Allergic and Nonallergic Rhinitis
Introduction
Chronic rhinitis is an increasingly common condition that is now recognized to have a major impact on human health. Persistent nasal dysfunction may have significant effects on physical and emotional functioning, which result in absences from school and work, reduced worker productivity, and impaired school performance. In addition, chronic nasal inflammation may aggravate or lead to the development of other significant disorders, including asthma, rhinosinusitis, and middle ear disease. Recent improvements in current understanding of the pathologic mechanisms of rhinitis are providing key insights into the development of new treatments, including novel immunologic therapies. This chapter presents an overview of the epidemiology, diagnosis, pathophysiology, and treatment of allergic and nonallergic rhinitis.
Epidemiology
Incidence and Prevalence
The increase in the prevalence of allergic diseases began to garner attention from epidemiologists in the late 1980s. The International Study of Asthma and Allergies in Childhood (ISAAC) was initiated to establish the prevalence of allergic diseases in 257,800 school children aged 6 to 7 years and in 463,801 children aged 13 to 14 years using standardized, validated questionnaires.1 Phase 1 of ISAAC, which began to enroll patients in 1992, sought to establish prevalence rates in nearly 60 countries on every continent; phase 2 investigated variables contributing to rhinitis (e.g., environmental exposures); and phase 3 provided follow-up data on the patients at least 5 years after entry into the study. In phase 1, the prevalence rates for rhinitis collected across all centers ranged from 0.8% to 14.9% (median, 6.9%) in the 6- to 7-year-olds and from 1.4% to 39.7% (median, 13.6%) in the 13- to 14-year-olds.1 The highest prevalence rates for rhinitis were observed in parts of Western Europe, North America, and Australia, whereas the lowest rates were found in parts of Eastern Europe and south and central Asia.
The phase 3 analyses revealed that the prevalence rates had increased, with 12-month prevalence rates of 1.8% to 24.2% in children aged 6 to 7 years (median, 8.5%) and 1.0% to 45% (median, 14.6%) in 13- to 14-year-olds.2 In the 6- to 7-year-old group, most centers (67%) recorded significant increases in prevalence, 14% showed a decrease, and 19% were stable. In the 13- to 14-year-old group; 45% had increases, 25% showed a decrease, and 30% were stable. These findings strongly indicate that the prevalence of rhinitis has increased over a relatively short period of time, mostly in Westernized countries with a higher standard of living.
Subgroup analyses of the ISAAC cohort have provided additional important insights into the natural history of allergic rhinitis. In a prospective substudy following 2810 German children from age 9 to 11 years until age 15 to 18 years,3 the incidence of allergic rhinitis increased from an initial rate of 7% to 14%. In a similar study of 467 children assessed at age 3 years and again at 13 years, the 12-month prevalence rose from 6% to 24% in children without a family history of allergy and from 13% to 44% in those with at least one allergic parent.4 These longitudinal data offer compelling evidence that the incidence of allergic rhinitis increases significantly as children grow from childhood into adolescence.
Historically, the available data regarding the epidemiology of chronic rhinitis in adults are much more limited. Based on data for 15,394 adults 20 to 44 years of age, in the European Community Respiratory Health Survey I (ECRHS I), the prevalence of allergic rhinitis ranged from 4.6% in Oviedo, Spain, to 31.8% in Melbourne, Australia.5 In the most recent (U.S.) National Health and Nutrition Examination Survey (NHANES), conducted in 2005 to 2006, total immunoglobulin E (IgE), specific IgE, and nasal symptoms were assessed in 7398 patients, 4492 of whom were older than 20 years of age.6 The 12-month prevalence of rhinitis for the entire cohort was 23.5%, with a peak of 31.3% in patients 40 to 49 years of age. For the group as a whole, 24% had seasonal rhinitis and 10% had perennial rhinitis. Of importance, 60% of patients with rhinitis exhibited positive reactions for specific IgE. These findings suggest that chronic rhinitis affects close to one third of the adult population in countries like the United States and that a majority would be classified as allergic.
Risk Factors
A number of exposures in early childhood may act to increase the risk of developing rhinitis (Box 42-1). Gender has been identified as a potential factor in the development of rhinitis, and an analysis of 8486 patients who participated in the ECRHS I study revealed that the crude lifelong incidence of rhinitis was approximately 14% higher in women than in men; this predilection was heavily weighted in adult-onset disease.7 Regarding the relationship between outdoor air pollution and development of rhinitis, conflicting data have emerged from a limited number of studies. Although a large analysis from the ISAAC study did not demonstrate a relationship between particulate air pollution (defined as presence of “coarse” airborne particles less than 10 µm in diameter [PM 10]) and the development of rhinitis,8 increased levels of self-reported exposure to truck traffic were associated with significantly higher prevalence of symptoms.9 Parental tobacco smoking, particularly by the mother, which constitutes the principal form of indoor air pollution, also has been identified as a significant risk factor in the development of rhinitis in childhood.10
A number of other factors may have a protective effect against the development of rhinitis (see Box 42-1). The number of siblings at home and use of day care have been shown to be inversely correlated with the risk of developing rhinitis.11 It is likely that sibling number is acting as a surrogate marker for viral respiratory infection frequency in early childhood, which has been shown to promote a nonallergic T helper cell phenotype. Airborne allergen exposure has been cited as another possible factor. An ecologic analysis of ISAAC data investigated the effects of pollen exposure on the prevalence of allergic rhinitis in 13- to 14-year-olds. A significant inverse association was found between grass pollen counts and lifetime prevalence of the symptoms of allergic rhinitis.12 Rather than a direct effect of pollen, this relationship has been attributed to the effects of rural living and the likely presence of endotoxins in the immediate environment.13 Dietary factors also have been implicated in the development of rhinitis. Specifically, a number of small, cross-sectional, population-based surveys have suggested that the so-called Mediterranean diet, which is replete with fresh fruits and vegetables and whole grains and low in saturated fats, may reduce the chances of having asthma and allergic rhinitis.14,15 Although the question of diet and allergy has not been definitively answered, diets high in antioxidants and omega-3 fatty acids and low in certain fats may be specifically beneficial to overall health compared with the more typical Western diet.
Quality of Life and Economic Impact
Large, population-based studies have revealed that chronic rhinitis significantly impairs health-related quality of life. Questionnaires that focus on general quality of life (as used in the SF 36 Health Survey) have demonstrated significant decreases in physical functioning, energy, general health perception, social functioning, emotions, mental health, and pain in patients with moderate to severe perennial allergic rhinitis compared with control subjects.16 In particular, individuals experiencing at least 1 month of rhinitis symptoms per year noted the most significant impairment of quality of life, with repeated need to blow the nose, disrupted sleep, and inability to concentrate listed as the most severe problems.17 Sleep loss may play a key role in determining quality of life in that it may lead to daytime fatigue and poor concentration in school, resulting in learning impairment.18
Quality of life questionnaires have shown that chronic rhinitis may influence mood and cognitive function. Studies conducted during and after the allergy season reveal that subjects with seasonal allergic rhinitis had significant decreases in verbal learning, decision-making speed, psychomotor speed, reaction time tests, and positive affect scores compared with those reported for nonallergic control subjects.19
Rhinitis symptoms also have been found to impair productivity in the workplace. In studies using an instrument designed and validated to measure the effects of rhinitis on work activities (Work Productivity and Activity Impairment–Allergy Specific [WPAI-AS]), moderate to severe seasonal allergic rhinitis symptoms were determined to be responsible for 23% to 40% impairment of normal productivity at work.20,21
Associated Diseases
Asthma
Approximately 40% of patients with chronic rhinitis have asthma, and 80% of patients with asthma suffer with persistent nasal symptoms.22 This close relationship suggests that modulation of nasal function and/or inflammation may have an impact on the lower airways. In histopathologic terms, both allergic rhinitis and asthma are chronic inflammatory diseases of the airways sharing similar mediators, patterns of cellular infiltration, and immunologic regulation. In patients with allergic rhinitis and no clinical or physiologic evidence of asthma, inflammation frequently is present in the bronchi.23 Lower airway inflammation in rhinitic patients has physiologic consequences: A significant proportion of patients with nasal allergy exhibit nonspecific bronchial hyperresponsiveness in the absence of asthma symptoms.24 Some data suggest that nasal allergic responses can have a direct impact on both bronchial reactivity25 and bronchial inflammation.26
Nasal disease is an important risk factor for worsening asthma in patients who have both rhinitis and asthma. The frequency of both emergency department visits and hospitalizations is greater in patients with moderate to severe rhinitis than in patients who have mild or no rhinitis.27 Allergic rhinitis, particularly perennial disease, also is a significant independent risk factor for the development of asthma.28 Small studies indicate that patients with rhinitis who have concomitant bronchial hyperresponsiveness are at highest risk for this outcome.29
Rhinosinusitis
Rhinosinusitis is common in patients with allergic rhinitis. As many as 30% of patients with acute sinusitis, 67% with unilateral chronic sinusitis, and 80% with bilateral chronic sinusitis have allergic rhinitis.30 Nasal allergy most likely precipitates acute sinusitis by inducing sinus ostial edema, resulting in impairment of sinus drainage, a shift to anaerobic conditions inside of the sinus cavity, and finally bacterial proliferation. The relationship between allergy and chronic sinus disease is more complex and involves antistaphylococcal IgE antibodies in some patients.31
Otits Media with Effusion
A considerable proportion of patients with allergic rhinitis have concomitant otitis media with effusion (OME).32 Pollen exposure has been shown to cause eustachian tube dysfunction, which induces negative pressure in the middle ear space, followed by transudation of fluid.33
Sleep Disorders
Adults and children with allergic rhinitis frequently have poor-quality sleep, including difficulty getting to sleep, waking up during the night, and lack of a “good night's sleep.”34 Nasal obstruction associated with allergic rhinitis has been shown to be a risk factor for a variety of problems during sleep, including microarousals, hypopneas, and apnea.
Dental Malocclusion
Persistent, severe rhinitis in children may cause chronic mouth breathing, which has been linked to alterations in the palatal anatomy and dental malocclusion.35 Although a more recent study did not demonstrate an association between allergic rhinitis and malocclusive disease,36 this question has yet to be fully resolved.
Diagnosis
History
Typical signs and symptoms of chronic rhinitis include some combination of congestion, sneezing, rhinorrhea (anterior and/or posterior), and pruritus of the nose, eyes, oral mucosa, or face. Nasal congestion frequently alternates between both sides of the nose as a function of the physiologic nasal cycle.37 In addition, during sleep, the dependent side of the nose may become preferentially obstructed.38 Persistent unilateral obstruction strongly suggests the possibility of an anatomic defect (e.g., nasal septal deviation, concha bullosa of the middle turbinate), inflammatory mass (e.g., nasal polyp), or tumor. Sneezing may be extremely variable but in allergic disease often marked is by explosive paroxysms of 5 to 10 sneezes or more. In most of the rhinitis syndromes, rhinorrhea fluid most often is clear to white in color, and the presence of purulent secretions strongly indicates the possibility of chronic sinusitis or atrophic rhinitis. Ocular signs and symptoms, including redness, itching, and watering, constitute a major cause of suffering in at least half of the patients with allergic rhinitis,39 the presence of which will dramatically alter which therapy is selected. Other signs and symptoms, such as headache, a feeling of facial fullness, reduction in or loss of sense of smell, cough, and halitosis, should be noted, because presence of any of these will affect both the diagnosis and choice of treatment. When anosmia is the most prominent symptom and nasal or ocular symptoms are minimal or absent, primary central nervous system lesions should be considered.40
Once the spectrum of symptoms has been established, the presence of temporal patterns should be sought. Rhinitis symptoms, irrespective of cause, often are most intense during the early morning hours as a consequence of circadian variations in inflammation.41 A decrease in symptoms throughout the day, especially when the patient moves out of doors, suggests the presence of an indoor allergen (e.g., house-dust mite, animal dander, cockroach, or mold), whereas clear-cut worsening of symptoms in outside environments indicates the probability of allergy to an outdoor allergen (e.g., pollen, mold). Occurrence of symptoms during well-demarcated seasons, as documented in the medical history, usually is diagnostic of allergic rhinitis that is due to an outdoor allergen.
Finally, determination of possible triggers may provide information that is critical in establishing a diagnosis. Obvious precipitation of symptoms on exposure to house dust, furry pets, mildew, or cockroaches suggests the presence of IgE-mediated allergy. Along with these protein-based allergens, other triggers may include airborne substances traditionally categorized as irritants, including volatile organic compounds (e.g., perfumes, paint, cleaning fluids, cooking odors)42 and particulates (e.g., outdoor air pollution, road dust, construction dust), which appear to be most important in provoking nonallergic rhinitis. Changes in climatic factors, such as temperature, humidity, and barometric pressure, are similarly important in nonallergic rhinitis.43 The possibility of work-related symptoms should always be investigated, followed when indicated by a thorough review of potential triggers in the workplace. Finally, a complete list of current medications should be collected, because the principal cause of nasal symptoms may be drug-related (see Table 42-2).44
Physical Examination
Routine Examination
The routine physical examination provides important information regarding both the cause and severity of rhinitis, as well as potential comorbid conditions, such as conjunctivitis, otitis, asthma, and atopic dermatitis. Additionally, in young children the examination may suggest the presence of dental malocclusion and/or facial deformities (e.g., retracted mandible, high-arched palate) that may result from chronic, severe nasal obstruction.45
The nose should first be examined for outward signs of prior bony fractures (seen as deformities of the nasal bridge), asymmetry of the nostrils, and in children, a transverse crease over the lower portion of the nose caused by repetitive pushing of the nose upward in response to nasal itching or discharge. The interior of each nostril should be carefully examined using either a handheld otoscope or nasal speculum and headlamp. In patients with moderate to severe mucosal swelling of the inferior or middle turbinates, the examination also should be conducted after the instillation of a topical decongestant such as phenylephrine. The nasal airway should be examined systematically, to look for and establish the degree of swelling and color of the mucosa; the presence, color, and consistency of secretions; alterations in internal structures (e.g., septal deviation or perforation); and the presence of any abnormal mass lesions (e.g., nasal polyp) or foreign body. The mucosa in patients with symptomatic nasal allergy or nonallergic rhinitis with eosinophilia most often is swollen and pale in color, whereas patients with idiopathic rhinitis more typically have pink or erythematous mucous membranes. Great variability in appearance of the nasal airway is the rule, however, and these characteristics are not reliable for establishing a diagnosis. In patients with most forms of chronic rhinitis, the discharge is clear to white in color; the presence of discolored secretions suggests a chronic rhinosinusitis. Crusting, particularly with dried blood, should alert the physician to the possibility of atrophic rhinitis. An anterior nasal septal deviation may be easily visible, whereas more posterior abnormalities may be detected only with flexible rhinoscopy or computed tomography (CT) imaging. Nasal polyps most commonly are seen coming from the superior portion of the airway and are not difficult to distinguish from turbinates by virtue of their gray, glistening, “grapelike” appearance.
Examination of the eyes most often reveals conjunctival injection in patients with allergic rhinitis, which may be associated with erythema and bogginess of the upper and lower eyelids brought on by frequent rubbing. Cyanosis of the infraorbital tissues (“allergic shiners”) is thought to be caused by venous stasis and may be seen with any chronic nasal or sinus disorder and is not pathognomonic of allergy.46
Fiberoptic Rhinoscopy
Visualization of the nasal airway with a rhinoscope may serve as a very useful adjunct to the routine examination.47 Flexible rhinoscopes are employed regularly by otorhinolaryngologists, as well as some allergists and primary care physicians, and provide an enhanced view of structures in the superior and posterior regions of the nose. These normally unseen regions include the posterior nasal septum, superior nasal turbinates, middle meatus, adenoid gland, and eustachian tube orifices. Flexible rhinoscopy should therefore be considered in cases of rhinitis in which nasal obstruction is unilateral or refractory to therapy in the absence of any discernible anatomic cause on routine examination. Rigid rhinoscopes are used nearly exclusively by otorhinolaryngologists for visualizing the ostiomeatal complexes of the paranasal sinuses as well as performing nasal or sinus surgery.
Laboratory Testing
Testing for Specific Immunoglobulin E
Assessments of allergen-specific IgE are necessary to distinguish allergic rhinitis from nonallergic rhinitis. Allergy skin testing using the prick-puncture method is considered to provide the best combination of sensitivity and specificity, although in vitro testing has demonstrated comparable performance characteristics for some but not all allergens48 (see Chapter 74 for a complete discussion of skin and in vitro testing).
Nasal Cytology
Cytologic stains of mucus blown from the nose or epithelium scraped from the inferior turbinate can be assessed for multiple cell types, including eosinophils and neutrophils. These stained smears have been proposed as a means for differentiating allergic rhinitis from nonallergic rhinitis or sinusitis.49 Although the presence of significant nasal eosinophilia (more than 10 cells per high-power field) has an approximate 80% positive predictive value for the diagnosis of allergic rhinitis, other conditions also are associated with this pattern of inflammation, including asthma without symptoms of nasal allergy, nonallergic rhinitis with eosinophilia syndrome (NARES), and chronic rhinosinusitis with nasal polyposis. Although routine use of this test for the diagnosis of chronic rhinitis is not recommended, nasal cytology may be helpful in differentiating idiopathic rhinitis from NARES and in choosing optimal therapy.50 In addition, patients with nasal eosinophilia and a negative reaction on skin or blood allergy testing would be more likely to suffer from local allergic rhinitis (see later).
Blood Eosinophils and Total Serum Immunoglobulin E
Large, population-based studies reveal that mean concentrations of total serum IgE and circulating blood eosinophils are increased in allergic rhinitis. Although recent analyses have demonstrated utility using a combination of threshold values for total IgE and blood eosinophils,51 a great deal of overlap with values in asymptomatic persons is typical, thereby limiting the diagnostic value of these markers.
Radiographic Imaging
The most accurate test for evaluating possible sinusitis is CT.52 Frequently, mild mucoperiosteal thickening can be seen in patients with uncomplicated allergic rhinitis and NARES.53 Radiographic studies should be considered in patients with symptoms that are not typical of chronic rhinitis, such as chronic purulent rhinorrhea, alterations in sense of smell, or headaches, and are not responsive to therapy for rhinitis.
Measurements of Nasal Patency
An accurate assessment of nasal airway swelling is helpful in estimating the severity of the patient's rhinitis, deciding on initial therapy, and monitoring the patient's condition over time. Objective evaluations of the nasal airway can be made by assessing the anatomy of the airway and by measuring nasal airflow or resistance.
The most common technical method for examining nasal airway anatomy is acoustic rhinometry, which uses sound impulse emission to determine the cross-sectional area and volume of the nasal cavity.54 Measurements of acoustic rhinometry correlate with the sensation of nasal obstruction as well as imaging studies (i.e., CT and magnetic resonance imaging [MRI]) and physiologic measurements (i.e., posterior rhinomanometry, nasal peak inspiratory flow rate). Whereas acoustic rhinomanometry may serve as a valuable aid in assessing the nasal response to provocative challenge, the expense of the equipment, time required to make accurate measurements, and lack of additional information provided by the test have limited its role in clinical practice.
Nasal function can be assessed by measuring nasal peak flow or active rhinomanometry. Nasal peak flow may be measured as either inspiratory or expiratory flow rates; both methods are simple, quick, and inexpensive to do. Although nasal peak inspiratory flow rate has been shown to correlate well with subjective measurements of nasal congestion, the results provided may be quite variable owing to the effort-dependent nature of the test.55 Non–effort-dependent tests of nasal function include active rhinomanometry, which measures nasal airway resistance or its inverse, conductance.56 Posterior rhinomanometry has a higher degree of accuracy than anterior rhinomanometry but may be too technically demanding for some patients to perform successfully. Anterior rhinomanometry often is easier for patients to perform but may not be accurate when severe unilateral nasal obstruction is present. These physiologic measurements provide more objective descriptions of nasal patency; their cost and inconvenience, however, relegate their use primarily to clinical research.
Classification of Rhinitis Syndromes
The classification of chronic rhinitis is complex, and no mutually agreed-upon scheme has been established. In the following discussion, the categories of classification are those commonly used to describe various syndromes and subtypes, which relate primarily to etiology (Box 42-2).
Allergic Rhinitis
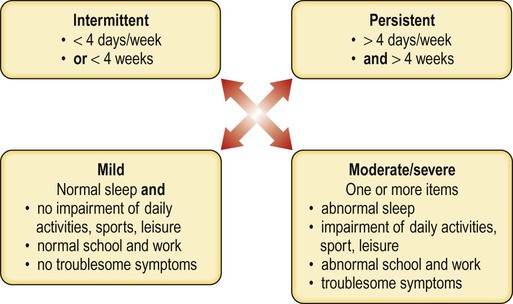
Allergic rhinitis is caused by hypersensitivity to airborne substances and accounts for approximately 50% of cases. The classic, cardinal symptoms and signs of allergic rhinitis are congestion, discharge (usually clear and watery), sneezing, and pruritus of the nose, palate, throat, or ears. In approximately two thirds of patients, eye symptoms and signs may be present, including itching, conjunctival injection, and watering.57 Prominent nasal symptoms of itching and sneezing and ocular symptoms help to distinguish allergic rhinitis from other causes of rhinitis.58 Patients with predominant congestion and discharge alone, however, may still have allergy as the primary cause of their rhinitis. Clinical diagnosis of seasonal allergic rhinitis may be straightforward in patients who live in areas where there are clearly defined pollen or mold seasons and experience purely seasonal symptoms. Symptoms that occur during the spring usually are ascribed to tree pollen exposure, in summer to grass and outdoor molds, and in fall to weeds and outdoor molds; precise start and stop dates of specific pollination seasons varies geographically. A large number of patients, however, do not demonstrate this clear seasonal occurrence of rhinitis and may experience intermittent symptoms of variable degree. This type of pattern prompted the development of a new system for classifying allergic rhinitis that characterizes allergic rhinitis by severity level and duration22 (Fig. 42-1).
The hallmark of allergic rhinitis is evidence of specific IgE to a relevant allergen. Although IgE most commonly is distributed systemically and can be identified by allergy skin testing or blood assays, in a subset of patients with allergic rhinitis, specific IgE can be identified only in the nose. This finding, manifesting as local allergic rhinitis, or entopy, has been suspected for several decades but has only recently undergone rigorous investigation (see further on).59 Nasal allergen challenge is required to clinically confirm this diagnosis, which is performed primarily in research settings. In the near future, this procedure may become part of the clinically accepted evaluation for patients with suspected local allergic rhinitis.
Work-Related Rhinitis
Rhinitis related to the workplace is characterized by intermittent or persistent nasal symptoms attributable to exposures incurred in a particular work environment.60 Work-related rhinitis may due to immunologic hypersensitivity, including the presence of IgE, or may be nonallergic in etiology. The first type of work-related rhinitis is occupational rhinitis, in which the primary cause of nasal symptoms arises from exposures occurring in the work environment. The second type, referred to as work-exacerbated rhinitis, occurs in persons with preexisting or concurrent rhinitis that is worsened by workplace exposures. Occupations that carry a high risk for development of work-related rhinitis include laboratory workers, furriers, and bakers and many others (Table 42-1).
TABLE 42-1
Occupations with Increased Prevalence of Work-Related Rhinitis
| Category | Occupation | Likely Trigger |
| Irritant | Drywall installer | Gypsum dust |
| Makeup artist | Cosmetic power, perfume | |
| Corrosive | Janitor | Ammonia |
| Chemistry technician | Hydrochloric acid | |
| Immunologic | ||
| Immunoglobulin E | Baker | Grain flour |
| Furrier | Animal dander | |
| Livestock breeder | Animal dander | |
| Veterinarian | Animal dander | |
| Food processing worker | Foodstuffs | |
| Pharmacist | Medication powders | |
| Low-molecular-weight substances | Boat builder | Anhydrides |
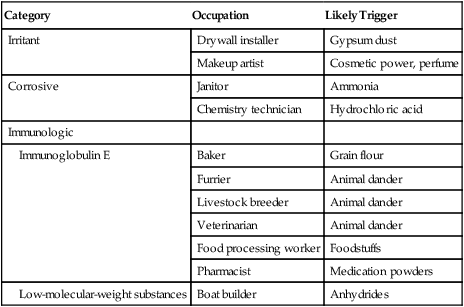
Work-related rhinitis may be divided into three main categories defined by the types of implicated substances: irritant-induced, corrosive, and immunologic (Box 42-2). Irritant-induced rhinitis, is caused by small airborne substances not typically categorized as allergens and not shown in appropriate studies to elicit a specific immune response.61 Irritant rhinitis may be associated with exposure to a wide variety of substances, including volatile organic compounds (e.g., perfume, paint fumes), particulates (e.g., chalk dust, coal dust, construction dust), and smoke (e.g., wood-burning fire, tobacco). Whereas irritant-induced rhinitis due to volatile organic compounds may cause transient symptoms that abate once the exposure is stopped, exposure involving cleaning fluids, particulates, and smoke may lead to more persistent symptoms. The second category of work-related rhinitis, corrosive rhinitis, results from exposure to a high concentration of such chemical gases, causing sufficient nasal inflammation that the mucosa may break down and ulcerate.62 Substances that have been linked to this condition include chlorine, sulfur dioxide, and ammonia. Some patients have reported that a single large exposure to these types of gases resulted in long-lasting symptoms of rhinitis; this clinical entity has been termed reactive upper airways dysfunction syndrome (RUDS). The final category of work-related rhinitis, immunologic rhinitis, is characterized by a specific immune response to a substance found in the workplace. Substances that most commonly cause immunologic rhinitis are proteins that elicit an IgE response, such as animal danders (e.g., in laboratory workers) or grains (e.g., in bakers). Low-molecular-weight substances, such as anhydrides (e.g., plastics manufacturers), act as haptens and induce an immunologic response similar to that seen in persons with occupational asthma.63
Diagnosis of work-related rhinitis relies heavily on a history of symptomatic worsening during the work week, with improvement over the weekend and during vacations, when the putative trigger is absent. Symptom diaries and self-administered assessments of nasal peak flow may establish a clinical pattern suggesting that the workplace is causing or aggravating symptoms. Eventually, however, symptoms may eventually persist during periods away from work as mucosal inflammation becomes more established, making the diagnosis more difficult to establish. In many situations, skin or blood testing for specific IgE may be very helpful, and occasionally a provocative nasal challenge may be required to identify a specific causative agent.
Chronic Rhinosinusitis with and without Nasal Polyps
Chronic rhinosinusitis (CRS) is an inflammatory disease of the paranasal sinuses that has been present 12 weeks or longer.64 The four cardinal symptoms of CRS are mucopurulent drainage, nasal obstruction, facial discomfort, and decreased sense of smell; two of these must be present, along with CT or endoscopic evidence of sinus mucosal inflammation in order to consider the diagnosis. Up to one third of patients with CRS present with nasal polyps, which are likely to cause anosmia.65
Idiopathic Rhinitis
Idiopathic rhinitis, also referred to as vasomotor rhinitis, manifests with symptoms of nasal congestion and/or watery rhinorrhea that worsen acutely in response to nonspecific provocateurs; cold air, exercise, pungent odors, tobacco smoke, alcohol, and specific physiologic states, including sexual arousal and emotional upset, all have been implicated.66,67 Patients with idiopathic rhinitis have negative responses on skin or blood tests for specific IgE, although occasionally patients may exhibit a small number of positive reactions that do not correlate with the clinical pattern of symptoms and are considered clinically irrelevant. With idiopathic rhinitis, samples of nasal tissue sent for cytologic analysis will not demonstrate eosinophils or other inflammatory cells.
Exercise may induce recurrent rhinitis in nonatopic patients who do not normally suffer from nasal symptoms.68 The most common clinical finding is clear, watery rhinorrhea, but patients also may experience acute nasal congestion, itching, and sneezing.69 Up to 20% of elite runners and swimmers experience exercise-induced nasal symptoms during routine workouts.70
Nasal symptoms induced by exposure to cold air may occur in patients with underlying chronic rhinitis as well as those with no chronic nasal disease.71 This form of rhinitis is characterized by watery discharge, congestion, and burning of the nasal mucosa that develop within minutes of exposure to cold air and stop soon after the end of exposure. It is particularly common in areas with low outdoor relative humidity, and the cold air may work in conjunction with vigorous exercise to cause very severe acute rhinitis.
Gustatory rhinitis is characterized by watery rhinorrhea that begins soon after beginning to eat.72 Virtually all foods have been reported to cause these symptoms, but hot and spicy foods are implicated most commonly.73 The discharge may be unilateral but most often is bilateral and is rarely associated with other nasal symptoms. Although a small number of children and adults may acquire specific IgE to select foods, with consequent development of acute food-induced rhinitis, patients who experience recurrent nasal symptoms after eating virtually any food are rarely found to have an atopic etiology. Gustatory rhinitis may occur in patients with underlying chronic rhinitis or may be an individual’s only source of nasal symptoms.
Nonallergic Rhinitis with Eosinophilia
NARES accounts for approximately one third of the cases of nonallergic rhinitis.74 Affected patients have perennial nasal symptoms and signs, with congestion and clear discharge being most prominent, although significant sneezing and pruritus are described as well. In addition, a small percentage of patients report anosmia, which is unusual in uncomplicated allergic rhinitis.75 Nasal smears reveal large numbers of eosinophils, as seen in patients with allergic rhinitis, despite the absence of systemic allergy as assessed by allergy skin or blood testing.74 As noted previously, these patients may have a local form of allergic rhinitis in which IgE is present in the nasal mucosa but absent from other body tissues.
Atrophic Rhinitis
Atrophic rhinitis is a chronic condition characterized by symptoms of crusting, purulent discharge, nasal obstruction, and halitosis.76 Diagnosis is based largely on clinical characteristics, and this entity should be considered in any patient who complains of significant nasal crusting. Examination may reveal an ulcerated mucosa covered by thick yellow, brown, or green crusts with possible evidence of bleeding.77 The nasal cavities may be enlarged, with bowing of the lateral nasal wall; in advanced cases, saddle nose deformity and nasal septal perforation may occur.77
Primary atrophic rhinitis is most prevalent in areas with prolonged warm seasons (e.g., India, Saudi Arabia) and is unusual in North America and northern Europe.78 The primary form of this disease typically afflicts middle-aged adults, being more common in women, and is not seen in children. Although primary atrophic rhinitis has no known specific cause, many patients are found to have chronic bacterial infection of the nose and sinuses due to any of a large number of organisms, including Klebsiella ozaenae, Coccobacillus foetidus ozaena, Pseudomonas aeruginosa, and Proteus spp.
Secondary atrophic rhinitis most commonly occurs in older patients who have undergone multiple nasal sinus surgeries.76 In addition, trauma, irradiation, and granulomatous diseases (e.g., leprosy, sarcoidosis, Wegener granulomatosis, syphilis) of the nose have been reported to result in secondary atrophic rhinitis. As in the primary disease, manifestations may include crusting, obstruction, halitosis, and recurrent epistaxis. The so-called empty nose syndrome often is included with secondary forms of atrophic rhinitis.79 Empty nose syndrome usually follows aggressive resection of the inferior and occasionally middle turbinates and manifests with symptoms of severe nasal obstruction and inability to sense airflow through the nose despite complete patency of the nasal airways.79 This clinical picture may be associated with a profound sense of dyspnea in the absence of any objective findings of pulmonary disease.
Rhinitis Associated with Drugs
Repetitive use of topical α-adrenergic decongestant nasal sprays (e.g., oxymetazoline, phenylephrine [Neo-Synephrine]) for more than a few days may result in rebound nasal congestion,80 most likely secondary to downregulation of the α-agonist receptor.81 With long-term use of these agents, usually several months, a chronic form of rhinitis referred to as rhinitis medicamentosa ensues. This disorder most often manifests with severe nasal congestion without other significant symptoms. Rarely, chronic overuse of topical decongestants may result in septal perforation.82 Cocaine use also has been implicated in causing rhinitis medicamentosa but usually results in significantly more crusting, bleeding, and ultimately septal perforation than topical decongestant drugs.83 Physical examination in patients with rhinitis medicamentosa often reveals swollen, red nasal mucous membranes with minimal discharge.80
It also has been suggested that the antibacterial agent benzalkonium chloride, which is present in many intranasal medications, can damage the nasal mucosa. A review of 18 published studies, however, did not support this assertion,84 indicating that if a harmful effect exists, it probably is not clinically significant.
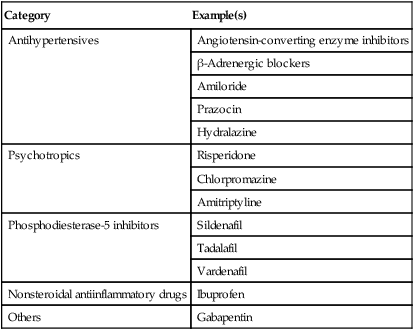
A number of systemic medications have been shown to be associated with increased nasal symptoms, particularly congestion and rhinorrhea.85 These medications are believed to induce changes in nasal function by causing inflammation, through neurogenic effects, or by unknown mechanisms. For most classes of medications, the evidence supporting this relationship is anecdotal and not supported by rigorous investigation. General classes of medications that have been implicated in causing rhinitis symptoms include antihypertensives, drugs for erectile dysfunction, psychiatric drugs, and nonsteroidal antiinflammatory drugs (Table 42-2).
TABLE 42-2
Medications Associated with Chronic Nasal Symptoms
| Category | Example(s) |
| Antihypertensives | Angiotensin-converting enzyme inhibitors |
| β-Adrenergic blockers | |
| Amiloride | |
| Prazocin | |
| Hydralazine | |
| Psychotropics | Risperidone |
| Chlorpromazine | |
| Amitriptyline | |
| Phosphodiesterase-5 inhibitors | Sildenafil |
| Tadalafil | |
| Vardenafil | |
| Nonsteroidal antiinflammatory drugs | Ibuprofen |
| Others | Gabapentin |
Hormonal Rhinitis
The most frequently encountered hormonal state associated with rhinitis is pregnancy. The most common causes of nasal symptoms requiring treatment during pregnancy include rhinitis of pregnancy, allergic rhinitis, rhinitis medicamentosa, and sinusitis.86
From 20% to 30% of pregnant women will acquire rhinitis of pregnancy, defined as new-onset nasal symptoms (usually congestion and/or rhinorrhea) in the absence of another known cause that lasts 6 or more weeks and resolves within 2 weeks after delivery.87 The pathophysiology of pregnancy rhinitis is unknown. Although the condition has been attributed to changes in estrogen or progesterone, or both, little evidence has emerged to support this assertion.88 Preexisting chronic rhinitis has been reported to worsen, improve, or remain unchanged at approximately equal rates among pregnant women.86 These findings are similar to those in asthma, and one study found concordance between the course of asthma and that of rhinitis during pregnancy.89 This correlation suggests that mechanical factors involved in both diseases may be similarly altered during pregnancy. Uncontrolled rhinitis during pregnancy may be a cause of severe snoring, which has been associated with an increased risk of gestational hypertension, preeclampsia, and intrauterine growth retardation.90,91
Although abundant data are available to link pregnancy to nasal symptoms, much less is known regarding the relationship between the menstrual cycle or use of exogenous ovarian hormones (i.e., oral contraceptives, hormone replacement therapy) and rhinitis.88 Although exogenous estrogen and progesterone both have been suspected of causing nasal symptoms, at least one carefully designed clinical trial showed that hormone replacement therapy had no effect on quality of life, nasal airway resistance, or nasal mucociliary clearance.92
Hypothyroidism frequently is mentioned as a cause of chronic nasal congestion and discharge, although the evidence linking these two conditions is limited and may merely represent the concomitant occurrence of two common disorders.93
Rhinitis Related to Aging
As people grow older, important changes in nasal physiology occur, including a general decrease in total body water content, decrease in nasal blood flow, and degeneration of mucous glands.94 In addition, collagen fibers in cartilage and elastic fibers in the dermis become progressively more atrophic, leading to retraction of the nasal columella and downward rotation of the nasal tip.94 These physiologic and structural changes often result in symptoms of nasal mucosal dryness and increased nasal airway resistance in patients who have not previously experienced chronic rhinitis.
In patients with previously established allergic rhinitis, advancing age is associated with a gradual diminution in clinical symptoms.95 Immunologically, both skin tests and in vitro tests for allergy also decrease in magnitude during long-term follow-up.95 Despite these age-related reductions in symptom severity, quality of life related to allergic rhinitis remains significantly impaired in patients older than 65 years.96
Rhinitis Related to Systemic Disease
A number of systemic diseases may be occasionally associated with symptoms of rhinitis. These include granulomatous diseases (e.g., granulomatosis with polyangiitis, sarcoidosis, midline granuloma), cystic fibrosis, ciliary dyskinesia syndromes, and immunodeficiencies. In most of these conditions, typically the nose and sinuses are affected, rather than the nose alone; the symptoms often extend to involve other organ systems, particularly the lungs; and associated constitutional complaints, such as fatigue and poor appetite, are common.
Differential Diagnosis in Chronic Rhinitis
Patients presenting with chronic nasal complaints may suffer from upper airway disorders other than rhinitis (Box 42-3). A number of anatomic abnormalities in the nose and pharynx can cause chronic partial or complete nasal blockage without other significant symptoms. Concha bullosa (aeration of the middle turbinate bones with expansion of the turbinates) has been shown to be present in various degrees in up to 67.5% of the general population; in a small number of affected persons, however, the condition is extensive enough to result in unilateral or bilateral nasal obstruction.97 Nasal septal deviation can be identified in nearly 20% of people, and as with concha bullosa, a fraction of that group will present with significant symptoms.97 Adenoidal enlargement also is very common. In a study limited to adults, 55% of asymptomatic subjects had some degree of adenoidal hypertrophy, whereas 63% of patients with nasal obstructive symptoms showed signs of enlargement.98 In another study in children, approximately 55%, 35%, and 14% of the subjects had grade 1, 2, and 3 hypertrophy, respectively, and only those with grades 2 and 3 had symptomatic obstruction.99 These findings suggest that nasal anatomic defects are common in the general population and should be considered in all patients presenting with nasal obstruction.
Children presenting with chronic unilateral nasal obstruction, frequently but not always associated with purulent secretions, should be evaluated for a foreign body in the nose.100 A peanut, bead, button, piece of small plastic toy, or small battery may be pushed into the nose by the child, which then falls into a posterior position and is not always visible to inspection. Purulence indicates the probable presence of sinusitis secondary to the foreign body.
Nasal cancers are very rare, constituting 3% of head and neck cancers, with a prevalence of 1 case in 100,000 people.101 Nasal cancer should be suspected in older persons with unilateral nasal obstruction and bleeding of gradual onset. Such patients should be referred promptly to an otorhinolaryngologist.
Pathophysiology
Allergic Rhinitis
Sensitization and Immunoglobulin E Production
Sensitization is initiated in nasal tissues when antigen that is deposited on the nasal mucosa is engulfed by antigen-presenting cells (APC)—macrophages, dendritic cells, Langerhans cells—and partially degraded within their phagolysosomes into antigenic peptides. These peptides are then externalized on the surfaces of APCs and are presented to naïve CD4+ T lymphocytes. CD4+ lymphocyte activation requires the interaction of specific T cell receptors on the surface of T cells with allergen peptide–MHC class II complexes on the APCs and the ligation of costimulatory receptors of the CD28 family on T cells by B7 family members of costimulatory molecules (CD80 and CD86) on APCs.102 If given the proper stimulus, naïve helper CD4+ cells can differentiate into the biased helper T cell Th1 or Th2 subsets. In the case of allergy, the Th2 subset plays a central role and requires interleukin (IL)-4 for development. These cells secrete the cytokines IL-4, IL-5, and IL-13, which all are central to the production of IgE and recruitment and survival of eosinophils at sites of allergic reaction.
In addition to presenting antigen, dendritic cells can polarize naïve T cells into either Th1 or Th2 cells according to their own phenotype and with signals received from processed antigens and from the tissue microenvironment during antigen presentation. To illustrate this point, experiments show that plasmacytoid dendritic cells matured by exposure to IL-3 and CD40 ligand engagement promote development of T cells toward a Th2 phenotype, whereas cells that mature through contact with a virus promote a Th1 phenotype.103 Other signals that affect dendritic cells and their influence on Th2 polarization include prostaglandin E2 and thymic stromal lymphopoeitin (TSLP) released from epithelial cells that switch the maturation of myeloid dendritic cells into Th2-promoting dendritic cells.104 Another distinct subtype of T cells that has been recognized to be important in the regulation of immune responses are known as regulatory T cells (Tregs).105 These cells suppress both Th1 and Th2 immune responses through the secretion of inhibitory cytokines and cell surface molecules such as IL-10, transforming growth factor-β (TGF-β), cytotoxic T lymphocyte antigen-4 (CTLA-4), and programmed death protein 1 (PD1). Tregs can also inhibit effector T cells by a direct cell-to-cell contact mechanism that induces apoptosis and by influencing APCs to suppress T cell activation. They are categorized as either natural or inducible and typically exhibit high levels of CD25 on their surface, as well as the transcription factor forkhead box P3 (Foxp3). The balance between Th2 and certain Treg populations may decide whether clinical allergy will develop,106 and evidence suggests that CD25+ Tregs are defective in patients with allergic rhinitis.107
The secretion of IgE from B cells requires two essential signals, the first of which is in the form of IL-4 and IL-13 secreted from Th2 lymphocytes, which drive B cells to IgE production by inducing ε-germline gene transcription. The other signal is a costimulatory interaction between CD40 ligand on the T cell surface and CD40 on the surface of B cells, which promotes B cell activation and switch recombination for the production of IgE.108 Antigen-specific IgE then attaches to high-affinity receptors on mast cells and basophils and to low-affinity receptors on other cells, thereby sensitizing the nasal mucosa. On subsequent exposure to the offending allergen, the IgE antibodies on the surface of these cells serve as receptors for the antigen molecules. Augmentation of FcεRI expression on mast cells has been shown to bind an increased number of IgE-antigen complexes, which may result in enhanced production of immunomodulatory cytokines and chemical mediators, forming a positive feedback amplification loop involving the IgE-IgE receptor mast cell cascade.109 Cross-linking of adjacent IgE molecules on mast cells leads to the release of inflammatory mediators that stimulate nerves, glands, and blood vessels to cause the clinical manifestations of the disease—namely, sneezing, pruritus, rhinorrhea, and nasal obstruction.
Early Response to Allergen
Within minutes after exposure of an allergic patient to antigen, a symptomatic response occurs. The patient first senses tingling and pruritus, followed by onset of sneezing, rhinorrhea, and nasal congestion. These clinical manifestations correlate with physiologic changes that are measured after antigen provocation, such as increase in nasal airway resistance (NAR).110 In addition to these physiologic changes, increases are noted in the levels of several mediators including histamine, kinins, tryptase, prostaglandin D2 (PGD2), leukotriene C4 (LTC4), leukotriene B4 (LTB4), major basic protein (MBP), and platelet-activating factor (PAF).111-117 These mediators induce onset of the various symptoms of allergic rhinitis by their effects on end-organs and nerves of the nasal mucosa. Histamine and tryptase are found in mast cell granules, and their detection in nasal secretions after antigen provocation provides support for mast cell degranulation during the nasal allergic reaction. PGD2 and the cysteinyl leukotrienes, which are newly synthesized by the arachidonic acid pathway, also are secreted by mast cells. Further evidence for the role of nasal mast cells in the immediate allergic reaction was provided by the demonstration of degranulated mast cells in nasal mucosal biopsy specimens from allergic patients after allergen challenge.118
Late Response to Allergen
The response to allergen exposure is not limited to the acute events that occur a few minutes after the exposure. Hours after antigen challenge, some patients experience a recurrence of symptoms, particularly nasal congestion, which is termed the late response. Several investigators have documented elevations in NAR 4 to 10 hours after antigen challenge, with a peak around 6 hours and resolution by 24 hours.119 Along with increases in nasal symptoms and NAR, increases also were observed in the levels of histamine, tosyl-l-arginine methyl ester (TAME)-esterase, and kinins, but not PGD2.120 These events are accompanied by an inflammatory cellular influx.
In addition to the different preformed and newly generated inflammatory mediators secreted by mast cells and other inflammatory cells during the allergic reaction, cytokines have been identified in the nasal mucosa and in nasal secretions of allergic patients after allergen provocation as well as natural exposure. In different allergen challenge experiments, increased levels of IL-1β, tumor necrosis factor (TNF)-α, and granulocyte-macrophage colony-stimulating factor (GM-CSF) were detected during the early hours after provocation, and increased levels of IL-5, IL-6, IL-8, GM-CSF, and TNF were detected during the late phase response.121,122
Investigations relating to the role of cytokines in allergic rhinitis have been performed using nasal biopsies during the allergy season or after-challenge assay for protein expression (using immunohistochemistry techniques) or messenger RNA (mRNA) (by in situ hybridization). Compared with those from healthy subjects, nasal biopsy specimens from patients with perennial allergic rhinitis show significantly more IL-4+ cells, which are predominantly identified as mast cells.123 By contrast, in this study immunoreactivity for IL-5, IL-6, and IL-8 was not significantly different between patients with rhinitis and healthy subjects.123a,123b,124 The lack of localization of any of these cytokines to T lymphocytes was attributed by the investigators to the fact that cytokines generated by activated T cells are rapidly transported from the cell and do not accumulate in sufficient concentrations to be detected by the techniques used. These data also support a role for mast cells in contributing to the cytokines released in the local milieu after exposure to allergen.
Looking for mRNA for the different cytokines in nasal biopsy specimens after allergen challenge of allergic subjects, Durham and coworkers found significant increases in cells bearing mRNA for IL-3, IL-4, IL-5, and GM-CSF, but not for IL-2 or interferon (IFN)-γ compared with biopsies obtained after a control challenge.124 Activated eosinophils (EG2+) increased significantly after allergen challenge, and levels correlated positively with mRNA expression for IL-4, IL-5, GM-CSF, IL-3, and IL-2 but not for IFN-γ. Approximately 80% of IL-5+ mRNA cells also were shown to be CD3+, and the rest were positive for tryptase.125 Other biopsy studies also have shown significant increases in mRNA IL-10+ and IL-13+ cells after allergen challenge.126
These findings suggest that both T lymphocytes and mast cells are contributors to cytokine production during the allergic reaction. The cytokine profile observed after exposure to allergen emphasizes the importance of Th2 cells and their cytokines in the allergic reaction. IL-5 exerts its main effects on eosinophils, promoting the differentiation, vascular adhesion, and in vitro survival of eosinophils and enhancing histamine release from basophils.127-130 IL-4 is an important mast cell growth factor and promotes the switching of B cells to the production of IgE.131-132 IL-13, which shares most of its functions with IL-4, may be important in contributing to late phase inflammation and symptoms of allergic rhinitis, although it is unclear whether IL-13 has a significant impact on the influx of eosinophils into the nasal mucosa.133-134 Thus mast cells are not only effector cells of the immediate phase response but also may function as immunoregulatory cells of allergic inflammation.
The role of epithelial cells as immune mediators has been increasingly recognized. Either through direct cell-to-cell interaction or through the release of cytokines and chemokines, epithelial cells can regulate other resident cells such as dendritic cells and mast cells.135 Epithelium-derived cytokines, including IL-25,136 IL-33,137 and thymic stromal lymphopoietin (TSLP),139 have been identified in humans and appear to play important roles in the development and perpetuation of allergic rhinitis through regulation of Th2 cytokines.138
Neurogenic Activity
Sneezing and itching during the early response to allergen provocation both result from stimulation of nerves originating in the nose. Unilateral intranasal antigen challenge experiments have supported the role of the nervous system in amplifying the allergic response: Challenge testing leads not only to an increase in sneezes, rhinorrhea, nasal secretions, histamine level, NAR, and PGD2 concentrations on the side of challenge but also to an increase in rhinorrhea, secretion weights, and PGD2 level contralateral to the challenge.139 The contralateral secretory response was rich in glandular markers and was inhibited by atropine, an anticholinergic, suggesting that the efferent limb was cholinergically mediated.
Also clear is that the nasal response to allergen is accompanied by an ocular, pulmonary, and paranasal sinus response that can be explained, at least in part, by a neural reflex. Monitoring ocular symptoms and secretions after unilateral allergen challenge has shown an ocular symptomatic and secretory response that is inhibited by pretreatment with an intranasal antihistamine, suggesting that histamine's action on nasal afferent nerves initiates this reflex.140
In addition to sympathetic and parasympathetic nerves and their transmitters, several neuropeptides are found in the nasal mucosa. These neuropeptides are secreted by unmyelinated nociceptive C fibers (for tachykinins, calcitonin gene–related peptide [CGRP], neurokininA, and gastrin-releasing peptide), parasympathetic nerve endings (for vasoactive intestinal peptide [VIP] and peptide histidine-methionine), and sympathetic nerve endings (for neuropeptide Y). Substance P, a member of the tachykinin family, often is found as a cotransmitter with neurokinin A and CGRP; it has been found in high density in arterial vessels and, to some extent, in veins, gland acini, and epithelium.141 Several studies support the concept that neuronal mechanisms mediated by these peptides amplify the inflammatory allergic reaction.142-146
In a group of patients with allergic rhinitis, Mosimann and colleagues were able to demonstrate significant increases in the levels of substance P, CGRP, and VIP immediately after allergen challenge and in patients who experienced a late reaction.147 These experiments suggest that neuropeptides are released in humans after allergen challenge and may be partly responsible for symptoms of the allergic reaction. Repetitive application of capsaicin, the essence of chili peppers, releases substance P and CGRP from sensory nerves and initiates both central and axonal reflexes.148 Capsaicin produces a burning sensation accompanied by profuse bilateral rhinorrhea when applied to one side of the nasal cavity, and repeated administration results in tachyphylaxis.149 The capsaicin-induced nasal secretory response in humans is glandular and not caused by increased vascular permeability.150 Furthermore, capsaicin desensitization reduces sneezing in response to antigen and histamine challenges.151 All of these findings point to the importance of the participation of neurogenic elements to the allergic response and more specific delineation of the role of each of these neuropeptides awaits the development of specific antagonists.
Cellular Events
Along with the physiologic changes and mediator production that occur hours after allergen provocation, inflammatory cellular influx occurs in the nasal mucosa and in nasal secretions recovered after experimental provocation and in seasonally exposed patients (Fig. 42-2). Using different sampling techniques, studies in allergic inflammation show that the predominant cell types in nasal secretions are polymorphonuclear cells and eosinophils, with mononuclear cells predominating in the nasal mucosa, suggesting that nasal secretions and the nasal mucosa are two separate compartments, with different cellular predominance during allergic inflammation.152

Typically, a slight initial increase in eosinophils in nasal secretions is observed within 1 to 2 hours of challenge and usually is followed by a peak 6 to 8 hours later.153 MBP, a mediator secreted by eosinophils, also is recovered in nasal lavage fluid hours after antigen provocation, and its levels correlate with the number of eosinophils, suggesting that these cells influx into nasal secretions and release inflammatory mediators.154 Basophils constitute 1% of the recovered cells. Their number correlates significantly with levels of histamine recovered in nasal secretions during the late phase response, suggesting that these cells are the source of the late rise in histamine.153
Similar cellular changes have been observed during seasonal exposure of allergic patients, lending credibility to the observations after experimental allergen challenge.155 A seasonal increase in mast cells occurs on the surface of the nasal epithelium after 4 or 5 days of exposure to pollen, which seems to be the result of migration of mast cells from the deeper layers of the lamina propria to the surface.156 The consensus is that basophils predominate in nasal secretions, whereas mast cells are more abundant in the epithelium and lamina propria of allergic patients exposed to antigen either experimentally or naturally.
Although eosinophils and mast cells are found in the nasal submucosa, the majority of cells identified in the submucosa are mononuclear cells, including lymphocytes and monocytes. Numbers of CD4+ lymphocytes and CD25+ cells are significantly increased after antigen challenge compared with sham challenge.157 As noted earlier, a significant source of cytokine production in the nasal mucosa during allergic inflammation are CD4+ Th2 cells.
Another important cell type detected in the nasal mucosa of allergic patients is Langerhans cells, which are large dendritic cells important in antigen presentation. Whereas the numbers of intraepithelial CD1+ Langerhans cells in healthy subjects and grass-allergic patients are not different outside of the pollen season, the numbers of intraepithelial CD1+ cells are significantly increased during the allergy season.158 Thus Langerhans cells appear important in the allergic reaction and are upregulated after exposure to allergen.
Adhesion Molecules
Cellular trafficking is integral to human immune response because it allows cells to be selectively recruited from the bloodstream into sites of tissue inflammation. Recruitment of cells such as eosinophils and activated T lymphocytes are mediated, in part, by interactions between adhesion molecules on these cells and their ligands on vascular endothelial cells.
Clear evidence shows that endothelial activation occurs during allergic rhinitis. Enhanced expression of intercellular adhesion molecule 1 (ICAM-1) (i.e., CD54) and vascular cell adhesion molecule 1 (VCAM-1) (i.e., CD106), but not E-selectin, has been described in the mucosa of allergic patients.159 In nasal biopsy specimens, the expression of VCAM-1 was found to be significantly upregulated 24 hours after allergen challenge, in concert with a significant increase in eosinophils.160 These studies of adhesion molecules in vivo suggest that these molecules, along with their counter ligands on circulating leukocytes, have an important role in cellular recruitment to allergic inflammatory sites.
Nasal Hyperresponsiveness
One of the hallmarks of allergic rhinitis is hyperresponsiveness to specific stimuli, such as allergens, and nonspecific stimuli, such as methacholine.
Specific hyperresponsiveness refers to the alteration in dose of allergen required to evoke a clinical response, a phenomenon known as priming. Many allergic patients report worsening symptoms as the allergy season progresses, despite unchanged or decreased pollen counts. This phenomenon probably is caused by a shift in the threshold of responsiveness. Connell found that the dose of pollen necessary to create symptoms decreased more than fivefold by the fourth day of consecutive allergen challenges.161 In other studies, consecutive nasal allergen challenges caused significantly more sneezing along with higher concentrations of histamine and kinins and an increase in the number of neutrophils, eosinophils, and basophils in nasal lavage fluid samples.162 These observations suggest that mechanisms of priming involve cellular infiltration, increased mediator production, and possible increased end-organ responsiveness. Influxing inflammatory cells are hypothesized to alter the mucosal penetration of antigen and to provide additional targets for allergen stimulation and increased generation of inflammatory mediators. These changes presumably lead in turn to the exaggerated response noted after repeated allergen exposure.
Nonspecific hyperresponsiveness is defined as the capacity of the nose to respond to a variety of nonspecific substances, such as irritants. In the laboratory, this phenomenon has been studied by observation of the nasal response to nasal secretagogues, such as histamine and methacholine. Patients challenged with allergen, followed 24 hours later by a histamine challenge, showed increased sensitivity to histamine compared with a baseline histamine challenge.163 In another investigation, allergen-induced increases in eosinophils 24 hours after challenge correlated with the magnitude of reactivity to histamine.164 Nasal provocation also has been shown to cause nasal hyperresponsiveness to methacholine.165 In allergic patients during the allergy season, the hyperresponsiveness caused by nonspecific irritants probably reflects complex interactions among inflammatory cellular influx, epithelial injury, and increased end-organ responsiveness caused by exposure to allergen.
Integration of Pathophysiologic Events
Sensitization of the nasal mucosa to a certain allergen entails multiple interactions among APCs, T lymphocytes, and B cells that lead to the production of antigen-specific IgE antibodies, which then bind to mast cells and basophils. Subsequent allergen exposure leads to cross-linking of specific IgE molecules on mast cells and their resultant degranulation, with the release of preformed mediators and synthesis of newly generated mediators. Other proinflammatory substances also are generated after allergen exposure, including eosinophil products and cytokines. Cytokines are thought to be generated in part by Th2 lymphocytes and by mast cells. Cytokines upregulate adhesion molecules on the vascular endothelium, and possibly on marginating leukocytes, and lead to the migration of these inflammatory cells into the site of tissue inflammation. Various cytokines will also promote the chemotaxis and survival of these recruited inflammatory cells and lead to a secondary immune response by virtue of their capability to promote IgE synthesis by B cells. The nervous system also plays an important role by amplifying and perpetuating allergic reactions. These inflammatory changes lower the threshold of mucosal responsiveness to various specific and nonspecific stimuli, making allergic patients more responsive to stimuli to which they are exposed every day (Fig. 42-3).

Local Allergic Rhinitis
More recently, investigators have described a subgroup of patients who were initially classified as having nonallergic rhinitis but exhibited symptoms resembling those in patients with allergic rhinitis despite a negative response on allergy testing. These subjects frequently exhibited an increase in eosinophils and mast cells in their nasal mucosa, and most important, they responded to localized nasal allergen challenge with clinical symptoms. Several studies have confirmed that IgE can be produced locally in the target tissue.166,167 Discrepancies between systemic evidence of sensitization and clinical symptoms may therefore be explained by local IgE production. This entity has been termed local allergic rhinitis and may account for a subset of patients who have been diagnosed as having NARES. The hallmark of this type of rhinitis is a positive response to nasal allergen challenge. Although as noted, the production of IgE locally in the nose in the context of a local allergic response is not a new concept,168 interest in this issue has recently been renewed. Carney and colleagues evaluated three groups of subjects: asymptomatic normal subjects, patients with allergic rhinitis and positive reaction on allergy testing (R+ST), and subjects with chronic rhinitis and negative response on allergy testing (R−ST).169 They performed nasal allergen challenges in all groups and found that although none of the control group subjects had a positive response to challenge, all of the R+ST patients and 62% of the R−ST patients had positive responses to challenge. A majority of the responders (85%) had the response after house dust mite provocation. In a similar study, investigators compared the nasal and serum inflammatory profiles for these same categories of patients.59 In the R−ST group, 27 of 50 patients had a positive response to nasal challenge with dust mite. In evaluating inflammatory markers of the R−ST group, levels of nasal eosinophils, T cells, eosinophil cationic protein (ECP), and dust mite–specific IgE were higher than in normal control subjects. In a follow-up study, Rondon and associates performed nasal allergen challenges in R−ST patients and noted significant increases in tryptase, ECP, and specific IgE in nasal lavage fluid samples compared with baseline.170 These changes are comparable with those in patients with R+ST, demonstrating that local allergic rhinitis is truly an allergic phenomenon.
Nonallergic Rhinitis
Nonallergic rhinitis is characterized by symptoms of rhinitis without evidence of atopy on either skin or serum specific IgE testing. This entity encompasses different phenotypes that have not been very well characterized and are hard to include in one category.
In patients characterized as having idiopathic, or vasomotor, rhinitis, the nasal mucosa often does not show any evidence of inflammation.171 Furthermore, these individuals do not exhibit hyperresponsiveness to histamine, a hallmark of allergic rhinitis but rather show increased reactivity to cold dry air.172 Both symptoms and hyperresponsiveness to cold dry air decrease after capsaicin treatment.173 These observations suggest that the processes underlying this phenotype of nonallergic rhinitis probably involve a sensory neural dysregulation in which capsaicin-sensitive nerves may be important.
Other patients with presumed idiopathic rhinitis demonstrate evidence of autonomic imbalance with parasympathetic dominance, which theoretically can produce excessive rhinorrhea. A few studies have provided some data suggesting abnormal responses to autonomic tests in those patients. In some patients, increased parasympathetic activity is reported,174 whereas in others, more generalized autonomic dysfunction including both the sympathetic and parasympathetic nervous systems have been demonstrated.175
Treatment
Allergen Avoidance Measures
Avoidance of offending allergens is considered the first line of treatment for allergic rhinitis. Multiple measures for avoidance have been advocated, and these measures typically are targeted at controlling indoor allergens, especially dust mites, animal danders, and molds.
With regard to house-dust mite control measures, a recent systematic review demonstrated that single measures are not effective in reducing symptoms in patients with allergic rhinitis.176 In an expanded analysis of data on patients with mite rhinitis, nine additional placebo-controlled trials of mite avoidance measures were evaluated.177 Despite the limitations of this review, which included trials that were either small in size or of suboptimal methodologic quality, the authors conclude that the use of acaricides and extensive bedroom-based environmental control programs are beneficial in reducing rhinitis symptoms due to dust mites. Of importance, the isolated use of dust mite–impermeable bedding is unlikely to prove effective. Supporting these conclusions, a large study investigated the effects of allergen-impermeable casings in patients with mite-induced rhinitis and showed that mattress and pillow covers reduced the levels of mattress of dust mite allergen Der p 1 by 30% of baseline but resulted in no difference in the clinical symptoms of allergic rhinitis.178
A number of different strategies have also been used to reduce cat allergen in homes. One study has demonstrated that several preventive measures including removal of carpeting, tannic acid application, washing bedding, and washing the cat resulted in a reduction of levels of Fel d 1 in the house and abatement of clinical symptoms of allergic rhinitis.179 HEPA (high-efficiency particulate air) filters also have been used as a solitary means to reduce symptoms and have not been found effective.180 Overall, the most effective approach to reduction of indoor cat allergen is removal of the cat from the indoor environment. Even this measure, however, may not be immediately effective, because residual allergen may remain at relatively high levels in the carpeting and upholstered furniture for several months or longer.180 After removal of the cat, therefore, all carpeting should be taken up and upholstered furniture cleaned.
Exposure to outdoor allergens, such as grass, tree and weed pollens, and outdoor mold spores, is very difficult to control. Allergy to these ubiquitous triggers is therefore best addressed with pharmacotherapy and/or immunotherapy.
Pharmacotherapy
Antihistamines
H1 antihistamines block histamine at the H1 receptor and are commonly used in the treatment of allergic rhinitis. These medications include older first-generation drugs (e.g., diphenhydramine) that are highly lipophilic and newer, second-generation antihistamines (e.g., loratadine), which are significantly less lipophiic.
Oral H1 antihistamines have been shown to reduce histamine-mediated symptoms and signs such as sneezing, itching, rhinorrhea, and eye symptoms but are not as effective in alleviating nasal congestion.181 Several agents in this category have been demonstrated to improve quality of life as measured by generic and disease-specific tools.182 They are rapidly absorbed after oral administration and begin to provide relief within 1 to 2 hours. Oral H1 antihistamines also have been shown to be safe and effective in children, and many are available in liquid form.183
In addition to antagonizing histamine at the H1 receptor, some antihistamines have antiinflammatory properties such as inhibiting histamine release, reducing the production of leukotrienes, inhibiting allergen-induced nonspecific responsiveness, and reduction of soluble ICAM-1 levels in nasal secretions.184,185 These additional properties, however, do not seem to translate into enhanced clinical efficacy, so their clinical importance is not clear.
The side effects of first-generation antihistamines can be bothersome. The most important of these is sedation, which is reported in approximately 20% of patients. It is therefore essential to warn patients receiving these drugs about their effect on daily activities such as driving or operating heavy machinery. The development of nonsedating antihistamines in the 1980s eliminated this problem. The newer nonsedating antihistamines have few effects on performance and a low reported incidence of sedation. The second-generation antihistamines include loratadine, cetirizine (both available over the counter), desloratadine, fexofenadine, and levocetirizine. Both cetirizine and levocetirizine are labeled by the U.S. Food and Drug Administration (FDA) as sedating but cause less sedation than the first-generation antihistamines.
H1 antihistamines also are available for intranasal administration. Azelastine, a phthalazinone derivative, is available in the United States for the treatment of allergic rhinitis. The efficacy of topical azelastine is comparable with that of oral antihistamines; This agent, which usually is given twice daily, may cause alteration of taste sensation and has been reported to occasionally cause somnolence.186 Azelastine can be distinguished from oral antihistamines in that it significantly reduces nasal congestion as well as itching, sneezing, and runny nose. A reformulated preparation of intranasal azelastine with sucralose as a taste-masking agent is comparable in efficacy with the original formulation in seasonal allergic rhinitis, with less bitter taste side effects.
Olopatadine hydrochloride has been shown to be safe and effective for the treatment of seasonal allergic rhinitis and usually is administered twice daily. The most commonly reported adverse reaction is bitter taste, and the incidence of somnolence is minimally higher than with placebo vehicle.187
Intranasal azelastine also is indicated for the relief of nasal symptoms in so-called vasomotor nonallergic rhinitis. Banov and colleagues reported the results of two parallel, randomized, placebo-controlled, double-blind studies evaluating 3 weeks of treatment with intranasal azelastine, 2 sprays per nostril twice daily, in subjects with vasomotor rhinitis with symptoms for at least 1 year, negative responses on skin testing, and a nasal cytology examination negative for eosinophilia.188 These investigators showed significant improvement in sneezing, nasal congestion, postnasal drip, and rhinorrhea in the actively treated group of patients compared with those receiving placebo.
Decongestants
Decongestants reduce nasal congestion but have no other significant effects on the symptoms of rhinitis. Both topical and systemic decongestants act by α-adrenergic stimulation, which results in vascular constriction and a reduction of nasal blood supply to the sinusoids. Topical decongestants can be either catecholamines (such as phenylephrine) or imidazoline derivatives (such as xylometazoline or oxymetazoline) and have a more rapid onset of action and stronger effect than systemic decongestants. Topical decongestants do not have systemic side effects; however, in children there have been rare case reports of seizures. When these agents are used for longer than 5 days, rebound nasal congestion may develop in some patients (see earlier). Therefore topical decongestants should be used primarily to reduce nasal congestion in patients with acutely severe rhinitis due to allergy or viral infections in order to facilitate the penetration of intranasal corticosteroids.
Oral decongestants do not cause rebound congestion but are not as effective as topical formulations. Pseudoephedrine hydrochloride and phenylephrine are the most commonly used. Phenylpropanolamine, a once-popular drug, has been taken off the market in the United States because of increased risk of hemorrhagic stroke in women when used as an appetite suppressant.189 Agents that combine an oral decongestant, usually pseudoephedrine, with an antihistamine are used for the treatment of allergic rhinitis as well as for cough and cold. Phenylephrine is another over-the-counter decongestant, also used in combination products, but a recent meta-analysis showed lack of efficacy of this agent on both objective and subjective measures of nasal congestion compared with placebo.190 The most common side effects of oral decongestants are insomnia and irritability, which can occur in as many as 25% of patients taking these medications. At normal doses, aggravation of hypertension and cardiac arrhythmias may occur. Taken in overdose, these agents may result in renal failure, psychosis, strokes, and seizures. They should therefore be largely avoided in patients with hypertension, heart disease, seizure disorders, hyperthyroidism, and prostatic hypertrophy and in those taking monoamine oxidase inhibitors.
Intranasal Corticosteroids
Intranasal corticosteroids are the most potent drugs available for the management of allergic rhinitis, which may relate to their diverse antiinflammatory effects. In nasal allergen challenge models of allergic rhinitis, pretreatment with an intranasal steroid (INS) results in significant inhibition of mediator release during both the early and late phase reactions, along with a significant inhibition of the influx of basophils, eosinophils, neutrophils, and mononuclear cells in nasal secretions.191 These agents also cause a reduction in the number of inflammatory cells and Th2-type cytokines within the nasal mucosa of patients with allergic rhinitis.192 INSs also reduce the antigen-induced hyperresponsiveness of the nasal mucosa to subsequent antigen and histamine provocation.191 On the basis of these favorable antiinflammatory effects of INSs, several placebo-controlled clinical trials using a variety of these agents demonstrated their effectiveness in the reduction of all nasal symptoms in both seasonal193 and perennial194 allergic rhinitis. In comparative studies in allergic rhinitis, INSs have been shown to be superior in efficacy to both H1 antihistamines195 and leukotriene receptor antagonists.196 An unexpected benefit of use of INSs in patients with allergic rhinitis is a significant reduction in concomitant allergic ocular symptoms197 (see “Medications for Ocular Symptoms”).
INSs begin to have effects within 7 to 8 hours of dosing, although some reports demonstrate an effect within 2 hours.198,199 With known seasonal allergic rhinitis, it often is reasonable to start treatment 1 week before the beginning of the pollen season and then reevaluate the patient 2 weeks later. During this visit, the nose should be examined for signs of local irritation from the drug or mechanical trauma from the applicator itself, and the patient's response to treatment should be assessed. If a favorable clinical response is reported, the dose of INS can be lowered, while keeping in mind the load of allergen in the environment, with the aim of reaching the minimal dose that will provide symptomatic relief. Although continuous use usually is recommended, some studies have demonstrated the superiority of as-needed use of intranasal fluticasone propionate to placebo.200
Local nasal irritation, the principal side effect of INSs, occurs in approximately 10% of patients. The incidence of epistaxis with different INS preparations ranges from 4% to 8% during 2 weeks of use, with higher incidence in studies conducted for more than 1 year. In patients with perennial rhinitis treated with fluticasone propionate or mometasone furoate continuously for 1 year, nasal mucosal biopsy specimens showed no evidence of atrophy and normalization of the epithelium.201 Rarely, septal perforations and Candida overgrowth have been reported. With regard to potential systemic effects, INSs that have been subjected to rigorous study have not been shown to affect parameters such as growth in children.202 Despite these reassuring findings, it is recommended that pediatric patients receiving INSs be evaluated every 6 months using a stadiometer to monitor growth.
INSs also have been shown to be effective in the treatment of nonallergic rhinitis. Among the available preparations, fluticasone propionate and fluticasone furoate are approved by the FDA for the treatment of nonallergic rhinitis in addition to allergic rhinitis. In a large study that included patients with nonallergic rhinitis with and without eosinophilia, fluticasone propionate nasal spray in tw different doses (200 and also 400 µg daily) was shown to be significantly more effective than placebo in reduction of the total nasal symptom score, with no difference between the two concentrations.203 In addition, other evidence supports efficacy of intranasal budesonide and mometasone in some patients with perennial nonallergic rhinitis.204,205 On the other hand, a more recent study evaluating the effect of fluticasone furoate administered intranasally in patients with weather- or temperature-sensitive vasomotor rhinitis showed no significant benefit over placebo, suggesting that all types of nonallergic rhinitis may not be equally responsive to INSs.43 Because of the preponderance of positive data, however, a reasonable approach is to use these INSs or intranasal antihistamines as first-line agents for therapy of nonallergic rhinitis.
Systemic Corticosteroids
The role of systemic steroids in the treatment of rhinitis is limited because of their adverse effects and the limited morbidity of the disease. They are best reserved for patients with any type of rhinitis, including the allergic form, NARES, or rhinitis medicamentosa, who present initially with severe nasal obstruction. A short course of oral prednisone, 30 mg daily for 3 to 5 days, with or without a rapid taper (depending on the severity of the condition) usually will significantly decrease nasal edema and allow for enhanced penetration of INS.
Intramuscular injections of corticosteroids have been a popular therapy dating back many years. Data demonstrating efficacy are limited, however. Use of intramuscular injections of depot steroids generally should be avoided for the treatment of seasonal allergic rhinitis because of the risk of rare but potentially catastrophic side effects, particularly aseptic necrosis of the femoral head. In addition, as seasonal rhinitis is usually a life-long disease, patients who request and receive this treatment multiple times per year for many years may be at increased risk for long-term effects of systemic corticosteroids, such as cataracts and osteoporosis
Leukotriene Inhibitors
Because leukotrienes are generated in allergic rhinitis, the effects of inhibitors of the 5-lipoxygenase pathway (zileuton) and leukotriene receptor antagonists (montelukast and zafirlukast) have been investigated. By far, the most commonly used agent in this category is montelukast, which is approved in the United States for the treatment of seasonal and perennial allergic rhinitis in adults and children. In placebo-controlled studies, montelukast has repeatedly been shown to be more effective than placebo and equal in effectiveness to antihistamines for relief of all ocular and nasal symptoms of allergic rhinitis, including congestion, rhinorrhea, and sneezing.206 The combination of montelukast and loratadine was found to be superior to either agent used alone. Despite initial enthusiasm for combining a leukotriene receptor antagonist with an antihistamine in allergic rhinitis, subsequent large studies have not found benefit over either agent used alone.207
Cromolyn Sodium
Intranasal cromolyn sodium 4% solution is available over the counter and has been shown to be clinically effective in the treatment of allergic rhinitis. As with antihistamines, it is more helpful for sneezing, itching, and rhinorrhea and less effective in relieving nasal congestion. Its mode of action is unclear, and treatment is most effective when dosing is started before the onset of symptoms. The recommended dosage frequency is four to six times daily, leading to compliance problems, but the drug is very safe, especially in children and pregnant women.
Anticholinergics
Anticholinergic drugs are useful in the treatment of those patients in whom rhinorrhea is the predominant complaint. Ipratropium bromide has little or no systemic effect when administered intranasally and has been shown to be effective in controlling watery nasal discharge in perennial allergic rhinitis.208 It has no effect, however, on sneezing, itching, or nasal congestion. Ipratropium can be used in conjunction with drugs of other classes, such as antihistamines or intranasal corticosteroids, for the treatment of rhinorrhea in patients with allergic rhinitis.
Ipratropium bromide also is useful for the treatment of watery discharge that occurs in patients with perennial nonallergic rhinitis.209 In addition, ipratropium has been found to effectively reduce rhinorrhea associated with gustatory rhinitis and rhinorrhea induced by exposure to cold, dry air.210,211
Medications for Ocular Symptoms
Allergic rhinitis often is associated with eye symptoms, which represent a combination of the direct effects of allergen deposition on the conjunctiva as well as reflexes between the nose and the eye. Oral H1 antihistamines and leukotriene receptor antagonists have demonstrated efficacy in reducing ocular redness, tearing, and itch. Topical ocular antihistamines frequently are prescribed as adjunctive agents for patients with rhinoconjunctivitis and as the primary medication for patients with isolated allergic conjunctivitis.212 As would be expected with topical therapy, these drugs begin to work within a few minutes and have a 12- to 24-hour duration of action. The various agents are available as both over-the-counter and prescription products.
INSs also have been shown to have significant effects in reducing allergic eye symptoms. In a meta-analysis comparing oral H1 antihistamines and intranasal corticosteroids for the control of ocular symptoms, no difference was found in the efficacy of these two classes.213 The mechanism of this favorable effect of INSs is speculated to be reduced intranasal inflammation, which in turn inhibits the nasal ocular reflex initiated by allergen contact to the nasal mucosa.
Combinations of Medications
Often, a single pharmacologic agent does not effectively reduce symptoms of rhinitis. As noted above, oral antihistamines are frequently combined with oral decongestants to treat allergic rhinitis. More recently, physicians have been combining intranasal antihistamines with intranasal corticosteroids. In a study of intranasal azelastine plus intranasal fluticasone propionate versus individual components in patients with seasonal allergic rhinitis, the combination was statistically superior to placebo, as well as to either active agent alone.214 Compared with the azelastine-fluticasone combination, olopatadine nasal spray coupled with fluticasone seemed to be equally effective in symptom control.215 The combination of these two classes appears to improve upon the efficacy of INS, with minimal side effects.
In clinical practice, oral antihistamines frequently are combined with INSs in patients who do not respond to antihistamines alone. Nevertheless, studies of INS given together with oral H1 antihistamines, including loratadine and cetirizine, have not shown that the combination is significantly better than INS given alone.216,217 These data suggest that patients who do not respond adequately to oral antihistamines can be switched to the INS and then the antihistamine can be stopped. With respect to combination treatment of eye symptoms, intranasal fluticasone propionate plus intraocular olopatadine was significantly more effective than the combination of fluticasone and fexofenadine, tested using an ocular challenge model.218
Allergen Immunotherapy
Specific allergen immunotherapy has been shown to be effective in seasonal and perennial allergic rhinitis.219 The principal advantages of immunotherapy over pharmacotherapy are that it generally is more efficacious and that 2 consecutive years of treatment results in persistent tolerance.219a Immunotherapy should be considered in a number of clinical scenarios, including severe allergic rhinitis unresponsive to usual pharmacotherapy and allergen avoidance measures; allergic rhinitis complicated by other disorders, particularly new-onset or worsening asthma; and occurrence of significant adverse effects from medications for rhinitis. In addition, in patients who desire a more lasting improvement in their allergic rhinitis, a strong case can be made that immunotherapy is a cost-effective alternative to pharmacotherapy.220 Allergy immunotherapy is most effective when a single dominant allergen, such as dust mite or pet dander, is identified. In much of Europe, sublingual immunotherapy is the method of choice, and a limited number of allergens are administered, whereas in the United States, the subcutaneous route is used, and most or all sensitized allergens are included in the therapeutic extract. Experimental comparisons between these two modes of delivery, as well as studies of which allergens provide optimal efficacy, are ongoing and conceivably will resolve many of the controversies that currently exist.
Surgery
Individuals with a significant anatomic nasal defect (e.g., nasal septal deviation) may require surgery if nasal obstruction is of a degree that adversely affects quality of life. In patients with chronic rhinitis, in the absence of a structural abnormality, surgery is rarely indicated. Turbinate reduction surgery should be used in patients with refractory mucosal edema only if pharmacotherapy and immunotherapy have been tried and failed.
Overall Approach to Treatment
Allergic Rhinitis
The following approach to treatment is based on recent national and global recommendations219,221 (Fig. 42-4). In patients with mild, intermittent symptoms of allergic rhinitis who complain primarily of rhinorrhea or sneezing, a nonsedating oral or topical intranasal antihistamine, taken as needed, often is very effective. In patients with a significant component of nasal congestion, an INS, an antihistamine-decongestant combination pill, or montelukast, taken as needed, may be helpful. If persistent symptoms are present, particularly nasal congestion, an INS given regularly may be effective.
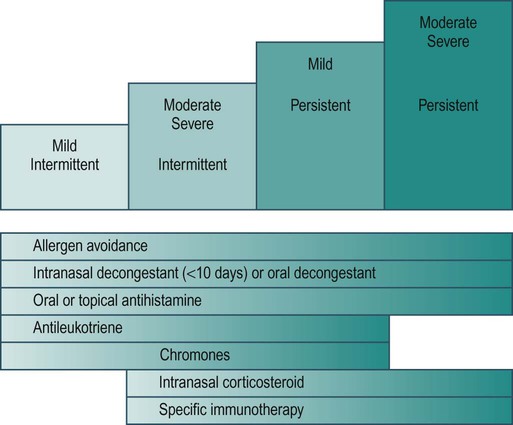
Patients with moderate to severe symptoms should be reevaluated after 2 weeks to assess response to therapy. With an excellent response, anticipated exposures should be considered and the patient treated accordingly. With a partial response, residual complaints should be identified and targeted with specific medications. For significant eye symptoms, an intraocular antihistamine can be taken as needed. If significant redness of the eye persists, referral to an ophthalmologist should be considered. For residual nasal congestion, the addition of an intranasal antihistamine may be the most useful of all options. If rhinorrhea persists as a primary problem, ipratropium bromide may provide additional benefit. If the patient does not improve after maximal medical therapy, the diagnosis should be reconsidered, along with the need for additional diagnostic testing (e.g., CT of the sinuses or nasal endoscopy). For refractory allergic rhinitis that fails to respond to the foregoing treatments, in the absence of obvious complicating factors, consideration for allergy immunotherapy is in order. A stepped-care approach to the treatment of allergic rhinitis is shown in Figure 42-4.
Nonallergic Rhinitis
In patients with persistent anterior or posterior discharge associated with any of the forms of nonallergic rhinitis, particularly when it is thick in consistency, nasal irrigation with saline may be very helpful. Nasal saline washes also are extremely important in the management of nasal crusting, as seen in atrophic rhinitis. Nasal saline may have no effect on nasal congestion, however, and other medications will be important in alleviating this symptom.
In patients with chronic congestion, an INS or intranasal azelastine should be administered as a first-line pharmacologic agent, used on an intermittent or as-needed basis. Nasal cytology may be helpful in guiding therapy, as a predominance of eosinophils (i.e., NARES) would suggest the use of INS, whereas an absence of eosinophils makes azelastine a preferred choice. As in allergic rhinitis, if either agent alone is not completely effective, the addition of the other drug may be useful.
In patients with intermittent acute, watery rhinorrhea caused by irritant or cold air exposure, exercise, or food, ipratroprium bromide used before symptoms occur can be very effective.
For patients using medications, such as antihypertensives, that are probable factors in the pathogenesis of their rhinitis, a change in therapy should be considered. If, however, a particular medication is deemed necessary and irreplaceable (e.g., phosphodiesterase-5 [PDE5] inhibitor in prostate disease), the nasal side effects may need to be medicated. This is best accomplished with topical therapy in order to avoid drug interactions and/or additional systemic adverse effects.
Treatment in Special Populations
Pregnancy
In women with rhinitis of pregnancy, nondrug therapies should be tried first. A controlled trial of nasal rinsing with hypertonic saline has been shown to be significantly more effective than no therapy, with reductions in nasal symptoms and antihistamine use.222 Over-the-counter mechanical nasal dilators223 also may be helpful, although this means of relief of obstruction may be unacceptable to many patients. Intranasal corticosteroids, although quite effective in allergic and nonallergic rhinitis, have not been shown to reduce the symptoms of rhinitis of pregnancy.224
In patients with allergic rhinitis who are sensitive to indoor allergens, environmental control measures should be used aggressively as a means of reducing the need for medication, and nasal saline rinses should be performed on a regular basis. In many women, medications will be required. Nasal cromolyn, up to one spray 4 to 6 times daily, should be tried next, because of its excellent safety profile and FDA pregnancy category B rating.225
If a 2-week course of cromolyn is not helpful, particularly if nasal congestion is present, a trial of an INS is indicated. Although most intranasal corticosteroids are given an FDA pregnancy category C rating (with the exception of budesonide, in category B), gestational risk has not been confirmed in observational human data, and the reported safety data on all of the available compounds are reassuring. A recent meta-analysis concluded that the use of intranasal corticosteroids during pregnancy does not increase the risk of major malformations, preterm delivery, low birth weight, and pregnancy-induced hypertension.226 If the patient is already being treated with an INS and her rhinitis is well controlled, continuation of her current therapy is reasonable, although some physicians may opt to switch the medication to budesonide. When intranasal corticosteroid therapy is started during pregnancy, budesonide frequently is the drug of choice because of the category B rating.227
Oral antihistamines may be worth considering if primary complaints include rhinorrhea, sneezing, and pruritus and the patient prefers oral therapy. If use of an oral antihistamine is appropriate, both diphenhydramine and chlorpheniramine have a very long record of use in pregnancy and frequently are the drugs of choice for obstetric patients.228 In a significant subset of women, however, the central nervous system and anticholinergic effects of these agents will prove difficult to tolerate. Loratadine and cetirizine have been extensively studied during pregnancy, and both belong to pregnancy category B. Topical antihistamines, including olapatadine and azelastine, do not have a long history of use in pregnancy and belong to FDA category C. For these reasons, the other medications listed here would be considered more appropriate choices in pregnancy.
Oral decongestants should be avoided, if possible, during the first trimester because of conflicting reports of an association of phenylephrine and pseudoephedrine with congenital malformations such as gastroschisis and small intestinal atresia.229
Specific allergen immunotherapy for allergic rhinitis may be continued during pregnancy if it is providing significant benefit and has not caused systemic reactions. Allergen extract doses should be maintained and not increased until the completion of the pregnancy. For these same reasons, immunotherapy should not be started during pregnancy.
Elderly
Two of the most important aspects of treating rhinitis in older patients are improving intranasal moisture content and removing dried secretions.94 Nasal irrigation using buffered saline or a saline nasal spray should be used by most elderly people with chronic rhinitis, particularly those with nonallergic rhinitis. INS, although generally safe, may cause more bleeding than is usually seen in younger patients, owing to the increased fragility of the nasal mucous membranes in this population. In general, older-generation oral antihistamines should be avoided because of their potential to sedate or cause anticholinergic effects. Oral decongestants should be similarly avoided owing to possible adverse effects on blood pressure (hypertension), cardiac rhythm (extrasystoles, arrhythmias), central nervous system (insomnia, agitation), and urinary tract (obstruction).
Competitive Athletes
Treatment of rhinitis in competitive athletes must consider whether a medication is banned by specific sports bodies, such as the U.S. or International Olympic committees. Intranasal corticosteroids and topical nasal decongestants are approved by the U.S. Olympic committee, whereas oral decongestants are completely banned.
Effect of Rhinitis Therapy on Asthma
In population-based studies, treatment of rhinitis with INS has been shown to reduce the need for hospitalization and emergency department visits.230 Whereas an initial small study of intranasal corticosteroids in patients with seasonal allergy demonstrated a significant reduction in asthma symptoms,231 a recent large-scale study did not.232 A growing number of small trials have revealed that intranasal corticosteroids do reduce bronchial hyperresponsiveness to inhaled methacholine233 and exercise234 in patients with seasonal or perennial allergic rhinitis and mild asthma. Taken together, these results suggest that treatment of asthma with INS may have a salutary effect on asthma severity.
Summary
During the past 10 to 15 years, prospective studies of large populations have significantly improved our understanding of the epidemiology of chronic rhinitis in both children and adults. Simultaneously, advances in the basic science of allergic mechanisms have provided new and important insights into the pathophysiology of rhinitis. An integrated approach to therapy, including environmental control measures, pharmacotherapy, and allergy immunotherapy, will provide significant relief of symptoms and improvements in quality of life in the vast majority of patients with allergic rhinitis.