Psychosocial Influences on Health
Syed M. Ahmed, Paul J. Hershberger, Jeanne Parr Lemkau
▪ An overweight 11-year-old boy with abnormal lipids tells his family physician that his favorite activity is playing online video games.
▪ A middle-aged woman emphatically asserts that her blood pressure is elevated only when she has it taken in a medical setting.
▪ A single mother with a part-time job but no health insurance tells her doctor that she can only take medications that have low co-pays.
Psychosocial factors influence health. Assessing and treating patients in a manner that integrates psychosocial and biologic aspects of care is the essence of excellent family medicine and its greatest challenge. The following example is illustrative.
Mr. Ramirez is a 52-year-old man who lost his well-paying job as a software engineer several years ago. After 8 months of unemployment, he took a less satisfying job for less money. Mr. Ramirez has type II diabetes, diagnosed when he was 45 years old and well-controlled before he lost his job. He has taken diabetes education classes and can accurately describe what he must do to maintain good glucose control. Reluctantly, Mr. Ramirez acknowledges to his physician that he does not follow his diet as closely as he once did and more frequently eats fast food. He also misses the exercise facility at his former workplace and struggles with motivation to exercise. His marriage “isn't as good as it used to be,” and he reports decreased interest in sex. When the physician asks him about feelings of depression, Mr. Ramirez says that he never thought he was a weak person, but he just does not enjoy things as he once did. His physician summarizes the changes Mr. Ramirez has experienced in the past few years and acknowledges the emotional toll of such stress. She briefly describes how stress and depression make diabetes more difficult to control and how she and Mr. Ramirez can collaboratively work on strategies to improve his health and quality of life.
This case highlights the following three imperatives for providing care that is appropriately responsive to psychosocial issues:
1. The physician sees the person first, conceptualizing symptoms and behaviors in his social and psychological context and responding with sensitivity to the patient's experience and priorities.
2. The physician understands the interactive nature of multiple biopsychosocial variables and communicates this effectively to the patient.
3. The physician fosters a supportive and empathic physician–patient relationship to provide the foundation for gathering information and intervening effectively.
As the case illustrates, biomedical factors may be only a small part of what patients bring to their physicians. The biomedical model, based on the assumptions of mind–body dualism, biologic reductionism, and linear causality, has resulted in miraculous achievements of high-technology medicine, but primary care physicians who restrict their attention to purely medical considerations are of limited use to their patients. Nevertheless, the shift from a biomedical to a biopsychosocial paradigm has been a major challenge to modern medicine.
In 1977, psychiatrist George Engel proposed a biopsychosocial model that included social and psychological variables as crucial determinants of disease and illness. According to his new framework, the subsystems of the body interact to produce successively more complex biologic systems, which are simultaneously affected by social and psychological factors. The organism is thus conceptualized in terms of complex interacting systems of biologic, psychological, and social forces, and neither disease nor illness is seen as understandable only in terms of smaller and smaller biologic components. Engel (1980) believed that systemic interactions of biopsychosocial factors were relevant to all disease processes and to the individual's experience of illness. Accordingly, understanding a person's response to a disease requires consideration of such interacting factors as the social and cultural environment, the individual's psychological resources, and the biochemistry and genetics of the disorder in the population (Brody, 1999).
In the following section, we present a number of conceptual models and perspectives that emphasize different but overlapping psychosocial dimensions that influence health (Table 3-1). These models can aid practicing physicians in thinking about their patients in psychosocial context and conceptualizing potentially helpful interventions. Subsequently, we elaborate on practical strategies for gathering and using psychosocial information in clinical practice and discuss a pragmatic approach to addressing psychosocial considerations in primary care. We conclude with brief discussions of evidence-based practice and how current challenges and trends in the health care system may affect the practice of family medicine.

Conceptual Models
The Biopsychosocial Model
As previously noted, the biopsychosocial model was proposed as a scientific paradigm by Engel (1977), who encouraged the clinician to observe biochemical and morphologic changes in relation to a patient's emotional patterns, life goals, attitudes toward illness, and social environment. Engel proposed that the brain and peripheral organs were linked in complex, mutually adjusting relationships, affected by changes in social as well as physical stimuli. Within this model, environmental and psychological stress is seen as potentially pathogenic for the individual. Emotions may serve as the organism's bridge between the meaning (or significance) of stressful events and the changes in physiologic function (Zegans, 1983). Engel urged physicians to evaluate the patient on biologic, psychological, and social factors to understand and manage clinical problems effectively (Wise, 1997). For example, a workplace accident could be seen as resulting from poorly designed equipment (social) and inattentiveness (psychological) brought about by low blood sugar (biologic). Similarly, the accident could result in damage to internal organs (biologic), distress (psychological), and lost income (social), any or all of which may become the focus of physician intervention.
Comprehensive evaluation of biopsychosocial dimensions would assess the following:
▪ Biologic factors, including genetics, medical history, and environmental factors that affect physiologic functioning (e.g., those causing cancer)
▪ Psychological factors, including affective, cognitive, and behavioral components, such as feelings, beliefs, expectations, personality, coping style, and health behaviors (e.g., exercise, diet, smoking) that contribute to patients' experience of health and illness
▪ Social factors, including access to health care, quality of available health care, social systems (e.g., family, school, work, church, government), social values, customs, and social support
Further discussion of biologic influences on health is beyond the scope of this chapter. Psychological and social factors known to affect health are discussed next.
Psychological Factors
Numerous psychological factors affect health. We discuss here a common approach to personality, the five-factor model, and an essential psychological resource for healthy behavior, self-control. We also review key findings from the literature on the relationship between emotions and health.
The most prominent approach to personality at present is the five-factor model (Goldberg, 1993). The five broad personality domains of this model, for which OCEAN is an acronym, are openness to experience, conscientiousness, extraversion, agreeableness, and neuroticism (Table 3-2). Research on the relationship of these factors to health variables has generated several findings. Whereas conscientiousness has been associated with longevity among healthy individuals and better functional status in those with physical illnesses or impairments, neuroticism is consistently found to be negatively correlated with health (Bogg and Roberts, 2013; Goodwin and Friedman, 2006; Smith and Mackenzie, 2006). Agreeableness, extraversion, and openness to experience generally tend to have weaker associations with health.
Table 3-2
Five-Factor Model of Personality

Because personality style tends to be quite stable across the life span, physician focus on changing personality for health reasons is not a sensible pursuit. However, an understanding of a particular patient's personality can help guide the physician toward interventions that are more likely to be effective.
Because health behaviors are a major factor in the development of, management of, and morbidity from chronic illnesses, self-control or willpower is a critical psychological resource. Children with more self-control have been found to have better health as adults. Adults with more self-control have healthier behaviors. Research indicates that willpower operates like a muscle; it is a resource that people have in limited supply, and it can be exhausted (Baumeister and Tierney, 2011). Fortunately, it can also be replenished. Importantly, various demands for willpower draw from the same common resource. Willpower is used to control thoughts, regulate emotions, manage impulses (the task most commonly associated with willpower), and direct performance. Making decisions uses willpower. Numerous studies have demonstrated that tasks requiring willpower deplete the self-control resource, so that performance declines on subsequent tasks requiring willpower. Interestingly, when there are competing demands for the self-control resource, managing negative emotions predictably takes precedence over other demands. Given the multiple emotional and behavioral challenges associated with the management of chronic illness, a patient with excessive demands on the limited self-control resource is particularly vulnerable to worsening health. See Table 3-3 for a summary of key factors about self-control, including how it can be replenished.
Table 3-3
Self-Control
The ongoing experience of chronic negative emotions (depression, anxiety, and anger) tends to be associated with poorer health. There is an extensive research literature linking negative affectivity and pessimism to adverse health outcomes (Peterson et al., 1988; Salovey et al., 2000). Although the experience of negative emotions is a natural part of the human experience, effective management of such emotions through cognitive strategies, active coping, and social support can be learned, and medications can be a helpful adjunct when negative emotional states are prolonged or severe.
Likewise, a large body of research indicates that positive emotional states are associated with better health and longevity. Happiness, optimism, and positive attitudes toward aging have been associated with 7 more years of life (Danner et al., 2001; Levy et al., 2002). Almost three decades of research have shown that an optimistic outlook has a positive effect on coping and on mental and physical health outcomes (Peterson and Steen, 2002). Family physicians have long recognized the importance of mobilizing and maintaining patient hopefulness through encouraging words that foster positive expectations of medical treatment. The demonstrated efficacy of placebos affirms the importance of this approach (Sobel, 1991).
Social Factors
A gradient between socioeconomic status (SES) and health is consistently found in epidemiologic studies (Marmot, 2004). Persons with less education and income tend to have poorer health than their better educated and richer counterparts. A recent analysis indicates that in the year 2000 in the United States, 245,000 deaths could be attributed to low education, 176,000 to racial segregation, 162,000 to low social support, and 133,000 to poverty (Galea et al., 2011). Interestingly, subjective SES (i.e., individuals' perceptions of where they view themselves on the social ladder) has an even stronger relationship to health than objective SES (Singh-Manoux et al., 2005). Negative affect, stress, pessimism, and a decreased sense of control are among the factors thought to contribute to the relationship between lower subjective SES and poorer health (Operario et al., 2004).
In general, social support reduces stress and contributes to more positive health outcomes. Social support refers to the process by which a social network provides psychological and material resources to enhance an individual's ability to cope with stress (Cohen, 2004). Both quantity and quality of support are important, and sources of support include spouses, lovers, friends, family, coworkers, and health care professionals. A person who has many friends but no confidant may have inadequate social support in a time of need. Some people report high levels of satisfaction with just a few close friends, but others require larger social networks.
There are several varieties of social support (Cohen, 2004). Emotional support involves the expression of caring, concern, and empathy toward the person and typically involves opportunities for the recipient to express emotions. Instrumental support involves providing some type of direct assistance, which might include financial resources, transportation, or help with daily tasks. Informational support involves giving advice or information relevant to an individual's situation.
Social support appears to undergird health by buffering the person against negative effects of stress, perhaps by affecting the cognitive appraisal of stress. When people encounter a strong stressor, such as a major financial crisis, individuals with high levels of social support may appraise the situation as less stressful than will those with low levels of support. Social support may further buffer the stress by modifying people's response to a stressor as they turn to friends for advice, reassurance, or material aid. Social integration, or participating in a broad range of social relationships, benefits health and well-being by enhancing self-esteem and fostering positive health behaviors in people who believe that others count on them. Social integration is beneficial, whether or not an individual is experiencing stress (Cohen, 2004).
Relationships also can involve significant negative social exchange and be harmful to health; negative interactions in troubled marriages have adverse effects on cardiovascular, endocrine, and immune system function (Robles and Kiecolt-Glaser, 2003). Recent research has found specific links between negativity in relationships and cellular aging, such as shortening telomere length (Uchino et al., 2012).
Misconceptions
Polan (1993) identified and addressed two common misconceptions about the biopsychosocial model. First, contrary to popular belief, a physician who is “humanistic” is not necessarily practicing biopsychosocial medicine. A physician can be ethical and caring but still neglect scientific knowledge from the social and behavioral sciences and relevant data from the patient's life. For example, compassion by itself is of limited usefulness to a physician who needs an effective treatment plan for a patient with asthma who smokes. Interventions should be informed by knowledge of the social environment and the individual psychology of the patient.
The second misconception is that people can be reduced to distinct biologic, psychological, and social categories or that their problems can then be expressed as a set of scientific principles from which diagnosis and treatment can be neatly derived. In fact, use of the biopsychosocial model increases rather than decreases the level of complexity required to understand patient status, introducing multiple avenues for intervention. Interpreting the biopsychosocial model as a new opportunity for reductionist thinking diminishes its power to inform more holistic treatment. Borrell-Carrio and colleagues (2004) proposed a biopsychosocially oriented clinical practice based on self-awareness, active cultivation of trust, an emotional style characterized by empathic curiosity, self-calibration to reduce bias, cultivation of emotional sensitivity to assist with diagnosis and therapeutic relationships, use of informed intuition, and communication of clinical evidence to foster dialogue.
Another important misconception is that educating patients about important biologic, psychological, social, or environmental factors will necessarily change behavior. Much of human behavior is automatic, cued by environmental or situational factors. Health behaviors are frequently less a product of thoughtful choices than of nonconscious factors (Sheeran et al., 2013). Although intention and motivation affect adherence to treatment regimens and health behavior recommendations, multiple other factors (e.g., depletion of self-control, media and peer influences, physical environment) play important roles.
The Systems Approach
Humans are infinitely complex. Adequately conceptualizing a person in health or illness requires a systems approach that encompasses this complexity. The concept of systems was first developed by von Bertalanffy (1968) to refer to the dynamic interrelationships of various components. A systems approach rejects the notion of linear causality in favor of multidimensional and multidirectional models.
The systems approach has strongly influenced conceptualizations of family functioning. Smilkstein (1978) developed one of the first applications of “family systems” thinking for family medicine. Physician attention is important in the systemic interactions of family members and the impact of crisis, coping styles, and resources on family functioning. He incorporated these components into the “family APGAR” (adaptation, partnership, growth, affection, and resolve), a simple instrument and mnemonic device for assessing the functioning of a family system in health and illness (not to be confused with the newborn Apgar score).
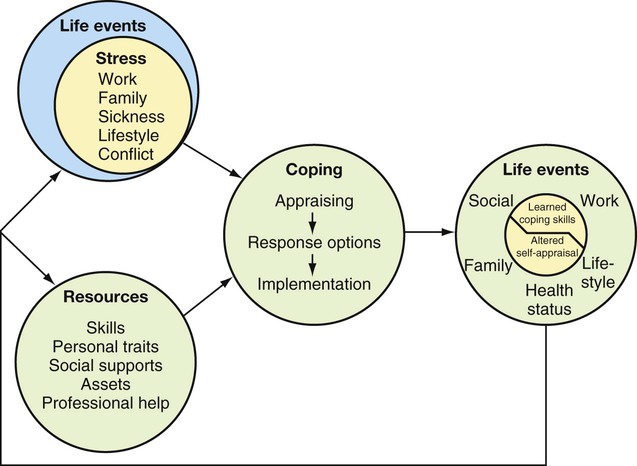
The Stress and Coping Model
General relationships among life stresses, coping resources, and health outcomes are presented schematically in Figure 3-1. This approach represents another example of the application of a systems model. In this model, health outcomes are impacted by how life stresses affect the individual. The effect of stress is moderated by the individual's appraisal and coping responses, personality, and the person's available social resources. Although the complex synergistic interactions that characterize these relationships are beyond the scope of this chapter, the major variables provide a basis for considering physician interventions.
Definitions of Stress
Stress has been variously defined as an environmental event, a response to an event or circumstance, and a process. One approach defines stress in terms of life events—as a stimulus—circumstances or events that require the person to adapt produce feelings of tension. These stressors may be major catastrophic events (e.g., natural disaster), major life events (e.g., death of a loved one), or recurrent daily hassles (e.g., need to manage a chronic medical condition).
Stress can also be seen as a response. For example, a person with a social phobia feels stressed at a party, experiencing a psychological state of nervousness with associated physical symptoms of dry mouth, palpitations, and sweating. This physiologic and psychological response to a stressor is often called strain.
A third approach emphasizes stress as a process in which “environmental demands tax or exceed the adaptive capacity of an organism, resulting in psychological and biologic changes that may place persons at risk for disease” (Cohen et al., 1995). Within this approach, stress includes stressors and strains along with the relationship between the person and the environment. The process involves transactions between the person and the environment, with each affecting and being affected by the other (Sarafino, 1990). “Adaptive capacity” is operationalized in terms of resilience and vulnerability; within this model, the physician considers aspects of a person's psychological makeup and social world that may render the patient more susceptible or more resilient (Steptoe, 1998).
Stress Appraisal and Coping
Every family physician sees patients under stress who present with a wide spectrum of stress-related symptoms and coping responses. How the individual interprets and copes with stress are as significant as the stressor itself. Cognitive appraisal of a stressor, rather than severity or duration alone, determines physiologic and behavioral responses (Epel et al., 1998).
Coping refers to how individuals manage the real or imagined discrepancy between environmental demands and their resources for addressing the stressful situation. According to Lazarus and Folkman (1984), adaptation to stress is mediated by appraisal (i.e., personal meaning of a stressor and one's sense of resources for dealing with it) and coping (i.e., thoughts and behaviors used to manage stress). Whereas with emotion-focused coping, a person directs energy to regulating internal feeling states, with problem-focused coping, a person directs attention to reducing the stressor or expanding resources for dealing with it (Sarafino, 1990). The effect of stressful life events on health is determined by many factors related to coping, including cognitive style, personality characteristics, and social and behavioral tendencies.
Personal Control
An individual's perception of the extent of his or her control in a stressful circumstance is a critical component of the appraisal process in coping. This includes control over the stressor as well as control over one's responses, whether problem-focused or emotion-focused. How a person deals with the loss of control precipitated by stressful life events can affect health outcomes.
Personal control can be defined as the feeling that one can make decisions and take effective action to produce desirable outcomes and avoid undesirable ones (Rodin, 1986). Mobilizing a strong sense of personal control can significantly reduce the impact of stressors on the individual, particularly when the response is appropriate to the circumstance. Sarafino (1990) classified personal control into the following five types:
1. Behavioral control involves the ability to take concrete action to reduce the impact of a stressor. For example, using a special breathing technique may help reduce pain.
2. Cognitive control involves the ability to use thought processes or strategies to modify the impact of a stressor. For example, focusing on a pleasant thought during suturing of a laceration may decrease the pain sensation.
3. Decisional control involves the opportunity to choose among alternative procedures or courses of action. For example, a victim of domestic violence may benefit from considering various options for when and how she will leave her abuser.
4. Informational control involves the opportunity to obtain knowledge about a stressful event, what will happen, why, and what consequences are likely. For example, a patient may feel less anxious about upcoming surgery upon learning more about managing discomfort from the procedure.
5. Retrospective control involves beliefs about causation of a stressful event after it has occurred. The attribution that the person makes about the adversity can affect future perspective and behavior. For example, attributing misfortune to factors that are temporary and specific leaves an individual feeling more optimistic than when misfortune is attributed to stable and global factors (Seligman, 1990).
Life stresses affect health outcomes. These effects are moderated not only by individual differences in genetics and pathophysiology but also by psychosocial factors. Psychosocial influences include appraisal and coping, personality traits, cognitive style, and such resources as social support.
The Life Span Perspective
The life span perspective emphasizes the importance of an individual's place on his or her personal developmental trajectory. Past development, current status, and anticipated developmental changes and challenges are taken into account. On the biologic level, changes in cellular functions occur from infancy through old age; decline in physical stamina is one manifestation of this dynamic change. On the psychological level, personality interacts with ongoing changes that occur across the life span (e.g., becoming a parent), and each developmental stage brings its own psychosocial challenges. Erikson's eight stages of development highlight the importance of trust issues in infancy, autonomy issues in early childhood, and issues of generativity and meaning in old age (Erickson, 1959). On the social level, family and peer relationships change throughout life, with significant implications for health, which may be either positive or negative. For example, the typical adolescent's shift toward greater reliance on peer relationships may lead to behaviors that endanger health, such as smoking or substance abuse. The death of a husband who has been physically abusive may lead to improved well-being for the surviving wife. The primary care physician needs to keep the life span model in mind and assist patients in addressing psychosocial factors that facilitate or block health and development.
The Ethnomedical Cultural Model
Every encounter between a patient and a physician is a cross-cultural transaction. Each person brings to the physician–patient relationship a unique mix of culturally embedded attitudes, knowledge, and beliefs. Ethnicity, gender, religion, language, education, and personal history shape expectations and behavior on both sides of the relationship. A physician's cultural proficiency is instrumental in establishing rapport and gathering information for accurate and comprehensive diagnosis and treatment (Carrillo et al., 1999). The patient's acculturation status and cultural background are important to understand, and physicians should become familiar with the dominant cultural groups they serve.
The ethnomedical cultural model emphasizes cultural concepts relevant to health and illness (Kleinman et al., 1978), including patient beliefs and expectations about the body, illness, and treatment. Berlin and Fowkes (1983) operationalize this model in clinical encounters with their LEARN acronym, exhorting physicians to do the following:
▪ Listen with empathy a nd understanding to the patient's perception of the problem by eliciting the patient's explanatory model for the illness.
▪ Explain your perceptions or explanatory model in language the patient can understand.
▪ Acknowledge the differences and similarities between your explanatory model and that of the patient and discuss any significant discrepancies.
▪ Recommend treatment that you decide is optimal within your explanatory model.
▪ Negotiate treatment with the patient, seeking a compromise that is acceptable to the patient, is consistent with your ethical standards, and uses the patient's social network when necessary.
The ethnomedical cultural model highlights cross-cultural elements in all physician–patient interactions.
Integration of Psychosocial Issues in Clinical Practice
Wynne (2003) states, “In the ‘real’ world of health care, systems thinking is more needed than ever before, but its increased complexity challenges both clinicians and researchers to the depths of their resources.” Knowledge, attitudes, beliefs, emotions, behaviors, relationships, and social/environmental factors interact to affect the experience of illness or well-being. Accordingly, physicians' ability to promote health and relieve suffering depends on their ability to engage effectively in this complex web of interrelationships. This is a daunting task that depends on fostering a quality relationship over time, gathering sufficient biopsychosocial data about each patient, and integrating data with theoretic understanding to inform interventions.
The challenge for even the most astute physician is to assess and address psychosocially important issues within the limited time available for each patient. In a 10- to 15-minute period, a detailed evaluation of all relevant psychosocial factors is an impractical goal. Using a pragmatic approach that balances this goal with time constraints, a physician can maintain awareness of psychosocial cues and information in all patient encounters while restricting direct inquiry, depending on the specific situation. A physician may not need to elicit a detailed psychosocial assessment with every patient who presents with an upper respiratory infection, but knowing if the patient smokes would be useful, leading to further inquiry and potential smoking intervention.
Following pragmatic considerations, a physician should work collaboratively with patients to identify problems of highest priority and to address less pressing issues in subsequent encounters. For example, in the case of domestic violence, immediate needs for patient safety must be addressed. Addressing long-standing issues, such as dysfunctional means of coping with stress, must be a secondary concern in the face of the primary need to achieve safety. Similarly, every physician learns to place high priority on patient complaints of chest pain, adjusting questioning depending on the patient's age, gender, family history of coronary heart disease, and patient medical history. Nevertheless, the physician must look for psychosocial clues, evaluate stressors, and be aware of factors that suggest an anxiety or somatization disorder. These secondary factors can be addressed in more depth when the physician is assured that a cardiac crisis is not imminent.
Collection of Psychosocial Data
In family practice settings, the most common and natural approach to gathering psychosocial data is interviewing the patient over time. Freud suggested that the major achievements of healthy development were the abilities “to work and to love,” and this is often a good place to start. Where does this patient work, and how does he or she feel about the job, school, or household responsibilities? Who is “family” for this patient, and what is the nature of the support system? Detailed inquiries about work and love made in the context of the ongoing physician–patient relationship result in significant accretion of knowledge over time and make it easy to flag stressful changes in these important arenas.
Other important areas of inquiry include the patient's physical and social environment. Factors such as the quality of housing, neighborhood, food, and financial resources all affect patient safety, health care use, family stress, and physical health. Understanding the ethnic, religious, and political culture of a patient and family is important for guiding culturally appropriate care. Personal and family history, usually gathered gradually over time, can alert the physician to important family coping patterns, strengths, and liabilities. Of special importance is information on major personal family “dislocations,” including losses, illness, and trauma. Knowledge of any traumatic encounters with previous health professionals or with previous medical procedures may help the physician anticipate and manage potential crisis situations.
Information from patient dialogue can be supplemented by standard measures such as health questionnaires (e.g., Short Form 36); screening inventories (e.g., Beck Depression Inventory); and stress, coping, and social support tools. Other means of gathering relevant data include informal interviews with family members, structured assessments (e.g., family APGAR), review of existing records (e.g., school records), consultation with nonmedical colleagues (e.g., psychologist, occupational therapist), observation of the patient's environment through home visits, and consultation with cultural informants and translators. Perhaps most important is the ongoing use of open-ended questions, so that important psychosocial data are elicited from the patient in the patient's own words.
Interventions Using Psychosocial Data
A comprehensive review of interventions addressing psychosocial influences in health is beyond the scope of this chapter and would require discussions of clinical psychology, social work, nursing, occupational therapy, and public health. Even in optimal circumstances, competency can be achieved only within a limited range. Realistically, family physicians should pursue basic proficiency in selected interventional strategies and additional training in areas of interest relevant to their specific practice needs and the population they serve. Here we discuss pragmatic interventions for practicing physicians based on the general model of stress, life events, coping, and health discussed earlier.
Because health outcomes are affected by stressful life events, coping (e.g., stress appraisal), and resources (e.g., personality, social support), addressing any of these dimensions can have a positive effect on functioning. As stress increases relative to available support and coping capacities, disequilibrium results. Put simply, interventions that decrease stress or enhance support tend to improve well-being. Physician attention to factors that exacerbate or mitigate is always valuable. For example, because a new medical diagnosis is stressful but a loving partnership is a source of support, assuring the presence of a loving family member when bad news is to be shared with a patient may lessen its negative impact. Some life events, such as the death of a supportive partner, affect several elements in the model, as the bereaved partner confronts a major loss (stress) without the person who had previously offered comfort in such times (decreased support). Not surprisingly, persons who are grieving are at higher risk for experiencing health problems (Rogers and Reich, 1988), and a focus on their support systems and coping strategies is almost always warranted.
Interventions that should be part of the standard repertoire for family physicians are those that do no harm, usually help, and use traditional skills. Specifically, physicians can work with patients directly to reduce stress, to enhance or mobilize social support resources, and to reinforce or model positive stress appraisal and coping. Direct approaches to stress reduction may include intervening in the patient's environment (e.g., arranging respite care for an older patient to relieve stress on his middle-aged daughter) and allaying a patient's unrealistic fears about an illness. Social support can be enhanced directly through the provision of more contact with the physician or indirectly through mobilizing the patient to increase contact with family or friends. Physicians can support positive coping through instilling hope, modeling optimism, and encouraging patients who adapt. Reminding patients of personal strengths previously used to confront crises is also helpful. The physician often can implement these strategies by asking questions that allow the patient to respond in a broader perspective (e.g., “What do you remember doing to help you cope with the death of your good friend several years ago?”). Especially when behavior change is indicated, collaborating in discussing options rather than giving advice is more likely to be effective. One collaborative approach that has demonstrated efficacy is motivational interviewing (Rollnick et al., 2008; Rubac et al., 2005).
In the provision of care within a biopsychosocial model, interdisciplinary teams, rather than solo practitioners, have the advantage, and physicians can have more positive impact on their patients' lives when they harness the wisdom of colleagues from other fields through referral or consultation. Depending on physician training, interest, and time, these basic categories of intervention can be supplemented by a wide range of psychosocial interventions, from family therapy to behavior modification.
Important Times for Psychosocial Interventions
Interventions that attend to psychosocial issues are especially important at specific times in the provision of family medical care. Natural transitions in the family life cycle, such as the birth of a child or the death of a spouse, call on the physician to provide empathic support, assess the patient's support system, normalize emotional reactions, and provide anticipatory guidance as patients confront changing family roles and functioning.
When adherence or lifestyle issues impinge on health, interventions that focus on biologic mechanisms alone are likely to be ineffective. The health effects of substance abuse, domestic violence, poverty, or inactivity are often best addressed through attention to social environment and psychological concerns.
A dramatic change in patient symptoms also indicates consideration of psychosocial factors. A psychosocial crisis can provoke an exacerbation of a chronic condition (e.g., rheumatoid arthritis), a new manifestation of illness (e.g., myocardial infarction), or emotional-psychiatric symptoms (e.g., anxiety, trouble sleeping) best treated through stress reduction and symptomatic care.
A significant medical diagnosis may precipitate emotional distress or psychosocial upheaval and requires physician attention to the context of the patient's life. Effective physician intervention may involve anticipating the nature of the potential family crisis, including family members in discussions with the patient, and addressing family needs for support. Timely provision of accurate information can enhance a patient's sense of control. Direct support by the physician during the initial adjustment phase can minimize more serious emotional disruption.
Patients living with chronic illness require sensitive psychosocial care. Managing a chronic health problem challenges a person's ability to adhere to medical recommendations and to cope with other life stressors. Patients often cope in highly idiosyncratic ways. Pollin (1995) identified eight emotionally charged issues that patients with chronic illnesses inevitably confront: control, self-image, dependency, stigma, abandonment, anger, isolation, and death. These issues can often be effectively addressed within the physician–patient relationship and through judicious referral to support groups for chronically ill patients. As elaborated by Pollin, each issue can be met by an appropriate and helpful professional stance. In response to control issues, for example, professionals should help patients express their feelings of loss of control and identify areas where they may feel powerless. Normalizing the patient's feelings and fears is the first step in helping address control issues. The goal of intervening in regard to the issue of loss of control is to reinforce the patient's confidence in being able to cope with the demands of the medical condition.
Evidence-Based Practice
Increasingly, high-quality data are available that support the therapeutic efficiency of a variety of general and specific behavioral interventions relevant to primary care practice (Trask et al., 2002). A systematic review by Di Blasi and colleagues (2002) on the consequences of nonspecific effects of the physician–patient relationship found that providing information and emotional support contributed to recovery or improvement from physical illness. Because coping with stress and managing chronic illness often involve behavior change, physicians may use “motivational interviewing” approaches to assist these patients (Rollnick et al., 2008).
Much research demonstrates the efficacy of psychosocial interventions in diseases that have been historically viewed as purely medical, including cancer (Anderson et al., 2007; Edwards et al., 2008; Rehse and Pukrop, 2003; Spiegel et al., 1989) and diabetes (Bogner et al., 2007), and the efficacy of behavioral interventions such as exercise for cardiovascular disease (Taylor et al., 2004). Online resources are available to search for study results (see Web Resources at end of chapter).
Given the time constraints primary care physicians face and the expertise required to use behavioral interventions effectively, the physician should know behavioral health providers in the community and refer to them promptly and often. The evidence base for effective behavioral interventions in numerous psychiatric and psychosocial problems, as well as medical problems, continues to expand (e.g., mood and anxiety disorders, trauma victims). Highly effective treatments are underused when physicians underrefer to mental health professionals with specialized training and overrely on the use of psychotropic medicines alone. Unfortunately, even when guidelines are available that physicians could follow themselves, resistance to change impedes their implementation (Torrey et al., 2001).
The Patient-Centered Medical Home
Health care spending currently represents approximately 18% of the U.S. gross domestic product and is projected to surpass 20% within a decade (Sisko et al., 2009). There is ongoing concern about the number of uninsured and underinsured persons, although new legislation to expand insurance coverage took effect in 2014.
Numerous perspectives exist on how the health care system needs to change, but a consensus is emerging that focuses on the importance of primary care medicine and on managing chronic disease in the context of a high-quality physician–patient relationship (Bein, 2009). This consensus reflects the accumulating evidence that higher quality health care at lower cost is achieved when primary care is emphasized (Starfield et al., 2005).
The concept of the patient-centered medical home (PCMH) embodies this emerging emphasis. As discussed in Chapter 2, the numerous components of a PCMH (or “health home”) include the use of an electronic health record, better access and scheduling processes, use of evidence-based medicine, more point-of-care services (e.g., multidisciplinary teams, group visits), and ongoing emphasis on quality improvement. Some argue that incremental change in this regard is insufficient and that transformation of practices is necessary (Nutting et al., 2009). Such transformation would include a broad, population-based approach to preventive services and chronic care beyond a “single patient at a time” approach. However, even within such a model, services would need to be individualized based on the patient's goals and unique situation, including attention to the psychosocial factors that affect chronic disease prevention and management.
These trends represent an opportunity for family medicine to take a leadership role in health care reform, with an emphasis on psychosocial aspects. The PCMH philosophy is consistent with family medicine's long-standing emphasis on whole-person care in the context of a high-quality physician–patient relationship. Ideally, the family physician in a PCMH will address the psychosocial needs of patients in collaboration with ancillary providers as needed.
Conclusion
To practice in a way that sensitively integrates psychosocial concerns, a physician needs to have a solid knowledge base in the social and behavioral sciences (Cuff and Vanselow, 2004). This general knowledge base complements specific knowledge of self, patients, practice, and community. Self-knowledge entails an honest assessment of the physician's knowledge base, skills, and attitudes relevant to comprehensive care. Acknowledging limitations in dealing with psychosocial issues in primary care is vital and can serve as an impetus for further training and the development of collaborative relationships with other professionals. A responsible physician feigns neither knowledge nor empathy but relies on an interdisciplinary network of professional and community resources to complement personal limitations.
As Osler (1904) emphasized, knowing what kind of person has a disease is as important as knowing the disease. Knowledge of each patient is requisite to the provision of sensitive psychosocial care, with attention to life stresses, coping, personality, and social resources. Furthermore, the physician needs to know details about the population he or she serves, including demographic, socioeconomic, cultural, and epidemiologic dimensions. Addressing psychosocial issues in a practice that serves an ethnically diverse, indigent population presents different challenges than addressing the needs of an affluent population from a familiar ethnic and cultural background. Understanding the practice also entails knowing the health care economics and current systems of care, which inevitably introduce challenges to comprehensive care.