Common Soft Tissue Tumors/Proliferations
Neural/Neuroendocrine
Neurofibroma
• Skin-colored to pink, soft papulonodule, often on the trunk (see Fig. 50.2).
• Compressible (the tumor often herniates inward upon palpation – this is referred to as the ‘button-hole’ sign); it is sometimes pedunculated.
• Usually solitary in most individuals.
• When multiple, need to distinguish linear form (segmental; mosaic) from a generalized distribution pattern (neurofibromatosis type I) (see Chapter 50).
• Histopathology: wavy, delicate spindle cells with tapered nuclei in a pink stroma.
• Plexiform type has been likened to a ‘bag of worms’ (Fig. 95.1); it is generally on the trunk and proximal extremities, highly associated with neurofibromatosis type I, and prone to malignant degeneration (2–13%).

Fig. 95.1 Plexiform neurofibroma in a child with neurofibromatosis. Bag-like mass with overlying patches of hyperpigmentation. Courtesy, Zsolt B. Argenyi, MD.
Schwannoma/Neurilemmoma
• Solitary, pink-yellow, soft, smooth papulonodule; generally seen in adults.
• Often on the extremities or head (Fig. 95.2).

Fig. 95.2 Solitary schwannoma. Skin-colored nodule on the plantar surface of the great toe. Courtesy, Julie V. Schaffer, MD.
• Asymptomatic (rarely painful).
• Histopathology: encapsulated tumor with foci of wavy, spindled nuclei in palisades and foci of myxoid change.
Granular Cell Tumor
• Often in adults; skin-colored to brown-red, firm papulonodule; sometimes ulcerated or verrucous.
• Multiple tumors in 10% of patients.
• Histopathology: polygonal cells with oval nuclei and characteristic granular cytoplasm.
Traumatic Neuroma
• Skin-colored papulonodule(s) at a site of prior trauma.
• Often painful or ‘sensitive’ (Fig. 95.3).

Fig. 95.3 Traumatic neuroma. A painful, firm papule that appeared after a deep puncture injury. Courtesy, Zsolt B. Argenyi, MD.
• Histopathology: haphazardly distributed fascicles of spindle cells with tapered nuclei.
Merkel Cell Carcinoma
• In older adults; solitary, rapidly growing, pink to red to violaceous nodule (Fig. 95.4).

Fig. 95.4 Merkel cell carcinoma (primary cutaneous neuroendocrine carcinoma). Eroded erythematous nodule arising within sun-damaged skin of the cheek. Courtesy, Lorenzo Cerroni, MD.
• Commonly on the head and neck.
• Aggressive behavior: distant metastases in 40%; 70% survival at 5 years if primary lesion is <2 cm in diameter; 18% survival at 5 years if distant metastatic disease.
• Histopathology: islands or trabeculae of blue cells that on high-power magnification have chromatin that appears speckled like ‘salt and pepper’; characteristically cytokeratin 20 (CK20)-positive and thyroid transcription factor-1 (TTF1)-negative.
• Rx: optimally includes wide excision, accompanied by sentinel lymph node biopsy (SLNB); adjuvant radiation treatment recommended for most patients (exceptions: primary ≤1 cm, SLNB negative, no immunosuppression).
Fibrous/Fibrohistiocytic
Skin Tag (Acrochordon, Fibroepithelial Polyp, Soft Fibroma)
• Common; skin-colored to pink or occasionally hyperpigmented, pedunculated papule.
• Sites of predilection: neck, axilla, groin (Fig. 95.5).

Angiofibroma (Fibrous Papule)
• Solitary, skin-colored to pink, shiny papule; commonly on the nose (Fig. 95.6).

Fig. 95.6 Fibrous papule of the nose. A smooth, dome-shaped, skin-colored papule. Courtesy, Hideko Kamino, MD.
• When multiple, need to consider genodermatoses (e.g. tuberous sclerosis, multiple endocrine neoplasia type I).
• Histopathology: stellate spindle cells in a hyalinized stroma with dilated vessels.
• DDx: basal cell carcinoma, intradermal melanocytic nevus, adnexal tumors.
Pearly Penile Papules
• Multiple, small, white to light pink papules along the corona of the glans penis, often with a multilayered distribution (Fig. 95.7).

Fig. 95.7 Pearly penile papules. Multiple small white papules along the corona of the glans penis. Note the multilayered distribution. Courtesy, Kalman Watsky, MD.
Dermatofibroma
• 6- to 10-mm pink (especially in fair-skinned individuals), tan, or brown papule (Fig. 95.8); firm; dimples inward with lateral pressure.
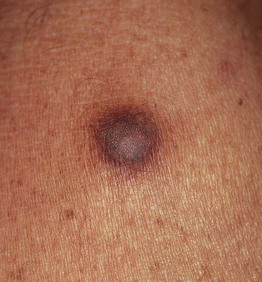
Fig. 95.8 Dermatofibroma. Hyperpigmented firm papule on the lower extremity. Courtesy, Jean L. Bolognia, MD.
• Often on the lower extremities; women > men.
• Common; multiple lesions can be seen in normal individuals but also are associated with lupus erythematosus and immunosuppresion (e.g. HIV infection).
• Histopathology: epidermal hyperplasia (sometimes with basaloid induction that resembles basal cell carcinoma) above a spindle cell proliferation that entraps collagen.
• Dermoscopic features are shown in Fig. 1.13.
Acral Fibrokeratoma
• 4- to 10-mm solitary, skin-colored to pink, cone-shaped, keratotic papule with a collarette of elevated skin (Fig. 95.9).

Fig. 95.9 Acral fibrokeratoma. A light pink exophytic papule arising from the dorsal surface of the finger. Courtesy, Hideko Kamino, MD.
Sclerotic Fibroma
• 2- to 9-mm dome-shaped, pearly papule or nodule in adults.
Giant Cell Tumor of Tendon Sheath
• Firm nodule (1–2 cm), generally on the fingers or toes (Fig. 95.10).

Fig. 95.10 Giant cell tumor of tendon sheath. A skin-colored nodule on the lateral aspect of the index finger. Courtesy, Hideko Kamino, MD.
Nodular Fasciitis
• Benign, reactive process in young adults.
• Rapidly growing subcutaneous nodule (1–5 cm in diameter).
• Commonly on the distal upper extremity.
• Sometimes associated with trauma.
• Histopathology: subcutaneous nodule of elongated spindle cells in a myxoid matrix.
Connective Tissue Nevus
• Skin-colored to yellow-tan (more yellow when composed predominantly of elastic tissue), firm papulonodules or plaques; solitary or multiple (often grouped) (Fig. 95.11).

Fig. 95.11 Connective tissue nevus. Coalescence of multiple tan papules and plaques on the lower back. The lesion was firm to palpation and histologically had increased collagen.
• Present at birth or arise during childhood.
• May be associated with genodermatoses (e.g. tuberous sclerosis, Buschke–Ollendorf syndrome, Proteus syndrome).
• Histopathology: increased collagen (sometimes subtle) and/or elastic tissue; diagnosis may require special stains for elastic fibers and collagen.
Infantile Digital Fibroma
• Firm, skin-colored to pink papulonodule on the fingers or toes (tends to spare the thumb and great toe) (Fig. 95.12).

Fig. 95.12 Infantile digital fibroma. Firm skin-colored nodule on the dorsolateral aspect of the second toe in a young child.
• Solitary or multiple; generally present before 1 year of age.
Infantile Myofibromatosis
• One or more skin-colored to pink to violet, firm to rubbery dermal/subcutaneous nodules.
• Most commonly on the head and neck or trunk.
• Rare; lesions present at birth or appear during the first 2 years of life.
• Can have cutaneous lesions alone or systemic involvement (bone, gastrointestinal, kidneys, lungs, heart).
• Tumors tend to self-regress.
• Histopathology: biphasic pattern of spindle cells in nodular arrangements with vessels at the periphery.
Fibromatoses
• Five subtypes, four of which are superficial: (1) palmar (Dupuytren's contracture); (2) plantar (Ledderhose disease); (3) penile (Peyronie's); and (4) knuckle pads (Fig. 95.13).

Fig. 95.13 Knuckle pads. Note the localization to the skin overlying the knuckles. Courtesy, Ronald P. Rapini, MD.
• One deep form: extra-abdominal desmoid tumor.
• Slowly growing nodules or plaques or cord-like tumors.
• Palmar fibromatosis can result in flexion contractures, especially of the 4th and/or 5th finger (see Chapter 81).
• Penile fibromatosis can result in pain and erectile dysfunction.
Muscle/Adipose
Leiomyoma
• Solitary or multiple red-brown papules or nodules, often grouped (Fig. 95.14).

Fig. 95.14 Clustered piloleiomyomas on the back. The trunk is a common location for multiple piloleiomyomas. Patients with this clinical presentation need to be evaluated for the possibility of Reed syndrome.
• When multiple, consider association with uterine leiomyomas and papillary renal cell carcinoma (Reed syndrome).
• Histopathology: fascicles of spindle cells with cigar-shaped nuclei that have perinuclear vacuoles.
Smooth Muscle Hamartoma
• Congenital or acquired, skin-colored to hyperpigmented plaque on the trunk > proximal extremities (Fig. 95.15).

Fig. 95.15 Smooth muscle hamartoma. This infant presented with a firm plaque on the thigh. Courtesy, Ronald P. Rapini, MD.
• Follicular prominence and hypertrichosis may be present.
Lipoma
• Common tumor of mature fat; soft, mobile subcutaneous nodule.
• Generally on the trunk and extremities, but any site possible.
• Multiple lesions may be associated with a lipomatosis (e.g. familial type; Fig. 95.16) or a genodermatosis (e.g. Gardner syndrome, Proteus syndrome).

• DDx: see Fig. 95.17.
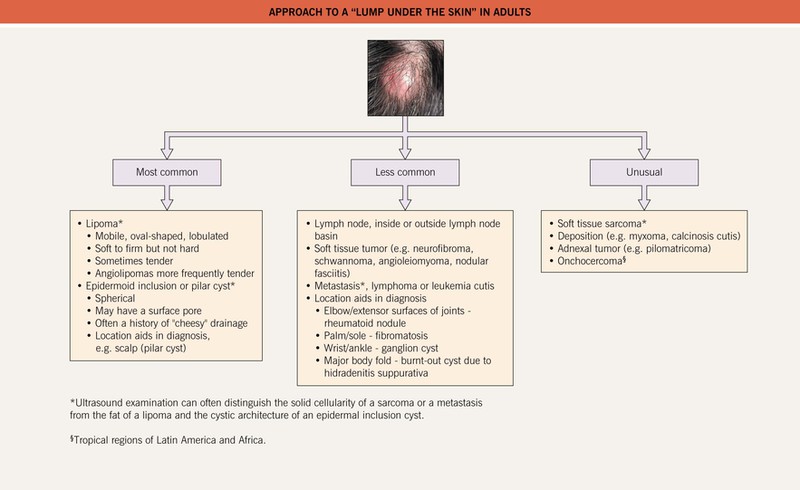
Fig. 95.17 Approach to a “lump under the skin” in adults. Incisional biopsy is preferred for the histopathologic evaluation of subcutaneous nodules while a punch biopsy suffices for dermal lesions. For bedside diagnosis of an epidermal inclusion cyst: after local anesthesia and superficial incision with a #11 blade, keratin is expressed.
Nevus Lipomatosus
• Grouped, soft, yellow to skin-colored papulonodules on the hips and/or upper thighs (Fig. 95.18).
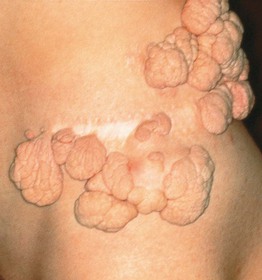
Fig. 95.18 Nevus lipomatosus superficialis. This hamartoma is characterized by grouped, soft, pedunculated, skin-colored tumors; a partial resection had been performed. With permission from Kopf AW and Bart RS, J. Dermatol. Surg. Oncol. 9:279–281, 1983.
Soft Tissue Sarcomas (See Table 95.1)
• Rare in comparison to benign soft tissue tumors.
• Generally presents as a nonspecific, deep-seated nodule.
• Dermatofibrosarcoma protuberans (DFSP) is characteristically multinodular (Fig. 95.19).
• Most DFSPs have a translocation t(17;22) that fuses the collagen I and platelet-derived growth factor genes; expression of this fusion gene results in high levels of platelet-derived growth factor that stimulates proliferation of fibroblasts.
Table 95.1
Selected soft tissue sarcomas.
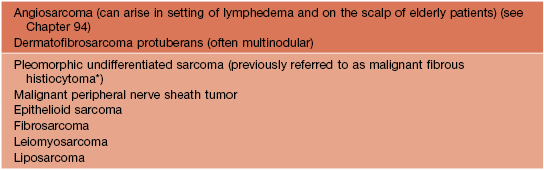
* Some pathologists consider atypical fibroxanthoma (AFX) to be a superficial variant of malignant fibrous histiocytoma (MFH); dermatologists see AFXs more commonly than MFHs.

Fig. 95.19 Dermatofibrosarcoma protuberans. A broad, pink-brown, multinodular, firm plaque on the back. Histopathologically, bland spindle cells are arranged in storiform (‘cartwheel’) patterns. Courtesy, Hideko Kamino, MD.
For further information see Chs. 115, 116 and Ch. 117. From Dermatology, Third Edition.