Care of the Patient With a Gastrointestinal Disorder
Objectives
Anatomy and Physiology
1. List in sequence each of the parts or segments of the alimentary canal and identify the accessory organs of digestion.
2. Discuss the function of each digestive and accessory organ.
Medical-Surgical
3. Discuss the laboratory and diagnostic examinations associated with the gastrointestinal system.
4. Identify nursing interventions associated with disorders of the gastrointestinal tract.
5. Explain the etiology and pathophysiology, clinical manifestations, assessments, diagnostic tests, medical-surgical management, and nursing interventions for the patient with disorders of the mouth, esophagus, stomach, and intestines.
6. Identify nursing interventions for preoperative and postoperative care of the patient who requires gastric surgery.
7. Compare and contrast the inflammatory bowel diseases of ulcerative colitis and Crohn's disease.
8. Identify nursing interventions for the patient with a stoma for fecal diversion.
9. Discuss the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, and nursing interventions for the patient with acute abdominal inflammations (appendicitis, diverticulitis, and peritonitis), for the patient with hernias, and for the patient with colorectal cancer.
10. Differentiate between mechanical and nonmechanical intestinal obstruction, including causes, medical management, and nursing interventions.
11. Explain the etiologies, medical management, and nursing interventions for the patient with fecal incontinence.
Key Terms
http://evolve.elsevier.com/Cooper/adult/
Anatomy and Physiology of the Gastrointestinal System
Digestive System
The digestive tract, or alimentary canal, is a muscular tube containing a mucous membrane lining that extends from the mouth to the anus (Figure 5-1), and is approximately 9 meters (30 feet) long. It consists of the mouth, pharynx, esophagus, stomach, small intestine, large intestine, and anus. Peristalsis is the coordinated, rhythmic, sequential contraction of smooth muscle that pushes food through the digestive tract, as well as bile through the bile duct.
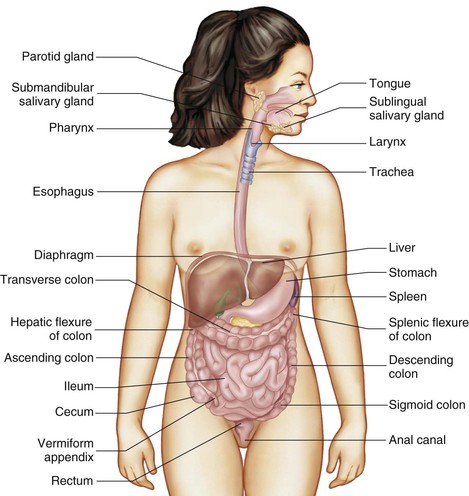
Accessory organs aid in the digestive process but are not considered part of the digestive tract. They release chemicals into the system through a series of ducts. The teeth, tongue, salivary glands, liver, gallbladder, pancreas, and appendix are considered accessory organs.
Organs of the Digestive System and Their Functions 
Box 5-1 lists various organs of the digestive system and the accessory organs involved in digestion.
Mouth.
The mouth marks the entrance to the digestive system. The floor of the mouth contains a muscular appendage, the tongue. The tongue is involved in chewing, swallowing, and the formation of speech. Tiny elevations, called papillae, contain the taste buds. They differentiate between bitter, sweet, sour, and salty sensations.
Digestion begins in the mouth. Here the teeth mechanically shred and grind food and enzymes begin the chemical breakdown of carbohydrates.
Teeth.
Each tooth is designed to carry out a specific task. At the front of the mouth are the incisors, which are structured for biting and cutting. Posterior to the incisors are the canines, pointed teeth used for tearing and shredding food. The molars are to the rear of the jaw. These teeth have four cusps (points) and are used for mastication (the crushing and grinding of food).
Salivary glands.
The three pairs of salivary glands are the parotid, submandibular, and sublingual glands (see Figure 5-1). They secrete fluid called saliva, which is approximately 99% water with enzymes and mucus. Normally these glands secrete enough saliva to keep the mucous membranes of the mouth moist. Once food enters the mouth, the secretion increases to lubricate and dissolve the food and to begin the chemical process of digestion. The salivary glands secrete about 1000 to 1500 mL of saliva daily. The major enzyme is salivary amylase (ptyalin), which initiates carbohydrate metabolism. Another enzyme, lysozyme, destroys bacteria and thus protects the mucous membrane from infections and the teeth from decay. After food has been ingested, the salivary glands continue to secrete saliva, which cleanses the mouth.
Esophagus.
The esophagus is a muscular, collapsible tube that is approximately 25 cm (10 inches) long, extending from the mouth through the thoracic cavity and the esophageal hiatus (a hole in the diaphragm) to the stomach. Digestion does not take place in the esophagus. Peristalsis moves the bolus (food broken down and mixed with saliva, ready to pass to the stomach) through the pharynx, to the esophagus, and then to the stomach in 5 or 6 seconds.
Stomach. 
The stomach is in the left upper quadrant of the abdomen, directly inferior to the diaphragm (Figure 5-2). A filled stomach is the size of a football and can hold a volume of approximately 1 to 1.5 L. The stomach entrance is at the cardiac sphincter (so named because it is close to the heart); the exit is at the pyloric sphincter. As food leaves the esophagus, it enters the stomach through the relaxed cardiac sphincter. The sphincter then contracts, preventing reflux (splashing or return flow), which can be irritating to the esophagus.
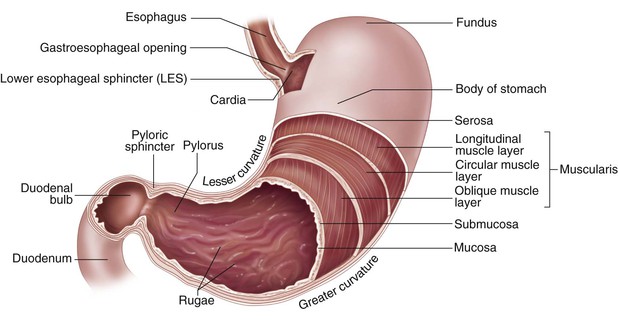
Once the bolus has entered the stomach, the muscular layers of the stomach churn and contract to mix and compress the contents with the gastric juices and water. The gastric juices are secretions released by the gastric glands. Digestion of protein begins in the stomach. Hydrochloric acid softens the connective tissue of meats, kills bacteria, and activates pepsin (the chief enzyme of gastric juices that converts proteins into proteoses and peptones). Mucin is released to protect the stomach lining. Intrinsic factor (a substance secreted by the gastric mucosa) is produced to allow absorption of vitamin B12. The stomach breaks the food down into a viscous semiliquid substance called chyme. The chyme passes through the pyloric sphincter into the duodenum for the next phase of digestion.
Small intestine.
The small intestine (Figure 5-3) is a tube that is 6 meters (20 feet) long and 2.5 cm (1 inch) in diameter. It begins at the pyloric sphincter, ends at the ileocecal valve, and is divided into three major sections: duodenum, jejunum, and ileum. Up to 90% of digestion takes place in the small intestine. The intestinal juices finish the metabolism of carbohydrates and proteins. Bile and pancreatic juices enter the duodenum. Bile from the liver breaks molecules into smaller droplets, which enables the digestive juices to complete their process. Pancreatic juices contain water, protein, inorganic salts, and enzymes. Pancreatic juices are essential in breaking down proteins into their amino acid components, in reducing dietary fats to glycerol and fatty acids, and in converting starch to simple sugars.
The inner surface of the small intestine contains millions of tiny fingerlike projections called villi, which are clustered over the entire mucous membrane surface. The villi aid in the digestive process by absorbing the products of digestion into the bloodstream. They increase the absorption area of the small intestine by about 600 times. Inside each villus is a rich capillary bed, along with modified lymph capillaries called lacteals. The primary function of the lacteals is to absorb metabolized fats.
Large intestine.
Once the small intestine has completed its tasks of digestion, the ileocecal valve opens and releases the contents of digestion into the large intestine. The large intestine is a tube that is larger in diameter (6 cm, or 2 inches), but shorter at 1.5 to 1.8 meters (5 to 6 feet), than the small intestine. The large intestine consists of the cecum; appendix; ascending colon, hepatic flexure, transverse colon, splenic flexure, descending colon, and sigmoid colon; rectum; and anus (Figure 5-4). This is the terminal portion of the digestive tract, where the process of digestion is completed. The large intestine has four major functions: (1) completion of absorption of water, (2) manufacture of certain vitamins (such as vitamins K and B7), (3) formation of feces, and (4) expulsion of feces.
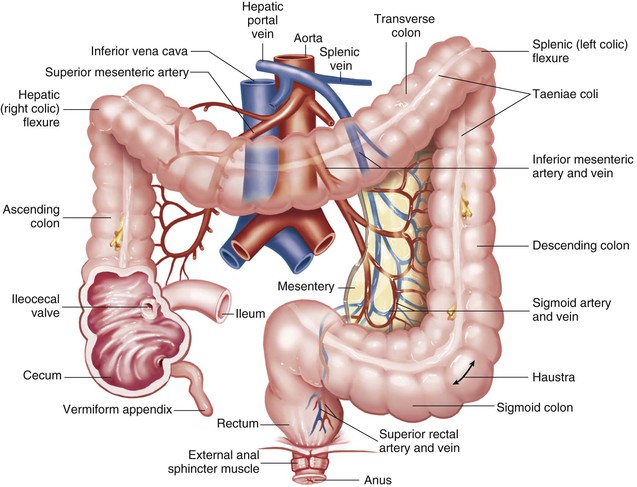
Just inferior to the ileocecal valve is the cecum, a blind pouch approximately 2 to 3 inches long. The vermiform appendix, a small wormlike, tubular structure, dangles from the cecum. Research has revealed that the appendix functions as an area where nonpathologic bacteria live safely until they are needed for digestion. In addition, the appendix houses immune system cells and tissue (Duke University Medical Center, 2007). The open end of the cecum connects to the ascending colon, which continues upward on the right side of the abdomen to the inferior area of the liver. The ascending colon then becomes the transverse colon. It crosses to the left side of the abdomen, where it becomes the descending colon. When the descending colon reaches the level of the iliac crest, the sigmoid colon begins and continues toward the midline to the level of the third sacral vertebra.
Bacteria in the large intestine change the chyme into fecal material by releasing the remaining nutrients. The bacteria are also responsible for the synthesis of vitamin K, which is needed for normal blood clotting, and the production of some of the B-complex vitamins. As the fecal material continues its journey, the remaining water and vitamins are absorbed into the bloodstream by osmosis.
Rectum.
The rectum is the last 20 cm (8 inches) of the intestine, where fecal material is expelled. The anus is the opening to the outside of the body where feces are passed.
Accessory Organs of Digestion
Liver
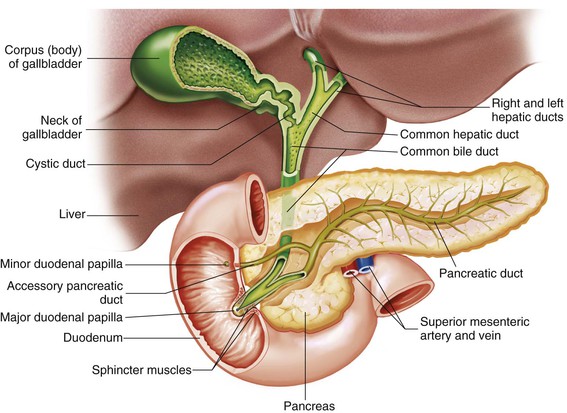
The liver is the largest glandular organ in the body, weighing approximately 1.5 kg (3 to 4 pounds) in the adult, and is one of the more complex organs in the body. It is located just inferior to the diaphragm, covering most of the upper right quadrant and extending into the left epigastrium, and it is divided into two lobes. The lobes are further divided into several lobules (smaller lobes) containing small blood vessels. Approximately 1500 mL of blood is delivered to the liver every minute by the portal vein and the hepatic portal artery. The cells of the liver produce a product called bile, a yellow-brown or green-brown liquid; bile is necessary for the emulsification of fats. The liver releases approximately 500 to 1000 mL of bile per day, which then travels to the gallbladder through hepatic ducts. The gallbladder is a sac about 8 to 9 cm (3 to 4 inches) long, located on the right inferior surface of the liver. Bile is stored in the gallbladder until it is needed for fat digestion (Figure 5-5).
In addition to producing bile, the liver's functions include managing blood coagulation; metabolizing proteins, fats, and carbohydrates; manufacturing cholesterol; manufacturing albumin to maintain normal blood volume; filtering out old red blood cells (RBCs) and bacteria; detoxifying poisons (alcohol, nicotine, drugs); converting ammonia to urea; providing the main source of body heat at rest; storing glycogen for later use; activating vitamin D; and breaking down nitrogenous waste (from protein metabolism) to urea, which the kidneys can excrete as waste from the body.
Gallbladder
The gallbladder is a pear-shaped organ measuring approximately 7 to 10 cm (3 to 4 inches) long. Areolar connective tissue connects it to the underside of the liver. The gallbladder can store 30 to 50 mL of bile and its primary function is to store and eject bile into the duodenum for digestion of fats.
Pancreas
The pancreas is an elongated gland, approximately 12 to 15 cm (6 to 9 inches) long, that lies posterior to the stomach (see Figure 5-4). It is involved in both endocrine and exocrine duties. In this chapter, discussion of the pancreas is limited to its exocrine activities.
Each day the pancreas produces 1000 to 1500 mL of pancreatic juice to aid in digestion. This pancreatic juice contains the digestive enzymes protease (trypsin), lipase (steapsin), and amylase (amylopsin). These enzymes are important because they digest the three major components of chyme: proteins, fats, and carbohydrates. The enzymes are transported through an excretory duct to the duodenum. This pancreatic duct connects to the common bile duct from the liver and gallbladder and empties through a small orifice in the duodenum called the major duodenal papilla. In addition, the pancreas contains an alkaline substance, sodium bicarbonate, which neutralizes hydrochloric acid in the gastric juices that enter the small intestine from the stomach.
Regulation of Food Intake
The hypothalamus, a portion of the brain, contains two appetite centers that have an effect on eating. One center stimulates the individual to eat, and the other signals the individual to stop eating. These centers work in conjunction with the rest of the brain to balance eating habits. In addition to the hypothalamus, factors that also affect food intake include lifestyle, culture, eating habits, emotions, and genetics.
Laboratory and Diagnostic Examinations
Upper Gastrointestinal Study (Upper GI Series, UGI)
Rationale
The upper gastrointestinal study (UGI) consists of a series of radiographs of the lower esophagus, stomach, and duodenum, using barium sulfate as the contrast medium. A UGI series detects any abnormal conditions of the upper gastrointestinal (GI) tract, any tumors, or other ulcerative lesions.
Nursing Interventions
The patient should take nothing by mouth (NPO) and avoid smoking after midnight the night before the study. Explain the importance of rectally expelling all the barium after the examination. Feces (stools) will be light in color until all the barium is expelled (up to 72 hours after the test). Eventual absorption of fecal water may cause a hardened barium impaction. The patient should be instructed to increase his fluid intake in order to help in expelling the barium, thus preventing constipation or blockage. The health care provider may order a laxative to be given in addition to increasing fluid intake.
Tube Gastric Analysis
Rationale
The stomach contents are aspirated to determine the amount of acid produced by the parietal cells in the stomach. The analysis helps determine the completeness of a vagotomy, confirm hypersecretion or achlorhydria (an abnormal condition characterized by the absence of hydrochloric acid in the gastric juice), estimate acid secretory capacity, or test for intrinsic factor.
Nursing Interventions
The patient should receive no anticholinergic medications for 24 hours before the test and should maintain NPO status after midnight to avoid altering the rate of gastric acid secretion. The patient should also be instructed that smoking is prohibited before the test because nicotine stimulates the flow of gastric secretions.
The nurse or radiology personnel inserts a nasogastric (NG) tube into the stomach to aspirate gastric content. Specimens are properly labeled and sent to the laboratory immediately. The NG tube is removed and the patient may eat and drink without restrictions unless otherwise ordered.
Esophagogastroduodenoscopy (EGD, UGI Endoscopy, Gastroscopy)
Rationale
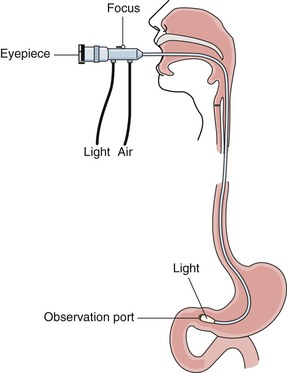
Endoscopy (from endo, within, inward; and scope, to look) enables direct visualization of a particular hollow organ or cavity by means of a long, flexible fiberoptic scope (Figure 5-6). An EGD visualizes the esophagus, stomach, and duodenum for routine screening as well as for examination of tumors, varices (abnormally enlarged veins), mucosal inflammation, hiatal hernias, polyps (small tissue growths projecting from a mucous membrane), ulcers, Helicobacter pylori, strictures (narrowings), and obstructions. The endoscopist can also remove polyps, coagulate sources of active GI bleeding, and perform sclerotherapy (injection of a solution into the vein causing it to shrink and eventually disappear) of esophageal varices. Areas of narrowing can be dilated by the endoscope itself or by passing a dilator through the scope. Camera equipment can be attached to the viewing lens to photograph a pathologic condition. The endoscope can also obtain tissue specimens for biopsy or culture to determine the presence of H. pylori.
Endoscopy enables evaluation of the esophagus, stomach, and duodenum. A longer fiberoptic scope allows evaluation of the upper small intestine. This is referred to as enteroscopy.
Nursing Interventions
The patient should maintain NPO status after midnight prior to the test, and an informed consent form must be signed. The patient is usually given a preprocedure intravenous (IV) sedative such as midazolam (Versed), and the patient's pharynx is anesthetized by spraying it with lidocaine hydrochloride (Xylocaine). Following the procedure the patient will not be allowed to eat or drink until the gag reflex returns, which is usually soon after the procedure and can be assessed by placing a tongue blade to the back of the pharynx. The patient's vital signs and oxygen saturation are monitored after the procedure, as well as assessing for any signs and symptoms of perforation, including abdominal pain and tenderness, guarding, oral bleeding, melena (tarlike, fetid-smelling stool containing undigested blood), and hypovolemic shock.
Capsule Endoscopy
Rationale
For capsule endoscopy, the patient swallows a capsule (approximately the size of a large vitamin) containing a camera that provides endoscopic evaluation of the GI tract. It is commonly used to visualize the small intestine and diagnose diseases such as Crohn's disease, celiac disease, and malabsorption syndrome. It also helps identify sources of possible GI bleeding in areas not accessible by upper endoscopy or colonoscopy. The camera takes tens of thousands of images during an 8-hour examination. The capsule relays images to a data recorder that the patient wears on a belt. After the examination, images are viewed on a monitor (Mayo Clinic, 2012a).
Nursing Interventions
The patient will be NPO for approximately 10 hours prior to the test and should not smoke for 24 hours prior to the test. The patient swallows the video capsule and is usually kept NPO until 4 to 6 hours later. The procedure is comfortable for most patients. Eight hours after swallowing the capsule, the patient returns to have the monitoring device removed. Peristalsis causes passage of the disposable capsule with a bowel movement, usually in 2 to 3 days. The pill camera does not need to be retrieved (American Gastroenterological Association, 2010).
Barium Swallow and Gastrografin Studies
Rationale
A barium swallow study allows a clearer view of the esophagus than that provided by most UGI examinations; this is because the esophageal movements don't show up well on x-rays. When the patient swallows barium, however, the outline of the esophagus is quite clear. As in most barium contrast studies, defects in luminal filling and narrowing of the barium column indicate tumor, scarred stricture, or esophageal varices. A barium swallow allows easy recognition of swallowing difficulties resulting from conditions such as cerebrovascular accidents (stroke or brain attack), and of anatomical abnormalities, such as hiatal hernia. Cancers of the esophagus, gastroesophageal reflux disease (GERD) and ulcers, and muscle disorders are other reasons for a barium swallow to be performed (Johns Hopkins University, n.d.).
Gastrografin (diatrizoate meglumine and diatrizoate sodium) is a product used in place of barium for patients who are susceptible to bleeding from the GI tract and who are being considered for surgery. Gastrografin is water soluble and rapidly absorbed, so it is preferable when a perforation is suspected. Gastrografin facilitates imaging through radiographs, but if the product escapes from the GI tract, it is absorbed by the surrounding tissue. In contrast, if barium leaks from the GI tract, it is not absorbed and can lead to complications (eMC, 2012).
Nursing Interventions
The patient is NPO after midnight. Food and fluid in the stomach prevent barium from accurately outlining the GI tract, and the radiographic results may be misleading. Explain the importance of rectally expelling all barium. Stools will be light in color until this occurs. Eventual absorption of fecal water may cause a hardened barium impaction. The patient should be instructed to increase his or her fluid intake to help in expelling the barium, thus preventing constipation or blockage. The health care provider may order a laxative to be given in addition to increasing fluid intake.
Esophageal Function Studies (Bernstein Test)
Rationale
The Bernstein test, an acid perfusion test, is an attempt to reproduce the symptoms of gastroesophageal reflux. It helps differentiate esophageal pain caused by esophageal reflux from that caused by angina pectoris. If the patient suffers pain with the instillation of hydrochloric acid into the esophagus, the test is positive and indicates reflux esophagitis (National Library of Medicine [NLM], 2012a).
Nursing Interventions
The patient is NPO for 8 hours before the examination, and any medications that may interfere with the production of acid, such as antacids and analgesics, are withheld. An NG tube is inserted and mild hydrochloric acid is instilled followed by saline. The patient will be asked if any pain or discomfort is felt during instillation of the hydrochloric acid.
Examination of Stool for Occult Blood
Rationale
Tumors of the large intestine grow into the lumen (the cavity or channel within a tube or tubular organ) and are subject to repeated trauma by the fecal stream. Eventually the tumor ulcerates and bleeding occurs. Sometimes the bleeding is so slight that gross blood is not seen in the stool. If this occult blood (blood that is obscure or hidden from view) is detected in the stool, a benign or malignant GI tumor is suspected. Tests for occult blood include the stool guaiac test, Hemoccult test, and Hematest.
Occult blood in the stool may also occur in ulceration and inflammation of the upper or lower GI system, as well as with internal hemorrhoids that are bleeding. Other causes include swallowing blood of oral or nasopharyngeal origin. For specimen collection the patient is usually asked to collect stool in an appropriate container.
Nursing Interventions
The patient is instructed to keep the stool specimen free of urine or toilet paper, since either can alter the test results. The nurse or patient should don gloves and use tongue blades or an appropriate specimen collection device for stool to transfer the stool to the proper receptacle. The patient should not eat any organ meat for 24 to 48 hours before a guaiac test. A specimen slide and developer are used by the nurse to test the stool for occult blood. The health care provider sometimes orders that three consecutive stools be tested for occult blood.
Sigmoidoscopy (Lower GI Endoscopy)
Rationale
Endoscopy of the lower GI tract allows visualization of the inner lining of the sigmoid colon and, if indicated, access to obtain biopsy specimens of tumors, polyps, or ulcerations of the anus, rectum, and sigmoid colon. The lower GI tract is difficult to visualize radiographically, but sigmoidoscopy allows direct visualization. Microscopic review of tissue specimens obtained using this procedure lead to diagnoses of many lower bowel disorders.
Nursing Interventions
The patient should maintain NPO status after midnight prior to the test and an informed consent form must be signed. The specific bowel preparation is determined by the health care provider performing the procedure, usually a gastroenterologist, and usually consists of laxatives, enemas, or a combination of both. After the examination, the patient should be observed for evidence of bowel perforation (abdominal pain, tenderness, distention, and bleeding), and should be instructed to watch for these symptoms at home.
Barium Enema Study (Lower GI Series)
Rationale
The barium enema (BE) study consists of a series of radiographs of the colon used to detect the presence and location of abnormalities such as polyps, tumors, and diverticula. Barium sulfate also assists in visualization of mucosal detail. Therapeutically, a BE may be used to reduce (treat) a nonstrangulated ileocolic intussusception (infolding of one segment of the intestine into the lumen of another segment) in children (Punnoose, 2012). The contrast agent causes the infolded portion to move back into its normal position.
Nursing Interventions
The evening before the BE, cathartics such as magnesium citrate, or other cathartics designated by facility policy, are administered. A cleansing enema the evening before or the morning of the BE is administered if directed by the health care provider's order or facility policy. Fluids should be encouraged and a laxative may be ordered after the BE to stimulate evacuation of the barium.
After the BE study, the nurse should assess the patient for complete evacuation of the barium, or instruct the patient to monitor stools at home. Patients typically expel most of the barium prior to leaving the radiology department. Retained barium may cause constipation or a hardened impaction. Stool will be light in color until all the barium has been expelled.
Colonoscopy
Rationale
The development of the fiberoptic colonoscope has enabled examination of the entire colon, from the anus to the cecum, in most patients. Colonoscopy can detect lesions in the proximal colon, which would not be found by sigmoidoscopy. Benign and malignant neoplasms, mucosal inflammation or ulceration, and sites of active hemorrhage can also be visualized. Biopsy specimens can be obtained and small tumors removed through the scope. Actively bleeding vessels can be coagulated.
A less invasive test than a standard colonoscopy is called virtual colonoscopy. This test uses computed tomography (CT) scanning or magnetic resonance imaging (MRI) with computer software to produce images of the colon and rectum. For both procedures a small tube is inserted through the anus and into the rectum. With the CT procedure the colon is expanded by instillation of carbon dioxide gas, to aid in visualization. For the MRI method a contrast medium is given to expand the colon. The colon preparation is similar to that for a regular colonoscopic examination. Sedatives are not required and no scope is needed. One disadvantage of this procedure is that it does not allow for biopsies, removal of polyps, or coagulation of vessels (National Digestive Disease Information Clearinghouse [NDDIC], 2012). Patients who have had cancer of the colon are at high risk for developing a subsequent colon cancer; patients who have a family history of colon cancer are also at high risk. For these patients, colonoscopy allows early detection of any primary or secondary tumors.
Nursing Interventions
Informed consent is necessary for a colonoscopy to be performed. Dietary restrictions include a clear liquid diet for 1 to 3 days before the procedure in order to decrease the residue in the bowel, and then NPO status is maintained for 8 hours before the procedure. Laxatives and/or enemas, and premedication, such as a stool softener, are ordered to cleanse the bowel. The bowel preparation will depend on the health care provider's preference and the patient's condition.
After the colonoscopy, the patient must be monitored for evidence of bowel perforation (abdominal pain, guarding, distention, tenderness, excessive rectal bleeding, or blood clots) and the stools should be examined for gross blood. The patient should also be monitored for hypovolemic shock.
Stool Culture
Rationale
The feces (stool) can be examined for the presence of bacteria, ova, and parasites (a plant or animal that lives on or within another living organism and obtains some advantage at its host's expense). The health care provider may order a stool for culture of bacteria or of ova and parasites (O&P). Many bacteria (such as Escherichia coli) are indigenous in the bowel. Bacterial cultures are usually done to detect enteropathogens (such as Staphylococcus aureus, Salmonella or Shigella organisms, E. coli O157:H7, or Clostridium difficile) (Centers for Disease Control and Prevention [CDC], 2013).
When a patient is suspected of having a parasitic infection, the stool is examined for O&P. Usually at least three stool specimens are collected on consecutive days. Because culture results are not available for several days, they do not influence initial treatment, but they do guide subsequent treatment if bacterial infection is present.
Nursing Interventions
If an enema must be administered to collect specimens, only normal saline or tap water is used. Soapsuds or any other substance could affect the viability of the organisms collected.
Stool samples for O&P are obtained before barium examinations. The nurse must be sure that urine is not mixed with feces in the sample. Gloves are worn for sample collection and the specimen is taken to the laboratory within 30 minutes of collection in a specified container.
Obstruction Series (Flat Plate of the Abdomen)
Rationale
The obstruction series is a group of radiographic studies performed on the abdomen of patients who have suspected bowel obstruction, paralytic ileus, perforated viscus (a viscus is any large interior organ in any of the great body cavities), or abdominal abscess. The series usually consists of at least two radiographic studies. The first is an erect abdominal radiographic study that allows visualization of the diaphragm. Radiographs are examined for evidence of free air under the diaphragm, which is pathognomonic (signs or symptoms specific to a disease condition) of a perforated viscus (hollow organ). This radiographic study is also used to detect air–fluid levels within the intestine (NLM, 2013).
Nursing Interventions
For adequate visualization, the nurse must ensure that this study is scheduled before any barium studies.
Disorders of the Mouth
Common disorders of the mouth and esophagus that interfere with adequate nutrition include poor dental hygiene, infections, inflammation, and cancer.
Dental Plaque and Caries
Etiology and Pathophysiology
Dental decay is an erosive process that results from the action of bacteria on carbohydrates in the mouth, which in turn produce acids that dissolve tooth enamel. Many Americans experience tooth decay at some time in their life. Dental decay can be caused by several factors.
• Dental plaque, a thin film on the teeth made of mucin and colloidal material found in saliva and often secondarily invaded by bacteria
• The strength of acids and the inability of the saliva to neutralize them
• The length of time the acids are in contact with the teeth
Medical Management
Dental caries are treated by removal of affected areas of the tooth and replacement with some form of dental material. Treatment of periodontal disease centers on removal of plaque from the teeth. If the disease is advanced, surgical interventions on the gingivae and alveolar bone may be necessary.
Nursing Interventions and Patient Teaching
Proper technique for brushing and flossing the teeth at least twice a day is the primary focus for teaching patients. Plaque forms continuously and must be removed periodically through regular visits to the dentist. The importance of prevention through continual care should be stressed. Because carbohydrates create an environment in which caries develop and plaque accumulates more easily, proper nutrition should be included in patient teaching. When the patient is ill, the mouth's normal cleansing action is impaired. Illnesses, drugs, and irradiation all interfere with the normal action of saliva. If the patient is unable to manage oral hygiene, the nurse must assume this responsibility.
Nursing diagnoses and interventions for the patient with dental plaque and caries include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |

Ackley BJ, Ladwig GB: Nursing diagnosis handbook: An evidence-based guide to planning care, ed 9, St. Louis, 2011, Mosby.
The prevention and elimination of dental plaque and caries are directly related to oral hygiene, dental care, nutrition, and heredity. All but heredity are controllable factors. The prognosis is more favorable for people who brush, floss, regularly visit the dentist for removal of affected areas, eat low-carbohydrate foods, and drink fluoridated water.
Candidiasis
Etiology and Pathophysiology
Candidiasis is any infection caused by a species of Candida, usually C. albicans. Candida is a fungal organism normally present in the mucous membranes of the mouth, intestinal tract, and vagina; it is also found on the skin of healthy people. This infection is also referred to as thrush or moniliasis.
This disease appears more commonly in the newborn infant, who becomes infected while passing through the birth canal. In the older individual, candidiasis may be found in patients with leukemia, diabetes mellitus, or alcoholism, and in patients who are taking antibiotics (chlortetracycline or tetracycline), are undergoing corticosteroid inhalant treatment, or are immunosuppressed (e.g., patients with acquired immunodeficiency syndrome [AIDS] or those receiving chemotherapy or radiation therapy).
Clinical Manifestations
Candidiasis appears as pearly, bluish white “milk-curd” membranous lesions on the mucous membranes of the mouth, tongue, and larynx. One or more lesions may be on the mucosa, depending on the duration of the infection (see Chapter 16, Figure 16-4 for illustration). If the patch or plaque is removed, painful bleeding can occur.
Assessment
Assessment of the patient with oral candidiasis may reveal subjective complaints of soreness, and difficulty swallowing. Angular cheilitis (cracks at the corners of the mouth) is an objective sign of oral candidiasis. Failure to eat is an objective sign of candidiasis of the GI tract that is seen in infants and adults who are unable to communicate (CDC, 2012).
Medical Management
Nystatin or amphotericin B (an oral suspension) or buccal tablets of fluconazole (Diflucan), one-third–strength hydrogen peroxide, and saline mouth rinses may provide some relief. In addition, eating unsweetened yogurt or taking acidophilus capsules or liquid can restore normal bacterial flora (NLM, 2012b).
Nursing Interventions
Meticulous hand hygiene should be used to prevent spread of the infection. For infants, hand hygiene, care of feeding equipment, and cleanliness of the mother's nipples are important to prevent spread. The infant's mouth should be assessed regularly.
For adults, the patient should be encouraged to use a soft-bristled toothbrush, and avoid hot, cold, spicy, fried, or citrus foods. A topical anesthetic such as lidocaine or benzocaine may be ordered to be administered to the mouth 1 hour before meals (Mayo Clinic, 2011).
Prognosis
If the host has a strong defense system and medical treatment is initiated early in the course of the disease, the prognosis is good.
Carcinoma of the Oral Cavity
Etiology and Pathophysiology
Oral (or oropharyngeal) cancer may occur on the lips, the oral cavity, the tongue, and the pharynx. The tonsils are occasionally involved. Most of these tumors are squamous cell epitheliomas that grow rapidly and metastasize to adjacent structures more quickly than do most malignant tumors of the skin. An estimated 41,380 new cases and 7890 deaths from oral cavity and pharynx cancer are expected to occur in 2013. Death rates have been decreasing since the 1970s, with rates declining faster in the 2000s (American Cancer Society [ACS], 2012a).
Tumors of the salivary glands occur primarily in the parotid gland and are usually benign. Tumors of the submaxillary gland have a high incidence of malignancy. These malignant tumors grow rapidly and may be accompanied by pain and impaired facial function.
Kaposi's sarcoma is a malignant skin tumor that occurs primarily on the skin or on mucosal surfaces such as in the mouth. It is seen at a rate of 6 cases per million people infected with AIDS, and at a rate of 1 in 200 for patients receiving immunosuppressive therapy following organ transplantation. The lesions are purple and nonulcerated. Irradiation is the treatment of choice (ACS, 2013a).
The types of cancers of the lip that are usually seen are basal cell carcinoma and squamous cell carcinoma. Cancer of the lip occurs most frequently as a chronic ulcer of the lower lip in men over the age of 50. The cure rate for cancer of the lip is high because the lesion is apparent to the patient and to others, so patients often seek early treatment. If early detection and treatment do not occur, metastasis to regional lymph nodes may occur. In some instances a lesion may spread rapidly and involve the mandible and the floor of the mouth by direct extension. On occasion, the tumor may be a basal cell lesion that starts in the skin and spreads to the lip (Skin Cancer Foundation, 2013).
Cancer of the anterior tongue and floor of the mouth may seem to occur together because their spread to adjacent tissues is so rapid. Because of the tongue's abundant vascular and lymphatic drainage, metastasis to the neck may occur. There is a higher incidence of cancers of the mouth and throat among people who are heavy drinkers, and who have a history of tobacco use (e.g., cigar, cigarette, pipe, chewing tobacco) and exposure to human papillomavirus (HPV) (National Cancer Institute, n.d.a). Also, data show that men are more likely to develop tongue cancer than women, and an estimated 9900 men and 3690 women will be diagnosed with tongue cancer in 2013 (ACS, 2013b).
Clinical Manifestations
Leukoplakia (a white, firmly attached patch on the mouth or tongue mucosa) may appear on the lips and buccal mucosa. These nonsloughing lesions cannot be rubbed off by simple mechanical force. They can be benign or malignant. A small percentage develop into squamous cell carcinomas, and biopsy is recommended if the lesions persist for longer than 2 weeks.
Assessment
Collection of subjective data includes understanding that malignant lesions of the mouth may be asymptomatic. The patient may feel only a roughened area with the tongue. As the disease progresses, the first complaints may be (1) difficulty in chewing, swallowing, or speaking; (2) edema, numbness, or loss of feeling in any part of the mouth; and (3) earache, facial pain, and toothache, which may become constant. Cancer of the lip is associated with discomfort and irritation caused by a nonhealing lesion, which may be raised or ulcerated. Malignancy at the base of the tongue produces less obvious symptoms: slight dysphagia (difficulty in swallowing), sore throat, and salivation. Most oral cancers occur in males over the age of 60, but it is important for the nurse to not overlook symptoms based on age and gender.
Diagnostic Tests
Direct and indirect laryngoscopy are important diagnostic tests for examination of the soft tissue. This procedure allows direct visualization of the oral cavity and both can be performed in the health care provider's office. If necessary, panendoscopy—a more invasive form of laryngoscopy—may be performed with an endoscope. Radiographic evaluation of the mandibular structures is another essential part of the head and neck examination to rule out cancer. Excisional biopsy is the most accurate method for making a definitive diagnosis. Oral exfoliative cytology, in which a scraping of a lesion provides cells for cytologic examination, is used to screen intraoral lesions (ACS, 2013c).
Medical Management
Treatment depends on the location and staging of the malignant tumor. Stage I oral cancers are treated by surgery or radiation. Stage II and III cancers require both surgery and radiation. Chemotherapy may also be used when surgery and radiation therapy fail or as the initial therapy for smaller tumors. Treatment for stage IV cancer may include all three treatment modalities, or treatment may be palliative if metastasis is extensive. The 5-year survival rate for patients with oral cancers that have metastasized averages less than 50% (National Cancer Institute, n.d.b.).
Small, accessible tumors can be excised surgically. Surgical options include a glossectomy, removal of the tongue; hemiglossectomy, removal of part of the tongue; mandibulectomy, removal of the mandible; and total or supraglottic laryngectomy, removal of the entire larynx or the portion above the true vocal cords.
Large tumors usually require more extensive and traumatic surgery. In a functional neck dissection of neck cancer with no growth in the lymph nodes, the surgeon removes the lymph nodes but preserves the jugular vein, the sternocleidomastoid muscle, and the spinal accessory nerve. In radical neck dissection, all these structures are removed and reconstructive surgery is necessary after tissue resection. Patients may have drains in the incision sites that are connected to suction to aid healing and reduce hematomas. A tracheostomy may also be performed, depending on the degree of tumor invasion.
Because of the location of the surgery, complications can occur. These include airway obstruction, hemorrhage, tracheal aspiration, facial edema, formation of fistulas (abnormal passages connecting internal organs, or to the surface of the body), and necrosis of the skin flaps. If the patient has difficulty swallowing, a percutaneous endoscopic gastrostomy (PEG) tube may be inserted to allow for adequate nutritional intake. Neurologic complications can occur because of nerves being severed and manipulated during surgery.
Radiation therapy may involve (1) external radiation beam radiation therapy or (2) internal radiation by means of needles or seeds. The purpose of radiation therapy is to shrink the tumor. It can be given preoperatively or postoperatively, depending on the health care provider's preference and the patient's disease process. In more advanced cases, chemotherapy may be combined with radiation postoperatively to make the patient more comfortable. Other treatment options include laser excision.
Nursing Interventions and Patient Teaching
A holistic approach to patient care includes awareness of the patient's level of knowledge regarding the disease, emotional response and coping abilities, and spiritual needs. Nursing interventions must be individualized to the patient—beginning with the preoperative stage, continuing through the postoperative stage, and ending after the patient's rehabilitation in the home environment. Family members, hospice workers, close friends, social workers, and pastoral care staff may provide information and support during this potentially fatal disease.
Nursing diagnoses and interventions for the patient with oral cancer include but are not limited to the following:

From Ackley BJ, Ladwig GB: Nursing diagnosis handbook: An evidence-based guide to planning care, ed 9, St. Louis, 2011, Mosby.
Prevention is the key to successful treatment or cure for cancer of the oral cavity, and should include education on avoiding excess exposure to sun and wind on the lips, eliminating smoking or chewing tobacco, eliminating plaque and caries through good oral and dental care, and decreasing the intake of excessive amounts of alcohol. Individuals infected with HPV should also be monitored for the development of oral cavity cancer. Early detection of oral cancer can increase the patient's chance of survival. Any person with a mouth lesion that does not heal within 2 to 3 weeks is urged to seek medical care.
The nurse should provide instruction regarding preoperative and postoperative care, with full explanations regarding potential speech loss and alternative methods of nutritional intake if warranted by the extent of cancer or anticipated surgical procedure. Explanation of tracheostomy care and other tubes the patient may have on discharge helps reduce anxiety and increase the patient's sense of control over the situation.
Prognosis
Staging and biologic characterization of the neoplasm provide prognostic information. The prognosis of carcinoma in the oral cavity is directly related to the size of the primary tumor, the involvement of regional lymph nodes, and the presence or absence of metastasis. The patient's immunologic response and general condition also influence the prognosis and the choice of therapy.
Carcinomas of the lip can generally be detected early by the patient, the health care provider, or the dentist during examination, and the prognosis for cure is good. If the carcinoma is difficult to detect, as on the anterior tongue and the floor of the mouth, it is often in a more advanced stage when detected, making the prognosis poor.
Disorders of the Esophagus
Gastroesophageal Reflux Disease
Etiology and Pathophysiology
Gastroesophageal reflux disease (GERD) is a backward flow of stomach acid up into the esophagus. Symptoms typically include burning and pressure behind the sternum, often described by patients as heartburn. Most cases are thought to be caused by the inappropriate relaxation of the lower esophageal sphincter (LES) in response to an unknown stimulus. Symptoms of GERD develop when the LES is weak or experiences prolonged or frequent transient relaxation, conditions that allow gastric acids and enzymes to flow into the esophagus. Reflux is much more common in the postprandial state (after meals) as this position allows more reflux of gastric juices when the LES is relaxed. GERD occurs in all age groups and is estimated to affect approximately 19 million people. GERD is the most common upper GI problem seen in adults (American Gastrointestinal Association, 2011).
Clinical Manifestations
The clinical manifestations of GERD are consistent, but vary substantially in severity. The irritation of chronic reflux produces the primary symptom, which is heartburn (pyrosis). Heartburn is often described as a substernal or retrosternal burning sensation that tends to radiate upward and may involve the neck, the jaw, or the back. Heartburn is usually experienced after eating. An atypical pain pattern that closely mimics angina may also occur and must be carefully differentiated from true cardiac disease. The second major symptom of GERD is regurgitation. The individual experiences a feeling of warm fluid moving up the throat and may experience a sour taste in the mouth (Mayo Clinic, 2012b; Livestrong, 2010).
GERD can produce symptoms such as dysphagia or odynophagia (painful swallowing), dry cough, hoarseness, and a sore throat. Eructation (belching) and a feeling of flatulence are other common complaints. The frequency and severity of reflux episodes usually determine the severity of the symptoms.
Assessment
Subjective data include heartburn, a substernal or retrosternal burning sensation that may radiate to the back or jaw (in some cases the pain may mimic angina); and regurgitation, which causes a sour or bitter taste in the pharynx. Frequent eructation, flatulence, and dysphagia or odynophagia usually occur only in severe cases.
Objective data include nocturnal cough, wheezing, and hoarseness.
Diagnostic Tests
When a mild case of GERD is suspected, treatment is initiated on the basis of the presumptive diagnosis. More involved cases may require other screening tools such as esophageal pH test. In this test the patient is fitted with a small nasogastric tube that remains in place and is connected to a small computer that may be worn on the belt or on a shoulder strap. The probe, in the esophagus, monitors acid levels for 24 to 48 hours. An esophageal motility test and Bernstein test can be performed in conjunction with pH monitoring to evaluate LES competence and the response of the esophagus to acid infusion. The barium swallow with fluoroscopy is widely used to document the presence of hiatal hernia. Endoscopy is routinely performed to evaluate for LES competence, potential scarring and strictures, and the presence and severity of esophagitis, and to rule out malignancy (Kahrilas, 2012).
Medical Management
In its simplest form, GERD produces mild symptoms that occur infrequently (twice a week or less). In these cases, encouraging the patient to avoid problem foods or beverages, stopping smoking, elevating the head of the bed, or losing weight may solve the problem. Medication therapy for GERD focuses on improving LES function, increasing esophageal clearance, decreasing volume and acidity of reflux, and protecting the esophageal mucosa. Treatment with antacids or acid-blocking medications called H2 receptor antagonists—such as cimetidine (Tagamet), ranitidine (Zantac), famotidine (Pepcid), or nizatidine (Axid)—may also be used. More severe and frequent episodes of GERD can trigger asthma attacks, cause severe chest pain, result in bleeding, or promote a narrowing (stricture) or chronic irritation of the esophagus. In these cases, more powerful inhibitors of stomach acid production called proton pump inhibitors (PPIs), such as omeprazole (Prilosec), esomeprazole (Nexium), pantoprazole (Protonix), rabeprazole (Aciphex), and lansoprazole (Prevacid), may be added to the treatment prescribed. Sucralfate (Carafate) is an antiulcer drug that may be used in patients with GERD for its protective properties by forming a complex that adheres to an ulcer. Metoclopramide (Reglan) is used in moderate to severe cases of GERD. It is in a class of drugs called promotility agents, which increase peristalsis and therefore promote gastric emptying and reduce the risk of gastric acid reflux.
If conventional treatments fail, the health care provider may suggest a surgical procedure to treat the condition. Nissen fundoplication is one surgical procedure that can be performed to strengthen the sphincter. The procedure involves wrapping a layer of the upper stomach wall (fundus) around the sphincter and terminal esophagus to lessen the possibility of acid reflux (see Figure 5-14). Surgery may also be performed to create a barrier that will prevent the backup of gastric acid. A device called an EsophyX folds the tissue at the base of the stomach, acting as a sphincter valve. Another surgical approach is the Stretta procedure. This procedure uses electrodes to heat the tissue in the esophagus in order to create scar tissue that strengthens the esophagus. The LINX is another surgical device that is used to treat GERD; it consists of a band of titanium beads with magnetic cores that, when implanted around the LES, strengthens it by closing the sphincter when necessary. If GERD is left untreated, serious pathologic (precancerous) changes in the esophageal lining may develop—a condition called Barrett's esophagus (esophageal metaplasia). In Barrett's esophagus the normal squamous epithelium of the esophagus is replaced by columnar epithelium. Because patients with Barrett's esophagus are at higher risk for esophageal cancer, they may need to be monitored regularly (every 1 to 3 years) by endoscopy and biopsy (Mayo Clinic, 2012b).
Nursing Interventions and Patient Teaching
Nursing interventions involve educating the patient about diet and lifestyle modifications that may alleviate symptoms of GERD.
Dietary instructions include: (1) eat four to six small meals daily; (2) follow a low-fat, adequate-protein diet; (3) reduce intake of chocolate, tea, and other foods and beverages that contain caffeine; (4) limit or eliminate alcohol intake; (5) eat slowly, and chew food thoroughly; (6) avoid evening snacking, and do not eat for 2 to 3 hours before bedtime; (7) remain upright for 1 to 2 hours after meals when possible, and never eat in bed; (8) avoid any food that directly produces heartburn; and (9) reduce overall body weight if needed.
Numerous lifestyle changes are also indicated in the treatment of GERD. Patients who smoke should be encouraged to stop. Cigarette smoking has been associated with decreased acid clearance from the lower esophagus. Patients should be advised to avoid constrictive clothing over the abdomen, and should avoid activities that involve straining, heavy lifting, or working in a bent-over position. Also, patients should be instructed never to sleep flat in bed. They should elevate the head of the bed at least 6 to 8 inches for sleep, using wooden blocks or a thick foam wedge.
Prognosis
If GERD is not successfully controlled, it can progress to serious and even life-threatening problems. Esophageal ulceration and hemorrhage may result from severe erosion, and chronic nighttime reflux is accompanied by a significant risk of aspiration. Adenocarcinoma can develop from the premalignant tissue (termed Barrett's epithelium). Gradual or repeated scarring can permanently damage esophageal tissue and produce strictures (American College of Gastroenterology, 2013).
Carcinoma of the Esophagus
Etiology and Pathophysiology
Carcinoma of the esophagus is a malignant epithelial neoplasm that has invaded the esophagus and has been diagnosed as a squamous cell carcinoma or an adenocarcinoma. In 2013 an estimated 12,000 Americans will be diagnosed with adenocarcinoma of the esophagus, and 6000 will be diagnosed with squamous cell carcinoma. Risk factors for esophageal cancer include alcohol and tobacco use, acid reflux, and obesity. Environmental carcinogens, nutritional deficiencies, chronic irritation, and mucosal damage have also been considered as causes of esophageal cancer. Another risk factor is Barrett's esophagus (National Cancer Institute, n.d.d). It is estimated that 1 of 200 cases of Barrett's esophagus will progress to esophageal adenocarcinoma (see Health Promotion box) (American Society for Gastrointestinal Endoscopy, 2013).
 Health Promotion
Health Promotion
Prevention or Early Detection of Esophageal Cancer
• Patients with diagnosed gastroesophageal reflux disease and hiatal hernia need counseling regarding regular follow-up evaluation.
• Health teaching should focus on elimination of smoking and excessive alcohol intake.
• Maintenance of good oral hygiene and dietary habits (intake of fresh fruits and vegetables) may be helpful.
• Patients diagnosed with Barrett's esophagus need to be monitored because this is considered a premalignant condition. Regular endoscopic screening with biopsy is required.
• Encourage patients to seek medical attention for any esophageal problems, especially dysphagia.
Unfortunately, early esophageal cancer typically has no symptoms, making early diagnosis difficult. The stage of esophageal cancer greatly impacts the 5-year survival rate. The overall 5-year survival rate for a person with cancer of the esophagus that is localized is approximately 40%; regional metastasis is approximately 20%; and distant metastasis is 3%. Less than 15% of all cases of esophageal cancer occur before the age of 55, and it is more prevalent in men (ACS, 2012b).
Clinical Manifestations
The most common clinical symptom is progressive dysphagia over a 6-month period. The patient may have a substernal feeling, as though food is not passing through the esophagus.
Assessment
Collection of subjective data includes noting that initially the patient may have difficulty swallowing when eating bulky foods such as meat; later the difficulty occurs with soft foods and finally with liquids and even saliva. Another symptom is odynophagia (painful swallowing). Pain is a late symptom and indicates local extension of the malignancy. Additional subjective symptoms include chest pain, pressure, or burning; indigestion; heartburn; and fatigue.
Collection of objective data includes observing the patient for regurgitation (backward flowing or casting up of undigested food), vomiting, hoarseness, chronic cough, choking, and iron deficiency anemia. Weight loss may be directly related to the cancer itself or to the difficulty in swallowing. Hemorrhage may occur if the cancer erodes through the esophagus. Esophageal perforation may result in the formation of a tracheoesophageal fistula (an abnormal passage between two internal organs), causing the patient to cough when swallowing anything, including saliva. Esophageal tumors may enlarge enough to cause esophageal obstruction, causing increased dysphagia. The cancer spreads via the lymph system, with the liver and lung being common sites of metastasis.
Diagnostic Tests
A barium swallow examination with fluoroscopy and endoscopy is used to detect esophageal cancer. An endoscopy with biopsy and cytologic examination provides a highly accurate diagnosis. Endoscopic ultrasonography is an important tool used to stage esophageal cancer. Computed tomography (CT), positron emission tomography (PET), and magnetic resonance imaging (MRI) also are used to assess the extent of the disease.
Medical Management
The treatment of esophageal cancer depends on the tumor's location and whether invasion or metastasis has occurred. Tumor staging must be determined to guide patient management. In advanced cases, surgery is palliative to relieve dysphagia and restore continuity of the alimentary tract. An aggressive approach provides excellent palliation (therapy designed to relieve or reduce intensity of uncomfortable symptoms but not to produce a cure), increased longevity, and a chance for a cure. Standard resection seems to give as good a result as a radical procedure (Mayo Clinic, 2011b).
Radiation therapy may be curative or palliative. Problems associated with radiation therapy include the development of a tracheoesophageal fistula, and burning. The burning that occurs may result in sunburned-like skin when external radiation is used, or damage to nearby organs such as the lungs and heart if internal radiation therapy is used. Aspiration from the fistula and edema from the radiation are common as well. Chemotherapeutic agents cisplatin (Platinol), paclitaxel (Taxol), and fluorouracil (5-FU) are currently used, as well as other chemotherapy agents, in combination with radiation before and/or after surgery (ACS, 2012b). Because of the extreme toxicity of these drugs, the nurse should expect the patient to experience side effects of respiratory and liver dysfunction, nausea and vomiting, leukopenia, and sepsis. If the tumor is in the upper third of the esophagus, radiation is indicated. A tumor in the lower third is usually resected surgically.
The following four types of surgical procedures can be performed:
1. Esophagogastrectomy: Resection of a lower esophageal section with a proximal portion of the stomach, followed by anastomosis (surgical joining of two ducts, blood vessels, or bowel segments to allow flow from one to the other) of the remaining portions of the esophagus and stomach
2. Esophagogastrostomy or esophagectomy: Resection of a portion of the esophagus with anastomosis to the stomach
3. Esophagoenterostomy: Resection of the esophagus and anastomosis to a portion of the small intestine
4. Gastrostomy: Insertion of a catheter into the stomach and suture to the abdominal wall; performed when the patient cannot take food orally because inoperable cancer of the esophagus interferes with swallowing
Nursing Interventions and Patient Teaching
Nursing diagnoses and interventions for the patient with esophageal carcinoma include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Ineffective breathing pattern, related to: | |
| Imbalanced nutrition: Less than body requirements, related to: |

The nurse should discuss with the patient and family all aspects of care, including surgery, radiation, and chemotherapy. Psychological adjustment of the patient who cannot ingest food orally, whether temporary or permanent, is difficult. Thorough explanations of all diagnostic tests, medications, procedures, and the treatment plan will help relieve the patient's anxiety. Support is given to the patient with this serious diagnosis by allowing time for questions.
Prognosis
In carcinoma of the esophagus, the disease is often well advanced by the time symptoms appear. The delay between the onset of early symptoms and when the patient seeks medical advice may be extensive. High mortality rates among these patients are affected by the following issues: (1) the patient is generally older; (2) the tumor has usually invaded surrounding structures by the time diagnosis is made; (3) the malignancy tends to spread to nearby lymph nodes; and (4) the esophagus is close to the heart and lungs, making these organs accessible to tumor extension.
The esophagus has an extensive lymphatic network, which facilitates the rapid spread of malignant cells to various local and distant sites. As discussed earlier in this section, the stage of the disease when diagnosed directly impacts the survival rate.
Collection of objective data includes observing for premalignant lesions, including leukoplakia. Unusual bleeding in the mouth, some blood-tinged sputum, lumps or edema in the neck, and hoarseness may be observed.
Achalasia
Etiology and Pathophysiology
Achalasia, also called cardiospasm, is an abnormal condition characterized by the inability of a muscle to relax, particularly the cardiac sphincter of the stomach. Although the cause is unknown, nerve degeneration, esophageal dilation, and hypertrophy are thought to contribute to the disruption of the esophagus's normal neuromuscular activity. This results in decreased motility and dilation of the lower portion of the esophagus, along with an absence of peristalsis. Thus, little or no food can enter the stomach, and in extreme cases the dilated portion of the esophagus holds as much as a liter or more of fluid. This disease may occur in people of any age, but is more prevalent in those between 20 and 50 years (Cleveland Clinic, 2013).
Clinical Manifestations
The primary symptom of achalasia is dysphagia. The patient has a sensation of food sticking in the lower portion of the esophagus. As the condition progresses, the patient complains of regurgitation of food, which relieves prolonged distention of the esophagus. The patient may also have substernal chest pain.
Assessment
The nurse should observe for loss of weight, poor skin turgor, and weakness.
Diagnostic Tests
Radiologic studies show esophageal dilation above the narrowing at the cardioesophageal junction. The diagnosis is confirmed by manometry, which shows the absence of primary peristalsis. Esophagoscopy is also used to confirm the diagnosis.
Medical Management
Conservative treatment of achalasia includes drug therapy and forceful dilation of the narrowed area of the esophagus. Anticholinergics, nitrates, and calcium channel blockers reduce pressure in the lower esophageal sphincter.
Dilation is done by first emptying the esophagus. Then a dilator with a deflated balloon is passed down to the sphincter. The balloon is inflated and remains so for 1 minute; it may need to be reinflated once or twice.
The preferred surgical approach is a cardiomyotomy. The muscular layer is incised longitudinally down to but not through the mucosa. Two thirds of the incision is in the esophagus, and the remaining one third is in the stomach; this permits the mucosa to expand so that food can pass easily into the stomach.
Nursing Interventions and Patient Teaching
Nursing interventions for esophageal surgery are presented in Box 5-2.
Nursing diagnoses and interventions for the patient with achalasia include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Imbalanced nutrition: Less than body requirements, related to difficulty swallowing both liquids and solids |

Discuss home care and follow-up care in preparation for dismissal. Include a family member or support person if possible, and involve the patient as an active participant in the planning. Explain the need to eat high-calorie, high-protein foods, and provide printed material in support of such a diet. Explain the need to sleep with the head elevated and to avoid bending over and stooping. Discuss medications if prescribed (including name, dose, time of administration, purpose, and side effects). Discuss ways to avoid constipation by eating high-fiber foods (if tolerated) and natural laxatives. Explain the importance of follow-up care with the health care provider. Finally, discuss symptoms of recurrence or progression of disease and the need to report these to the health care provider.
Prognosis
Surgical separation, in addition to bag dilation, permits the return of normal peristalsis in approximately 10% of patients with achalasia.
Disorders of the Stomach
Gastritis (Acute)
Etiology and Pathophysiology
Gastritis is an inflammation of the lining of the stomach. Acute gastritis is a temporary inflammation associated with alcoholism, smoking, and stressful physical problems, such as burns; major surgery; food allergens; viral, bacterial, or chemical toxins; chemotherapy; or radiation therapy. Changes in the mucosal lining from gastritis damages the cells that secrete acid and pepsin. Acute gastritis is often a single incident that resolves when the offending agent is removed.
Clinical Manifestations
If the condition is acute, the patient may experience fever, epigastric pain, nausea, vomiting, headache, coating of the tongue, and loss of appetite. If the condition results from ingestion of contaminated food, the intestines are usually affected and diarrhea may occur. Some patients with gastritis have no symptoms.
Assessment
Collection of subjective data includes observing for anorexia, nausea, discomfort after eating, and pain.
Collection of objective data includes observing for vomiting, hematemesis (vomiting blood), and melena caused by gastric bleeding.
Diagnostic Tests
Diagnosis is based on testing the stools for occult blood, noting white blood cell (WBC) differential increases related to certain bacteria, evaluating serum electrolytes, and observing for elevated hematocrit related to dehydration.
Medical Management
If medical treatment is required, an antiemetic—such as prochlorperazine (Compazine), promethazine (Phenergan), or trimethobenzamide (Tigan)—may be prescribed. Antacids and cimetidine (Tagamet) or ranitidine (Zantac) may be given in combination. Antibiotics are given if the cause is a bacterial agent. IV fluids are used to correct fluid and electrolyte imbalances. Patients who experience GI bleeding from hemorrhagic gastritis require fluid and blood replacement and NG lavage.
Nursing Interventions and Patient Teaching
The patient's I&O should be monitored and recorded. Foods and fluids are withheld orally as prescribed until signs and symptoms of gastritis subside. Tolerance to oral feedings is monitored and IV feedings are administered as prescribed. Clear liquids are increased to a diet as tolerated when the patient's symptoms improve.
A nursing diagnosis and interventions for the patient with gastritis include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Deficient fluid volume, related to vomiting, diarrhea, and blood loss |

Patient education includes explanations of (1) the effects of stress on the mucosal lining of the stomach; (2) how salicylates, nonsteroidal antiinflammatory drugs (NSAIDs), and particular foods may be irritating; and (3) how lifestyles that include alcohol and tobacco may be harmful. Assist the patient in locating self-help groups in the community to deal with these behaviors.
Prognosis
Because of the many classifications and causes of gastritis, prognosis is variable. In general, the prognosis is good for individuals who are willing to change their lifestyles and follow a medical regimen.
Peptic Ulcer Disease
Etiology and Pathophysiology
Peptic ulcers are ulcerations of the mucous membrane or deeper structures of the GI tract. They most commonly occur in the stomach (gastric ulcer) and duodenum (duodenal ulcer). The term peptic ulcer refers to acid in the digestive tract eroding the mucosal lining of the stomach, esophagus, or duodenum. Peptic ulcer disease (PUD) is most common in persons between the ages of 55 and 65 years (NDDIC, 2012b).
The stomach is normally protected from autodigestion by the gastric mucosal barrier. The GI tract has a high cell turnover rate, and the stomach's surface mucosa is renewed about every 3 days. As a result, the mucosa continuously repairs itself except in extreme instances when cell breakdown surpasses the cell renewal rate. In such cases, peptic ulcers can occur. The most common causes of peptic ulcer disease include the presence of Helicobacter pylori (H. pylori) bacteria in the stomach, regularly taking NSAIDs, smoking or chewing tobacco, excessive alcohol intake, and physical or emotional stress (NLM, 2011a).
Understanding of the factors that contribute to ulcer formation is developing rapidly. The discovery of the bacterium H. pylori provided new insight to ulcer formation. H. pylori has been identified in more than 80% of patients with gastric ulcers and 90% of those with duodenal ulcers. In Western cultures, half of all people over age 50 harbor H. pylori, yet most do not develop peptic ulcer disease. Scientists still need to determine what triggers ulcers in those with H. pylori (Johns Hopkins University, n.d.c).
Physiologic stress ulcer or stress-related mucosal disease is an acute ulcer that develops after a major physiologic insult such as trauma or surgery (Rohan, 2011). A stress ulcer is a form of erosive gastritis. It is believed that the gastric mucosa of the stomach undergoes a period of transient ischemia in association with hypotension, severe injury, extensive burns, and complicated surgery. The ischemia is due to decreased capillary blood flow as blood is shunted away from the GI tract, so that blood flow bypasses the gastric mucosa. This occurs as a compensatory mechanism in hypotension or shock. The decrease in blood flow produces an imbalance between the destructive properties of hydrochloric acid and pepsin and protective factors of the stomach's mucosal barrier, especially in the fundus portion. Multiple superficial erosions result, and these may bleed. Because of the possibility of development of physiologic stress ulcers and high morbidity, patients at risk receive prophylaxis with antisecretory agents, including H2 receptor blockers and proton pump inhibitors.
Clinical Manifestations
Both gastric and duodenal ulcers may have similar symptoms but may differ in timing, degree, or factors that worsen or alleviate the symptoms. Pain is the characteristic symptom and is described as dull, burning, or gnawing; it is located in the epigastric region.
Assessment
Collection of subjective data requires awareness that in patients with gastric ulcers, the pain is closely associated with food intake and usually does not awaken the patient at night or when the stomach is empty, as does the pain experienced by those with duodenal ulcers. Nausea, weight loss, eructation (belching), and distention are also common complaints made by patients with PUD. These additional vague feelings of epigastric discomfort are sometimes referred to as dyspepsia. All these subjective symptoms intensify if perforation and obstruction occur (NDDIC, 2012b).
Collection of objective data includes observing for signs of complications of PUD. Hemorrhage is a potential complication.
• Hematemesis and melena: When GI bleeding occurs, one sign is the vomiting of blood (hematemesis) that is either bright red or has a “coffee grounds” appearance resulting from the action of the gastric acid on hemoglobin. The patient may produce melena (stool that is black and tarry with undigested blood), which occurs when the blood passes through the digestive tract. Both salicylates and alcohol aggravate bleeding in patients with a history of peptic ulcers.
• Hemorrhage: Bleeding from a gastric ulcer can quickly worsen into an emergency situation if erosion is extensive. Hemorrhage, with accompanying symptoms of shock, occurs when the ulcer erodes into a blood vessel. Surgical intervention is indicated if the patient remains unstable after receiving blood over several hours.
• Perforation: Perforation occurs when the ulcer crater penetrates the entire thickness of the wall of the stomach or duodenum. The release of air, gastric acid, pancreatic enzymes, or bile into the peritoneal cavity causes pain, emesis, fever, hypotension, and hematemesis. Perforation is considered the most lethal complication of peptic ulcer. Bacterial peritonitis may occur within hours. The severity of the peritonitis is proportional to the amount and duration of the spillage through the perforation.
• Gastric outlet obstruction: Gastric outlet obstruction is a complication of peptic ulcer disease that can occur, but is rare. It is a blockage, located close to the pylorus (that part of the stomach that connects to the duodenum) and caused by gastric stasis and dilation. This condition results from factors such as scarring and inflammation associated with PUD. Symptoms may be relieved by constant NG aspiration of stomach contents. This allows edema and inflammation to subside and permits normal flow of gastric contents through the pylorus (Ignatavicius, 2013).
Diagnostic Tests
Fiberoptic endoscopy can detect both gastric and duodenal ulcers. This is called esophagogastroduodenoscopy (EGD). Fiberoptic endoscopy is more reliable than barium contrast studies because of the maneuverability of fiberoptic scopes and direct visualization of the entire esophagus and gastric and duodenal mucosa. This procedure also can be used to determine the degree of ulcer healing after treatment. During endoscopy, specimens can be obtained for identification of H. pylori or tissue specimens for biopsy. The patient is sedated but remains conscious throughout the endoscopy procedure. Local anesthetics in the throat are used to decrease the gag reflex and minimize pain during the procedure. No liquids or food are allowed following the procedure until the patient's gag reflex returns.
A noninvasive test used for diagnostic purposes is a breath test to detect H. pylori. The test calls for the patient to drink a solution containing carbon 13–enriched urea, a natural, nonradioactive substance. If H. pylori infection is present, it breaks down the compound and releases carbon-13 dioxide (13CO2). Thirty minutes after drinking the solution, the patient exhales into a collection bag, which is sent to the manufacturer for analysis. A finding of 13CO2 confirms H. pylori infection. The test may prove especially useful in determining whether antibiotic therapy eradicated an H. pylori infection. A fecal assay antigen test for H. pylori is another test that is especially useful to determine eradication of the bacteria after antibiotic treatment. An additional noninvasive way to confirm H. pylori infection is a serum or whole blood antibody test, in particular, immunoglobulin G. This test is approximately 90% to 95% sensitive for H. pylori infection but cannot distinguish active from recently treated disease (Johns Hopkins, n.d.b).
Barium contrast studies (UGI) are not as accurate as endoscopy, especially for small lesions, but are still occasionally used. Testing of feces for occult blood in the intestinal tract is also used for diagnosis.
Medical Management
The health care provider may order insertion of an NG tube to remove gastric contents and blood. Surgery is usually indicated for complications of perforation, penetration, or obstruction, or for PUD that is no longer responding to medical management.
Scar tissue builds up with repeat episodes of ulceration and healing, causing obstruction, particularly at the pylorus. The patient may experience gastric dilation, vomiting, and distention. When fluid and electrolyte balance are achieved, surgical intervention is possible.
The primary treatment for peptic ulcers is to reduce signs and symptoms by decreasing or neutralizing normal gastric acidity with drug therapy. The types of drugs most commonly used include the following (Table 5-1):
• Antacids: Neutralize or reduce the acidity of stomach contents (e.g., Maalox, Gaviscon, Rolaids, Tums, Mylanta, and Riopan).
• Histamine (H2) receptor blockers: Decrease acid secretions by blocking histamine (H2) receptors (e.g., cimetidine, ranitidine, famotidine, and nizatidine). Do not give within 2 hours of antacids.
• Proton pump inhibitors: Antisecretory agents that inhibit secretion of gastrin by the parietal cells of the stomach (e.g., omeprazole, lansoprazole, pantoprazole, rabeprazole, and esomeprazole).
• Mucosal healing agent: Heals ulcers without antisecretory properties. Sucralfate is a cytoprotective drug. It accelerates ulcer healing, presumably because of the formation of an ulcer-adherent complex that covers the ulcer and protects it from erosion by pepsin, acid, and bile salts.
• Antisecretory and cytoprotective agent: Inhibits gastric acid secretion and protects gastric mucosa (misoprostol [Cytotec]). Cytotec is the only drug approved in the United States for the prevention of gastric ulcers induced by NSAIDs and aspirin (Skidmore-Roth, 2013).
 Table 5-1
Table 5-1
Medications for Gastrointestinal Disorders
| GENERIC NAME (TRADE NAME) | ACTION | SIDE EFFECTS | NURSING IMPLICATIONS |
| Antacids, e.g., aluminum, calcium, magnesium salts, and sodium bicarbonate (Maalox, Mylanta, Titralac, Alternagel, and others) | Neutralizes gastric acid; aluminum and calcium antacids also bind phosphates in patients with renal failure | Aluminum: Constipation, hypophosphatemia Calcium: Constipation, rebound hyperacidity, hypercalcemia Magnesium: Diarrhea, hypermagnesemia Sodium bicarbonate: Sodium and water retention, alkalosis, rebound hyperacidity | Monitor serum electrolytes with long-term use; do not give antacid simultaneously with other medications because absorption of the other medication may be affected; best to separate administration by 2 hr; magnesium salts are contraindicated in patients with renal disease |
| Antispasmodics, including atropine, scopolamine, hyoscyamine, dicyclomine, clidinium (Donnatal, Bentyl, and others) | Anticholinergic agents that decrease GI motility by relaxing GI smooth muscle | Dry mouth and skin, constipation, paralytic ileus, urinary retention, tachycardia, drowsiness, dizziness, confusion, altered vision | Avoid using other CNS depressants or alcohol at the same time; avoid driving or other potentially hazardous tasks until accustomed to sedating effects |
| bismuth subsalicylate (Pepto-Bismol) | Antidiarrheal agent; also used in peptic ulcer disease caused by Helicobacter pylori | Fecal impaction, tinnitus | May turn stools dark gray to black; avoid use with aspirin; consult health care provider if diarrhea is accompanied by high fever or lasts more than 2 day |
| cimetidine (Tagamet) | H2 receptor antagonist; inhibits gastric acid secretion | Confusion, headache, gynecomastia, bone marrow suppression (rare) | Increases serum levels and clinical effects of oral anticoagulants, theophylline, phenytoin, some benzodiazepines, and propranolol (these medications may require dosage reduction) |
| dimenhydrinate (Dramamine, others) | Antiemetic agent; blocks central vomiting center | Drowsiness, dry mouth, constipation | Avoid use with other CNS depressants and alcohol; avoid driving or other hazardous activities until accustomed to sedating effects |
| diphenoxylate with atropine (Lomotil) | Antidiarrheal agent (diphenoxylate: narcotic; atropine: anticholinergic) | Drowsiness, sedation, constipation, dry mouth, urinary retention | Avoid use with other CNS depressants and alcohol; avoid driving or other hazardous activities until accustomed to sedating effects; do not use in infectious diarrhea |
| famotidine (Pepcid) | H2 receptor antagonist; inhibits gastric acid secretion | Headache, dizziness, constipation, thrombocytopenia (rare) | Unlike cimetidine, does not affect serum levels of hepatically metabolized drugs (warfarin, phenytoin, theophylline) |
| kaolin-pectin (Kaopectate) | Antidiarrheal agent | Constipation | Shake well before using |
| ketoconazole (Nizoral) | Antifungal agent | Gynecomastia, impotence, hepatotoxicity, abdominal pain | Requires acid environment for absorption; do not use with antacids, H2 receptor blockers, or omeprazole; do not use with terfenadine, astemizole, or loratadine (has caused dysrhythmias and death); monitor liver function tests often; monitor serum levels and clinical effects of warfarin, cyclosporine, and theophylline |
| lansoprazole (Prevacid) | Binds to an enzyme in the presence of acid gastric pH, preventing the final transport of hydrogen ions into the gastric lumen | Drowsiness, abdominal pain, diarrhea, nausea | Sucralfate (Carafate) decreases absorption of lansoprazole (take 30 min before sucralfate); administer before meals. Assess patient routinely for epigastric or abdominal pain. May cause abnormal liver function test results |
| loperamide (Imodium) | Antidiarrheal agent | Drowsiness, dry mouth, constipation | Monitor for dehydration; do not use in infectious diarrhea |
| mesalamine (Rowasa, Asacol) | GI antiinflammatory agent | Abdominal cramps and gas, rash, headache, dizziness | Swallow tablets whole; give enema at bedtime, retain 10-15 min |
| misoprostol (Cytotec) | Prostaglandin analog that acts as gastric mucosal protectant against NSAID-induced ulcers | Diarrhea, nausea, vomiting, flatulence, uterine cramping | Absolutely contraindicated in pregnant women; women of childbearing age must use reliable contraception |
| nizatidine (Axid) | H2 receptor antagonist, inhibits gastric acid secretion | Drowsiness, headache, dizziness, sweating, thrombocytopenia (rare) | Does not affect serum levels of hepatically metabolized drugs (warfarin, phenytoin, theophylline) |
| nystatin (Mycostatin, Nilstat, others) | Antifungal agent, available as oral suspension and topical product | Oral: Nausea, vomiting, diarrhea | Long-term therapy may be needed to clear infection; use for entire course |
| Topical: Local irritation | |||
| olsalazine (Dipentum) | GI antiinflammatory agent | Diarrhea, abdominal pain and cramps, nausea, allergic reactions, arthralgia, rash, anaphylaxis | Take with food; notify health care provider if severe diarrhea occurs |
| omeprazole (Prilosec) | Proton pump inhibitor; totally eradicates gastric acid production | Headache, dizziness, abdominal pain, nausea, vomiting, rare bone marrow suppression | Inhibits hepatic metabolism of warfarin, phenytoin, benzodiazepines, and other drugs metabolized by liver; do not crush or chew capsule contents |
| ranitidine (Zantac) | H2 receptor antagonist; inhibits gastric acid secretion | Headache, abdominal discomfort; granulocytopenia and thrombocytopenia (both rare) | Minimal effect on serum levels of hepatically metabolized drugs (phenytoin, warfarin, theophylline) |
| sucralfate (Carafate) | Gastric mucosal protectant agent; adheres to site of ulcer | Constipation, hypophosphatemia | Do not give with other drugs; coating action may interfere with the absorption of other drugs—separate by 2 hr |
| sulfasalazine (Azulfidine) | GI antiinflammatory agent | Nausea, vomiting, abdominal pain, photosensitivity, rash, Stevens-Johnson syndrome (rare), renal failure, bone marrow suppression (rare), allergic reactions, anaphylaxis | Ensure adequate hydration to prevent crystallization in kidneys; avoid exposure to sunlight; women taking oral contraceptives need to use alternative methods because of decreased effectiveness of oral contraceptives; monitor CBC and renal function; take with meals |
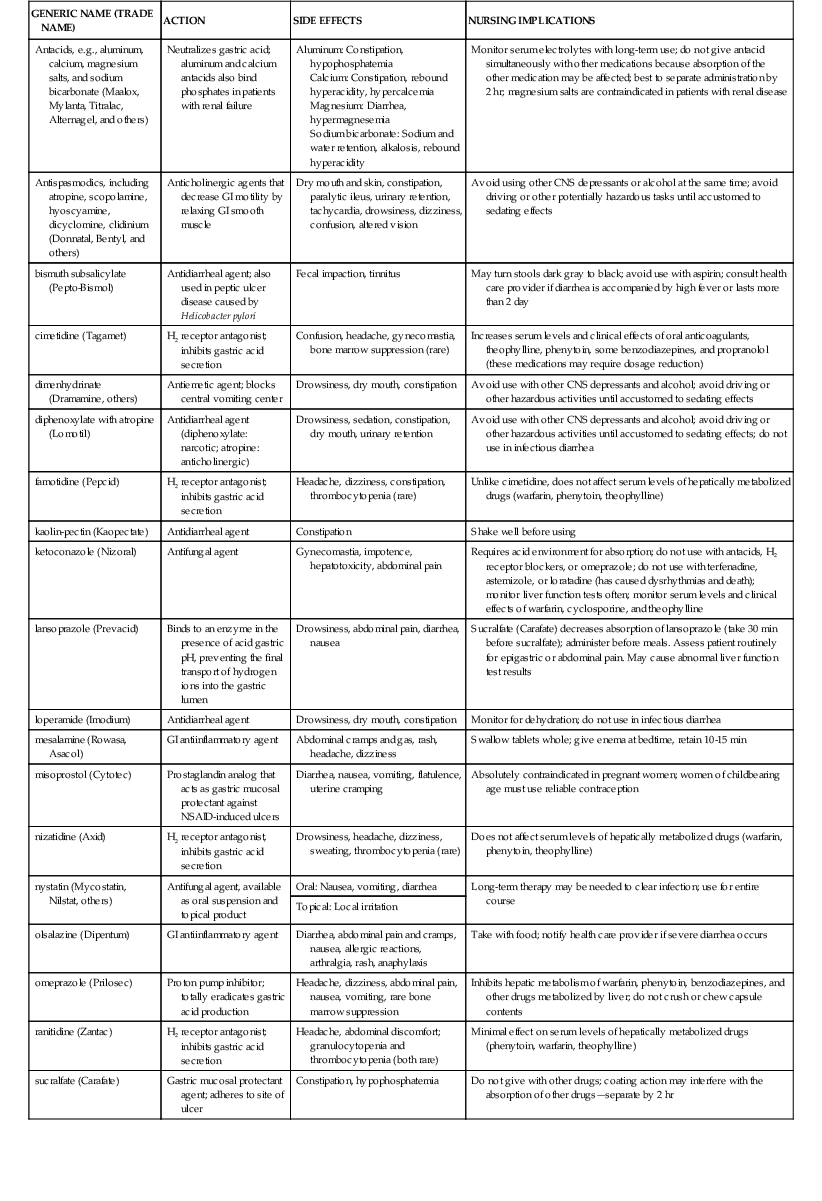

CNS, central nervous system; GI, gastrointestinal; CBC, complete blood count; NSAID, nonsteroidal antiinflammatory drug.
Antibiotic therapy eradicates H. pylori. The drugs used include metronidazole (Flagyl), tetracycline, amoxicillin, and clarithromycin (Biaxin). Treatment is typically combined in a therapeutic regimen with other medications, such as bismuth or omeprazole. Another weapon that has entered the battle against H. pylori is a combination of bismuth, metronidazole, and tetracycline. Marketed under the brand name Helidac, the medication kit contains a 14-day supply of the three drugs, with each daily dose packaged on a blister card to improve patient compliance.
Among patients whose H. pylori is treated with antibiotics, the peptic ulcer recurrence may be as low as 10%. Patients who do not receive antibiotics have a relapse rate of 75% to 90%.
Dietary modification may be necessary to avoid foods and beverages that irritate the ulcer. There is considerable controversy over the therapeutic benefits of a bland diet, since the rationale is not supported by scientific evidence. Therefore, it is recommended that the patient eat smaller meals more frequently throughout the day to decrease the degree of gastric motor activity.
Smoking has an irritating effect on the mucosa, increases gastric motility, and delays mucosal healing. Smoking should be eliminated completely or severely reduced. The combination of adequate rest and cessation of smoking accelerates ulcer healing. Because caffeinated and decaffeinated coffee, tobacco, alcohol, and aspirin aggravate the mucosal lining of the stomach and duodenum, educate patients with ulcers about the need for lifestyle change.
Surgical intervention has decreased drastically with more effective diagnosis and medical treatment with antisecretory agents and antibiotics. Approximately 20% of patients with ulcers require surgical intervention. These are patients who are unresponsive to medical management, raising concerns about gastric cancer; patients whose ulcers are drug induced but who cannot be withdrawn from the drugs (e.g., patients with rheumatoid arthritis); or patients who develop complications. Surgical procedures that may be performed are the same as those listed for cancer of the stomach.
Nursing Interventions and Patient Teaching
NG or intestinal tube insertion, irrigation, and intermittent suctioning are often performed while the patient is feeling ill and uncomfortable from PUD. In addition to being skilled and knowledgeable in performing these procedures, the nurse is responsible for easing the patient's fears and anxieties. Patient cooperation not only makes the procedures easier but also reduces patient discomfort.
Helping patients through the experience of GI intubation requires understanding of the following points:
• For most patients, NG or intestinal tube placement is a new and frightening experience. The nurse should explain the rationale for this therapy to the anxious patient and family. Help the patient and family understand that the advantages far outweigh the discomfort.
• Inability to chew, taste, and swallow food and liquids may contribute to patient anxiety during GI intubation.
• A patient with an NG or intestinal tube is usually on NPO status. On occasion, ice chips are allowed.
• An NG or intestinal tube is connected to either continuous or intermittent suctioning, usually at 100 to 125 mm Hg for decompression.
• An NG or intestinal tube is a constant irritant to the nasopharynx and nares, requiring frequent care to the mouth and nose.
• A patient with a GI tube may be afraid that moving will dislodge the tube. Implement frequent position changes to enhance tube functioning and prevent complications of immobility.
An NG tube is inserted through the nose, pharynx, and esophagus into the stomach. Various tubes are available, depending on the purpose (Table 5-2).
Table 5-2
Purposes of Nasogastric Intubation
| PURPOSE | DESCRIPTION | TYPE OF TUBE |
| Decompression | Removal of secretions and gaseous substances from GI tract; prevention or relief of abdominal distention | Salem sump, Miller-Abbott |
| Feeding (gavage) | Instillation of liquid nutritional supplements or feedings into stomach for patients unable to swallow fluid | Duo, Dobhoff |
| Compression | Internal application of pressure by means of inflated balloon to prevent internal GI hemorrhage | Sengstaken-Blakemore |
| Lavage | Irrigation of stomach in cases of active bleeding, poisoning, gastric dilation, or intestinal obstruction | Ewald, Salem sump |
GI, Gastrointestinal.
Nursing interventions depend on the stage of the ulcer disease. The emphasis in patient care should always be on prevention and early detection of pain in the epigastric region, hematemesis, melena, or tenderness and rigidity of the abdomen (see Communication box and Nursing Care Plan 5-1).
 Nursing Care Plan 5-1
Nursing Care Plan 5-1
The Patient With Gastrointestinal Bleeding
Mr. D., 33 years of age, is admitted with pain in the epigastric region and copious hematemesis. He appears anxious; his skin is pale, cool, and clammy; and he is breathing rapidly. This patient has a history of recurrent episodes of vomiting blood that has a coffee grounds appearance. He denies passing blood rectally but admits his stools have changed in consistency.
Nursing Diagnosis
Risk for deficient fluid volume, related to hemorrhage, vomiting, and diarrhea

Nursing Diagnosis
Anxiety, related to hospitalization and illness

Critical Thinking Questions
1. Mr. D. has an NG tube connected to wall suction that is draining sanguineous fluid. He complains of severe fatigue and epigastric pain. He is pale and drawn, with a hemoglobin level of 5.1 g/dL. Mr. D. puts his call light on and requests the nurse to assist him to the bathroom for a bowel movement. What appropriate interventions will ensure Mr. D.'s safety?
2. During assessment of Mr. D., what signs and symptoms would indicate deficient fluid volume?
3. Mr. D. says to the nurse that he fears he may die. He appears anxious and tremulous. What is the most therapeutic approach to help decrease his fears?
Nursing diagnoses and interventions for the specific stages of ulcer care include but are not limited to the following:
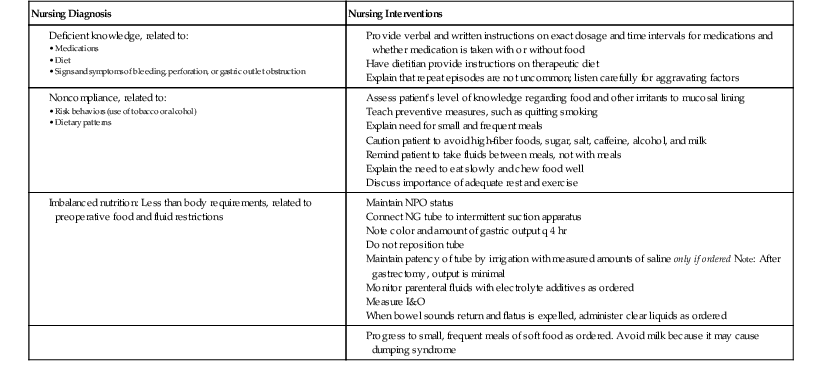
 Communication
Communication
Patient With GI Bleeding
Nurse: You look like you are resting better, Mrs. S. How have you been feeling? (Reaffirming a relationship that was begun yesterday.)
Patient: Hello, Mrs. F. My stomach pain is much better. The medicine helped.
Nurse: If you are comfortable, perhaps you and your husband have some questions about why you are here. (Trying to determine whether the patient is receptive to patient teaching. A knowledge deficit was suspected on admission.)
Patient: I was scared when I started to vomit blood. It has happened before but not this much. Where does the blood come from?
Nurse: You have a diagnosis of GI bleeding with questionable duodenal ulcer. This means that the bleeding is coming from somewhere in your digestive tract or from an ulcer that has formed in the first part of your small intestine. The ulcer is an erosion of the lining of your stomach or small intestine. Do you understand what I have said so far? (The nurse begins with the admitting diagnosis and explains one thing at a time, making sure the patient verbalizes understanding before continuing. It is beneficial for the nurse to show the patient a diagram of the GI system.)
Patient: Well, I understand where the bleeding is coming from, but why am I bleeding there?
Nurse: We are not sure yet, Mrs. S., but you are scheduled for a procedure that will allow the health care provider to actually look at the surface of the stomach and a portion of the intestine. It is called an endoscopy, and it will be done tomorrow morning. Did someone explain this to you? (The nurse answers the patient's question openly and honestly and uses her answer to lead into further patient education.)
It is necessary to form a trusting relationship with the patient with an ulcer because of the severity of the condition and the need for long-term treatment. Include the family in patient education sessions to increase understanding and support, and involve the patient in goal setting to increase compliance (see Home Care Considerations box).
 Home Care Considerations
Home Care Considerations
Peptic Ulcer Disease
• The patient who has recurrent ulcer disease after initial healing must learn to live with a chronic disease.
• The patient may be angry and frustrated, especially if he or she has faithfully followed the prescribed therapy but failed to prevent the recurrence or extension of the disease process.
• Unfortunately, many patients do not comply with the care plan and experience repeated exacerbations.
• Changes in lifestyle are difficult for most people and may be resisted.
• The patient who is instructed to stop smoking or avoid alcohol may resist.
• The goal should be to adhere to the prescribed therapeutic regimen, including nutritional management, cessation of smoking, and decreased use of alcohol and caffeine.
• A patient with chronic ulcers needs to be aware of the complications that may result from the disease, the clinical manifestations indicating their presence, and what to do until the health care provider can be seen.
• Teach the patient to take all medications as prescribed. This includes both antisecretory and antibiotic drugs. Failure to take prescribed medications can result in relapse.
Instruct the patient to seek medical attention immediately if severe and sudden pain occurs. Assist the patient in describing signs and symptoms of weakness, anorexia, nausea, diarrhea, constipation, anxiety, or restlessness. When medications are prescribed, the patient must fully understand (1) the purpose of taking antibiotic therapy to eradicate H. pylori; (2) the importance of taking all medications such as H2 receptor antagonists, antiulcer drugs, prostaglandin E analog, and proton pump inhibitors as prescribed; (3) why the antacids are taken in specific dosages and at the specific times ordered; and (4) the known side effects (diarrhea and constipation). Preventive teaching includes identifying high-risk behaviors, such as the use of tobacco, caffeine, and alcohol. Emphasize that the patient should eat six smaller meals daily and avoid any foods that cause noticeable stomach discomfort.
If surgery is required, explain the procedures thoroughly, including the reasons for them. Explain immediate postoperative care, including deep breathing; coughing; position changes; frequent monitoring of vital signs; IV tubing, NG tubing, catheters, and other drainage tubes; and the use of patient-controlled analgesia (PCA) or other medications for pain relief. The patient's ability to eat normally after healing depends on the type of surgery and when peristalsis returns. Help the patient realize that symptoms often recur and he or she should seek medical care if they do.
Prognosis for Peptic Ulcers
Recurrence of an ulcer may happen within 2 years in about one third of all patients. Among patients whose H. pylori is treated with antibiotics, the peptic ulcer recurrence drops to 20%. Patients who do not receive antibiotics have a relapse rate of 75% to 90%. The likelihood of recurrence is lessened by eliminating foods that aggravate the condition and following prescribed therapies such as taking proton pump inhibitors and avoiding NSAIDs. If symptoms recur, the prognosis is better in patients who seek immediate medical treatment and comply with the prescribed regimen (Best Practice, 2012).
Cancer of the Stomach
Etiology and Pathophysiology
Stomach, or gastric, cancer saw its peak in the 1930s, being the leading cause of death. While those numbers have decreased significantly over the years, the American Cancer Society estimates that 2013 will see 21,600 new cases of stomach cancer in the United States and nearly 11,000 people will die from the disease. Men will be affected more often than women, with over 13,000 of those cases being diagnosed and almost 7000 dying. The incidence and mortality rate are greatly increased outside of the United States, especially in less developed areas. Rates are highest in Japan, China, Southern and Eastern Europe, and South and Central America. Gastric cancer affects mostly the elderly population; nearly two thirds of those diagnosed are over the age of 65 (ACS, 2013d). The most common neoplasm or malignant growth in the stomach is adenocarcinoma. The primary location is the pyloric area, but the incidence of proximal tumors appears to be rising. Because of its location, the tumor may metastasize to lymph nodes, liver, spleen, pancreas, or esophagus.
Many factors have been implicated in the development of stomach cancer, yet no single causative agent has been identified. Stomach carcinogenesis probably begins with a nonspecific mucosal injury as a result of aging; autoimmune disease; or repeated exposure to irritants such as bile, antiinflammatory agents, or smoking. Other factors include history of polyps, pernicious anemia, hypochlorhydria (deficiency of hydrochloride in the stomach's gastric juice), chronic atrophic gastritis, and gastric ulcer. Because the stomach has prolonged contact with food, cancer in this part of the body is associated with diets that are high in salt, smoked and preserved foods (which contain nitrites and nitrates), and carbohydrates, and low in fresh fruits and vegetables. Whole grains and fresh fruits and vegetables are associated with reduced rates of stomach cancer. Infection with H. pylori, especially at an early age, is considered a definite risk factor for gastric cancer.
Clinical Manifestations
The patient may be asymptomatic in early stages of the disease. Stomach cancer often spreads to adjacent organs before any distressing symptoms occur. With more advanced disease, the patient may appear pale and lethargic if anemia is present. With a poor appetite and significant weight loss, the patient may appear cachectic (weak and emaciated).
Assessment
Subjective data include complaints of vague epigastric discomfort or indigestion, early satiety, and postprandial (after meal) fullness. Some patients complain of an ulcer-like pain that does not respond to therapy. Anorexia and weakness are also common.
Objective data include weight loss, bleeding in the stools, hematemesis, and vomiting after drinking or eating. Anemia is common. It is caused by chronic blood loss as the lesion erodes through the mucosa or as a direct result of pernicious anemia, which develops when intrinsic factor is lost. The presence of ascites is a poor prognostic sign.
Diagnostic Tests
The tumor is diagnosed by radiographic barium studies (GI series). Endoscopic or gastroscopic examinations with biopsy remain the best diagnostic tool. The stomach can be distended with air during the procedure to stretch mucosal folds. Tissue samples for the growth-promoting protein, HER2/neu, can be obtained during endoscopic examination. Findings of increased levels are seen in gastric adenocarcinoma. Endoscopic ultrasound and CT and PET scans can be used to stage the disease. Stool examination provides evidence of occult or gross bleeding. Carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 tumor markers are usually elevated in advanced gastric cancer. Serum tumor markers correlate with the degree of invasion, liver metastasis, and cure rate. Laboratory studies of RBCs, hemoglobin, hematocrit, and serum B12 assist in the detection of anemia and determination of severity (ACS, 2013d).
Medical Management
The most therapeutic management of stomach cancer is surgical removal. Surgery may be done as an exploratory celiotomy to determine involvement. The surgical interventions used in treating gastric cancer are typically the same procedures used for peptic ulcer disease. A partial or total gastric resection is the treatment of choice for an extensive lesion. Surgery for advanced gastric cancer carries high morbidity and mortality rates (Mayo Clinic, 2013). Types of surgical procedures include the following:
• Antrectomy: Removal of the entire antrum, the gastric-producing portion of the lower stomach, to eliminate the main stimulus to acid production.
• Gastroduodenostomy (Billroth I) (Figure 5-7, A): Direct anastomosis of the fundus of the stomach to the duodenum; used to remove ulcers or cancer located in the antrum of the stomach.


• Gastrojejunostomy (Billroth II) (Figure 5-7, B): Closure of the duodenum, and anastomosis of the fundus of the stomach into the jejunum; used to remove ulcers or cancer located in the body of the fundus.
• Total gastrectomy: Removal of the entire stomach; rarely used for patients with gastric cancer.
• Vagotomy: Removal of the vagal innervation to the fundus, decreasing acid produced by the parietal cells of the stomach (Figure 5-8); usually done with a Billroth I or II procedure or with a pyloroplasty.
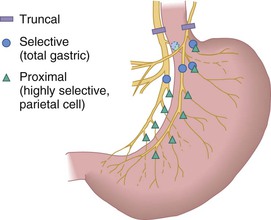
• Pyloroplasty: Surgical enlargement of the pyloric sphincter to facilitate passage of contents from the stomach; commonly done after vagotomy or to enlarge an opening that has been constricted from scar tissue. A vagotomy decreases gastric motility and subsequently gastric emptying. A pyloroplasty accompanying vagotomy increases gastric emptying (Johns Hopkins, n.d.c).
The choice of which procedure to use is difficult and depends on the surgeon's preference and results of diagnostic testing. Regardless of the procedure selected, postoperative complications are possible. Bleeding may occur up to 7 days after gastric surgery. Abdominal rigidity, abdominal pain, restlessness, elevated temperature, increased pulse, decreased blood pressure, and leukocytosis are all possible indications of postoperative bleeding. Note the amount and type of drainage from the incision. Surgical intervention may be necessary to correct the bleeding.
Dumping syndrome is a rapid gastric emptying of undigested food from the stomach to the small intestine, causing distention of the duodenum or jejunum. Increased intestinal motility and peristalsis and changes in blood glucose levels occur. Patients may report diaphoresis, nausea, vomiting, epigastric pain, explosive diarrhea, borborygmi (rumbling noises made by gas passing through the liquid of the small intestine), and dyspepsia. Dumping syndrome is the direct result of surgical removal of a large portion of the stomach and the pyloric sphincter. Approximately one third to one half of patients experience dumping syndrome after peptic ulcer surgery. Treatment includes eating six small meals daily that are high in protein and fat and low in carbohydrates, eating slowly, and avoiding fluids during meals. Treatment also includes (1) anticholinergic agents to decrease stomach motility, and (2) reclining for approximately 1 hour after meals. To increase long-term compliance, reassure patients that following the recommended treatment will decrease symptoms within a few months. The symptoms are self-limiting and often disappear within several months to a year after surgery.
Several other complications after gastric surgery present serious health threats. Diarrhea is common and usually responds to conservative treatment of controlled diet and antidiarrheal agents. Diphenoxylate with atropine (Lomotil), loperamide (Imodium), paregoric, or codeine is often used. Reflux esophagitis and nutritional deficits—leading to weight loss, malabsorption, anemia, and vitamin deficiency—can also be life-threatening.
Pernicious anemia is a serious potential complication for any patient who has had a total gastrectomy or extensive resections. This is caused by a deficiency of intrinsic factor, produced exclusively by the stomach, which aids intestinal absorption of vitamin B12. Recommend that all patients with a partial gastrectomy have a blood serum vitamin B12 level measured every 1 to 2 years so that replacement therapy of vitamin B12 via a monthly injection, or weekly via the nasal route, can be instituted before anemia appears.
Wound healing may be disrupted by dehiscence (a partial or complete separation of the wound edges) or by evisceration (protrusion of viscera through the disrupted wound). Dehiscence and evisceration may be caused by problems in suturing the wound or by poor tissue integrity. Excessive coughing, straining, malnutrition, obesity, and infection may also increase the chances of dehiscence. Nursing interventions for dehiscence include instructing the patient to remain quiet, to cover the wound with a dry sterile dressing, and to avoid coughing or straining. Keep the patient in a dorsal recumbent position (on the back with the knees flexed) to remove stress on the wound and notify the surgeon. If evisceration occurs, keep the patient on bed rest and loosely cover the protruding viscera with a warm sterile saline dressing. Notify the surgeon immediately because treatment consists of reapproximating (i.e., drawing together) the wound edges.
Chemotherapy yields greater response and longer survival rates than radiation. Because the radiosensitivity of stomach cancer is low, radiation therapy is of little value. Radiation therapy may be used as a palliative measure to decrease tumor mass and temporarily relieve obstruction. The combination of chemotherapy and radiation therapy is sometimes used for patients who are at high risk for disease recurrence after surgery. These treatment modalities are often used in conjunction with surgery (Mayo Clinic, 2013).
Nursing Interventions and Patient Teaching
The nurse must provide further clarification about the disease and the surgical intervention to the patient and family. Preoperative preparation includes improving the patient's nutritional status by monitoring total parenteral nutrition (TPN; complete nutrition provided intravenously) and providing supplemental feedings. Postoperative teaching is necessary to relieve anxiety and promote understanding of drainage tubes, feeding tubes, dressing changes, weakness, medications, and other routine care. Close monitoring of intake and output, maintenance of TPN, and being alert to weight loss are important in the postoperative period for surgeries involving the stomach.
Nursing diagnoses and interventions for the patient with cancer of the stomach include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |

Ackley BJ, Ladwig GB: Nursing diagnosis handbook: An evidence-based guide to planning care, ed 9, St. Louis, 2011, Mosby.
Because care encompasses so many areas, instruction should be (1) planned according to the patient's needs and level of understanding, (2) given when the patient is free of pain, and (3) communicated both verbally and in print. The nurse should address areas such as surgery, chemotherapy, radiation therapy, continued nutritional needs, pain relief, and support groups for psychosocial needs.
Weight loss indicates the need for additional caloric intake and can be measured by monitoring weight and comparing it with the patient's normal weight before illness. If a gastrostomy tube (G-tube) is necessary, prevention of skin excoriation around the G-tube site should be ensured. Hypermotility or diarrhea that follows radiation therapy can be treated with dietary therapy and/or medication. The debilitated patient and family may require referral for hospice care.
Prognosis
The prognosis for patients with gastric cancer depends on the stage at which the cancer was detected. The overall average 5-year survival rate is about 30%. Five-year survival rates range from 71% if the gastric cancer is at stage 1A (i.e., cancer cells are limited to the gastric mucosa) to a 4% survival rate for stage IV (i.e., cancer has extended into nearby organs or has metastasized to more distant areas in the body) (NCI, n.d.b; Mayo Clinic, 2013).