Chapter 7
Cardiology
, and
I. Websites
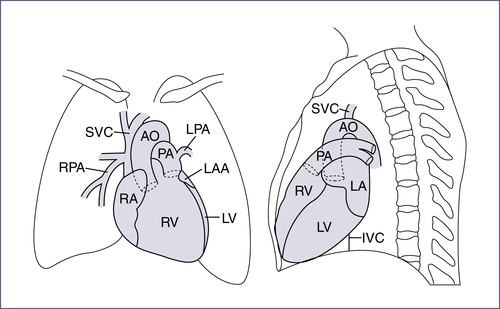
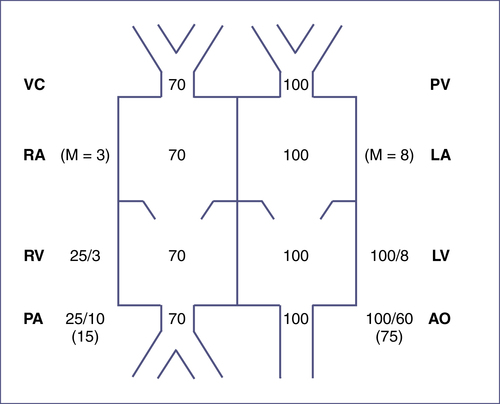
II. The Cardiac Cycle (Fig. 7-1)

III. Physical Examination
A. Heart Rate
Refer to Table 7-4 for normal heart rate (HR) by age.
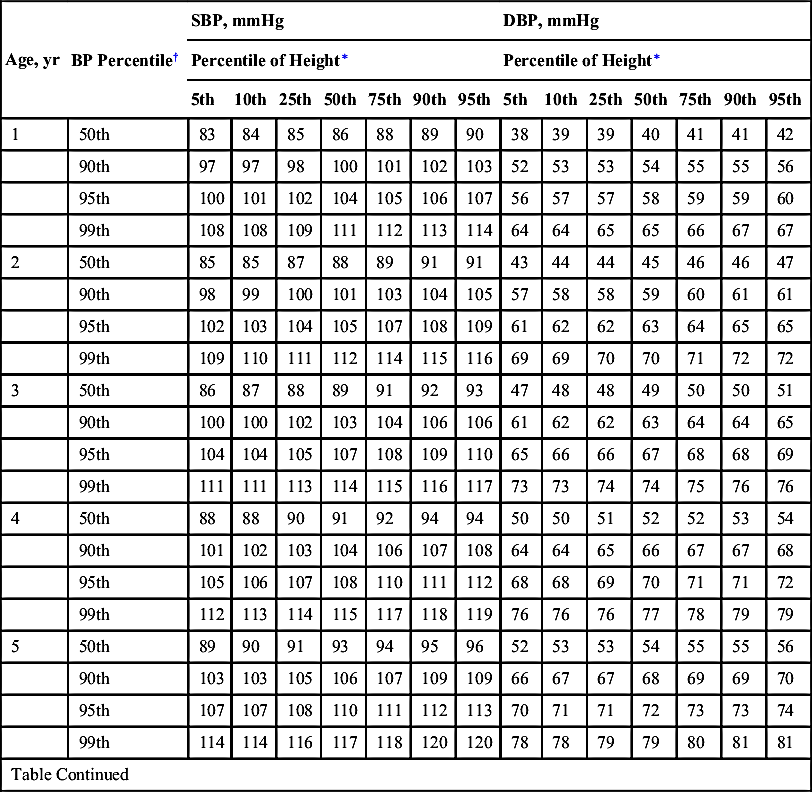
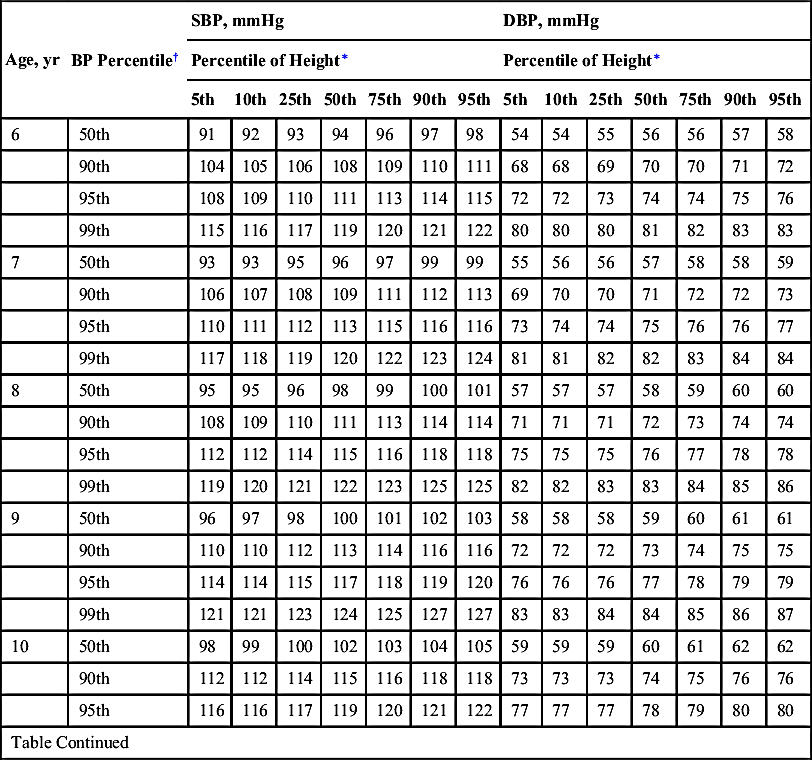
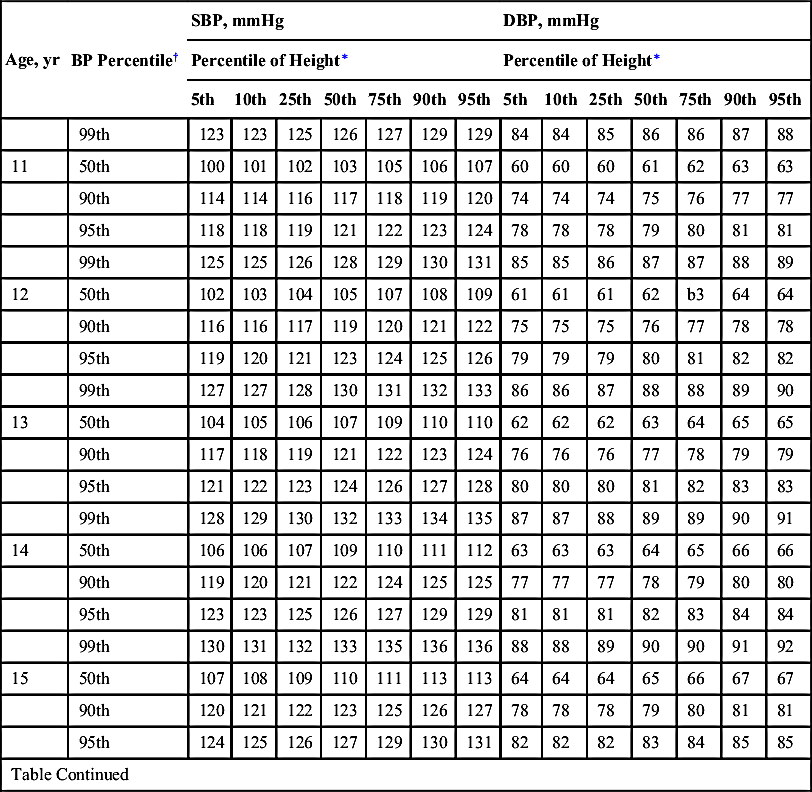
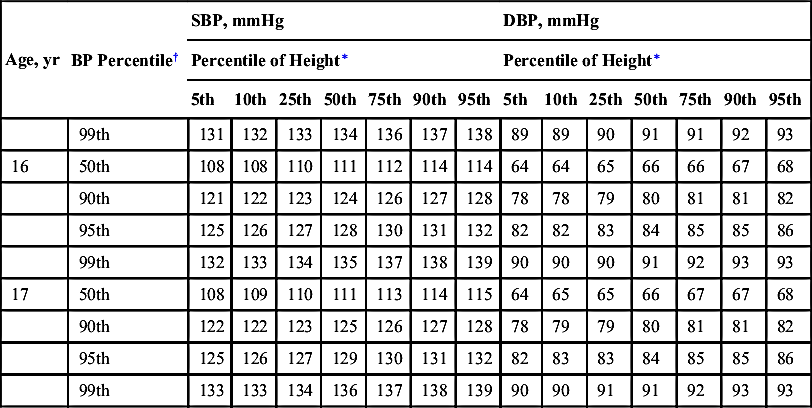
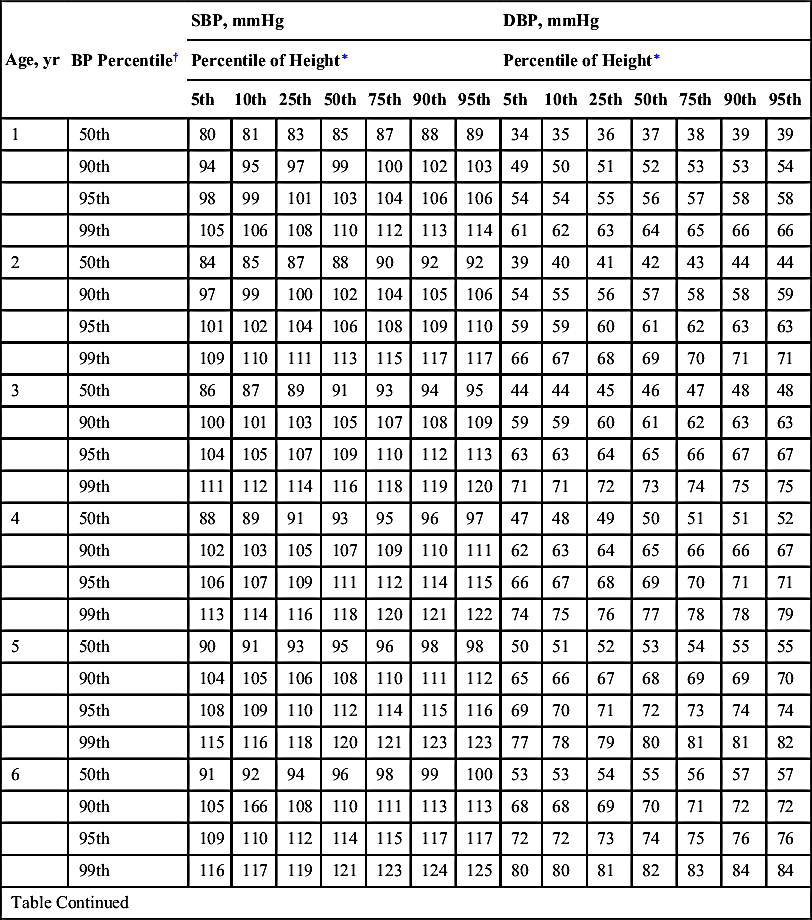
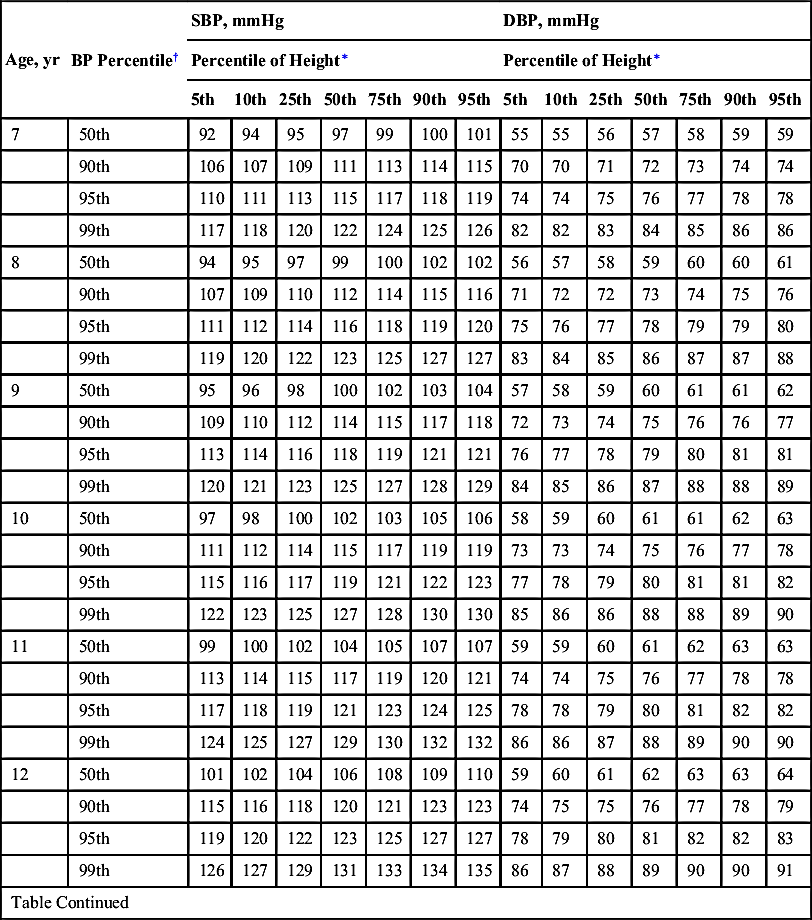
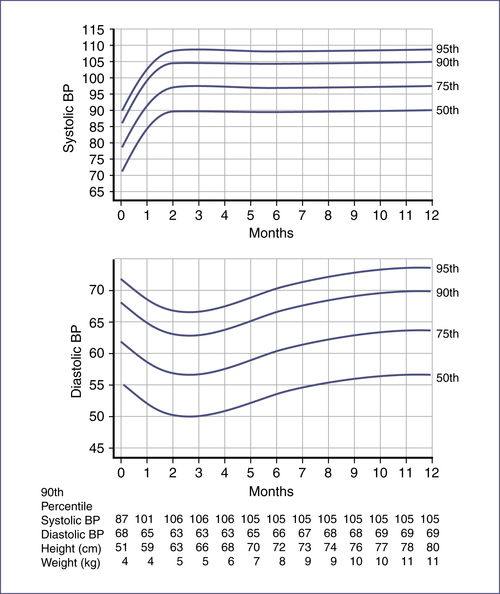
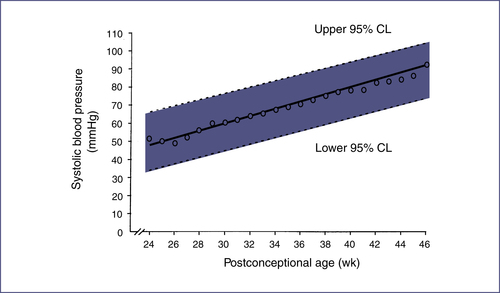
B. Blood Pressure
1. Blood pressure:
a. Blood pressure norms (systolic blood pressure [SBP], diastolic blood pressure [DBP]) by age1,2: Tables 7-1 and 7-2; Figs. 7-2, 7-3, and 7-4
For blood pressure norms for preterm infants, see Expert Consult: Table EC 7-A
.
2. Pulse pressure = systolic pressure − diastolic pressure.
a. Wide pulse pressure (>40 mmHg): Differential diagnosis includes aortic insufficiency, arteriovenous fistula, patent ductus arteriosus, thyrotoxicosis, warm shock.
b. Narrow pulse pressure (<25 mmHg): Differential diagnosis includes aortic stenosis, pericardial effusion, pericardial tamponade, pericarditis, significant tachycardia, cold shock.
3. Mean arterial pressure (MAP)
a. MAP = diastolic pressure + (pulse pressure/3) OR 1/3 systolic pressure + 2/3 diastolic pressure.
b. Preterm infants and newborns: Normal MAP = gestational age in weeks + 5.
4. Abnormalities in blood pressure
a. Four-limb blood pressure measurements can be used to assess for coarctation of the aorta; pressure must be measured in both the right and left arms because of the possibility of an aberrant right subclavian artery.
b. Pulsus paradoxus: Exaggeration of the normal drop in SBP seen with inspiration. Determine SBP at the end of exhalation and then during inhalation; if the difference is > 10 mmHg, consider pericardial effusion, tamponade, pericarditis, severe asthma, or restrictive cardiomyopathies.
C. Heart Sounds
1. S1: Associated with closure of mitral and tricuspid valves; heard best at the apex or left lower sternal border (LLSB).
2. S2: Associated with closure of pulmonary and aortic valves; heard best at the left upper sternal border (LUSB) and has normal physiologic splitting that increases with inspiration.
3. S3: Heard best at the apex or LLSB.
4. S4: Heard at the apex.
E. Murmurs4
TABLE EC7-A
BLOOD PRESSURES AFTER 2 WEEKS OF AGE IN INFANTS FROM 26–44 WEEKS POSTCONCEPTIONAL AGE
| Postconceptional Age | 50th Percentile | 95th Percentile | 99th Percentile |
| 44 WEEKS | |||
| SBP | 88 | 105 | 110 |
| DBP | 50 | 68 | 73 |
| MAP | 63 | 80 | 85 |
| 42 WEEKS | |||
| SBP | 85 | 98 | 102 |
| DBP | 50 | 65 | 70 |
| MAP | 62 | 76 | 81 |
| 40 WEEKS | |||
| SBP | 80 | 95 | 100 |
| DBP | 50 | 65 | 70 |
| MAP | 60 | 75 | 80 |
| 38 WEEKS | |||
| SBP | 77 | 92 | 97 |
| DBP | 50 | 65 | 70 |
| MAP | 59 | 74 | 79 |
| 36 WEEKS | |||
| SBP | 72 | 87 | 92 |
| DBP | 50 | 65 | 70 |
| MAP | 57 | 72 | 71 |
| 34 WEEKS | |||
| SBP | 70 | 85 | 90 |
| DBP | 40 | 55 | 60 |
| MAP | 50 | 65 | 70 |
| 32 WEEKS | |||
| SBP | 68 | 83 | 88 |
| DBP | 40 | 55 | 60 |
| MAP | 48 | 62 | 69 |
| 30 WEEKS | |||
| SBP | 65 | 80 | 85 |
| DBP | 40 | 55 | 60 |
| MAP | 48 | 65 | 68 |
| 28 WEEKS | |||
| SBP | 60 | 75 | 80 |
| DBP | 38 | 50 | 54 |
| MAP | 45 | 58 | 63 |
| 26 WEEKS | |||
| SBP | 55 | 72 | 77 |
| DBP | 30 | 50 | 56 |
| MAP | 38 | 57 | 63 |

DBP, Diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure.
Data from Dionne J et al. Hypertension in infancy: diagnosis, management, and outcome. Pediatr Nephrol. 2012;27:17-32.
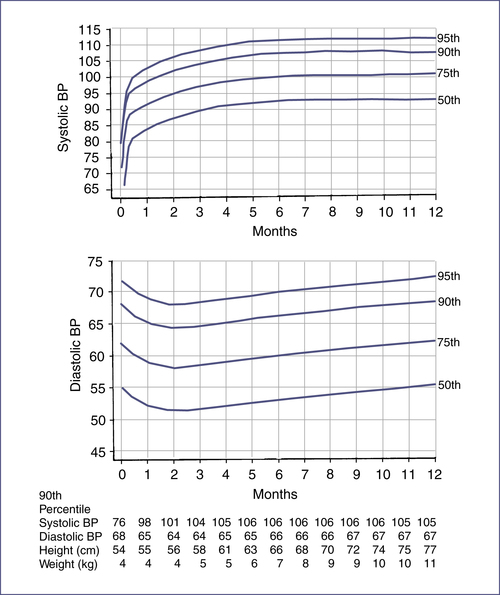
TABLE 7-1
BLOOD PRESSURE LEVELS FOR THE 50TH, 90TH, 95TH, AND 99TH PERCENTILES OF BLOOD PRESSURE FOR GIRLS AGE 1–17 YEARS BY PERCENTILES OF HEIGHT2
| Age, yr | BP Percentile† | SBP, mmHg | DBP, mmHg | ||||||||||||
| Percentile of Height∗ | Percentile of Height∗ | ||||||||||||||
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 1 | 50th | 83 | 84 | 85 | 86 | 88 | 89 | 90 | 38 | 39 | 39 | 40 | 41 | 41 | 42 |
| 90th | 97 | 97 | 98 | 100 | 101 | 102 | 103 | 52 | 53 | 53 | 54 | 55 | 55 | 56 | |
| 95th | 100 | 101 | 102 | 104 | 105 | 106 | 107 | 56 | 57 | 57 | 58 | 59 | 59 | 60 | |
| 99th | 108 | 108 | 109 | 111 | 112 | 113 | 114 | 64 | 64 | 65 | 65 | 66 | 67 | 67 | |
| 2 | 50th | 85 | 85 | 87 | 88 | 89 | 91 | 91 | 43 | 44 | 44 | 45 | 46 | 46 | 47 |
| 90th | 98 | 99 | 100 | 101 | 103 | 104 | 105 | 57 | 58 | 58 | 59 | 60 | 61 | 61 | |
| 95th | 102 | 103 | 104 | 105 | 107 | 108 | 109 | 61 | 62 | 62 | 63 | 64 | 65 | 65 | |
| 99th | 109 | 110 | 111 | 112 | 114 | 115 | 116 | 69 | 69 | 70 | 70 | 71 | 72 | 72 | |
| 3 | 50th | 86 | 87 | 88 | 89 | 91 | 92 | 93 | 47 | 48 | 48 | 49 | 50 | 50 | 51 |
| 90th | 100 | 100 | 102 | 103 | 104 | 106 | 106 | 61 | 62 | 62 | 63 | 64 | 64 | 65 | |
| 95th | 104 | 104 | 105 | 107 | 108 | 109 | 110 | 65 | 66 | 66 | 67 | 68 | 68 | 69 | |
| 99th | 111 | 111 | 113 | 114 | 115 | 116 | 117 | 73 | 73 | 74 | 74 | 75 | 76 | 76 | |
| 4 | 50th | 88 | 88 | 90 | 91 | 92 | 94 | 94 | 50 | 50 | 51 | 52 | 52 | 53 | 54 |
| 90th | 101 | 102 | 103 | 104 | 106 | 107 | 108 | 64 | 64 | 65 | 66 | 67 | 67 | 68 | |
| 95th | 105 | 106 | 107 | 108 | 110 | 111 | 112 | 68 | 68 | 69 | 70 | 71 | 71 | 72 | |
| 99th | 112 | 113 | 114 | 115 | 117 | 118 | 119 | 76 | 76 | 76 | 77 | 78 | 79 | 79 | |
| 5 | 50th | 89 | 90 | 91 | 93 | 94 | 95 | 96 | 52 | 53 | 53 | 54 | 55 | 55 | 56 |
| 90th | 103 | 103 | 105 | 106 | 107 | 109 | 109 | 66 | 67 | 67 | 68 | 69 | 69 | 70 | |
| 95th | 107 | 107 | 108 | 110 | 111 | 112 | 113 | 70 | 71 | 71 | 72 | 73 | 73 | 74 | |
| 99th | 114 | 114 | 116 | 117 | 118 | 120 | 120 | 78 | 78 | 79 | 79 | 80 | 81 | 81 | |
| Table Continued | |||||||||||||||
| Age, yr | BP Percentile† | SBP, mmHg | DBP, mmHg | ||||||||||||
| Percentile of Height∗ | Percentile of Height∗ | ||||||||||||||
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 6 | 50th | 91 | 92 | 93 | 94 | 96 | 97 | 98 | 54 | 54 | 55 | 56 | 56 | 57 | 58 |
| 90th | 104 | 105 | 106 | 108 | 109 | 110 | 111 | 68 | 68 | 69 | 70 | 70 | 71 | 72 | |
| 95th | 108 | 109 | 110 | 111 | 113 | 114 | 115 | 72 | 72 | 73 | 74 | 74 | 75 | 76 | |
| 99th | 115 | 116 | 117 | 119 | 120 | 121 | 122 | 80 | 80 | 80 | 81 | 82 | 83 | 83 | |
| 7 | 50th | 93 | 93 | 95 | 96 | 97 | 99 | 99 | 55 | 56 | 56 | 57 | 58 | 58 | 59 |
| 90th | 106 | 107 | 108 | 109 | 111 | 112 | 113 | 69 | 70 | 70 | 71 | 72 | 72 | 73 | |
| 95th | 110 | 111 | 112 | 113 | 115 | 116 | 116 | 73 | 74 | 74 | 75 | 76 | 76 | 77 | |
| 99th | 117 | 118 | 119 | 120 | 122 | 123 | 124 | 81 | 81 | 82 | 82 | 83 | 84 | 84 | |
| 8 | 50th | 95 | 95 | 96 | 98 | 99 | 100 | 101 | 57 | 57 | 57 | 58 | 59 | 60 | 60 |
| 90th | 108 | 109 | 110 | 111 | 113 | 114 | 114 | 71 | 71 | 71 | 72 | 73 | 74 | 74 | |
| 95th | 112 | 112 | 114 | 115 | 116 | 118 | 118 | 75 | 75 | 75 | 76 | 77 | 78 | 78 | |
| 99th | 119 | 120 | 121 | 122 | 123 | 125 | 125 | 82 | 82 | 83 | 83 | 84 | 85 | 86 | |
| 9 | 50th | 96 | 97 | 98 | 100 | 101 | 102 | 103 | 58 | 58 | 58 | 59 | 60 | 61 | 61 |
| 90th | 110 | 110 | 112 | 113 | 114 | 116 | 116 | 72 | 72 | 72 | 73 | 74 | 75 | 75 | |
| 95th | 114 | 114 | 115 | 117 | 118 | 119 | 120 | 76 | 76 | 76 | 77 | 78 | 79 | 79 | |
| 99th | 121 | 121 | 123 | 124 | 125 | 127 | 127 | 83 | 83 | 84 | 84 | 85 | 86 | 87 | |
| 10 | 50th | 98 | 99 | 100 | 102 | 103 | 104 | 105 | 59 | 59 | 59 | 60 | 61 | 62 | 62 |
| 90th | 112 | 112 | 114 | 115 | 116 | 118 | 118 | 73 | 73 | 73 | 74 | 75 | 76 | 76 | |
| 95th | 116 | 116 | 117 | 119 | 120 | 121 | 122 | 77 | 77 | 77 | 78 | 79 | 80 | 80 | |
| Table Continued | |||||||||||||||
| Age, yr | BP Percentile† | SBP, mmHg | DBP, mmHg | ||||||||||||
| Percentile of Height∗ | Percentile of Height∗ | ||||||||||||||
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 99th | 123 | 123 | 125 | 126 | 127 | 129 | 129 | 84 | 84 | 85 | 86 | 86 | 87 | 88 | |
| 11 | 50th | 100 | 101 | 102 | 103 | 105 | 106 | 107 | 60 | 60 | 60 | 61 | 62 | 63 | 63 |
| 90th | 114 | 114 | 116 | 117 | 118 | 119 | 120 | 74 | 74 | 74 | 75 | 76 | 77 | 77 | |
| 95th | 118 | 118 | 119 | 121 | 122 | 123 | 124 | 78 | 78 | 78 | 79 | 80 | 81 | 81 | |
| 99th | 125 | 125 | 126 | 128 | 129 | 130 | 131 | 85 | 85 | 86 | 87 | 87 | 88 | 89 | |
| 12 | 50th | 102 | 103 | 104 | 105 | 107 | 108 | 109 | 61 | 61 | 61 | 62 | b3 | 64 | 64 |
| 90th | 116 | 116 | 117 | 119 | 120 | 121 | 122 | 75 | 75 | 75 | 76 | 77 | 78 | 78 | |
| 95th | 119 | 120 | 121 | 123 | 124 | 125 | 126 | 79 | 79 | 79 | 80 | 81 | 82 | 82 | |
| 99th | 127 | 127 | 128 | 130 | 131 | 132 | 133 | 86 | 86 | 87 | 88 | 88 | 89 | 90 | |
| 13 | 50th | 104 | 105 | 106 | 107 | 109 | 110 | 110 | 62 | 62 | 62 | 63 | 64 | 65 | 65 |
| 90th | 117 | 118 | 119 | 121 | 122 | 123 | 124 | 76 | 76 | 76 | 77 | 78 | 79 | 79 | |
| 95th | 121 | 122 | 123 | 124 | 126 | 127 | 128 | 80 | 80 | 80 | 81 | 82 | 83 | 83 | |
| 99th | 128 | 129 | 130 | 132 | 133 | 134 | 135 | 87 | 87 | 88 | 89 | 89 | 90 | 91 | |
| 14 | 50th | 106 | 106 | 107 | 109 | 110 | 111 | 112 | 63 | 63 | 63 | 64 | 65 | 66 | 66 |
| 90th | 119 | 120 | 121 | 122 | 124 | 125 | 125 | 77 | 77 | 77 | 78 | 79 | 80 | 80 | |
| 95th | 123 | 123 | 125 | 126 | 127 | 129 | 129 | 81 | 81 | 81 | 82 | 83 | 84 | 84 | |
| 99th | 130 | 131 | 132 | 133 | 135 | 136 | 136 | 88 | 88 | 89 | 90 | 90 | 91 | 92 | |
| 15 | 50th | 107 | 108 | 109 | 110 | 111 | 113 | 113 | 64 | 64 | 64 | 65 | 66 | 67 | 67 |
| 90th | 120 | 121 | 122 | 123 | 125 | 126 | 127 | 78 | 78 | 78 | 79 | 80 | 81 | 81 | |
| 95th | 124 | 125 | 126 | 127 | 129 | 130 | 131 | 82 | 82 | 82 | 83 | 84 | 85 | 85 | |
| Table Continued | |||||||||||||||
| Age, yr | BP Percentile† | SBP, mmHg | DBP, mmHg | ||||||||||||
| Percentile of Height∗ | Percentile of Height∗ | ||||||||||||||
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 99th | 131 | 132 | 133 | 134 | 136 | 137 | 138 | 89 | 89 | 90 | 91 | 91 | 92 | 93 | |
| 16 | 50th | 108 | 108 | 110 | 111 | 112 | 114 | 114 | 64 | 64 | 65 | 66 | 66 | 67 | 68 |
| 90th | 121 | 122 | 123 | 124 | 126 | 127 | 128 | 78 | 78 | 79 | 80 | 81 | 81 | 82 | |
| 95th | 125 | 126 | 127 | 128 | 130 | 131 | 132 | 82 | 82 | 83 | 84 | 85 | 85 | 86 | |
| 99th | 132 | 133 | 134 | 135 | 137 | 138 | 139 | 90 | 90 | 90 | 91 | 92 | 93 | 93 | |
| 17 | 50th | 108 | 109 | 110 | 111 | 113 | 114 | 115 | 64 | 65 | 65 | 66 | 67 | 67 | 68 |
| 90th | 122 | 122 | 123 | 125 | 126 | 127 | 128 | 78 | 79 | 79 | 80 | 81 | 81 | 82 | |
| 95th | 125 | 126 | 127 | 129 | 130 | 131 | 132 | 82 | 83 | 83 | 84 | 85 | 85 | 86 | |
| 99th | 133 | 133 | 134 | 136 | 137 | 138 | 139 | 90 | 90 | 91 | 91 | 92 | 93 | 93 | |
∗ Height percentile determined by standard growth curves.
† Blood pressure percentile determined by a single measurement.
Adapted from National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2 Suppl):555-576.
TABLE 7-2
BLOOD PRESSURE LEVELS FOR THE 50TH, 90TH, 95TH, AND 99TH PERCENTILES OF BLOOD PRESSURE FOR BOYS AGE 1–17 YEARS BY PERCENTILES OF HEIGHT2
| Age, yr | BP Percentile† | SBP, mmHg | DBP, mmHg | ||||||||||||
| Percentile of Height∗ | Percentile of Height∗ | ||||||||||||||
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 1 | 50th | 80 | 81 | 83 | 85 | 87 | 88 | 89 | 34 | 35 | 36 | 37 | 38 | 39 | 39 |
| 90th | 94 | 95 | 97 | 99 | 100 | 102 | 103 | 49 | 50 | 51 | 52 | 53 | 53 | 54 | |
| 95th | 98 | 99 | 101 | 103 | 104 | 106 | 106 | 54 | 54 | 55 | 56 | 57 | 58 | 58 | |
| 99th | 105 | 106 | 108 | 110 | 112 | 113 | 114 | 61 | 62 | 63 | 64 | 65 | 66 | 66 | |
| 2 | 50th | 84 | 85 | 87 | 88 | 90 | 92 | 92 | 39 | 40 | 41 | 42 | 43 | 44 | 44 |
| 90th | 97 | 99 | 100 | 102 | 104 | 105 | 106 | 54 | 55 | 56 | 57 | 58 | 58 | 59 | |
| 95th | 101 | 102 | 104 | 106 | 108 | 109 | 110 | 59 | 59 | 60 | 61 | 62 | 63 | 63 | |
| 99th | 109 | 110 | 111 | 113 | 115 | 117 | 117 | 66 | 67 | 68 | 69 | 70 | 71 | 71 | |
| 3 | 50th | 86 | 87 | 89 | 91 | 93 | 94 | 95 | 44 | 44 | 45 | 46 | 47 | 48 | 48 |
| 90th | 100 | 101 | 103 | 105 | 107 | 108 | 109 | 59 | 59 | 60 | 61 | 62 | 63 | 63 | |
| 95th | 104 | 105 | 107 | 109 | 110 | 112 | 113 | 63 | 63 | 64 | 65 | 66 | 67 | 67 | |
| 99th | 111 | 112 | 114 | 116 | 118 | 119 | 120 | 71 | 71 | 72 | 73 | 74 | 75 | 75 | |
| 4 | 50th | 88 | 89 | 91 | 93 | 95 | 96 | 97 | 47 | 48 | 49 | 50 | 51 | 51 | 52 |
| 90th | 102 | 103 | 105 | 107 | 109 | 110 | 111 | 62 | 63 | 64 | 65 | 66 | 66 | 67 | |
| 95th | 106 | 107 | 109 | 111 | 112 | 114 | 115 | 66 | 67 | 68 | 69 | 70 | 71 | 71 | |
| 99th | 113 | 114 | 116 | 118 | 120 | 121 | 122 | 74 | 75 | 76 | 77 | 78 | 78 | 79 | |
| 5 | 50th | 90 | 91 | 93 | 95 | 96 | 98 | 98 | 50 | 51 | 52 | 53 | 54 | 55 | 55 |
| 90th | 104 | 105 | 106 | 108 | 110 | 111 | 112 | 65 | 66 | 67 | 68 | 69 | 69 | 70 | |
| 95th | 108 | 109 | 110 | 112 | 114 | 115 | 116 | 69 | 70 | 71 | 72 | 73 | 74 | 74 | |
| 99th | 115 | 116 | 118 | 120 | 121 | 123 | 123 | 77 | 78 | 79 | 80 | 81 | 81 | 82 | |
| 6 | 50th | 91 | 92 | 94 | 96 | 98 | 99 | 100 | 53 | 53 | 54 | 55 | 56 | 57 | 57 |
| 90th | 105 | 166 | 108 | 110 | 111 | 113 | 113 | 68 | 68 | 69 | 70 | 71 | 72 | 72 | |
| 95th | 109 | 110 | 112 | 114 | 115 | 117 | 117 | 72 | 72 | 73 | 74 | 75 | 76 | 76 | |
| 99th | 116 | 117 | 119 | 121 | 123 | 124 | 125 | 80 | 80 | 81 | 82 | 83 | 84 | 84 | |
| Table Continued | |||||||||||||||
| Age, yr | BP Percentile† | SBP, mmHg | DBP, mmHg | ||||||||||||
| Percentile of Height∗ | Percentile of Height∗ | ||||||||||||||
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 7 | 50th | 92 | 94 | 95 | 97 | 99 | 100 | 101 | 55 | 55 | 56 | 57 | 58 | 59 | 59 |
| 90th | 106 | 107 | 109 | 111 | 113 | 114 | 115 | 70 | 70 | 71 | 72 | 73 | 74 | 74 | |
| 95th | 110 | 111 | 113 | 115 | 117 | 118 | 119 | 74 | 74 | 75 | 76 | 77 | 78 | 78 | |
| 99th | 117 | 118 | 120 | 122 | 124 | 125 | 126 | 82 | 82 | 83 | 84 | 85 | 86 | 86 | |
| 8 | 50th | 94 | 95 | 97 | 99 | 100 | 102 | 102 | 56 | 57 | 58 | 59 | 60 | 60 | 61 |
| 90th | 107 | 109 | 110 | 112 | 114 | 115 | 116 | 71 | 72 | 72 | 73 | 74 | 75 | 76 | |
| 95th | 111 | 112 | 114 | 116 | 118 | 119 | 120 | 75 | 76 | 77 | 78 | 79 | 79 | 80 | |
| 99th | 119 | 120 | 122 | 123 | 125 | 127 | 127 | 83 | 84 | 85 | 86 | 87 | 87 | 88 | |
| 9 | 50th | 95 | 96 | 98 | 100 | 102 | 103 | 104 | 57 | 58 | 59 | 60 | 61 | 61 | 62 |
| 90th | 109 | 110 | 112 | 114 | 115 | 117 | 118 | 72 | 73 | 74 | 75 | 76 | 76 | 77 | |
| 95th | 113 | 114 | 116 | 118 | 119 | 121 | 121 | 76 | 77 | 78 | 79 | 80 | 81 | 81 | |
| 99th | 120 | 121 | 123 | 125 | 127 | 128 | 129 | 84 | 85 | 86 | 87 | 88 | 88 | 89 | |
| 10 | 50th | 97 | 98 | 100 | 102 | 103 | 105 | 106 | 58 | 59 | 60 | 61 | 61 | 62 | 63 |
| 90th | 111 | 112 | 114 | 115 | 117 | 119 | 119 | 73 | 73 | 74 | 75 | 76 | 77 | 78 | |
| 95th | 115 | 116 | 117 | 119 | 121 | 122 | 123 | 77 | 78 | 79 | 80 | 81 | 81 | 82 | |
| 99th | 122 | 123 | 125 | 127 | 128 | 130 | 130 | 85 | 86 | 86 | 88 | 88 | 89 | 90 | |
| 11 | 50th | 99 | 100 | 102 | 104 | 105 | 107 | 107 | 59 | 59 | 60 | 61 | 62 | 63 | 63 |
| 90th | 113 | 114 | 115 | 117 | 119 | 120 | 121 | 74 | 74 | 75 | 76 | 77 | 78 | 78 | |
| 95th | 117 | 118 | 119 | 121 | 123 | 124 | 125 | 78 | 78 | 79 | 80 | 81 | 82 | 82 | |
| 99th | 124 | 125 | 127 | 129 | 130 | 132 | 132 | 86 | 86 | 87 | 88 | 89 | 90 | 90 | |
| 12 | 50th | 101 | 102 | 104 | 106 | 108 | 109 | 110 | 59 | 60 | 61 | 62 | 63 | 63 | 64 |
| 90th | 115 | 116 | 118 | 120 | 121 | 123 | 123 | 74 | 75 | 75 | 76 | 77 | 78 | 79 | |
| 95th | 119 | 120 | 122 | 123 | 125 | 127 | 127 | 78 | 79 | 80 | 81 | 82 | 82 | 83 | |
| 99th | 126 | 127 | 129 | 131 | 133 | 134 | 135 | 86 | 87 | 88 | 89 | 90 | 90 | 91 | |
| Table Continued | |||||||||||||||
| Age, yr | BP Percentile† | SBP, mmHg | DBP, mmHg | ||||||||||||
| Percentile of Height∗ | Percentile of Height∗ | ||||||||||||||
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 13 | 50th | 104 | 105 | 106 | 108 | 110 | 111 | 112 | 60 | 60 | 61 | 62 | 63 | 64 | 64 |
| 90th | 117 | 118 | 120 | 122 | 124 | 125 | 126 | 75 | 75 | 76 | 77 | 78 | 79 | 79 | |
| 95th | 121 | 122 | 124 | 126 | 128 | 129 | 130 | 79 | 79 | 80 | 81 | 82 | 83 | 83 | |
| 99th | 128 | 130 | 131 | 133 | 135 | 136 | 137 | 87 | 87 | 88 | 89 | 90 | 91 | 91 | |
| 14 | 50th | 106 | 107 | 109 | 111 | 113 | 114 | 115 | 60 | 61 | 62 | 63 | 64 | 65 | 65 |
| 90th | 120 | 121 | 123 | 125 | 126 | 128 | 128 | 75 | 76 | 77 | 78 | 79 | 79 | 80 | |
| 95th | 124 | 125 | 127 | 128 | 130 | 132 | 132 | 80 | 80 | 81 | 82 | 83 | 84 | 84 | |
| 99th | 131 | 132 | 134 | 136 | 138 | 139 | 140 | 87 | 88 | 89 | 90 | 91 | 92 | 92 | |
| 15 | 50th | 109 | 110 | 112 | 113 | 115 | 117 | 117 | 61 | 62 | 63 | 64 | 65 | 66 | 66 |
| 90th | 122 | 124 | 125 | 127 | 129 | 130 | 131 | 76 | 77 | 78 | 79 | 80 | 80 | 81 | |
| 95th | 126 | 127 | 129 | 131 | 133 | 134 | 135 | 81 | 81 | 82 | 83 | 84 | 85 | 85 | |
| 99th | 134 | 135 | 136 | 138 | 140 | 142 | 142 | 88 | 89 | 90 | 91 | 92 | 93 | 93 | |
| 16 | 50th | 111 | 112 | 114 | 116 | 118 | 119 | 120 | 63 | 63 | 64 | 65 | 66 | 67 | 67 |
| 90th | 125 | 126 | 128 | 130 | 131 | 133 | 134 | 78 | 78 | 79 | 80 | 81 | 82 | 82 | |
| 95th | 129 | 130 | 132 | 134 | 135 | 137 | 137 | 82 | 83 | 83 | 84 | 85 | 86 | 87 | |
| 99th | 136 | 137 | 139 | 141 | 143 | 144 | 145 | 90 | 90 | 91 | 92 | 93 | 94 | 94 | |
| 17 | 50th | 114 | 115 | 116 | 118 | 120 | 121 | 122 | 65 | 66 | 66 | 67 | 68 | 69 | 70 |
| 90th | 127 | 128 | 130 | 132 | 134 | 135 | 136 | 80 | 80 | 81 | 82 | 83 | 84 | 84 | |
| 95th | 131 | 232 | 134 | 136 | 138 | 139 | 140 | 84 | 85 | 86 | 87 | 87 | 88 | 89 | |
| 99th | 139 | 140 | 141 | 143 | 145 | 146 | 147 | 92 | 93 | 93 | 94 | 95 | 96 | 97 | |
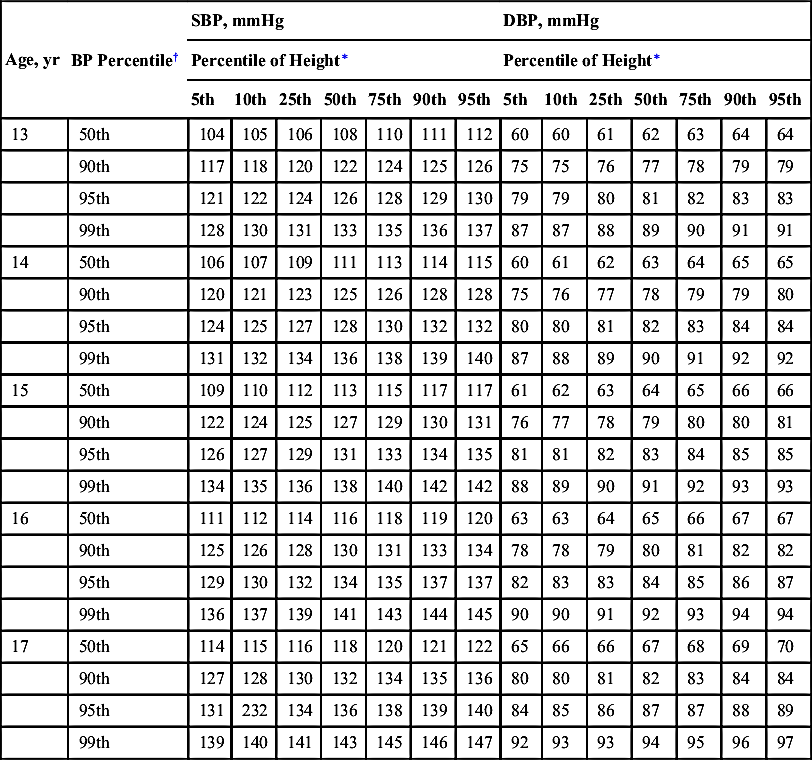
∗ Height percentile determined by standard growth curves.
† Blood pressure percentile determined by a single measurement.
Adapted from National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents: The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004;114(2 Suppl):555–576.
1. Grading of heart murmurs: Intensified by states of higher cardiac output (e.g., anemia, anxiety, fever, exercise)3
2. Benign heart murmurs:
a. Caused by a disturbance of the laminar flow of blood; frequently produced as the diameter of the blood's pathway decreases and velocity increases.
b. Present in > 80% of children sometime during childhood, most commonly beginning at age 3 to 4 years.
c. Accentuated in high-output states, especially with fever and anemia.
d. Normal electrocardiogram (ECG) and radiographic findings.
NOTE: ECG and chest radiograph are not routinely useful or cost-effective screening tools for distinguishing benign from pathologic murmurs.
3. Likely pathologic murmur when one or more of the following are present: Symptoms; cyanosis; systolic murmur that is loud (grade ≥3/6), harsh, pansystolic, or long in duration; diastolic murmur; abnormal heart sounds; presence of a click; abnormally strong or weak pulses.
4. Systolic and diastolic heart murmurs (Box 7-2)
TABLE 7-3
| Type (Timing) | Description of Murmur | Age Group |
| Classic vibratory murmur (Still's murmur; systolic) | Maximal at LMSB or between LLSB and apex Grade 2–3/6 in intensity Low-frequency vibratory, twanging string, groaning, squeaking, or musical | 3–6 yr; occasionally in infancy |
| Pulmonary ejection murmur (systolic) | Maximal at LUSB Early to midsystolic Grade 1–3/6 in intensity Blowing in quality | 8–14 yr |
| Pulmonary flow murmur of newborn (systolic) | Maximal at LUSB Transmits well to left and right chest, axilla, and back Grade 1–2/6 in intensity | Premature and full-term newborns Usually disappears by 3–6 mo |
| Venous hum (continuous) | Maximal at right (or left) supraclavicular and infraclavicular areas Grade 1–3/6 in intensity Inaudible in supine position Intensity changes with rotation of head and disappears with compression of jugular vein. | 3–6 yr |
| Carotid bruit (systolic) | Right supraclavicular area over carotids Grade 2–3/6 in intensity Occasional thrill over carotid | Any age |
LLSB, Left lower sternal border; LMSB, left middle sternal border; LUSB, left upper sternal border.
From Park MK. Pediatric Cardiology for Practitioners. 5th ed. St Louis: Mosby; 2008:36.
IV. Electrocardiography
A. Basic Electrocardiography Principles
1. Lead placement (Fig. 7-5)
2. ECG complexes (see Fig. 7-1)
a. P wave: Represents atrial depolarization
b. QRS complex: Represents ventricular depolarization
c. T wave: Represents ventricular repolarization
d. U wave: May follow T wave, representing late phases of ventricular repolarization
a. Rate
(1) Standardization: Paper speed is 25 mm/sec. One small square = 1 mm = 0.04 sec. One large square = 5 mm = 0.2 sec. Amplitude standard: 10 mm = 1 mV
(2) Calculation: HR (beats per minute) = 60 divided by the average R-R interval in seconds, or 1500 divided by the R-R interval in millimeters
b. Rhythm

d. Intervals (PR, QRS, QTc): See Table 7-4 for normal PR and QRS intervals. The QTc is calculated using the Bazett formula:

(average 3 measurements taken from same lead)
R-R interval should extend from the R wave in the QRS complex where you are measuring QT to the preceding R wave. Normal values for QTc are:
(1) 0.44 sec is 97th percentile for infants 3–4 days old6
(2) ≤0.45 sec in all males >1 week of age and prepubescent females
(3) ≤0.46 sec for postpubescent females
e. P-wave size and shape: Normal P wave should be <0.10 sec in children, <0.08 sec in infants, with amplitude <0.3 mV (3 mm in height, with normal standardization)
f. R-wave progression: Generally a normal increase in R-wave size and decrease in S-wave size from leads V1 to V6 (with dominant S waves in right precordial leads and dominant R waves in left precordial leads), representing dominance of left ventricular forces. However, newborns and infants have a normal dominance of the right ventricle.
TABLE 7-4
NORMAL PEDIATRIC ELECTROCARDIOGRAM (ECG) PARAMETERS
| Age | Heart Rate (bpm) | QRS Axis∗ | PR Interval (sec)∗ | QRS Duration (sec)† | Lead V1 | Lead V6 | ||||
| R-Wave Amplitude (mm)† | S-Wave Amplitude (mm)† | R/S Ratio | R-Wave Amplitude (mm)† | S-Wave Amplitude (mm)† | R/S Ratio | |||||
| 0–7 days | 95–160 (125) | +30 to 180 (110) | 0.08–0.12 (0.10) | 0.05 (0.07) | 13.3 (25.5) | 7.7 (18.8) | 2.5 | 4.8 (11.8) | 3.2 (9.6) | 2.2 |
| 1–3 wk | 105–180 (145) | +30 to 180 (110) | 0.08–0.12 (0.10) | 0.05 (0.07) | 10.6 (20.8) | 4.2 (10.8) | 2.9 | 7.6 (16.4) | 3.4 (9.8) | 3.3 |
| 1–6 mo | 110–180 (145) | +10 to +125 (+70) | 0.08–0.13 (0.11) | 0.05 (0.07) | 9.7 (19) | 5.4 (15) | 2.3 | 12.4 (22) | 2.8 (8.3) | 5.6 |
| 6–12 mo | 110–170 (135) | +10 to +125 (+60) | 0.10–0.14 (0.12) | 0.05 (0.07) | 9.4 (20.3) | 6.4 (18.1) | 1.6 | 12.6 (22.7) | 2.1 (7.2) | 7.6 |
| 1–3 yr | 90–150 (120) | +10 to +125 (+60) | 0.10–0.14 (0.12) | 0.06 (0.07) | 8.5 (18) | 9 (21) | 1.2 | 14 (23.3) | 1.7 (6) | 10 |
| 4–5 yr | 65–135 (110) | 0 to +110 (+60) | 0.11–0.15 (0.13) | 0.07 (0.08) | 7.6 (16) | 11 (22.5) | 0.8 | 15.6 (25) | 1.4 (4.7) | 11.2 |
| 6–8 yr | 60–130 (100) | −15 to +110 (+60) | 0.12–0.16 (0.14) | 0.07 (0.08) | 6 (13) | 12 (24.5) | 0.6 | 16.3 (26) | 1.1 (3.9) | 13 |
| 9–11 yr | 60–110 (85) | −15 to +110 (+60) | 0.12–0.17 (0.14) | 0.07 (0.09) | 5.4 (12.1) | 11.9 (25.4) | 0.5 | 16.3 (25.4) | 1.0 (3.9) | 14.3 |
| 12–16 yr | 60–110 (85) | −15 to +110 (+60) | 0.12–0.17 (0.15) | 0.07 (0.10) | 4.1 (9.9) | 10.8 (21.2) | 0.5 | 14.3 (23) | 0.8 (3.7) | 14.7 |
| >16 yr | 60–100 (80) | −15 to +110 (+60) | 0.12–0.20 (0.15) | 0.08 (0.10) | 3 (9) | 10 (20) | 0.3 | 10 (20) | 0.8 (3.7) | 12 |
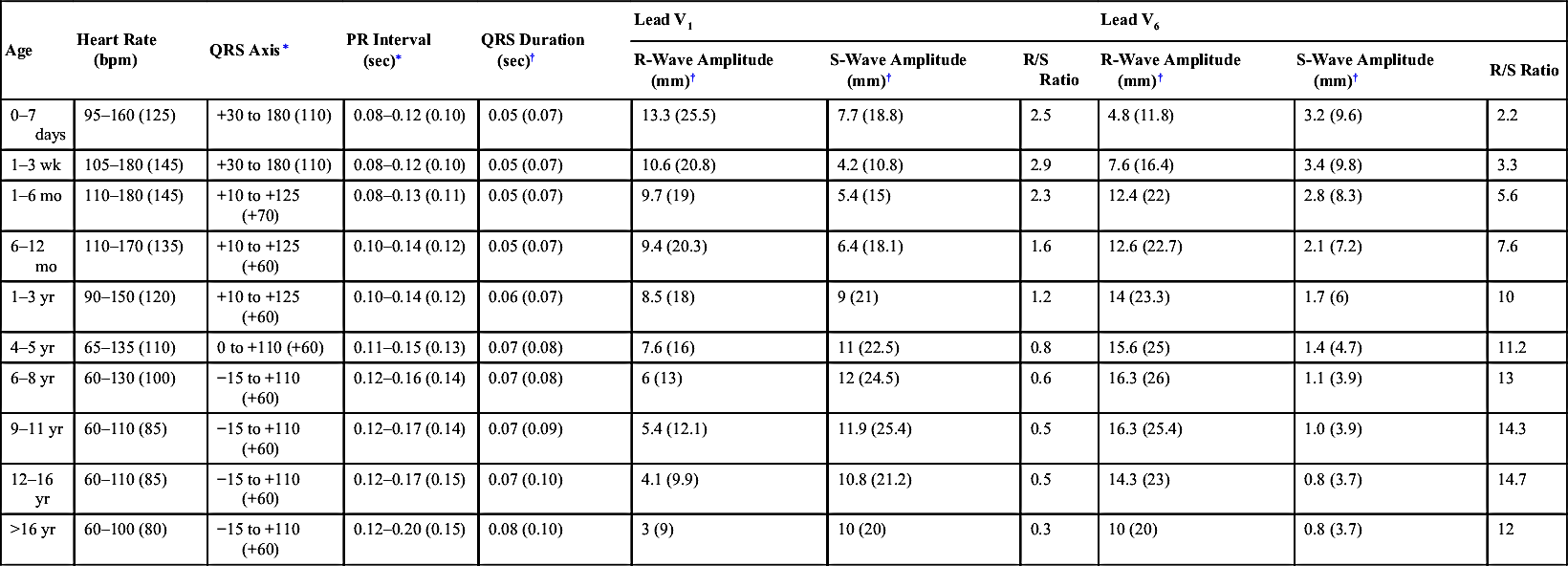
∗ Normal range and (mean).
† Mean and (98th percentile).
Adapted from Park MK. Pediatric Cardiology for Practitioners. 5th ed. St Louis: Mosby; 2008; and Davignon A et al. Normal ECG standards for infants and children. Pediatr Cardiol. 1979;1:123-131.

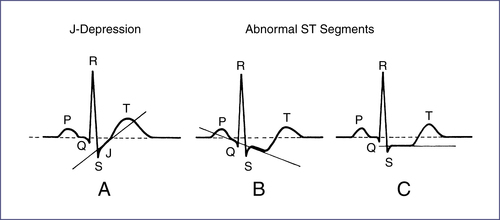
h. ST-segment (Fig. 7-7): ST-segment elevation or depression >1 mm in limb leads and >2 mm in precordial leads is consistent with myocardial ischemia or injury. Note: J-depression is an upsloping of the ST segment and a normal variant.
i. T wave:
(1) Inverted T waves in V1 and V2 can be normal in children up to adolescence (Table 7-5).
(2) Tall, peaked T waves may be seen in hyperkalemia.
B. ECG Abnormalities
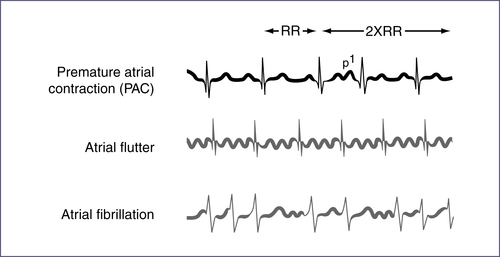
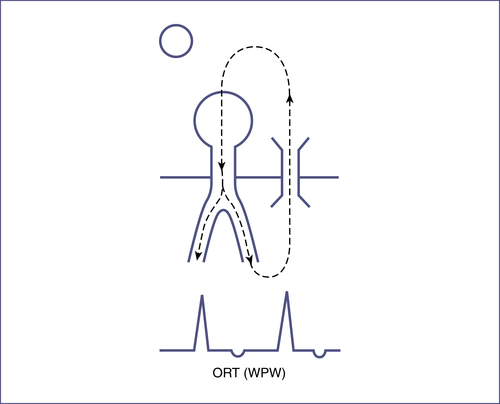
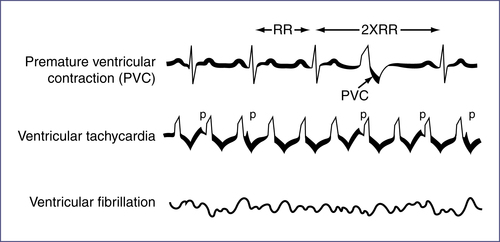
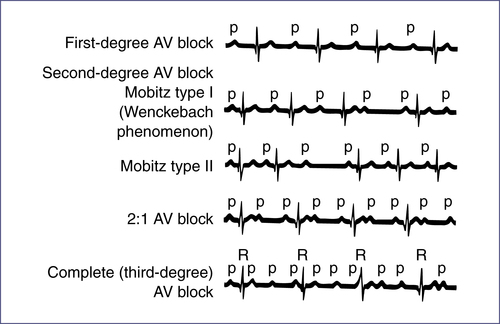
TABLE 7-6
| Name/Description | Cause | Treatment |
| SINUS | ||
| TACHYCARDIA | ||
| Normal sinus rhythm with HR >95th percentile for age (usually infants: <220 beats/min and children: <180 beats/min) | Hypovolemia, shock, anemia, sepsis, fever, anxiety, CHF, PE, myocardial disease, drugs (e.g., β-agonists, albuterol, caffeine, atropine) | Address underlying cause |
| BRADYCARDIA | ||
| Normal sinus rhythm with HR <5th percentile for age | Normal (especially in athletic individuals), increased ICP, hypoxia, hyperkalemia, hypercalcemia, vagal stimulation, hypothyroidism, hypothermia, drugs (e.g., opioids, digoxin, β-blockers), long QT | Address underlying cause; if symptomatic, refer to inside back cover for bradycardia algorithm |
| SUPRAVENTRICULAR∗ | ||
| PREMATURE ATRIAL CONTRACTION (PAC) | ||
| Narrow QRS complex; ectopic focus in atria with abnormal P-wave morphology | Digitalis toxicity, medications (e.g., caffeine, theophylline, sympathomimetics), normal variant | Treat digitalis toxicity; otherwise no treatment needed |
| ATRIAL FLUTTER | ||
| Atrial rate 250–350 beats/min; characteristic sawtooth or flutter pattern with variable ventricular response rate and normal QRS complex | Dilated atria, previous intra-atrial surgery, valvular or ischemic heart disease, idiopathic in newborns | Synchronized cardioversion or overdrive pacing; treat underlying cause |
| Table Continued | ||

| Name/Description | Cause | Treatment |
| ATRIAL FIBRILLATION | ||
| Irregular; atrial rate 350–600 beats/min, yielding characteristic fibrillatory pattern (no discrete P waves) and irregular ventricular response rate of about 110–150 beats/min with normal QRS complex | Wolff-Parkinson-White syndrome and those listed previously for atrial flutter (except not idiopathic), alcohol exposure, familial | Synchronized cardioversion; then may need anticoagulation pretreatment |
| SVT | ||
| Sudden run of three or more consecutive premature supraventricular beats at >220 beats/min(infant) or >180 beats/min (child), with narrow QRS complex and absent/abnormal P wave; either sustained (>30 sec) or nonsustained | Most commonly idiopathic but may be seen in congenital heart disease (e.g., Ebstein anomaly, transposition) | Vagal maneuvers, adenosine; if unstable, need immediate synchronized cardioversion (0.5 J/kg up to 1 J/kg). Consult cardiologist. See “Tachycardia with Poor Perfusion” or “Tachycardia with Adequate Perfusion” algorithms in back of handbook. |
| I. AV Reentrant: Presence of accessory bypass pathway, in conjunction with AV node, establishes cyclic pattern of reentry independent of SA node; most common cause of nonsinus tachycardia in children (see Wolff-Parkinson-White syndrome, Table 7-9 and Fig. 7-10) | ||
| II. Junctional: Automatic focus; simultaneous depolarization of atria and ventricles yields invisible P wave or retrograde P wave | Cardiac surgery, idiopathic | Adjust for clinical situation; consult cardiology |
| III. Ectopic atrial tachycardia: Rapid firing of ectopic focus in atrium | Idiopathic | AV nodal blockade, ablation |
| NODAL ESCAPE/JUNCTIONAL RHYTHM | ||
| Abnormal rhythm driven by AV node impulse, giving normal QRS complex and invisible P wave (buried in preceding QRS or T wave) or retrograde P wave (negative in lead II, positive in aVR); seen in sinus bradycardia | Common after surgery of atria | Often requires no treatment. If rate is slow enough, may require pacemaker. |

AV, Atrioventricular; CHF, congestive heart failure; HR, heart rate; ICP, intracranial pressure; PE, pulmonary embolism; SA, sinoatrial; SVT, supraventricular tachycardia.
∗ Abnormal rhythm resulting from ectopic focus in atria or AV node, or from accessory conduction pathways. Characterized by different P-wave shape and abnormal P-wave axis. QRS morphology usually normal. See Figures 7-9, 7-10.6
TABLE 7-7
| Name/Description | Cause | Treatment |
| PREMATURE VENTRICULAR CONTRACTION (PVC) | ||
| Ectopic ventricular focus causing early depolarization. Abnormally wide QRS complex appears prematurely, usually with full compensatory pause. May be unifocal or multifocal. Bigeminy: Alternating normal and abnormal QRS complexes. Trigeminy: Two normal QRS complexes followed by an abnormal one. Couplet: Two consecutive PVCs. | Myocarditis, myocardial injury, cardiomyopathy, long QT, congenital and acquired heart disease, drugs (catecholamines, theophylline, caffeine, anesthetics), MVP, anxiety, hypokalemia, hypoxia, hypomagnesemia. Can be normal variant. | None. More worrisome if associated with underlying heart disease or syncope, if worse with activity, or if they are multiform (especially couplets). Address underlying cause, rule out structural heart disease. |
| VENTRICULAR TACHYCARDIA | ||
| Series of three or more PVCs at rapid rate (120–250 beats/min), with wide QRS complex and dissociated, retrograde, or no P wave | See causes of PVCs (70% have underlying cause). | See “Tachycardia with Poor Perfusion” and “Tachycardia with Adequate Perfusion” algorithms in back of handbook. |
| VENTRICULAR FIBRILLATION | ||
| Depolarization of ventricles in uncoordinated asynchronous pattern, yielding abnormal QRS complexes of varying size and morphology with irregular, rapid rate. Rare in children. | Myocarditis, MI, postoperative state, digitalis or quinidine toxicity, catecholamines, severe hypoxia, electrolyte disturbances, long QT | Requires immediate defibrillation. See algorithm for “Asystole and Pulseless Arrest” at back of book. |
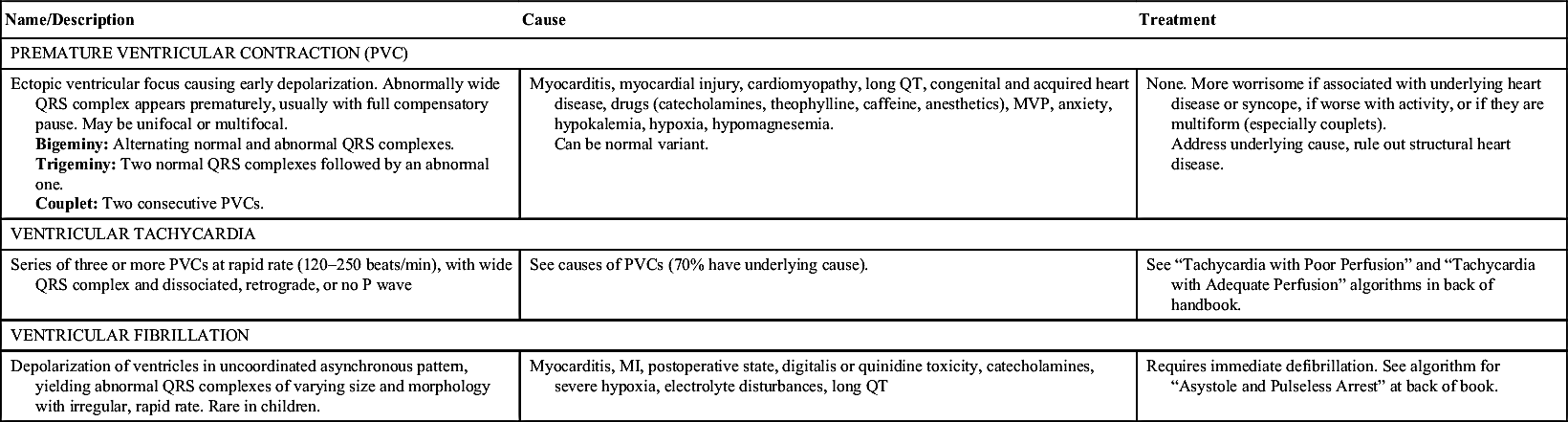
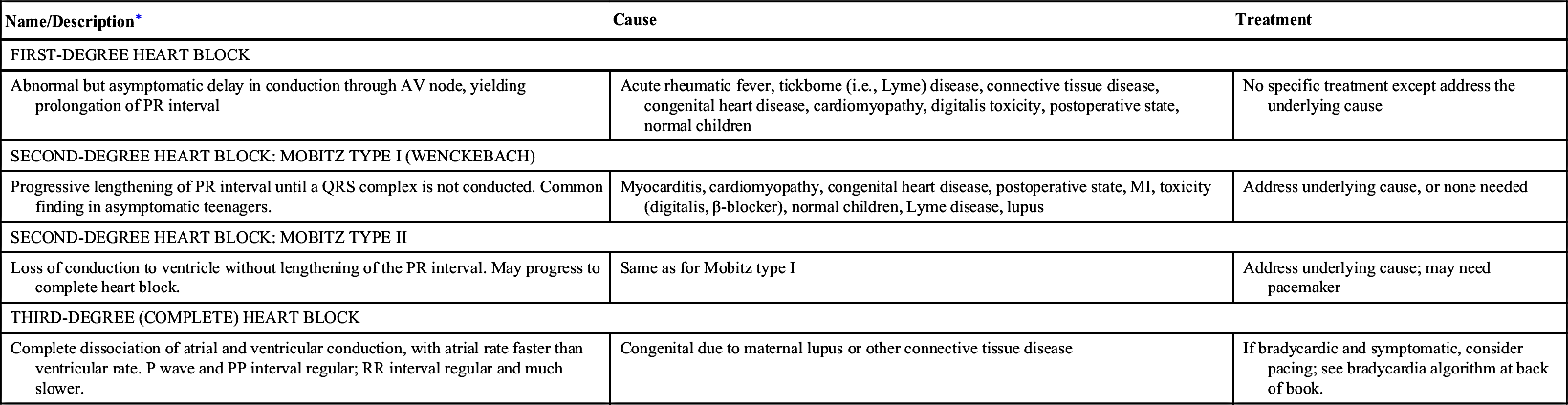
TABLE 7-8
NONVENTRICULAR CONDUCTION DISTURBANCES
| Name/Description∗ | Cause | Treatment |
| FIRST-DEGREE HEART BLOCK | ||
| Abnormal but asymptomatic delay in conduction through AV node, yielding prolongation of PR interval | Acute rheumatic fever, tickborne (i.e., Lyme) disease, connective tissue disease, congenital heart disease, cardiomyopathy, digitalis toxicity, postoperative state, normal children | No specific treatment except address the underlying cause |
| SECOND-DEGREE HEART BLOCK: MOBITZ TYPE I (WENCKEBACH) | ||
| Progressive lengthening of PR interval until a QRS complex is not conducted. Common finding in asymptomatic teenagers. | Myocarditis, cardiomyopathy, congenital heart disease, postoperative state, MI, toxicity (digitalis, β-blocker), normal children, Lyme disease, lupus | Address underlying cause, or none needed |
| SECOND-DEGREE HEART BLOCK: MOBITZ TYPE II | ||
| Loss of conduction to ventricle without lengthening of the PR interval. May progress to complete heart block. | Same as for Mobitz type I | Address underlying cause; may need pacemaker |
| THIRD-DEGREE (COMPLETE) HEART BLOCK | ||
| Complete dissociation of atrial and ventricular conduction, with atrial rate faster than ventricular rate. P wave and PP interval regular; RR interval regular and much slower. | Congenital due to maternal lupus or other connective tissue disease | If bradycardic and symptomatic, consider pacing; see bradycardia algorithm at back of book. |
AV, Atrioventricular; MI, myocardial infarction.
∗ High-degree AV block: Conduction of atrial impulse at regular intervals, yielding 2:1 block (two atrial impulses for each ventricular response), 3:1 block, etc.
TABLE 7-9
VENTRICULAR CONDUCTION DISTURBANCES
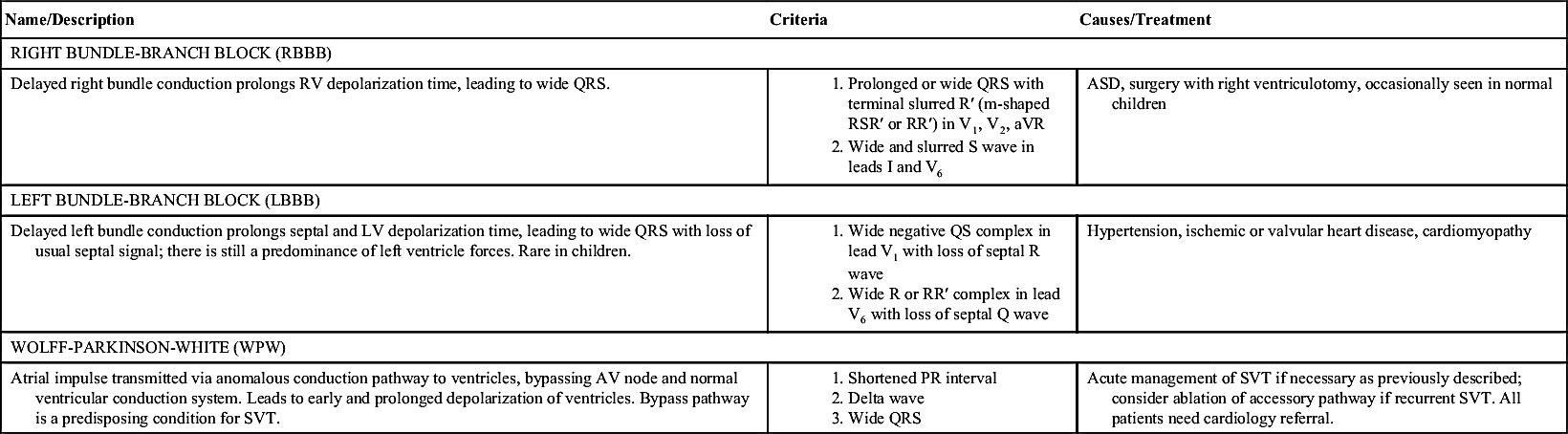
ASD, Atrial septal defect; LV, left ventricle; RV, right ventricle; SVT, supraventricular tachycardia.
C. ECG Findings Secondary to Electrolyte Disturbances, Medications, and Systemic Illnesses (Table 7-10)7,20
D. Long QT
1. Diagnosis:
a. In general, QTc is similar in males and females from birth until late adolescence (0.37–0.44 sec).
b. In adults, prolonged QTc is > 0.45 sec for males and > 0.45–0.46 sec for females.
c. In approximately 10% of cases, patients may have a normal QTc on ECG. Patients may also have a family history of long QT with unexplained syncope, seizure, or cardiac arrest without prolongation of QTc on ECG.
d. Treadmill exercise test may prolong the QTc and will sometimes incite arrythmias.
2. Complications: Associated with ventricular arrhythmias (torsades de pointes), syncope, and sudden death
3. Management:
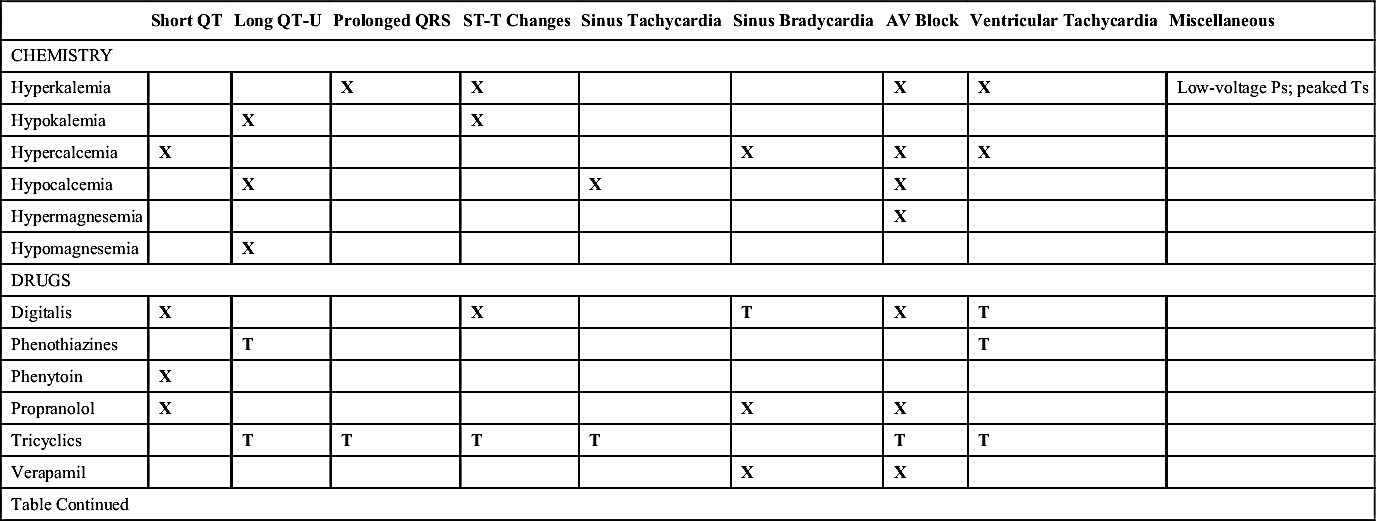
TABLE 7-10
SYSTEMIC EFFECTS ON ELECTROCARDIOGRAM
| Short QT | Long QT-U | Prolonged QRS | ST-T Changes | Sinus Tachycardia | Sinus Bradycardia | AV Block | Ventricular Tachycardia | Miscellaneous | |
| CHEMISTRY | |||||||||
| Hyperkalemia | X | X | X | X | Low-voltage Ps; peaked Ts | ||||
| Hypokalemia | X | X | |||||||
| Hypercalcemia | X | X | X | X | |||||
| Hypocalcemia | X | X | X | ||||||
| Hypermagnesemia | X | ||||||||
| Hypomagnesemia | X | ||||||||
| DRUGS | |||||||||
| Digitalis | X | X | T | X | T | ||||
| Phenothiazines | T | T | |||||||
| Phenytoin | X | ||||||||
| Propranolol | X | X | X | ||||||
| Tricyclics | T | T | T | T | T | T | |||
| Verapamil | X | X | |||||||
| Table Continued | |||||||||
| Short QT | Long QT-U | Prolonged QRS | ST-T Changes | Sinus Tachycardia | Sinus Bradycardia | AV Block | Ventricular Tachycardia | Miscellaneous | |
| MISCELLANEOUS | |||||||||
| CNS injury | X | X | X | X | X | ||||
| Friedreich ataxia | X | X | Atrial flutter | ||||||
| Duchenne muscular dystrophy | X | X | Atrial flutter | ||||||
| Myotonic dystrophy | X | X | X | X | |||||
| Collagen vascular disease | X | X | X | ||||||
| Hypothyroidism | X | Low voltage | |||||||
| Hyperthyroidism | X | X | X | X | |||||
| Lyme disease | X | X | |||||||
| Holt-Oram, maternal lupus | X | ||||||||
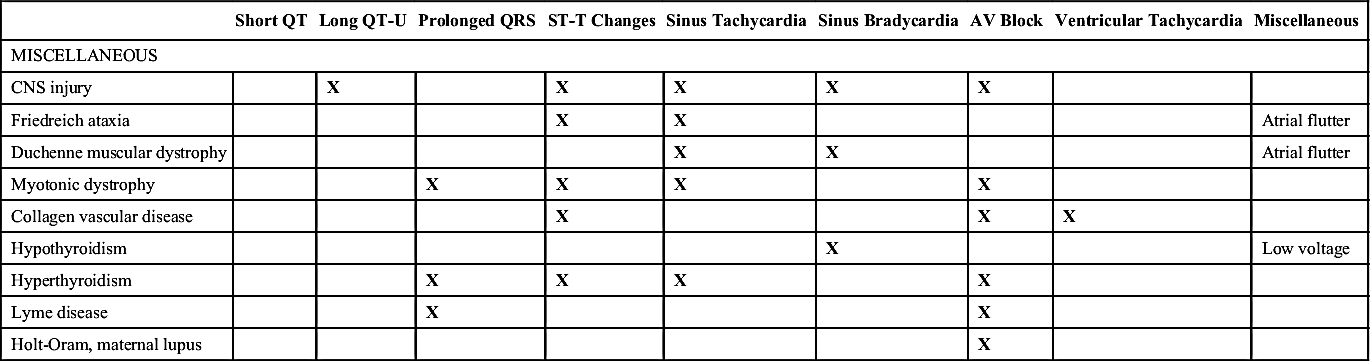
CNS, Central nervous system; T, present only with drug toxicity; X, present.
Adapted from Garson A Jr. The Electrocardiogram in Infants and Children: A Systematic Approach. Philadelphia: Lea & Febiger; 1983:172; and Walsh EP. Cardiac arrhythmias. In: Fyler DC, Nadas A,eds. Pediatric Cardiology. Philadelphia: Hanley & Belfus; 1992:141-143.
b. Acquired long QT: Treatment of arrhythmias, discontinue precipitating drug, correction of metabolic abnormalities
E. Hyperkalemia: ECG changes dependent on serum K+level; may have normal ECG with level between 2.5 and 6
1. Serum K+ <2.5: Depressed ST segment, diphasic T wave
2. Serum K+ >6: Tall T wave
3. Serum K+ >7.5: Long PR interval, wide QRS, tall T wave
4. Serum K+ >9: Absent P wave, sinusoidal
F. Myocardial Infarction (MI) in Children
1. Etiology: Anomalous origin or aberrant course of a coronary artery, Kawasaki disease, congenital heart disease (presurgical and postsurgical), and dilated cardiomyopathy. Less often associated with hypertension, lupus, myocarditis, cocaine ingestion, and use of adrenergic drugs (e.g., β-agonists used for asthma). Rare in children.
a. New-onset wide Q waves (>0.035 sec) seen within first few hours (persist over several years)
b. ST-segment elevation (>2 mm) seen within first few hours
c. Diphasic T waves seen within first few days (becoming sharply inverted, then normalizing over time)
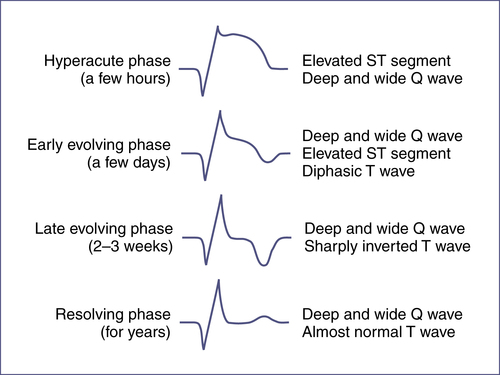
e. Deep, wide Q waves in leads I, aVL, or V6, without Q waves in II, III, aVF, suggest anomalous origin of the left coronary artery.
3. Other criteria:
a. Elevated creatine kinase (CK)/MB fraction: Not specific for acute MI in children
b. Cardiac troponin I: More sensitive indicator of early myocardial damage in children.10 Becomes elevated within hours of cardiac injury, persists for 4–7 days, is specific for cardiac injury.
V. Imaging
A. Chest Radiograph
Please see Chapter 25 for more information on the chest radiograph.
1. Evaluate the heart:
a. Size: Cardiac shadow should be <50% of thoracic width (maximal width between inner margins of ribs, as measured on a posteroanterior radiograph during inspiration)
b. Shape: Can aid in diagnosis of chamber/vessel enlargement and some congenital heart disease (Fig. 7-14)
c. Situs (levocardia, mesocardia, dextrocardia)
2. Evaluate the lung fields:
a. Decreased pulmonary blood flow: Seen in pulmonary or tricuspid stenosis/atresia, TOF, pulmonary hypertension (peripheral pruning)
b. Increased pulmonary blood flow: Seen as increased pulmonary vascular markings (PVMs) with redistribution from bases to apices of lungs and extension to lateral lung fields (see Tables 7-12 and 7-13)
c. Venous congestion, or congestive heart failure (CHF): Increased PVMs centrally, interstitial and alveolar pulmonary edema (air bronchograms), septal lines, and pleural effusions (see Tables 7-12 and 7-13)
3. Evaluate the trachea: Usually bends slightly to the right above the carina in normal patients with a left-sided aortic arch. A perfectly straight or left-bending trachea suggests a right aortic arch, which may be associated with other defects (TOF, truncus arteriosus, vascular rings, chromosome 22 microdeletion).
4. Skeletal anomalies:
a. Rib notching (e.g., from collateral vessels in patients >5 years of age with coarctation of the aorta)
b. Sternal abnormalities (e.g., Holt-Oram syndrome, pectus excavatum in Marfan, Ehlers-Danlos, and Noonan syndromes)
c. Vertebral anomalies (e.g., VATER/VACTERL syndrome: Vertebral anomalies, Anal atresia, Tracheoesophageal fistula, Radial and Renal, Cardiac, and Limb anomalies)
B. Echocardiography
1. Approach:
a. Transthoracic echocardiography (TTE): Does not require general anesthesia, is simpler to perform than transesophageal echocardiography (TEE), but does have limitations in some patients (e.g., uncooperative, obese, or those with suspected endocarditis)
b. TEE: Uses an ultrasound transducer on the end of a modified endoscope to view the heart from the esophagus and stomach, allowing for better imaging of intracardiac structures. TEE allows for better imaging in obese and intraoperative patients and is also useful for visualizing very small lesions, such as some vegetations.
2. Shortening fraction: Very reliable index of left ventricular function. Normal values range from 30%–45%, depending on age.11
C. Cardiac Catheterization
VI. Congenital Heart Disease
A. Pulse Oximetry Screening for Critical Congenital Heart Disease
1. Recommended after 24 hours of life or as late as possible if earlier discharge from the nursery. There is a lower false-positive rate after 24 hours of life.
2. Screening recommended on the right hand and on one foot, either in parallel or direct sequence.
3. Modes
a. M mode: Ice pick view—limited ability to show spatial structural relationship. Replaced by two-dimensional echo. Currently still used to measure dimensions of vessels and heart chambers, evaluate for pericardial effusion, assess valve motion, left ventricular (LV) systolic function.
b. Two-dimensional: Better demonstration of spatial structure relationship
c. Doppler: To demonstrate flow, cardiac output, and pressure gradients
d. Shortening fraction: Evaluates LV systolic function. Formula: FS (%) = Dd − Ds/Dd × 100 (Dd, End-diastolic dimension; Ds, end-systolic dimension). Normal value mean is 36%.
c. There is a >3% absolute difference in oxygen saturation between the right hand and foot on 3 measures, each separated by 1 hour.
B. Common Syndromes Associated with Cardiac Lesions (Table 7-11)
C. Acyanotic Lesions (Table 7-12)
D. Cyanotic Lesions (Table 7-13)
An oxygen challenge test is used to evaluate the etiology of cyanosis in neonates. Obtain baseline arterial blood gas (ABG) with saturation at FiO2= 0.21, then place infant in an oxygen hood at FiO2= 1 for a minimum of 10 min, and repeat ABG. In cardiac disease, there will not be a significant change in PaO2 following the oxygen challenge test. Note: Pulse oximetry will not be useful for following the change in oxygenation once the saturations reach 100% (approximately PaO2 >90 mmHg).11-14
TABLE 7-11
MAJOR SYNDROMES ASSOCIATED WITH CARDIAC DEFECTS
| Syndrome | Dominant Cardiac Defect |
| CHARGE | TOF, truncus arteriosus, aortic arch abnormalities |
| DiGeorge | Aortic arch anomalies, TOF, truncus arteriosus, VSD, PDA |
| Trisomy 21 | Atrioventricular septal defect, VSD |
| Marfan | Aortic root dilation, mitral valve prolapse |
| Loeys-Dietz | Aortic root dilation with higher risk of rupture at smaller dimensions |
| Noonan | Supravalvular pulmonic stenosis, LVH |
| Turner | COA, bicuspid aortic valve, aortic root dilation as a teenager |
| Williams | Supravalvular aortic stenosis, pulmonary artery stenosis |
| FAS | Occasional: VSD, PDA, ASD, TOF |
| IDM | TGA, VSD, COA, cardiomyopathy |
| VATER/VACTERL | VSD |
| VCFS | Truncus arteriosus, TOF, pulmonary atresia with VSD, TGA, interrupted aortic arch |
ASD, Atrial septal defect; CHARGE, a syndrome of associated defects including Coloboma of the eye, Heart anomaly, choanal Atresia, Retardation, and Genital and Ear anomalies; COA, coarctation of aorta; FAS, fetal alcohol syndrome; IDM, infant of diabetic mother; LVH, left ventricular hypertrophy; PDA, patent ductus arteriosis; TGA, transposition of the great arteries; TOF, tetralogy of Fallot; VATER/VACTERL, association of Vertebral anomalies, Anal atresia, Cardiac anomalies, Tracheoesophageal fistula, Renal/radial anomalies, Limb defects; VCFS, velocardiofacial syndrome; VSD, ventricular septal defect.
Adapted from Park MK. Pediatric Cardiology for Practitioners. 5th ed. St Louis: Mosby; 2008:10-12.
TABLE EC 7-B
INTERPRETATION OF OXYGEN CHALLENGE TEST
| Condition | FIO2= 0.21 PaO2 (% Saturation) | FIO2= 1.00 PaO2 (% Saturation) | PaCO2 | |
| Normal | 70 (95) | >200 (100) | 35 | |
| Pulmonary disease | 50 (85) | >150 (100) | 50 | |
| Neurologic disease | 50 (85) | >150 (100) | 50 | |
| Methemoglobinemia | 70 (85) | >200 (85) | 35 | |
| Cardiac disease | ||||
| • Separate circulation∗ | <40 (<75) | <50 (<85) | 35 | |
| • Restricted PBF† | <40 (<75) | <50 (<85) | 35 | |
| • Complete mixing without restricted PBF‡ | 50 (85) | <150 (<100) | 35 | |
| Persistent pulmonary hypertension | Preductal | Postductal | ||
| PFO (no R–L shunt) | 70 (95) | <40 (<75) | Variable | 35–50 |
| PFO (with R–L shunt) | <40 (<75) | <40 (<75) | Variable | 35–50 |
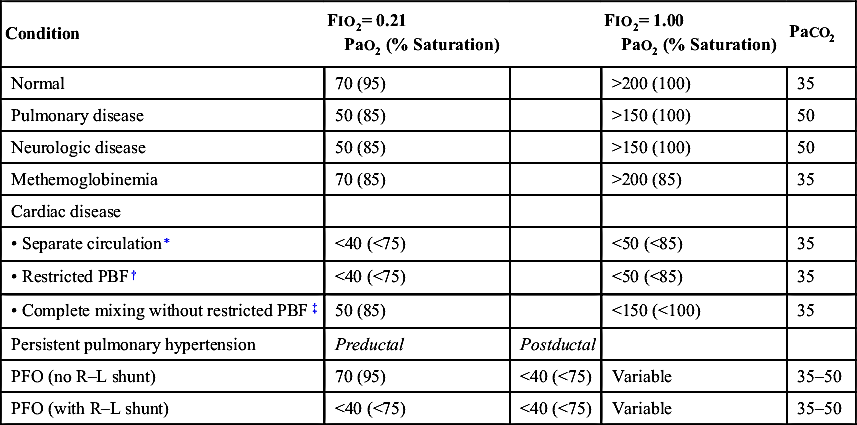
PBF, Pulmonary blood flow; PFO, patent foramen ovale.
∗ D-Transposition of the great arteries (D-TGA) with intact ventricular septum.
† Tricuspid atresia with pulmonary stenosis or atresia, pulmonary atresia or critical pulmonary stenosis with intact ventricular septum, or tetralogy of Fallot.
‡ Truncus, total anomalous pulmonary venous return, single ventricle, hypoplastic left heart, D-TGA with ventricular septal defect, tricuspid atresia without pulmonary stenosis or atresia.
Adapted from Lees MH. Cyanosis of the newborn infant: Recognition and clinical evaluation. J Pediatr. 1970;77:484; Kitterman JA. Cyanosis in the newborn infant. Pediatr Rev. 1982;4:13; and Jones RW, Baumer JH, Joseph MC, et al. Arterial oxygen tension and response to oxygen breathing in differential diagnosis of heart disease in infancy. Arch Dis Child. 1976;51:667-673.
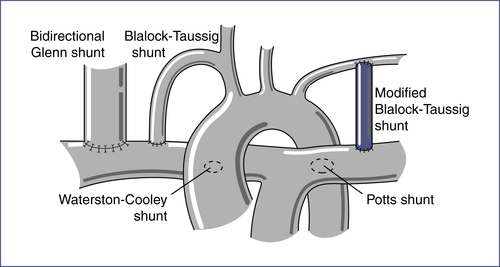
TABLE 7-12
ACYANOTIC CONGENITAL HEART DISEASE
| Lesion Type | % of CHD/Examination Findings | CDG Findings | Chest Radiograph Findings |
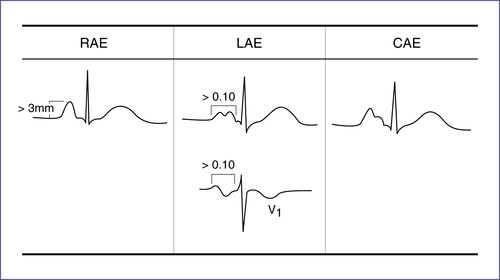
| Ventricular septal defect (VSD) | 2–5/6 holosystolic murmur, loudest at the LLSB, ± systolic thrill ± apical diastolic rumble with large shunt With large VSD and pulmonary hypertension, S2 may be narrow | Small VSD: Normal Medium VSD: LVH ± LAE Large VSD: BVH ± LAE, pure RVH | May show cardiomegaly and increased PVMs, depending on amount of left-to-right shunting |
| Atrial septal defect (ASD) | Wide, fixed split S2 with grade 2–3/6 SEM at the LUSB May have mid-diastolic rumble at LLSB | Small ASD: Normal Large ASD: RAD and mild RVH or RBBB with RSR′ in V1 | May show cardiomegaly with increased PVMs if hemodynamically significant ASD |
| Patent ductus arteriosus (PDA) | 40%–60% in VLBW infants 1–4/6 continuous “machinery” murmur loudest at LUSB Wide pulse pressure | Small–moderate PDA: Normal or LVH Large PDA: BVH | May have cardiomegaly and increased PVMs, depending on size of shunt (see Chapter 18 Section IX.A for treatment) |
| Atrioventricular septal defects | Most occur in Down syndrome Hyperactive precordium with systolic thrill at LLSB and loud S2 ± grade 3–4/6 holosystolic regurgitant murmur along LLSB ± systolic murmur of MR at apex ± mid-diastolic rumble at LLSB or at apex ± gallop rhythm | Superior QRS axis RVH and LVH may be present | Cardiomegaly with increased PVMs |
| Pulmonary stenosis (PS) | Ejection click at LUSB with valvular PS—click intensity varies with respiration, decreasing with inspiration and increasing with expiration S2 may split widely with P2 diminished in intensity SEM (2–5/6) ± thrill at LUSB with radiation to back and sides | Mild PS: Normal Moderate PS: RAD and RVH Severe PS: RAE and RVH with strain | Normal heart size with normal to decreased PVMs |
| Aortic stenosis (AS) | Systolic thrill at RUSB, suprasternal notch, or over carotids Ejection click that does not vary with respiration if valvular AS Harsh SEM (2–4/6) at second RICS or third LICS, with radiation to neck and apex ± early diastolic decrescendo murmur due to AR Narrow pulse pressure if severe stenosis | Mild AS: Normal Moderate–severe AS: LVH ± strain | Usually normal |
| Table Continued | |||
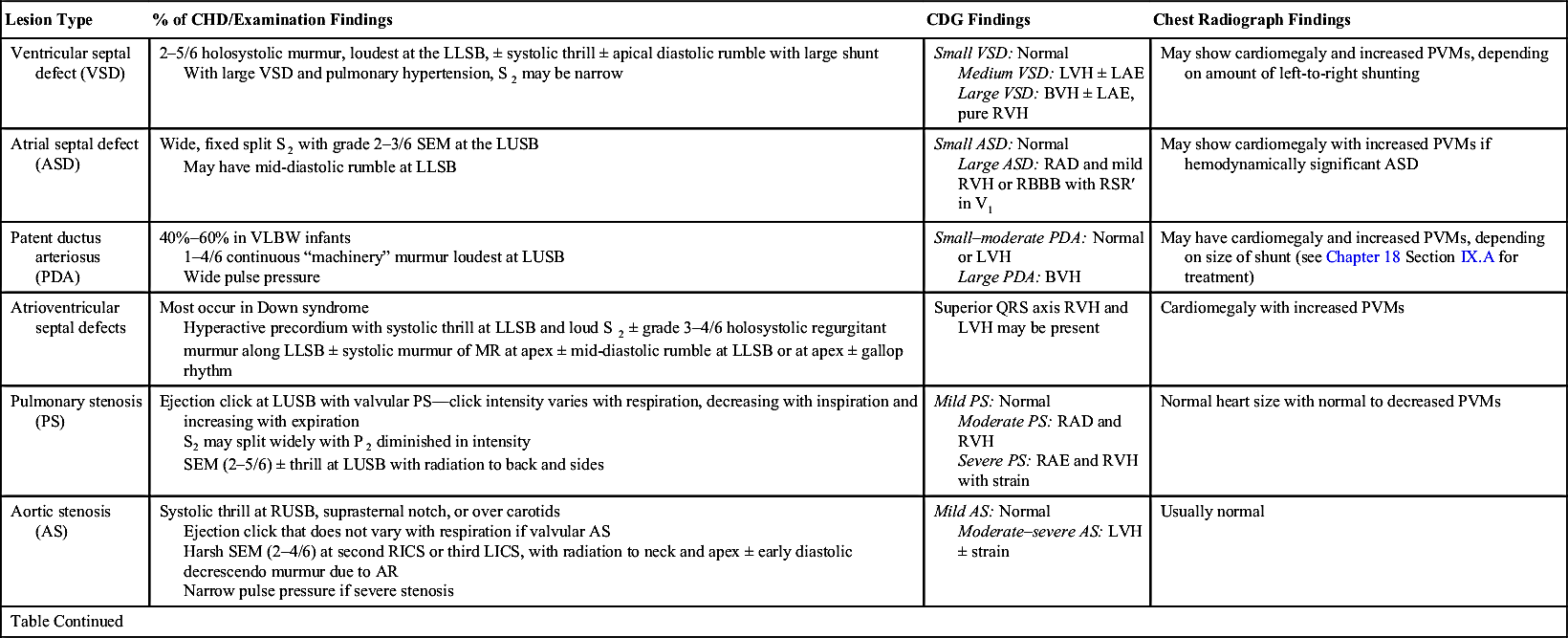

AR, Aortic regurgitation; ASD, atrial septal defect; BP, blood pressure; BVH, biventricular hypertrophy; CHD, congenital heart disease; CHF, congestive heart failure; HTN, hypertension; LAE, left atrial enlargement; LICS, left intercostal space; LLSB, left lower sternal border; LUSB, left upper sternal border; LVH, left ventricular hypertrophy; MR, mitral regurgitation; PVM, pulmonary vascular markings; RAD, right axis deviation; RAE, right atrial enlargement; RBBB, right bundle-branch block; RICS, right intercostal space; RUSB, right upper sternal border; RVH, right ventricular hypertrophy; SEM, systolic ejection murmur; VLBW, very low birth weight (i.e. <1500 g); VSD, ventricular septal defect.
TABLE 7-13
CYANOTIC CONGENITAL HEART DISEASE
| Lesion | Examination Findings | ECG Findings | Chest Radiograph Findings |
| Tetralogy of Fallot: 1. Large VSD 2. RVOT obstruction 3. RVH 4. Overriding aorta Degree of RVOT obstruction will determine whether there is clinical cyanosis. If PS is mild, there will be a left-to-right shunt, and child will be acyanotic. Increased obstruction leads to increased right-to-left shunting across VSD, and child will be cyanotic. | Loud SEM at LMSB and LUSB and a loud, single S2 ± thrill at LMSB and LLSB. Tet spells: Occur in young infants. As RVOT obstruction increases or systemic resistance decreases, right-to-left shunting across VSD occurs. May present with tachypnea, increasing cyanosis, and decreasing murmur. See Table 7-14 for treatment. | RAD and RVH | Boot-shaped heart with normal heart size ± decreased PVMs |
| Table Continued | |||

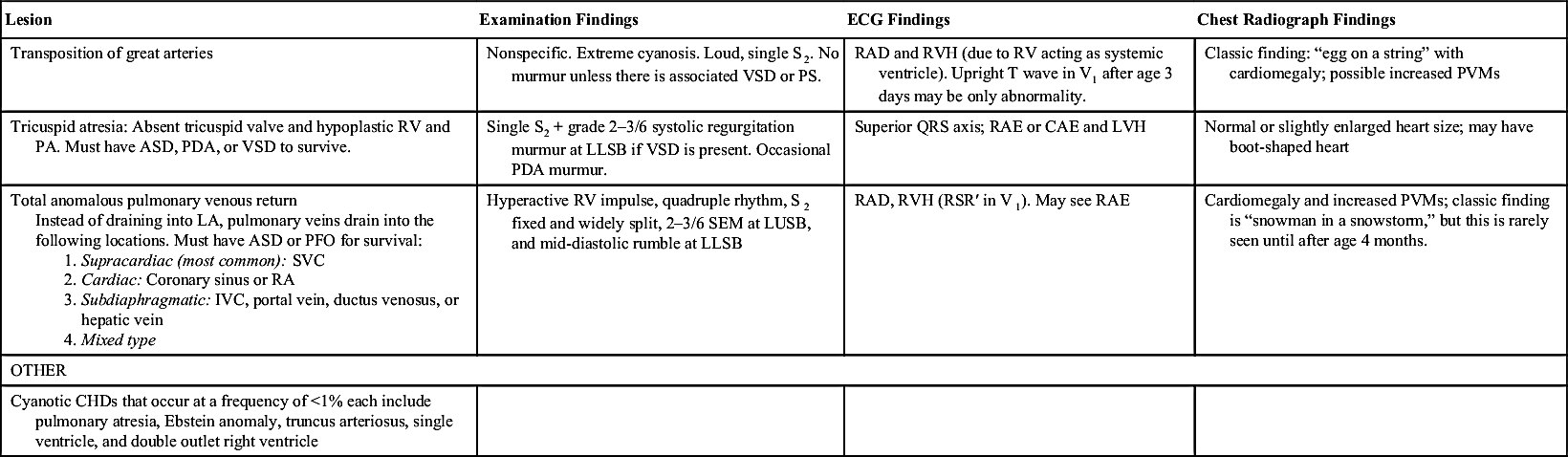
ASD, Atrial septal defect; CAE, common atrial enlargement; ECG, electrocardiogram; IVC, inferior vena cava; LA, left atrium; LLSB, left lower sternal border; LMSB, left mid-sternal border; LUSB, left upper sternal border; LVH, left ventricular hypertrophy; PA, pulmonary artery; PDA, patent ductus arteriosus; PFO, patent foramen ovale; PVM, pulmonary vascular markings; PS, pulmonary stenosis; RA, right atrium; RAD, right-axis deviation; RAE, right atrial enlargement; RV, right ventricle; RVH, right ventricular hypertrophy; RVOT, right ventricular outflow tract; SEM, systolic ejection murmur; SVC, superior vena cava; VSD, ventricular septal defect.
TABLE 7-14
TREATMENT OPTIONS FOR TET SPELLS
| Treatment | Rationale |
| INITIAL OPTIONS | |
| Calm child | Decreases PVR |
| Encourage knee-chest position | Decreases venous return and increases SVR |
| Oxygen | Reduces hypoxemia, decreases PVR |
| Intravenous fluids | Provides volume resuscitation |
| Morphine (morphine sulfate 0.1–0.2 mg/kg SQ or IM) | Decreases venous return, decreases PVR, relaxes infundibulum. Do not try to establish IV access initially; use SQ route. |
| IF THERE IS NO RESPONSE TO INITIAL MEASURES | |
| Phenylephrine (0.02 mg/kg IV) | Increases SVR |
| Propranolol (0.01–0.25 mg/kg slow IV push) | Has negative inotropic effect on infundibular myocardium; may block drop in SVR |
| Ketamine 1–3 mg/kg | Increases SVR and sedates |
| OTHER | |
| Correct anemia | Increases delivery of oxygen to tissues |
| Correct pathologic tachyarrhythmias | May abort hypoxic spell |
| Infuse glucose | Avoids hypoglycemia from increased utilization and depletion of glycogen stores |
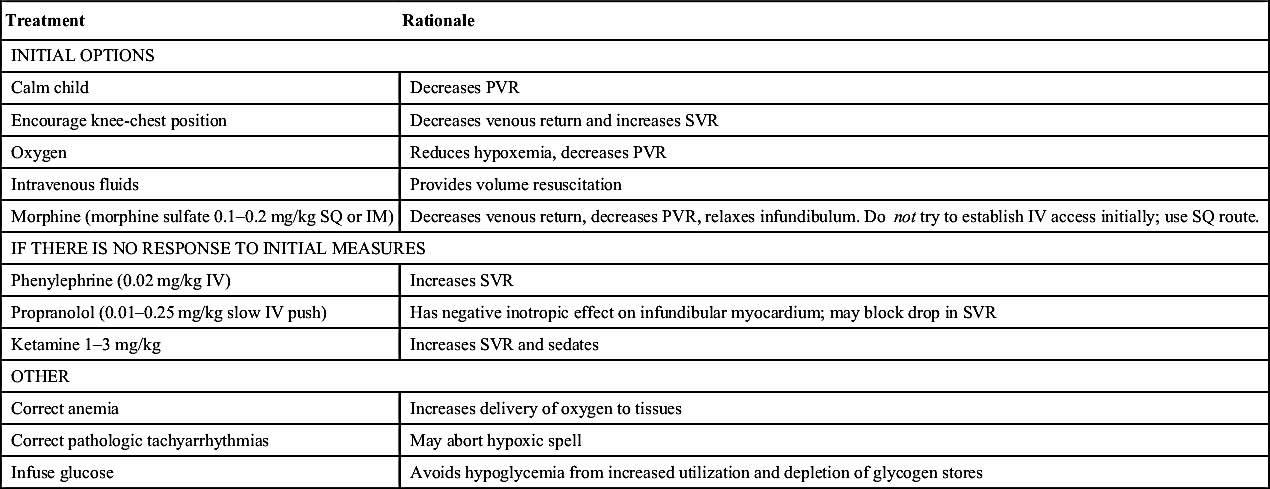
IM, Intramuscular; IV, intravenous; PVR, peripheral venous resistance; SQ, subcutaneous; SVR, systemic vascular resistance.
From Park MK. Pediatric Cardiology for Practitioners. 5th ed. St Louis: Mosby; 2008:239.
E. Surgeries and Other Interventions (Fig. 7-15)
1. Atrial septostomy: Creates an intra-atrial opening to allow for mixing or shunting between atria of systemic and pulmonary venous blood. Used for transposition of the great arteries (TGA), tricuspid, mitral, tricuspid and pulmonary atresia, and sometimes total anomalous pulmonary venous return. Most commonly performed percutaneously with a balloon-tipped catheter (Rashkind procedure).
2. Palliative systemic-to–pulmonary artery shunts, such as the Blalock-Taussig shunt (subclavian artery to pulmonary artery [PA]): Use systemic arterial flow to increase pulmonary blood flow in cardiac lesions with impaired pulmonary perfusion (e.g., TOF, hypoplastic right heart, tricuspid atresia, pulmonary atresia)
3. Palliative superior vena cava–to–pulmonary artery shunts, such as the Glenn shunt, also known as the hemi-Fontan (superior vena cava [SVC] to the right pulmonary artery [RPA]): Directs a portion of the systemic venous return directly into the pulmonary blood flow as an intermediate step to a Fontan procedure. This procedure is usually performed outside the neonatal period, when there is lower pulmonary vascular resistance.
4. Fontan procedure: Performed after the Glenn shunt; involves anastomosis of the right atria and/or inferior vena cava (IVC) to pulmonary arteries via conduits; separates systemic and pulmonary circulations in patients with functionally single ventricles (tricuspid atresia, hypoplastic left heart syndrome)
5. Norwood procedure: Used for hypoplastic left heart syndrome
a. Stage 1 (neonatal period): To provide systemic blood flow, anastomosis of the proximal main pulmonary artery (MPA) is made to the aorta, with aortic arch reconstruction and patch closure of the distal MPA. To provide pulmonary blood flow, a modified right Blalock-Taussig shunt (subclavian artery to RPA) or Sano modification (RV to PA conduit) is performed. An atrial septal defect is created if needed to decompress the left atrium and allow for adequate left-to-right flow. Expected O2 saturations: 75%–85%.
b. Stage 2 (3–6 months of age): Bidirectional Glenn shunt or hemi-Fontan to reduce volume overload of single right ventricle. Expected O2 saturations: 80%–85%.
c. Modified Fontan (age 18 mo–4 yr): Needed to completely separate systemic and pulmonary circulations. Restores normal O2 saturation, with expected O2 saturation >92%.
6. Arterial switch procedure: Used for repair of TGA. Connects aorta to left ventricle and pulmonary artery to right ventricle. Procedure also involves reconnecting coronary arteries to aorta.
7. Ross procedure: Pulmonary root autograft for aortic stenosis; autologous pulmonary valve replaces aortic valve, and aortic or pulmonary allograft replaces pulmonary valve.
VII. Acquired Heart Disease
A. Endocarditis
2. Clinical findings: New heart murmur, recurrent fever, splenomegaly, petechiae, fatigue, Osler nodes (tender nodules at fingertips), Janeway lesions (painless hemorrhagic areas on palms or soles), splinter hemorrhages, and Roth spots (retinal hemorrhages)
B. Bacterial Endocarditis Prophylaxis
1. All dental procedures that involve treatment of gingival tissue or periapical region of the teeth or oral mucosal perforation
2. Invasive procedures that involve incision or biopsy of respiratory mucosa, such as tonsillectomy and adenoidectomy
3. Not recommended for genitourinary or gastrointestinal tract procedures; solely for bacterial endocarditis prevention
C. Myocardial Disease
1. Dilated cardiomyopathy: End result of myocardial damage, leading to atrial and ventricular dilation with decreased systolic contractile function of the ventricles
a. Etiology: Infectious, toxic (alcohol, anthracyclines), metabolic (hypothyroidism, muscular dystrophy), immunologic, collagen vascular disease, nutritional deficiency (kwashiorkor, beriberi)
b. Symptoms: Fatigue, weakness, shortness of breath
c. Examination: Look for signs of CHF(e.g., tachycardia, tachypnea, rales, cold extremities, jugular venous distention, hepatomegaly, peripheral edema, S3 gallop, displacement of point of maximal impulse to the left and inferiorly)
d. Chest radiograph: Generalized cardiomegaly, pulmonary congestion
TABLE 7-15
PROPHYLACTIC REGIMENS FOR DENTAL AND RESPIRATORY TRACT PROCEDURES
| Drug | Dosing∗ (not to exceed adult dose) |
| Amoxicillin† | Adult: 2 g; Child: 50 mg/kg PO |
| Ampicillin | Adult: 2 g; Child: 50 mg/kg IM/IV |
| Cefazolin or ceftriaxone‡ | Adult: 1 g; Child: 50 mg/kg IM/IV |
| Cephalexin‡ | Adult: 2 g; Child: 50 mg/kg PO |
| Clindamycin | Adult: 600 mg; Child: 20 mg/kg PO/IM/IV |
| Azithromycin/clarithromycin | Adult: 500 mg; Child:15 mg/kg PO |
∗ Oral (PO) medications should be given 1 hour before procedure; intramuscular/intravenous (IM/IV) medications should be given within 30 min prior to procedure.
† Standard general prophylaxis.
‡ Cephalosporins should not be used in persons with intermediate-type hypersensitivity reaction to penicillins or ampicillin.
Adapted from Wilson W, Taubert KA, Gewitz M, et al. Prevention of infectiveendocarditis: Guidelines from the American Heart Association: A guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116:1736-1754.
f. Echocardiography: Enlarged ventricles (increased end-diastolic and end-systolic dimensions) with little or no wall thickening; decreased shortening fraction
g. Treatment: Management of CHF (digoxin, diuretics, vasodilation, angiotensin-converting enzyme [ACE] inhibitors, rest). Consider anticoagulants to decrease risk for thrombus formation.
2. Hypertrophic cardiomyopathy: Abnormality of myocardial cells leading to significant ventricular hypertrophy, particularly of left ventricle, with small to normal ventricular dimensions. Increased contractile function but impaired filling secondary to stiff ventricles. The most common type is asymmetrical septal hypertrophy, also called idiopathic hypertrophic subaortic stenosis (IHSS), with varying degrees of obstruction. A 4%–6% incidence of sudden death in children and adolescents with hypertrophic obstructive cardiomyopathy (HOCM).
a. Etiology: Genetic (autosomal dominant, 60% of cases) or sporadic (40% of cases)
b. Symptoms: Easy fatigability, anginal pain, shortness of breath, occasional palpitations
c. Examination: Usually in adolescents or young adults; signs include left ventricular heave, sharp upstroke of arterial pulse, murmur of mitral regurgitation, midsystolic ejection murmur along left midsternal border (LMSB) that increases in intensity in the standing position (in patients with midcavity left ventricular obstruction)
d. Chest radiograph: Globular-shaped heart with left ventricular enlargement
f. Echocardiography: Extent and location of hypertrophy, obstruction, increased contractility
g. Treatment: Moderate restriction of physical activity, administration of negative inotropes (β-blocker, calcium channel blocker) to help improve filling and subacute bacterial endocarditis prophylaxis. If at increased risk for sudden death, may consider implantable defibrillator. If symptomatic with subaortic obstruction, may benefit from myectomy.
3. Restrictive cardiomyopathy: Myocardial or endocardial disease (usually infiltrative or fibrotic) resulting in stiff ventricular walls, with restriction of diastolic filling but normal contractile function. Results in atrial enlargement. Associated with a high mortality rate. Very rare in children.
a. Etiology: Scleroderma, amyloidosis, sarcoidosis, mucopolysaccharidosis
b. Treatment: Supportive, poor prognosis. Diuretics, anticoagulants, calcium channel blockers, pacemaker for heart block, cardiac transplantation if severe.
4. Myocarditis: Inflammation of myocardial tissue
a. Etiology: Viral (coxsackievirus, echovirus, adenovirus, poliomyelitis, mumps, measles, rubella, cytomegalovirus, HIV, arbovirus, influenza); bacterial, rickettsial, fungal, or parasitic infection; immune-mediated disease (Kawasaki disease, acute rheumatic fever); collagen vascular disease; toxin-induced
b. Symptoms: Nonspecific and inconsistent, depending on severity of disease. Variably anorexia, lethargy, emesis, lightheadedness, cold extremities, shortness of breath.
c. Examination: Look for signs of CHF (tachycardia, tachypnea, jugular venous distention, rales, gallop, hepatomegaly); occasionally a soft systolic murmur or arrhythmia may be noted.
d. Chest radiograph: Variable cardiomegaly and pulmonary edema
e. ECG: Low QRS voltages throughout (<5 mm), ST-segment and T-wave changes (e.g., decreased T-wave amplitude), prolongation of QT interval, arrhythmias (especially premature contractions, first- or second-degree AV block)
f. Laboratory tests: CK, troponin
g. Echocardiography: Enlargement of heart chambers, impaired left ventricular function
h. Treatment: Bed rest, diuretics, inotropes (dopamine, dobutamine, milrinone), digoxin, gamma globulin (2 g/kg over 24 hours), ACE inhibitors, possibly steroids. May require heart transplantation if no improvement (≈20%–25% of cases)
D. Pericardial Disease
1. Pericarditis: Inflammation of visceral and parietal layers of pericardium
b. Symptoms: Chest pain (retrosternal or precordial, radiating to back or shoulder, pleuritic in nature, alleviated by leaning forward, aggravated by supine position), dyspnea
c. Examination: Pericardial friction rub, distant heart sounds, fever, tachypnea
d. ECG: Diffuse ST-segment elevation in almost all leads (representing inflammation of adjacent myocardium); PR-segment depression
e. Treatment: Often self-limited. Treat underlying condition and provide symptomatic treatment with rest, analgesia, and antiinflammatory drugs
2. Pericardial effusion: Accumulation of excess fluid in pericardial sac
a. Etiology: Associated with acute pericarditis (exudative fluid) or serous effusion resulting from increased capillary hydrostatic pressure (e.g., CHF), decreased plasma oncotic pressure (e.g., hypoproteinemia), and increased capillary permeability (transudative fluid)
b. Symptoms: Can present with no symptoms, dull ache in left chest, abdominal pain, or symptoms of cardiac tamponade (see later)
c. Examination: Muffled distant heart sounds, dullness to percussion of posterior left chest (secondary to atelectasis from large pericardial sac), hemodynamic signs of cardiac compression
d. Chest radiograph: Globular symmetrical cardiomegaly
e. ECG: Decreased voltage of QRS complexes, electrical alternans (variation of QRS axis with each beat secondary to swinging of heart within pericardial fluid)
f. Echocardiography shows extent and location of hypertrophy, obstruction, increased contractility
g. Treatment: Address underlying condition. Observe if asymptomatic; use pericardiocentesis if there is sudden increase in volume or hemodynamic compromise. Nonsteroidal antiinflammatory drugs (NSAIDs) or steroids may be of benefit, depending on etiology.
3. Cardiac tamponade: Accumulation of pericardial fluid under high pressure, causing compression of cardiac chambers, limiting filling, and decreasing stroke volume and cardiac output
a. Etiology: Same as pericardial effusion; most commonly associated with viral infection, neoplasm, uremia, and acute hemorrhage
b. Symptoms: Dyspnea, fatigue, cold extremities
c. Examination: Jugular venous distention, hepatomegaly, peripheral edema, tachypnea, rales (from increased systemic and pulmonary venous pressure), hypotension, tachycardia, pulsus paradoxus (decrease in systolic blood pressure by >10 mmHg with each inspiration), decreased capillary refill (from decreased stroke volume and cardiac output), quiet precordium, and muffled heart sounds
d. ECG: Sinus tachycardia, decreased voltage, electrical alternans
e. Echocardiography: Right ventricle collapse in early diastole, right atrial/left atrial collapse in end-diastole and early systole
f. Treatment: Pericardiocentesis with temporary catheter left in place if necessary (see Chapter 3, Figs. 3-15 and 3-16); pericardial window or stripping if it is a recurrent condition
E. Kawasaki Disease
Acute febrile vasculitis of unknown etiology, common in children < 8 years of age, and the leading cause of acquired heart disease in children in developed countries
1. Etiology: Unknown; thought to be immune regulated in response to infectious agents or environmental toxins
2. Diagnosis:
a. Typical Kawasaki disease: Based on clinical criteria. These include high fever lasting 5 days or more, plus at least 4 of the following 5 criteria:
(1) Bilateral painless bulbar conjunctival injection without exudate
(2) Erythematous mouth and pharynx, strawberry tongue, or red cracked lips
(3) Polymorphous exanthem (may be morbilliform, maculopapular, or scarlatiniform)
(4) Swelling of hands and feet, with erythema of palms and soles
(5) Cervical lymphadenopathy (>1.5 cm in diameter), usually single and unilateral
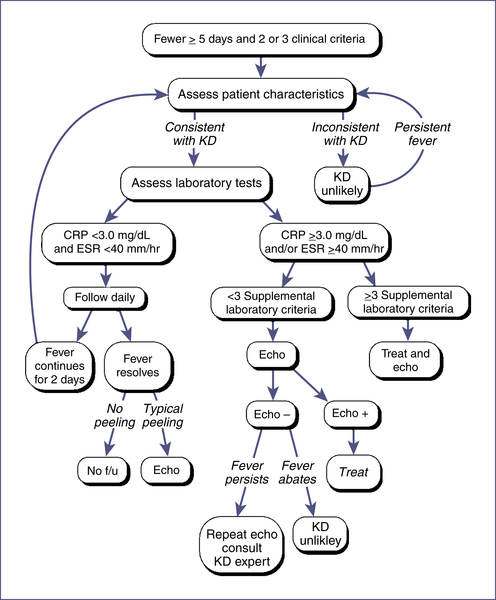
b. Atypical/incomplete Kawasaki disease: A suspicion of Kawasaki but with fewer of the criteria required for diagnosis. Even without all criteria, there is a risk for coronary artery abnormalities.
(1) More often seen in infants. Echocardiography should be considered in any infant < 6 months with fever > 7 days duration, laboratory evidence of systemic inflammation, and no other explanation for the febrile illness.
(2) See Fig. 7-16 for evaluation of incomplete Kawasaki disease.
(3) Supplemental laboratory criteria: Albumin ≤ 3.0 g/dL, anemia for age, elevation of alanine aminotransferase, platelets after 7 days ≥ 450,000 / mm3, white blood cell count ≥ 15,000 / mm3, and urine white blood cells/hpf ≥ 10.
3. Other clinical findings: Often associated with extreme irritability, abdominal pain, diarrhea, vomiting. Also seen are arthritis and arthralgias, hepatic enlargement, jaundice, acute acalculous distention of the gallbladder, carditis, aseptic meningitis (50% of those undergoing LP).
4. Laboratory findings: Leukocytosis with left shift, neutrophils with vacuoles or toxic granules, elevated C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) (seen acutely), thrombocytosis (after first week, peaking at 3 weeks), normocytic and normochromic anemia, sterile pyuria (33%), increased transaminases (40%), hyperbilirubinemia (10%)
5. Subacute phase (11–25 days after onset of illness): Resolution of fever, rash, and lymphadenopathy. Often, desquamation of the fingertips or toes and thrombocytosis occur.
Cardiovascular complications: If untreated, 20%–25% develop coronary artery aneurysms and dilation in subacute phase (peak prevalence occurs about 2–4 weeks after onset of disease; rarely appears after 6 weeks) and are at risk for coronary thrombosis acutely and coronary stenosis chronically. Carditis; aortic, mitral, and tricuspid regurgitation; pericardial effusion; CHF; MI; left ventricular dysfunction; and ECG changes may also occur.
6. Convalescent phase: ESR, CRP, and platelet count return to normal. Those with coronary artery abnormalities are at increased risk for MI, arrhythmias, and sudden death.
a. Intravenous immunoglobulin (IVIG)
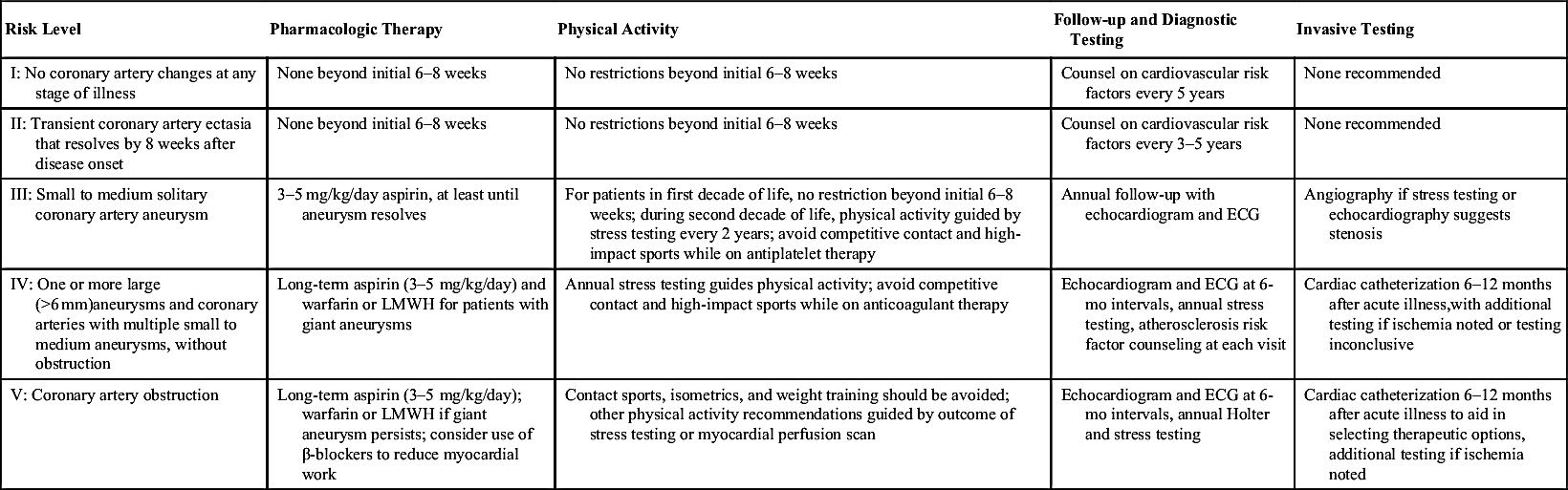
TABLE EC 7-C
GUIDELINES FOR TREATMENT AND FOLLOW-UP OF CHILDREN WITH KAWASAKI DISEASE
| Risk Level | Pharmacologic Therapy | Physical Activity | Follow-up and Diagnostic Testing | Invasive Testing |
| I: No coronary artery changes at any stage of illness | None beyond initial 6–8 weeks | No restrictions beyond initial 6–8 weeks | Counsel on cardiovascular risk factors every 5 years | None recommended |
| II: Transient coronary artery ectasia that resolves by 8 weeks after disease onset | None beyond initial 6–8 weeks | No restrictions beyond initial 6–8 weeks | Counsel on cardiovascular risk factors every 3–5 years | None recommended |
| III: Small to medium solitary coronary artery aneurysm | 3–5 mg/kg/day aspirin, at least until aneurysm resolves | For patients in first decade of life, no restriction beyond initial 6–8 weeks; during second decade of life, physical activity guided by stress testing every 2 years; avoid competitive contact and high-impact sports while on antiplatelet therapy | Annual follow-up with echocardiogram and ECG | Angiography if stress testing or echocardiography suggests stenosis |
| IV: One or more large (>6 mm)aneurysms and coronary arteries with multiple small to medium aneurysms, without obstruction | Long-term aspirin (3–5 mg/kg/day) and warfarin or LMWH for patients with giant aneurysms | Annual stress testing guides physical activity; avoid competitive contact and high-impact sports while on anticoagulant therapy | Echocardiogram and ECG at 6-mo intervals, annual stress testing, atherosclerosis risk factor counseling at each visit | Cardiac catheterization 6–12 months after acute illness,with additional testing if ischemia noted or testing inconclusive |
| V: Coronary artery obstruction | Long-term aspirin (3–5 mg/kg/day); warfarin or LMWH if giant aneurysm persists; consider use of β-blockers to reduce myocardial work | Contact sports, isometrics, and weight training should be avoided; other physical activity recommendations guided by outcome of stress testing or myocardial perfusion scan | Echocardiogram and ECG at 6-mo intervals, annual Holter and stress testing | Cardiac catheterization 6–12 months after acute illness to aid in selecting therapeutic options, additional testing if ischemia noted |
(2) Some 10% of patients treated with IVIG fail to respond (persistent or recurrent fever ≥36 hr after IVIG completion). Re-treat with second dose.
b. Aspirin is recommended for both its antiinflammatory and antiplatelet effects. American Heart Association (AHA) recommends initial high-dose aspirin (80–100 mg/kg/day divided in four doses) until 48–72 hours after defervescence. Given with IVIG. Then continue with low-dose aspirin (3–5 mg/kg/day as a single daily dose) for 6–8 weeks or until platelet count and ESR are normal (if there are no coronary artery abnormalities) or indefinitely if coronary artery abnormalities persist.
c. Dipyridamole, 4 mg/kg divided in three doses, is sometimes used as an alternative to aspirin, particularly if symptoms of influenza or varicella arise while on aspirin (concern for Reye syndrome).
d. Follow-up: Serial echocardiography is recommended to assess coronary arteries and left ventricular function (at time of diagnosis, at 2 weeks, at 6–8 weeks, and at 12 months [optional]). More frequent intervals and long-term follow-up are recommended if abnormalities are seen on echocardiography. Cardiac catheterization may be necessary.
F. Rheumatic Heart Disease
1. Etiology: Believed to be immunologically mediated delayed sequela of group A streptococcal pharyngitis
2. Clinical findings: History of streptococcal pharyngitis 1–5 weeks before onset of symptoms. Often with pallor, malaise, easy fatigability.
3. Diagnosis: Jones criteria (Box 7-5)
4. Management: Penicillin, bed rest, salicylates, supportive management of CHF (if present) with diuretics, digoxin, morphine
G. Lyme Disease
1. Etiology: Following infection with Borrelia burgdorferi
2. Clinical symptoms: About 8%–10% of patients will get AV block. Other possible cardiac symptoms include myocarditis and pericarditis.
VIII. Exercise Recommendations for Congenital Heart Disease
IX. Lipid Monitoring Recommendations
A. Screening of Children and Adolescents18
1. Universal screening of non-fasting non-HDL cholesterol in children 9–11 years old (prior to onset of puberty) and again in individuals 17–21 years
2. Targeted screening should occur in children 2–8 years old and adolescents 12–16 years old, with two fasting lipid profiles (between 2 weeks and 3 months apart, results averaged) for the following risk factors:
TABLE EC 7-D
EXERCISE RECOMMENDATIONS FOR CONGENITAL HEART DISEASE AND SPORTS ALLOWED FOR SOME SPECIFIC CARDIAC LESIONS15
| Diagnosis | Sports Allowed |
| Small ASD or VSD | All |
| Mild aortic stenosis | All |
| MVP (without other risk factors) | All |
| Moderate aortic stenosis | IA, IB, IIA |
| Mild LV dysfunction | IA, IB, IC |
| Moderate LV dysfunction | IA only |
| Long QT syndrome | IA only |
| Hypertrophic cardiomyopathy | None (or IA only) |
| Severe aortic stenosis | None |
| Sports Classification | Low Dynamic (A) | Moderate Dynamic (B) | High Dynamic (C) |
| I. Low static | Billiards Bowling Golf Riflery | Baseball/softball Table tennis Volleyball Fencing | Racket sports Cross-country skiing Field hockey∗ Race walking Running (long distance) Soccer∗ |
| II. Moderate static | Archery Auto racing∗,† Diving∗,† Equestrian∗,† Motorcycling∗,† | Fencing Field events (jumping) Figure skating∗ Football (American)∗ Surfing Rugby∗ Running (sprint) Synchronized swim† | Basketball∗ Ice hockey∗ Cross-country skiing (skating technique) Swimming Lacrosse∗ Running (middle distance) Team handball |
| III. High static | Bobsledding Field events Gymnastics∗,† Rock climbing Sailing Windsurfing∗,† Waterskiing∗,† Weight lifting∗,† | Body building∗,† Downhill skiing∗,† Skateboarding∗,† | Boxing/wrestling∗ Martial arts∗ Rowing Speed skating Cycling∗,† |
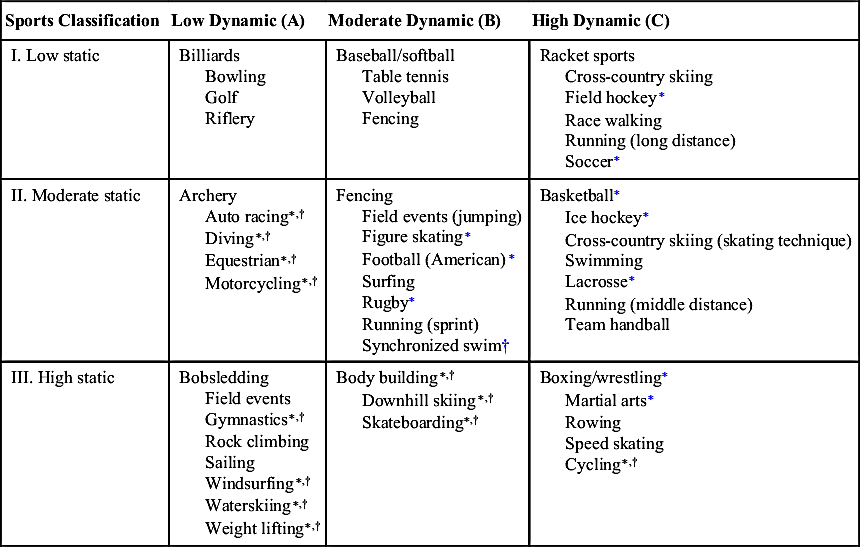
ASD, Atrial septal defect; LV, left ventricular; MVP, mitral valve prolapse; VSD, ventricular septal defect.
∗ Danger of bodily collision.
† Increased risk if syncope occurs.
Adapted from Maron BJ, Zipes DP. 36th Bethesda Conference: Eligibility recommendations for competitive athletes with cardiovascular abnormalities. J Am Coll Cardiol. 2005;45:1313-1375; and Committee on Sports Medicine and Fitness, American Academy of Pediatrics. Medical conditions affecting sports participation. Pediatrics. 2001;107:1205-1209.
| Major Manifestations | Minor Manifestations |
| Carditis | Clinical findings: |
| Polyarthritis | Arthralgia |
| Chorea | Fever |
| Erythema marginatum | Laboratory findings: |
| Subcutaneous nodule | Elevated acute phase reactants (erythrocyte sedimentation rate, C-reactive protein) |
| Prolonged PR interval | |
| Plus | |
| Supporting evidence of antecedent group A streptococcal infection | |
| Positive throat culture or rapid streptococcal antigen test | |
| Elevated or rising streptococcal antibody titer | |

NOTE: If supported by evidence of preceding group A streptococcal infection, the presence of two major manifestations or of one major and two minor manifestations indicates a high probability of acute rheumatic fever.
tract infections, known renal or urologic malformations, family history of congenital renal disease, solid organ transplant, malignancy or bone marrow transplant, treatment with drugs known to raise blood pressure, other systemic illness associated with hypertension (neurofibromatosis, tuberous sclerosis), evidence of elevated intracranial pressure
b. Have other cardiovascular risk factors (diabetes, hypertension, body mass index [BMI] ≥ 95th percentile, smoke cigarettes)
c. Have a family history of early cardiovascular disease (CVD) or severe hypercholesterolemia
(1) Parent or grandparent who is < 55 years old (males) or < 65 years old (females) and had suffered a myocardial infarction or sudden death, undergone a coronary artery procedure, or who otherwise had evidence of coronary atherosclerosis, peripheral vascular disease, or cerebrovascular disease
(2) Parent with total cholesterol ≥ 240 mg/dL or known dyslipidemia
B. Goals for Lipid Levels in Childhood
1. Total cholesterol
a. Acceptable (<170 mg/dL): Repeat measurement in 3–5 years
b. Borderline (170–199 mg/dL): Repeat cholesterol and average with previous measurement. If <170, repeat in 3–5 years. If ≥170, obtain lipoprotein analysis.
c. High (≥200 mg/dL): Obtain lipoprotein analysis
C. Management of Hyperlipidemia18
1. Normal and borderline elevated LDL levels: Education, risk factor intervention including diet, smoking cessation, and an exercise program. For borderline levels, reevaluate in 1 year.
2. High LDL levels: Examine for secondary causes (liver, thyroid, renal disorders) and familial disorders. Initiate low-fat, low-cholesterol diet; reevaluate in 6 months. Note: For LDL cholesterol > 250 or triglyceridemia >500, refer directly to a lipid specialist.
3. Drug therapy: Should be considered in children >10 years of age after failure of 6- to 12-month trial of diet therapy as follows:
a. LDL >190 mg/dL without other cardiovascular disease risk factors
b. LDL >160 mg/dL with risk factors (diabetes, obesity, hypertension, positive family history of premature CVD)
c. LDL >130 mg/dL in children with diabetes mellitus
d. Bile acid sequestrants and statins are the usual first-line drugs for treatment in children.
4. Persistently high triglycerides (>150 mg/dL) and reduced HDL (<35 mg/dL): Evaluate for secondary causes (diabetes, alcohol abuse, renal or thyroid disease). Treatment is diet and exercise.