Dental Hygiene Care Plan, Evaluation, and Documentation
1. Discuss the planning phase in the dental hygiene process of care, including:
• Explain the purpose of the planning phase and the client's role in care plan development.
• Identify the sequence for developing a dental hygiene care plan and how each step relates to the dental hygiene diagnosis.
2. Do the following regarding the evaluation phase of client care:
• Explain the purpose of the evaluation phase and its significance to the process of care.
• Formulate a client-centered care plan from a dental hygiene diagnosis.
3. Discuss documentation, including its significance to the process of care and practitioner liability.
Care planning, evaluation, and documentation are processes applied daily by the dental hygienist in clinical practice. They are integral to the process of care and dependent on the preceding phases of care, assessing, and diagnosing. Integrating care planning, evaluation, and documentation into dental hygiene care ensures a client-centered approach to care.
Planning
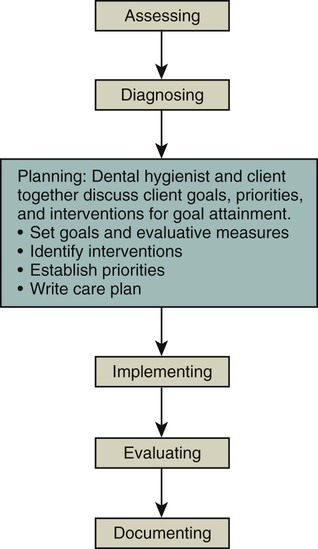
Planning is that phase of the process of care in which diagnosed client needs are prioritized, client goals and evaluative measures are established, and intervention strategies are determined (Figure 22-1). The purpose of the planning phase is to develop a plan of care that results in the resolution of an oral health problem amenable to dental hygiene care, the prevention of a problem, or the promotion of oral and general health. Therefore the term dental hygiene care plan rather than dental hygiene treatment plan is used intentionally to denote the broad range of preventive, educational, therapeutic, and support services within the scope of dental hygiene practice. In keeping with standards of practice and evidence-based interventions, the dental hygienist engages the client in formulating a client-centered plan with clearly defined tangible and measurable outcomes.
To formulate a care plan the dental hygienist must do the following effectively:
• Use parameters or standards of dental hygiene care.
• Collect, analyze, and interpret comprehensive client findings.
• Integrate evidence-based knowledge and theory, professional judgment, and the client's values.
• Develop dental hygiene diagnoses and formulate client-centered goals, which include the action required by the client, a specific date each goal is to be achieved, a criterion-based objective outcome measure, and supportive dental hygiene interventions.
• Synthesize this aforementioned information into a written plan.
• Communicate oral health needs to clients.
• Position the dental hygiene care plan within the context of the total dental treatment plan.
Dental Treatment Plan
The general dentist or dental specialist develops a comprehensive dental treatment plan for the client. This plan includes the dental diagnosis; all essential phases of therapy to be carried out by the dentist, dental hygienist, and client to eliminate and manage disease or promote health; and the prognosis. Components of a dental treatment plan are shown in Table 22-1. The dental hygiene care plan supports the overall dental plan. Ongoing collaboration between the dental hygienist, dentist, physician (when warranted), and client is critical to attaining a successful outcome.
TABLE 22-1
Components of the Overall Dental Care Plan
| Components | Included in the Dental Hygiene Care Plan |
| Preliminary Phase: Emergency Care | |
| Relief of pain | |
| Laboratory tests for suspected pathology | |
| Emergency needs (e.g., treatment of periodontal or periapical abscess) | |
| Extraction of hopeless teeth (in some cases may be postponed to later phases of care) | |
| Provisional replacement to restore function, as needed (in some cases may be postponed to later phases of care) | |
| Phase I: Nonsurgical Therapy | |
| Client education and self-care instruction | x |
| Dietary guidance (e.g., caries risk prevention, tissue healing) | x |
| Tobacco cessation counseling | x |
| Fluoride and remineralization therapy | x |
| Placement of pit and fissure sealants | x |
| Therapeutic periodontal debridement | x |
| Hard-tissue desensitization | x |
| Correction of restorative and prosthetic irritational factors, excavation of caries and restorations (temporary or final as determined by the prognosis of the tooth and location of the caries) | |
| Antimicrobial (anti-infective) therapy (local or systemic) | x |
| Occlusal therapy, minor orthodontics | |
| Coronal polishing | x |
| Phase I: Evaluation of Response to Nonsurgical Therapy | |
| Reassessment of gingival and periodontal health, hard and soft deposits, host response, caries risk factors | x |
| Review and reinforcement of self-care | x |
| Debridement of residual hard and soft deposits | x |
| Recommend a schedule for Phase IV: Maintenance Therapy | x |
| Phase II: Surgical Therapy | |
| Periodontal surgery | |
| Implant surgery | |
| Endodontic therapy | |
| Phase III: Restorative Therapy | |
| Restorative care and final management of dental caries | |
| Fixed and removable prosthodontic appliances | |
| Evaluation of response to restorative procedures (e.g., periodontal status, host response) | |
| Phase IV: Maintenance Therapy | |
| Reassess oral health (e.g., hard and soft deposits, gingival and periodontal inflammation, client adherence to oral self-care, caries risk) | x |
| Supportive, preventive, and therapeutic periodontal maintenance therapy | x |
| Self-care education (e.g., review, modify as needed, reinforce) | x |
| Evaluation and recommendation for schedule of continued-care interval | x |
Adapted from Carranza FA, Takei HH: The treatment plan. In Newman MG, Takei HH, Klokkevold PR, et al, eds: Carranza's clinical periodontology, ed 11, St Louis, 2012, Elsevier/Saunders; Nield-Gehrig JS, Willmann DE: Decision-making during treatment planning. In Nield-Gehrig JS, Willmann DE: Foundations in periodontics for the dental hygienist, ed 3, Philadelphia, 2011, Lippincott Williams and Wilkins.
Dental Hygiene Care Plan
The dental hygiene care plan is the written blueprint that directs the dental hygienist and client as they work together to meet the client's oral health goals.1 The plan encourages the oral healthcare team to work collaboratively to deliver client-centered, goal-oriented care. The plan facilitates the monitoring of client progress, ensures continuity of care, serves as a vehicle for communication among healthcare professionals, and increases the likelihood of high-quality care (Box 22-1).
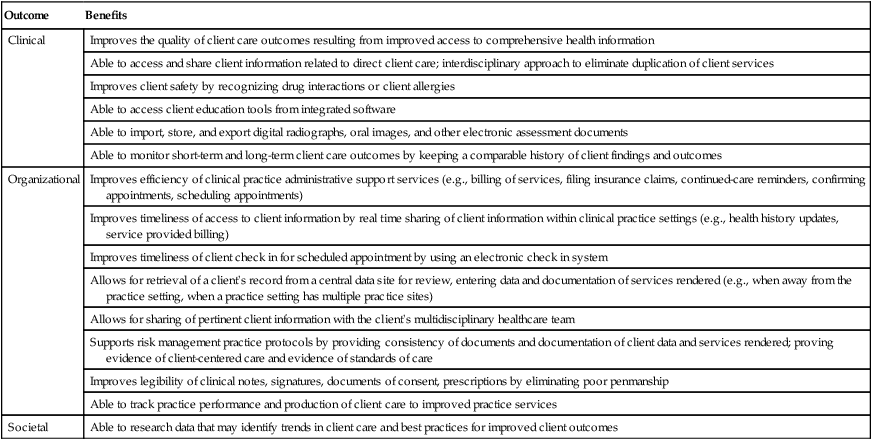
With the advent of the electronic health record (EHR), the attributes of the dental hygiene care plan can be strengthened. An EHR is a multipurpose health information technology system that compiles comprehensive client information and makes it readily available to the healthcare team. Use of an EHR system has the potential to improve clinical, organizational, and societal outcomes2,3 (Table 22-2). Therefore it is advantageous to include the dental hygiene care plan within the EHR.
TABLE 22-2
Potential Benefit of Electronic Health Records to Clinical, Organizational, and Societal Outcome2,3
| Outcome | Benefits |
| Clinical | Improves the quality of client care outcomes resulting from improved access to comprehensive health information |
| Able to access and share client information related to direct client care; interdisciplinary approach to eliminate duplication of client services | |
| Improves client safety by recognizing drug interactions or client allergies | |
| Able to access client education tools from integrated software | |
| Able to import, store, and export digital radiographs, oral images, and other electronic assessment documents | |
| Able to monitor short-term and long-term client care outcomes by keeping a comparable history of client findings and outcomes | |
| Organizational | Improves efficiency of clinical practice administrative support services (e.g., billing of services, filing insurance claims, continued-care reminders, confirming appointments, scheduling appointments) |
| Improves timeliness of access to client information by real time sharing of client information within clinical practice settings (e.g., health history updates, service provided billing) | |
| Improves timeliness of client check in for scheduled appointment by using an electronic check in system | |
| Allows for retrieval of a client's record from a central data site for review, entering data and documentation of services rendered (e.g., when away from the practice setting, when a practice setting has multiple practice sites) | |
| Allows for sharing of pertinent client information with the client's multidisciplinary healthcare team | |
| Supports risk management practice protocols by providing consistency of documents and documentation of client data and services rendered; proving evidence of client-centered care and evidence of standards of care | |
| Improves legibility of clinical notes, signatures, documents of consent, prescriptions by eliminating poor penmanship | |
| Able to track practice performance and production of client care to improved practice services | |
| Societal | Able to research data that may identify trends in client care and best practices for improved client outcomes |
The dental hygiene care plan is written immediately after the assessment and diagnosis phases of the process of care and in conjunction with the overall dental treatment plan prepared by the dentist. The dental hygiene care plan specifies the following:
• Dental hygiene diagnoses based on assessed deficits in eight human needs related to dental hygiene care
During the planning phase of care, dental hygiene diagnoses are prioritized and each component of the care plan is developed sequentially and linked to the dental hygiene diagnoses. Establishing this link between the dental hygiene diagnosis, client goals, and dental hygiene interventions is critical to the outcome of the care plan (Figure 22-2).

Each dental hygiene care facility may have its own electronic care plan format to document assessment findings, dental hygiene diagnoses, client-centered goals, dental hygiene interventions, appointment schedule, and an evaluative statement of outcome. Although formats may differ, the critical point is that these components are documented in the client's permanent record and are followed to ensure high-quality dental hygiene care. The plan may use standardized abbreviations and key phrases as specified in the policy manual of the healthcare institution with which the dental hygienist is affiliated (Box 22-2). Figure 21-3 in Chapter 21 is a dental hygiene care plan form for documenting unmet human needs.
Sequence of Dental Hygiene Care Plan Development
Linking the Diagnosis and the Care Plan
A dental hygiene diagnosis is the foundation for care plan development. Basing dental hygiene care plans on the dental hygiene diagnosis, rather than on oral symptoms alone, ensures that care will be comprehensive, humanistic, and focused on client needs. A care plan may include a single or multiple dental hygiene diagnoses.
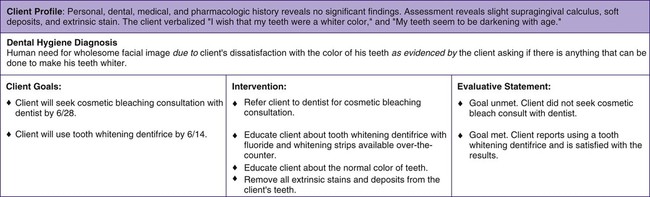
A complete dental hygiene diagnosis includes a statement of the problem (unmet human needs related to oral health within the scope of dental hygiene practice), cause of the problem (etiology or contributor), and signs and symptoms of the problem (evidence). By focusing on the causes of the problem and evidence of the unmet human needs, the clinician is able to develop client goals and intervention strategies that best meet the need or eliminate the problem. Therefore client care is individualized rather than generic routine care provided to all. Because signs and symptoms related to dental hygiene problems may have numerous causes, interventions must be selected carefully to ensure that the fundamental cause is addressed in dental hygiene care. For example, a dental hygiene diagnosis of an unmet human need in the area of wholesome facial image may result from the following:
• Client dissatisfaction with the color of his or her teeth
• Client embarrassment because of a disfiguring malocclusion
• Middle-aged client's loss of self-esteem associated with mobile teeth and oral malodor from chronic periodontal disease
• Nursing home resident who no longer wants to interact with friends and family because of lost dentures
These situations require the establishment of unique client goals and dental hygiene interventions to resolve them. Figure 22-3 provides an example of a dental hygiene diagnosis, related client-centered goals, planned dental hygiene interventions, and evaluation statements that focus on the unique needs of a client who is dissatisfied with his tooth color.
Establishing Priorities
In collaboration with the dentist, the dental hygienist considers the dental and dental hygiene diagnoses and determines their urgency.1 Priorities are based on the degree to which the dental hygiene diagnosis does the following:
• Threatens the client's well-being; it is important to distinguish unmet needs that pose the greatest threat to client safety, health, and comfort from those that are not life threatening and/or related to a current oral disease
Once these criteria are applied to the dental hygiene diagnoses, the dental hygienist ranks the unmet human needs in priority to be addressed. Other than meeting the client's unmet human need for safety (prevention of health risks), which in some instances requires emergency care or referral to a physician, dentists and dental hygienists most likely would identify the client's ability to assume responsibility for oral health as a primary priority. Factors influencing how priorities are established include the following:
Setting Goals
A client-centered goal is the client's desired outcome achieved through specific dental hygiene intervention strategies to satisfy an unmet human need related to dental hygiene care.1 The goal must reflect the signs and reported symptoms of the client's unmet needs. In this way, the clinician establishes a relationship that enables the clinician and client to measure the extent to which a goal has been achieved in terms of changes in the client's initial signs and symptoms. A dental hygiene diagnosis may have one or more defined goals.
A client-centered goal may address cognitive, psychomotor, affective, or oral health status needs:
• Cognitive goals target increases in the client's knowledge and understanding.
• Psychomotor goals focus on the client's skill development and skill mastery.
• Affective goals pinpoint desired changes in client values, beliefs, and attitudes.
• Oral health status goals address the signs and symptoms of oral disease (e.g., risk for caries, gingivitis, dentinal hypersensitivity) and reflect a desired health outcome achievable through dental hygiene interventions.
Knowledge and skill development may not result in client adherence to self-care and the resolution of an oral health condition. The client must internalize the desire and make modifications in behavior; therefore a variety of goals are necessary to achieve a positive oral health outcome.
Writing Client-Centered Goals
Adopting a format for writing client-centered goals simplifies the task (Box 22-3). Each client-centered goal should have a subject, a verb, a criterion for measurement, and a time dimension for evaluation:
• The subject is the client or client's caregiver.
• The verb is the client action desired to achieve the desired outcome; it is not the action of the dental hygienist.
• The criterion is the observable behavior or desired tangible outcome.
• Time dimension denotes when the client is to have achieved a goal. This target time may be a specific date or a statement (e.g., by next appointment, by the evaluation appointment, by end of treatment, or by next recare). Assigning a time frame to each client goal gives the client and the clinician a point of reference. Clients need time to do the following:
Goals evaluated too early restrict the clinician's and the client's ability to determine the impact of the care provided. At least one goal should be established for each dental hygiene diagnosis (Table 22-3).
TABLE 22-3
Sample Dental Hygiene Diagnoses with Related Client-Centered Goals
| Dental Hygiene Diagnosis | Goals |
| Unmet human need for protection from health risk is due to blood pressure elevated above normal limits as evidenced by a reading of 160/100 mm Hg. | Client will report having blood pressure evaluated by physician before rescheduled visit on 10/5. |
| Unmet human need in wholesome facial image is due to use of chew tobacco as evidenced by client dissatisfaction with stained teeth. | Client will complete successfully a formal program for chew tobacco cessation by 12/30. |
| Unmet human need for skin and mucous membrane integrity of the head and neck is due to generalized subgingival biofilm accumulation in 4-mm pockets as evidenced by generalized gingival bleeding. | Client will exhibit a gingival bleeding score of no more than 2 by 6/15. |
Involving the Client
Client goals are best established by the dental hygienist in collaboration with the client. Too often, individuals receiving care are referred to as “the Class II cavity preparation in treatment room 2” or “the advanced periodontal case at 4 pm.” These phrases communicate insensitivity to the individual, who is central in care. The dental hygienist who views the person as the focus of attention is more likely to establish a collaborative, co-therapeutic relationship with the client. This philosophy of care sets the stage for active client participation in identifying needs, readiness to change, priorities, goals, and interventions. Clients encouraged to participate in the process of care are more likely to communicate their wants, needs, and expectations than to relinquish decision making about their care to the dental hygienist. Individuals are more likely to express commitment to a care plan and their willingness to change if they shared in the development of goals, priorities, interventions, and appointment planning (Box 22-4).
At times, specific goals are valued more highly by the dental hygienist than by the client. When this occurs, the dental hygienist explains the professional judgment and decision relative to the goal, with a clear message that the client's readiness to change, wants, and needs are equally important to the overall plan. In addition to improving compliance, respecting the client's autonomy as a co-therapist and partner in decision making is an effective risk management strategy for avoiding legal problems.
Selecting Dental Hygiene Interventions
Dental hygiene interventions are the evidence-based strategies, products, and procedures that, if applied, reduce, eliminate, or prevent the oral health problem.1 Interventions, like client-centered goals, are linked to the dental hygiene diagnosis. However, interventions address the factors contributing to the client's human need deficit. For example, various factors may contribute to a client's unmet need for a biologically sound and functional dentition, including but not limited to the following:
• Lack of knowledge about dental caries process or its infectious, chronic nature
• Lack of knowledge about self-care for dental caries prevention
• Skill deficit in oral self-care
• Inadequate financial resources
Therefore not every client with a risk for dental caries is cared for in the same way. For dental hygiene care to achieve the desired outcomes, evidence-based interventions must address specifically the factors contributing to the client's unmet human need. For example, a dental hygiene intervention strategy for a caries risk contributor of “reduced salivary flow from medication” may include an oral self-care recommendation for incorporating a daily salivary substitute product or educating the client on the role of saliva in the caries process. Evidence-based interventions enable the clinician and client to achieve the proposed client-centered goals and resolve the client's unmet human need. Therefore professional dental hygiene care involves the careful tailoring of interventions to meet unique client needs, as directed by the dental hygiene diagnosis.
Appointment Schedule
Once the interventions have been decided, they must be put into action at planned appointments. The appointment schedule becomes a guide for implementing the proposed interventions and specifies the following:
Number of visits and sequencing of interventions at appointments vary among clinicians and clients. The following are considered when an appointment schedule is planned:
• Time needed for each intervention (e.g., self-care education, pain management)
• Logic of grouping interrelated procedures
• Status and severity of unmet human needs
• Client's tolerance for long sessions
• Client's scheduling requirements (e.g., early morning only, time limitations)
When unmet client needs and proposed care plan goals are easily attainable, the related interventions may be implemented in one visit. When diagnoses, client goals, and interventions are complex, multiple appointments are necessary.
Scheduling time for educational interventions and the sequencing of self-care strategies must be given consideration during appointment planning. Too often client education is squeezed in at the end of an appointment as time permits. Effectively addressing the client's cognitive, psychomotor, and affective needs influences oral health outcomes and the client's long-term adherence to self-care. Sequencing small increments of instruction into each visit may shape successfully the client's self-care responsibilities. For example, multiple appointment care plans may spread client education over several visits to include time to review and reinforce previously introduced self-care behaviors. Box 22-5 suggests strategies for planning client self-care.
Care Plan Presentation
Before presenting the care plan to the client, the dental hygienist assesses the plan comprehensiveness by answering the following questions:
• Does the care plan address the client's unmet human needs relative to oral health that are amenable to or affect the outcomes of dental hygiene care?
• What are the client's cultural beliefs and behaviors?
• What might the client's response be to the care plan (e.g., interest, commitment, worry, fear, discontent, lack of enthusiasm)?
• How should the care plan be presented to elicit client cooperation?
• How can client involvement be maximized?
• What is the dental hygienist's response if the client refuses care?
When the dental hygienist is satisfied with the completeness of the dental hygiene care plan, the plan is discussed with the client. The dental hygienist must explain all aspects of the care plan and involve the client in the discussion. Presentation and discussion of the dental hygiene care plan will include the following:
Once agreed on in writing by the client, the care plan becomes a legal contract between the dental hygienist and the client.
By using the EHR and digital images during the care plan presentation, the dental hygienist can strengthen a client's understanding and acceptance of the diagnosed condition and the proposed care plan. Digital images of the client's oral assessment findings (e.g., digital radiographs, dental and periodontal chart, intraoral photographs) can be displayed on a screen and used to provide the client with visual evidence of the condition and factors contributing to the condition. In addition, interactive educational software that is linked to the EHR can be used to familiarize the client with proposed treatment strategies or expected treatment outcomes as well as demonstrate the progression of an untreated condition. The dental hygienist and client can interact with these images to ensure that the client understands the nature of the condition and the proposed care plan. If the care plan is to achieve the desired outcome, the clinician and the client must support it. Therefore enhancing a client's self-awareness of the impact of his or her condition and the proposed treatment outcomes may improve the client's acceptance of the care plan including adherence to self-care recommendations.
Most consumers expect to participate in decision making regarding their healthcare needs and know they have the right to accept or refuse services. Therefore the care plan is presented to the client before preventive and therapeutic dental hygiene services are implemented. Failure to discuss the care plan with the client can result in services being performed without the client's knowledge or informed consent. Also, the client may not recognize the importance of self-care or may have unrealistic care expectations.
Informed Consent
The process of informed consent is the client's acceptance of care after a discussion with the healthcare provider regarding the proposed care plan and risks of not receiving care (Figure 22-4). Informed consent should not be viewed as a one-time activity but as an ongoing process in which the client is informed continuously and reminded of the terms of care. For informed consent to be achieved, the client must be knowledgeable about what the healthcare provider plans to do, have enough information to make a rational choice, and give permission for the plan to be carried out. The client must give consent

• For a procedure that is legal
• Under truthful conditions (e.g., the consent cannot be obtained through fraud, deceit, misrepresentation, or trickery)
In addition to the client being informed, the client must be legally competent to give consent for care. For example, in the case of a minor, consent must be given by the parent or legal guardian (healthcare decision maker). Although implied consent is given when a client voluntarily comes to the oral care setting and sits in the dental chair, this consent applies only to the assessment, diagnosis, and planning components of the dental hygiene process of care. The dental hygienist cannot assume that the client consents to any further care. The client's consent must be obtained for additional services to be implemented and is best documented in writing. Therefore having an automated informed consent document linked to the dental hygiene care plan ensures that this step will not be overlooked. The client's written consent is secured by having the client sign an electronic signature pad that transfers the signature to the informed consent document. This remains a permanent entry into the client's EHR.
Informed Refusal
Given all information necessary for a client to make an informed decision, the possibility exists that a client may decline all or part of the proposed care plan, such as in the following situations:
• Refusal of fluoride therapy, radiographs, or antimicrobial agents
• Noncompliance with referral to a dental specialist or physician
• Nonadherence to a specific oral self-care recommendation
• Decision to terminate care before goal attainment
• Refusal to give up a behavior that increases the risk of periodontal disease progression (e.g., tobacco use)
Although troubling, client refusal must be analyzed to determine how or why the client arrived at that decision. The clinician should engage the client in conversation, listen, and evaluate the client's reasons for declining the services. At this time the clinician may choose to reopen the discussion of treatment needs. If after this discussion the client makes an informed refusal, the clinician should have the client sign an electronic declaration of informed refusal that remains part of the client's EHR (Figure 22-5). A copy of the refusal form can be given or e-mailed to the client. Box 22-6 offers suggested client reasons for refusal of care, clinician actions, and documentation of informed refusal as a legal risk management strategy.

In some situations the client may request care that, in the opinion of the dentist or dental hygienist, is unwarranted, inappropriate, or dangerous. If the dental hygienist is faced with this dilemma, he or she should refuse to provide the care and should encourage the client to seek a second professional opinion. As a rule, the client never should be allowed to dictate treatment.
See Procedure 22-1 and corresponding Competency Form for steps for dental hygiene planning.
Evaluation
Goal of Evaluation
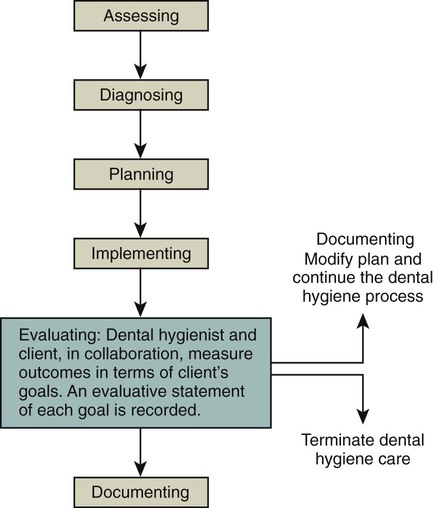
The evaluation goal in the process of care is to document success of the care plan intervention strategies at achieving the proposed care plan goals, that is to say, fulfillment of the client's unmet human needs related to oral health and wellness (Figure 22-6). Evaluation is a critical component to the successful outcome of dental hygiene care. Specifically, evaluation allows the clinician to measure the short-term achievement of client-centered goals as well as to anticipate the client's long-term prognosis in maintaining the goals achieved.
The evaluation phase of the dental hygiene process is linked inherently to each phase of care. The foundation for formulating an evaluation strategy consists of the baseline signs and symptoms that support the dental hygiene diagnosis. Evaluation strategies are defined by the client-centered goals during the planning phase and applied during the care implementation phase, at the completion of the dental hygiene care planned, and at the subsequent continued-care visit to measure the client's continued success at maintaining the previously achieved outcome. The dental hygienist employs evaluation strategies for the following:
• Ongoing monitoring of client progress during care implementation
• Determining a dental hygiene prognosis and supportive continued cycle of care at termination of the care plan
• Determining continued oral health outcomes and formulating a supportive care plan at the continued-care appointment.
See Procedure 22-2 and corresponding Competency Form for steps for integrating evaluation into client-centered care.
Ongoing Monitoring
As the appointment schedule is put into action and the dental hygiene intervention strategies are implemented, the clinician continually measures client progress toward achieving the goals, or the desired outcomes. During the initial treatment appointment, the clinician implements evaluation strategies to measure the client's newly learned cognitive and psychomotor skills and adapts oral self-care strategies to guide the client's skill development. For example, when multiple treatment appointments are planned to complete phase I nonsurgical therapy, the clinician continues to monitor (reassess) the client's progress towards goal attainment related to oral self-care behaviors, indicators of oral health and disease, and adherence to professional recommendations. At each dental hygiene care appointment, the dental hygienist shares with clients their progress towards achieving the desired care plan goals and reviews and reinforces recommended self-care strategies.
The dental hygienist and the client have an active role in evaluation. For example, a dental hygienist may have performed an intervention competently, but if the intervention or therapy was unsuccessful at helping the client achieve the desired goal, a new strategy must be considered. Therefore evaluation of a client's progress toward achieving a desired outcome is ongoing so that the clinician can do the following:
• Modify the care plan because the client is having difficulty in achieving the goal.
• Modify the care plan because the client is not ready to achieve the goal.
• Continue the care plan because the client needs more time to achieve the goal.
• Terminate the care plan because the client has achieved the goal.
Evaluation of Client-Centered Goals
Evaluation of client-centered goals determines whether dental hygiene care has achieved the client's unmet human need. Evaluation methods should reflect the intent of the goal statement (e.g., cognitive, psychomotor, affective, or oral health status). An evaluation strategy may be as follows:
• Asking the client open-ended questions to measure acquisition of new knowledge (cognitive)
• Having the client demonstrate a newly learned interdental cleaning technique (psychomotor)
• Having the client report increased motivation to stop smoking by attempting to smoke fewer cigarettes per day (affective)
• Showing the client clinical improvements in oral health, such as decreased probing depth and bleeding points (oral health status)
Each client-centered goal is evaluated to determine the degree to which it has been achieved (Figure 22-7). Based on the new findings the dental hygienist determines one of the following outcomes:

A written evaluative statement includes the dental hygienist's decision on the degree to which the goal was achieved and concrete evidence that supports the decision. This evaluation statement is recorded in the client's permanent record and signed and dated by the dental hygienist. Samples of evaluative statements as they relate to a dental hygiene diagnosis and client goal are displayed in Table 22-4.
TABLE 22-4
Sample of Evaluative Statements as Related to the Dental Hygiene Diagnosis and Client-Centered Goal Statements
| Dental Hygiene Diagnosis | Goal Statement | Evaluative Statement |
| Unmet human need for responsibility for oral health is due to impaired physical ability as evidenced by a plaque-free index score of 30%. | Client will use a manual toothbrush modified with an enlarged, elongated handle at least once daily by 11/1. Client will increase plaque-free index score to 80 by 11/1. |
11/1 Goals met. Client reported using modified toothbrush twice daily, and plaque-free index has increased to 85%. |
| Unmet human need for wholesome facial image is due to wearing a denture and halitosis as evidenced by client's concern with appearance of dentures, and client states that spouse complains she has frequent bad breath. | Client will meet at least two other individuals who successfully wear dentures by 12/1. Client will clean dentures, tongue, and oral cavity with appropriate brushes and dentifrice by 11/25. Client will use an ADA-accepted antimicrobial mouth rinse twice daily for 30 seconds by 11/25. |
12/5 Goal partially met. Client met one person who successfully wears dentures and verbalized that the dentures looked natural. 11/25 Goal met. Client reported cleaning and rinsing mouth twice daily as directed and that spouse no longer complains about her bad breath. |
| Unmet human need for conceptualization and problem solving is due to a knowledge deficit about the periodontal disease process as evidenced by bleeding on probing and slight radiographic horizontal bone loss. | Client will verbalize the periodontal disease process and identify oral biofilm as a prime causative agent by 9/20. | 9/20 Goal met. Client can describe the role of oral biofilm and the periodontal disease process. |
| Unmet human need for biologically sound dentition is due to infrequent dental visits as evidenced by signs of four carious lesions. | Client will follow up on a referral made to the dentist of record and have the four carious lesions diagnosed and restored by 8/1. | 8/15 Goal not met. Client canceled dental appointment. |
| Unmet human need for skin and mucous membrane integrity of the head and neck is due to inadequate self-care as evidenced by gingival bleeding. | Client will eliminate bleeding upon probing by 5/8. | 5/10 Goal met. Client no longer shows clinical signs of gingival bleeding. |
Failure to evaluate the client's status after care leaves the clinician unaware of the impact that the care may or may not have had. From a legal perspective, failure to evaluate the outcome of care may be grounds for negligence (malpractice).8 Unknown to the clinician and the client, the client's oral health knowledge, behaviors, oral health status, or values still may be contributing to an oral health deficit. The dental hygienist demonstrates professional practice by completing the cycle of care by measuring the extent to which client goals have been achieved and recommending continued care based on the evaluation outcomes.
Factors Influencing Client Goal Attainment
Client, dental hygienist, and clinical environment characteristics interact to enhance or hinder client goal attainment. The astute dental hygienist identifies positive and negative factors that may affect goal attainment. To facilitate the desired oral health outcome, positive factors are reinforced and negative factors managed.
Positive factors include the following:
• A client who values oral health, is motivated, and has a sense of inquiry
• A dental hygienist who maintains an evidence-based practice
• A work environment that values high-quality healthcare and offers incentives for care that meet or exceed recognized standards of practice
Table 22-5 presents common variables that can detract from quality of care. Possible dental hygiene responses are presented to initiate thinking about overcoming factors that impede goal attainment.
TABLE 22-5
Factors That May Detract from the Quality of Dental Hygiene Care
| Factors | Possible Dental Hygiene Action |
| Client Variables | |
| Client who refuses to cooperate with therapeutic regimen | Determine underlying reason for observed behavior and client readiness to change; consider possible socioethnocultural factors. |
| Counsel and educate appropriately. | |
| Client who rarely communicates needs | Encourage client to ask questions. |
| Be nondirective in the educational approach. | |
| Involve primary caregiver, family, or interpreter in communication process. | |
| Dental Hygiene Variables | |
| Dental hygienist who gives 200% of self when others do not | Learn to leave work on time, avoid assuming work of others, leave work-related concerns at the workplace. |
| Resolve work-related problems positively; seek strategies that improve motivation and morale of colleagues and self. | |
| View problems as challenges rather than insurmountable obstacles. | |
| Develop a realistic sense of what can be accomplished in amount of time given. | |
| When resources do not permit high-quality care and strategies do not result in positive change, explore other employment options. | |
| Dental hygienist is bored | Seek avenues for growth and development; participate in staff development and continuing education; identify a project and become involved; initiate strategies that result in positive change. |
| Evaluate long-term career goals; seek advanced degrees. | |
| Participate in professional associations. | |
| Search for new position. | |
| Dental hygienist is under stress from outside concerns (e.g., illness or death of significant others; marriage, childbirth, divorce, separation; role conflict as professional, parent, spouse; significant life changes) | Evaluate whether this is the exception or the rule. |
| Assess whether work performance is less than optimal. | |
| May need to reduce work hours rather than “cheat” clients. | |
| Seek counseling. | |
| Environmental Variables | |
| Inadequate supplies and equipment | Document problems with supplies and equipment. |
| Identify specific supply and equipment needs and discuss with employer. | |
| Inadequate time allotted to provide high-quality care | Identify and record type of dental hygiene care required. |
| Relate client needs and outcomes to level of care provided. | |
| Document how more time can improve client outcomes. | |
| Discuss with employer. | |
| Inadequate respect, recognition, and reward from employer | Document incidents when respect, recognition, or reward were withheld. |
| Talk with employer about specific incidents. | |
| Give employer suggestions on how situation can be improved. | |
| Search for new position. | |
| Initiate new policies, procedures, and training in the workplace. | |
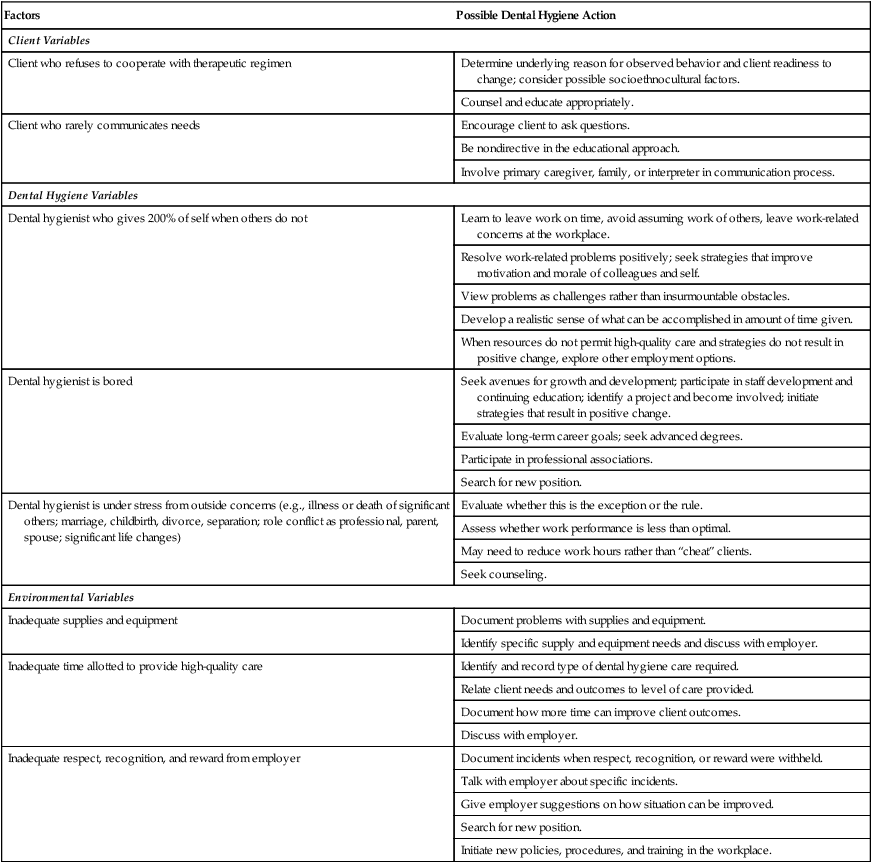
Adapted from Taylor C, Lillis C, LeMone P, Lynn P: Fundamentals of nursing, ed 7, Philadelphia, 2011, Lippincott Williams and Wilkins.
Modifying or Terminating the Care Plan
When evaluation reveals that the client has made little progress toward goal attainment (i.e., goal partially met or goal not met), the dental hygienist reassesses the client's readiness to change, attitudes, beliefs, and practices, and new findings are discussed with the dentist. These evaluation findings may lead to new diagnoses, revised goals, and alternative interventions. Client reassessment identifies barriers that continue to contribute to the client's unmet human needs, such as the following:
• Improperly developed client goals; goals that, if achieved, do not guarantee problem resolution
• Unrealistic goals for the client to achieve; immeasurable goals
• Care plan that does not specifically address the client's goals and unique socioethnocultural characteristics; plan contains only general information
Once it is clear why the client has failed to achieve goals, the evaluative statement can be used to redirect the care plan.
When client goals have been met and no new problems identified, the dental hygienist and client have achieved the outcome of care. The care plan is terminated, and responsibility for continued oral health falls on the individual. Written and verbal instructions are given to the client to take home, and signs and symptoms of any possible future problems should be understood clearly by the client.
Dental Hygiene Prognosis and Continued Care
At the termination of the dental hygiene care plan, a new process-of-care cycle is recommended to the client for continued care. A continued-care interval that will support the client's efforts to maintain the oral health status achieved during active therapy is determined. The dental hygienist determines the cycle of periodic reassessment and continued care from the client's prognosis.
The dental hygiene prognosis is contingent on the following:
• Overall appraisal of the evaluative statements
A favorable prognosis occurs when risk for a new disease or recurrence of the previous conditions is low. A prognosis is guarded when risk for a new disease or recurrence of the previous condition is moderate to high.
Client-centered goals may be achieved successfully during active therapy; however, the prognosis may be guarded because of risk factors such as smoking or an uncontrolled systemic disease. Therefore the client and dental hygienist would select a frequent continued-care interval to monitor oral health. Periodically the continued-care plan is reviewed and adjusted to meet client needs. Continued-care appointments are scheduled at 2- to 12-month intervals based on client need.
Outcome at Continued-Care Visit
Each continued-care visit begins with reassessment of the client's human needs related to oral health to provide evidence of the long-term outcome of the previous care plan and need for supportive care. Determining outcomes at the continued-care visit is critical to ensuring that the client's continued success will be re-enforced and continued need deficits will be recognized and addressed. The goals of evaluation at the continued-care visit are as follows:
• Document client evidence of continued oral health from previous cycle of care.
• Identify a reoccurrence of an unmet need.
• Identify a new condition that may be present.
• Formulate a care plan that supports the client's continued needs.
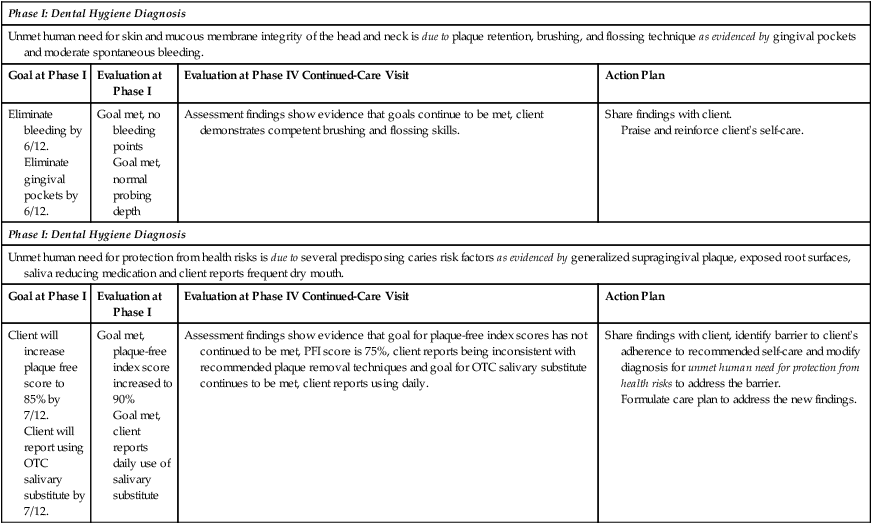
Therefore the reassessment findings are applied to the previous care plan goals and the outcome at continued care is the foundation for determining a dental hygiene diagnosis and care plan for the continued-care visit (Table 22-6).
TABLE 22-6
Sample of Evaluative Statements for Continued Health at Continued-Care Visit and Action Plan
| Phase I: Dental Hygiene Diagnosis | |||
| Unmet human need for skin and mucous membrane integrity of the head and neck is due to plaque retention, brushing, and flossing technique as evidenced by gingival pockets and moderate spontaneous bleeding. | |||
| Goal at Phase I | Evaluation at Phase I | Evaluation at Phase IV Continued-Care Visit | Action Plan |
| Eliminate bleeding by 6/12. Eliminate gingival pockets by 6/12. |
Goal met, no bleeding points Goal met, normal probing depth |
Assessment findings show evidence that goals continue to be met, client demonstrates competent brushing and flossing skills. | Share findings with client. Praise and reinforce client's self-care. |
| Phase I: Dental Hygiene Diagnosis | |||
| Unmet human need for protection from health risks is due to several predisposing caries risk factors as evidenced by generalized supragingival plaque, exposed root surfaces, saliva reducing medication and client reports frequent dry mouth. | |||
| Goal at Phase I | Evaluation at Phase I | Evaluation at Phase IV Continued-Care Visit | Action Plan |
| Client will increase plaque free score to 85% by 7/12. Client will report using OTC salivary substitute by 7/12. |
Goal met, plaque-free index score increased to 90% Goal met, client reports daily use of salivary substitute |
Assessment findings show evidence that goal for plaque-free index scores has not continued to be met, PFI score is 75%, client reports being inconsistent with recommended plaque removal techniques and goal for OTC salivary substitute continues to be met, client reports using daily. | Share findings with client, identify barrier to client's adherence to recommended self-care and modify diagnosis for unmet human need for protection from health risks to address the barrier. Formulate care plan to address the new findings. |
Failure to evaluate a client's progress at each subsequent continued-care visit can lead to what has been referred to as supervised neglect. Supervised neglect occurs when the client continues to require further dental hygiene care to achieve higher levels of oral wellness or to prevent or control oral disease progression, yet the client has been discharged erroneously from care, thinking that a healthy state was achieved. Supervised neglect can occur in practices that have a service-oriented approach to client care rather than a client-centered approach. A service-oriented practice applies the same series of services, appointment time, and continued-care recommendations to all clients. The emphasis is on completing the mechanics of a procedure, without considering the needs of the client, risk factors, and the influences of care on the client's health status. In contrast, the dental hygiene process of care supports a client-centered approach, in which the focus is the client and satisfying the client's unmet human needs related to oral disease prevention and health promotion. Integrating evaluation into the process of care demonstrates the dental hygienists' commitment to achievement of the desired client outcomes. Evaluation provides assurance that unmet needs are not overlooked or neglected.
Documentation
Documentation is the complete and accurate recording of all collected data, care planned and provided, recommendations, and other information relevant to client care. The dental hygienist documents all other components of the dental hygiene process of care (i.e., assessment, dental hygiene diagnosis, planning, implementation, and evaluation). This documentation involves objective, accurate, concise, and legible recording of all information and interactions between the client and the dental hygienist (i.e., telephone calls, emergencies, prescriptions, including dates and signatures) to ensure that subsequent providers can understand all clinical information relevant to the client of record.
The processes of informed consent and informed refusal relate to the client's acceptance or rejection of care after a discussion with the healthcare provider regarding the proposed care plan and risks of not receiving care. The client's consent or refusal must be documented in the client's permanent health record.
A legal risk management strategy is to document evidence of the process of care in each client's permanent record.4,5 Documentation that demonstrates a relationship among assessment, diagnosis, client-centered care plan, implemented intervention strategies, and evaluative statements of outcomes is evidence that the services rendered reflected client needs. An EHR provides the aforementioned evidence of a client-centered process of care. Documentation of each component of the process of care in the client's EHR is the best defense against a client's accusation of negligence (Figure 22-8).
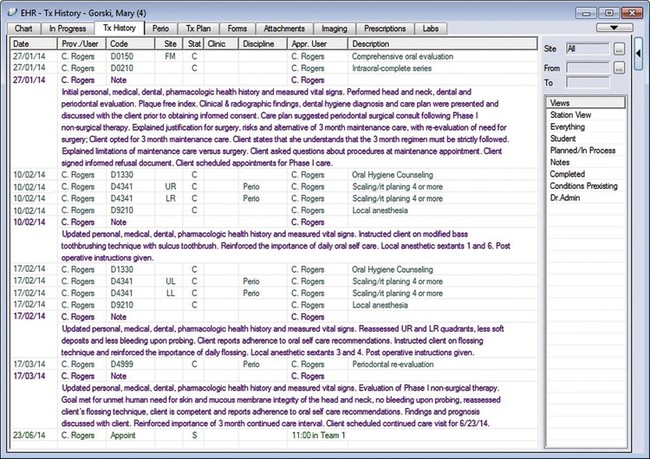
Documentation of services rendered represents a legal record of all services performed for the client. Services rendered should be recorded in the client's EHR at the time they are performed. The method of documenting the services rendered may include electronically entering a corresponding dental procedure code or a customized electronic note and supplementing the entry with a typed narrative describing relevant events of client care. Dental procedure codes denote standardized assessment and treatment codes used by the dental profession to indicate services rendered as defined by the American Dental Association (ADA) Current Dental Terminology (CDT).6 A customized electronic note is designed specially by an institution to document a frequently used entry to a client's EHR.
All entries must be accurate and factual and provide enough detail to describe how the client progressed through each phase of care to attain the proposed desired outcome. The services rendered and the client's response to those services should be documented by the clinician who performed the services, signed, and dated. The clinician signature may be entered into the EHR by using a signature pad. If an error in documentation is identified after storage, the clinician may correct the error by marking the entry as a mistaken entry and entering the correct information.7 The new entry must be dated and initialed by the clinician.
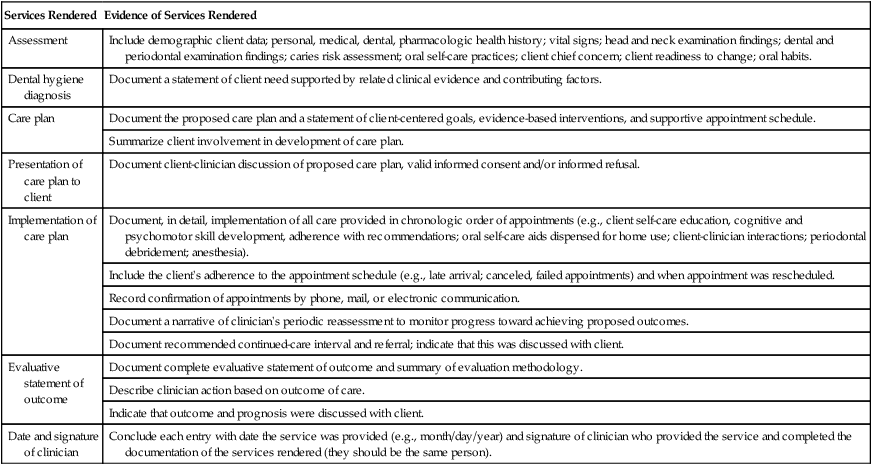
Table 22-7 suggests guidelines for documentation of care planning and evaluation in the client's EHR under “Services Rendered.”
TABLE 22-7
Guidelines for Documenting Planning and Evaluation in Client Electronic Health Record
| Services Rendered | Evidence of Services Rendered |
| Assessment | Include demographic client data; personal, medical, dental, pharmacologic health history; vital signs; head and neck examination findings; dental and periodontal examination findings; caries risk assessment; oral self-care practices; client chief concern; client readiness to change; oral habits. |
| Dental hygiene diagnosis | Document a statement of client need supported by related clinical evidence and contributing factors. |
| Care plan | Document the proposed care plan and a statement of client-centered goals, evidence-based interventions, and supportive appointment schedule. |
| Summarize client involvement in development of care plan. | |
| Presentation of care plan to client | Document client-clinician discussion of proposed care plan, valid informed consent and/or informed refusal. |
| Implementation of care plan | Document, in detail, implementation of all care provided in chronologic order of appointments (e.g., client self-care education, cognitive and psychomotor skill development, adherence with recommendations; oral self-care aids dispensed for home use; client-clinician interactions; periodontal debridement; anesthesia). |
| Include the client's adherence to the appointment schedule (e.g., late arrival; canceled, failed appointments) and when appointment was rescheduled. | |
| Record confirmation of appointments by phone, mail, or electronic communication. | |
| Document a narrative of clinician's periodic reassessment to monitor progress toward achieving proposed outcomes. | |
| Document recommended continued-care interval and referral; indicate that this was discussed with client. | |
| Evaluative statement of outcome | Document complete evaluative statement of outcome and summary of evaluation methodology. |
| Describe clinician action based on outcome of care. | |
| Indicate that outcome and prognosis were discussed with client. | |
| Date and signature of clinician | Conclude each entry with date the service was provided (e.g., month/day/year) and signature of clinician who provided the service and completed the documentation of the services rendered (they should be the same person). |
Scenarios 22-1 and 22-2 and care plans are provided as examples.
Additional scenarios can be found on the website for the following examples:
• Preliminary Phase: Emergency Care
• Phase I: Nonsurgical Therapy
See Procedure 22-3 and corresponding Competency Form for steps for evaluation of care.
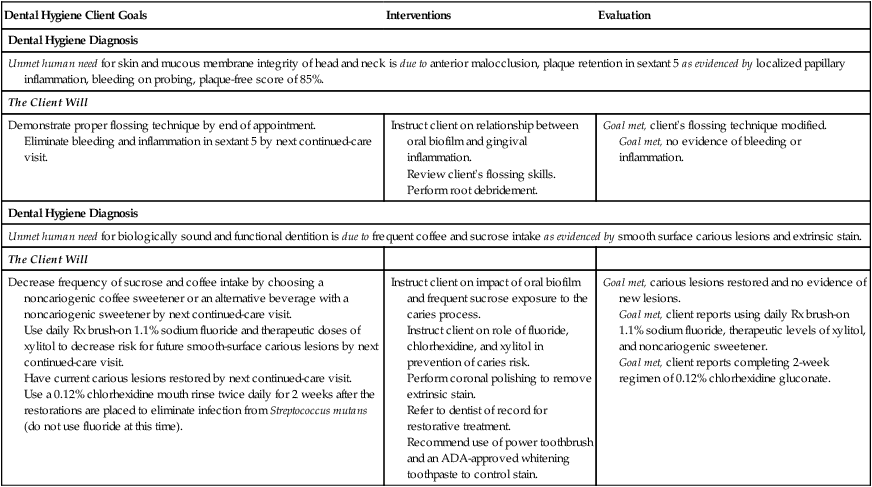
Scenario 22-1 Client with Plaque-Induced Gingivitis and Dental Caries and Sample Dental Hygiene Care Plan
Susie S., a healthy 19-year-old single woman without dental insurance, is a second-year student living at the local university. Her last preventive dental appointment was 3 years ago and included a prophylaxis and four bitewing radiographs. She brushes twice daily with fluoride toothpaste and flosses occasionally. Her chief complaint is, “I hate the brown stain on my teeth.”
Clinical assessment reveals soft tissues within normal limits, Class I malocclusion with a slight anterior overbite, and crowding in mandibular anteriors. Gingival evaluation indicates localized slight papillary inflammation, sulcus depths within 3 mm, no attachment loss, and slight bleeding on probing in sextant 5. Plaque-free index is 85%. Dental examination indicates that 30 teeth are present, including partially erupted third molars (No. 17/No. 32), extrinsic brown stain from coffee, and slight lingual and proximal calculus in sextant 5. No restorations are present; molars have pit-and-fissure sealants. Bitewing radiographs reveal Class II carious lesions on the mesial surface of teeth 2 and 15 and incipient carious lesions on the mesial surface of teeth 19 and 30. Susie reports that she drinks three to four cups of coffee with 2 teaspoons of sugar daily.
| Dental Hygiene Client Goals | Interventions | Evaluation |
| Dental Hygiene Diagnosis | ||
| Unmet human need for skin and mucous membrane integrity of head and neck is due to anterior malocclusion, plaque retention in sextant 5 as evidenced by localized papillary inflammation, bleeding on probing, plaque-free score of 85%. | ||
| The Client Will | ||
| Demonstrate proper flossing technique by end of appointment. Eliminate bleeding and inflammation in sextant 5 by next continued-care visit. |
Instruct client on relationship between oral biofilm and gingival inflammation. Review client's flossing skills. Perform root debridement. |
Goal met, client's flossing technique modified. Goal met, no evidence of bleeding or inflammation. |
| Dental Hygiene Diagnosis | ||
| Unmet human need for biologically sound and functional dentition is due to frequent coffee and sucrose intake as evidenced by smooth surface carious lesions and extrinsic stain. | ||
| The Client Will | ||
| Decrease frequency of sucrose and coffee intake by choosing a noncariogenic coffee sweetener or an alternative beverage with a noncariogenic sweetener by next continued-care visit. Use daily Rx brush-on 1.1% sodium fluoride and therapeutic doses of xylitol to decrease risk for future smooth-surface carious lesions by next continued-care visit. Have current carious lesions restored by next continued-care visit. Use a 0.12% chlorhexidine mouth rinse twice daily for 2 weeks after the restorations are placed to eliminate infection from Streptococcus mutans (do not use fluoride at this time). |
Instruct client on impact of oral biofilm and frequent sucrose exposure to the caries process. Instruct client on role of fluoride, chlorhexidine, and xylitol in prevention of caries risk. Perform coronal polishing to remove extrinsic stain. Refer to dentist of record for restorative treatment. Recommend use of power toothbrush and an ADA-approved whitening toothpaste to control stain. |
Goal met, carious lesions restored and no evidence of new lesions. Goal met, client reports using daily Rx brush-on 1.1% sodium fluoride, therapeutic levels of xylitol, and noncariogenic sweetener. Goal met, client reports completing 2-week regimen of 0.12% chlorhexidine gluconate. |
| CDT-2013 Dental Procedure Code | Appointment 1 (50 minutes) |
| D0150 | Initial personal, medical, dental, pharmacologic health history, measure vital signs; perform comprehensive oral assessment: head and neck, dental and periodontal; determine plaque-free or gingival index. |
| D0274 | Bitewing radiographs: four films. |
| Inform client of clinical findings, diagnosis, and recommended care plan; obtain informed consent (or informed refusal). | |
| D1330 | Oral self-care instruction: flossing. |
| Client education: oral biofilm and gingival health and caries process, benefits of daily fluoride to prevent smooth surface caries, benefits of a power toothbrush and whitening toothpaste. Use of chlorhexidine mouth rinse to eliminate source of caries infection. | |
| Discuss need to keep the chlorhexidine rinse and fluoride separate. | |
| D1110 | Adult prophylaxis: full-mouth debridement, coronal polishing with mild abrasive. |
| Continued-care interval: 6 months. |

Scenario 22-2 Client with Plaque-Induced Gingivitis Modified by Systemic Factors (Pregnancy-Associated Gingivitis) and Sample Dental Hygiene Care Plan
Renee B. is a 29-year-old married woman with a 5-year-old child. Renee, 8 months pregnant and in good health, is taking Pepcid at bedtime for heartburn. She reports that her pregnancy is becoming uncomfortable.
Her last oral prophylaxis was 6 months ago and included oral hygiene instruction. Full-mouth radiographs were taken 1 year ago, and findings were within normal limits. She brushes once daily and flosses sometimes. Her chief complaint is, “My gums are bleeding when I brush and I always have a bad taste in my mouth.”
Clinical examination reveals soft tissues within normal limits, Class I malocclusion, generalized moderate marginal gingival erythema and edema, moderately bulbous interdental papilla, spontaneous heavy bleeding on probing, and probing depths of 4 to 5 mm with no attachment loss evident. Plaque-free index is 75.8%. Generalized subgingival calculus can be felt with the explorer and probe; supragingival calculus is visible on the mandibular anterior lingual teeth and facial surface of the maxillary molars. Dental examination reveals 28 teeth present (third molars were previously extracted) and multiple Class I and II amalgam restorations.
| Dental Hygiene Client Goal | Interventions | Evaluation |
| Dental Hygiene Diagnosis | ||
| Unmet human need for conceptualization and problem solving is due to client's lack of knowledge about pathogenicity of oral biofilm as evidenced by the client's bleeding gums when brushing. | ||
| The Client Will | ||
| Explain composition of oral biofilm and impact on soft tissue and halitosis by 4/16. Verbalize how pregnancy can enhance gingivitis in the presence of oral biofilm by 4/16. |
Instruct client on composition of oral biofilm and impact on gingival tissues, tongue, and halitosis. Instruct client on how pregnancy can enhance the incidence of gingivitis and periodontal disease progression, and how premature birth and low birth weight babies are linked to oral inflammation. |
Goal met, client verbalized role of oral biofilm and effects on oral health. Goal met, client explained pregnancy-associated gingivitis and how oral inflammation may be linked to preterm birth. |
| Dental Hygiene Diagnosis | ||
| Unmet human need for wholesome facial image is due to plaque retention plus elevated hormone levels as evidenced by plaque-free index of 75.8%, gingivitis, and client's concern about bad taste in her mouth and bad breath. | ||
| The Client Will | ||
| Recognize the importance of daily management of oral biofilm for oral and systemic health by 4/26. Use an ADA-accepted antimicrobial mouth rinse twice daily to control oral biofilm and gingivitis by 4/26. Increase plaque-free index score to 90% by 4/26. |
Assist client in identifying plaque-retentive sites with bleeding points and disclosing agent. Instruct client on the value of using an ADA-accepted mouth rinse to help control plaque and gingivitis. |
Goal met, client reports daily flossing, mouth rinsing, and extended brushing time. Client also reports that the bad taste in her mouth is gone. Goal met, client increased plaque-free index score to 95%. |
| Dental Hygiene Diagnosis | ||
| Unmet human need for skin and mucous membrane integrity of the head and neck is due to plaque retention, infrequent flossing, and hormones associated with pregnancy as evidenced by gingival pockets, spontaneous bleeding. | ||
| The Client Will | ||
| Decrease bleeding by 80% by 5/10. Decrease probing depths by 1 mm by 5/10. |
Instruct client on modified Bass toothbrushing. Use sulcus toothbrush for the disruption of subgingival plaque biofilm. Instruct client on flossing to disrupt proximal bacterial plaque biofilm. Instruct client on use of an ADA-accepted antimicrobial dentifrice and mouth rinse to control plaque and gingivitis. Perform therapeutic periodontal debridement: one visit for quadrants 1 and 4; second visit for quadrants 2 and 3. Perform coronal polishing. |
Goal partially met, bleeding points decreased by 70%. Goal met, decreased gingival pockets by 1 mm. |
| Dental Hygiene Diagnosis | ||
| Unmet human need for protection from health risk is due to risk of orthostatic hypotension as evidenced by client report that her pregnancy is becoming uncomfortable in the eighth month. | ||
| The Client Will | ||
| Position client in semi-upright position (45-degree angle) to alleviate fetal pressure on vena cava. Give client a pillow placed under the right hip while she is in chair. | Goal met, client was asymptomatic of orthostatic hypotension during appointment. | |

| CDT-2013 Dental Procedure Code8 | Phase I: Nonsurgical Therapy Appointment 1 (1 hour)—4/16 |
| D0150 | Update personal, health, dental, pharmacologic health history; measure vital signs; perform comprehensive oral evaluation: head and neck, dental, and periodontal; determine plaque-free index. |
| Inform client of diagnosis and recommended care plan, including clinical findings, and obtain informed consent. | |
| D1330 | Oral self-care instruction: modified Bass toothbrushing technique. |
| Client education: oral biofilm, gingivitis, halitosis, hormone-influenced gingivitis. Instruct client on use of an ADA-accepted antimicrobial dentifrice and mouth rinse to control plaque and gingivitis. | |
| D4341 | Therapeutic periodontal debridement of quadrants 1 and 4. |
| Appointment 2 (1 hour)—4/26 | |
| Update health history and measure vital signs. Assess tissue response to self-care and periodontal debridement of quadrants 1 and 4, determine plaque-free index. | |
| D1330 | Self-care instruction: review toothbrushing if needed and instruct on flossing. |
| D4341 | Therapeutic periodontal debridement of quadrants 2 and 3. |
| Phase I: Evaluation of Response to Nonsurgical Therapy Appointment 3 (1 hour)—5/10 | |
| D4999* | Update health history and measure vital signs. Assess all quadrants for tissue response to self-care and periodontal debridement, determine plaque-free index. |
| D1330 | Review and reinforce oral self-care. |
| In preparation for new baby, dispense literature on preventive oral health for infants, vertical transmission of caries from mother to infant, early childhood caries. | |
| D1110 | Adult prophylaxis to remove residual calculus (if any) and extrinsic stain with mild abrasive. |
| Continued-care interval: 3 months. | |

*Indicates unspecified periodontal procedure, may be used to report a periodontal re-evaluation.7
Client Education Tips
• Explain the importance of developing a care plan.
• Explain how the dental hygiene care plan is integrated with the overall dental care plan.
• Incorporate client's chief complaint; readiness to change; goals, needs, preferences, and values into the care plan.
• Involve the client in the development of client-centered goals (augments commitment). Use electronic imaging technology and educational materials to enhance clients' awareness of unmet needs and their responsibility in achieving the desired care plan outcomes.
• Explain that clinical outcomes of care will be related to the original goals.
• Reinforce the dental hygienist and client partnership as co-therapists to achieve client-centered goals.
• Explain that the client's readiness to change, wants, and needs are essential to the overall success of the plan.
Legal, Ethical, and Safety Issues
Inherent in the process of care is the legal and ethical responsibility of healthcare providers to do the following:
• Complete a comprehensive assessment of client unmet needs.
• Formulate a diagnosis and care plan based on that assessment.
• Communicate the recommended care plan to the client.
• Secure informed consent before implementing the care plan.
• Monitor the client's progress toward achieving desired oral health outcomes.
• Evaluate the outcome of care.
• Recommend a continued-care schedule.
• Keep adequate client records that are legible, dated, and signed with the title of the individual making the entry.
• Document clinical and radiographic findings as evidence that the diagnosis and care plan are based on client needs.
• Provide evidence of medical consultation, when needed, and written response with information requested.
• Provide evidence of informed consent before implementation of care, signed and dated.
• Provide evidence of informed refusal when client refuses care or recommendations, signed and dated.
• Document self-care education, status of client compliance, failed or canceled appointments, postoperative instructions provided, modifications made in care plan and supportive facts, referrals, and continued-care schedule.
• Never release client record without written authorization from the client or court subpoena.
• Never share personal password or electronic signature with another member of the staff.7
• Recognize ethical and legal responsibilities of record keeping including guidelines outlined in state regulations and statutes.
• Ensure compliance with the federal Health Information Portability and Accountability Act (HIPAA).
• Respect and protect the confidentiality of client information displayed on an unattended monitor in your operatory.7
Key Concepts
• A dental hygiene care plan is an evidence-based, client-centered written proposal to meet the unmet human needs of a client that are related to oral health and within the scope of dental hygiene practice.
• The dental hygiene diagnosis provides the foundation for care plan development.
• The care plan reflects the dental hygiene diagnosis, client-centered goals, dental hygiene interventions, detailed appointment schedule, and expected outcomes.
• A well-formulated and executed care plan increases the likelihood of a positive outcome in the dental hygiene care process.
• Evaluation is a critical component of the dental hygiene process and a necessary step to document evidence of care plan success in achieving a desired outcome in the client's oral health status.
• Documentation of the dental hygiene process of care in the client's record is a management strategy to minimize the risk of litigation.
• Without evaluation, a dental hygienist's contribution to the oral health of the client is invisible and undervalued.
Critical Thinking Exercises
Client Profile 1
James W., a 50-year-old man, is a long-haul truck driver who is taking hydrochlorothiazide for hypertension, drinks two to three cups of coffee per day, and smokes one pack of cigarettes per day.
Dental History: James' last dental appointment was 1 month ago for extraction of tooth 2, which was periodontally involved; before this time, 10 years had passed since his last dental appointment. He brushes once daily with fluoride toothpaste, and his chief complaint is, “I have pain in the upper left molar region, and I do not want to lose any more teeth.”
Assessment: Clinical examination reveals nicotine stomatitis, Class II malocclusion with a moderate overbite, and a coated tongue. Dental examination reveals missing third molars and maxillary right second molar; generalized moderate brown stain; slight subgingival calculus; localized moderate supragingival calculus in sextant 5; and Class I and II amalgam restorations.
Gingival and periodontal assessment findings reveal generalized moderate marginal inflammation, generalized slight recession; localized moderate recession on facial surfaces of sextants 3 and 4; bleeding on probing; pocket depths of 3 to 5 mm with clinical attachment loss at 4 to 5 mm; Class II and III furcations and Class I mobility on teeth No. 14 and No. 15. Full-mouth periapical and vertical bitewing radiographs show evidence of a recurrent carious lesion on tooth 30 and root caries on the distal surface of tooth 14, generalized moderate horizontal bone loss in molar regions, and localized vertical bone loss on the distal surface of tooth 14.
1. Formulate a comprehensive dental hygiene care plan for this client.
2. Refer to Table 22-1 and identify the phase of care that is being planned and implemented for this client.
3. Discuss the client's likely prognosis after implementation of the dental hygiene care plan and propose a continued-care interval to support the client's needs.
Client Profile 2
Mrs. Wilton is a 57-year-old woman who has been married for 35 years. She cares for her two grandchildren, Dayne, age 2, and Katie, age 4, 3 days per week while the children's mother works.
Health History: Mrs. Wilton has type 2 diabetes, controlled by oral hypoglycemic medication and diet, and hypertension, controlled by Avapro. She sees her physician on a regular basis for her diabetes and hypertension.
Dental History: Mrs. Wilton has not seen a dentist in 7 years. She is a client of record at the local university dental hygiene clinic where she has been treated every 4 to 6 months for the past 4 years because she does not have dental insurance. At each past continued-care appointment, she has had generalized slight chronic periodontitis. Each past care plan has indicated the dental hygiene diagnosis: “Human need for skin and mucous membrane integrity of the head and neck due to inadequate oral biofilm management by the client and generalized moderate calculus as evidenced by generalized bleeding on probing.” The care plans have emphasized the same intervention strategies (i.e., modified Bass toothbrushing and flossing followed by a series of quadrant root debridement appointments). Appointment notes indicate that the client keeps her scheduled appointments and properly demonstrates recommended toothbrushing and flossing skills; however, she states she does not like to floss.
Supplemental Notes: Mrs. Wilton arrives today at the dental hygiene clinic for a scheduled continued-care visit. No changes have occurred in her health history; all medications are taken as prescribed; blood pressure is within normal limits. Assessment findings reveal no change in oral health status since the last continued-care appointment. Reason for her visit: “to have my teeth cleaned.”
1. Considering the dental hygiene process of care, what legal and ethical issues are present?
2. Discuss possible factors influencing why the client's oral health has not improved at each continued-care visit.
3. Suggest alternative dental hygiene diagnoses and formulate a dental hygiene care plan.
4. Role-play a clinician's presentation of the care plan to the client for informed consent.
5. Complete services rendered notes for this scenario that document evidence of the dental hygiene process of care including assessment, diagnosis, and care plan presentation for informed consent.