The Stuart Stress Adaptation Model of Psychiatric Nursing Care
1. Discuss the theoretical assumptions underlying the Stuart Stress Adaptation Model of psychiatric nursing care.
2. Describe dimensions of mental health and mental illness in the United States.
3. Analyze the biopsychosocial components of the Stuart Stress Adaptation Model of psychiatric nursing care.
4. Compare coping responses, nursing diagnoses, health problems, and medical diagnoses.
5. Evaluate nursing activities appropriate to the various stages of psychiatric treatment.

Models provide a structure for thinking, observing, and interpreting what is seen. Nursing models can explain a person’s response to stress and the process and desired outcomes of nursing interventions. Psychiatric nurses enhance their practice by basing their actions on a model of psychiatric nursing care that is inclusive, holistic, and relevant to the needs of patients, families, groups, and communities.
This textbook is based on the Stuart Stress Adaptation Model of psychiatric nursing care, which integrates biological, psychological, sociocultural, legal, ethical, policy, and advocacy aspects of patient care into a unified framework for practice. It was developed by Gail Stuart as a synthesis of diverse bodies of knowledge from the perspective of psychiatric nursing and, equally important, as an application of this knowledge to clinical practice. This model is based on five theoretical assumptions.
Theoretical Assumptions
The first assumption of the Stuart Stress Adaptation Model is that nature is ordered as a social hierarchy from the simplest unit to the most complex (Figure 3-1). Each level of this hierarchy is an organized whole. Each level also is a part of all of the other levels, so nothing exists in isolation. Thus the individual is a part of the family, group, community, society, and the larger biosphere. Material and information flow across levels, and each level is influenced by all the others. The most basic level of nursing intervention is the individual. However, in working with the individual, the nurse also must consider how the individual relates to the whole.

The second assumption of the model is that nursing care is provided within a biological, psychological, sociocultural, legal, ethical, policy and advocacy context. Each of these aspects of care is described in detail in Chapters 5 through 9. The nurse must understand each of them in order to provide competent, holistic psychiatric nursing care. The theoretical basis for psychiatric nursing practice is derived from nursing science as well as from the behavioral, social, and biological sciences. The range of theories used by psychiatric nurses includes nursing, developmental psychology, neurobiology, pharmacology, psychopathology, learning, sociocultural, cognitive, behavioral, economic, organizational, political, legal, ethical, interpersonal, group, family, and milieu.
The third assumption of the model is that health/illness and adaptation/maladaptation are two distinct continuums:
• The health/illness continuum comes from a medical world view.
• The adaptation/maladaptation continuum comes from a nursing world view.
This means that a person with a medically diagnosed illness may be adapting well to it. An example is the adaptive coping responses used by some people who have chronic physical or psychiatric illnesses. In contrast, a person without a medically diagnosed illness may have many maladaptive coping responses. This can be seen in the adolescent whose problematic behaviors reflect poor coping responses to the many issues that must be resolved during adolescence. These two continuums thus reflect the complementary nature of the nursing and medical models of practice.
The fourth assumption is that the model includes prevention, treatment and recovery by describing four stages of psychiatric care: crisis, acute, health maintenance, and health promotion. For each stage of treatment the model suggests a treatment goal, a focus of the nursing assessment, the nature of nursing interventions, and the expected outcome of nursing care. Because it includes the full continuum of care, it can direct nursing practice in the hospital, community, and home settings.
The fifth assumption of the Stuart Stress Adaptation Model is that it is based on the use of the nursing process and the standards of care and professional performance for psychiatric nurses (Chapter 11). Psychiatric nursing care is provided through assessment, diagnosis, outcome identification, planning, implementation, and evaluation. Each step of the process is important, and the nurse assumes full responsibility for all nursing actions implemented and the enactment of a professional nursing role.
The assumptions of the Stuart Stress Adaptation Model are summarized in Box 3-1.
Describing Mental Health and Illness
The standards of mental health are less clear than those of mental illness. It is dangerous to assume that an unusual lifestyle is a sign of illness or abnormality. This can be avoided if one thinks of health/illness and conformity/deviance as separate concepts. Combining them creates four patterns: the healthy conformist, the healthy deviant, the unhealthy conformist, and the unhealthy deviant (Figure 3-2). Psychiatric nurses must carefully consider the meaning of an individual’s behavior and its context, because it reflects an adaptation to issues in the individual’s life and one’s social and cultural environment.

A person should not be assessed against some vague or ideal notion of mental health. Each person should be seen in both a group and an individual context. The issue is not how well someone fits an arbitrary sociocultural standard, but rather what is reasonable for a particular person in their life situation. Is there continuity or discontinuity with the past? Does the person adapt to changing needs throughout the life cycle?
Defining Mental Health
Mental health is a state of well-being associated with happiness, contentment, satisfaction, achievement, optimism, or hope. However these terms are difficult to define, and their meanings change as they relate to a particular person and life situation. Some suggest that mental health is not a simple concept or a single aspect of behavior. Instead, mental health involves a number of criteria that exist on a continuum. Although no one reaches the ideal in all the criteria, most people can approach the optimum.
Criteria of Mental Health.
The following six criteria are indicators of mental health:
Positive attitudes toward self include an acceptance of oneself and self-awareness. A person must have some objectivity about the self and realistic aspirations that necessarily change with age. A healthy person also must have a sense of identity, wholeness, belongingness, security, and meaningfulness.
Growth, self-actualization and resilience mean that the individual seeks new experiences to more fully explore aspects of oneself. Maslow (1958) and Rogers (1961) developed theories on the realization of the human potential. Maslow describes the concept of self-actualization, and Rogers emphasizes the fully functioning person. Both theories focus on the entire range of human adjustment. They describe a self as always seeking new growth, development, and challenges. These theories focus on the total person and whether the person has the following characteristics:
• Is in touch with one’s self and able to use the available resources
• Has access to personal feelings and can integrate them with thoughts and behaviors
• Can interact freely and openly with the environment
• Can share with other people and grow from such experiences
This criterion includes the concept of resilience, which is the ability to achieve, retain, or regain a level of physical or emotional health after a tragedy, trauma, adversity or significant stressor. It is the idea that some people “bounce back” after a problem, and proposes that humans must weather periods of stress and change throughout life. Successfully weathering each period of disruption and reintegration leaves the person better able to deal with the next life change (Wagnild and Collins, 2009; Resnick and Inguito, 2011).
Integration is a balance between what is expressed and what is repressed, between outer and inner conflicts. It includes the regulation of emotional responses and a unified philosophy of life. This criterion can be measured by the person’s ability to withstand stress and cope with anxiety. A strong but not rigid ego allows the person to handle change and grow as a result of it.
Autonomy involves self-determination, a balance between dependence and independence, and acceptance of the consequences of one’s actions. It implies that the person is self-responsible for decisions, actions, thoughts, and feelings. As a result the person can respect autonomy and freedom in others.
Reality perception is the individual’s ability to test assumptions about the world and to change perceptions based on new information. This criterion includes empathy, social sensitivity, and a respect for the feelings and attitudes of others.
Environmental mastery allows a mentally healthy person to feel success in an approved role in society. The person can deal effectively with the world, work out personal problems, and obtain satisfaction from life. The person should be able to cope with loneliness, aggression, and frustration without being overwhelmed. The mentally healthy person can respond to others, love and be loved, build new friendships and have satisfactory social group involvement.
Defining Mental Illness
Mental illness is a behavioral or psychological pattern demonstrated by an individual that causes significant distress, impaired functioning, and decreased quality of life. It reflects an underlying psychobiological dysfunction and is not the result of social deviance or conflicts with society.
Mental disorders are a major contributor to the burden of illness in the United States (Kessler et al, 2005a,b).
• Nearly 50% of all people ages 18 years and older have had a psychiatric or substance abuse disorder in their lifetimes.
• Half of all these lifetime cases start by age 14 and three-fourths start by age 24.
The seriousness and persistence of some disorders cause great strain on affected individuals, their families, communities, and the larger health care system. In addition, there is a substantial increased risk of premature death from natural and unnatural causes for people with common mental disorders (Druss and Bornemann, 2010). The Substance Abuse and Mental Health Services Administration (SAMHSA) has thus identified four important messages:
• Behavioral health is an essential part of all health.
• People recover from mental health and substance use disorders.
Box 3-2 presents other key facts about mental illness (SAMHSA, 2011).
In 1996 the Global Burden of Disease Study examined the disabling outcomes of 107 diseases around the world. Of the 15 specific leading causes of disability in developed countries, five are mental health problems: (1) major depressive disorder, (2) alcohol use, (3) schizophrenia, (4) self-inflicted injuries, and (5) bipolar disorder (Murray and Lopez, 1996). Depressive disorders as a single diagnostic category were the leading cause of disability worldwide. Further, by the year 2020, mental disorders are projected to increase, and major depression is predicted to become the second leading cause in disease burden worldwide.
Biopsychosocial Components
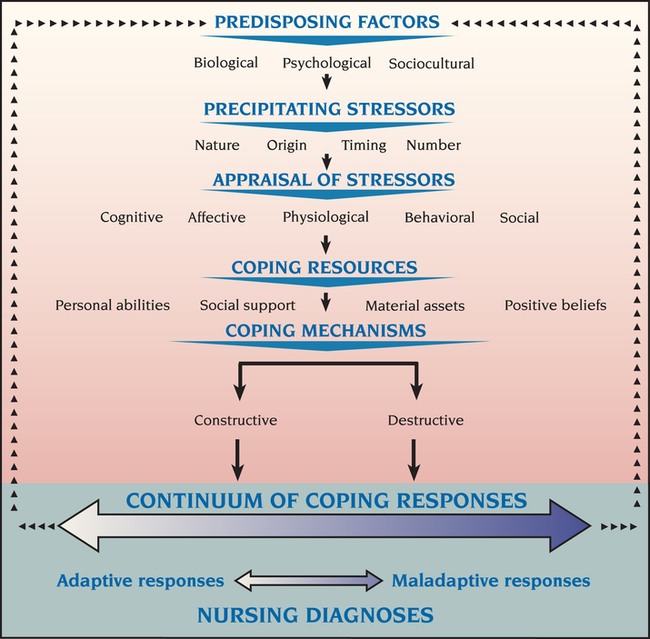
The Stuart Stress Adaptation Model of psychiatric nursing care views human behavior from a holistic perspective that integrates biological, psychological, and sociocultural aspects of care. For instance, a man who has had a myocardial infarction also may be severely depressed because he fears he will lose his ability to work and to satisfy his wife sexually. He also may have a family history of depression. Likewise, patients who seek treatment for major depression also may have gastric ulcers that are exacerbated by their depression. The holistic nature of psychiatric nursing practice examines all aspects of the individual, family, community and the environment. The specific biopsychosocial components of the Stuart Stress Adaptation Model are shown in Figure 3-3.
Predisposing Factors
Predisposing factors are risk and protective factors that influence the type and amount of resources the person can use to handle stress. They are biological, psychological, and sociocultural.
• Biological predisposing risk factors include genetic background, nutritional status, biological sensitivities, general health, and exposure to toxins.
• Psychological predisposing risk factors include intelligence, verbal skills, morale, personality, past experiences, self-concept and motivation, psychological defenses, and locus of control, or a sense of control over one’s own fate.
• Sociocultural predisposing risk factors include age, gender, education, income, occupation, social position, cultural background, religious upbringing and beliefs, political affiliation, socialization experiences, and level of social integration or relatedness.
Precipitating Stressors
Precipitating stressors are stimuli that are challenging, threatening, or demanding to the individual. They require excess energy and produce a state of tension and stress. They may be biological, psychological, or sociocultural in nature. They may originate either in the person’s internal environment or in the person’s external environment. It also is important to assess the timing of the stressor, which includes when the stressor occurred, how long the person was exposed to the stressor, and the frequency with which it occurred. A final factor is the number of stressors an individual experiences within a certain period because stressful events may be more difficult to deal with when many of them occur close together.
Stressful Life Events.
The relationship of stressful life events to the cause, onset, course, and outcomes of psychiatric illnesses has been the focus of much research. Focus has been on the nature of the event and the amount of change it requires. There are three ways to categorize life events:
1. By social activity. This includes family, work, educational, social, health, financial, legal, or community crises.
2. By social field. These events are defined as entrances and exits. An entrance is the introduction of a new person into the individual’s social field; an exit is the departure of a significant other from the person’s social field.
3. By social desirability. Within social norms, events can be considered generally desirable, such as promotion, engagement, and marriage, or generally undesirable, such as death, financial problems, being fired, and divorce.
Unfortunately, it is hard to determine the exact role played by stressful life events. Although they have been correlated with the onset of anxiety and disease symptoms, the research has been criticized. For example, the particular events listed on a stressful life event scale may not be the most relevant to certain groups, such as students, working mothers, different cultural groups, the elderly, the poor, or the persistently mentally ill. Also the life-events approach provides no clues to the specific way in which the events affect physical or mental health.
It is better, therefore, to think about stressful life events along a continuum that can influence the development of psychiatric illness. At one end of the continuum, they may act as triggers that precipitate an illness in people who would have developed the illness eventually for one reason or another. At the other end of the continuum, stressful life events may make a person more vulnerable, reduce an individual’s resistance and coping resources, and thus make the person more susceptible to psychiatric distress and illness.
Life Strains and Hassles.
The stressful life-events theory is built on the idea of change in response to major life events. However, small daily strains or hassles may have a greater effect on a person’s mood and health than do major misfortunes. Stress also can arise from smaller but more chronic problems or life strains, such as ongoing family tension, job dissatisfaction, and loneliness. Such life strains commonly occur in four areas:
Hassles are irritating, frustrating, or distressing incidents that occur in everyday life. These may include disagreements, disappointments, and unpleasant occurrences, such as losing a wallet, getting stuck in a traffic jam, or arguing with a family member. Research suggests that daily hassles may be better predictors of psychological and physical health than major life events. It has been shown that people who reported being exposed to more frequent and intense hassles had poorer overall mental and physical health. Major events did have some long-term effects, but these effects may be due to the daily hassles that are associated with them.
It is true that a certain amount of stress is necessary for survival, and degrees of it can challenge the individual to grow in new ways. However, too much stress at inappropriate times can place excessive demands on the individual and interfere with integrated functioning. The questions to be asked are these: How much stress is too much, and what is a stressful life event? These questions lead the nurse to explore the significance of the event as it relates to the individual’s value system.
Appraisal of Stressors
Appraisal of a stressor involves determining the meaning of and understanding the impact of the stressful situation for the individual. It includes cognitive, affective, physiological, behavioral, and social responses. Appraisal is an evaluation of the significance of an event in relation to a person’s well-being. The stressor assumes its meaning, intensity, and importance by the unique interpretation and significance given to it by the person at risk.
Cognitive Responses.
Cognitive responses are a critical part of this model (Monat and Lazarus, 1991). Cognitive factors play a central role in adaptation. They account for the impact of the stressful event; the choice of coping patterns used; and the person’s emotional, physiological, behavioral, and social reactions.
Cognitive appraisal mediates psychologically between the person and the environment in any stressful encounter. This means that the damage or potential damage of a situation is determined on the basis of the person’s understanding of the situation’s ability to do harm and the resources the person has available to neutralize or tolerate the harm. The three types of cognitive responses to stress are as follows:
1. Harm/loss that has already occurred
2. Threat of anticipated or future harm
3. Challenge that focuses on potential gain, growth, or mastery rather than on the possible risks
The perception of challenge plays an important role in resilience, psychological hardiness or resistance to stress. Resilient people are less likely to become ill as a result of stressful life events as seen in Box 3-3 (Alim et al, 2008). Resilient people typically possess the following characteristics:
• Commitment―the ability to involve oneself in whatever one is doing
• Challenge―- the belief that change rather than stability is to be expected in life, so events are seen as stimulating rather than threatening
• Control―the tendency to feel and believe that one is influencing events, rather than feeling helpless in the face of life’s problems
In summary, resilient or stress-resistant people have a positive attitude toward life, an openness to change, a feeling of involvement in whatever they are doing, and a sense of control over events. Those who view stress as a challenge are more likely to turn events to their advantage and thus reduce their level of stress. In contrast, if a person uses passive, hostile, blaming, avoidant, or self-defeating tactics, the source of stress is not likely to resolve.
Affective Responses.
An affective response is the arousal of a feeling. In the appraisal of a stressor, the major affective response is a generalized anxiety reaction, which becomes expressed as emotions. These may include joy, sadness, fear, anger, acceptance, distrust, anticipation, or surprise.
Emotions also may be described according to their type, duration, and intensity—characteristics that change over time and as a result of events. For example, when an emotion continues over a long period of time, it can be classified as a mood; when prolonged over an even longer time, it can be considered an attitude. An insightful, optimistic, and positive attitude in dealing with life events can lead to greater feelings of well-being and perhaps even a longer life (Lazarus, 1991).
Physiological Responses.
Physiological responses reflect the interaction of several neuroendocrine axes involving growth hormones, prolactin, adrenocorticotropic hormones (ACTH), luteinizing hormones, follicle-stimulating hormones, thyroid-stimulating hormones, vasopressin, oxytocin, insulin, epinephrine, norepinephrine, and a variety of other neurotransmitters in the brain. The fight-or-flight physiological response stimulates the sympathetic division of the autonomic nervous system and increases activity of the pituitary-adrenal axis. In addition, stress has been shown to affect the body’s immune system, influencing one’s ability to fight disease.
Behavioral Responses.
Behavioral responses are the result of emotional and physiological responses, as well as one’s cognitive analysis of the stressful situation. Caplan (1981) described four phases of an individual’s behavioral responses to a stressful event:
• Phase 1 is behavior that changes the stressful environment or allows the individual to escape from it.
• Phase 2 is behavior that allows the individual to change the external circumstances and their aftermath.
• Phase 3 is intrapsychic behavior that serves to defend against unpleasant emotional arousal.
• Phase 4 is intrapsychic behavior that helps one come to terms with the event and its sequelae by internal readjustment.
Social Responses.
Finally, the possible social responses to stress and illness are many and are based on three activities (Mechanic, 1977):
1. Search for meaning, in which people seek information about their problem. This is necessary for devising a coping strategy because only through having some idea of what is occurring can one develop a reasonable response.
2. Social attribution, in which the person tries to identify the factors that contributed to the situation. Patients who see their problems as resulting from their own negligence may be “blocked” and not able to activate a coping response. They may see their problems as a sign of their personal failure and engage in self-blame and passive, defeatist, and withdrawn behavior.
3. Social comparison, in which people compare skills and capacities with those of others with similar problems. A person’s self-assessment depends very much on those with whom comparisons are made. The outcome is an evaluation of the need for support from the person’s social network or support system. Predisposing factors, such as age, developmental level, and cultural background, as well as the characteristics of the precipitating stressor, determine the perceived need for social support.
In summary the way a person appraises an event is the psychological key to understanding coping efforts and the nature and intensity of the stress response. Unfortunately, many nurses and other health professionals ignore this fact when they presume to know how certain stressors will affect a patient and thus provide “routine” care. This practice not only depersonalizes the patient but also undermines the basis of nursing care. The patient’s appraisal of life stressors, with its cognitive, affective, physiological, behavioral, and social components, must be an essential part of the psychiatric nurse’s assessment.
Coping Resources
Coping resources are options or strategies that help determine what can be done as well as what is at stake. They can take into account the coping options that are available, the chances that a given option will be successful and the likelihood that the person can apply a particular strategy effectively.
Coping resources are protective factors. They include economic assets, abilities and skills, social supports, and motivation, and incorporate all levels of the social hierarchy represented in Figure 3-1. Relationships among the individual, family, group, and society are critically important at this point of the model. Other coping resources include health and energy, spiritual supports, positive beliefs, problem-solving and social skills, social and material resources, and physical well-being.
• Spiritual beliefs can serve as a basis of hope and can sustain a person’s coping efforts under the most adverse circumstances.
• Problem-solving skills include the ability to search for information, identify the problem, weigh alternatives, and implement a plan of action.
• Social skills help solve problems involving other people, increase the likelihood of getting cooperation and support from others, and give the individual greater social control.
• Material assets refer to money and the goods and services that money can buy. Obviously, monetary resources greatly increase a person’s coping options in almost any stressful situation.
• Knowledge and intelligence are coping resources that allow people to identify different ways of dealing with stress.
• Strong ego identity, commitment to a social network, cultural stability, a stable system of values and beliefs, and a preventive health orientation are other coping resources.
Coping Mechanisms
It is at this point in the model that coping mechanisms emerge. This is an important time for nursing activities directed toward primary prevention. Coping mechanisms are any efforts directed at stress management and they can be constructive or destructive. The three main types of coping mechanisms are as follows:
1. Problem-focused coping mechanisms, which involve tasks and direct efforts to cope with the threat itself. Examples include negotiation, confrontation, and seeking advice.
2. Cognitively-focused coping mechanisms, by which the person attempts to control the meaning of the problem and thus neutralize it. Examples include positive comparison, selective ignorance, substitution of rewards, and the devaluation of desired objects.
3. Emotion-focused coping mechanisms, by which the patient is oriented to moderating emotional distress. Examples include the use of ego defense mechanisms, such as denial, suppression, or projection. A detailed discussion of coping and defense mechanisms appears in Chapter 15.
Coping mechanisms are constructive when anxiety is treated as a warning signal and the individual accepts it as a challenge to resolve the problem. In this way anxiety can be compared with a fever: both serve as warnings that the system is under attack. Once used successfully, constructive coping mechanisms modify the way past experiences are used to meet future threats. Destructive coping mechanisms ward off anxiety without resolving the conflict, using evasion instead of resolution.
Patterns of Response
According to the Stuart Stress Adaptation Model an individual’s response to stress is based on specific predisposing factors, the nature of the stressor, the perception of the situation, and an analysis of coping resources and mechanisms. Coping responses of the patient are then evaluated on a continuum of adaptation/maladaptation (see Figure 3-3).
• Responses that support integrated functioning are seen as adaptive. They lead to growth, learning, and goal achievement.
• Responses that block integrated functioning are seen as maladaptive. They prevent growth, decrease autonomy, and interfere with mastery of the environment.
Nursing Diagnoses
Responses to stress, whether actual or potential, are the subject of nursing diagnoses. A nursing diagnosis is a clinical judgment about individual, family, or community responses to stress. It is a statement of the patient’s problem from a nursing perspective that includes both the adaptive and maladaptive responses and contributing stressors. These responses may be overt, covert, existing, or potential and may lie anywhere on the continuum from adaptive to maladaptive. Formulating the diagnosis and implementing treatment are nursing functions for which the nurse is accountable. NANDA International (NANDA-I)–approved nursing diagnoses are listed in Appendix A.
Relationship to Medical Diagnoses
A medical diagnosis is the health problem or disease state of the patient. In the medical model of psychiatry, these health problems are mental disorders or mental illnesses. It is important for psychiatric nurses to distinguish between nursing and medical models of care, as shown in Figure 3-4. In particular, the following differences should be noted:

• Nurses assess risk factors and look for vulnerabilities; physicians assess disease states and look for causes.
• Nursing diagnoses focus on the adaptive/maladaptive coping continuum of human responses; medical diagnoses focus on the health/illness continuum of health problems.
• Nursing intervention consists of caregiving activities; medical intervention consists of curative treatments.
A nurse implements the nursing process for maladaptive responses based on the Stuart Stress Adaptation Model regardless of whether a physician has diagnosed the presence of a medical or psychiatric illness. Also, patients with a persistent psychiatric illness may be adapting well to it. People can successfully adapt to an illness without recovering from it. This is an important aspect of the Stuart Stress Adaptation Model. It means that psychiatric nurses can promote their patients’ adaptive responses regardless of their health or illness state.
Classifying Mental Disorders
Mental illnesses can be broadly differentiated as neurotic or psychotic. Neuroses have the following characteristics:
• A symptom or group of symptoms is distressing and is recognized as unacceptable and alien to the individual.
• Behavior does not violate major social norms (although functioning may be significantly impaired).
• The disturbance is enduring or recurrent without treatment and is not a short-term reaction to stressors.
However, in situations of extreme conflict, the person may distort reality, such as in psychosis. Psychosis consists of the following characteristics:
This last characteristic is critical. When people demonstrate gross impairment in reality testing, their perceptions are not accurate and they draw incorrect inferences about external reality, even in the face of contrary evidence. Direct evidence of psychosis is the presence of delusions or hallucinations without insight into their pathological nature. Psychotic health problems reflect the most severe level of psychiatric illness.
DSM-IV-TR.
Medical diagnoses are classified according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR) of the American Psychiatric Association (2000). The fifth edition of the DSM is scheduled for publication in 2013 (Kupfer and Reiger, 2010). The various illnesses are accompanied by a description of diagnostic criteria, tested for reliability by psychiatric practitioners. It has been noted, however, that the DSM diagnoses are not as precise as the diagnostic processes in the rest of medicine (Kendler, 2008; Pierre, 2010).
DSM-IV-TR uses a multiaxial system of various mental disorders, general medical conditions, aspects of the environment, and areas of functioning that might be overlooked if the focus were only on assessing a single presenting problem. Thus the individual is evaluated on the following axes:
• Axis II: Personality disorders
• Axis III: General medical conditions
Axes I and II include the entire classification of mental disorders plus conditions that are not attributable to a mental disorder but that are a focus of attention or treatment. Axis III allows the clinician to identify any physical disorder relevant to the understanding or treatment of the individual. Axis IV is for reporting psychosocial and environmental problems that may affect the diagnosis, treatment, and prognosis of mental disorders. Axis V is for reporting the clinician’s judgment of the individual’s overall level of functioning. This information is useful in planning treatment, measuring its impact, and predicting outcomes (Smith et al, 2011). Axes I to V are presented in Appendix B. Psychiatric nurses use all five axes of the DSM-IV-TR and integrate the axes with related nursing diagnoses.
Cultural formulation
In addition to Axes I to V, the DSM-IV-TR has an outline for cultural formulation designed to help the clinician in systematically evaluating the person’s cultural and social reference group and ways in which the cultural context is relevant to clinical care (Chapter 7). It is suggested that the clinician provide a narrative summary of the evaluation of the categories listed in Box 3-4 (see Appendix B for added detail).
The DSM-IV-TR also includes a list of culture-bound syndromes that are recurrent, locality-specific patterns of aberrant behavior and troubling experiences that may be linked to a particular DSM-IV-TR diagnostic category (Table 3-1). Although behaviors related to most DSM-IV-TR categories can be found throughout the world, the particular symptoms, course of illness, and social response are often influenced by cultural factors. In contrast, culture-bound syndromes are generally limited to specific societies or culture areas and are localized, folk, diagnostic categories that give coherent meanings for certain common, patterned, and troubling sets of experiences and observations.
TABLE 3-1
COMMON CULTURE-BOUND SYNDROMES
| SYNDROME | REGION/POPULATION AFFECTED | DESCRIPTION |
| Amok | Malaysia | This is a dissociative episode typically preceded by a period of reflection and brooding, followed by an outburst of violent, aggressive, or homicidal behavior directed at people and objects. If the attacker is not killed, they often collapse and claim amnesia upon gaining consciousness. |
| Ataque de nervios | Latin America | Its literal translation is “attack of the nerves.” The symptoms are transient, typically occur suddenly in response to a severe psychosocial stressor, and include impulsive, dramatic behaviors such as screaming uncontrollably, crying, trembling and nervousness, and anger and violence. |
| Brain fag | West Africa | Seen predominantly in male West African students, it generally manifests as vague somatic symptoms, depression, and difficulty concentrating. |
| Koro | South and east Asia | In men, it is the belief that the genitals are retracting into the abdomen, are shrinking and will soon disappear. For females, the belief focuses on the nipples retracting or shrinking. It is associated with anxiety symptoms. |
| Mal de ojo (“evil eye”) | Mediterranean cultures and elsewhere in the world | Sometimes called “evil eye,” it is a folk illness which most commonly affects children. It has been defined as a hex caused by a gaze from a more powerful or stronger person looking a weaker person (usually an infant or child but sometimes a woman). Symptoms include headaches, high fever, diarrhea, not sleeping well, increased fussiness, and weeping. |
Treatment Stages and Activities
The final aspect of the Stuart Stress Adaptation Model is the integration of the theoretical basis, biopsychosocial components, patterns of response, and nursing activities based on the patient’s treatment stage. Once patterns of coping responses have been identified, the nurse determines the patient’s treatment stage and implements the most appropriate nursing activities. The model identifies four possible treatment stages: (1) crisis, (2) acute, (3) health maintenance, and (4) health promotion. These stages reflect the range of the adaptive/maladaptive continuum and suggest a variety of nursing activities. For each stage the nurse identifies the treatment goal, focus of the nursing assessment, nature of the nursing intervention, and expected outcome of nursing care (Figure 3-5).

Health Promotion Stage
Nursing goal: achievement of the patient’s optimal level of wellness
Nursing assessment: focuses on the patient’s quality of life and well-being
Nursing intervention: directed toward inspiring and validating the patient
Nursing expected outcome of care: optimal quality of life for the patient
This aspect of the model moves the field of psychiatric nursing beyond the usual activities associated with the stabilization of patients in crisis and remission of the acutely ill patient’s symptoms. It identifies nursing responsibilities in the health maintenance and health promotion treatment stages as improving patients’ functional status, enhancing their quality of life, and preventing future health problems.
These treatment stages are often overlooked but they are essential aspects of the contemporary psychiatric nursing role. These stages also relate to the levels of prevention in psychiatric care and the clinical chapters of this text, as shown in Table 3-2.
TABLE 3-2
STAGES OF TREATMENT RELATED TO LEVELS OF PREVENTION AND CHAPTERS OF THE TEXT
| STAGE OF TREATMENT | LEVEL OF PREVENTION | CHAPTER(S) |
| Health promotion | Primary prevention | 12: Prevention and Mental Health Promotion |
| Crisis | Secondary prevention | 13: Crisis Intervention |
| Acute | Secondary prevention | 15-25: Clinical chapters |
| Health maintenance | Tertiary prevention | 14: Recovery Support |
The synthesis of all elements of the Stuart Stress Adaptation Model of psychiatric nursing care is displayed in Figure 3-6. These elements also are summarized in Table 3-3. On the far left side of Figure 3-6 one can see the many theories that contribute to psychiatric nursing care. On the far right side are the six steps of the nursing process. In the middle of the figure, the top portion shows the impact of predisposing factors, precipitating stressors, appraisal of stressors, coping resources, and coping mechanisms, all of which lead to either adaptive or maladaptive coping responses and related nursing diagnoses. Also in the middle of the figure one sees each treatment stage with its related treatment goal, nursing assessment, nursing intervention, and expected outcome of care.
TABLE 3-3
SUMMARY OF THE ELEMENTS OF THE STUART STRESS ADAPTATION MODEL
| ELEMENT | DEFINITION | EXAMPLES |
| Predisposing factors | Risk factors that influence both type and amount of resources person can elicit to cope with stress | Genetic background, intelligence, self-concept, age, ethnicity, education, gender, belief systems |
| Precipitating stressors | Stimuli that person perceives as challenging, threatening, or demanding and that require excess energy for coping | Life events, injury, hassles, strains |
| Appraisal of stressor | Evaluation of significance of a stressor for a person’s well-being, considering stressor’s meaning, intensity, and importance | Hardiness, perceived seriousness, anxiety, attribution |
| Coping resources | Evaluation of a person’s coping options and strategies | Finances, social support, ego integrity |
| Coping mechanisms | Any effort directed at stress management | Problem solving, compliance, defense mechanisms |
| Continuum of coping responses | Range of adaptive or maladaptive human responses | Social changes, physical symptoms, emotional well-being |
| Treatment stage activities | Range of nursing functions related to treatment goal, nursing assessment, nursing intervention, and expected outcome | Environment management, patient teaching, role modeling, advocacy |

Chapters 15 through 25 of this text explore various maladaptive coping responses and related medical diagnoses. The phases of the nursing process are described for patients with maladaptive responses. Each chapter begins with a continuum of coping responses, followed by a discussion of behaviors, predisposing factors, precipitating stressors, appraisal of stressor, coping resources, coping mechanisms, nursing diagnoses, and related interventions. Through consistent application of the Stuart Stress Adaptation Model, the art and science of psychiatric nursing practice emerge.