Establishing Rapport
Robert E. Rakel
Rapport comes from the French en rapport, which means “in harmony with.” Rapport is most easily established during the patient's first visit, and achieving rapport enhances the likelihood that the patient will comply with the treatment plan. When rapport has been established, patients are more likely to forgive a less than perfect experience or an unexpected poor clinical outcome.
Even the most knowledgeable and skilled physician will have limited effectiveness if he or she is unable to develop rapport with patients. Unfortunately, rapport is one of those intangibles that is more than the sum of its parts. Rapport is not analyzed easily within any one body of knowledge. The basis of rapport, however, is the development of communication skills that instill in patients a sense of confidence and trust by conveying sincerity and an interest in their care and well-being. The patient's satisfaction and compliance with the physician's instructions (both measures of rapport) depend on the ability of the physician to communicate understanding, compassion, and genuine interest in the patient and to display a thorough approach to solving the patient's problems. Patient satisfaction also is related to the physician's efforts in educating patients about the disease process and motivating them to participate in their treatment.
Failure of communication between physician and patient also can affect the outcome of treatment, often as seriously as an error in treatment. More complaints against physicians result from a breakdown of the caring aspect of the doctor-patient relationship than from the technical quality of treatment.
Most complaints against physicians—and those that too frequently lead to legal action—are the result of a lack of communication between physician and patient. The potential for a serious problem always exists when a patient is inadequately informed regarding a diagnostic procedure, treatment, prognosis, or anticipated cost. The misunderstandings that result cause unnecessary expense and grief for both parties.
Similarly, the worries that result from distorted information can jeopardize the physician-patient relationship. When a patient is discussed on hospital rounds or with a colleague in the office, take care that the discussion is not within the patient's hearing distance or within that of other patients. Patients overhearing the conversation may believe the comments apply to them, or they may know the patient involved and relay the information in a distorted manner. Fragments of such conversations, overheard by the patient or others, are too easily taken out of context and can become the focus of fearful fantasies that only serve to increase uneasiness and apprehension.
Compassion, interest, and thoroughness are essential components of successful patient care. These features traditionally have been embodied in the term bedside manner, which also connotes qualities of concern, kindness, friendliness, wit, and cheerfulness, all of which result in an atmosphere of trust and confidence between physician and patient. The physician with the best bedside manner may be the one who makes no special effort to communicate these feelings but acts in a concerned, natural, and comfortable manner.
Oliver Wendell Holmes said that to be effective, the physician should “speak softly, be well-dressed, have quiet ways and have eyes that do not wander” (1883, p. 388). Lack of eye contact may be interpreted as a lack of concern. A good first impression is certainly great help in establishing rapport. It takes less than 7 seconds to form a first impression. You do not get a second chance to create a first impression. The physician should approach the patient in an assured, confident manner with a smile and a handshake if the occasion is appropriate.
Personal appearance is a significant part of nonverbal communication. Patients consider house staff who wear white coats with conventional street clothes as more competent than those who wear scrub suits. If white coats are worn, the patient sees only the collar, tie, and shoes, and it is therefore important to keep these items neat.
Posture is also important in conveying an image of confidence and competence. Standing erect, moving briskly with head up and stomach in, is better than slouching. Energetic people seldom slump; they sit upright and appear alert. A listless or lethargic appearance can be interpreted as lack of concern.
Before entering the examining room or hospital room to see a patient, review the record briefly and become familiar with the patient's name and its proper pronunciation. If the pronunciation is unusual or difficult, place phonetic markings on the chart as a reminder for future use. Repeat the patient's name when first given it to confirm the pronunciation, and then use the name twice in the first minute to help it register. Review the medical record for particular aspects of the previous visit that should be remembered and commented on, such as the illness treated at that time, family conditions, or other problems. Patients will believe that the well-informed physician is truly interested in them. Additional courtesy, such as opening the door and assisting patients with their coats (especially elderly patients), shows a consideration that aids in establishing and maintaining rapport.
Respect
Patients should believe that their comments are being listened to, carefully considered, and taken seriously. They must believe that the physician values their comments and opinions before trusting him or her with information of a more personal nature. As long as the physician's attitude toward the patient embodies respect, concern, and kindness and a sincere effort is made to understand the patient's difficulties, the patient will overlook or forgive myriad other problems.
Oliver Wendell Holmes advised patients to “Choose a man who is personally agreeable, for a daily visit from an intelligent, amiable, pleasant, sympathetic person will cost you no more than one from a sloven or a boor, and his presence will do more for you than any prescription the other will order” (1883, p. 391).
A lack of confidence, rather than an excess of it, may lead physicians to appear aloof and unconcerned. Too often, physicians think that a godlike image of omnipotence is necessary for the maintenance of the patient's respect and confidence. It is usually a lack of self-confidence that causes physicians to retreat behind this protective image, which limits their ability to help. Secure physicians are freer to establish close personal relationships with patients without fearing their position will be threatened. A physician with a positive self-image is also willing to recognize and admit the limits of personal competence and feels comfortable seeking help from a colleague when such consultation is of value to the patient's care.
The bond of mutual respect is enhanced if the physician makes positive statements about other people. Patients find it difficult to respect a physician who is regularly detractive, making negative statements about other people or other physicians. Any comments that can be interpreted as “building yourself up by tearing someone else down” merely accomplish the reverse.
The effectiveness of physicians depends on the degree of their insight into the limitations of their personalities and the psychological defenses that distort their perceptions of patients. Physicians must recognize patients or situations that make them unreasonably angry or provoked (e.g., a whining, complaining individual who shows no interest in being rehabilitated, preferring a role of social dependency). The physician's emotions, if they go unrecognized, can serve as a barrier to the development of mutual respect. If the physician is aware of negative feelings toward a patient, an effort can be made to avoid showing signs of irritation or anger. It has been said that clenching of the physician's fist is a clinical sign of a hysterical patient. The physician should attempt to remain objective and analyze the situation for its diagnostic value.
Patients with trivial complaints or somatic manifestations of emotional disease sometimes are given less attention than those with clear-cut organic abnormalities. The frequency with which a physician complains about the triviality and inappropriateness of patients' problems has been found to be related to the volume of patients seen and the degree to which the physician feels overburdened. The more patients that physicians see and the more overloaded their practices, the more likely they are to describe patients' complaints as trivial, inappropriate, or bothersome. Physicians who have more time or take more time per patient, and who investigate the patient's complaints more thoroughly, frequently uncover significant factors and less often tend to view the complaints as trivial. Respect for patients involves taking their fears and apprehensions seriously and withholding value judgments. Patients who frequently seek help for nonspecific somatic and functional complaints may be depressed (Widmer et al., 1980).
Patient Satisfaction
A close relationship exists between rapport and patient satisfaction, and this chapter deals with the many facets of that relationship. It is important that the physician make an effort to understand what patients are “going through” (not only their pain and discomfort, but also the effect these have on their lives) and communicate this understanding to them.
Most studies indicate that patient satisfaction depends on information and the degree to which the patient understands the illness. Joos and associates (1993) found that patients whose desires for information and attention to emotional and family problems went unmet were significantly less satisfied with their physicians than those whose desires were met. Even patients with chronic diseases who had lived with the problem for years had questions they wanted answered. Their satisfaction was related more strongly to the desire for information and affective support than to whether the physician conducted examinations and tests. The greater the patients' satisfaction, the more likely they are to comply with treatment recommendations.
Although patient satisfaction is strongly associated with the length of the visit, it can be further enhanced by spending some time talking about nonmedical topics. Even brief chatting about the weather or something nonmedical can give the impression that more time was taken with the patient, thereby reducing the feeling of being rushed through the visit (Gross et al., 1998).
Patient Dissatisfaction
In a typical business, only 4% of customers voice their dissatisfaction. The other 96% say nothing, and 91% never return. This has led to many practices conducting regular patient satisfaction surveys so that problems can be identified.
Communication
The patient should be able to gain access to the clinician on the phone, by e-mail, or by an early appointment without having to run an obstacle course created by an overly protective staff. Delay in returning a phone call may result in a patient remaining home all day waiting; if the call is not returned at all, the negative effect on rapport is great.
Unwillingness to make communication convenient for the patient usually results in a spiral of increasingly frequent attempts to reach the physician and mounting frustration for everyone. In contrast, physicians who give a high priority to communicating discover that most patients are considerate and even protective of the physician's time. At the beginning of a practice, patients do a certain amount of testing to determine a physician's accessibility; physicians who pass the test find that they are rarely inconvenienced by unnecessary calls or patient visits.
Verbal Communication
Much of the communication process in the clinical interview centers on verbal interchange. Symptoms, past medical history, family medical history, and psychosocial data are transmitted primarily by verbal means. The chief complaint is extremely important because it explains why patients believe they need the physician's help.
Patients who do not mention a concern and who withhold requests are less satisfied with their care and experience less improvement in their symptoms. Bell and colleagues (2001) found that 9% of patients had one or more unvoiced desires and were most hesitant to ask their physician for referrals and for physical therapy. These patients were also less likely to trust their physician. This is an important reason to be sensitive to subtle clues that the patient may be suppressing something important to them. What the patient does not say may be as important as what the patient says.
“Slips of the tongue” or major areas of omission (e.g., a married person who never mentions a spouse) may signify problem areas that, when explored, help establish the interviewer as a perceptive person who understands the underlying issues. The interviewer constantly must consider, “Why is the patient telling me that?” Even simple, casual remarks may be the patient's way of broaching issues of great concern; the man who says, “Oh, by the way, a friend of mine has been having some chest pain when he walks a lot. Do you think that sounds serious?” may actually be talking about his own concern that he is unable to face directly. A child may be brought to the office with a trivial problem so that the mother has a chance to discuss with the physician something that is troubling her; the child is a calling card, signaling the need to open the communication channel. The physician who is sensitive to these subtle clues and encourages the patient to discuss what is actually troublesome will find that the rapport established allows future interviews to be much more open and direct.
Hand-on-the-Doorknob Syndrome
The patient's parting phrase is sometimes a clue to the primary reason for the visit, or it may reflect another issue of great concern that is emotionally threatening and could not be voiced until adequate courage was summoned at the moment of departure. It sometimes surfaces as a last, desperate attempt to communicate because, with a hand on door, escape is readily accessible if the physician's reaction is unfavorable. Reasons for this hidden communication by the patient are important and must be recognized and addressed. Because of fear of rejection or humiliation, the patient may test the physician with minor complaints before mentioning the real reason for the visit (Quill, 1989). The physician must be alert to any unusual behavior during an interview (e.g., slips of the tongue, unexpected responses, overenthusiastic denials) and should search further for the underlying reason for the visit when a patient presents with a trivial complaint that appears inappropriate. It is a good practice to ask the patient routinely at the end of a visit, “Is there anything we have not covered, or anything else you would like to ask me?”
Patients with a fear of cancer, for example, often are unable to voice their concern to the physician. Instead, they present with somatic complaints or contrived reasons that necessitate a complete examination. They are hopeful that the examination will allay their fears without it being necessary to express them openly. A female patient presenting for a complete physical examination actually may be concerned over the possibility of a carcinoma of the breast, which her elder sister might have had at the same age or for which a friend recently had surgery. Such situations emphasize the need for a complete family history and a discussion of any patient concerns in an effort to allow these feelings to surface. Attention then should be paid to alleviating the anxiety. Apprehension regarding cancer is widespread, and the only cure for this fear often is a therapeutic conversation with the physician.
Physicians in private practice who have established rapport during an ongoing relationship with patients communicate more easily than do physicians seeing a patient for the first time in an emergency department (ED). Korsch and Negrete (1972) showed that ED physicians did more talking than the patients, although their perception was just the opposite. This was attributed to interaction with unfamiliar patients by house staff in a setting where the stress level is high and the orientation therapeutic. However, Arntson and Philipsborn (1982) found that physicians in private practice for 26 years who knew their patients and saw them in a low-stress situation for diagnosis or health maintenance also talked more than the patients (twice as long). One difference in the two settings was a strong, reciprocal affective relationship between physician and patient in the private office. If either made an affective statement, the other would respond similarly, whereas in the ED, patients expressed twice as many affective statements as did the physicians.
Vocabulary
The use of appropriate vocabulary assists in establishing rapport by ensuring easy and accurate communication. Phrasing questions in simple language appropriate to the patient's level of understanding and avoidance of medical jargon help establish a sense of working together. The patient's cultural background and educational level should be considered, and the physician should avoid using slang or a contrived accent because the patient will detect the artificiality and consider this patronizing.
Patients prefer to be enlightened, and they demand maximum insight into their care. It is best to start all explanations at a basic level and proceed only as rapidly as the patient's understanding permits. An analysis of 1057 audiotaped patient interviews with 59 primary care physicians and 65 surgeons showed that in 9 of 10 cases, patients did not receive good explanations of proposed treatments or tests (Braddock et al., 1999).
Medical terminology should be avoided unless it is familiar to the patient. For example, some patients have interpreted “lumbar puncture” to mean “an operation to drain the lungs.” No longer does the physician gain a therapeutic advantage by writing prescriptions in Latin or impressing the patient with medical terms.
Metaphors can be harmful and are often used without the physician being aware of the negative connotation, unknowingly raising the patient's anxiety level. Attempts to coerce a patient into having surgery with phrases such as “you are living on borrowed time” may cause anxiety and increase postoperative morbidity (Bedell et al., 2004).
Physicians should be sure of what patients mean to convey by their word selection and make certain they are operating at a common level of understanding. When the patient says he or she “drinks a little,” inquire further to clarify “a little.” If the patient “spits up blood,” determine whether it is truly spitting or really vomiting. A major barrier to accurate interpersonal communication is the tendency of people to react to a statement from their own points of view, rather than attempting to interpret it from the speaker's vantage point. If a question exists regarding the clarity of the interpretation, it is best to repeat it to the speaker's satisfaction. Contract negotiators have found that when parties in a dispute realize that they are being understood and each party sees how the situation appears to the other, there is less need to exaggerate and act defensively. Korsch and Negrete (1972) found that some of the longest interviews between physician and patient were caused by failures in communication; they had to spend considerable time trying to “get on the same wavelength.” An analysis of the conversations revealed that less than 5% of the physician's conversation was personal or friendly in nature, and that although most of the physicians believed that they had been friendly, fewer than half of patients had this impression.
Nonverbal Communication
Verbal communication occupies so much of daily social interaction that nonverbal communication often is ignored. However, much that is said is unspoken. Communications specialists have demonstrated convincingly that nonverbal messages play a major role in validating or contradicting verbal messages, with great influence as communication symbols in their own right. When there is conflict between the verbal and nonverbal, believe the latter.
Communication between two people is usually one-third nonverbal, although some say communication is 93% nonverbal and 7% verbal (Secrets of Body Language, 2008). What is said verbally often is emphasized nonverbally, and personal attitudes and emotions usually are communicated at the nonverbal level. Nonverbal communicative signals are under less censorship from conscious control than are verbal messages, so they are likely to be more genuine.
Charles Darwin held that there is a unique pattern of nonverbal actions for each emotion. In Expressions of the Emotions in Man and Animals (1872), Darwin suggested that emotional expressions are evolutionary remnants of previous adaptive behavior that persist even though currently useless. Snarling as a sign of aggression is one example. Although recent knowledge indicates that emotional expression is learned and genetically mediated, Darwin's idea of a unique pattern of actions has been shown for depression and anxiety and is likely in the future to be demonstrated for other emotional states.
Paralanguage
Paralanguage is the voice effect that accompanies or modifies talking and often communicates meaning. It includes velocity of speech (e.g., fast, slow, hesitant), tone and volume of voice, sighs and grunts, pauses, and inflections. Urgency, sincerity, confidence, hesitation, thoughtfulness, gaiety, sadness, and apprehension all are conveyed by qualities of voice. McCaskey (1979) believes that the literal interpretation (i.e., definition) of words accounts for only 10% of communication between two people, whereas facial expression and tone of voice account for up to 90% of the communication.
There is a real difference between verbal and vocal information. The verbal message refers to the words literally transmitted. The vocal message includes the emotional quality, the tone of voice, and the frequency and length of pauses—information that is lost when the words are written. Tone of voice, for example, can reverse the meaning of words. Sarcasm is a common example of a contradiction between vocal and verbal messages. Comparative studies have shown that when the vocal and verbal messages transmit contradictory information, the vocal is more accurate.
Physicians should be alert to subtle changes of tone, such as when patients ask whether everything will be all right. Are they asking for reassurance, showing fear, or doubting the diagnosis? Rather than concentrating exclusively on what patients are saying, the astute physician will concentrate on how they are saying it.
In a study of recordings of surgeons who had been sued and those who had not, the sued group could be identified by their tone of voice. They sounded dominant, whereas the nonsued group sounded less dominant and more concerned. “In the end it comes down to a matter of respect, and the simplest way that respect is communicated is through tone of voice” (Gladwell, 2005, p. 43).
Touch
A close personal interest in the patient can be communicated by the appropriate use of touch. The most socially acceptable method in this country is a handshake, enabling the physician to establish early contact with the patient (Colgan, 2009). The handshake, properly used, can convey to the patient sincerity and interest as well as security and poise. It is an inoffensive intrusion into the other person's area of privacy and can be extended under certain circumstances to include the application of the left hand to the lower or upper arm. This technique is often used by politicians to emphasize sincerity and concern (Figure 13-1). A variation of the politician's handshake is the “double-hander,” which some equate to a miniature hug.

Politicians also “gain the upper hand” by positioning themselves to the right of the other person so that when shaking hands theirs is on top. Another way to show dominance is to make sure they go through a door last, often with a pat on the back. This shows that the one going through the door last is in charge. This was well illustrated when President Clinton welcomed the Israeli and Palestinian leaders into a building and each insisted the other go first. While this would be considered polite in the United States, in the Middle East it reflects a power struggle. The winner (the last one through the door) emphasizes this with a pat on the back as the other enters (Secrets of Body Language, 2008).
The handshake as a traditional greeting of friendship began by the raising of exposed hands by two approaching individuals to give evidence that they held no weapons. This proceeded to the grasping of hands or, in the Roman society, the forearms. In the United States, a firm handshake is most acceptable. Usually, the limp or “wet dishrag” handshake indicates lack of interest or insincerity, especially if it is rapidly withdrawn. A moist palm is a sign of nervousness or apprehension, and the “halfway there,” fingers-only handshake indicates reluctance or indecision. However, the handshake continues to be modified culturally, and a person should be extremely wary of misinterpreting another person's handshake without understanding his or her cultural background.
In the past in China, the Confucian code of etiquette dictated that there should never be a touching of persons, and even today, Chinese officials may appear reluctant to grasp an extended hand; a Chinese man formerly shook his own hand (Butterfield, 1982). Some young people in the United States have modified the traditional palm-to-palm handshake to a grasping of the thumb and thenar eminence and continue to develop new variations reminiscent of the secret handshakes of fraternal groups.
Touching can be an effective method for communicating concern or compassion and can break down some of the defensive barriers to communication. Caution should be exercised, however, not to use it excessively or earlier than is socially permissible. If used without adequate preparation, touch can be interpreted as an invasion of privacy and a forward and inconsiderate act. During the physical examination, it is best to talk before touching by explaining to the patient what will be done next. Studies of primates have shown that touching gestures usually are considered nonaggressive and calming in nature. When used properly by the physician, touch can be facilitative and welcome.
The tremendous symbolic value of touch as a healing power was demonstrated during the Middle Ages, when people sought relief from scrofula (i.e., tuberculous lymphadenitis) through the king's touch, or royal touch, despite the notoriously low cure rates. This power has been transferred to physicians, and patients often feel better after a routine physical examination. Friedman (1979) stated that 85% of patients leaving a physician's office feel better even if they have not received medication or treatment, and 50% of patients in the waiting room feel better in anticipation of the help they will receive.
Touch, or “laying on of hands,” may promote healing, especially if it is imbued by the patient with a special symbolic value. Franz Mesmer (1734-1815) was among the first to emphasize the medical importance of laying on of hands. Mesmer, however, believed that there was a magnetic power in his hands, which he called “animal magnetism” and which he applied to ailing individuals. His theory was unscientific, and although he became famous for successfully treating a number of hysterical patients, he finally was discredited by a committee that included Benjamin Franklin and Antoine Lavoisier. They found his treatments to be without magnetism and essentially useless. They did agree, however, that he had helped many people and had brought about many cures. They attributed these cures to unknown factors rather than to the animal magnetism he claimed. Mesmerism was the forerunner of hypnosis, initially called “artificial somnambulism,” developed by Puységur, a disciple of Mesmer.
The magic of touch can be good medicine, especially when combined with concern, support, and reassurance. Stroking, a special kind of touching, describes a physical or symbolic recognition of a person's finer attributes. A stroke may be a kind word, a warm gesture, or a simple touch of the hand. Infants deprived of touch and stroking suffer mental and physical deterioration. Adults also require stroking to maintain a healthy emotional state. Stroking occurs when an interchange between two people leaves one or both with a good or fulfilled feeling.
Lightly touching someone's elbow for less than 3 seconds can give you up to three times the chance of getting what you want (Pease and Pease, 2004). Elbow touching works better in places where touching is not the cultural norm, such as Great Britain and Germany.
Body Language
It is said that body language is the unspoken truth. The astute physician will cultivate observational skills that enable the detection of hidden or subtle clues to diagnosis contained in the patient's nonverbal behavior. Kinesics is the study of nonverbal gestures, or body movements, and their meaning as a form of communication. However, specific gestures and their interpretation are of importance only when judged in the context of the circumstances surrounding them. Body language alone does not reveal the entire behavioral image any more than verbal language does alone. Just as one word does not make a sentence or even have much meaning without the sentence, a single gesture has clinical relevance only as part of a sequence of actions. Although they have significance, individual signs are not reliable when they stand alone; they are meaningful only when considered in the context of a person's total behavioral pattern.
When there is congruence between the verbal and nonverbal message—when the gesture conveys the same message as the spoken word—communication and its meaning are probably in agreement. When a person indicates something different from the other, however, the nonverbal message usually is more accurate. Unless body language, tone of voice, and words spoken all match, look more closely for the reason.
Attempts by the patient to mask feelings can be detected readily by observing body behavior. True feelings are more likely to leak through conscious efforts to conceal feelings. Likewise, a physician's attempt at deception will be detected by patients and can destroy confidence and damage rapport. Positive verbal communication (e.g., “You're looking better today”) accompanied by negative nonverbal cues will be interpreted by the patient as insincere. For example, a patient who is not told the true nature of a terminal illness usually knows it anyway and may distrust family, friends, and physician if they persist in the charade.
In a medical school commencement address, Alan Alda (star of TV's M*A*S*H) challenged new physicians to be able to read a patient's involuntary muscles as well as their radiographic studies. He asked, “Can you see the fear and uncertainty in my face? If I tell you where it hurts, can you hear in my voice where I ache? I show you my body, but I bring you my person. Will you tell me what you are doing and in words I can understand? Will you tell me when you don't know what to do?” (Time, May 28, 1979, p. 68). The physician will see the fear and uncertainty in the patient's face only if she or he is looking at the patient rather than the medical record. Alda's statement reflects the concern and compassion that patients desire. By using appropriate body language, the physician can convey this attention and concern in the most effective manner possible.
Body Position
The body position when sitting can show various degrees of tension or relaxation. The tense person sits erect with a fairly rigid posture. A person who is moderately relaxed has a forward lean of approximately 20 degrees and a side lean of up to 10 degrees. A very relaxed position (usually too relaxed for physicians interacting with patients) is a backward lean (i.e., recline) of 20 degrees and a sideways lean of more than 10 degrees.
Higher patient satisfaction is associated with a physician's forward body lean and rotation of the torso toward the patient. Larsen and Smith (1981, p. 487) found that “the patient also responds more favorably to the physician who relaxes his chin in his hands and gazes directly at the patient, rather than a physician who elevates his chin (unsupported) as if to imply a more superior status.” Physicians whose communication styles have been considered patient oriented have been observed to change body position more frequently than physicians whose conversations were physician centered.
An attempt should be made, whenever possible, to sit rather than stand when interviewing a patient. Rapport is improved if the physician does not intimidate the patient by placing him or her in a submissive position. Patients feel more comfortable and less helpless speaking in a sitting position rather than prone. Sitting on the patient's bed is usually not recommended, but for some patients, it is an effective means of establishing closeness and conveying warmth in a relaxed yet attentive manner.
Mirroring
When good rapport exists between two people, each will mirror the other's movements. Some people unconsciously establish rapport with another by mirroring that person's movements or body posture (Key, 1980) (Figure 13-2). Disruptions in this mirroring may signal that one member disagrees with what the other has said or feels betrayed or insulted but cannot express this idea verbally. If the physician notices this sudden disruption of mirroring activity by the patient, more attention should be focused on the comment that led to the change of position. Renegotiation or further explanation may be indicated. A powerful way to establish rapport is to match intentionally the body language of another.

Head Position
Typically, the head is held forward in anger and back in defiance, anxiety, or fear. It is down or bowed in sadness, submissiveness, shame, or guilt. The head tilted to one side indicates interest and attention (Scheflen, 1972) (Figure 13-3); under certain circumstances, this can be a flirtation. The erect head indicates self-confidence and maturity. It is almost impossible to tilt the head in front of someone who is not trusted or of whom we are afraid.

When listening to a patient, the physician should show interest and concern by an attentive position, which is best illustrated by sitting forward in the chair with an interested, attentive facial expression and the head slightly tilted. Darwin was one of the first to notice that animals assume a head tilt when listening intently.
Face
The human face can create more than 7000 expressions using 44 muscles (Cleese, 2001); some say 10,000 expressions are possible (Ekman, 2003).
Darwin (1872) proposed that cultures throughout the world express similar emotions or states of mind with remarkably uniform body movements. His information was gathered from missionary friends working with aborigines, persons under hypnosis, infants, and patients with mental disease. He also studied blind and deaf persons who, without benefit of learning from others, were observed to raise eyebrows when surprised and shrug their shoulders to indicate helplessness.
Darwin held that the facial expression of emotion, when undisguised, is independent of culture and is identical throughout the world. The facial expressions of joy, sadness, and anger are the same in the Australian aborigine, the American farmer, and the Norwegian fisherman (Ekman, 2006). Various cultures, however, do disguise the facial expression in different ways. In American culture, the mouth is used most often to disguise feelings. A person in a social gathering may be smiling, although inwardly sad or angry. The eyebrows, eyes, and forehead are least affected by these cultural disguises and are the most consistently dependable indicators of emotion. The current popularity of Botox injections, however, may mask these expressions by showing no wrinkling of the forehead. “A 50-year-old person with no wrinkling has almost certainly had some kind of cosmetic procedure or treatment.” (Hartley and Karinch, 2010, p. 88). As Shakespeare wrote, “I saw his heart in his face” (The Winter's Tale, Act I, Scene II).
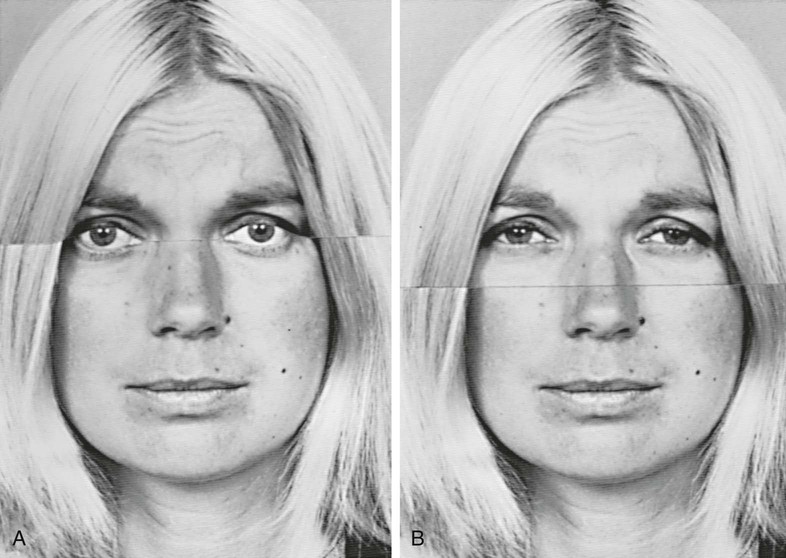
Ekman and Friesen (1975) found that the facial expressions of fear, disgust, happiness, and anger were the same in countries with widely disparate languages and cultures. They used composite facial photographs to show how each part of the face contributes to the expressions of emotion, especially surprise, fear, disgust, anger, happiness, and sadness. In American culture, when people want to disguise their true feelings and convey a more socially acceptable impression, they do so by smiling. This may be especially true in patients who are sad or depressed. Figure 13-4 is a composite showing sadness in the eyes, brow, and forehead being masked by a smile.
Smile
A genuine smile can be helpful in quickly establishing a friendly atmosphere and developing a warm, interpersonal relationship. A grin can be the physician's most effective weapon for breaking down resistance or apprehension in patients, especially children or young adults. A number of studies have shown that patients are more positively disposed to physicians who smile. The smile must be genuine, however; patients can easily spot a phony smile.
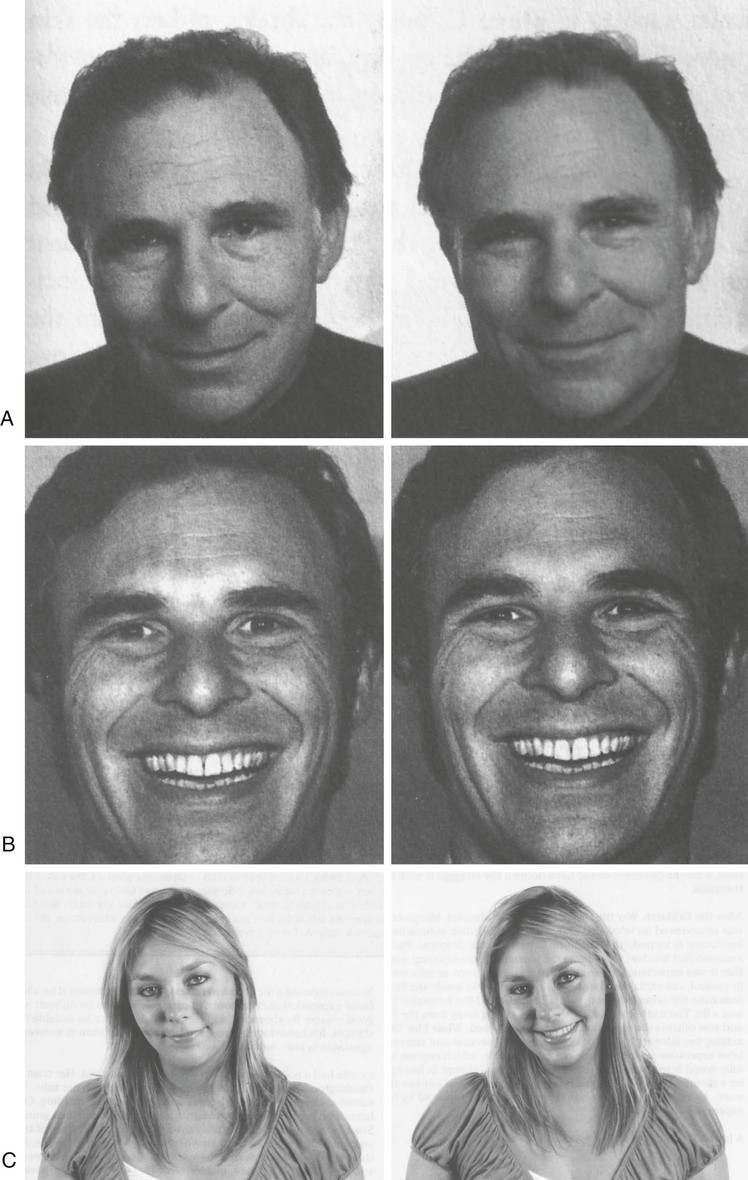
Smiles are controlled by the zygomatic major muscles that connect to the corners of the mouth and the orbicularis oculi muscles. The latter are not under conscious control and reveal a true smile that involves characteristic creases around the eyes (crow's feet). A genuine smile lights up the whole face; one that does not is more likely a deception (Ekman et al., 2005). In Figure 13-5, A, the man on the left has a broad nonenjoyment smile whereas on the right there is true enjoyment shown by the eyes. Similarly, in Figure 13-5, B, the genuine smile on the right pulls back both the mouth and the eyes. An excellent overview of facial expressions can be viewed on the DVD The Human Face by John Cleese (2001).
Micro-Expressions
Ekman and Friesen (1975) describe micro-expressions as a valuable indication of masking or deception. “Micro-expressions are caused by the face's all too rapid efficiency in registering inner feelings” (Morris, 1977, p. 110). Most facial expressions last more than 1 second, but micro-expressions last only about one-fifth of a second (Ekman, 2003). This is approximately the time it takes to blink an eye, and micro-expressions easily can be missed if the physician is not carefully observing the patient. Micro-expressions tend to occur when emotion is concealed unwittingly by repression or deliberately by suppression. They are seen when the patient begins to show a true facial expression, senses this, and immediately neutralizes or masks the expression. Some micro-expressions are complete enough to show the true emotion felt, but most often, they are squelched to such an extent that the physician has only a clue that the patient is concealing some emotion.
Most expressions last about 2 seconds (0.5 to 4 seconds). Surprise is the briefest expression (Ekman, 2003).
Eyes
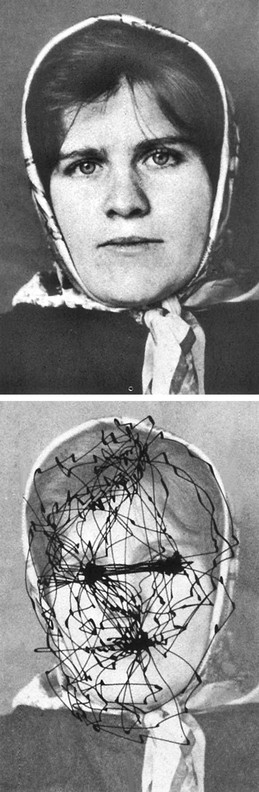
The eyes are probably the principal organs of expression. They are so important to a person's appearance that when anonymity is desired, only the eyes need to be covered. The eyebrows have been shown to have 40 different positions of expression and the eyelids have 23. Consider the magnitude of possible combinations when all facial elements are involved as indicators of expression. The message conveyed by each position can be further modified by the length of a glance and its intensity.
In most cultures, good rapport is enhanced when one's gaze meets the other's 60% to 70% of the time. When we talk, we maintain eye contact about 40% of the time and 80% when listening. Ninety percent of the gaze will be in a triangular area between the eyes and the mouth (Pease and Pease, 2004). On meeting, two people will scan each other's face for about 3 seconds, then briefly gaze downward. An upward eye break may be disconcerting or convey a lack of interest (Lewis, 1989) (Figure 13-6).
The eyes can give more information for some emotions than others. Knapp (1978) found that the eyes were better than the brow, forehead, or lower face for the accurate portrayal of fear but were less accurate for anger and disgust. Even the lower eyelid alone can convey considerable information. In Figure 13-5, it is apparent that the person in B depicts more sadness than the one in A, but the pictures differ in only one respect: the lower eyelid.
It has long been known that pupils dilate when the person sees something pleasant and contract when something unpleasant is viewed. This involuntary signal can be a valuable indication of what is really going on. Asian jade dealers wore dark glasses so that no one could see their pupils dilate when they discovered an especially valuable piece of jade. Likewise, a magician doing card tricks can tell when a preselected card is seen by a subject because of the sudden pupil enlargement. In one experiment (Hess, 1975), the pupils of males dilated when the men were shown photographs of nude females and constricted for nude males. Homosexuals demonstrated the opposite. Dilated pupils also can indicate that listeners are interested, whereas constricted pupils suggest that they do not like what is being said (or viewed).
Sincerity is expressed with the eyes. The best method for conveying sincerity is frequent eye contact, a technique most appropriately used when listening to the other person. One trait of good listeners is that they constantly look at the speaker. A listener who does not maintain eye contact but continues to look down or away from the speaker may be shy, depressed, or indicating rejection of the speaker or the comments being made. One patient said, “I had one student doctor who looked at his toes instead of me. If he ever opens a practice, I don't believe I would trust him.” Conversely, speakers frequently may break eye contact when talking and are permitted a distant stare when formulating ideas and selecting phrases. However, they still should try to make frequent, although less prolonged and intense, eye contact.
A special form of human-to-human awareness is conveyed by eye contact. Prolonged eye contact, or staring, can be offensive. Monkeys can be provoked to combat by a person staring at them because it represents a threat of aggression. Under other circumstances, however, staring can be flirtatious, emphasizing that the meaning of eye behavior depends on other factors in the situation.
The acceptability of eye contact varies significantly among different cultures. In the United States, focusing the eyes on the speaker indicates respect and attention, regardless of the age of the individuals involved. However, Mexican Americans tend not to maintain as much eye contact while listening as do other Americans and may look away from the speaker more often. This is not a sign of disrespect or inattention. In Latin American countries, a younger person may be thought disrespectful if his or her eyes meet those of the adult who is speaking. A physician could be considered seductive in that culture if he or she maintained steady eye contact while talking to a patient. In the United States, it is impolite to maintain eye contact with a stranger for more than 3 seconds, but Europeans believe that longer periods of eye contact are normal. The physician needs to consider the patient's cultural background when interpreting the meaning of eye contact behavior. Looking away from the speaker from time to time may be a sign of respect and sensitivity rather than the opposite. At the same time, the physician's failure to look a patient in the eye can be dehumanizing and can cause the patient to feel more like an object than a person. Patients are most comfortable when the physician looks at them approximately 50% of the time and are uncomfortable when eye contact is avoided. Some feel that rapport is improved if a person's gaze is met 60% to 70% of the time (Kuhnke, 2007).
The frequency of eye contact also can provide clues to whether the patient is anxious or depressed. The eyes of anxious patients blink frequently or dart back and forth. They look at the interviewer as frequently as low-anxiety patients but maintain eye contact for less time on each gaze. Similarly, the patient may interpret the physician's lack of eye contact as indicative of anxiety or discomfort, even rejection.
Frequent blinking of the eyes can be a sign of pressure or stress. In a political debate between Senator Bob Dole and President Bill Clinton in 1996, Dole blinked an average of 105 times per minute, showing more pressure than Clinton's 48 times per minute.
Depressed patients maintain eye contact only one-fourth as long as nondepressed patients. Downward contraction of the mouth and a downward angling of the head are also cues to depression. As with the anxious patient, there is no difference in frequency of eye contact in the depressed patient; the difference is only in the duration of contact.
Patients with abdominal pain caused by organic disease are more likely to keep their eyes open during palpation of the abdomen than those with nonspecific pain (Gray et al., 1988). The patient with genuine abdominal tenderness may apprehensively watch the physician's hand as it approaches the tender area.
Hands
The hands will be droopy and flaccid with sadness, fidgety or grasping in anxiety, and clenched in anger. When a speaker joins her or his hands, with fingers extended and fingertips touching, it is called steepling and indicates confidence and assurance in the comments being made (Figure 13-7). It can be taken to extremes if held too high and convey arrogance instead of self-assurance (Kuhnke, 2007).

Palms usually are held in the palm-in position. Turning the palms outward can be a subtle courting behavior (usually used by women), but it more likely indicates a warm and friendly greeting (Davis, 1975).
The hands of an anxious patient can be observed to shake when holding a pen, to twitch, or to be braced unnaturally. The white-knuckle pose of tightly locked fingers can be an effort to mask anxiety.
Hands can be a subtle indicator of the urge to interrupt. Be alert for this sign in a patient so that important information will not be suppressed, and the patient can be given every opportunity to supply valuable information. Indications of this urge to interrupt are a slight raising of the hand or perhaps the index finger only, pulling at the earlobe, or raising the index finger to the lips. The latter gesture also may indicate an attempt to suppress a comment and should alert the physician to inquire further and elicit the hidden information. A patient listening in “The Thinker” position, with the index finger across the lips or extended along the cheek, or one sitting with elbows on the table and hands clenched in front of the mouth, although listening intently, may not believe or understand the physician's words (Figure 13-8). The physician should take additional time to amplify the issue or explain the diagnosis or treatment regimen further.

Arms
Although folded arms are found in all cultures, this is considered a discovered action rather than an inborn trait because it is a natural position of comfort that is as easily discovered by the African tribesman as the New York banker. It is the subtle ways in which the arms are held that can give clues to underlying emotions. Crossed arms can be a defensive posture, indicating disagreement with another's view, or it can be a sign of insecurity. It can also be nothing more than a position of comfort and should, as with all other signs, be considered in the context of the individual's total behavior.
Notice the manner in which the arms are crossed. Are they relaxed in the normal position of comfort, or are they in a self-hugging posture, reflecting insecurity or sadness and indicating a need for reassurance? Anger can be seen in clenched fists that are held tightly against the body in a holding-back manner, preventing them from hitting (Figure 13-9). If the patient has assumed a position of resistance or defensiveness, sitting with arms and legs crossed and perhaps with body turned away, search for the reason for this defensiveness and try to eliminate it. Perhaps a recommendation that the patient stop smoking is threatening and difficult to accept. In that case, it is important to make an additional effort to explain the rationale for the recommendation; do not hurry over it with a brief comment or admonition.

Men who are under stress will often cross their hands in front of them as if protecting their genitals, called the fig-leaf position or “protecting the precious.” Women may cross arms over their abdomen referred to as “egg protecting” (Hartley and Karinch, 2010).
Legs
Although crossing the legs is a common position of comfort, it can also indicate a shutting out of or protection against the outside world. If crossed legs in a patient confirm the total kinesic picture of resistance, including crossed arms and other signals discussed earlier (Figure 13-10), make every effort to identify the reason for the resistance and correct it before proceeding further. Likewise, locked ankles can indicate defensiveness. Diagnostic information obtained from a resistant patient is likely to be incomplete, and instructions are unlikely to be followed.

When seated, a person's legs are pointed in the direction of interest and if disinterested will point away. Similarly, when legs are crossed, the upper knee dictates the direction of interest.
Notice the position of the feet and their movement. As with fidgety hand movements, anxiety is associated with the fidgety, constantly moving foot. An anxious or scared person may sit forward in the chair with feet placed in the ready-to-run position, with one foot in front of the other. The angry person is more likely to place the feet widely apart in a position of stability, whereas the feet of a sad person tend to move in a slow, circular pattern.
Gestures
The thumbs-up sign in the United States means “good going,” but in some Islamic countries, it is the equivalent of an upraised middle finger. Similarly, the extended hand with palm forward means “stop” in the United States, but in West Africa, it is an insult greater than the upraised middle finger.
Joining the thumb and index finger in a circle to indicate “OK” is an insult in many Latin American countries and in France means zero or worthless. In Texas, raising the index and little finger with the middle two fingers folded down is the “Hook 'em Horns” gesture of the University of Texas Longhorns, but in parts of Africa this gesture is a curse and in Italy it means your spouse is unfaithful.
American television and the movies have dulled these differences worldwide, although some still exist. In the 1978 movie Inglorious Bastards (remade in 2009) the American posing as a German was detected because he displayed the number 2 using index and middle fingers, whereas Europeans would hold up the thumb and index finger with the thumb being number 1.
Preening
Preening gestures, such as the male pulling up socks, adjusting a tie, or combing hair and the female adjusting clothing or using a mirror to review makeup, may not necessarily be seductive in nature but can be an attempt to establish rapport and good interpersonal relations. If the preening is intended to be flirtatious, however, the woman may cross her legs, place a hand on her hip, caress her leg, or stroke the arm or thigh in some fashion. The flirtatious male typically uses gaze holding and head tilt to accentuate normal preening gestures or may stretch to make himself look larger. Both genders may use “accidental” touching as a flirting signal. When someone's attention is completely focused on the other, legs, knees, and feet are usually extended in the direction of the other. The physician should remain alert to the accentuation of normal preening gestures into courtship actions to identify the seductive patient and deal with the issue early, before unknowingly encouraging the patient to proceed further along this course.
Respiratory Avoidance Response
The respiratory avoidance response involves a frequent clearing of the throat when no phlegm or mucus is present. All animals exhibit a respiratory avoidance response as a means of clearing something unpleasant or undesirable from the respiratory tract. This action also can be a nonverbal indication of disgust or rejection. When physicians find themselves doing this, they should observe the accompanying circumstances and notice whether posterior pharyngeal mucus is truly present.
Nose Rub
Another component of the respiratory avoidance response is the nose rub (Figure 13-11). This involves a light or subtle rub of the nose with the index finger and signals rejection of a statement being made by the subject or by another individual. The nose rub to relieve an itch is usually vigorous and involves a repeated series of rubs, whereas that of the respiratory avoidance response is soft and consists of one or two light strokes, often involving nothing more than a light flick of the nose. Morris (1977, p. 111) described the nose flick as “a reflection of the fact that a split is being forced between inner thoughts and outward action.” It can be associated with lying or with the struggle to appear calm while suppressing anger or discomfort. During Bill Clinton's testimony to the grand jury regarding his affair with Monica Lewinsky, he rarely touched his nose when telling the truth, but when he lied he gave a split-second frown, then touched his nose. During the testimony he touched it 26 times (Pease and Pease, 2004). Variations of the nose rub include pulling at the earlobe, scratching the side of the neck or rubbing one eye. Someone aware of the nose rub will often notice it in themselves and realize they are uncomfortable with what is being said by themselves or others. Watching for this during interviews on television may indicate the person being interviewed is uncomfortable with the question, or the person asking may realize it is a “testy” point.

This sign can be quite useful in patient interviewing. For example, the physician may ask a patient, “How are things at home?” The patient may answer, “Fine,” but then clears his or her throat and lightly rubs the nose with the index finger. He or she is actually saying, “I don't like what you are asking me,” or “I feel uncomfortable with my answer; things really aren't going very well at home.” If there is a cause to pursue the issue further, a simple comment such as “Really?” or “You mean not even an occasional argument?” may lead to a flood of information masked by the previous response.
Verbal-Nonverbal Mismatch
Another indication that what a patient is saying may be in conflict with what is being felt is a verbal-nonverbal mismatch, such as when the patient answers “fine” to “how are things between you and your husband?” while looking sad and avoiding eye contact (Quill, 1989). If the patient answered negatively to the question, “Have you ever had a venereal disease?” and at the same time exhibited a nose rub, this topic should be followed up with a similar inquiry later, perhaps while doing the physical examination, when the patient may feel more comfortable after better rapport has been established.
Other clues that the patient may not be telling the truth or that there are repressed feelings are asymmetric facial expressions and a prolonged smile or expression of amazement. Almost all authentic facial expressions fade after 4 or 5 seconds (Ekman, 1985).
Neurolinguistic Programming
Neurolinguistic programming (NLP) involves the eye movements performed while thinking and depends on whether a person is thinking visually, aurally, or kinesthetically. A right-handed person who is visually oriented will look up and to his or her left when recalling something visually, but up and to the right if creating something visually or, in other words, making it up or lying. Similarly, a right-handed person will look sideways to his or her left when recalling sounds and sideways to the right when imagining sounds (Ritch, 2004). A person who is looking up and to his or her right (i.e., your left) probably is imagining things he or she has never seen before. This technique is used by police investigators when interviewing suspects. A left-handed person will respond in opposite directions (Brooks, 1989; Zellmann, 2004) (Figure 13-12).

Detecting Lying
In addition to looking up and to the right to create an image or a fact, a person who is lying is also likely to do the following:
▪ Pull at the ear, or rub behind the ear.
▪ Blink excessively (although absence of blinking is also possible).
▪ Have a micro-expression indicating something is different than what is said.
The liar will also rarely touch the other person or point a finger at them or others, and the story will not include negative details (Lieberman, 1998). The liar is not comfortable with silence and may speak more than normal to convince the other. Persons suspected of lying should be encouraged to talk because verbal and nonverbal clues will then be easier to detect (Vrij, 2005). Liars are also likely to slouch, unlike a confident person, who will sit upright. Remember that it takes a combination of verbal and nonverbal clues to detect lying, and no single action is likely to be dependable other than to raise doubt or suspicion.
Proxemics: Spatial Factors
Proxemics is the study of how people unconsciously structure the space around them. This structuring varies with every culture. North Americans, for example, maintain a protective “body bubble” of space about 2 feet in diameter around them when they interact with strangers or casual acquaintances. Violators of that space are considered intruders and cause the person to become defensive (Figure 13-13). In the Middle East, no such bubble exists, and it is proper to invade this area. In fact, not to do so may be interpreted as unfriendly and aloof. Arabs prefer to stand close enough to touch and smell the other person. Americans, however, if forced to stand close together, as on a crowded subway, will use their eyes (i.e., distant gaze) to maintain a more proper distance. An arm's length is a good measure of the appropriate personal distance for most people. A wife can stand inside her husband's bubble, but she will be unhappy if another woman invades this sphere of privacy, and vice versa.

Robert Frost said, “Good fences make good neighbors.” In suburbs and small towns, people are more likely to talk to each other while in their backyards if a fence indicates the boundary than if there is a communal yard (McCaskey, 1979). Marking the boundary helps maintain territoriality and actually brings the neighbors closer together than when there is no fence.
Intimate space has been classified as that ranging from close physical contact to 18 inches, personal space from 18 inches to 4 feet, social space from 4 feet to 12 feet, and public space from 12 feet and beyond (Lambert, 2008). Placing a desk between two people shifts personal space to social space. The office desk also can be a barrier to communication when it is placed between the physician and patient, thereby emphasizing the illusion of the physician's importance and power. There may be occasions when this is desired, but it usually is not necessary in a family physician's office. Office furniture should be arranged so that a minimum number of obstacles lie between physician and patient.
Automobiles magnify the size of one's personal space up to 10 times. Compare the relationship of two people having a conversation with that of “road rage” when one invades the other's space by cutting in front of them.
Hidden or Masked Communication and Patients' Expectations
Although the average person has a symptom about every 6 days, he or she visits a physician only once every 4 months. Some people visit a physician much more frequently than others for the same symptom. The group who visits more frequently tends to have a higher level of anxiety, fear, grief, or frustration. It is the physician's responsibility to search for, identify, and treat organic disease if it is present, but in about one half of cases, none will be found. It is equally important to identify the reason for these visits—the basis for the heightened concern or increased anxiety. A person may see a minor symptom as a potential catastrophe if she or he thinks it may be a sign of cancer similar to that causing a parent's death. Is the patient really there “just for a blood pressure check,” or because of concern about the condition of his or her coronary arteries since a friend recently had an acute myocardial infarction? If the physician deals only with the symptoms, the real concerns may go undetected, and the result will be a dissatisfied and noncompliant patient.
Barsky (1981, p. 492) cautioned, “Patients who express dissatisfaction with their medical care should be questioned about this, as they may be dissatisfied because their real motivation in seeking care has not been illuminated.” He also advised the physician to investigate the patient's current life stresses when visits are made if there is no change in clinical status.
Patients may come to a physician because of what they imagine is causing their symptoms rather than because of the symptoms themselves. Identifying what patients hope can be done for them—focusing on their expectations for the visit—often reveals hidden reasons for the visit. The physician should be sure to address the patient's expectations and make certain that the interpretation is correct. Rapport and satisfaction will be enhanced if the physician identifies and satisfies the patient's expectations for the visit. Dissatisfaction results when these expectations go unmet.
Listening Well
A good family physician must be a good listener. Of all the communication skills essential to rapport, the ability to listen well is probably the most important. All the information in the world about body language, vocal messages, and nonverbal cues is of limited value unless it helps the family physician be a better listener.
As Lown (1996) states, “In the brief time available to take a history, the aim is to obtain, in addition to essential facts, insight into the human being. This seems easy, but listening is the most complex and difficult of all the tools in a doctor's repertory. One must be an active listener to hear an unspoken problem” (p. 10). The appearance of readiness to listen is aided by bending forward and maintaining eye contact. The physician can discourage a patient from talking by looking away or writing in the medical record. Well-chosen questions can be rendered useless by inappropriate nonverbal behavior. Even great questions are of no value if you do not know how to listen.
For many people, the opposite of talking is not “listening” but rather “waiting to talk.” It is impossible to listen attentively when you are planning what to say next. Besides, learning to listen is more difficult than learning to ask good questions (Dimitrius and Mazzarella, 1999).
The average listening efficiency of most people is only 25% because we do not concentrate on what is being said. Effective listening requires focus on what is being said and on voice tone, facial expression, and body movements. Hearing what someone says and truly listening to what they are saying is quite different (Zellmann, 2004).
Analyses of physician-patient interviews reveal that, on average, the physician rather than the patient does most of the talking, although when questioned, physicians usually imagine the reverse. In general, the less the physician says during an interview, the more the patient will say.
Boredom is one of the most difficult states to conceal. It is very difficult to appear attentive and interested if you are bored, and it takes considerable effort to appear interested (Dimitrius and Mazzarella, 1999).
Silence
Silence can be as effective a means of eliciting further information as direct questions. The timing is important, however, and silence should be used as a technique only when the physician is relatively certain that there is more information to follow the last statement. A shift of position or a nod and a smile, properly timed and coupled with silence, can be more effective than an encouraging comment. Nonverbal encouragement to continue is less distracting and may be more facilitative than the verbal form.
Attorneys use silence in the courtroom to get witnesses to say more than they had intended. They wait silently as if the witness has not given a complete answer, and usually they do receive additional information. Silence can be effective as long as the patient feels more inclined to fill the void than the physician. This is of value, however, only when there is more information to be obtained. It is said that Charles DeGaulle thought that silence was the ultimate power tool, and in his speeches, he gained control by looking at the audience, never breaking eye contact, and saying nothing.
Interruption
The patient may be following a line of thought and may be about to open up more but must stop and refocus if the physician captures the patient's attention with a question. The physician should interrupt a patient's statement only if it is necessary to change the conversation to a new topic, clarify an issue, elicit information not produced spontaneously, offer reassurance, or reduce patient anxiety.
Physicians usually use closed-ended questions to interrupt the patient and thereby inappropriately control the interview. Beckman and Frankel (1984) found that 69% of patients (52 of 74) had only 18 seconds to complete their initial complaint before being interrupted by their physician. This usually occurred after the patient stated only a single concern, and it effectively halted the further flow of information from the patient. This prematurely terminates opportunities for patients to present their primary concerns. Only one of the 52 patients subsequently returned to and completed the opening statement. In these recorded office interviews, only 23% of the patients were permitted to complete their list of problems uninterrupted; when they were, the complete statements usually took less than 60 seconds, and none required more than 2.5 minutes.
Humor
The art of medicine consists of amusing the patient while nature cures the disease.
—VOLTAIRE
Humor can be helpful in establishing rapport and can strengthen the physician-patient relationship. It can be used to “break the ice” and is most useful if it communicates the feeling that “we are all in this together.” Humor is an effective way for physicians to appear human while supporting and empathizing with their patients. Physicians who score high in empathy also tend to have a good sense of humor (Hampes, 2001). Empathic humor can promote a stronger physician-patient relationship and enhance the effectiveness of other, more traditional as well as nontraditional forms of therapy (Berger et al., 2004).
Care must be taken, however, because humor can be a two-edged sword that can cut either way if used inappropriately. The least risk is when the humor is self-deprecating or focused on neutral topics such as the weather or parking. It can even alienate the patient if they feel the joking around is inappropriate at the very time they want serious attention paid to their problem.
More research is needed on the value of humor in medicine so that we will know when and how to use it effectively. Norman Cousins, former editor of the Saturday Review, had ankylosing spondylitis. He received 3 hours of pain relief after watching comedy videotapes of The Three Stooges and Abbott and Costello but obtained only one-half hour of pain relief from an oral analgesic. Some physicians write prescriptions for patients to laugh out loud three times each day. In India, more than 600 Laughter Clubs convene for 15 to 20 minutes at the beginning of each day to laugh out loud. Even a fake laugh makes one feel better throughout the day. Laughter boosts the immune system and even forced laughter leads to a good feeling and relieves stress and anger (Cleese, 2001).
Physicians who express interest in patient opinions and who use humor more often are sued less often. Tasteful humor can reduce anxiety and create a bond of friendship, but humor used inappropriately can magnify the distance between patient and physician, especially if it belittles the patient.
See eAppendix 13-1 online for interviewing effectively (including facilitating techniques) and eAppendix 13-2 for care with caring.
Interviewing Effectively
The patient history is the most likely assessment activity to provide a diagnosis. The final diagnosis is evident in almost 80% of cases after the history alone and in an additional 12% of cases after the history and physical examination; laboratory testing is required to make the diagnosis in only 11% of cases (Schmitt et al., 1986).
The skilled family physician can spend 10 minutes with a patient, but the patient may think it was 20 minutes. This is much better than the physician who spends 20 minutes but leaves patients thinking that he was in a hurry and that they were encroaching on his time. Overly brief or abrupt conversations in the office or at the bedside can damage rapport severely. Physicians signal how much time they plan to spend by a variety of nonverbal cues, and patients rarely have the courage to counter this by asking for more time. The physician who hurriedly asks, “How are you?” while flipping through a chart with only a quick glance at the patient destroys communication. Even the busiest physicians can accomplish much quickly by giving full attention to the patient: Patients remember the outstanding physician who truly communicated with a relaxed posture and attentive manner in whatever time was available.
Analysis of taped physician-patient encounters in a pediatric clinic revealed that many of the mothers were dissatisfied because the physician paid too little attention to their concerns and apprehensions about their children. Their attitude had little relation to the amount of attention the physician actually paid to the infant, which was usually adequate (Korsch and Negrete, 1972).
Even in an established family practice where essentially none of the patients was dissatisfied with the physician, 54% of the patients either forgot to mention something of concern or misunderstood facts about diagnosis or treatment (Snyder et al., 1976). Of the 84 patients, 29 forgot to tell the physician something that was bothering them. This illustrates the wisdom of concluding every interview with the statement, “Is there anything else bothering you that we haven't discussed?”
When meeting a new patient, the method used to address the patient during the introduction can help establish rapport by conveying an atmosphere of mutual respect. Greet the patient warmly with a handshake and a smile while maintaining eye contact. Giving the patient undivided attention for just 60 seconds conveys the impression that you are truly interested. Use the patient's name during the introduction, during the interview, and on leaving. An appropriate introduction would be, “Good morning, Mrs. Brown, I'm Dr. —,” or, “Good morning, Mrs. Brown. I'm —, a second-year medical student, and I'll be taking your medical history and examining you today.” It is also better to show concern for the patient with an opening statement such as, “How can I help you?” rather than, “What brings you here today?”
Facilitating Techniques
In addition to the nonverbal facilitating techniques of silence and body positioning, patients can be encouraged to talk further with simple comments such as, “And then?” or by repeating a portion of the statement just made:
Patient: I have been very nervous lately.
Doctor: Nervous?
Confrontation
Confrontation, wisely used, can help establish communication and rapport. Statements such as, “You look unhappy,” or “You appear very anxious,” are based on the physician's observation of the patient. If the physician has been unable to establish rapport, it may help to approach the issue openly and frankly: “We don't seem to be communicating very well. Can you tell me what is wrong?” This is also a useful maneuver when a previously good relationship suddenly turns sour.
Summarization or Paraphrasing
Summarization is a brief restatement of what the patient has said and gives the interviewer and the patient a chance to correct errors or misunderstanding. It demonstrates the physician's interest in the patient's history and his or her effort to collect the facts accurately. A summary gives the patient an opportunity to add more details but also lets him or her know that the physician was listening. The physician can restate what the patient has said and emphasize the important points to ensure clear understanding. Summarization ensures that both parties are using the same definitions and minimizes inappropriate assumptions. “Let me see if I have understood you correctly,” or, “Am I understanding this correctly?” are good ways to introduce a paraphrase.
Summarizing is also a subtle way of focusing on the important facts in the history without asking closed-ended questions that may inhibit the patient. A summary also can be used to change the subject when the physician wants to move on to another topic.
Concluding a History
In an effort to avoid leaving gaps in the history or allowing patients' concerns to go unattended, it is wise to conclude every complete history with, “Is there anything else you would like to mention?” or “Is there anything that we have not discussed?” This excellent practice is of little value, however, if at the same time the physician puts away pen and pad, closes the chart, and starts edging toward the door.
Open-Ended Questions
Probably the single most valuable rapport-promoting element of verbal communication is the use of open-ended questions at the onset of an interview. “Tell me more about it” is an interview technique and a state of mind. The physician who understands that no checklist of yes-or-no questions can possibly portray the patient as a unique human will create an atmosphere of sensitivity and interest that contributes greatly to the early establishment of rapport. Once the broad outlines of the patient's unique situation are indicated, detailed questioning moves along quickly.
An open-ended question does not suggest what you would like the answer to be, and the patient may include additional information that was unexpected. Even if you need specific information, a good rapport builder is to start with a few open-ended questions and become more focused as you go (Dimitrius and Mazzarella, 1999).
Specific questions beget specific answers and rarely anything more. However, the physician may want to use this technique on occasion, as when dealing with the verbose, rambling patient who refuses to stick to the point, or when specific information is needed. When more general or hidden data are sought, however, the physician must choose questions and gestures that offer the maximal potential for obtaining information. To be effective, open-ended questioning requires that the physician appear relaxed and ready to listen regardless of the amount of pressure from waiting patients. After it becomes apparent that more time is necessary than is available, a new appointment is made to ensure adequate time.
Signals That Discourage Communication
While appearing to respond affirmatively and facilitate the conversation, people in fact can turn off the speaker if they frequently comment “yes” in a manner that conveys disinterest or impatience. Everyone has experienced the person who says “yes” before the sentence is finished or the point made. Patients can be subdued and reduced to silence in a similar manner, intentionally or unintentionally.
Confidentiality
Confidentiality is a cardinal principle of professionalism. Effective communication requires that the patient feel secure in the knowledge that all information will be kept strictly confidential. It is the ethical responsibility of each physician to maintain this bond of confidentiality. The family physician must appreciate this intimate and confidential bond and avoid any threat to its dissolution. Hippocrates said, “And whatever I shall see or hear in the course of my profession, as well as outside my profession in my intercourse with men, if it be what should not be published abroad, I will never divulge, holding such things to be holy secrets” (Strauss, 1968, p. 325).
Assurance that all information and actions will be kept confidential is especially important when dealing with adolescents. They may not be aware of this basic ethical principle in the medical profession or realize that it applies to them. They may be reluctant to share information and trust completely for fear that parents or peers may find out.
Complex problems of confidentiality can arise for the physician who cares for several members of the same family. Family members often can provide important information that supplements what the clinician learns directly from the patient. Unfortunately, information sometimes may be offered only on the promise that it will not be disclosed to the patient. Secrets rarely can be kept for long; the patient sooner or later learns what has been confided, straining the bonds of trust. In general, it is best not to be a party to secrets but rather to find a way to discuss sensitive material. If rapport is to be maintained, the physician must diplomatically explore the possibility of dealing with such problems in a constructive manner as soon as the patient's situation permits.
Rapport with Families
No patient exists in a social vacuum. Visible or invisible, family and friends provide a social environment that exerts an important influence on the clinical course of disease. Because the family usually has a stronger emotional influence on the patient than the physician, effective communication with the patient's family is an important element in successful patient care. Their positive support is necessary if the physician's plan of management is to be carried out. Family support of the physician's treatment regimen can help ensure that a patient remains on a prescribed diet, takes medication as instructed, rests appropriately, or maintains a proper exercise program. An unsupportive family attitude can negate or severely jeopardize previous gains in treatment.
Family, friends, and colleagues can be valuable sources of important information regarding the patient's illness beyond that given by the patient, including facts that were forgotten, repressed, or even unknown to the patient. Communication should be established through the most responsible family member (other than the patient). However, it is important that such discussion be known to patients, and that a summary of the discussion be shared with them by the physician to avoid a misunderstanding or conflict of ideas when patient and family interact. If the patient and the family have different sets of information, they may become suspicious of future communications with the physician.
Communication with concerned family and friends need not be time-consuming. If a serious or prolonged illness is involved, a family conference can outline what can be expected and what will be done. It is usually possible to identify one family member as the communication channel to whom future reports will be given, avoiding frequent and repetitious calls. Many clinicians find that optimal control and satisfaction are achieved by initiating the calls themselves on a regular schedule.
Lack of understanding of the family's concerns and inadequate communication with family members are major factors leading to malpractice suits. Devaluing the patient or family views and failing to understand their concerns was a major reason mentioned by plaintiffs (Beckman et al., 1994). The most common complaint was the feeling of being deserted by the physician and feeling alone when the physician would not return calls or return to the bedside as promised, especially after an adverse event.
Rapport with Children
Working with children is one of the delights of practice. Children have a quality of freshness and directness that adults often lack. There are no secret formulas for interacting with the young, although there are cautions to be observed. Most procedures are not uncomfortable if the physician exercises patience, but forced gaiety and false promises that “it won't hurt” immediately are perceived as dishonest, and once trust is destroyed, it may never be regained by any physician. Examining the ear of the mother or an older sibling, for example, before examining the child often allays anxiety. Let the child handle the stethoscope or otoscope. Simple rewards also can make the physician's office a place of interest for the child. Accompanying other members of the family on visits to the physician helps the child gain familiarity with the office and staff. The physician who spends a few extra minutes with children and family early in the professional relationship will reap enormous dividends in years to come.
Care with Caring
“One of the essential qualities of the clinician is interest in humanity, for the secret of the care of the patient is in caring for the patient.” This statement by Francis Peabody (1930, p. 57) could serve as the maxim for establishing patient rapport. While continuing to emphasize the curing aspects of medicine, family medicine places increased emphasis on its caring aspects. Caring is the opposite of apathy and implies the application of human tenderness and compassion to the curing of individuals. It involves respect for the individual and enables the physician to motivate patients to participate in their care. Physicians must convince patients that they care and are sincerely interested in providing help.
“Caring without science is well-intentioned kindness, but not medicine. Conversely, science without caring empties medicine of healing and negates the great potential of an ancient profession. The two complement and are essential to the art of doctoring” (Lown, 1996, p. 223). It has been said that more mistakes in medicine are made by those who do not care than by those who do not know. The caring implies an empathetic relationship between physician and patient. Empathy is the capacity of physicians to understand what the patient is experiencing, and it is best accomplished if physicians place themselves in the role of patients in an effort to understand their feelings. The capacity to understand another person's feelings is the foundation of the physician-patient relationship.
Chekov, a physician himself, believed that medical students should spend one half of their time learning what it feels like to be ill. Although this may be an extreme method for developing empathy, it is important that the student, before becoming immersed in the technical and cognitive aspects of medicine, be able to identify with the patient's feelings, fears, apprehensions, and expectations so that the knowledge acquired during medical school can be applied meaningfully in the context of these needs. Exposing students to patients in the first year of medical school, before they have been preoccupied with the diagnosis and treatment of disease, offers them an opportunity to focus on the process of communication under the watchful gaze of an instructor. Barriers to effective communication then can be identified. For example, a student may have difficulty permitting a patient with terminal cancer to talk about impending death. More than one student has been known to convey discomfort nonverbally by conducting the interview standing at the foot of the hospital bed, adjacent to the door and ready to escape.
Although a physician may be able to cure a disease only occasionally, the physician always can console the patient. An unknown French author admonished the medical profession “to cure sometimes, to relieve often, to comfort always.” The family physician provides personalized patient care and attempts to minimize the often frightening and dehumanizing experience to which patients are subjected in our highly structured modern medical system. The physician must strive constantly to preserve personal dignity for the patient, especially when his or her identity is threatened by a strange and somewhat frightening hospital environment. Care for a patient is more personal than the care of a patient.
Most patients have some degree of stress related to their presenting complaint, and it is important that family physicians convey a sense of caring when attempting to resolve the problem. As Fuller (1993) stated, “On a daily basis, I assess the disease process and adjust the medical management as needed, but my joy comes from listening carefully, helping people to identify their stressors, providing my best advice when I think it is appropriate, but always offering my caring and understanding. … I am both rewarded and fascinated to observe that people feel better just by recognizing that I care.” One of his patients said it best: “No one cares how much you know, until they know how much you care.”