused public health functions. Unfortunately, the public is largely unaware of the contributions of public health practice. Federal and private monies were sparse in their support of public health, so public health agencies began to provide personal care services for persons who could not receive care elsewhere. The health departments benefited by receiving Medicaid and Medicare funds. The result was a shift of resources and energy away from public health’s traditional and unique population-focused perspective to include a primary care focus (USDHHS, 2002). As overall health needs become the focus of care in the United States, a stronger commitment to population-focused services is emerging. In July 2008, the Trust for America’s Health released a study that highlighted the effects of preventive services on improving lives and reducing costs as well as ways to change the health care system. The threats of bioterrorism, highlighted by the events of September 11, 2001, and the anthrax scares increase awareness for public safety. Important to the public health community is the emergence of modern-day epidemics and infectious diseases, such as the mosquito-borne West Nile virus and other causes of mortality, many of which affect the very young. Most of the causes are preventable (American College of Physicians, 2012).
Public health is best described as what society collectively does to ensure that conditions exist in which people can be healthy (Institute of Medicine, 2003). Public health is a community-oriented, population-focused specialty area. The overall mission of public health is to organize community efforts that will use scientific and technical knowledge to prevent disease and promote health (Institute of Medicine, 2003). The three public health core functions are assessment, policy development, and assurance.
Public health core functions defined
Figure 1-1 describes public health in America. These functions provide a framework for defining the services to be provided by the public health system. The core functions are defined as follows:

• Assessment is systematic data collection on the population, monitoring the population’s health status, and making information available about the health of the community.
• Policy development refers to efforts to develop policies that support the health of the population, including using a scientific knowledge base to make policy decisions.
• Assurance is making sure that essential community-oriented health services are available. These services might include providing essential personal health services for those who would otherwise not receive them. Assurance also includes making sure that a competent public health and personal health care workforce is available.
A working group within the U.S. Public Health Service developed the Health Services Pyramid (Figure 1-2). In this pyramid, population-focused public health programs with the goals of disease prevention, health protection, and health promotion provide a foundation for primary, secondary, and tertiary health care services. Each service level in the pyramid is important to the health of the population. The base of the pyramid shows the effective services that support the top tiers and contribute to better health. All tiers of the pyramid need to be adequately financed (U.S. Public Health Service, 1994/2008). Since the pyramid was developed it has been referenced to show how health care services can be offered to specific population groups (Frieden, 2010). In reality, health care in the United States has been organized with the pyramid upside down. That is, more attention, support, and funding are given to tertiary and secondary care than to primary and preventive services including population-focused care. The “How To” box on p. 5 lists the essential public health services.
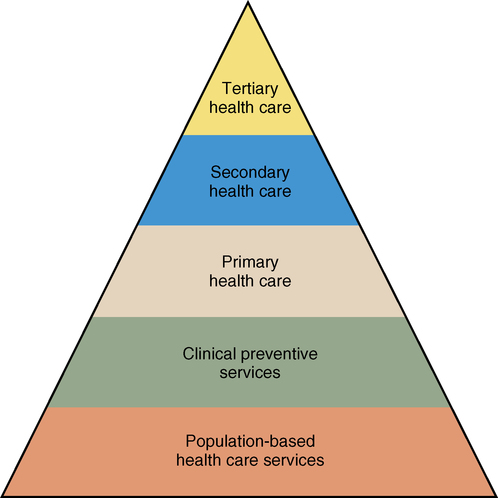
These services need to be implemented to support the base of the pyramid and to support the services offered through the top tiers of the pyramid. Together, all services at all levels contribute to better health in America.
Population-focused nursing practice
PHN is a specialty with a distinct focus and scope of practice; it requires a special knowledge base. The role of the public health nurse has changed over the years in response to the following:
As noted in Chapter 2, PHN began more than 100 years ago; early public health nurses provided direct care to people, most often in their homes. The Henry Street Settlement, established in New York City in the late 1800s by Lillian Wald, was an early model for PHN. At Henry Street Settlement the nurses took care of the sick in their homes and also looked at the overall population of low-income people in the community from which their home care clients came. The primary focus that has differentiated PHN from other specialties has been the emphasis on the population rather than on single individuals or families. Following the example of Lillian Wald, public health nurses have done the following:
• Looked at the community or population as a whole
• Raised questions about the overall health status and the factors associated with that status, including environmental factors such as physical, biological, social, economic, and cultural aspects
• Worked with the community to improve health status
• Provided health education to individuals, families, and groups to encourage healthier living
The primary goal of public health—the prevention of disease and disability—is achieved by ensuring that conditions exist in which people can remain healthy. The Policy Development process “How To” box describes ways to distinguish what actually makes up the specialty of PHN.
In 1981 the PHN section of the American Public Health Association (APHA) defined PHN and described how this role contributes to health care delivery. This statement was reaffirmed in 1996 (American Public Health Association, 1996). PHN is defined as a specialty that brings together knowledge from the public health sciences and nursing to improve the health of the community. It is defined by the Quad Council of Public Health Nursing Organizations as population-focused, community-oriented nursing practice. The goals of PHN are “the promotion of health, the prevention of disease and disability for all people through the creation of conditions in which people can be healthy” (American Nurses Association, 2007). Box 1-1 presents the process of PHN from the APHA definition.
Public health nurses, like others in public health, engage in assessment, policy development, and assurance activities. These functions are achieved when nurses work in partnerships with others, including nations, states, communities, organizations, groups, and individuals. Public health nurses carry out this mission by participating in the essential public health services described earlier in the chapter.
Although population-focused practice is the central feature of PHN, many of the skills and activities are used when community-oriented nurses and community-based nurses work in the community. For this reason, these practices are described in detail here. A population or aggregate is a collection of people who share one or more personal or environmental characteristics. Members of a community can be defined in terms of either geography (e.g., a county, a group of counties, or a state) or a special interest (e.g., children attending a particular school). These members make up a population. Generally, there are subpopulations within the larger population. Examples of a subpopulation within a population of a county are high-risk infants younger than 1 year old, unmarried pregnant adolescents, or individuals exposed to a particular event such as a chemical spill.
In population-focused practice, problems are defined (assessments/diagnoses) and solutions (interventions), such as policy development or providing a given preventive service, are implemented for or with a defined population or subpopulation as opposed to diagnoses, interventions, and treatment carried out at the individual level. This contrasts with basic professional education in nursing, medicine, and other clinical disciplines, which emphasizes developing competence in decision making at the level of the individual client by assessing health status, making management decisions (ideally with the client), and evaluating the effects of care. The ways in which nurses provide care to people with high blood pressure can demonstrate how population-focused practice differs from the clinical direct care practice so often used in nursing. Specifically, in a clinical direct care situation a nurse practicing in the community might decide that a person is hypertensive based on certain clinical signs. The nurse would evaluate different interventions to find the best one for this person and implement an intervention such as a change in diet. In contrast, a public health nurse engaged in population-focused practice would ask the following questions:
• What is the prevalence rate of hypertension among various age, race, and gender groups?
• Which subpopulations have the highest rates of untreated hypertension?
• What programs could reduce the problem of untreated hypertension and decrease the risk for further cardiovascular morbidity and mortality?
Public health nurses are typically concerned with more than one subpopulation, and they often deal with the health of the entire community. Assessment, one of the public health core functions, is a logical first step in examining a community setting to determine its health status.
The core public health function of assessment includes the following:
• Engaging in activities that involve the collection, analysis, and dissemination of information on both the health and health-relevant aspects of a community or a specific population.
• Questioning, for example, whether the health services of the community are available to the population and are adequate to address needs.
• Monitoring the health status of the community or population and the services provided over time.
• Evaluating the social, economic, environmental, and lifestyle characteristics and practices of a population, as well as the health services and capacity available within the community to support good health for the population.
Listed in the “How To” box is a general set of questions that can be used or modified to gather assessment data.
Excellent examples of assessment at the national level are the U.S. Department of Health and Human Services’ efforts to organize the goal-setting, data collection and analysis, and monitoring necessary to develop the series of publications describing the health status and health-related aspects of the U.S. population. These efforts began with Healthy People in 1980 and continued with Promoting Health, Preventing Disease: 1990 Health Objectives for the Nation, Healthy People 2000, Healthy People 2010, and are now moving forward into the future with Healthy People 2020 (USDHHS, 1979, 1991, 2000, 2010b).*
 HEALTHY PEOPLE 2020
HEALTHY PEOPLE 2020
Overview and Goals
In 1979, the Surgeon General issued a report that began a 20-year focus on promoting health and preventing disease for all Americans. The report, entitled Healthy People, used morbidity rates to track the health of individuals through the five major life cycles of infancy, childhood, adolescence, adulthood, and older age.
In 1989, Healthy People 2000 became a national effort of representatives from government agencies, academia, and health organizations. Their goal was to present a strategy for improving the health of the American people. Their objectives are being used by public and community health organizations to assess current health trends, health programs, and disease-prevention programs.
Throughout the 1990s, all states used Healthy People 2000 objectives to identify emerging public health issues. The success of the program on a national level was accomplished through state and local efforts. Early in the 1990s, surveys from public health departments indicated that 8% of the national objectives had been met and progress on an additional 40% of the objectives was noted. In the mid-course review published in 1995, it was noted that significant progress had been made toward meeting 50% of the objectives.
Using the progress made in the past decade, the committee for Healthy People 2010 proposed the following two goals:
They hope to reach these goals by measures such as promoting healthy behaviors, increasing access to quality health care, and strengthening community prevention.
The major premise of Healthy People 2010 is that the health of the individual can rarely be separated from the health of the larger community. Therefore, the vision for Healthy People 2010 was “Healthy People in Healthy Communities.”
The vision for Healthy People 2020 is: A society in which all people live long, healthy lives. The overarching goals for 2020 are:
• To eliminate preventable disease, disability injury, and premature death
• To achieve health equity, eliminate disparities, and improve the health of all groups
• To create social and physical environments that promote good health for all
• To promote healthy development and healthy behaviors across every stage of life
In contrast to previous years, Healthy People 2020 has a web-accessible database that will be searchable, multilevel, and interactive to be more useful. The objectives for 2020 are now available on the website: http://healthypeople.gov/2020/topicsobjectives2020/default.aspx.
Data from U.S. Department of Health and Human Services: Healthy People 2000: national health promotion and disease prevention objectives, DHHS Pub. No. 91-50212, Washington, DC, 1991, U.S. Government Printing Office; U.S. Department of Health and Human Services: Healthy People 2010: understanding and improving health, ed 2, Washington, DC, 2000, U.S. Government Printing Office; U.S. Department of Health, Education, and Welfare: Healthy People: the Surgeon General’s report on health promotion and disease prevention, DHEW Pub. No. 79-55071, Washington, DC, 1979, U.S. Government Printing Office; U.S. Department of Health and Human Services: Healthy People 2020: the road ahead, Washington, DC, 2010, U.S. Government Printing Office. Retrieved October 8, 2010 from http://www.healthypeople.gov/hp2020/default.asp.
In a local health department, public health nurses would participate in and provide leadership for assessing community needs, the health status of populations within the community, and environmental and behavioral risks. They also look at trends in the factors that determine health in the community, identify priority health needs, and determine the adequacy of existing community resources.
Policy development is a core function of public health and one of the core intervention strategies used by PHN specialists. Policy development relies heavily on planning and begins with the identified needs and priorities set by the people involved. It also includes building constituencies that can bring about policy changes. It is important to know what the powerful people in the community think about a specific public health concern. Health and human services providers, as well as the people who will be served or affected, must be included. PHN is a “with the people,” not a “to the people” or “for the people,” approach to planning. Historically, health care providers have been accused of providing care for or to people without actually involving the recipients in the decisions. The beneficiaries of services in public health need to be included from the very beginning in identifying the need, planning the intervention, and deciding on the format for the evaluation (Box 1-2).
The third core public health function, assurance, focuses on the responsibility of public health agencies to be sure that activities are appropriately carried out to meet public health goals and plans. Not only does PHN include assessment or investigative functions but the role also requires skill in collaboration, consultation, and cooperation. The assurance function makes sure that the activities designed during the policy development or planning phase are carried out. This is done through collaboration with people in a variety of health and human service organizations to promote, monitor, and improve both the availability and quality of providers and services. PHN is not a good field for people who like to work alone. Although considerable opportunity exists for autonomy in thinking and planning, effective and consistent collaboration is vital to success. Assurance does not always mean to provide something. Rather, another agency may provide the needed service. Assurance means making certain that the services determined to be needed are provided by some agency within the community. Further, assurance includes assisting communities to implement and evaluate plans and projects. It includes maintaining the ability of both public health agencies and private providers to manage day-to-day operations, as well as the capacity to respond to critical situations and emergencies.
In PHN, the nurse often reaches out to those who might benefit from a service or intervention. In other forms of nursing, the client is more likely to seek and request assistance. As is discussed in later chapters, often the people or populations most in need of public health services are the least likely to ask for them. Examples include homeless, poor, and mentally ill people. The dominant needs of the population outweigh the expressed needs of one or a few people. Because resources are often limited, careful assessment to identify key needs is important.
However, the special contributions of public health nurse specialists include looking at the community or population as a whole, raising questions about its overall health status and factors associated with that status, including environmental factors (i.e., physical, biological, sociocultural), and working with the community to improve the population’s health status.
Practice focusing on individuals, families, and groups
As mentioned, community-based nursing practice, with its focus on the provision or assurance of care to individuals and families in the community, is different from community-oriented practice. The latter is broader in scope and is a form of care in which the nurse provides health care after doing a community diagnosis to determine what conditions need to be altered for individuals, families, and groups in the community to stay healthy. Although it is hoped that all direct care providers contribute to the community’s health in the broadest sense, not all are primarily concerned with the population focus, or the “big picture.” All nurses in a given community, including those working in hospitals, physicians’ offices, and health clinics, contribute positively to the health of the community. Examples of community settings for treating individuals include ambulatory surgery clinics, outpatient clinics, physician and advanced-practice nursing offices and clinics, and employment and school sites, as well as preschool programs, housing projects, and migrant camps. These sites often provide individual-focused health care services. This contrasts to population-focused services (i.e., services focused on a large group). A specific example is the federally funded program for preschool children, Head Start. From a community-oriented nursing care perspective, nursing services could be provided to individual children by conducting developmental-level screening tests to evaluate each child’s level of cognitive and psychomotor development in contrast to established standards for children of the same age. The community-based nurse may deliver illness care to the children in the school. In contrast, a public health or population-focused approach would look at the entire group of children being served by the program and the characteristics of the facility and its programs to see if they are effective in achieving the goals of making the school population healthier.
Community-oriented nursing
Most nurses practicing in the community and many staff public health nurses—both historically and at present—focus on providing direct care services, including health education, to persons or families outside of institutional settings, either in the home or in a clinic. Historically, the term community health nurse applied to all nurses who practiced in the community, regardless of whether they had preparation in PHN. Thus, nurses providing secondary or tertiary care in a home, school, or clinic or any nurse who did not practice in an institutional setting could be considered a “community health nurse.” To a large extent the development of what has been called community health nursing was influenced by the development within medicine of the specialty of community medicine. At that time both community medicine and community health nursing reached out to the community and began doing community assessments to determine more effectively the needs of the people. Thus, disease prevention and health promotion could be targeted to specific needs in a given community. Specifically, the community health nurse operated from a health care focus based on an understanding of broader community needs.
The nurse is continually evaluating the community to see if changes are occurring that will influence the health of the people who live there. The case study on the Evolve website is an example of community-oriented nursing practice. Work through the case study and answer the questions for understanding this area of specialty.
The practice of community-oriented nursing involves health promotion, health maintenance, health education, management, coordination, and continuity of care in the management of the health care of individuals, families, and groups in a community. A holistic approach is used, and the goal of this care is to provide personal health services that promote and preserve the health of the community in which the clients live. This nurse uses both nursing and public health theory to guide practice.
Evidence that entry-level nurses are practicing effectively in the community includes the following (Turnock, 2009):
• Provides quality services that can control costs
• Focuses on disease prevention and health promotion
• Organizes services where people live, work, play, and learn
• Provides referrals when clients need them
• Works in partnerships and with coalitions and other health care providers
• Works across the life span and with culturally diverse populations
• Works with at-risk populations to promote access to services
• Participates in epidemiological investigations and disaster services
• Develops the community’s capacity for health
As can be seen, community-oriented nurses emphasize health protection, maintenance, and promotion, and disease prevention, as well as self-reliance among clients. Regardless of whether the client is a person, a family, or a group, the goal is to promote health through education about prevailing health problems, proper nutrition, beneficial forms of exercise, and environmental factors such as safe food, water, air, and buildings. The nurse is likely to be involved in immunizing individuals as well as organizing the immunization programs for vaccinating the community for influenza, for example, and educating the community about the value of this service. Other individual and family services include provision of maternal and child health care, treatment of common communicable and infectious diseases and injuries, and provision of basic screening programs for problems such as lice, vision, hearing, and scoliosis.
Nurses have always been involved in providing family-centered care to individuals, families, and groups across the life span; however, they also work to identify high-risk groups in the community. Once such groups are identified, the nurse can work with others to develop appropriate policies and interventions to reduce risk and provide beneficial services. Both community-oriented nurses and community-based nurses must be aware of cultural diversity and provide care that is appropriate to the needs of the recipient. Likewise, both groups of nurses provide care in homes. The Focus on Quality and Safety Education for Nurses box provides the list of competencies a nurse will need to improve the quality and safety of interventions and outcomes in the community. Compare these competencies to the public health nursing competencies in Appendix C.3.
 FOCUS ON QUALITY AND SAFETY EDUCATION FOR NURSES
FOCUS ON QUALITY AND SAFETY EDUCATION FOR NURSES
Quality and Safety Education for Nurses (QSEN) Competencies
| QSEN COMPETENCY | COMPETENCY DEFINITION |
| Client-Centered Care | Recognize the client or designee as the source of control and full partner in providing compassionate and coordinated care based on respect for client preferences, values, and needs. |
| Teamwork and Collaboration | Function effectively within nursing and interprofessional teams, fostering open communication, mutual respect, and shared decision making to achieve quality care. |
| Evidence-Based Practice | Integrate best current evidence with clinical expertise and client/family preferences and values for delivery of optimal health care. |
| Quality Improvement | Use data to monitor the outcomes of care processes and use improvement methods to design and test changes to continuously improve the quality and safety of health care systems. |
| Safety | Minimizes risk for harm to clients and providers through both system effectiveness and individual performance. |
| Informatics | Use information and technology to communicate, manage knowledge, mitigate error, and support decision making. |
Prepared by Gail Armstrong, DNP, ACNS-BC, CNE, Associate Professor, University of Colorado Denver College of Nursing.
 LEVELS OF PREVENTION
LEVELS OF PREVENTION
Related to Public Health
The public health nurse develops a health education program for a population of school-age children that teaches them about the effects of smoking on health.
Community-based nursing
As mentioned, the goal of CBN is to manage acute or chronic conditions while promoting self-care among individuals and families (Lundy and Janes, 2009). In CBN the nursing care is family centered, which means that the nurse works to improve the competencies of families to enable them to take better care of themselves. The nurse pays particular attention to the uniqueness of each family and works to plan the most useful interventions. A “cookbook” approach cannot be used because no one nursing approach will fit each family or individual. Cultural diversity is taken into account, as are the situations and stressors facing the person or the family at a given time. The nurse promotes client autonomy and helps clients learn to do as much as possible for themselves.
The nurse practicing CBN is more likely to give direct care to people than are nurses who practice from a community-oriented framework. To plan the most appropriate course of action, the nurse assesses client needs and the services available to meet those needs. Throughout care delivery, the nurse teaches and counsels clients so they can more fully develop their own ways of taking care of themselves. Box 1-3 provides definitions of each of the four key modes of nursing practice seen in the community.
Challenges for the future
Over the past few years, the places in which care is given have changed dramatically. In previous decades the majority of care was given in an inpatient setting. At present, the trend is to move more care into community settings and to reduce the number of hospital days for “sick” clients. A variety of reasons explain the change. First, community care is often much less expensive than hospital care. Because the cost of health care in the United States has risen considerably over the past decade, it is increasingly necessary to find new ways to deliver care that are accessible to the recipients, less expensive, and of adequate quality to meet client needs. Also, care in the community is usually more appealing to people who prefer to remain at home rather than be treated in a hospital. Currently, care is given in homes, schools, and at the work site, as well as in a variety of outpatient clinics. This trend is expected to grow, and it is expected that the role of the nurse in community settings will likewise grow and continue to change. Many factors will affect the changing role of the nurse in the community, such as the new and emerging infectious diseases, the need for emergency preparedness, the increases in chronic illness, and the continued reduction of numbers of days in the hospital for serious illnesses.
Clinical application
Debate with classmates where and how PHN specialists practice and how their practice compares with what has been defined as CBN. Be specific about the differences.
Debate with classmates which of the nurses in the following categories are practicing population-focused nursing:
C Director of nursing for a home care agency
D Nurse practitioners in a health maintenance organization
E Vice president of nursing in a hospital
F Staff nurses in a public health clinic or community health center
Choose three categories from the list above and interview at least one nurse in each category.
1. Determine the scope of their practice.
2. Are they carrying out population-focused practice?
5. Ask them if they would change their role if this were possible.
6. Inquire whether they believe their role is either community-oriented nursing or CBN practice. Compare and contrast their answers with what you have learned about these roles.
Remember this!
• Public health is what members of a society do collectively to ensure that conditions exist in which people can be healthy.
• Assessment, policy development, and assurance are the core public health functions at all levels of government.
• Assessment refers to systematic data collection on the population, monitoring of the population’s health status, and making information available on the health of the community.
• Policy development refers to the need to provide leadership in developing policies that support the health of the population, including use of the scientific knowledge base in decision making about policy.
• Assurance refers to the way public health practice makes sure that essential community-wide health services are available. This may include providing essential personal health services for those who would otherwise not receive them. Assurance also includes making sure that a competent public health and personal health care workforce is available.
• Setting is frequently viewed as the feature that distinguishes PHN from other specialties. A more useful approach is to use characteristics such as the following: a focus on populations who live in the community, an emphasis on prevention, concern for the interface between health status of the population and the environment (i.e., physical, biological, sociocultural), and the use of political processes to influence public policy to achieve goals.
• Specialization in PHN is seen as a subset of community-oriented nursing practice.
• Population-focused practice is the focus of specialization in PHN. The focus on populations in the community and the emphasis on health protection, health promotion, and disease prevention are the fundamental factors that distinguish PHN from other nursing specialties.
• Population is defined as a collection of individuals who share one or more personal or environmental characteristics. The term population may be used interchangeably with the term aggregate.
What would you do?
1. Define each of the following:
2. Discuss with classmates examples in your community in which the CBN role is the ideal role to meet client needs. Also identify examples in which the most useful nursing role would be that of the community-oriented nurse. How can you justify your opinion if classmates disagree?
3. With three or four of your classmates, develop a plan for identifying two or three nurses in your community who are in an administrative role and discuss the following with them:
A How they define the populations they serve
B The strategies they use to monitor the population’s health status
C The strategies they use to ensure that the populations are receiving basic needed services
4. Can you compare and contrast their answers to what you have learned about roles in different settings?
Additional resources
Appendixes
• Appendix A.1: The Health Insurance Portability and Accountability Act (HIPAA): What Does It Mean for Public Health Nurses?
• Appendix C.1: Examples of Public Health Nursing Roles and Implementing Public Health Functions
• Appendix C.2: American Nurses Association Standards of Care of Public Health Nursing Practice
• Appendix C.3: Quad Council Public Health Nursing Core Competencies and Skill Levels

