Appendix D Herbs and children: basic dosage rules
Given the difficulties with metabolism of xenobiotics in young children, it is acknowledged in conventional medicine that dosing in young children is an imprecise affair. The following quotation from Neonatal and Pediatric Pharmacology: Therapeutic Principles in Practice, a major textbook in the field, is relevant:1
Optimal tailoring of a drug’s (and we can also read herb’s) dose to the newborn infant and child is a delicate obligation of the treating physician. All suggestions and dosing rules that have been proposed reveal the complexity of the problem. No universal dosage rule can be recommended.
So with that in mind, and the need to be flexible and to use our judgement, the various dosing rules (including briefly how they were developed) are discussed below.2
Dosage rules are based on age, weight and, more recently (in the last few decades), the sophisticated concept of body surface area. Most experts agree that body surface area is probably the most valid concept to use in terms of dosage calculations, but the computations can be very complex. There are some simple dosage rules that approximate body surface area (BSA) and can be used as a good substitute in the clinic (see later). The earlier dosage rules used age as the basis for calculation, and Dilling’s rule, which is simply the age in years divided by 20 as the fraction of the adult dose, is the oldest. Dilling’s rule is said to date from the 8th century, so even as long ago as this it was recognised that a dosage rule for children was needed. This is a very simple rule; in fact, it is overly simplistic and not recommended. Note that in the context of this and other dosage rules, the ‘adult dose’ is the dose for an adult under similar circumstances.
One of the most commonly used age-based rules, which is more sophisticated and reasonable to use, is Young’s rule. The formula is age in years divided by age plus 12 as the fraction of the adult dose. It is debated whether Young’s rule becomes valid at the age of 1 or 2, so that is why its applicable range is variously given as children aged 1 to 12 years or children age 2 to 12. A very useful age-based rule for infants is Fried’s rule, which is age in months divided by 150 as the fraction of the adult dose. It dictates quite low doses to infants. For example, in the case of a neonate up to 1 month, only 1/150th of the adult dose is given. Fried’s rule is a conservative dosage rule, but it should be considered for children up to about 2 years. Where this rule cuts out and another rule cuts in requires some discretion, and the discretionary aspects of Fried’s rule will be discussed later. Another age-based rule that is less useful is Gabius’ rule which is a simple fixed relationship between age and the fraction of the adult dose: 1 year is 1/12th, 2 years is 1/8th and 3 years 1/6th and so on.
More relevant and useful are the weight-based rules; the first such rule was said to have been proposed by Clark in the 1930s, less than 100 years ago. Only at that time were we becoming sophisticated about understanding dosage rules for children, so this is a very recent phenomenon. Clark’s rule was developed in the days before metric weights were widely used in medicine and so was based on pounds. It is weight in pounds divided by 150 as the fraction of the adult dose. This rule is not very sophisticated and not that useful. A much better rule, that represents a refinement of Clark’s rule, was developed by Augsberger in the 1960s. He added a factor of 10, in recognition of the faster metabolism of children. The rule is one and a half times the weight in kilograms plus 10 as the percentage of the adult dose. If a child weighs 20 kg, the calculation is 1½ times 20, which equals 30, plus 10, giving 40. Hence, the percentage of the adult dose from Augsberger’s rule for this example is 40%. As noted previously, most experts agree that BSA is the best parameter to use in any dosage calculation. Augsberger’s rule has been shown to be a good approximation to a body surface area curve in children.3
A group of anaesthetists at Salisbury Hospital in the UK have come up with a very simple rule that closely approximates BSA calculations.3 Anaesthetists, of course, have to know about giving the right doses to children. The rule is weight in kg times 2 as the percentage of the adult dose if the weight of the child is less than 30 kg, and weight plus 30 if the weight is greater than 30 kg. This is called the Salisbury rule. So for a 20 kg child the dose is 40% (20 times 2) of the adult dose. However, for a 35 kg child the dose is 65% (35 plus 30) of the adult dose.
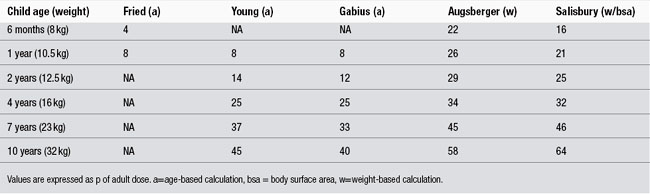
Table 1 provides a comparison of the calculations from the different dosage rules expressed as a percentage of the adult dose. Naturally, the weights of different children vary for any given age, so average weights were used for the purpose of comparison. For the Fried, Young and Gabius rules, and there is an (a) indicating they are based on age. For the Augsberger and Salisbury rules, there is a (w) to indicate they are based on weight, although for the Salisbury rule BSA is added, because that is actually what it aims to approximate. Looking first at the example of a 10-year-old child (average weight 32 kg), the table indicates that there is not a large variation from the various rules that are applicable. The Augsberger and Salisbury rules are in quite good agreement at around 60% of the adult dose. Gabius’ and Young’s rule tend to be around 40% and probably predict doses that are too low. This is where the age-based rules probably break down: for an older child they tend to lead to underdosing. Looking now at a very young child, say 6 months, there are marked differences. Young’s and Gabius’ rules do not apply. Fried’s rule predicts 4% of the adult dose, Augsberger’s predicts 22% and the Salisbury rule indicates 16%. Probably the most accurate rule in this context is the 16% from the Salisbury rule, but we need to take into account that infants have a very high degree of uncertainty because of the factors discussed previously. Consequently, Fried’s rule is recommended as the starting point for dosage in such young patients. The dose can be subsequently adjusted upwards, depending on the response of the patient. But it should be adjusted to no more than that indicated by the Salisbury rule.
The key dosage rules are summarised in Table 2 and the summary recommendations are as follows: for children aged 2 years or older, Augsberger’s or the Salisbury rule can be used. For infants less than 2 years, caution dictates that Fried’s rule should be used as the dosage starting point, working on the basis of beginning with the minimum effective dosage. This is especially the case when using alcohol-based extracts. The dose can then be increased if necessary towards that predicted by the Salisbury rule, but applying Augsberger’s rule to infants is not recommended because it will typically result in overdosing.
Table 2 Summary of key dosage rules
| Young’s rule | age/(age+12) is the FRACTION of the adult dose where age=age in years |
| Fried’s rule | (age in months/150) is the FRACTION of the adult dose used for infants up to 24 months |
| Augsberger’s rule | ((1.5×weight(kg))+10) is the PERCENTAGE of the adult dose |
| Salisbury rule | weight(kg)×2 (if weight <30 kg) is the PERCENTAGE of the adult dose weight(kg)+30 (if weight >30 kg) is the PERCENTAGE of the adult dose |
While infants do tend to have a reduced capacity to metabolise alcohol, it is usually fully developed by the age of 2 or 3. However, alcohol-based extracts can be given to young children without any associated problems if the above dosage guidelines are observed. As long as these rules are followed, it is safe to give an ethanolic extract to children of any age.
References
1. Sumner JY, Jacob VA, eds. Neonatal and Pediatric: Pharmacology Therapeutic Principles in Practice, 3rd ed., USA: Lippincott Williams & Wilkins, 2004. p. 37
2. Santich R, Bone KM. Healthy Children: Optimising Children’s Health with Herbs. Warwick: Phytotherapy Press, 2008.
3. Lack JA, Stuart-Taylor ME. Br J Anaesth. 1997;78:601–605.