Care of the Patient With a Cardiovascular or a Peripheral Vascular Disorder
Objectives
Anatomy and Physiology
1. Discuss the location, size, and position of the heart.
2. Identify the chambers and valves of the heart and their functions.
3. Discuss the electrical conduction system that causes the cardiac muscle fibers to contract.
4. Explain what produces the two main heart sounds.
5. Trace the path of blood through the coronary circulation.
Medical-Surgical
6. List diagnostic tests used to evaluate cardiovascular function.
7. For coronary artery disease, compare nonmodifiable risk factors with factors that are modifiable in lifestyle and health management.
8. Describe five cardiac dysrhythmias.
9. Compare the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, nursing interventions, and prognosis for patients with angina pectoris, myocardial infarction, or heart failure.
10. Specify patient teaching for patients with cardiac dysrhythmias, angina pectoris, myocardial infarction, heart failure, and valvular heart disease.
11. Discuss the purposes of cardiac rehabilitation.
12. Discuss the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, nursing interventions, and prognosis for the patient with pulmonary edema.
13. Compare and contrast the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, nursing interventions, and prognosis for the patient with rheumatic heart disease, pericarditis, and endocarditis.
14. Identify 10 conditions which may result in the development of secondary cardiomyopathy.
15. Discuss the indications and contraindications for cardiac transplant.
16. Identify risk factors and the effects of aging associated with peripheral vascular disorders.
17. Compare and contrast signs and symptoms and discuss nursing interventions associated with arterial and venous disorders.
18. Compare essential (primary) hypertension, secondary hypertension, and malignant hypertension.
19. Discuss the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, and nursing interventions and the importance of patient education for the patient with hypertension.
20. Compare and contrast the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, nursing interventions, and prognosis for patients with arterial aneurysm, Buerger's disease, and Raynaud's disease.
21. Discuss the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, nursing interventions, and prognosis and discuss appropriate patient education for patients with thrombophlebitis, varicose veins, and stasis ulcer.
Key Terms
http://evolve.elsevier.com/Cooper/adult
Anatomy and Physiology of the Cardiovascular System
The cardiovascular (circulatory) system is the transportation system of the body. It delivers oxygen and nutrients to the cells to support their individual activities and transports the cells' waste products to the appropriate organs for disposal. This chapter discusses the structure and function of the blood vessels and the heart.
 Heart
Heart
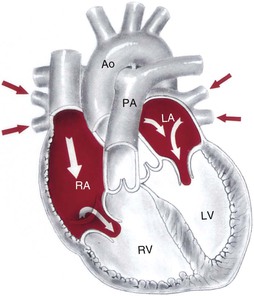
The heart is a remarkable organ, not much bigger than a fist (Figure 8-1). It pumps 1000 gallons of blood every day through the closed circuit of blood vessels. It beats 100,000 times a day and transports the blood 60,000 miles through a network of blood vessels. The heart is a hollow organ composed mainly of muscle tissue with a series of one-way valves.
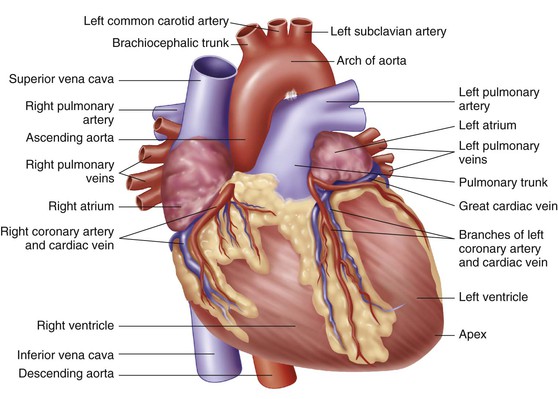
The heart is located in the chest cavity between the lungs in a region called the mediastinum (the organs and tissues separating the lungs; in addition to the heart and its greater vessels, the mediastinum contains the trachea and the esophagus). Two-thirds of the heart lies left of the midline. The wider base of the heart lies superior to and beneath the second rib. The apex, or narrow part, of the heart lies inferiorly, slightly to the left between the fifth and sixth ribs near the diaphragm.
Heart Wall
The heart wall is composed of three layers: pericardium, myocardium, and endocardium. The pericardium is a two-layered, serous membrane that covers the entire structure. Between the two thin membranes is a serous fluid that allows friction-free movement of the heart as it contracts and relaxes. The pericardium is the outermost layer of the heart. The myocardium forms the bulk of the heart wall and is the thickest and strongest layer of the heart. It is composed of cardiac muscle tissue. Contraction of this tissue is responsible for pumping blood. The endocardium (innermost layer) is composed of a thin layer of connective tissue. This structure lines the interior of the heart, the valves, and the larger vessels of the heart.
Heart Chambers
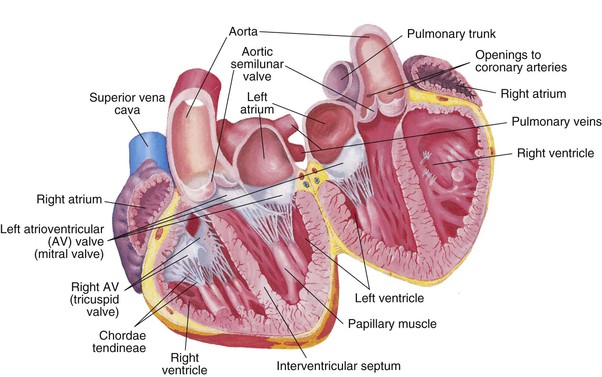
The heart is divided into right and left halves by a muscular partition called the septum (Figure 8-2). The heart has the following four chambers:
1. The right atrium is the upper right chamber. It receives deoxygenated blood from the entire body. The superior vena cava returns blood from the head, the neck, and the arms. The inferior vena cava returns blood from the lower body. The coronary vein returns it from the heart muscle to the coronary sinus.
2. The right ventricle is the lower right chamber. It receives deoxygenated blood from the right atrium. The right ventricle pumps blood to the lungs via the pulmonary artery to release carbon dioxide and receive oxygen.
3. The left atrium is the upper left chamber. It receives oxygenated blood from the lungs via the pulmonary veins.
4. The left ventricle is the lower left chamber. It receives oxygenated blood from the left atrium. It is the thickest, most muscular section of the heart and pumps the oxygenated blood out through the aorta to all parts of the body.
The heart actually functions as two separate pumps: (1) the right side receives deoxygenated blood and pumps it to the lungs, and (2) the left side receives oxygenated blood from the lungs and pumps it throughout the body.
Heart Valves
Located within the heart are four valves that keep the blood moving forward and prevent backflow. The heart has two atrioventricular (AV) valves. They are located between the atrium and the ventricles. The right AV valve, located between the right atrium and the right ventricle, is called the tricuspid valve because it contains three flaps, or cusps. The left AV valve is composed of two cusps (bicuspid) and is commonly called the mitral valve. It is located between the left atrium and the left ventricle. Both of these valves rapidly close to prevent backflow of blood. Small cordlike structures, chordae tendineae, connect the AV valves to the walls of the heart and work with the papillary muscles located in the walls of the ventricles to make a tight seal to prevent backflow when the ventricles contract.
The two remaining valves, the semilunar valves, are located at the points where the blood exits the ventricles. The pulmonary semilunar valve is located between the right ventricle and the pulmonary artery. Blood is pushed out of the right ventricle and travels to the lungs via the pulmonary artery. The aortic semilunar valve is located between the left ventricle and the aorta. When the left ventricle contracts, the blood is forced into the aorta and the aortic semilunar valve closes. Both of the semilunar valves have three cusps in the shape of a half moon, hence the name semilunar (see Figure 8-2).
Electrical Conduction System
Heart muscle tissue has an inherent ability to contract in a rhythmic pattern. This ability is called automaticity. If heart muscle cells are removed and placed under a microscope, they continue to beat. In addition, they can respond to a stimulus in the same way that nerve cells do. This unique property is called irritability. Automaticity and irritability are two characteristics that affect the functions of the conduction system. Hormones, ion concentration, and changes in body temperature also affect the conduction of messages around the heart, initiation of heartbeat, and coordination of beating patterns between the atria and the ventricles.
The heartbeat is initiated in the sinoatrial (SA) node, which is located in the upper part of the right atrium, just beneath the opening of the superior vena cava (Figure 8-3). Because it regulates the heartbeat, the SA node is known as the pacemaker. Impulses are passed to the AV node, which is located in the base of the right atrium. The AV node slows the impulses to allow the atrium to complete contraction and to allow the ventricles to fill. The impulses then pass to a group of conduction fibers called the bundle of His, which divides into right and left bundle branches to travel to smaller branches called the Purkinje fibers, which surround the ventricles. The message travels rapidly through the ventricles and causes contractions, which empty the ventricles.
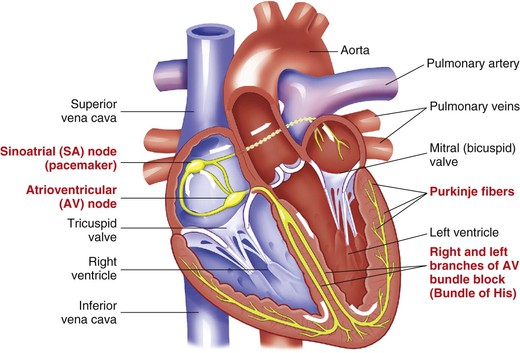
The impulse pathway is as follows:
SA node → AV node → Bundle of His →
Right and left bundle branches → Purkinje fibers
Cardiac Cycle
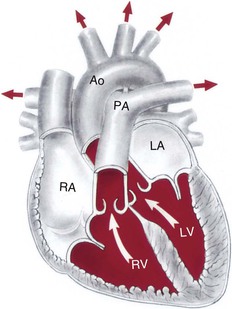
The cardiac cycle refers to a complete heartbeat. The two atria contract while the two ventricles relax. When the ventricles contract, the two atria relax. The phase of contraction is called systole (Figure 8-4), and the phase of relaxation is called diastole (the period between contraction of the atria or the ventricles during which blood enters the relaxed chambers from the systemic circulation and the lungs [Figure 8-5]). Complete diastole and systole of both atria and ventricles constitute a cardiac cycle; this takes an average of 0.8 second.
The heart sounds, lubb and dubb, are produced by closure of the valves. The first sound, lubb (long duration and low pitch), is heard when the AV valves close. The second sound, dubb (short duration, sharp sound), is heard when the semilunar valves close. On occasion, a murmur (swishing sound) can be heard. This can be a normal functional phenomenon produced by rapid filling of the ventricles, or it can be an abnormal condition produced by ineffective closure of the valves.
Blood Vessels
Three main types of blood vessels are organized to carry blood to and from the heart: arteries, veins, and capillaries. The heart delivers the blood to large vessels called arteries, which carry blood away from the heart. The arteries branch into smaller vessels called arterioles, which deliver the blood to the tissues. Within the tissues, the arterioles divide into microscopic vessels called capillaries, which form an extensive (50,000-mile) network that allows exchange of products and by-products between the tissues and blood. The capillaries then join to form tiny veins, or venules, that link with larger veins, which carry the blood toward the heart. The pattern is as follows:
Artery → Arteriole → Capillary → Venule → Vein
Circulation
Coronary Blood Supply
To sustain life, the heart must pump blood throughout the body on a continuous basis. As a result, the heart muscle (or myocardium) requires a constant supply of blood containing nutrients and oxygen to function effectively. The delivery of oxygen and nutrient-rich arterial blood to cardiac muscle tissue and the return of oxygen-poor blood from this active tissue to the venous system are called the coronary circulation (Figure 8-6).
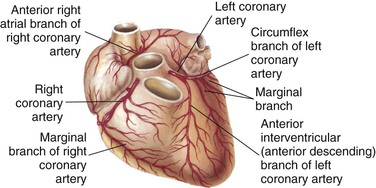
Blood flows into the heart muscle by way of two small vessels, the right and left coronary arteries. The coronary arteries wrap around the myocardium (see Figures 8-1 and 8-6). The openings into these vessels lie behind the flaps of the aortic semilunar valves (see Figure 8-6). The coronary arteries bring oxygen and nutrition to the myocardium. Once the circulation is completed and the carbon dioxide and waste products have been collected, the blood flows into a large coronary vein and finally into the coronary sinus, which empties into the right atrium. These two main arteries have many tiny branches that serve the heart muscle. If an artery becomes occluded (blocked or obstructed), these branches provide collateral circulation (alternate routes) to nourish the heart muscle. If the occlusion is severe, surgery and other procedures may be needed. These interventions are discussed later in this chapter.
Systemic Circulation
Systemic circulation occurs when blood is pumped from the left ventricle of the heart through all parts of the body and returns to the right atrium. When the oxygenated blood leaves the left ventricle, it enters the largest artery (1 inch [2.5 cm] in diameter) of the body, the aorta. This is the main trunk of the systemic arterial circulation and is composed of four parts: the ascending aorta, the arch, the thoracic portion of the descending aorta, and the abdominal portion of the descending aorta. As the blood flows through the artery branches, the branches become smaller in diameter (arterioles). The blood continues to flow into the capillaries. The capillaries surround the cells and exchange oxygen and nutrients for carbon dioxide and other waste products. The blood flows to the tiny venules, then to the larger veins, and finally returns to the right atrium via the largest vein, the vena cava (one of two large veins returning blood from the peripheral circulation to the right atrium of the heart).
The blood is now deoxygenated and needs to be replenished with oxygen. In addition, the blood is carrying a high concentration of carbon dioxide. Note that the upper portion of the vena cava (superior vena cava) returns deoxygenated blood from the head, neck, chest, and upper extremities. The inferior vena cava returns deoxygenated blood from parts of the body below the diaphragm.
Pulmonary Circulation
The deoxygenated blood now passes through the pulmonary circulation to pick up the needed oxygen. Blood is pumped from the right atrium to the right ventricle, where it leaves the heart to travel via the pulmonary artery to the lungs. Once the blood reaches the lungs, it travels through arterioles to microscopic capillaries surrounding the alveoli (air sacs), where oxygen diffuses into the bloodstream and carbon dioxide diffuses out. The capillaries then connect with the venules and finally with the four pulmonary veins, which return the oxygenated blood to the left atrium of the heart. It is then pumped to the left ventricle and to the aorta, and the systemic circulation is then repeated. The blood circulation pattern is as follows:
Superior or inferior vena cava → Right atrium →
Tricuspid valve → Right ventricle →
Pulmonary semilunar valve → Pulmonary artery →
Capillaries in the lungs → Pulmonary veins →
Left atrium → Bicuspid valve → Left ventricle →
Aortic semilunar valve → Aorta
 Laboratory and Diagnostic Examinations
Laboratory and Diagnostic Examinations
A number of diagnostic tests are used to evaluate cardiovascular function. The nursing responsibilities are to physically prepare the patient for diagnostic procedures and to explain the examination to the patient.
Diagnostic Imaging
Radiographic examination (i.e., an x-ray) of the chest provides a film record of heart size, shape, and position and outline of shadows. Lung congestion is also shown, indicating heart failure (HF), perhaps in the earliest stages. Pleural effusion (an abnormal accumulation of fluid in the thoracic cavity between the visceral and parietal pleurae) may be noted in left-sided HF. The nurse's role in preparation for this procedure is to explain the reasons for examination and what the examination will show.
Fluoroscopy allows observation of movement, and is invaluable in pacemaker or intracardial catheter placement. Using a fluoroscope, the motion of internal structures such as the heart is examined with a device that emits x-rays that pass through the patient and fluoresce on a special screen, producing a sort of x-ray–based motion picture.
An angiogram is a series of radiographs taken after a contrast medium (dye) is injected into an artery or vein. Picturing the circulatory process aids in diagnosis of vessel occlusion, pooling in various heart chambers, and congenital anomalies. Angiography allows x-ray visualization of the heart, aorta, inferior vena cava, pulmonary artery and vein, and coronary arteries.
In an aortogram, the abdominal aorta and the major leg arteries are examined by x-ray visualization after a contrast medium is injected via a catheter (a thin, flexible tube) passed through the femoral artery and into the aorta. Aneurysms (abnormal bulges in the wall of a blood vessel) and many other abnormalities can be diagnosed. Contrast media may also be used to visualize the aortic arch and branches.
The nurse's role in preparing the patient for the examination is to explain the procedure. Since dye is involved, it is very important to make sure the patient does not have an allergy to ingredients in the dye. This type of procedure requires the patient's informed consent. After the procedure, the nurse checks the site of catheter insertion (usually the groin area) for excess bleeding, ensures that a compression device is in place, and alerts the health care provider if excess bleeding is noted. The nurse also checks for circulation in the periphery below the site, monitors vital signs, and ensures that the patient remains supine (lying face up) for the recommended amount of time.
Cardiac Catheterization and Angiography
Cardiac catheterization is an invasive procedure used to visualize the heart's chambers, valves, great vessels, and coronary arteries. This procedure aids in diagnosis, prevention of progression of cardiac conditions, and accurate evaluation and treatment of the critically ill patient.
In cardiac catheterization, a catheter is passed through a peripheral vessel and into the vessels or chambers of the heart. It can reveal heart abnormalities, such as valvular defects, arterial occlusion, and congenital anomalies. Cardiac catheterization allows (1) measurement of blood pressure within the heart and (2) assessment of the blood in the heart. Blood samples may also be obtained. Contrast dye may be injected to allow better heart and vessel visualization (angiography). Cardiac catheterization is performed under sterile surgical conditions. Its invasive nature requires a prior signed consent from the patient. Because the contrast medium contains iodine, it is important to determine whether the patient is sensitive to iodine before injection, to avoid an allergic reaction. After the procedure, the nurse assesses the circulation to the extremity used for catheter insertion. Peripheral pulses, color, and sensation of the extremity should be checked every 15 minutes for 1 hour and then with decreasing frequency. The puncture site is observed for hematoma and bleeding. The nurse monitors the vital signs and checks for abnormal heart rate, dysrhythmias, and signs of pulmonary emboli (indicated by respiratory difficulty). The patient lies supine for a designated period with a compression device over the pressure dressing at the insertion site to prevent hemorrhage.
Electrocardiography
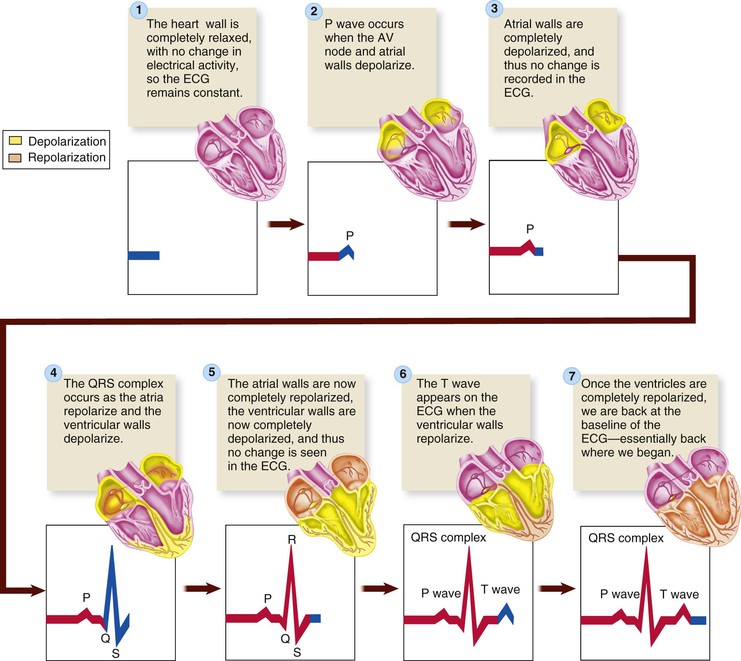
The electrocardiogram (ECG or EKG) is a graphic study of the electrical activities of the myocardium to determine transmission of cardiac impulses through the muscles and conduction tissue. Each ECG has three distinct waves, or deflections: the P wave, the QRS complex, and the T wave. Depolarization refers to the electrical activity when the heart contracts. Repolarization is the relaxation phase. The P wave represents the depolarization of the atria. The QRS complex represents the depolarization of the ventricles. The T wave represents the repolarization of the ventricles. Atrial repolarization is not represented but does occur; it is covered by the large QRS complex and cannot be seen on the ECG tracing.
A standard ECG has 12 electrodes attached to the skin surface to measure the total electrical activity of the heart. Each lead records the electrical potential between the limbs or between the heart and limbs. A conductive gel enhances the contact and transmission. The patient is typically placed in the supine position; ambulatory ECGs and exercise stress test ECGs require position variation. The machine, an electrocardiograph or galvanometer, records the energy wave of each heartbeat through a vibrating needle on graph paper, which feeds through the machine at a standard rate. Each ECG waveform represents a single electrical impulse as it travels through the heart (Figure 8-7).
The ECG tracing is read or interpreted by a cardiac specialist (cardiologist) or by internal medicine specialists, family practitioners, pediatricians, and emergency department practitioners. The reading can also be displayed on the fluorescent screen (oscilloscope) of a cardiac monitor. A graphic tracing may be printed out by the monitor.
Ambulatory ECGs can be used to monitor heart rhythm over prolonged periods—12, 24, or 48 hours—and compared with various activities or symptoms recorded in a diary kept by the patient. A Holter monitor (small portable recorder) is attached to the patient by leads, with a 2-pound tape recorder carried on a belt or shoulder strap. The monitor operates continuously to record the patterns and rhythms of the patient's heartbeat. In conjunction with the diary, the health care provider can note various events, times, and medication peaks that affect or precipitate dysrhythmias. An ambulatory ECG is particularly useful for patients whose clinical symptoms indicate heart disorders but who may have normal ECG tracings on a resting test. Thorough explanation by the health care provider is essential to ensure proper recordings by the patient, since this is an outpatient procedure.
Cardiac Monitors
It is common practice to continuously assess the cardiac electrical activity of patients who are known or suspected to have dysrhythmias or who are prone to develop dysrhythmias or acute cardiovascular symptoms. A cardiac monitor displays information on the electrical activity of the heart transferred via conductive electrodes placed on the chest.
Most monitors provide a visual display of cardiac electrical activity and the patient's heart rate. Preset alarms warn of heart rates that exceed or drop below limits considered acceptable for each patient and also warn of dysrhythmias.
Ambulatory patients (i.e., patients who are able to walk) are increasingly monitored by battery-powered ECG transmitters that do not directly connect the patient to an oscilloscope. This monitoring is called telemetry, which is the electronic transmission of data to a distant location. The electrodes placed on the patient's chest are attached to a transmitter the patient carries in a pocket or pouch. The transmitter sends a radio signal to a receiver, usually located at the nurse's station or a remote location within a hospital.
Patients need telemetry monitoring for various reasons, including a history of cardiac disease, angina pectoris, suspected dysrhythmias, a change in medications, an electrolyte abnormality, or unexplained syncope. Many of these patients are monitored in a centralized area such as an intermediate care or step-down unit (with monitors at the nurse's station). By remote telemetry, a patient on a medical-surgical unit may be monitored at a separate location, called the home unit, which is usually on a critical care unit. Remote telemetry patients are usually stable; but a stable patient's condition can change rapidly, and telemetry allows continuous heart monitoring to detect abnormalities.
Attachment to a cardiac monitor does not change a patient's need for nursing interventions. The monitoring electrodes are placed on the anterior thorax (chest) rather than the extremities, enabling the patient to be relatively free to carry on usual activities. Pay special attention to the electrode site to ensure a constant tight seal between the electrode and the skin and to note the development of any skin impairment. The conduction gel dries out, even if the pad is sealed; changing electrodes regularly is recommended. Check the telemetry pack for integrity of the lead wires and test the monitoring device's battery with a battery tester. Inform the monitoring area whenever the patient is moved off the unit for a diagnostic test, since the patient may go outside the monitor's range. Another important safety measure is never to remove the telemetry device and allow the patient to shower unless the health care provider has written the order to allow a shower. The patient could be subject to severe dysrhythmia, which would not be detected with the telemetry device removed.
Exercise-stress ECG is another form of monitoring the heart's capability, this time in a laboratory setting while the patient performs a prescribed exercise. Tasks include use of treadmills, stair climbing, and aerobic exercise. While being monitored carefully, the patient is coaxed to a limit of exertion to evaluate myocardial ischemia (reduced oxygen in the heart due to insufficient blood flow), dysrhythmia, and cardiac capability under extreme circumstances. The test sets the limit of exercise tolerance in cardiac disease. If the patient is unable to tolerate activity, a stress test can be done by administering dipyridamole (Persantine) or adenosine (Adenocard), which makes the patient's heart respond as if it were under stress or activity.
Thallium Scanning
Thallium-201 is a radioactive isotope (radioisotope) that is actively transported into normal cells. If the cells are ischemic or infarcted, the thallium will not be picked up. Thallium concentrates in tissue with normal blood flow; tissue with inadequate perfusion appears as dark areas on scanning—a “cold spot.” The radioisotope is injected intravenously while the patient exercises on a treadmill. (Note: Breast tissue in the female can produce artifact, leading to a false-positive result. Technetium-99 m sestamibi may be used instead of thallium to minimize artifact and thus improve accuracy.) In a patient who cannot tolerate physical exercise, dipyridamole is given before the thallium to physiologically simulate exercise-induced stress. After the procedure is over, caution the patient to avoid driving for the next 4 hours, and to stand slowly from a sitting or lying position to avoid orthostatic hypotension during that time.
Echocardiography
Echocardiography uses high-frequency ultrasound directed at the heart. The echo, or reflected sound, is graphically recorded as a sonogram, outlining the size, shape, and position of cardiac structures. This test is used to detect pericardial effusion (collection of blood or other fluid in the pericardial sac), ventricular function, cardiac chamber size and contents, ventricular muscle and septal motion and thickness, cardiac output (ejection fraction), cardiac tumors, valvular function, and congenital heart disorder.
The ventricular ejection fraction (EF) on an echocardiogram can be gauged as follows:
Positron Emission Tomography
Positron emission tomography (PET) is a computerized radiographic technique that uses radioactive substances to examine the metabolic activity of various body structures. In PET studies the patient either inhales or is injected with a radioactive biochemical substance. A computer interprets the data, depicting the various levels of metabolic activity as color-coded images. Used to study dementia, stroke, epilepsy, and tumors, PET is also useful in the diagnosis and treatment of cardiac disease. The ability of PET to distinguish between viable and nonviable myocardial tissue allows health care providers to identify the most appropriate candidates for bypass surgery or angioplasty. PET is also able to accurately detect coronary artery disease (CAD) noninvasively in an asymptomatic patient, prompting early intervention that can salvage a potentially ischemic myocardium.
MUGA Scan
A MUGA (multigated acquisition) scan uses a radioactive tracer and a special camera. The camera takes pictures of the heart as it pumps. The test may be done while the patient is resting, exercising, or both. This test is considered a noninvasive procedure, although a radioisotope is injected to assess the ejection fraction of the left ventricle.
Before the procedure begins, the nurse ensures that the patient has had no food or drink for at least 6 hours before the test and has avoided caffeine and tobacco use as well.
After the scan is done, the nurse should encourage the patient to drink plenty of fluids to flush out the radioactive dye. The patient should be able to resume normal activities after the procedure.
Laboratory Tests
The history, physical examination, and blood studies help the health care provider diagnose and monitor the cardiovascular disease process. The nurse's responsibility is to prepare the patient by explaining what the tests are for and the preparation required for each test.
Blood cultures to detect growth of bacteria in the blood are crucial to the diagnosis of infective endocarditis.
A complete blood count (CBC) is a determination of the number of red blood cells (erythrocytes) and white blood cells (WBCs; leukocytes) per cubic millimeter, as well as the proportions of the various kinds of white blood cells (the WBC differential), platelets, hemoglobin, and hematocrit (the volume percentage of red blood cells in whole blood). Lower hemoglobin levels reduce the ability of the blood to carry oxygen to the cells, resulting in anemia. An elevated WBC count indicates infection or inflammation. An elevated red blood cell count indicates that the body is compensating for chronic hypoxemia (an abnormal deficiency of oxygen in the arterial blood) by stimulating red blood cell production by the bone marrow, leading to secondary polycythemia (an abnormal increase in the number of red blood cells in the blood). Chronic hypoxemia is often found in heart failure.
Coagulation studies include prothrombin time (PT), international normalized ratio (INR), and partial thromboplastin time (PTT). These studies are used to monitor the patient receiving anticoagulant drug therapy, which is prescribed for patients after a myocardial infarction (MI) to dissolve the thrombus. Coagulation studies are also used in patients with chronic atrial fibrillation or those with atrial fibrillation who are undergoing electrical cardioversion (restoring the heart's normal sinus rhythm by delivering a synchronized electric shock through two metal paddles placed on the patient's chest).
The erythrocyte sedimentation rate (ESR) is determined to monitor or rule out inflammatory/infective conditions. The ESR is elevated with MI and infective endocarditis and decreases when healing begins. The ESR also indicates the extent of inflammation and infection in rheumatic fever.
Serum electrolyte tests focus on the body's balance of sodium, potassium, calcium, and magnesium, which are necessary for myocardial muscle function. Sodium (Na+) helps maintain fluid balance. Potassium (K+) is required for relaxation of cardiac muscle, and calcium (Ca2+) is necessary for contraction of cardiac muscle. Magnesium (Mg2+) helps maintain the correct level of electric excitability in the nerves and the muscles, including the myocardium and the cardiac conduction system. The health care provider compares serum electrolyte levels with ECG changes.
Serum lipids are associated with vascular disease, particularly CAD. Cholesterol and triglycerides bound to plasma proteins are found in the blood as lipoproteins. Density levels vary according to the protein-to-fat ratio. An elevated level of high-density lipoprotein (HDL) is desired, but an elevated level of low-density lipoprotein (LDL) or very-low-density lipoprotein (VLDL) increases the risk for cardiovascular disease (Box 8-1).
Arterial blood gases are measured to monitor oxygenation (PaO2, the partial pressure of oxygen in the blood; and PaCO2, the partial pressure of carbon dioxide in the blood) and acid-base balance (pH). These tests are used to monitor blood oxygenation in patients with unstable cardiac conditions and to evaluate patients in cardiac failure.
Serum cardiac markers are certain proteins released into the circulation in large quantities when cardiac cells die (National Library of Medicine, 2012a). These markers, specifically serum cardiac enzymes and troponin I, are important screening diagnostic criteria for an acute MI. The increase in serum cardiac enzymes that occurs after cell death can show whether cardiac damage is present and the approximate extent of the damage. The levels of cardiac enzyme creatine kinase (CK) and its isoenzyme, creatine phosphokinase (CK-MB), start to rise within 2 to 3 hours after the beginning of an MI, peak in 24 hours, and return to normal within 24 to 40 hours. CK and CK-MB have been the “gold standard” for years, but they have been replaced with troponins I and T. CK-MB is also found in skeletal muscle and its blood level can be elevated by surgery, muscle trauma, and muscle diseases, making the differential diagnosis more difficult, so it is not a specific indicator for MI.
Troponins are myocardial muscle proteins released into the circulation after a myocardial injury. In the heart there are two subtypes: cardiac-specific troponin T and troponin I. These sensitive markers can indicate a very small amount of myocardial damage. Troponin T appears in the blood 3 to 5 hours after an MI, and its level may remain elevated for up to 21 days. Like CK-MB, the level of troponin T is affected by skeletal muscle injury and renal disease. Troponin I is a sensitive and specific cardiac marker, not influenced by skeletal muscle trauma or renal failure. The troponin I level rises 3 hours after MI, peaks at 14 to 18 hours, and returns to normal in 5 to 7 days. Troponin I is useful in diagnosing an MI (American Heart Association, 2013a). The ability to measure the myocardial contractile proteins (troponins) in serum, which are often present in very small amounts, is a major advance in the diagnosis of acute MI and acute myocardial damage.
Myoglobin is released into circulation within a few hours after an MI. Although it is one of the first serum cardiac markers that increase after an MI, myoglobin is also present in skeletal muscle, so an increase can be associated with noncardiac causes. In addition, it is rapidly excreted in urine, and blood levels return to normal range within 24 hours after an MI.
B-type natriuretic peptide (BNP) is a hormone secreted by the heart in response to ventricular expansion and pressure overload. A BNP level above 100 pg/mL indicates HF. The higher the BNP level, the more severe the HF (American Heart Association, 2013a).
Homocysteine is an amino acid produced during protein digestion. Normal values range from 4 to 14 µmol/L. Elevated blood levels of homocysteine may be an independent risk factor for ischemic heart disease, cerebrovascular disease, peripheral arterial disease (PAD), and venous thrombosis. Homocysteine appears to promote the progression of atherosclerosis by causing endothelial damage, promoting LDL deposits, and stimulating vascular smooth muscle growth. Homocysteine plays an important role in blood clotting. An elevated level results in increased platelet aggregation. Screening for elevated homocysteine levels (greater than 14 µmol/L) should be considered in patients with progressive and unexplained atherosclerosis despite normal levels of lipoproteins and who have no other risk factors. It is also recommended in patients with an unusual family history of atherosclerosis, especially at a young age.
Dietary deficiency of vitamins B6 (pyridoxine), B12 (cobalamin), or folate is the most common cause of elevated homocysteine. Some researchers believe that an elevated level of homocysteine can be treated by giving vitamins B6, B12, and folate. Whether this treatment will reduce the incidence of MI remains to be proven (American Heart Association, 2013a).
The liver produces C-reactive protein (CRP) during periods of acute inflammation. The presence of CRP is a predictor of cardiac events and is emerging as an independent risk factor for CAD. People with diabetes mellitus are already at high risk for developing cardiovascular disease. If a patient has both an elevated level of CRP and diabetes, the risk for a cardiovascular disorder becomes even greater (Pagana and Pagana, 2008).
Disorders of the Cardiovascular System
Cardiovascular disorders are a major health care problem in the United States. Public awareness, modifications in lifestyle, and improvements in medical treatment have contributed to a decline in overall deaths. The nurse's role in caring for patients with cardiovascular disorders includes being aware of the prevalence of cardiac disease, risk factors, and the disease process; implementing nursing interventions; and patient teaching.
Effects of Normal Aging on the Cardiovascular System
By the time an individual reaches the age of 65 years, physiologic changes have reduced the heart's efficiency as a pump. Yet the heart still is capable of functioning adequately unless there is underlying cardiac disease (see Lifespan Considerations box). According to the National Heart, Lung, and Blood Institute (2011), all Americans should have their cholesterol levels checked once every 5 years. Older adults with high cholesterol should take steps to lower their cholesterol levels, including taking cholesterol-lowering medications, stopping smoking, increasing their activity levels, continuing their blood pressure medications, decreasing their weight, and, if they have diabetes, continuing to control their blood glucose level.
 Lifespan Considerations
Lifespan Considerations
Older Adults
Cardiac Disease
• Changes in the cardiac musculature lead to reduced efficiency and strength, resulting in decreased cardiac output.
• Disorientation, syncope, and decreased tissue perfusion to organs and other body tissues can occur as a result of decreased cardiac output.
• Aging causes sclerotic changes in blood vessels and leads to decreased elasticity and narrowing of the lumen. Arterial disease resulting from the aging process causes hypertension because of the increased cardiac effort needed to pump blood through the circulatory system.
• Progressive coronary artery changes can lead to the development of collateral coronary circulation. This can modify the severity of signs and symptoms seen in MI. Angina symptoms may be less pronounced, and dyspnea may replace angina as a key symptom of acute infarction.
• Heart failure can result from rapid intravenous infusion.
• Edema secondary to heart failure may cause tissue impairment in the immobile older adult. Immobility leads to venous stasis (i.e., a slowing or stoppage of venous blood flow), venous ulcer, and poor wound healing. It also increases the risk of venous thrombosis and embolus formation.
• Older adults with cardiac disease often receive several medications, which are often prescribed at lower doses than for younger adults. Even with lower doses of medications, observe the older adult closely for signs of toxicity, since the rate of drug metabolism and excretion decreases with age.
• Independent older adults with cardiac conditions should receive adequate teaching regarding medication, diet, and warning signs of complications. Encourage them to maintain regular contact with the health care provider and to seek care at the first sign of problems.
Risk Factors
Risk factors indicate predispositions for developing cardiovascular disease. The presence of more than one risk factor is associated with an increased risk for developing cardiovascular disease. Risk factors are classified as nonmodifiable and modifiable.
Nonmodifiable Factors
An important aspect of caring for the patient with a cardiovascular disorder is understanding the risk factors for cardiovascular disease and incorporating them into patient teaching. The nonmodifiable risk factors (risk factors that cannot be changed) associated with cardiovascular disorders include age, genetics, and heredity.
Family history.
A family member such as a parent or sibling who has a cardiovascular problem before 50 years of age puts the patient at greater risk for developing cardiovascular disease.
Age.
Normal physiologic changes that occur with aging and past lifestyle habits increase the patient's risk for developing cardiovascular disease with advancing age. CAD and MI occur most frequently among white, middle-aged men.
Gender.
Middle-aged men are at greater risk of developing cardiovascular disease than middle-aged women. Although the incidence in men and women equalizes after age 65, cardiovascular disease is a more common cause of death in women than in men. Women develop CAD about 10 years later than men because natural estrogen may have a cardioprotective effect before menopause. Despite this, the incidence of cardiovascular disease in women 50 years of age and older is increasing. Factors possibly responsible are increased social and economic pressures on women and changes in lifestyle. Ten times more women die from heart disease than die from breast cancer. The mortality rate for women with CAD has remained relatively constant even though cardiovascular disease remains the leading cause of death. Despite this statistic, only 15% of women consider CAD their greatest health risk. Recent research on CAD has shown that women often do not have the same signs and symptoms of an acute coronary event as those that are commonly seen in men (American Heart Association, 2012a).
Cultural and ethnic considerations.
African American men have a higher incidence of hypertension than do white men. African American women have a higher incidence of CAD, with greater severity and higher death rates, than do white women (American Heart Association, 2012a). Hispanics have rates similar to those of African Americans and whites. Heart disease is second only to cancer in American Indians, Alaska Natives, Asians, and/or Pacific Islanders (Centers for Disease Control and Prevention [CDC], 2011).
Modifiable Factors
Smoking.
Individuals who smoke cigarettes have a two to three times greater risk of developing cardiovascular disease than nonsmokers. The degree of risk is proportional to the number of cigarettes smoked. Individuals who quit smoking decrease their risk. Tobacco smoke contains nicotine, which causes the release of catecholamine (i.e., epinephrine, norepinephrine). Catecholamine release causes tachycardia, hypertension, and vasoconstriction of the peripheral arteries, which in turn increase the work of the heart and result in greater myocardial oxygen consumption (American Heart Association, 2011). Nicotine reduces the amount of available oxygen to the heart muscle. Nicotine also increases platelet adhesion, which results in increased risk of embolism (American Heart Association, 2011).
Hyperlipidemia.
Hyperlipidemia is elevated concentrations of any or all lipids in the plasma. The ratio of HDL to LDL is the best predictor for the development of cardiovascular disease. Density levels vary according to the protein-to-fat ratio:
• VLDL contains more fat than protein (primarily triglycerides); triglycerides are the main storage form of lipids and constitute approximately 95% of fatty tissue.
• LDL contains an equal amount of fat and protein (approximately 50%) with moderate amounts of phospholipid cholesterol.
| Less than 100 mg/dL | Optimal |
| 100 to 129 mg/dL | Near optimal to above optimal |
| 130 to 159 mg/dL | Borderline high |
| 160 to 189 mg/dL | High |
| More than 190 mg/dL | Very high |
• HDL contains more protein than fat (which serves a protective function, removing cholesterol from tissues). It is suspected that HDL also removes cholesterol from the peripheral tissues and transports it to the liver for excretion. HDL may have a protective effect by preventing cellular uptake of cholesterol and lipids. Low levels (less than 40 mg/dL) are believed to increase a person's risk for CAD, whereas high levels (more than 60 mg/dL) are considered protective (see Box 8-1).
A diet high in saturated fat, cholesterol, and calories contributes to hyperlipidemia. Therefore dietary control is an important aspect in modifying this risk factor. An overall serum cholesterol level of less than 200 mg/dL is desirable, 200 to 239 mg/dL is borderline high, and more than 239 mg/dL is high.
Change in diet is probably the most important method of lowering cholesterol level. Weight reduction in overweight patients with abnormal lipid profiles is an essential element of dietary intervention. In addition to lowering LDL levels, weight reduction leads to decreases in triglyceride level and blood pressure. A combination of weight reduction and physical exercise improves the lipid profile, with a decrease in LDL level, an increase in HDL level, and a decrease in triglyceride levels. Low HDL levels are often familial and only somewhat modifiable.
Cholesterol-lowering drugs are often included in treatment of hyperlipidemia. Cholesterol-lowering drugs are divided into six classes: (1) bile acid sequestrants; (2) nicotinic acid (niacin); (3) statins such as simvastatin (Zocor), pravastatin (Pravachol), and rosuvastatin (Crestor); (4) fibric acid derivatives such as gemfibrozil (Lopid) and probucol (Lorelco); (5) the cholesterol absorption inhibitor ezetimibe (Zetia); and (6) combination drugs such as ezetimibe and simvastatin (Vytorin). Pravastatin reduces the risk of a first MI by about one-third in hypercholesterolemic patients with no history of coronary disease. Simvastatin is now allowed by the U.S. Food and Drug Administration (FDA) to add a label statement that the drug can reduce deaths by lowering cholesterol.
Hypertension.
Hypertension is called the “silent killer” because a patient with elevated blood pressure does not display signs and symptoms of heart disease until damage has begun to develop. This damage increases the risks of heart disease, stroke, heart failure, or cardiovascular death. Prehypertension is defined as blood pressure of 120 to 139/80 to 89 mm Hg, which requires monitoring yearly to decrease a patient's risk of developing cardiac disease.
Hypertension is blood pressure higher than 140/90 mm Hg, taken on two separate occasions. Adhering to diet, exercise, and the prescribed pharmacological therapies to control elevated blood pressure helps modify the individual's risk.
Diabetes mellitus.
Cardiac disease has been found to be more prevalent in individuals with diabetes mellitus. Diabetes poses a greater risk than other factors, possibly because an elevated blood glucose level damages the arterial intima (the innermost layer of an artery) and contributes to atherosclerosis. Patients with diabetes also have alterations in lipid metabolism and tend to have high cholesterol and triglyceride levels. Keeping the blood glucose level under control helps modify the individual's risk. The CDC estimates that 68% of people with diabetes over the age of 65 will have heart disease (CDC, 2010). Adults with diabetes and heart disease are two to four times more likely than adults without diabetes to die from cardiac-related complications. Blood pressure control decreases these risks by 33% to 50%. In general, every 10-mm Hg drop in systolic blood pressure decreases the risk by 12%. Patients with diabetes who decrease their diastolic blood pressure by 10 mm Hg decrease their chance of a cardiovascular event by 50%.
Obesity.
Excess body weight increases the workload of the heart. It also contributes to the severity of other risk factors. The CDC estimates that 35.7% of Americans are obese. This correlates to 97 million Americans with a body mass index (BMI) of 30 or above. As the BMI increases, so do the risk factors for developing diabetes, cardiovascular events, and stroke. A weight reduction program and maintaining an ideal body weight help modify the individual's risk.
Sedentary lifestyle.
Lack of regular exercise has been correlated with an increased risk of developing cardiovascular disease. Regular aerobic exercise can improve the heart's efficiency and help lower the blood glucose level, improve the ratio of HDLs to LDLs, reduce weight, lower blood pressure, reduce stress, and improve overall feelings of well-being. Individuals with sedentary lifestyles should work with their health care provider to plan an exercise program that fits their lifestyle. Some health care providers define regular physical exercise as exercising at least three to five times a week for at least 30 minutes, causing perspiration and an increase in heart rate by 30 to 50 beats per minute (bpm). Yoga has been receiving increasing research as a form of exercise that increases musculoskeletal strengthening, flexibility, and relaxation. Yoga movements also have therapeutic cognitive effects of distraction and mindfulness, thereby reducing stress on the body. Another form of exercise receiving national attention is walking. Walking is one of the best forms of exercise because it is the simplest and easiest way to exercise. Walking can strengthen bones, tune up the cardiovascular system, and clear a cluttered mind. Walking is a remedy for stress as well.
Stress.
The body's stress response releases catecholamines that increase the heart rate. Catecholamines are hormones produced by the adrenal glands and released during times of physical and emotional stress. Catecholamines also affect myocardial cells and may cause cellular damage. The vasoconstriction that occurs may contribute to the development of cardiovascular disease. Stress reduction measures may help modify an individual's risk.
Psychosocial factors.
In the early 1970s, health care providers used the term “type A personality” to describe a person who is always in a hurry, impatient, and irritable, or always angry or hostile. Recent studies have found that the term type A does not always fit the person with cardiovascular risks. More recent studies have found that the type D personality is more likely to suffer from increased cardiovascular symptoms. The person with a type D personality has chronic negative emotions, is pessimistic, and socially inhibited. Type D personalities tend to have increased levels of anxiety, irritation, and depressed mood across most situations and times. Type D people do not share their feelings because they fear disapproval, thereby increasing their chance of a cardiovascular event.
 Cardiac Dysrhythmias
Cardiac Dysrhythmias
A cardiac dysrhythmia (or arrhythmia) is any cardiac rhythm that deviates from normal sinus rhythm. Normal sinus rhythm originates in the SA node and is characterized by the following:
• P waves: Precede each QRS complex (atrial depolarization)
• P-R interval: Interval between atrial and ventricular repolarization
• QRS complex: Ventricular depolarization
A dysrhythmia is the result of an alteration in the formation of impulses through the SA node to the rest of the myocardium. It also results from irritation of the myocardial cells that generate impulses, independent of the conduction system. Signs and symptoms of dysrhythmia vary, as do treatment options, depending on the type and severity of the dysrhythmia. A short overview of each dysrhythmia follows.
Types of Cardiac Dysrhythmias
Sinus tachycardia.
Sinus tachycardia is a rapid, regular rhythm originating in the SA node. It is characterized by a heartbeat of 100 to 150 bpm or more.
Causes of sinus tachycardia include exercise, anxiety, fever, shock, medications, HF, excessive caffeine, recreational drugs, and tobacco use. Tachycardia increases the amount of oxygen delivered to the cells by increasing the amount of blood circulated through the vessels.
Clinical manifestations include occasional palpitations. Many patients are asymptomatic. Other signs and symptoms may include hypotension and angina, if cardiovascular disease is also present.
Medical management is directed at the primary cause. This is a normal rhythm and is not usually caused by a cardiac problem.
Sinus bradycardia.
Sinus bradycardia is a slow rhythm originating in the SA node. It is characterized by a pulse rate of less than 60 bpm. Bradycardia can be life-threatening if the cause is not found. Bradycardia caused by an SA node dysfunction or other undetermined causes may be managed by the insertion of a pacemaker. Causes of sinus bradycardia include obstructive sleep apnea, vomiting, intracranial tumors, MI, medications (especially overuse of digitalis, beta-adrenergic blockers, or calcium channel blockers), carotid sinus massage, vagal stimulation, endocrine disturbances, increased intracranial pressure, and hypothermia. When found in association with MI, it is a beneficial rhythm because it reduces myocardial oxygen demand. An athlete's resting heart rhythm may normally be slow, because of the training the athlete undergoes.
Clinical manifestations of bradycardia may not be manifested in some patients until the heart drops to the 50s and may include fatigue, lightheadedness, and syncope. Some patients are asymptomatic.
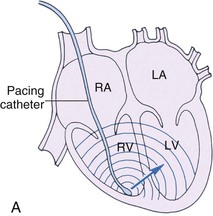
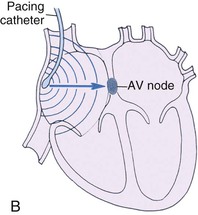
Medical management is directed toward the primary cause of the problem and maintaining cardiac output. If the cause is determined to be vagal stimulation, such as when bearing down with a bowel movement or vomiting, a stool softener is given or medication to stop the vomiting, and the patient is taught how to stop vagal stimulation. Atropine (Atreza, Sal-Tropine) may be prescribed to increase the heart rate. A temporary or permanent, implantable pacemaker is sometimes necessary (Figures 8-8 and 8-9). If the cause is suspected to be drug related, blood is drawn and the drug concentration is determined; if necessary, the drug is withheld.
Supraventricular tachycardia.
Supraventricular tachycardia (SVT) is the sudden onset of a rapid heartbeat. It originates in the atria. It is characterized by a pulse rate of 150 to 250 bpm.
Causes of SVT include medications, alcohol, mitral valve prolapse, emotional stress, smoking, and hormone imbalance such as decreases in estrogen in postmenopausal women. The cause is typically not associated with heart disease. Clinical manifestations include palpitations, lightheadedness, dyspnea, and anginal pain.
Medical management first looks at how well the patient tolerates the dysrhythmia and at the overall clinical picture. The focus is aimed at decreasing the heart rate and eliminating the underlying cause. Specific treatments may include carotid sinus pressure, adenosine, digoxin (Lanoxin), calcium channel blockers (e.g., diltiazem [Cardizem]), beta-adrenergic blockers, propranolol (Inderal), antidysrhythmics, amiodarone (Cordarone), and cardioversion. Persistent, recurring SVT caused by the presence of an accessory pathway (i.e., a second, abnormal electrical conduction pathway; see Electrical Conduction System, above) may ultimately be treated by radiofrequency catheter ablation (i.e., cutting away or eradication) of the accessory pathway.
Atrial fibrillation.
In atrial fibrillation, electrical activity in the atria is disorganized, causing the atria to fibrillate, or quiver, rather than contract as a unit. Atrial fibrillation is a very rapid production of atrial impulses. The atria beat chaotically and are not contracting properly. It is characterized by an atrial rate of 350 to 600 bpm. If untreated, the ventricular response rate may be 100 to 180 bpm.
Causes of atrial fibrillation include cardiac surgery, longstanding hypertension, pulmonary embolism, atherosclerosis, mitral valve disease, HF, cardiomyopathy, congenital abnormalities, chronic obstructive pulmonary disease, and thyrotoxicosis. Clinical manifestations include pulse deficit, palpitations, dyspnea, angina, lightheadedness, syncope, fatigue, change in level of consciousness, and pulmonary edema. Because of ventricular rhythm irregularity and ineffective atrial contractions, decreased cardiac output may be noted, resulting in HF, angina, and shock. Thrombi (blood clots) may form in the atria as a result of ineffective atrial contraction and cause emboli (i.e., thrombi that have moved from one point in the body to another), thus affecting the lungs or periphery. An embolized clot may pass to the brain, causing a stroke. Risk of stroke increases fivefold with atrial fibrillation. Risk of stroke is even higher in patients who have structural heart disease, hypertension, and are over 65 years of age.
Medical management focuses on treating the irritability of the atria, slowing the ventricular response to atrial stimulation, and correcting the primary cause. The goal of therapy is to prevent atrial thrombi from developing and embolizing, such as in the lungs or periphery. Specific pharmacologic treatments to achieve cardioversion may include (1) digitalis; (2) calcium channel blockers such as intravenous (IV) diltiazem (Cardizem) and verapamil (Calan, Isoptin); (3) antidysrhythmics such as procainamide (Procan SR, Pronestyl), amiodarone (Cordarone), dofetilide (Tikosyn), flecainide (Tambocor), and propafenone (Rythmol) (American Heart Association, 2012); and anticoagulants such as heparin and warfarin (Coumadin). Outpatients typically take oral warfarin to maintain anticoagulation. The goal of anticoagulation is to maintain an INR between 2 and 3. If pharmacologic cardioversion fails, the patient may need electrical cardioversion. Transesophageal echocardiography (TEE) is used to detect a thrombus in the atria before proceeding with electrical cardioversion. The Joint Commission recommends that patients with atrial fibrillation be prescribed warfarin and long-term antidysrhythmic medication therapy at discharge.
There are several new anticoagulants on the market that are also being prescribed to treat deep-vein thrombosis (DVT) and atrial fibrillation. Pradaxa (dabigatran etexilate mesylate) and Xarelto (rivaroxaban) are two of the newest that have been approved for this use. Unlike warfarin (Coumadin), these drugs do not require continuing modification of the dosages. Although these drugs do not require modification of dosages and long-term determination of PT, PT/INR blood levels, there are still issues with the drugs. Please see the Safety Alert box for drugs that interact unfavorably with Xarelto.
 Safety Alert
Safety Alert
Drugs That Interact Unfavorably With Xarelto
Antibiotics
Barbiturates
Calcium channel blockers
Heart and blood pressure medications
Herbals
NSAIDs (nonsteroidal antiinflammatory drugs)
Quinine
Salicylates
Seizure medications
For patients who do not respond to medication therapy or electrical conversion, catheter ablation (cutting or removal) with radiofrequency energy is used to destroy the areas in the atria that trigger abnormal electrical signals. The catheter is inserted into the femoral vein and threaded via fluoroscopy to the heart. The special ablation catheter is placed in strategic areas, and bursts of radiofrequency energy destroy the irritable area (American Heart Association, 2012b).
Catheter ablation to treat atrial fibrillation is usually performed on younger patients because of a better response rate and fewer complications than in the older adult. After the catheter ablation procedure, perform neurovascular assessment checks at the peripheral sites distal to the catheter insertion site (American Heart Association, 2011).
Atrioventricular block.
AV block occurs when a defect in the AV junction slows or impairs conduction of impulses from the SA node to the ventricles. Three types of blocks are seen: first degree, second degree, and third degree. A third-degree block indicates worsening of the impairment at the AV junction and a complete heart block.
Common causes of AV block include atherosclerotic heart disease (ASHD), MI, and heart failure (HF). Other causes may be digitalis toxicity, congenital abnormality, drugs, and hypokalemia (low potassium in the blood).
First-degree heart block is often asymptomatic. Vertigo, weakness, and irregular pulse are seen with second-degree block. Disease that is progressing, as with third-degree block, will be accompanied by hypotension, angina, and bradycardia. The heart rate is often quite low, often in the 30s.
Medical management involves evaluating the patient's response and determining the cause of the dysrhythmia. Atropine and isoproterenol may be prescribed. A pacemaker frequently is needed with third-degree block (see Figure 8-8).
Premature ventricular contractions.
Premature ventricular contractions (PVCs) are abnormal heartbeats that arise from the right or left ventricle. PVCs are early ventricular beats that occur in conjunction with the underlying rhythm, which is unchanged except for the PVC itself.
PVCs may originate from more than one location in the ventricles and be caused by irritability of the ventricular musculature, exercise, stress, electrolyte imbalance, digitalis toxicity, hypoxia, and MI.
Clinical manifestations depend on the frequency of PVCs and their effect on the heart's ability to pump blood effectively. Some patients are asymptomatic; others may experience palpitations, weakness, and lightheadedness. Other symptoms are associated with decreased cardiac output.
Medical management focuses on treating the underlying heart condition. Symptomatic PVCs can be treated with beta-adrenergic blockers such as carvedilol (Coreg), antianginals, propranolol (Inderal), and antidysrhythmics such as procainamide, amiodarone, or lidocaine (Xylocaine).
A PVC may be a single event or may occur several times in a minute or in pairs or strings. PVCs that last long enough to cause ventricular tachycardia may lead to death.
Ventricular tachycardia.
Ventricular tachycardia (VT) occurs when three or more successive PVCs occur. In VT the ventricular rate is greater than 100 bpm (usually 140 to 240 bpm). The rhythm is regular or slightly irregular. Conditions that can cause its occurrence include hypoxemia, drug toxicity such as with digitalis or quinidine, electrolyte imbalance (e.g., potassium, magnesium), and bradycardia. Repeated and prolonged episodes of VT in the second week after MI may be a warning of ventricular fibrillation and require aggressive evaluation and treatment.
Medical management focuses on intravenously administered procainamide or amiodarone. These drugs depress excitability of cardiac muscle to electrical stimulation and slow conduction in the atria, bundle of His, and ventricles. Lidocaine is used only if acute myocardial ischemia or MI is considered to be the cause of VT. If pharmacologic measures are unsuccessful, the alternative is cardioversion. Catheter ablation can be helpful. Ongoing VT suppression is obtained with oral beta-adrenergic blockers or calcium channel blockers.
Ventricular fibrillation.
Ventricular fibrillation occurs when the ventricular musculature of the heart is quivering. This medical emergency is characterized by rapid and disorganized ventricle pulsation.
The cause is usually myocardial ischemia or infarction. Other causes are untreated VT, electrolyte imbalances, digitalis or quinidine toxicity, and hypothermia. It may also occur with coronary reperfusion after thrombolytic therapy.
Clinical manifestations are the result of no cardiac output and include loss of consciousness, lack of a pulse, decreases in blood pressure and respirations, possible seizures, and sudden death if untreated.
Medical management focuses on providing emergency treatment, including cardiopulmonary resuscitation (CPR), defibrillation (the termination of ventricular fibrillation by delivering a direct electrical countershock to the patient's precordium, i.e., that part of the patient's body surface covering the heart and stomach), and medications such as lidocaine or procainamide. Defibrillation is the most effective method of ending ventricular fibrillation and should ideally be performed within 15 to 20 seconds of onset to avoid brain damage from the lack of blood flow.
Assessment
Subjective data for the patient with a cardiac dysrhythmia include the patient's report of symptoms associated with the specific dysrhythmia. Symptoms may include palpitations, skipped beats, nausea, lightheadedness, vertigo, anxiety, dyspnea, fatigue, and chest discomfort.
Collection of objective data includes immediate visual observation of the patient when ECG monitoring indicates a dysrhythmia. Signs may include syncope, irregular pulse, tachycardia, and tachypnea. Noting the patient's response to the dysrhythmia is important to plan and implement appropriate nursing interventions. Monitor vital signs and observe for signs of decreased cardiac output.
Diagnostic Tests
Prior to treating a patient with a dysrhythmia, the health care provider needs to know if this is an abnormal or normal conduction occurrence of the heart. To find the cause or abnormality diagnostic tests are scheduled. Some of these can be performed without hospitalization.
ECG monitoring, telemetry, and Holter monitoring are commonly used to confirm the diagnosis of cardiac dysrhythmias and can be done without hospitalization. Laboratory work is also done to detect a medication toxicity. Treatment is aimed at the findings of the diagnostic tests.
Medical Management
Treatment varies according to the type of cardiac dysrhythmia (Table 8-1).
 Table 8-1
Table 8-1
Medications for Cardiac Dysrhythmias
| Generic Name (Trade Name) | Action | Nursing Interventions |
| Cardiac Glycoside | ||
| digoxin (Lanoxin) | Used to control rapid ventricular rate in atrial fibrillation and to convert paroxysmal supraventricular tachycardia to normal sinus rhythm Increases cardiac force and efficiency, slows heart rate, increases cardiac output | Monitor apical pulse to ensure rate is above 60 bpm (call health care provider if digoxin withheld) Monitor for digitalis toxicity (nausea, vomiting, anorexia, dysrhythmias, bradycardia, tachycardia, headache, fatigue, visual disturbance) |
| Antidysrhythmic Agents | ||
| procainamide (Pronestyl, Procan SR) | IV solutions given for severe ventricular dysrhythmias | Observe for new dysrhythmias, dry mouth, blurred vision, bradycardia, hypotension, nausea, anorexia, dizziness, visual disturbances |
| Depresses excitability of cardiac muscle to electrical stimulation and slows conduction in atrium, bundle of His, and ventricle, thus increasing refractory period | ||
| lidocaine (IV) | Suppresses the impulse that triggers dysrhythmias | Monitor heart rate and BP closely |
| disopyramide (Norpace CR) | Provides long-term treatment of premature ventricular contractions, ventricular tachycardia, and atrial fibrillation | Monitor BP and apical pulse |
| adenosine (Adenocard) | Slows conduction through AV node, can interrupt reentry pathways through AV node, and can restore normal sinus rhythm in patients with paroxysmal supraventricular tachycardia (PSVT) | Monitor BP, pulse rate, and respirations Assess patient for headache, dizziness, gastrointestinal complaints, new dysrhythmias Do not give caffeine within 4-6 hr of adenosine because caffeine inhibits the effect of the drug |
| amiodarone (Cordarone, Pacerone) | Prolongs duration of action potential and effective refractory period; provides noncompetitive alpha- and beta-adrenergic inhibition; increases P-R and Q-T intervals; decreases sinus rate; decreases peripheral vascular resistance. Used for severe ventricular tachycardia, supraventricular tachycardia, atrial fibrillation, ventricular fibrillation not controlled by first-line agents, cardiac arrest | Observe for headache, dizziness, hypotension, bradycardia, sinus arrest, heart failure, dysrhythmia Assess BP continuously for hypotension or hypertension Report dysrhythmia or bradycardia Monitor for dyspnea, chest pain |
| mexiletine (Mexitil) propafenone (Rythmol) | Decrease excitability of cardiac muscle | Monitor pulse, BP Monitor for diarrhea, visual disturbances, respiratory distress |
| tocainide (Tonocard) | Suppresses automaticity of conduction tissue | Notify health care provider if cough, wheezing, or shortness of breath occurs |
| Beta-Adrenergic Blockers | ||
| propranolol (Inderal) sotalol (Betapace) acebutolol (Sectral) esmolol (Brevibloc) metoprolol (Lopressor) carvedilol (Coreg) | Used to treat supraventricular and ventricular dysrhythmias, persistent sinus tachycardia Decrease myocardial oxygen demand, decrease workload of the heart, decrease heart rate | Monitor heart rate and BP carefully. Use caution with patient with bronchospastic disease Monitor for bradycardia, hypotension, new dysrhythmias, dizziness, headache, nausea, diarrhea, sleep disturbances |
| Calcium Channel Blockers | ||
| verapamil (Calan, Isoptin) diltiazem (Cardizem) | Treat supraventricular tachycardia and control rapid rates in atrial tachycardia Produce relaxation of coronary vascular smooth muscle, dilate coronary arteries | Use caution in patients with CHF Monitor apical pulse and BP Watch for fatigue, headache, dizziness, peripheral edema, nausea, tachycardia Both verapamil and diltiazem increase the toxicity of digoxin |
| Inotropic Agent | ||
| dobutamine (Dobutrex) (IV) dopamine (Intropin) (IV) | Used in severe CHF with pulmonary edema Increase myocardial contractility Increase cardiac output, increase BP, and improve renal blood flow | Monitor BP, heart rate, and urinary output continuously during the administration Palpate peripheral pulses; notify health care provider if extremities become cold or mottled |
| Anticoagulant | ||
| warfarin (Coumadin) | Used in treatment of atrial fibrillation with embolization to prevent complication of stroke | Assess patient for signs of bleeding and hemorrhage Monitor prothrombin time and International Normalized Ratio (PT/INR) frequently during therapy Review foods high in vitamin K. Patient should have consistently limited intake of these foods because these foods will cause levels to fluctuate |
AV, Atrioventricular; BP, blood pressure; bpm, beats per minute; CHF, congestive heart failure; HCl, hydrochloride; IV, intravenous.
Nursing Interventions and Patient Teaching
Nursing interventions focus on symptomatic relief, promotion of comfort, relief of anxiety, emergency action as needed, and patient teaching.
Assess the patient's apical pulse to obtain an accurate pulse rate when dysrhythmias are present. Because the rhythm is irregular, take the apical pulse for 1 minute. Assess the patient's anxiety and degree of understanding, noting both verbal and nonverbal expressions regarding diagnosis, procedures, and treatments.
Explain the diagnostic and monitoring devices in use. Monitor heart rate and rhythm. Administer antidysrhythmic agents as ordered and monitor response. Maintain a quiet environment; administer sedation or analgesic medication as ordered. Administer oxygen per protocol.
Nursing diagnoses and interventions for the patient with a cardiac dysrhythmia include but are not limited to the following:
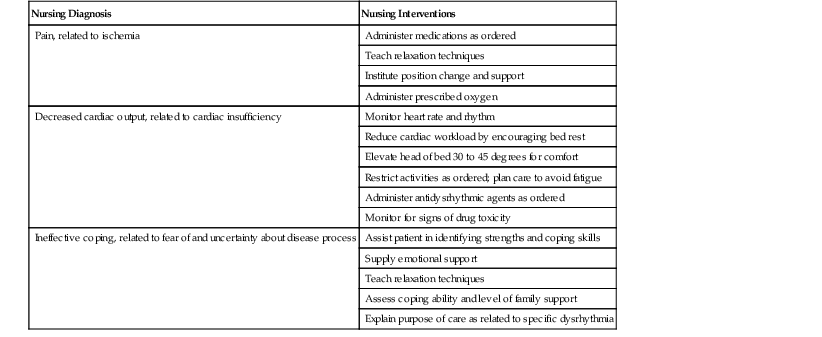
| Nursing Diagnosis | Nursing Interventions |
| Pain, related to ischemia | Administer medications as ordered |
| Teach relaxation techniques | |
| Institute position change and support | |
| Administer prescribed oxygen | |
| Decreased cardiac output, related to cardiac insufficiency | Monitor heart rate and rhythm |
| Reduce cardiac workload by encouraging bed rest | |
| Elevate head of bed 30 to 45 degrees for comfort | |
| Restrict activities as ordered; plan care to avoid fatigue | |
| Administer antidysrhythmic agents as ordered | |
| Monitor for signs of drug toxicity | |
| Ineffective coping, related to fear of and uncertainty about disease process | Assist patient in identifying strengths and coping skills |
| Supply emotional support | |
| Teach relaxation techniques | |
| Assess coping ability and level of family support | |
| Explain purpose of care as related to specific dysrhythmia |
Teach the patient the importance of lifestyle changes such as avoiding or stopping smoking or use of nicotine products. Teach the patient about medication therapy and its purposes, desired effects, and dosage and the side effects to report to the health care provider. Explain the reason for and method of taking pulse rate and rhythm. Explain the need to avoid exercising beyond the tolerance level, to avoid strenuous or isometric activity, and to check with the health care provider regarding limitations and allowances. Instruct the patient regarding conserving energy for activities of daily living (ADLs): taking regular rest periods between activities and for 1 hour after meals; when possible, sitting rather than standing while performing a task; and stopping an activity or task if symptoms such as fatigue, dyspnea, or palpitations begin. Stress management is important to promote healing and prevent further cardiac events.
Cardiac Arrest
The sudden cessation of cardiac output and circulatory process is termed cardiac arrest. Conditions leading to cardiac arrest are severe ventricular tachycardia, ventricular fibrillation, and ventricular asystole. The absence of oxygen–carbon dioxide exchange leads to symptoms of anaerobic tissue cell metabolism and respiratory and metabolic acidosis. Thus immediate CPR is necessary to prevent major organ damage. Signs and symptoms of cardiac arrest include abrupt loss of consciousness with no response to stimuli, gasping respirations followed by apnea, absence of pulse (radial, carotid, femoral, and apical), absence of blood pressure, pupil dilation, and pallor and cyanosis.
CPR is initiated by the first person to discover the condition. The aim is to reestablish circulation and ventilation. Prevention of severe damage to the brain, heart, liver, and kidneys as a result of anoxia (lack of oxygen) is of primary concern. Remember the CAB of CPR: C, circulation; A, restore airway; and B, restore breathing. Resuscitation measures are divided into two components: basic cardiac life support in the form of CPR and advanced cardiac life support (ACLS).
ACLS is a systematic approach to provide early treatment of cardiac emergencies. ACLS includes (1) basic life support, (2) the use of adjunctive equipment and special techniques for establishing and maintaining effective ventilation and circulation, (3) ECG monitoring and dysrhythmia recognition, (4) therapies for emergency treatment of patient with cardiac or respiratory arrest, and (5) treatment of patient with suspected acute MI.
Artificial Cardiac Pacemakers
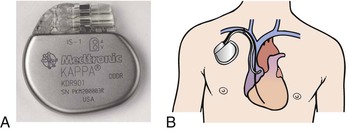
A pacemaker is made of titanium with computer circuits that control the pacing system; one or more leads are placed into the heart and a lithium battery is used (American Heart Association, 2012). It initiates and controls the heart rate by delivering an electrical impulse via an electrode to the myocardium. These catheter-like electrodes are placed within the area to be paced: right atrium, right ventricle, or both (see Figures 8-8 and 8-9). A permanent pacemaker power source is placed subcutaneously, usually over the pectoral muscle on the patient's nondominant side (American Heart Association, 2013a). Most are demand pacemakers, which send electrical stimuli to pace the heart when the heartbeat decreases below a preset rate. Some pacemakers have a single-chamber device with one lead that paces the right atrium or right ventricle; other pacemakers are dual-chamber with separate leads that connect to both the right atrium and the right ventricle (American Heart Association, 2013a).
Another pacemaker, the biventricular pacemaker, has three leads, one lead for each ventricle and one lead for the right atrium. This device restores normal simultaneous contraction of the ventricles. A biventricular pacemaker significantly improves left ventricular ejection fraction and exercise tolerance. It improves the quality of life for patients with worsening HF (American Heart Association, 2013a).
A pacemaker maintains a regular cardiac rhythm by electrically stimulating the heart muscle. It is used when patients experience adverse symptoms because of dysrhythmias that cannot be managed by medications alone. These include second- and third-degree AV block, bradydysrhythmia (slow and/or irregular heartbeat), and tachydysrhythmia (rapid heartbeat that can be regular or irregular).
An external pacemaker is used in emergency situations on a short-term basis. Temporary pacemakers are used for cardiac support after some MIs or open-heart surgery. A permanent pacemaker is placed when other measures have failed to convert the dysrhythmia or conduction problem. The batteries used in permanent pacemakers today are small, weighing less than 1 ounce, and can last 15 years or more.
Nursing Interventions and Patient Teaching
After placement of a pacemaker, closely monitor heart rate and rhythm by apical pulse and by ECG patterns. Check vital signs and level of consciousness frequently until stable. Observe the insertion site for erythema, edema, and tenderness, which could indicate infection. The patient may be on bed rest with the arm on the pacemaker side immobilized for the first few hours. Discharge teaching includes instructions not to lift the arm on the surgical side over the head for 6 to 8 weeks. The patient needs to refrain from swimming, golfing, and weight lifting until given permission by the health care provider (American Heart Association, 2013a).
Inform the patient of the necessity to continue medical management, and advise that he or she wear medical-alert identification and carry pacemaker information. Emphasize the importance of reporting signs and symptoms of pacemaker failure: weakness, vertigo, chest pain, and pulse changes.
Teach the patient to avoid potentially hazardous situations. Each pacemaker manufacturer can provide a list of devices that patients with pacemakers should avoid getting close to, such as high-output electrical generators or large magnets such as a magnetic resonance imaging (MRI) scanner. This may cause interference, placing the pacemaker in a fixed mode and interfering with its functioning. Instruct the patient to move away from any device that may cause untoward symptoms such as vertigo.
The pacemaker's pulse generator is set to produce a heart rate appropriate to the patient's clinical condition and the desired therapeutic goal. With rare exceptions, the rate is set between 70 and 80 bpm. If the heart rate falls below the preset level, notify the health care provider.
Teach the patient how and when to take a radial pulse. The pulse should be taken at the same time each day and when symptoms of vertigo or weakness occur. During patient education, remember to (1) list symptoms to expect and to report to the health care provider, (2) promote understanding of medication administration, (3) explain treatment outcomes, (4) explain the importance of maintaining prescribed diet and fluid amounts, and (5) explain the importance of not smoking. Teach the patient that shortness of breath occurring with exercise or exertion can be significant, because of the heart's inability to provide enough oxygen to the cells.
Prognosis
The patient can expect to lead a reasonably normal life with full resumption of most activities as prescribed by the health care provider.
Disorders of the Heart
Coronary Atherosclerotic Heart Disease
The coronary arteries arise from the base of the aorta just below the semilunar valves (see Figure 8-6). These arteries curve and branch to adequately supply the heart muscle with oxygen and nutrients. The shapes, contours, and arrangements of the vessels allow for easy entrapment of substances that interfere with blood flow.
Coronary artery disease (CAD) is the term used to describe a variety of conditions that obstruct blood flow in the coronary arteries. Atherosclerosis (a common arterial disorder characterized by yellowish plaques of cholesterol, lipids, and cellular debris in the inner layers of the walls of large and medium-size arteries) is the primary cause of ASHD. The lumen (a cavity or channel within any organ of the body) of the vessel narrows as the disease progresses. Blood flow to the heart is obstructed when this process occurs in the coronary arteries.
Atherosclerosis, the basic underlying disease affecting coronary lumen size, is characterized by changes in the intimal lining (the innermost layer) of the arteries. The severity of the disease is measured by the degree of obstruction within each artery and by the number of vessels involved. Obstructions exceeding 75% of the lumen of one or more of the three coronary arteries increase the risk of death.
The basic physiologic changes of the atherosclerotic process result in problems with myocardial oxygen supply and demand. When the myocardial oxygen demand exceeds the supply delivered by the coronary arteries, ischemia results (Figure 8-10). The artery walls also become less elastic and less responsive to blood flow (see Cultural Considerations box).

Angina Pectoris
Etiology and Pathophysiology
Angina means a spasmodic, cramplike, choking feeling. Pectoris refers to the breast or chest area. Angina pectoris refers to the paroxysmal (severe, usually episodic) thoracic pain and choking feeling caused by decreased oxygen flow to or lack of oxygen (anoxia) of the myocardium.
Angina pectoris occurs when the cardiac muscle is deprived of oxygen. Atherosclerosis of the coronary arteries is the most common cause. The narrowed lumina of the coronary arteries are unable to deliver enough oxygen-rich blood to the myocardium. When the myocardial oxygen demand exceeds the supply, ischemia (decreased blood supply to a body organ or part, often marked by pain and organ dysfunction) of the heart muscle occurs, resulting in chest pain or angina. Typically angina occurs with an increased cardiac workload brought on by exposure to intense cold, exercise, unusually heavy meals, emotional stress, or any other strenuous activity.
CAD is the number one killer in the United States. Many people who die from the disease, however, experience several episodes of unstable angina first. If unstable angina were accurately diagnosed and promptly managed, many deaths and much of the disability associated with CAD could be avoided.
 Cultural Considerations
Cultural Considerations
Cardiovascular Disorder
• White, middle-aged men have the highest incidence of coronary artery disease (CAD).
• African Americans and Hispanics have a higher incidence of hypertension than do white Americans.
• African Americans have an early age of onset of CAD.
• African American women have a higher incidence of CAD than do white American women.
• Native Americans younger than 35 years of age have a heart disease mortality rate twice as high as that of other Americans.
• Hispanics have a lower death rate from heart disease than do non-Hispanics.
• Major modifiable cardiovascular risk factors for Native Americans are obesity and diabetes mellitus.
Unstable angina is defined as an unpredictable and transient episode of severe and prolonged discomfort that appears at rest, has never been experienced before, or is considerably worse than previous episodes. It mimics an MI in that the discomfort it causes is often described as tightness or a crushing sensation in the chest, arms, back, neck, or jaw. For some patients, unstable angina is a red flag that an MI will occur.
Clinical Manifestations
Pain is the outstanding characteristic of angina pectoris (Figure 8-11). The patient usually describes the pain as a heaviness or tightness of the chest. At times it is thought to be indigestion. The pain is often substernal (below the sternum) or retrosternal (behind the sternum). Pain may radiate to other sites, or it may occur in only one site. The pain often radiates down the left inner arm to the little finger and also upward to the shoulder and jaw. Patients may also describe it as a pressure or a squeezing sensation, but usually not as a sharp pain. Sometimes a patient experiences posterior thoracic or jaw pain only. The chest pain may be accompanied by other signs and symptoms such as dyspnea, anxiety, apprehension, diaphoresis, and nausea. Symptoms of CAD in women vary and may be more subtle or generalized than in men. Women often report heaviness, squeezing, or pain in the left side of the chest, or pain in the abdomen, arm, mid-back, or scapular region. Women may also complain of palpitations and chest discomfort during rest, during sleep, or with exertion (American Heart Association, 2012a).

The signs and symptoms of angina are often similar to those of MI. Anginal pain is believed to be caused by a temporary lack of oxygen and blood supply to the heart. It is often relieved by rest or medication such as nitroglycerin, which dilates the coronary arteries and increases the flow of oxygenated blood to the myocardium. Nitroglycerin administered sublingually usually relieves angina symptoms but does not relieve the pain from an MI. This is often used as a preliminary diagnostic tool to quickly differentiate angina from an MI.
Diabetes can cause nerve damage that can make the usual signs and symptoms of chest pain harder to detect. The patient may have no pain with an MI. Patients with diabetes are still cautioned to go to the emergency room if they experience chest discomfort, sweating, or nausea and/or vomiting (American Diabetes Association, 2009).
Assessment
Subjective data include the patient's statements regarding the location, intensity, radiation, and duration of pain. The patient may express a feeling of impending death. Assess precipitating factors that led to the development of symptoms. Determine what relief measures have been used. Identify whether the symptoms have changed in frequency or severity, indicating a worsening of the ischemia.
Collection of objective data includes noting the patient's behavior, such as rubbing the left arm or pressing a fist against the sternum. Monitor vital signs and note changes or abnormalities. Increases in pulse rate, blood pressure, and respiratory rate may be noted. Identify the presence of diaphoresis or anxiety.
Diagnostic Tests
The diagnosis of angina pectoris is frequently based on the patient's history. The ECG may reveal ischemia and rhythm changes. Holter monitoring correlates activity with precipitating factors. The exercise stress test determines ischemic changes in a controlled environment. Thallium-201 scanning and PET are used to diagnose ischemic heart disease. Coronary angiography may be done to determine the extent of CAD.
Medical Management
The focus of medical management is to control symptoms by reducing cardiac ischemia. Cardiovascular risk factors are identified and corrected if possible. Precipitating factors—such as exposure to intense cold, strenuous exercise, smoking, heavy meals, and emotional stress—are identified and avoided. Anti–platelet aggregation therapy is a first-line treatment of angina. Aspirin (acetylsalicylic acid, ASA) is the drug of choice. Taking low-dose aspirin is reasonable for adults, who are at increased risk of cardiovascular disease. The American Heart Association recommends that men older than age 50 and women older than age 60 who have more than one cardiovascular risk factor take low-dose aspirin (American Heart Association, 2013). Risk calculations are aimed at people who have greater risk factors and are more likely to develop heart disease. For example, people who have a cholesterol level of 300 and smoke are at an increased risk of developing heart disease compared with someone who has a cholesterol level of 240 and doesn't smoke. Low-dose aspirin is indicated for people who have a calculated 10-year CAD risk of more than 10% (American Heart Association, 2013a). Aspirin, even at low doses (81 mg), is effective in inhibiting platelet aggregation. For patients unable to tolerate aspirin, ticlopidine (Ticlid) or clopidogrel (Plavix) may be given (Lewis et al., 2007). Medication therapy to dilate coronary arteries and decrease the workload of the heart consists of vasodilators (nitrates, especially nitroglycerin); beta-adrenergic blocking agents such as propranolol, metoprolol (Lopressor), nadolol (Corgard), atenolol (Tenormin), and timolol (Blocadren); and calcium channel blockers such as nifedipine (Procardia), verapamil, diltiazem, and nicardipine (Cardene). Give nitroglycerin sublingually for angina. Repeat the dose in 5 minutes if pain does not subside. Repeat two or three times at 5-minute intervals. Call the health care provider if pain has not subsided after a third nitroglycerin tablet. High-risk patients with unstable angina should be given supplemental oxygen.
Surgical interventions.
Coronary artery bypass graft: Surgical management of the patient with ASHD or CAD may consist of performing a coronary artery bypass graft (CABG) after diagnosis by cardiac catheterization. Any number of grafts can be done, depending on the areas of occlusion in the coronary arteries. Blood flows to the myocardium through the grafts, which bypass the occluded coronary arteries. The grafts are usually taken from sections of the saphenous veins in the legs, or the internal mammary (breast) artery is used.
When the saphenous vein is used for the graft, one end is sutured to the aorta and the other end is sutured to the coronary artery distal to the occlusion. When an internal mammary artery is used, the distal end of this vessel is freed from the anterior chest wall and sutured in place distal to the occlusion in the coronary artery. Internal mammary arteries are the preferred blood vessels for bypass surgery. A typical procedure involves one or two mammary arteries and saphenous vein grafts. Internal mammary arteries usually last more than 15 years, whereas saphenous vein grafts last an average of 5 to 10 years. Researchers continue to search for alternative blood vessels for CABG surgery (Figures 8-12 and 8-13).
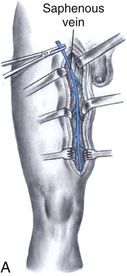
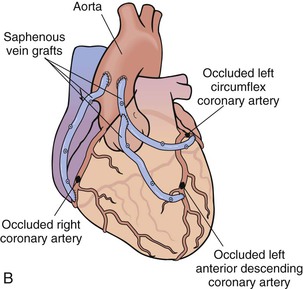
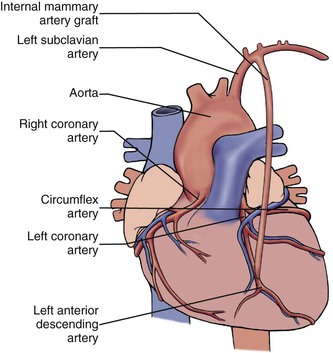
Percutaneous transluminal coronary angioplasty.
Percutaneous transluminal coronary angioplasty (PTCA) is a surgical procedure for management of the patient with CAD. PTCA is an invasive procedure performed in the cardiac catheterization laboratory. In an angioplasty, the narrowing in a coronary artery is widened without open-heart surgery. Percutaneous indicates that the procedure is performed through the skin; transluminal means that it is done within the lumen of the artery. Patients undergoing PTCA are required to sign an informed consent form allowing CABG surgery, because of the possibility of complications developing during the procedure that would require immediate surgical intervention. Fluoroscopy is used to guide a catheter from the femoral or brachial artery to the coronary arteries to be treated. A balloon catheter is inflated once it is positioned (Figure 8-14). The outward push of the balloon against the narrowed wall of the coronary artery reduces the constriction until it no longer interferes with blood flow to the heart muscle. Vessel patency (i.e., the state of being open, rather than blocked) is reestablished by angioplasty. This procedure may take 1 to 2 hours, with the patient usually awake but mildly sedated.
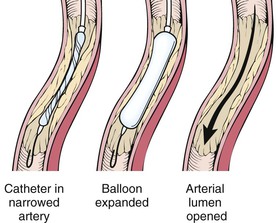
Postprocedure nursing interventions are to continually monitor the patient, as with any surgical recovery. Observe the area of catheter insertion for hemorrhage potential. Monitor the patient in the cardiac care unit, usually for 1 day before dismissal to the medical-surgical unit. The total hospitalization stay is 1 to 3 days compared with the 4- to 6-day stay after open heart surgery with a CABG; thus PTCA reduces hospital costs. Patients return to work rapidly (approximately 5 to 7 days after PTCA) rather than requiring the 2- to 8-week convalescence common after CABG.
Stent placement.
Stents are used to treat abrupt or threatened vessel closure after PTCA. Stents are expandable, meshlike structures designed to maintain vessel patency by compressing plaque against the arterial walls and resisting vasoconstriction. Stents are carefully placed at the angioplasty site to hold the vessel open. Stents are thrombogenic and require the patient to take anticoagulants for at least 3 months. The primary complications from stent placement are hemorrhage and vascular injury. Less common complications are stent thrombosis, acute MI, emergency CABG, and coronary spasms. The possibility of dysrhythmias is always present.
Nursing Interventions and Patient Teaching
Nursing interventions are based on the patient's individual needs. They focus on achievement of five major patient outcomes.
1. Ensure comfort. Reduce or remove any known factors that are contributing to increased pain. Assess for causes of decreased pain tolerance, such as anxiety, fatigue, or lack of knowledge. Fatigue from increased oxygen demands with a decreased oxygen supply increases pain perception. Promote measures to reduce fatigue, such as providing rest periods. Provide a calm environment to decrease stress and anxiety. Administer sublingual vasodilators, such as nitroglycerin, as ordered. Administer oxygen for high-risk patients with unstable angina and those with cyanosis or respiratory distress.
2. Promote tissue perfusion. Instruct the patient to avoid becoming overly fatigued and to stop activity immediately in the presence of chest pain, dyspnea, syncope, or vertigo, which indicate low tissue perfusion.
3. Encourage activity and rest. Increase the patient's activity tolerance by encouraging slower activity or shorter periods of activity with more rest periods. Most people with angina pectoris are able to tolerate mild exercise such as walking or playing golf, but exertion such as running or climbing stairs rapidly causes pain. Nitroglycerin may be used prophylactically to prevent pain from strenuous activities. Isosorbide mononitrate (Imdur) or isosorbide dinitrate (Isordil) are nitrates used for acute treatment of angina attacks (sublingual only) or orally for prophylactic management of angina pectoris. Anginal pain occurs more easily in cold weather. The key is to avoid overexertion.
4. Reduce anxiety and promote feelings of well-being. Help the patient reduce the level of anxiety. The patient should minimize emotional outbursts, worry, and tension. People with angina may need continuing help in accepting situations. Supportive family members, a spiritual adviser, business associates, and friends can sometimes be of assistance. Relaxation techniques and music therapy may be beneficial. Peer support groups and behavioral change programs are available. An optimistic outlook helps to relieve the work of the heart. Many people who learn to live within their limitations live out their expected lifespan despite the disease.
5. Provide education to the patient and the family. Delay teaching until the patient is ready (see Communication box). The patient needs to be relatively free of pain and anxiety to learn. Promote a positive attitude and active participation of patient and family to encourage compliance. The teaching plan should include information on medications, ways to minimize the events that trigger angina pectoris, effects of exercise on reduction of myocardial oxygen needs, the need to stop smoking because of the vasoconstriction of nicotine, and the need for regular medical follow-up (see Patient Teaching box).
 Communication
Communication
Methods to Decrease Angina Pectoris Attacks
Mrs. M., a patient with angina, has been admitted for further care, diagnosis, and treatment. After the initial nursing assessment, the nurse interviews the patient about the course of her anginal episodes. With the data she gathers, the nurse will participate in the development of a program to educate Mrs. M. how to minimize or control the attacks.
Nurse: I would like to ask you some questions about the anginal pain you are experiencing.
Patient: I already told the doctor about those attacks when I visited his office. Her nurse has all those records.
Nurse: Your health care provider asked us to help you plan a program for preventing or minimizing these attacks. With the information we gather, we can set goals for your care. We can also identify how angina relates to some of your activities.
Patient: OK, I would like to understand it better. Perhaps I would be less frightened when it happens. My friend told me about her aunt who had angina—she died. That really worries me.
Nurse: We hope to decrease some of your fears by helping you understand. First, when do your attacks usually occur?
Patient: Oh, mostly after a really busy day, you know—shopping or gardening or housecleaning. But a few times I had problems after my sister-in-law visited. She and my husband always seem to get into upsetting discussions. They never got along well. She upsets us both—she criticizes everything!
Nurse: Have you noticed if a big meal is related to the pain?
Patient: No, not really . . . well, only when my sister-in-law is there. We hardly ever eat big meals anymore, except when she comes. She expects to be fed well. My husband and I have cut down a lot. Big meals upset our systems—and then her, that harping on old problems, and how she thinks we should run our lives! She upsets me so!
Nurse: Mrs. M., I think we should talk about how to handle stressful situations like visits from your sister-in-law. But first, could you describe the pain for me? Does it come on suddenly? How long does it last? What does it feel like?
Patient: Oh, no, not all of a sudden. It is just dull at times, like an upset stomach. But then, it travels up in my chest and gets really heavy, like pressure. Sometimes it makes my face and teeth hurt . . . and my arm, too—this one [left]—all the way down to my little finger. If it's a really bad attack, I sometimes feel like I am going to vomit.
Nurse: On a scale of 0 to 10, how would you rate most of your angina attacks?
Patient: Probably 5 to 6 would be the average, but sometimes it's a 10.
Nurse: Does your heart beat faster?
Patient: Oh, yes, and I just have to sit down and be quiet or I can't catch my breath. That's when I take the nitroglycerin. I carry it with me all the time now, in this special little container.
Nurse: I see. And how long does it take for the pain to stop after you take the medicine?
Patient: I used to think it took forever, but my husband—he times it for me—says it lasts about 15 to 20 minutes. I relax a little, and it passes.
Nurse: What about the weather? Have you noticed that it affects your attacks in any way?
Patient: I don't know if it is all those clothes or the weather, but I get more pains if I get out in the cold.
Nurse: Do you or your husband smoke?
Patient: Not anymore. I gave up cigarettes when this angina started on me. I noticed the difference, too. Now I can't even stay in a room if people are smoking. I also cut down on coffee when I retired. My doctor said that too much caffeine isn't good for my heart. All the good things, they have to go when you get old!
Nurse: Maybe with some understanding of how certain activities and other factors affect your condition, you can find new “good things” that you'll enjoy just as much. We'll talk again soon. There are some effective coping methods we can explore to decrease your stress when your sister-in-law visits.
 Patient Teaching
Patient Teaching
Angina Pectoris
Using Nitrate Medications
• Use nitroglycerin prophylactically to avoid pain known to occur with certain activities.
• A burning sensation on the tongue indicates nitroglycerin is activated.
• A throbbing sensation in the head and flushing may occur.
• When changing to a sitting or standing position, do it slowly after taking nitroglycerin. Postural hypotension is a side effect of nitroglycerin.
• Place a nitroglycerin tablet under the tongue at the onset of anginal pain; a second tablet can be taken after 5 minutes and a third tablet after another 5 minutes if pain is unrelieved.
• Call the health care provider if pain does not subside after the third nitroglycerin tablet; go to the nearest emergency department; do not drive yourself.
• Always carry nitroglycerin on your person.
• Store nitroglycerin in a dark bottle and keep it in a dry place.
• Replenish nitroglycerin supply every 6 months or before the expiration date.
• Remove all old nitrate ointment before application of new cream.
• Place nitroglycerin patches on skin in the morning and remove at bedtime. This prevents development of tolerance and maintains effectiveness.
Minimizing Precipitating Events
• Use caution when taking medications for erectile dysfunction. Nitrate medications may result in severe hypotension.
• Avoid overexertion. Take nitroglycerin before exercise.
• Try to reduce stress and anxiety, which cause blood vessels to constrict.
• Avoid overeating because it places an increased workload on the heart.
• Avoid cold weather (constricts coronary vessels to conserve body heat; hence anginal pain can develop more easily).
• Dress warmly in cold weather.
• Avoid hot, humid conditions (increases workload on the heart).
• Avoid walking uphill, in the cold, or against strong wind, since these activities increase the workload on the heart.
• Discontinue smoking. Nicotine causes vasoconstriction of the arteries.
Nursing diagnoses and interventions for the patient with angina pectoris include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Pain, related to myocardial ischemia | Administer oxygen as ordered |
| Administer prescribed nitroglycerin. Repeat q 5 min, three times. If pain is unrelieved, notify health care provider | |
| Monitor blood pressure and pulse before and after administration of nitroglycerin | |
| Promote rest | |
| Maintain diet as ordered; if chest pain occurs while eating or immediately after, advise small feedings rather than two or three large meals | |
| Balance rest with activity | |
| Instruct patient to stop activity at the first sign of chest pain or other symptoms of cardiac ischemia | |
| Ineffective tissue perfusion, cardiovascular, related to narrowing of coronary arteries | Administer prescribed oxygen |
| Instruct patient that nitroglycerin may need to be taken before exercise and sexual activity to prevent cardiac ischemia | |
| Encourage less strenuous or shorter periods of activity interspersed with rest | |
| Avoid exercise in cold weather | |
| Take prescribed nitroglycerin before activities that will increase the workload of the heart |
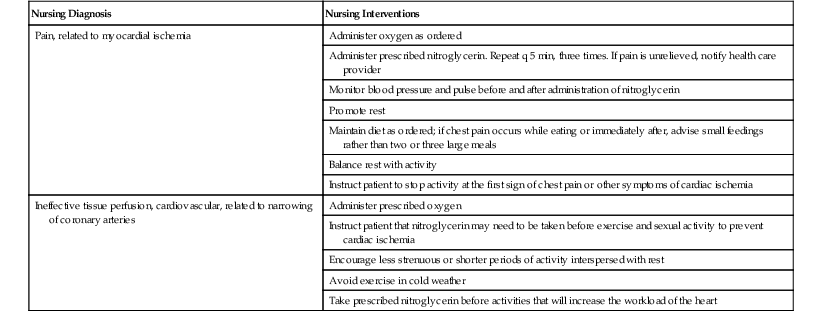
Prognosis
The prognosis for the patient with angina pectoris may be grave. Attacks may be intermittent. The patient with diabetes who also has coronary artery disease may have the highest risk of all. A patient with diabetes may have nerve damage, making the normal warning signs of a myocardial infarction (MI) more difficult to detect. Early management of the patient with diabetes includes teaching lifestyle changes as well as how to recognize the signs and symptoms of an MI. The mortality rate can be reduced with early and aggressive management of angina.
Myocardial Infarction
Etiology and Pathophysiology
A myocardial infarction (MI), or heart attack, is the necrosis (death) of heart muscle. It is caused by obstruction of a major coronary artery or one of its branches, either by an atherosclerotic plaque or by an embolus (a foreign object, a quantity of air or gas, a bit of tissue, or a piece of a thrombus that circulates in the bloodstream until it becomes lodged in a vessel). The obstruction leads to tissue ischemia (oxygen deprivation) due to the lack of blood supply. An occlusion can occur anywhere in the body; coronary occlusion refers specifically to the obstruction or closing off of a coronary artery. Eighty to ninety percent of all acute MIs are the result of thrombus formation (American Heart Association, 2012a), also called coronary thrombosis. Myocardial ischemia lasting more than 35 to 45 minutes produces cellular damage and necrosis. These conditions impair the ability of the cardiac muscle to contract and pump blood. The extent of damage to the surrounding tissues depends on the ability of the heart to develop collateral circulation. Collateral circulation is the development of new vessels in the heart that compensate for the loss of circulation from the occluded artery. The location of the occlusion and the extent of tissue damage affect the patient's response to the injury (Figure 8-15).
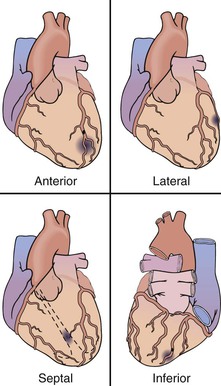
The body's response to cell injury is inflammation. Within 24 hours leukocytes infiltrate the area in response to chemicals released by the injured cardiac cells. (Note: Dying cardiac cells also release enzymes that are important diagnostic indicators; see the sections “Laboratory Tests” [above] and “Diagnostic Tests” [below] for a discussion on serum cardiac markers.) Phagocytes (neutrophils and monocytes)—a kind of leukocyte—clear the necrotic debris from the injured area, and by 6 weeks after an MI, scar tissue has replaced the necrotic tissue.
Clinical Manifestations
Sometimes an asymptomatic MI or silent MI may occur. Many symptoms of MI are associated with irreversible ischemia, but they are similar to those of angina pectoris. In an MI, the symptoms are more severe and last longer than during an angina attack. Pain is the foremost symptom of MI (Table 8-2).
Table 8-2
Signs and Symptoms of Myocardial Infarction
| SUBJECTIVE DATA (SYMPTOMS) | OBJECTIVE DATA (SIGNS) |

The pain location and radiation to other sites are depicted in Figure 8-11. The pain is often described as crushing or viselike, an oppressive sensation as though a heavy object is sitting on the chest. The pain is retrosternal (behind the sternum) and in the heart region. In men, it often radiates down the left arm and to the neck, jaws, teeth, and epigastric area. It may occur suddenly, or it may build up over a few minutes. It may occur in conjunction with intense emotion, during exertion, or at rest. The pain is prolonged and more intense than anginal pain. It lasts 30 minutes to several hours or longer. It is not relieved by changes in body position, nitroglycerin, or rest. Health care providers often tell patients who call complaining of chest pain to take an aspirin (chewable if they have it) and report to the hospital emergency department. Other signs and symptoms that may occur with the pain include nausea, dyspnea, dizziness, weakness, diaphoresis, pallor, ashen color, and a sense of impending doom. Early signs and symptoms of an acute MI in women are unusual fatigue, sleep disturbances, shortness of breath, weakness, indigestion, and anxiety. Often, acute chest pain is not present. With these signs and symptoms, an acute MI can commonly be misdiagnosed as indigestion, gallbladder disease, depression, or anxiety (Mayo Clinic, 2011). Table 8-3 provides a comparison of signs and symptoms and the medical management of angina pectoris and MI.
Table 8-3
Coronary Artery Disorders
| SIGNS AND SYMPTOMS | MEDICAL MANAGEMENT |
| Angina Pectoris | |
| Chest pain (substernal, retrosternal), may radiate to neck, jaw, left arm, and shoulder; great anxiety, fear of approaching death; face pale, ashen; pulse variable, usually tense and quick; blood pressure elevated during an attack; usually brought on by exertion, emotional upsets; relieved by rest, nitroglycerin | |
| Myocardial Infarction | |
| Severe, crushing chest pain; prolonged heavy pressure or squeezing pain in center of chest; may spread to shoulder, neck, arm, fourth and fifth fingers on left hand, teeth, and jaw; may radiate as with angina; not relieved with rest or nitroglycerin; may be associated with dyspnea, diaphoresis, apprehension, nausea, and vomiting; signs and symptoms of cardiogenic shock may develop; the pain is prolonged and more intense than anginal pain | |
| In women, these classic symptoms are far less common; most frequent early warning symptoms are unusual fatigue, sleep disturbances, shortness of breath, weakness, indigestion, and anxiety; in one study, only 30% of women reported chest pain, and acute chest pain was absent in 43% (Sherrod et al., 2007) | |
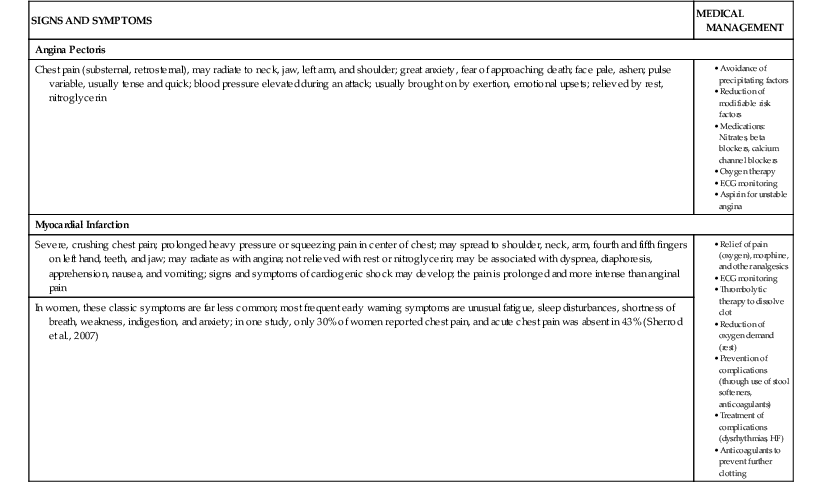
ECG, Electrocardiogram; HF, heart failure.
Assessment
Subjective data include the onset, location, quality, duration, and radiation of pain. The patient may complain of shortness of breath, dizziness, weakness, anxiety, fear, or unusual fatigue. Identify precipitating factors. Inquire about measures the patient has tried to relieve the pain.
Collection of objective data includes observation of the patient's behavior to detect apprehension and anxiety. Typical vital signs reveal hypotension, pulse abnormalities such as tachycardia or a barely perceptible pulse, and early temperature elevation. Note the presence of diaphoresis; vomiting; ashen color; cool, clammy skin; labored respirations; and cardiac dysrhythmias. If possible, find out about risk factors. A respiratory assessment should also be done.
Diagnostic Tests
Diagnostic tests are used to confirm the diagnosis of MI. Serum tests are initially obtained. Serum cardiac markers (e.g., CK-MB, myoglobin) are released into the vascular system when infarcted myocardial muscle cells die. A sensitive cardiac marker present in serum, called troponin I, has proven useful in detecting ischemic myocardial injury. Troponin I is cardiac specific and therefore a highly specific indicator of an MI. (See the section “Laboratory Tests,” above, for a discussion on serum cardiac markers.) An elevated white blood cell count of 12,000 to 15,000/mm3 is associated with severe infarcts. The increase begins a few hours after the onset of pain and lasts for 3 to 7 days. The ESR rises during the first week and may remain elevated for several weeks.
Twelve-lead ECG findings that support the diagnosis of MI include ST-segment elevation and the development of Q waves. In time the ST segment returns to normal and the T wave inverts. These ECG changes are important in confirming the diagnosis of MI. ECG findings are significantly different for men and women. A woman experiencing an MI is far less likely than a man to have concurrent ST-segment elevation, resulting in misdiagnosis and failure to receive the correct treatment. A chest radiograph is done to note size and configuration of the heart. More complex tests are occasionally done, including cardiac fluoroscopy, myocardial imaging (thallium scan), echocardiogram, PET, and multigated acquisition (MUGA) scanning. These tests may be done in conjunction with other tests to diagnose MI and determine the severity of CAD.
Medical Management
Medical management focuses on preventing further tissue injury and limiting the size of the infarction. It is extremely important that a patient with a suspected MI be rapidly diagnosed and treated to preserve cardiac muscle. Intervention is designed to restore cardiac tissue perfusion and reduce the workload of the heart. Promoting tissue oxygenation, relieving pain, preventing complications, improving tissue perfusion, and preventing further tissue damage are all important medical considerations.
Medications such as morphine and diazepam (Valium) are used to alleviate pain and anxiety. A continuous IV infusion of amiodarone may be given to the patient who has frequent PVCs, which may precede ventricular fibrillation. Prophylactic lidocaine is not recommended by the American College of Cardiology practice guidelines for the treatment of acute MI. Lidocaine may be a treatment option for the patient who has sustained VT or ventricular fibrillation. The use of beta-adrenergic blockers such as atenolol, metoprolol, propranolol, nadolol, and carvedilol (Coreg) early in the acute phase of an MI and during a 1-year follow-up regimen can decrease morbidity and mortality. Angiotensin-converting enzyme (ACE) inhibitors may be used after MIs. Their use can help to prevent or slow the progression of HF (Table 8-4). Calcium channel blockers or longer-acting nitrates can be added if the patient is already on adequate doses of beta-adrenergic blockers or cannot tolerate beta-adrenergic blockers. Examples of calcium channel blockers are amlodipine (Norvasc), diltiazem, nifedipine, and verapamil. An example of a long-acting nitrate is isosorbide dinitrate (National Library of Medicine, 2012b). Oxygen is prescribed to facilitate cardiac tissue perfusion. Attention is given to respiratory difficulties, fluid overload, and cardiac dysrhythmias.
Table 8-4
Medications for Myocardial Infarction
| CLASSIFICATION | GENERIC NAME (TRADE NAME) | ACTION |
| Vasopressor | dopamine (Intropin) | Raises systemic arterial pressure and cardiac output |
| Anticoagulants | heparin warfarin (Coumadin) | Reduce incidence of clotting |
| Platelet aggregation inhibitor | ticlopidine (Ticlid) | Decreases platelet release of thromboxane, so that vasoconstriction and platelet aggregation are decreased |
| aspirin (acetylsalicylic acid; ASA) | Decreases platelet aggregation | |
| Analgesic | morphine | Controls pain; reduces myocardial oxygen demand |
| Tranquilizer | diazepam (Valium) | Decreases anxiety and restlessness |
| Thrombolytic agent | streptokinase (Streptase) | Thrombolytic (pertaining to dissolution of blood clots) agent used when acute MI symptoms have been present less than 6 hr, preferably from 30 min to 1 hr; restores blood flow and therefore limits infarct size in certain patients |
| Tissue plasminogen activator | activase (Alteplase, recombinant) | Dissolves blood clots and reduces blood viscosity |
| Nitrates | nitroglycerin isosorbide atenolol (Tenormin) | Dilate blood vessels by reducing coronary artery spasm, increase coronary artery blood supply, and decrease oxygen demands |
| Beta-adrenergic blockers | propranolol (Inderal) nadolol (Corgard) metoprolol (Lopressor) carvedilol (Coreg) | Block beta-adrenergic stimulation and decrease myocardial oxygen demands, thus decreasing myocardial damage; decrease mortality rate |
| Calcium channel blockers | nifedipine (Procardia) diltiazem (Cardizem) verapamil (Calan, Isoptin) amlodipine (Norvasc) | Dilate blood vessels, increase coronary artery blood supply, and decrease myocardial oxygen demands |
| Angiotensin-converting enzyme (ACE) inhibitors | captopril (Capoten) enalapril (Vasotec) | Can help prevent ventricular remodeling and prevent or slow the progression of HF Prevent conversion of angiotensin I to angiotensin II Decrease endothelial dysfunction |
| Salicylates | aspirin | Decrease platelet adhesion and thus decrease thrombosis formation |
| Antidysrhythmics | lidocaine (Xylocaine) IV | Treat ventricular dysrhythmias (rarely used except for ventricular tachycardia) |
| Stool softeners | docusate calcium (Surfak) docusate sodium (Colace) | Reduce straining at stool; prevent constipation produced by decreased mobility and use of constipating narcotics |
| Diuretics | furosemide (Lasix) | Control edema |
| Electrolyte replacement | potassium chloride (Slow-K) | May be necessary when diuretics are used |
| Inotropic agents | digoxin (Lanoxin) amrinone (Inocor) IV dobutamine (Dobutrex) | Increase the heart's pumping action (contractility) Indicated when left ventricle failure is present |
HF, Heart failure; IV, intravenous; MI, myocardial infarction.
Medical therapy is also directed toward limiting the size and extent of injury by attempting to reperfuse (reinstitute blood flow to) the occluded coronary artery. Fibrinolytic agents such as streptokinase (Streptase), anistreplase, and a tissue plasminogen activator (tPA) such as alteplase are currently used to attempt reperfusion. Thrombolytic therapy is the standard practice in the treatment of acute MI. Thrombolytics salvage heart muscle by minimizing infarct size and maximizing heart function. They lyse (decompose or dissolve) the clot in the occluded coronary artery, reopening the vessel and allowing perfusion of the heart muscle.
The adage “Time is muscle” highlights the need for fast action and prompt treatment to restore myocardial blood flow, limit infarct size, preserve heart tissue, and improve the patient's chance of survival and recovery. To be effective, reperfusion must occur 3 to 5 hours after the onset of symptoms. Myocardial cells do not die instantly. In most patients, it takes approximately 4 to 6 hours for the entire thickness of the muscle to become necrosed. Mortality and infarction size can be significantly reduced if thrombolytic therapy starts within 30 to 60 minutes of symptom onset. Before a thrombolytic is administered, obtain a thorough history. Thrombolytics are not used for patients with active internal bleeding, suspected aortic dissecting aneurysm, recent head trauma, history of hemorrhagic stroke within the past year, or surgery within the past 10 days.
PTCA may be used instead of thrombolytic therapy as a primary treatment in some cases. This involves advancing a balloon-tipped catheter into the lumen of the obstructed coronary artery. The balloon is inflated intermittently to dilate the artery and improve blood flow (see Figure 8-14). Along with balloon compression, stents may be used to prevent acute closure and restenosis (i.e., repeat narrowing of the blood vessel).
CABG surgery may be considered for patients with multiple vessel disease and when less invasive interventions, such as thrombolysis and PTCA, have failed (see Figures 8-12 and 8-13).
Complications commonly associated with MI include ventricular fibrillation, cardiogenic shock (Box 8-2), HF, and dysrhythmias. Cardiogenic shock, often referred to as pump failure, is characterized by low cardiac output and peripheral vascular system collapse. Left ventricular function is severely decreased, resulting in an inadequate blood supply to the vital organs. Immediate detection and treatment are necessary to prevent irreversible shock and death. Cardiogenic shock proves fatal in 50% to 80% of cases. Other possible complications include ventricular aneurysm, pericarditis, and embolism.
Box 8-2
Cardiogenic Shock
| CLINICAL MANIFESTATIONS | SIGNS AND SYMPTOMS | MEDICAL MANAGEMENT | NURSING INTERVENTIONS |
Anxiety, agitation, restlessness, disorientation Urinary output diminished or absent Lactic acid accumulation in blood Tachycardia, thready pulse, tachypnea Narrowed pulse pressure* Cyanosis; cold, moist, pale, clammy skin | Recognition and control of life-threatening signs and symptoms Oxygenation to promote tissue perfusion • Vasopressors: Raise arterial blood pressure • Cardiac glycoside: Digoxin (Lanoxin) increases cardiac contraction (inotropic) and strengthens and corrects dysrhythmias • Adrenergic drugs: Dopamine (Intropin) at therapeutic levels increases cardiac output and blood pressure • Sodium bicarbonate: Combats lactic acidosis (given sparingly because it causes fluid retention) |

* Pulse pressure is based on blood pressure: It is the numeric difference between the systolic and diastolic blood pressure. For example, if the blood pressure is 100/70 mm Hg, the pulse pressure is 30.
Nursing Interventions and Patient Teaching
Administer oxygen per protocol or at 2 L/minute for 24 to 48 hours or longer if pain, hypotension, dyspnea, or dysrhythmias persist. Administer medications as prescribed (see Table 8-4).
• Administer lipid-lowering agents such as simvastatin, atorvastatin (Lipitor), or rosuvastatin to prevent elevated cholesterol levels.
• Stool softener may be prescribed to prevent rectal straining. The Valsalva maneuver may cause severe changes in blood pressure and heart rate, which may trigger ischemia, dysrhythmias, or cardiac arrest.
To help the patient recovering from an MI minimize straining, offer the use of a bedside commode or nearby bathroom whenever possible. The patient may use the Valsalva maneuver when straining to pass stool. Teach mouth breathing to help decrease the severity of straining, which is contraindicated for the patient after an MI.
Instruct the patient to avoid excessive fatigue and to stop activity immediately when chest pain, dyspnea, or faintness occur. Plan nursing interventions to promote rest and minimize disturbances. Monitor the vital signs; document the rate and rhythm of the pulse.
The patient is usually placed on bed rest with commode privileges for 24 to 48 hours. Assist the patient with ADLs. During this period, sedation with diazepam or an equivalent may be prescribed to relieve anxiety and restlessness and to promote sleep. After the first 24 to 48 hours, encourage the patient to increase activity gradually, depending on the severity of the infarction. Continually monitor the patient for signs of dysrhythmias, cardiac pain, and changes in vital signs.
Food is usually withheld until the patient's condition becomes stable because the patient may need to undergo cardiac catheterization, PTCA, or a CABG procedure. A liquid diet progresses as tolerated to a regular diet with modifications. A low-fat, low-sodium, easily digested diet is desirable.
To prevent complications, antiembolic stockings are used. Continue to assess and report cardiac status, dyspneic condition, and pulse change (rate, rhythm, and volume).
During hospitalization, many patients experience denial, depression, and anxiety. Anxiety varies in intensity, depending on the severity of the perceived threat and the patient's success in coping.
Nursing diagnoses and interventions for the patient with an MI include but are not limited to the following.
| Nursing Diagnosis | Nursing Interventions |
| Acute chest pain, related to myocardial ischemia | Assess original pain and location, duration, radiation, and onset of new symptoms |
| Administer prescribed analgesics (usually morphine sulfate, which relieves pain, reduces anxiety, causes vasodilation of vascular smooth muscle, and reduces myocardial workload) | |
| Maintain bed rest and reduced patient activity | |
| Administer oxygen as prescribed | |
| Record patient's response to pain relief measures | |
| Employ alternative methods of pain relief | |
| Provide calm, restful environment | |
| Decreased cardiac output, related to conduction defects (dysrhythmias) and decreased myocardial pumping action | Assess and monitor vital signs q 4 hr |
| Maintain bed rest with head of bed elevated 30 degrees for first 24-48 hr to reduce myocardial oxygen demand | |
| Monitor IV feedings; infuse according to health care provider's order | |
| Administer prescribed medications such as antidysrhythmics, nitrates, and beta blockers | |
| Auscultate breath sounds and heart rate q 4 hr; increase activity level as prescribed | |
| Palpate for pedal pulses, assess capillary refill, auscultate bowel sounds, assess for pedal or dependent edema q 4 hr, and strictly monitor intake and output (I&O) |
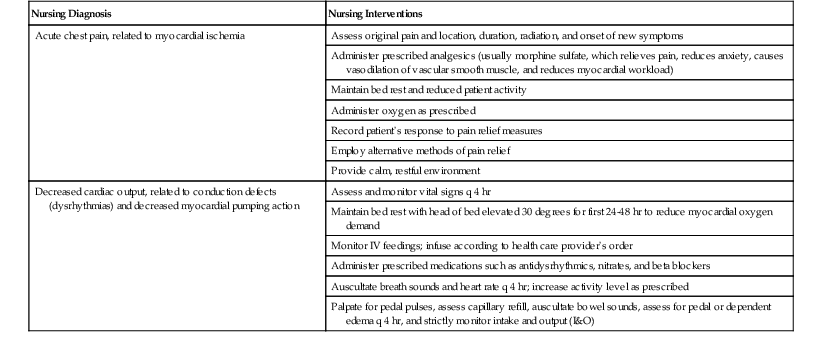
Patients and their family members need to be reassured of recovery. More than 85% of patients with an uncomplicated MI return to work. Provide information on resuming sexual activities. The patient with an uncomplicated MI who is able to climb two flights of stairs without difficulty is usually able to resume sexual activities. Approximately 80% of all postcoronary patients resume sexual activity without serious risks. The other 20% need not abstain totally, but should limit their sexual activity according to their cardiac capacity.
Cardiac rehabilitation.
The health care provider may prescribe cardiac rehabilitation after an MI. Before discharge from the hospital, discuss how participation in a monitored exercise program and continuing education as part of outpatient cardiac rehabilitation will help the patient recover faster and return to a full and productive life. Cardiac rehabilitation has two major parts:
1. Exercise training to teach the patient how to exercise safely, strengthen muscles, and improve stamina. The exercise plan is based on the individual's ability, needs, and interests.
2. Education, counseling, and training to help the patient understand his or her heart condition and find ways to reduce the risk of future heart problems. The cardiac rehabilitation team assists the patient in adjusting to a new lifestyle and dealing with fears about the future. Cardiac rehabilitation may last 6 weeks, 6 months, or longer. Cardiac rehabilitation has lifelong favorable effects (see Home Care Considerations box and Health Promotion box).
 Home Care Considerations
Home Care Considerations
Exercise Program After Myocardial Infarction
• After discharge from the hospital, many patients are encouraged to begin a 2- to 12-week walking program. This is a structured program designed to have the patient walking 2 miles in less than 60 minutes by the end of 12 weeks.
• Encourage patients to work through this program at their own rate until they achieve a pace below a slow jog and their heart rate is below the prescribed rate set by the cardiologist.
• Not all patients are physiologically capable of participating in a rigorous exercise program after an MI.
• Eventually, most patients are encouraged to participate in a maintenance (lifetime), unsupervised, home-based exercise program designed specifically for them.
• Almost everyone can benefit from some type of cardiac rehabilitation.
 Health Promotion
Health Promotion
Myocardial Infarction
• Teach the patient the following:
• The effects of MI, the healing process, and the treatment regimen.
• The effects of medications used to treat MI.
• The association between risk factors and coronary artery disease (CAD).
• How to identify nonmodifiable risk factors.
• How to identify modifiable risk factors (particularly cigarette smoking and stress). The patient should stop smoking and encourage family and significant others to stop.
• The effect of dietary restrictions on atherosclerotic heart disease or CAD. Recommended daily intake is 2 g of sodium, 1500 calories, low cholesterol, and fluid restrictions.
• To limit total fat intake to 25% to 35% of total calories each day. Limit intake of saturated fats to less than 7% of total fat intake. Saturated fats (e.g., shortening, lard, or butter) are solid at room temperature; better sources of fat include vegetable, olive, and fish oils.
• To avoid foods high in sodium, saturated fats, and triglycerides. Review alternative ways of seasoning foods to avoid cooking with salt. Explain the need to limit intake of eggs, cream, butter, and foods high in animal fat. Teach the patient and family how to read labels on foods.
• To eat 20 to 30 g of soluble fiber every day. Foods such as bran, beans, and peas help lower bad cholesterol (low-density lipoprotein).
• The effect of activity on the heart and the need to participate in a progressive activity plan.
• Refer the patient to social support groups as indicated.
• Stress the importance of participating in cardiac rehabilitation services.
• Explain cardiac warning symptoms. Patients and their partners are often unsure which symptoms should be reported. If nitroglycerin has been prescribed, advise the patient to take it when experiencing chest pain and to notify the health care provider if the pain is not relieved within 15 minutes. Other signs to report include shortness of breath, rapid heart rate, dizziness, insomnia, a persistent increase in heart rate or blood pressure, and extreme fatigue after sexual activity.
• Most patients have concerns about resuming sexual activity after an MI but may not express them to the nurse. The nurse should initiate the conversation and include the topic of sexual activity when discussing other physical activities. Explain what is safe and when. The joint guidelines of the American College of Cardiology and the American Heart Association recommend that after an “uncomplicated MI” (i.e., the patient's condition was stable with no complications), sexual intercourse can be resumed in a week to 10 days. However, many patients tend to resume sexual activity more gradually than this. A “complicated MI” means that the patient required CPR or had hypotension, serious dysrhythmia, or heart failure while hospitalized. Patients with complicated MIs should resume sexual activity more slowly, depending on their tolerance for exercise and activity. Encourage patients to talk to their health care providers about resuming sexual activity; the type and extent of damage from the MI might influence recommendations.
• Explain the importance of taking prescribed medications such as beta blockers. Patients who take beta-adrenergic blockers for 1 year after an MI have a reduced chance of reinfarction and increased survival. The patient should also continue to take lipid-lowering agents such as simvastatin (Zocor), atorvastatin (Lipitor), lovastatin (Mevacor), pravastatin (Pravachol), or rosuvastatin (Crestor).
Prognosis
Medical care must be instituted without delay. Many patients with an MI who are not treated before reaching the hospital die. The prognosis also depends on the area and extent of the damage and the presence or absence of complications.
Heart Failure
Etiology and Pathophysiology
When the heart cannot pump enough blood to sustain the body's metabolic needs, it is called heart failure or cardiac insufficiency. Heart failure (HF) is traditionally defined as circulatory congestion caused by the heart's inability to pump effectively. Many patients also have pulmonary or systemic congestion with HF, and the syndrome was commonly called congestive heart failure (CHF). However, this term excludes patients who do not have congestion. HF is currently understood to be a neurohormonal problem that progresses because of the chronic release of substances such as catecholamines (epinephrine and norepinephrine). Epinephrine and norepinephrine are hormones of the sympathetic nervous system and they can produce harmful effects on the failing heart and circulatory system.
Circulatory congestion and compensatory mechanisms may occur. HF may develop after an MI, in response to prolonged hypertension or diabetes mellitus, or in relation to valvular or inflammatory heart disease. Other factors associated with HF include infection, stress, hyperthyroidism, anemia, and fluid replacement therapy. HF is the most common diagnosis for the hospitalized patient over 65 years of age. It affects about 5 million Americans and accounts for 200,000 deaths annually. The increasing prevalence and incidence of HF result from people (1) living longer and (2) being more likely to survive cardiovascular disease.
Because the left ventricle is most often affected by coronary atherosclerosis and hypertension, HF usually begins there. If untreated, the condition progresses to right-sided failure. Right ventricular failure can occur separately from left ventricular failure, but its appearance is usually a consequence of left-sided failure. The signs and symptoms of HF result from decreased cardiac output, because of impaired cardiac pumping power, and congestion that involves the pulmonary and/or venous systems (Box 8-3).
Left ventricular failure.
When the left ventricle is unable to pump enough blood to meet the body's demands, major consequences occur. The first consequences are the signs and symptoms of decreased cardiac output. The second is pulmonary congestion. Increased pressure in the left side of the heart backs up into the pulmonary system, and the lungs become congested with fluid. Fluid leaks through the engorged capillaries and permeates air spaces in the lungs. If during each heartbeat the right ventricle pumps out just one more drop of blood than the left, then within only 3 hours the pulmonary blood volume will have expanded by 500 mL. Pulmonary edema and pleural effusion occur. Signs and symptoms of this condition include dyspnea; orthopnea; pulmonary crackles; wheezing; pink, frothy sputum; and cough.
Right ventricular failure.
Right ventricular failure occurs when the right ventricle is unable to pump effectively against increased pressure in the pulmonary circulation. The increased pressure is usually caused by blood backing up from a failing left ventricle, but right ventricular failure can also result from chronic pulmonary disease (cor pulmonale) and pulmonary hypertension. The right ventricle's inability to pump blood forward into the lungs results in peripheral congestion and an inability to accommodate all the venous blood that is normally returned to the right side of the heart. Venous blood is forced backward into the systemic circulation. Increased venous volume and pressure force fluid out of the vasculature into interstitial tissue (peripheral edema). Edema appears in dependent areas of the body such as the sacrum when the patient is supine and the feet and ankles while in an upright position. As right ventricular failure continues, edema may progress to pitting edema and move up the legs into the thighs, external genitalia, and lower trunk. To check for edema, press down on the tissue for several seconds and lift the finger. If the depression does not fill almost immediately, pitting edema is present (Figure 8-16 and Table 8-5).
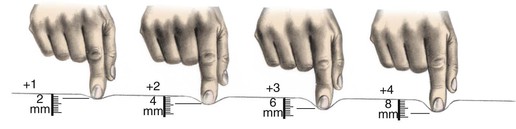
Table 8-5
Pitting Edema Scale
| SCALE | DEGREE | RESPONSE |
| +1: Trace | 2 mm (0- inch) inch) | Rapid |
| +2: Mild | 4 mm (0- inch) inch) | 10-15 sec |
| +3: Moderate | 6 mm ( - - inch) inch) | 1-2 min |
| +4: Severe | 8 mm ( -1 inch) -1 inch) | 2-5 min |
One liter of fluid equals 1 kg (2.2 lb); therefore a weight gain of 2.2 lb signifies a gain of 1 L of body fluid. The liver may become congested, and fluid can accumulate in the abdomen (ascites). Distended neck veins may be observed when the patient is sitting.
Clinical Manifestations
Manifestations of HF are those associated with decreased cardiac output, left ventricular failure, and right ventricular failure (Box 8-4).
Assessment
Subjective data include complaints of dyspnea, orthopnea (an abnormal condition in which a person must sit or stand to breathe deeply or comfortably), paroxysmal nocturnal dyspnea (sudden awakening from sleep because of shortness of breath), and cough. The patient may report fatigue, anxiety, weight gain from fluid retention, and edema. Physical symptoms and impaired physical function cause psychosocial stress. Patients with New York Heart Association (NYHA) class III or IV HF are at high risk for major depression (American Heart Association, 2012c). Document any pain (anginal or abdominal) and the patient's stated ability to perform ADLs.
Collection of objective data includes noting the presence of respiratory distress, the number of pillows required to breath comfortably while attempting to rest (orthopnea), edema (site, degree of pitting), abdominal distention secondary to ascites, weight gain, adventitious breath sounds, abnormal heart sounds (gallop and murmurs), activity intolerance, and jugular vein distention. Blood flow to the kidneys is diminished, resulting in reduction in the glomerular filtration rate, and ultimately oliguria. Oxygen deficit in tissues results in cyanosis and general debilitation.
Diagnostic Tests
Diagnosis is based on presenting signs and symptoms of HF and is confirmed by various diagnostic tests. A chest radiograph reveals pulmonary vascular congestion, pleural effusion, and cardiomegaly (cardiac enlargement). ECG shows cardiac dysrhythmias. The most noninvasive diagnostic test for evaluating a patient with HF is an echocardiogram. Echocardiography is done to assess the valves and chambers of the heart. It can be used to identify valvular heart disease and detect the presence of pericardial fluid. Pulmonary artery catheterization is done to assess right and left ventricular function.
Exercise stress testing is performed to determine activity tolerance and the severity of underlying ischemic cardiovascular disease. Cardiac catheterization may be done to detect cardiac abnormalities and underlying cardiovascular disease. MUGA scanning is used to evaluate cardiac function, ejection fraction, and wall motion abnormalities.
Laboratory studies include electrolytes, sodium, calcium, magnesium, and potassium levels. Blood chemistry will reveal elevated blood urea nitrogen (BUN) and creatinine resulting from decreased glomerular filtration; liver function values (alanine aminotransferase, aspartate transaminase, gamma-glutamyltransferase, alkaline phosphatase) will be mildly elevated. B-type natriuretic peptide (BNP) is a hormone secreted by the heart in response to ventricular expansion and pressure overload. A higher level of BNP correlates with an increase in the patient's signs and symptoms of HF:
• Less than 100 pg/mL (normal): The patient does not have HF
• Greater than 100 pg/mL: Suggestive of HF
• Greater than 700 pg/mL: Indicates decompensated HF (i.e., HF that is worsening)
Arterial blood gases may show hypoxemia and acid-base imbalance.
Medical Management
Medical management of HF includes increasing cardiac efficiency with digoxin and vasodilators (nitroglycerin, isosorbide) for expanded output. Digoxin was once the cornerstone of HF treatment, but is now used less often and at lower doses. Angiotensin-converting enzyme (ACE) inhibitors such as captopril (Capoten), enalapril (Vasotec), ramipril (Altace), benazepril (Lotensin), lisinopril (Prinivil, Zestril), quinapril (Accupril), and fosinopril (Monopril) decrease peripheral vascular resistance, and improve cardiac output. These drugs extend the lives of patients with HF and lengthen the time between hospital admissions (American Heart Association, 2012c). Remodeling occurs when the left ventricle dilates, hypertrophies, and develops a more spherical shape. The shape change puts extra stress on the ventricle walls, increases the amount of blood regurgitated through the mitral valve, and decreases the ventricle's ability to work. Two beta blockers approved by the FDA to treat HF are carvedilol (an alpha blocker and nonselective beta blocker) and metoprolol. Beta blockers inhibit chronic activation of the sympathetic nervous system. Beta blockers are so effective at reducing symptoms, improving clinical status, and decreasing mortality and hospitalizations, that they have become the most significant drugs for HF management. Angiotensin II receptor blockers such as irbesartan (Avapro), losartan (Cozaar), and valsartan (Diovan) selectively and competitively block the vasoconstrictive and aldosterone-secreting effects of angiotensin, leading to vasodilation. Research for their use in HF continues. Angiotensin II receptor blockers are not a substitute for ACE inhibitors unless an ACE inhibitor is clearly not tolerated. Nesiritide (Natrecor) is used intravenously in patients with acutely decompensated HF who have shortness of breath (i.e., dyspnea) at rest or with minimal activity. Nesiritide is the first of the drug class called human BNPs. It reduces pulmonary capillary pressure, helps improve breathing, and causes vasodilation with increase in stroke volume and cardiac output (American Heart Association, 2012c).
Therapeutic management also includes lowering the oxygen requirements of body systems. This is done by elevating the head of the bed to 45 degrees or by having the patient sit on the edge of the bed with arms resting on the overbed table to reduce myocardial oxygen demand and decrease circulating volume returning to the heart. Oxygen therapy provides oxygen to the tissues if the patient is hypoxic.
Edema and pulmonary congestion are treated with diuretics, a sodium-restricted diet, and restricted fluid intake. Weigh the patient daily to monitor fluid retention.
The health care provider commonly initiates medication therapy with digoxin, ACE inhibitors, thiazide, and loop diuretics (Table 8-6). Once the workload of the heart is decreased and the tissue and organ engorgement has abated, the patient's activity level will increase.
Table 8-6
Medications for Heart Failure
| GENERIC NAME (TRADE NAME) | ACTION | NURSING INTERVENTIONS |
| Cardiac Glycosides | ||
| Digitalis preparations, such as digoxin (Lanoxin) | Strengthen cardiac force and efficiency Slow heart rate Increase circulation, effecting diuresis | Monitor apical pulse to ensure rate greater than 60 bpm; monitor for toxicity (nausea, vomiting, anorexia, dysrhythmia, bradycardia, tachycardia, headache, fatigue, and blurred or colored vision) |
| Diuretics | ||
| Thiazides, such as chlorothiazide (Diuril), hydrochlorothiazide (Esidrix, Hydrodiuril) | Increase renal secretion of sodium Are safe for long-term use Block sodium and water reabsorption in kidney tubules | Monitor electrolyte depletion; weigh daily to ascertain fluid loss |
| Sulfonamides (loop diuretic), such as furosemide (Lasix), bumetanide (Bumex) | Act rapidly for less responsive edema | Administer in the morning to prevent nocturia Monitor for electrolyte depletion Consider sulfa allergy (furosemide) |
| Aldosterone antagonist (potassium-sparing), such as spironolactone (Aldactone) | Relieves edema and ascites that do not respond to usual diuretics Blocks sodium-retaining and potassium-excreting properties of aldosterone | Monitor for gastrointestinal irritation and hyperkalemia |
| Potassium Supplements | ||
| potassium (K-Lyte) | Restores electrolyte loss | Monitor blood potassium levels |
| Sedatives and Analgesics | ||
| temazepam (Restoril) | Promotes rest and comfort | Monitor rest and sleep benefits |
| morphine | Relieves chest and abdominal pain, reduces anxiety, and decreases myocardial oxygen demands Lessens dyspnea | |
| Nitrates | ||
| nitroglycerin (Cardabid) | Dilates arteries, improves blood flow Reduces blood pressure | Monitor blood pressure for hypotension Monitor for headache and flushing |
| Angiotensin-Converting Enzyme (ACE) Inhibitors | ||
| captopril (Capoten) enalapril (Vasotec) ramipril (Altace) benazepril (Lotensin) lisinopril (Prinivil; Zestril) quinapril (Accupril) fosinopril (Monopril) moexipril (Univasc) perindopril (Aceon) trandolapril (Mavik) | Act as antihypertensives, reduce peripheral arterial resistance, and improve cardiac output | Observe patient closely for a precipitous drop in blood pressure within 3 hr of initial dose; monitor blood pressure closely Monitor blood potassium levels |
| Beta-Adrenergic Blockers | ||
| carvedilol (Coreg) | Directly blocks the sympathetic nervous system's negative effects on the failing heart | Start at a low dose, increasing the dose slowly every 2 wk as tolerated by the patient Monitor blood pressure and notify health care provider of significant change Monitor pulse: If <50 bpm, withhold drug and call health care provider |
| metoprolol (Toprol-XL) | Blocks beta2-adrenergic receptors in bronchial and vascular smooth muscle. Lowers blood pressure by beta-blocking effects; reduces elevated renin plasma levels | Monitor I&O, weigh daily Monitor apical or radial pulse before administration Notify health care provider of any significant changes, or if pulse <50 bpm |
| Inotropic Agents | ||
| dobutamine (Dobutrex IV) dopamine (Intropin IV) | Low-dose dobutamine and low-dose dopamine are relatively safe on medical-surgical units; at low doses they dilate renal blood vessels, stimulating renal blood flow and glomerular filtration rate; this in turn promotes sodium excretion, often helping patients with CHF improve | Make certain patient is not taking monoamine oxidase (MAO) inhibitors, tricyclic antidepressants, phenytoin (Dilantin), or haloperidol (Haldol). Record accurate I&O; assess for dizziness, nausea, vomiting, headache. Assess vital signs carefully every 15 min for first 2 hr, then every 2 hr for the next 4 hr, and finally once a shift. Observe carefully for extravasation, tachycardia, bradycardia, angina, palpitations, hypotension, hypertension, azotemia, and anxiety |
| Human B-Type Natriuretic Peptides | ||
| nesiritide (Natrecor) | New class of synthetic HF drugs; causes arterial and venous dilation, thereby decreasing systemic vascular resistance and pulmonary arterial pressures; decreases blood pressure, promotes better left ventricle ejection, and increases cardiac output; may also promote diuresis; an IV treatment for patients with acutely decompensated CHF | Observe carefully for hypotension. Natrecor should not be used for patients with cardiogenic shock or with a systolic blood pressure <90 mm Hg |
ACE, Angiotensin-converting enzyme; bpm, beats per minute; CHF, congestive heart failure; HF, heart failure; I&O, intake and output.
A biventricular pacemaker can improve symptoms and function, improve quality of life, and decrease hospitalization for patients with HF who also have conduction system disorder. An implantable cardioverter-defibrillator can decrease the risk of sudden cardiac death for patients with a family history of sudden cardiac death, life-threatening dysrhythmias, or mild to moderate HF who have an ejection fraction of less than 30% (American Heart Association, 2013a) (see section on “Echocardiography“).
Oxygen administration and pharmacologic therapies are the primary concerns in the management of acute HF. Decreasing oxygen requirements through rest slows the heart rate and increases cardiac and respiratory reserves. Anxiety produced by the signs and symptoms and the fear of a life-threatening situation can be allayed by reassurance and explanation. Accurate interventions, observation, and reporting reduce the threat of complications such as embolus, thrombophlebitis, MI, and pulmonary edema.
Nursing Interventions
Nursing interventions include measures to prevent disease progression and complications. Monitor vital signs for changes. Note any signs of respiratory distress or pulmonary edema. Carefully monitor signs and symptoms of left-sided versus right-sided HF. Urinary output is typically low, and edema is soft and pitting; legs are elevated to decrease edema.
Also note an increase in abdominal girth and total body weight as indicators of fluid retention, which is common in HF. Auscultate the lung fields to detect the presence of crackles and wheezes; also note coughing and complaints of dyspnea. Restful sleep may be possible only in the sitting position or with the aid of extra pillows. Activity intolerance is accompanied by extreme fatigue and anxiety. Assess patients for depression. Explain to patients with HF and depression that the depression is readily treatable and that several approaches can be used separately or in combination, including pharmacologic therapy, psychosocial and psychotherapeutic interventions, and cardiac rehabilitation.
Key components of care.
The Institute for Healthcare Improvement recommends these components of care for all patients with HF (unless the patient cannot tolerate them or unless contraindicated):
• Assess left ventricular systolic function.
• At discharge from hospital (when left ventricular ejection fraction is less than 40%, indicating systolic dysfunction), administer ACE inhibitor or angiotensin.
• At discharge, administer an anticoagulant if the patient has chronic or recurrent atrial fibrillation.
• Encourage smoking cessation.
• Instruct the patient at discharge regarding activity, diet, medication, follow-up appointment, weight monitoring, and what to do if symptoms worsen.
• Provide influenza and pneumococcal immunization.
• At discharge, institute optional beta blocker therapy for stabilized patients with left ventricular systolic dysfunction who have no contraindications.
The new guidelines also recommend a discussion of end-of-life decisions with the patient and the family. Patients should talk with their health care providers about treatment preferences, advance directives, living wills, power of attorney for health care, and life support issues. HF is progressive and patients should make decisions concerning health care wishes and plans while they are capable of expressing choices. Hospice services, originally developed to assist patients with cancer, are appropriate for the patient with end-stage HF (Patient Teaching box, Nursing Care Plan 8-1 and Box 8-5).
Patient Teaching
Heart Failure
• Monitor for signs and symptoms of recurring heart failure and report them to the health care provider or clinic. The following signs and symptoms indicate worsening heart failure:
• Weight gain of 2 to 3 lb (1 to 1.5 kg) over a short period (about 2 days)
• Swelling of ankles, feet, or abdomen
• Frequent nighttime urination
• Avoid fatigue and plan activity to allow for rest periods.
• Plan and eat meals within prescribed sodium restrictions. Avoid salty foods.
• Avoid drugs with high sodium content (e.g., some laxatives and antacids, Alka-Seltzer); read the product labels. Ideally, limit sodium intake to 2 g/day.
• Maintain low-fat diet, with fat intake less than 30% of total calories.
• Eat several small meals rather than three large meals per day.
• Take medications as prescribed.
• If several medications are prescribed, develop a method to facilitate accurate administration.
• When taking digoxin, check own pulse rate daily; report a rate of less than 60 bpm to the health care provider. Do not take digoxin if pulse is less than 60 bpm.
• Take diuretics as prescribed.
• Weigh self daily at same time and in similar clothes.
• Eat foods high in potassium and low in sodium (such as oranges and bananas) if the patient is not taking a potassium-sparing diuretic.
• Take all prescribed medications.
• Report signs of hypotension (lightheadedness, rapid pulse, syncope) to the health care provider.
• Avoid alcohol when taking vasodilators.
• Reinforce the importance of regular exercise once heart failure is stabilized. A thorough treatment regimen may allow the patient to increase activity level over time. The health care provider may ultimately recommend 30 to 45 minutes of aerobic exercise three or four times a week to improve patient's well-being.
• Report to the health care provider for follow-up as directed.
 Nursing Care Plan 8-1
Nursing Care Plan 8-1
The Patient With Heart Failure
Mr. D. is a 61-year-old clinical administrator. He was admitted to the hospital with the diagnosis of heart failure. He has a history of hypertension and coronary artery disease. Six months ago he had a myocardial infarction. He has felt tired for the past 3 wk and has been experiencing increased dyspnea. He has noticed some edema in his ankles and is concerned about gaining 5 lb in the past week and having an increasing intolerance to exertion. The nursing admission history revealed:
• Mr. D. has not been taking his antihypertensive medication regularly. He did not like the side effects and stopped taking the medication, but he was too embarrassed to call his health care provider.
• Vital signs revealed an elevated blood pressure.
• He has shortness of breath during activities and when lying down.
Nursing Diagnosis
Decreased cardiac output, related to cardiac insufficiency

Nursing Diagnosis
Anxiety, related to change in health status, lifestyle changes, fear of death, or threats to self-concept