Clinical Approach to Regional Dermatoses
• Some inflammatory, infectious, metabolic, neoplastic, and genetic skin conditions have a predilection for particular areas of the body.
• This chapter addresses the diagnosis and treatment of regional dermatoses affecting the hands, feet, intertriginous regions, diaper area, lips, and eyelids.
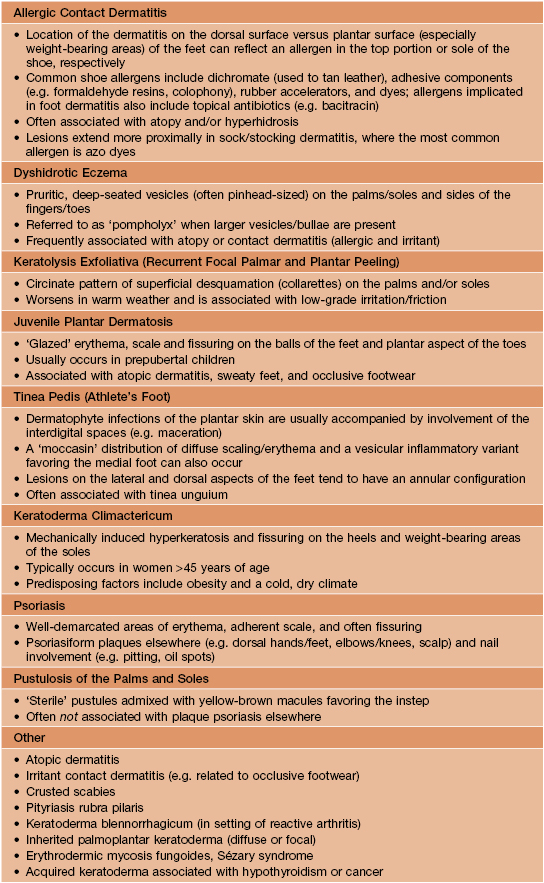
Dermatitis of the Hands and Feet
• An approach to the classification of hand dermatitis is presented in Fig. 13.1, and the differential diagnosis of foot dermatitis is summarized in Table 13.1.
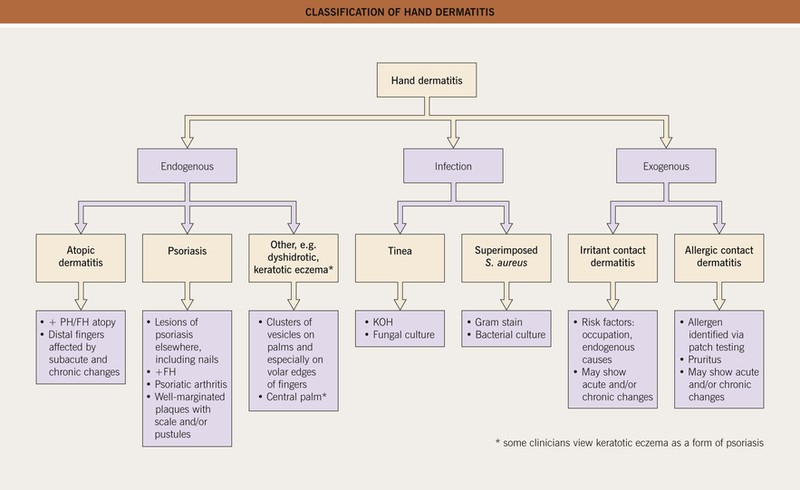
Fig. 13.1 Classification of hand dermatitis. More than one etiology may be present, e.g. atopic dermatitis plus irritant contact dermatitis. FH, family history; PH, personal history. Courtesy, David E. Cohen, MD.
• Because the hands and feet have a thicker stratum corneum than other areas of the body, percutaneous absorption of topical medications is decreased.
• High-potency topical CS or the use of occlusion may be needed to effectively treat inflammatory dermatoses in these sites.
Intertriginous Dermatitis
• Intertriginous areas include the inguinal creases, gluteal cleft, axillae, inframammary folds, and beneath pannus in obese patients.
• The differential diagnosis of dermatitis in the major skin folds is presented in Fig. 13.2.
Table 13.2
Symmetrical drug-related intertriginous and flexural exanthema (SDRIFE): clinical criteria.
This entity is also referred to as drug-induced intertrigo, flexural drug eruption, and baboon syndrome. The latter term is also used for a form of systemic contact dermatitis.
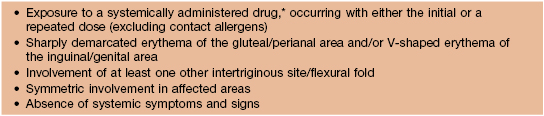
* Not a chemotherapeutic agent, so distinct from toxic erythema of chemotherapy.
Adapted from Häusermann P, Harr TH, Bircher AJ. Baboon syndrome resulting from systemic drugs: Is there strife between SDRIFE and allergic contact dermatitis syndrome? Contact Dermatitis 2004;51:297–310.
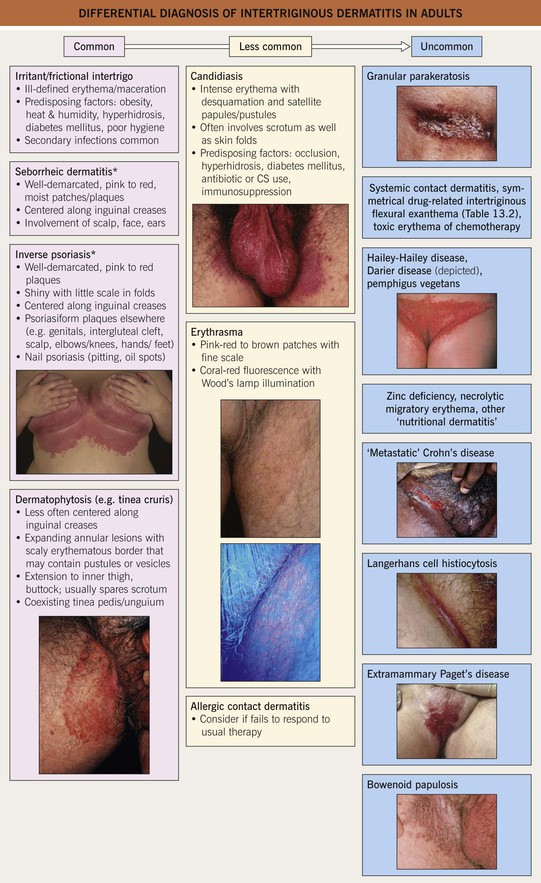
Fig. 13.2 Differential diagnosis of intertriginous dermatitis in adults. Individual patients often have multiple disorders superimposed upon one another. Bullous impetigo and streptococcal intertrigo are considerably more common in children than adults (see Fig. 13.4). *The term ‘sebopsoriasis’ may be used when features of both seborrheic dermatitis and psoriasis are present. Insets: Courtesy, Eugene Mirrer, MD; Louis Fragola, Jr., MD; David Mehregan, MD and Robert Hartman, MD.
• Other conditions with a predilection for intertriginous regions include skin tags, hidradenitis suppurativa, Fox–Fordyce disease, scabies, erythema migrans, variants of lichen planus (e.g. inverse, pigmentosus), inverse pityriasis rosea, vitiligo, lentigines in the setting of neurofibromatosis type 1, Dowling–Degos disease, and pseudoxanthoma elasticum.
• Occlusion and a high level of cutaneous hydration in intertriginous sites increase the absorption of topical medications.
• Low-potency topical CS are often effective for dermatoses in these areas, and prolonged use of more potent agents (including antifungal combination products; see below) has increased potential to result in side effects such as cutaneous atrophy (Fig. 13.3).

Fig. 13.3 Cutaneous atrophy in the inguinal fold from chronic use of a topical CS. This 10-year-old girl's seborrheic dermatitis had been treated with a mid-potency topical CS on a daily basis for several years, resulting in the development of striae. Courtesy, Julie V. Schaffer, MD.
Diaper Dermatitis
• Develops in >50% of infants and has a variety of causes (Fig. 13.4).
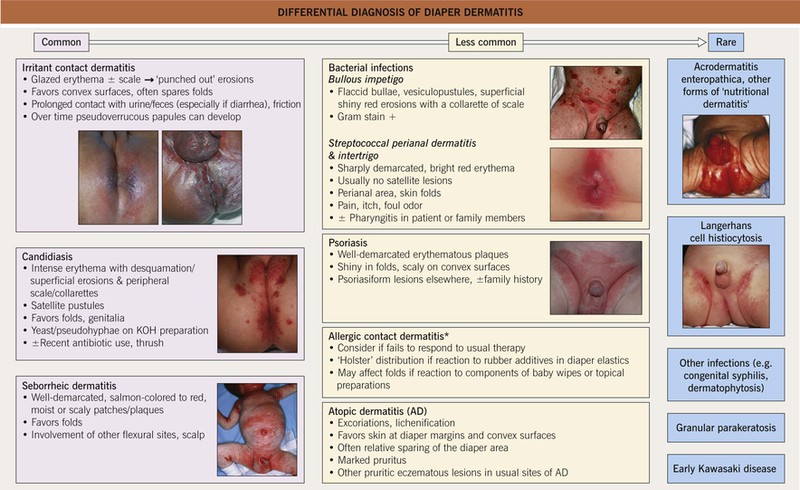
Fig. 13.4 Differential diagnosis of diaper dermatitis. Patients often have a combination of disorders, one superimposed upon another. Discrete papules or nodules can be seen in scabies, granuloma gluteale infantum, and perianal pseudoverrucous papules, whereas congenital syphilis may present with erosions or even ulcerations. *Potential allergens include sorbitan sesquioleate (an emulsifier in diaper balms), fragrances, disperse dyes, rubber additives (e.g. mercaptobenzothiazole), preservatives in baby wipes, and diaper components. Insets: Courtesy, Robert Hartman, MD, and Julie V. Schaffer, MD.
• Dampness and exposure to urine and feces represent factors in the etiology of irritant and infectious forms of diaper dermatitis.
• Frequent changing of highly absorbent disposable diapers decreases the incidence and severity of diaper dermatitis.
• Seborrheic dermatitis and psoriasis in the diaper area predispose infants and toddlers to other forms of diaper dermatitis.
• An exuberant, multifactorial diaper dermatitis (e.g. sebopsoriasis with Candida or bacterial superinfection) can trigger the rapid development of numerous small, scaly erythematous papules in a widespread distribution on the trunk and extremities (psoriasiform ‘id’ reaction).
• Mild topical CS are helpful for the inflammatory component of irritant dermatitis and primary dermatoses in the diaper area, while topical imidazole creams treat candidiasis and have additional anti-inflammatory effects; these agents can be used together for seborrheic dermatitis or psoriasis.
• Combination products containing a potent CS (e.g. Lotrisone® [clotrimazole + betamethasone dipropionate], Mycolog® [nystatin + triamcinolone]) and long-term daily use of any CS in the diaper area should be avoided (see above).
• Barrier ointments containing zinc oxide provide protective and soothing effects; a thick layer should be used (following application of anti-inflammatory/antimicrobial agents if needed) with each diaper change in patients with diaper dermatitis.
Cheilitis
• The differential diagnosis of cheilitis and clues to determining the etiology are outlined in Fig. 13.5.
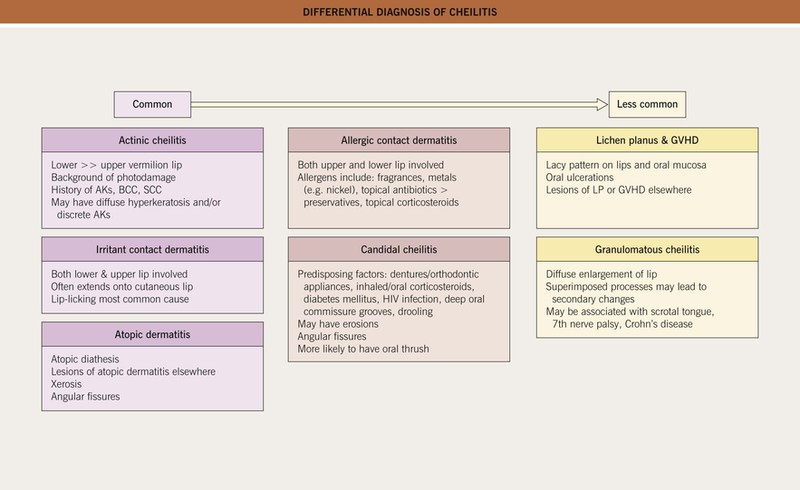
Fig. 13.5 Differential diagnosis of cheilitis. A combination of etiologies is often present, e.g. atopic dermatitis plus irritant contact dermatitis. Other uncommon causes include cheilitis glandularis, actinic prurigo, lichen sclerosus, and nutritional deficiencies. AKs, actinic keratoses; LP, lichen planus. Courtesy, Jean L. Bolognia, MD.
Eyelid Dermatitis
• An approach to the classification of eyelid dermatitis is presented in Fig. 13.6.
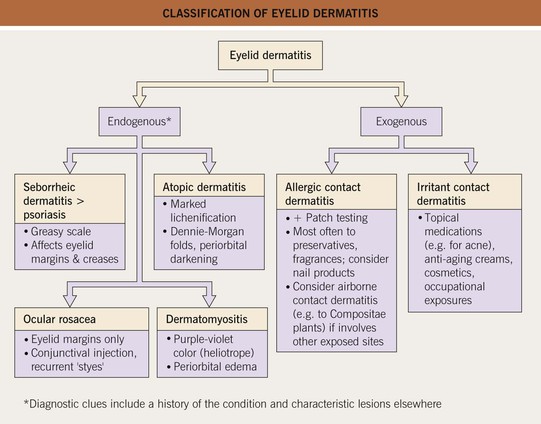
Fig. 13.6 Classification of eyelid dermatitis. More than one etiology may be present, e.g. atopic dermatitis plus irritant contact dermatitis.
• Low-potency topical CS are often effective for dermatitis on the eyelids because of the delicate skin in this site, and prolonged CS use (especially of more potent agents) may potentially lead to ocular side effects.
For further information see Chs. 13 and 15. From Dermatology, Third Edition.