Vascular Neoplasms and Reactive Proliferations
Lesions of vascular origin are broadly, and somewhat imperfectly, classified as neoplasms (tumors), malformations, telangiectasias, or reactive proliferations. The growth of a neoplasm is largely autonomous (i.e. not reactive). Malformations, in general, are not actively proliferating (see Chapter 85). Telangiectasias represent pre-existing capillaries that are persistently dilated but lack a proliferative component (see Chapter 87). Reactive proliferations represent endothelial cell proliferation that is in response to some factor (e.g. fibrin, hypoxia, trauma).
Neoplasms/Tumors
Cherry Angioma
• Bright red, 1- to 6-mm papule, commonly on the trunk or upper extremities (Fig. 94.1); appears during adulthood; early, tiny lesions can be macular.
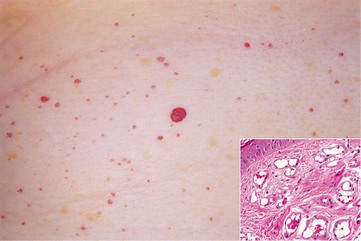
Fig. 94.1 Cherry angiomas. Multiple, slightly compressible red papules. Histologically, congested capillaries and postcapillary venules expand the papillary dermis (insert). Courtesy, Jean L. Bolognia, MD.
• Dermoscopy: red to red-blue lacunas (well-demarcated round to oval red to red-blue structures).
Glomus Tumor
• Solitary, painful papule or nodule on the extremities, or in the nail bed (beneath the nail plate) in young adults (Fig. 94.2).

Fig. 94.2 Glomus tumor. The lesion presented with pain and ill-defined subungual erythema. Courtesy, Ronald P. Rapini, MD.
• A glomus cell is a perivascular contractile cell that influences vessel diameter as a means of controlling temperature.
Tufted Angioma
• Pink to dark red patches and plaques with superimposed papules (Fig. 94.3) that slowly enlarge and occasionally regress.

Fig. 94.3 Tufted angioma. Mottled red patches and superimposed papules are typical clinical features. Courtesy, Julie V. Schaffer, MD.
• Commonly found on the neck and trunk.
• Congenital or acquired during childhood or young adulthood.
• On a spectrum with kaposiform hemangioendothelioma.
• Early-onset lesions can be associated with Kasabach–Merritt phenomenon (consumptive coagulopathy with decreased platelets).
Hobnail Hemangioma/Targetoid Hemosiderotic Hemangioma
• Uncommon red-purple papule on the trunk or extremities of children or young adults; papule may have a surrounding pale area and outer ecchymotic ring, thus creating a target lesion (Fig. 94.4).

Fig. 94.4 Hobnail hemangioma (targetoid hemosiderotic hemangioma). Note the target-like appearance. Courtesy, Ronald P. Rapini, MD.
Kaposiform Hemangioendothelioma
• Ill-defined, pink to violaceous plaques or nodules (Fig. 94.5); sometimes deeply seated; any site.

Fig. 94.5 Kaposiform hemangioendothelioma complicated by Kasabach–Merritt phenomenon. A large red-purple mass on the upper flank of an infant.
• May be congenital and generally appears by 2 years of age.
• Locally aggressive, persistent.
• Associated with Kasabach–Merritt phenomenon (treated with rapamycin or vincristine).
Kaposi's Sarcoma
• Multifocal systemic disease; extramucocutaneous sites include gastrointestinal tract, lymph nodes, and lungs.
• Four main variants: (1) older men from the Mediterranean basin or of Ashkenazi Jewish descent with lesions on the lower extremities (Fig. 94.6); (2) African endemic; (3) iatrogenic/immunocompromised; and (4) AIDS-related epidemic (Fig. 94.7).

Fig. 94.6 Classic Kaposi's sarcoma. Red macules and patches on the plantar surface of the foot, with violaceous plaques on the ankle. Courtesy, Paula North, MD.

Fig. 94.7 Kaposi's sarcoma in a patient with AIDS. Violet-red papules or nodules are often oval to lance-ovate and are usually more widely distributed than in classic KS. Courtesy, Paula North, MD.
• Pink to dark violet patches and plaques; with time, can become nodular.
• May have mucosal involvement, e.g. oral.
• Associated with HHV-8 infection.
• Histopathology varies from a subtle increase in slit-like vessels to nodular proliferations of spindle cells; HHV-8 can be detected in endothelial cells by immunohistochemistry.
• Rx: observation, surgical excision, laser removal, radiotherapy, intralesional or systemic vinblastine, taxanes, liposomal anthracyclines, reduction of immunosuppression.
Angiosarcoma
• Begins as a bruise-like patch in the head and neck region of older adults with color varying from pink to dark purple (likened to the color of an eggplant).
• With time nodules and ulceration can develop.
• Associated with lymphedema (Fig. 94.8).

Fig. 94.8 Angiosarcoma. Erythematous and purple hemorrhagic plaques as well as grouped vesicles with clear or hemorrhagic fluid (reminiscent of microcystic lymphatic malformation) are present. There is also induration and a pink hue to the left side of the face in addition to evidence of previous excisions and radiotherapy. Courtesy, Lorenzo Cerroni, MD.
• Rx: wide excision ± radiotherapy; consider systemic therapy with taxanes, sorafenib, or bevacizumab for larger lesions.
Malformations (See Chapter 85)
Glomuvenous Malformation (Previously Referred to as Glomangioma)
• Often multiple, bluish, partially compressible papulonodules that appear during infancy or childhood (Figs. 94.9 and 94.10); may be tender.

Fig. 94.9 Glomuvenous malformation (‘glomangioma’). Note the cluster of slightly compressible blue papules.

Fig. 94.10 Glomuvenous malformation (‘glomangioma’). Large cluster of blue papulonodules becoming confluent centrally.
• Autosomal dominant inheritance with incomplete penetrance.
• DDx: venous malformations or blue rubber bleb nevus syndrome (see Chapter 85).
Reactive Proliferations
• Some consider pyogenic granuloma, angiolymphoid hyperplasia with eosinophilia, and glomeruloid hemangioma to be tumors.
Pyogenic Granuloma
• Rapidly growing, friable, red papulonodule that is sometimes pedunculated; often ulcerates and bleeds; common in children and young adults.
• Gingival and fingers > lips > face > tongue (Fig. 94.11).



Fig. 94.11 Pyogenic granuloma. A Eroded pink-red papulonodule with a narrow base on the scalp. B Pedunculated papule on the finger. C Grouped red papules on the lip. The latter two are both common sites. By dermoscopy, red homogenous areas are intersected by white lines. A, Courtesy, Julie V. Schaffer, MD; B, C, Courtesy, Paula North, MD.
• May arise on the gingiva of pregnant women (granuloma gravidarum).
• Multiple tumors (especially periungual) may be seen in association with medications (e.g. oral retinoids, anti-retroviral protease inhibitors, EGFR inhibitors).
Angiolymphoid Hyperplasia with Eosinophilia
• Pink to red-brown nodules or plaques, often multiple and grouped.
• Favors the head and neck region, especially around ears (Fig. 94.12).

Fig. 94.12 Angiolymphoid hyperplasia with eosinophilia. Multiple pink papulonodules are often seen on the scalp.
Glomeruloid Hemangioma
• Firm red papules or nodules on the trunk and proximal extremities.
• Associated with POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin findings) syndrome.
Reactive Angioendotheliomatosis
• Erythematous nodules or plaques, often with petechiae or purpura.
• Associated with cryoglobulinemia (type I) or systemic disorders (e.g. renal failure).
• The form due to severe atherosclerosis leads to ulceration.
Diffuse Dermal Angiomatosis
• Some consider this a variant of reactive angioendotheliomatosis.
• This term has been used to describe an ulcerated lesion in the setting of severe atherosclerosis or vascular compromise; these ulcers usually occur on the lower extremities and resolve with revascularization; less often occurs on the breast.
For further information see Ch. 114. From Dermatology, Third Edition.