The Periodontal Pocket
The periodontal pocket, which is defined as a pathologically deepened gingival sulcus, is one of the most important clinical features of periodontal disease. All different types of periodontitis, as outlined in Chapter 4, share histopathologic features, such as tissue changes in the periodontal pocket, mechanisms of tissue destruction, and healing mechanisms. However, they differ with regard to their etiology, natural history, progression, and response to therapy.32
Classification
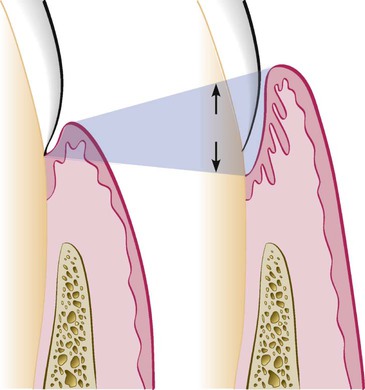
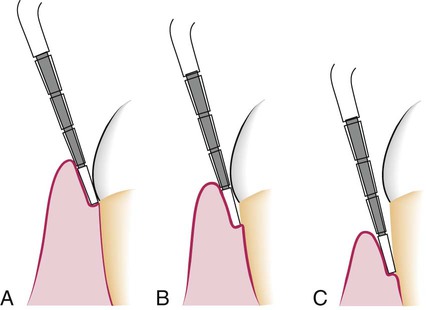
Deepening of the gingival sulcus may occur as a result of coronal movement of the gingival margin, apical displacement of the gingival attachment, or a combination of the two processes (Figure 20-1). Pockets can be classified as follows:
Gingival pocket is formed by gingival enlargement without destruction of the underlying periodontal tissues. The sulcus is deepened because of the increased bulk of the gingiva (Figure 20-2, A).
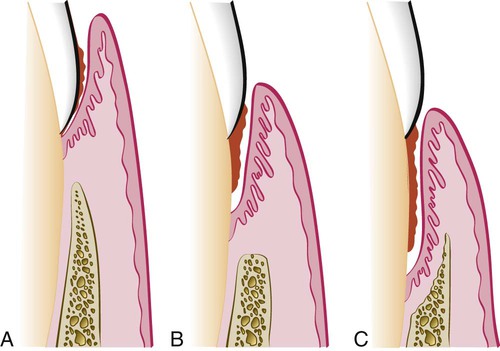
Periodontal pocket produces destruction of the supporting periodontal tissues, thereby leading to the loosening and exfoliation of the teeth. The remainder of this chapter refers to this type of pocket.
Two types of periodontal pockets exist, as follows:
Suprabony (supracrestal or supraalveolar) occurs when the bottom of the pocket is coronal to the underlying alveolar bone (Figure 20-2, B).
Intrabony (infrabony, subcrestal, or intraalveolar) occurs when the bottom of the pocket is apical to the level of the adjacent alveolar bone. With this second type, the lateral pocket wall lies between the tooth surface and the alveolar bone (Figure 20-2, C).
Pockets can involve one, two, or more tooth surfaces, and they can be of different depths and types on different surfaces of the same tooth and on approximal surfaces of the same interdental space.30,38 Pockets can also be spiral (i.e., originating on one tooth surface and twisting around the tooth to involve one or more additional surfaces) (Figure 20-3). These types of pockets are most common in furcation areas.
Clinical Features
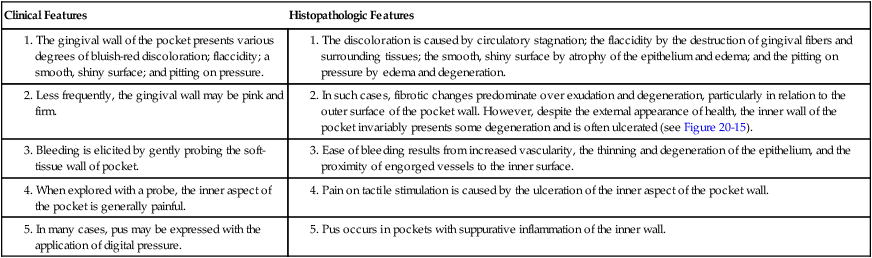
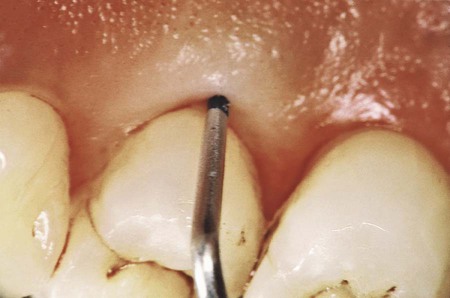
Clinical signs that suggest the presence of periodontal pockets include a bluish-red thickened marginal gingiva; a bluish-red vertical zone from the gingival margin to the alveolar mucosa; gingival bleeding and suppuration; tooth mobility; diastema formation; and symptoms such as localized pain or pain “deep in the bone.” The only reliable method of locating periodontal pockets and determining their extent is careful probing of the gingival margin along each tooth surface (Figure 20-4 and Table 20-1). On the basis of depth alone, however, it is sometimes difficult to differentiate between a deep normal sulcus and a shallow periodontal pocket. In such borderline cases, pathologic changes in the gingiva distinguish the two conditions.
TABLE 20-1
Correlation of Clinical and Histopathologic Features of the Periodontal Pocket
| Clinical Features | Histopathologic Features |
|
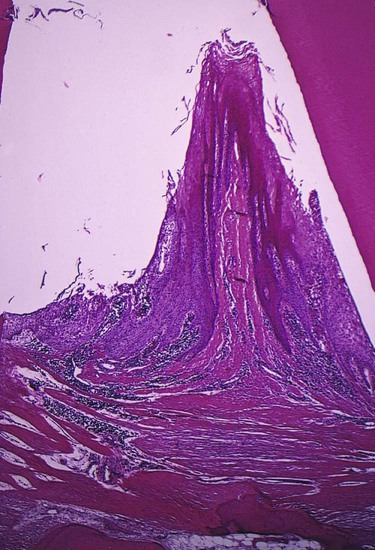
2. In such cases, fibrotic changes predominate over exudation and degeneration, particularly in relation to the outer surface of the pocket wall. However, despite the external appearance of health, the inner wall of the pocket invariably presents some degeneration and is often ulcerated (see Figure 20-15). |
|
For a more detailed discussion of the clinical aspects of periodontal pockets, see Chapter 30.
Pathogenesis
The initial lesion in the development of periodontitis is the inflammation of the gingiva in response to a bacterial challenge. Changes involved in the transition from the normal gingival sulcus to the pathologic periodontal pocket are associated with different proportions of bacterial cells in dental plaque. Healthy gingiva is associated with few microorganisms, mostly coccoid cells and straight rods. Diseased gingiva is associated with increased numbers of spirochetes and motile rods.40,41,43 However, the microbiota of diseased sites cannot be used as a predictor of future attachment or bone loss, because their presence alone is not sufficient for disease to start or progress.35
Pocket formation starts as an inflammatory change in the connective tissue wall of the gingival sulcus. The cellular and fluid inflammatory exudate causes degeneration of the surrounding connective tissue, including the gingival fibers. Just apical to the junctional epithelium, collagen fibers are destroyed,20,61 and the area is occupied by inflammatory cells and edema (Figure 20-5).
Early concepts assumed that, after the initial bacterial attack, periodontal tissue destruction continued to be linked to bacterial action. More recently, it was established that the host's immunoinflammatory response to the initial and persistent bacterial attack unleashes mechanisms that lead to collagen and bone destruction. These mechanisms are related to various cytokines, some of which are produced normally by cells in noninflamed tissue and others by cells that are involved in the inflammatory process, such as polymorphonuclear leukocytes (PMNs), monocytes, and other cells, thereby leading to collagen and bone destruction. This chapter describes the histologic aspects of gingival inflammation and tissue destruction. For further information about the molecular biology aspects of these mechanisms of tissue destruction, please see Chapter 25 and www.expertconsult.com.
The two mechanisms associated with collagen loss are as follows: (1) collagenases and other enzymes secreted by various cells in healthy and inflamed tissue, such as fibroblasts,74 PMNs,73 and macrophages,53 become extracellular and destroy collagen (these enzymes that degrade collagen and other matrix macromolecules into small peptides are called matrix metalloproteinases75); and (2) fibroblasts phagocytize collagen fibers by extending cytoplasmic processes to the ligament–cementum interface and degrading the inserted collagen fibrils and the fibrils of the cementum matrix.20,21
As a consequence of the loss of collagen, the apical cells of the junctional epithelium proliferate along the root and extend fingerlike projections that are two or three cells in thickness (Figure 20-6).

As a result of inflammation, PMNs invade the coronal end of the junctional epithelium in increasing numbers (Figure 20-7). The PMNs are not joined to one another or to the epithelial cells by desmosomes. When the relative volume of PMNs reaches approximately 60% or more of the junctional epithelium, the tissue loses cohesiveness and detaches from the tooth surface. Thus, the coronal portion of the junctional epithelium detaches from the root as the apical portion migrates, thereby resulting in its apical shift; the oral sulcular epithelium gradually occupies an increasing portion of the sulcus (then a pocket) lining.62

Extension of the junctional epithelium along the root requires the presence of healthy epithelial cells. Marked degeneration or necrosis of the junctional epithelium impairs rather than accelerates pocket formation. (This occurs in necrotizing ulcerative gingivitis, which results in an ulcer rather than pocket formation.)
Degenerative changes seen in the junctional epithelium at the base of periodontal pockets are usually less severe than those in the epithelium of the lateral pocket wall (see Figure 20-7). Because the migration of the junctional epithelium requires healthy, viable cells, it is reasonable to assume that the degenerative changes seen in this area occur after the junctional epithelium reaches its position on the cementum.
The transformation of a gingival sulcus into a periodontal pocket creates an area in which plaque removal becomes impossible, and a feedback mechanism is established. The rationale for pocket reduction is based on the need to eliminate areas of plaque accumulation.
Histopathology
Changes that occur during the initial stages of gingival inflammation are presented in Chapter 7. After the pocket is formed, several microscopic features are present, which will be discussed in this section.
Soft-Tissue Wall.
The connective tissue is edematous and densely infiltrated with plasma cells (approximately 80%), lymphocytes, and a scattering of PMNs.82 The blood vessels are increased in number, dilated, and engorged, particularly in the subepithelial connective tissue layer.10 The connective tissue exhibits varying degrees of degeneration. Single or multiple necrotic foci are occasionally present.52 In addition to exudative and degenerative changes, the connective tissue shows proliferation of the endothelial cells, with newly formed capillaries, fibroblasts, and collagen fibers (see Figure 20-5).
The junctional epithelium at the base of the pocket is usually much shorter than that of a normal sulcus. Although marked variations are found with regard to the length, width, and condition of the epithelial cells,63 usually the coronoapical length of the junctional epithelium is reduced to only 50 to 100 µm.14 The cells may be well formed and in good condition, or they may exhibit slight to marked degeneration (see Figures 20-6 and 20-9).
The most severe degenerative changes in the periodontal pocket occur along the lateral wall (see Figure 20-7). The epithelium of the lateral wall of the pocket presents striking proliferative and degenerative changes. Epithelial buds or interlacing cords of epithelial cells project from the lateral wall into the adjacent inflamed connective tissue, and they may extend farther apically than the junctional epithelium (Figures 20-8, A, and 20-9). These epithelial projections, as well as the remainder of the lateral epithelium, are densely infiltrated by leukocytes and edema from the inflamed connective tissue. The cells undergo vacuolar degeneration and rupture to form vesicles. Progressive degeneration and necrosis of the epithelium lead to ulceration of the lateral wall, exposure of the underlying inflamed connective tissue, and suppuration. In some cases, acute inflammation is superimposed on the underlying chronic changes.


A comparative study of gingival changes in aggressive and chronic periodontitis revealed more pronounced degenerative changes in the epithelium of aggressive cases with more open intercellular spaces, including microclefts and necrotic areas.35
The severity of the degenerative changes is not necessarily related to pocket depth. Ulceration of the lateral wall may occur in shallow pockets, and deep pockets are occasionally observed in which the lateral epithelium is relatively intact or shows only slight degeneration.
The epithelium at the gingival crest of a periodontal pocket is generally intact and thickened, with prominent rete pegs.
For a detailed electron microscopic study of the pocket epithelium in experimentally induced pockets in dogs, see the article by Müller-Glauser and Schröder.49
Bacterial Invasion
Bacterial invasion of the apical and lateral areas of the pocket wall has been described in human chronic periodontitis. Filaments, rods, and coccoid organisms with predominant gram-negative cell walls have been found in intercellular spaces of the epithelium.25,26 Hillmann and colleagues35 have reported the presence of Porphyromonas gingivalis and Prevotella intermedia in the gingiva of aggressive periodontitis cases. Actinobacillus actinomycetemcomitans has also been found in the tissues.16,47,58
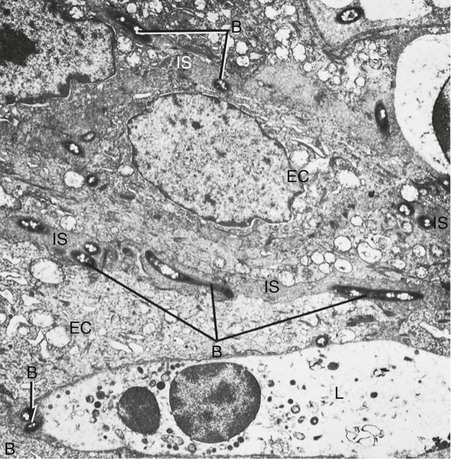
Bacteria may invade the intercellular space under exfoliating epithelial cells, but they are also found between deeper epithelial cells as well as accumulating on the basement lamina. Some bacteria traverse the basement lamina and invade the subepithelial connective tissue60 (Figures 20-10 and 20-11).
The presence of bacteria in the gingival tissues has been interpreted by different investigators as bacterial invasion or as the “passive translocation” of plaque bacteria.42 This important point has significant clinicopathologic implications and has not yet been clarified.17,39,43
Mechanisms of Tissue Destruction
The inflammatory response triggered by bacterial plaque unleashes a complex cascade of events aimed at destroying and removing bacteria, necrotic cells, and deleterious agents. However, this process is nonspecific; in an attempt to restore health, the host's cells (e.g., neutrophils, macrophages, fibroblasts, epithelial cells) produce proteinases, cytokines, and prostaglandins that can damage or destroy the tissues.
Chapter 25 describes in detail these aspects of inflammation and the mechanisms of tissue destruction at the molecular level.
Microtopography of the Gingival Wall
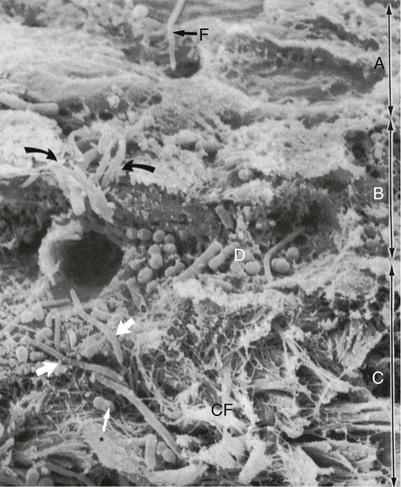
Scanning electron microscopy has permitted the description of several areas in the soft-tissue (gingival) wall of the periodontal pocket in which different types of activity take place.59 These areas are irregularly oval or elongated and adjacent to one another, and they measure about 50 to 200 µm. These findings suggest that the pocket wall is constantly changing as a result of the interaction between the host and the bacteria. The following areas have been noted:
1. Areas of relative quiescence, showing a relatively flat surface with minor depressions and mounds and occasional shedding of cells (Figure 20-12, area A).
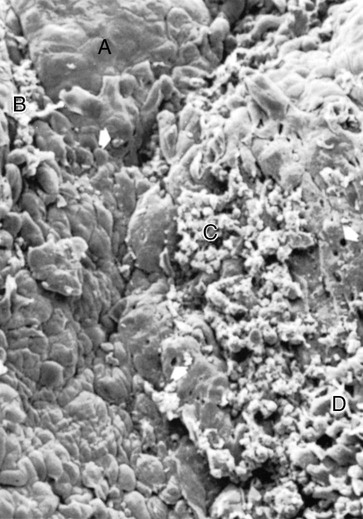
2. Areas of bacterial accumulation, which appear as depressions on the epithelial surface, with abundant debris and bacterial clumps penetrating into the enlarged intercellular spaces. These bacteria are mainly cocci, rods, and filaments, with a few spirochetes (Figure 20-12, area B).
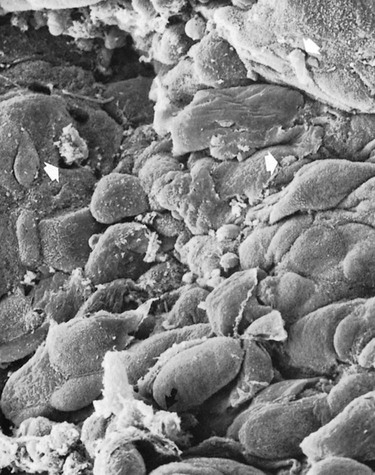
3. Areas of emergence of leukocytes, in which leukocytes appear in the pocket wall through holes located in the intercellular spaces (Figure 20-13).
4. Areas of leukocyte–bacteria interaction, in which numerous leukocytes are present and covered with bacteria in an apparent process of phagocytosis. Bacterial plaque associated with the epithelium is seen either as an organized matrix covered by a fibrinlike material in contact with the surface of cells or as bacteria penetrating into the intercellular spaces (Figure 20-12, area C).
5. Areas of intense epithelial desquamation, which consist of semiattached and folded epithelial squames, which are sometimes partially covered with bacteria (Figure 20-12, area D).
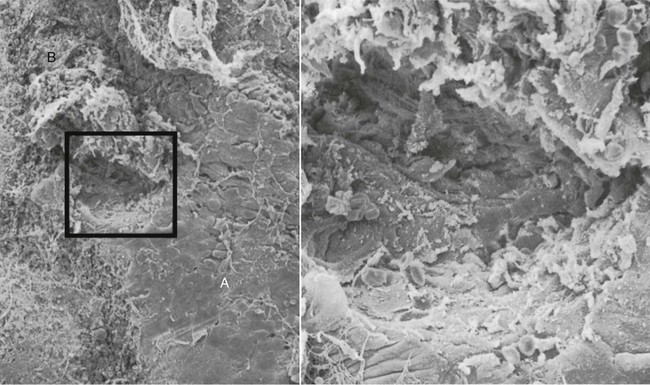
6. Areas of ulceration, with exposed connective tissue (Figure 20-14).
The transition from one area to another could result from bacteria accumulating in previously quiescent areas and triggering the emergence of leukocytes and the leukocyte–bacteria interaction. This would lead to intense epithelial desquamation and finally to ulceration and hemorrhage.
Periodontal Pockets as Healing Lesions
Periodontal pockets are chronic inflammatory lesions and thus are constantly undergoing repair. Complete healing does not occur because of the persistence of the bacterial attack, which continues to stimulate an inflammatory response, thereby causing degeneration of the new tissue elements formed during the continuous effort at repair.
The condition of the soft-tissue wall of the periodontal pocket results from the interplay of the destructive and constructive tissue changes. Their balance determines clinical features such as color, consistency, and surface texture of the pocket wall. If the inflammatory fluid and cellular exudate predominate, the pocket wall is bluish-red, soft, spongy, and friable, with a smooth, shiny surface; at the clinical level, this is generally referred to as an edematous pocket wall. If there is a relative predominance of newly formed connective tissue cells and fibers, the pocket wall is more firm and pink and clinically referred to as a fibrotic pocket wall (see Table 20-1 and Chapter 30).
Edematous and fibrotic pockets represent opposite extremes of the same pathologic process rather than different disease entities. They are subject to constant modification, depending on the relative predominance of exudative and constructive changes.
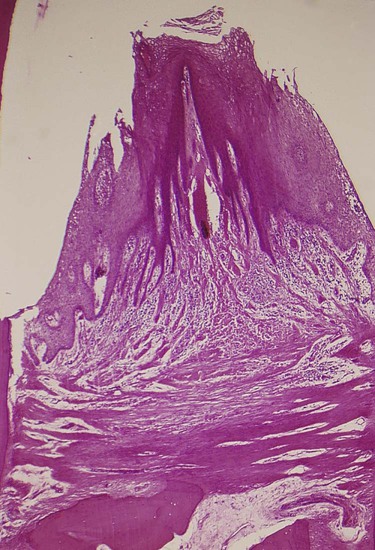
Fibrotic pocket walls may be misleading, because they do not necessarily reflect what is taking place throughout the pocket wall. The most severe degenerative changes in periodontal tissues occur adjacent to the tooth surface and the subgingival plaque. In some cases, inflammation and ulceration on the inside of the pocket are walled off by fibrous tissue on the outer aspect (Figure 20-15). Externally the pocket appears pink and fibrotic, despite the inflammatory changes occurring internally.

Pocket Contents
Periodontal pockets contain debris that consists principally of microorganisms and their products (enzymes, endotoxins, and other metabolic products), gingival fluid, food remnants, salivary mucin, desquamated epithelial cells, and leukocytes. Plaque-covered calculus usually projects from the tooth surface (Figure 20-16). Purulent exudate, if present in the patient, consists of living, degenerated, and necrotic leukocytes; living and dead bacteria; serum; and a scant amount of fibrin.46 The contents of periodontal pockets, when filtered free of organisms and debris, have been demonstrated to be toxic when injected subcutaneously into experimental animals.31
Pus is a common feature of periodontal disease, but it is only a secondary sign. The presence of pus or the ease with which it can be expressed from the pocket merely reflects the nature of the inflammatory changes in the pocket wall. It is not an indication of the depth of the pocket or the severity of the destruction of the supporting tissues. Extensive pus formation may occur in shallow pockets, whereas deep pockets may exhibit little or no pus. The localized accumulation of pus constitutes an abscess, which is discussed later in this chapter.
Root Surface Walls
The root surface wall of periodontal pockets often undergoes changes that are significant because they may perpetuate the periodontal infection, cause pain, and complicate periodontal treatment.11
Pathologic granules9 have been observed with light and electron microscopy,6,7 and they may represent areas of collagen degeneration or areas in which collagen fibrils have not been fully mineralized initially.
In addition, bacterial products (e.g., endotoxins3,5) have also been detected in the cementum wall of periodontal pockets. When root fragments from teeth with periodontal disease are placed in tissue culture, they induce irreversible morphologic changes in the cells of the culture. Such changes are not produced by normal roots.33 Diseased root fragments also prevent the in vitro attachment of human gingival fibroblasts, whereas normal root surfaces allow the cells to attach freely.4 When placed in the oral mucosa of the patient, diseased root fragments induce an inflammatory response, even if they have been autoclaved.44
These changes manifest clinically as softening of the cementum surface; this is usually asymptomatic, but it can be painful when a probe or explorer penetrates the area. They also constitute a possible reservoir for reinfection of the area after treatment. During the course of treatment, these necrotic areas are removed by root planing until a hard, smooth surface is reached. Cementum is very thin in the cervical areas, and scaling and root planing often remove it entirely, exposing the underlying dentin. Sensitivity to cold may result until secondary dentin is formed by the pulp tissue.
Decalcification and Remineralization of Cementum
Areas of increased mineralization65 are probably a result of an exchange of minerals and organic components at the cementum–saliva interface after exposure to the oral cavity. The mineral content of exposed cementum increases,64 and the minerals that are increased in diseased root surfaces include calcium,67 magnesium,50,67 phosphorus,50 and fluoride.50 Microhardness, however, remains unchanged.55,81 The development of a highly mineralized superficial layer may increase the tooth's resistance to decay.4
The hypermineralized zones are detectable by electron microscopy, and they are associated with increased perfection of the crystal structure and organic changes that are suggestive of a subsurface cuticle.64,65 These zones have also been seen in microradiographic studies66 as a layer that is generally 10 to 20 mm thick, with areas as thick as 50 mm. No decrease in mineralization was found in deeper areas, thereby indicating that increased mineralization does not come from adjacent areas. A loss of or reduction in the crossbanding of collagen near the cementum surface27,28 and a subsurface condensation of organic material of exogenous origin64 have also been reported.
Areas of demineralization are often related to root caries. Exposure to oral fluid and bacterial plaque results in proteolysis of the embedded remnants of Sharpey fibers; the cementum may be softened, and it may undergo fragmentation and cavitation.34 Unlike enamel caries, root surface caries tend to progress around rather than into the tooth.48 Active root caries lesions appear as well-defined yellowish or light-brown areas; they are frequently covered by plaque, and they have a softened or leathery consistency on probing. Inactive lesions are well-defined darker lesions with a smooth surface and a harder consistency on probing.24
The dominant microorganism in root surface caries is Actinomyces viscosus,72 although its specific role in the development of the lesion has not been established.24 Other bacteria, such as Actinomyces naeslundii, Streptococcus mutans, Streptococcus salivarius, Streptococcus sanguinis, and Bacillus cereus, have been found to produce root caries in animal models. Quirynen and colleagues54 reported that, when plaque levels and pocket depths decrease after periodontal therapy (both nonsurgical and surgical), a shift in oral bacteria occurs, thereby leading to a reduction in periodontal pathogens, an increase in S. mutans, and the development of root caries.
A prevalence rate study of root caries among 20- to 64-year-old individuals revealed that 42% had one or more root caries lesions and that these lesions tended to increase with age.37
The tooth may not be painful, but exploration of the root surface reveals the presence of a defect, and penetration of the involved area with a probe causes pain. Caries of the root may lead to pulpitis, sensitivity to sweets and thermal changes, or severe pain. Pathologic exposure of the pulp occurs in severe cases. Root caries may be the cause of toothache in patients with periodontal disease and no evidence of coronal decay.
Caries of the cementum requires special attention when the pocket is treated. The necrotic cementum must be removed by scaling and root planing until firm tooth surface is reached, even if this entails extension into the dentin.
Areas of cellular resorption of cementum and dentin are common in roots that are unexposed by periodontal disease.68 These areas are of no particular significance because they are symptom free, and, as long as the root is covered by the periodontal ligament, they are likely to undergo repair. However, if the root is exposed by progressive pocket formation before repair occurs, these areas appear as isolated cavitations that penetrate into the dentin. These areas can be differentiated from caries of the cementum by their clear-cut outline and hard surface. They may be sources of considerable pain that require the placement of a restoration.
Surface Morphology of Tooth Wall.78
The following zones can be found in the bottom of a periodontal pocket (Figure 20-17):

1. Cementum covered by calculus, in which all of the changes described in the preceding paragraphs can be found.
2. Attached plaque, which covers calculus and which extends apically from it to a variable degree (typically 100 to 500 µm).
3. The zone of unattached plaque that surrounds attached plaque and extends apically to it.
4. The zone of attachment of the junctional epithelium to the tooth. The extension of this zone, which in normal sulci is more than 500 µm, is usually reduced in periodontal pockets to less than 100 µm.
5. A zone of semidestroyed connective tissue fibers may be apical to the junctional epithelium60 (see the Pathogenesis section earlier in this chapter).
Zones 3, 4, and 5 make up the “plaque-free zone” seen in extracted teeth.8,12,36,57,78 The total width of the plaque-free zone varies according to the type of tooth (i.e., it is wider in the molars than in the incisors) and the depth of the pocket (i.e., it is narrower in deeper pockets).56 It is important to remember that the term plaque-free zone refers only to attached plaque, because unattached plaque contains a variety of gram-positive and gram-negative morphotypes, including cocci, rods, filaments, fusiforms, and spirochetes. The most apical zone contains predominantly gram-negative rods and cocci.76
Periodontal Disease Activity
For many years the loss of attachment produced by periodontal disease was thought to be a slow but continuously progressive phenomenon. More recently, as a result of studies of the specificity of plaque bacteria, the concept of periodontal disease activity has evolved.
According to this concept, periodontal pockets go through periods of exacerbation and quiescence as a result of episodic bursts of activity followed by periods of remission. Periods of quiescence are characterized by a reduced inflammatory response and little or no loss of bone and connective tissue attachment. A buildup of unattached plaque, with its gram-negative, motile, and anaerobic bacteria (see Chapter 23), starts a period of exacerbation during which bone and connective tissue attachment are lost and the pocket deepens. This period may last for days, weeks, or months, and it is eventually followed by a period of remission or quiescence during which gram-positive bacteria proliferate and a more stable condition is established. On the basis of a study of radioiodine125I absorptiometry, McHenry and colleagues45 confirmed that bone loss in patients with untreated periodontal disease occurs in an episodic manner.
These periods of quiescence and exacerbation are also known as periods of inactivity and periods of activity. Clinically, active periods show bleeding, either spontaneously or with probing, and greater amounts of gingival exudate. Histologically, the pocket epithelium appears thin and ulcerated, and an infiltrate composed predominantly of plasma cells,19 PMNs,53 or both is seen. Bacterial samples from the pocket lumen that are analyzed with dark-field microscopy show high proportions of motile organisms and spirochetes.43
Methods to detect periods of activity or inactivity are currently being investigated (see www.expertconsult.com).
Site Specificity
Periodontal destruction does not occur in all parts of the mouth at the same time; rather, it occurs on a few teeth at a time or even only on some aspects of some teeth at any given time. This is referred to as the site specificity of periodontal disease. Sites of periodontal destruction are often found next to sites with little or no destruction. Therefore, the severity of periodontitis increases with the development of new disease sites and with the increased breakdown of existing sites.
Pulp Changes Associated With Periodontal Pockets
The spread of infection from periodontal pockets may cause pathologic changes in the pulp. Such changes may give rise to painful symptoms, or they may adversely affect the response of the pulp to restorative procedures. Involvement of the pulp in periodontal disease occurs through either the apical foramen or the lateral pulp canals after pocket infection reaches them. Atrophic and inflammatory pulpal changes occur in such cases (see Chapters 52 and 63).
Relationship of Attachment Loss and Bone Loss to Pocket Depth
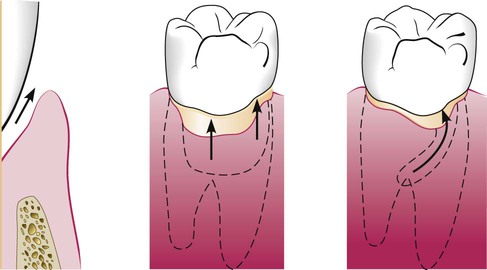
The severity of the attachment loss in pocket formation is generally but not always correlated with the depth of the pocket. This is because the degree of attachment loss depends on the location of the base of the pocket on the root surface, whereas pocket depth is the distance between the base of the pocket and the crest of the gingival margin. Pockets of the same depth may be associated with different degrees of attachment loss (Figure 20-18), and pockets of different depths may be associated with the same amount of attachment loss (Figure 20-19).
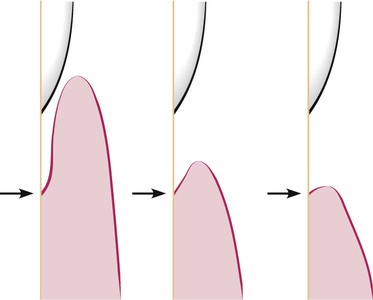
The severity of bone loss is generally but not always correlated with pocket depth. Extensive attachment and bone loss may be associated with shallow pockets if the attachment loss is accompanied by recession of the gingival margin, and slight bone loss can occur with deep pockets.
Area Between Base of Pocket and Alveolar Bone
Normally, the distance between the apical end of the junctional epithelium and the alveolar bone is relatively constant. The distance between the apical extent of calculus and the alveolar crest in human periodontal pockets is most constant, having a mean length of 1.97 mm (±33.16%).71,77
The distance from attached plaque to bone is never less than 0.5 mm and never more than 2.7 mm.78-80 These findings suggest that the bone-resorbing activity induced by the bacteria is exerted within these distances. However, the finding of isolated bacteria or clumps of bacteria in the connective tissue60 and on the bone surface26 may modify these considerations.
Relationship of Pocket to Bone
In infrabony pockets, the base of the pocket is apical to the crest of the alveolar bone, and the pocket wall lies between the tooth and the bone. The bone loss is in most cases vertical. Alternatively, in suprabony pockets, the base is coronal to the crest of the alveolar bone, and the pocket wall lies coronal to the bone. The type of bone loss is always horizontal.
This creates some microscopic differences that have some therapeutic importance. They are the relationship of the soft-tissue wall of the pocket to the alveolar bone, the pattern of bone destruction, and the direction of the transseptal fibers of the periodontal ligament15 (Figures 20-20, 20-21, and 20-22).
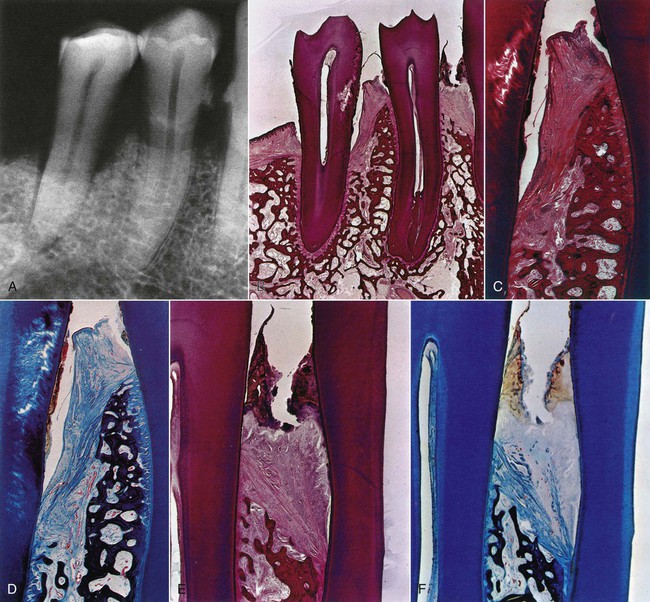

In suprabony pockets, the alveolar crest gradually attains a more apical position in relation to the tooth, but it retains its general morphology and architecture. The interdental fibers that run over the bone from one tooth to the other maintain their usual horizontal direction. In infrabony pockets, the morphology of the alveolar crest changes completely, with the formation of an angular bony defect. The interdental fibers in this case run over the bone in an oblique direction between the two teeth of the interdental space.15,80 This may affect the function of the area and also necessitate a modification in treatment techniques (see Chapters 60 and 62).13,15 Table 20-2 summarizes the distinguishing features of suprabony and infrabony pockets. The classification of infrabony pockets is discussed in Chapter 14.
TABLE 20-2
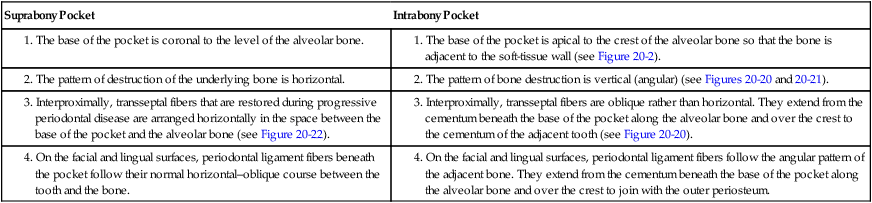
Distinguishing Features of Suprabony and Intrabony Periodontal Pockets
| Suprabony Pocket | Intrabony Pocket |
|
1. The base of the pocket is apical to the crest of the alveolar bone so that the bone is adjacent to the soft-tissue wall (see Figure 20-2). |
|
|
2. The pattern of bone destruction is vertical (angular) (see Figures 20-20 and 20-21). |
|
|
3. Interproximally, transseptal fibers that are restored during progressive periodontal disease are arranged horizontally in the space between the base of the pocket and the alveolar bone (see Figure 20-22). |
3. Interproximally, transseptal fibers are oblique rather than horizontal. They extend from the cementum beneath the base of the pocket along the alveolar bone and over the crest to the cementum of the adjacent tooth (see Figure 20-20). |
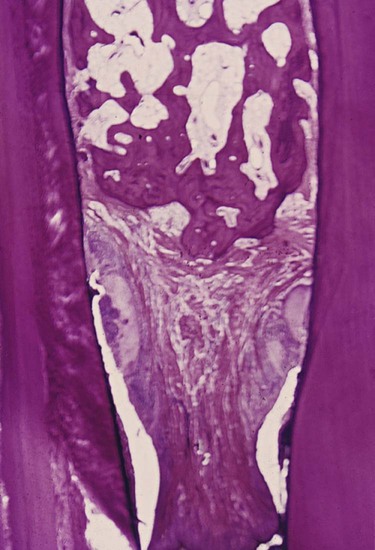
Periodontal Abscess
A periodontal abscess is a localized purulent inflammation in the periodontal tissues (Figure 20-23). It is also known as a lateral abscess or a parietal abscess. Abscesses that are localized in the gingiva, that are caused by injury to the outer surface of the gingiva, and that do not involve the supporting structures are called gingival abscesses. Gingival abscesses may occur in the presence or absence of a periodontal pocket (see Chapter 9).

Periodontal abscess formation may occur in the following ways:
1. Extension of infection from a periodontal pocket deeply into the supporting periodontal tissues and localization of the suppurative inflammatory process along the lateral aspect of the root.
2. Lateral extension of inflammation from the inner surface of a periodontal pocket into the connective tissue of the pocket wall. Formation of the abscess results when drainage into the pocket space is impaired.
3. Formation in a pocket with a tortuous course around the root. A periodontal abscess may form in the cul-de-sac, the deep end of which is shut off from the surface.
4. Incomplete removal of calculus during treatment of a periodontal pocket. The gingival wall shrinks, thereby occluding the pocket orifice, and a periodontal abscess occurs in the sealed-off portion of the pocket.
5. After trauma to the tooth or with perforation of the lateral wall of the root in endodontic therapy. In these situations, a periodontal abscess may occur in the absence of periodontal disease.
Periodontal abscesses are classified according to location as follows:
1. Abscess in the supporting periodontal tissues along the lateral aspect of the root. With this condition, a sinus generally occurs in the bone that extends laterally from the abscess to the external surface.
2. Abscess in the soft-tissue wall of a deep periodontal pocket.
Microscopically, an abscess is a localized accumulation of viable and nonviable PMNs within the periodontal pocket wall. The PMNs liberate enzymes that digest the cells and other tissue structures, thereby forming the liquid product known as pus, which constitutes the center of the abscess. An acute inflammatory reaction surrounds the purulent area, and the overlying epithelium exhibits intracellular and extracellular edema and the invasion of leukocytes (Figure 20-24).

The localized acute abscess becomes a chronic abscess when its purulent content drains through a fistula into the outer gingival surface or into the periodontal pocket and the infection that is causing the abscess is not resolved.
The bacterial invasion of tissues has been reported in abscesses; the invading organisms were identified as gram-negative cocci, diplococci, fusiforms, and spirochetes. Invasive fungi were also found and were interpreted as being “opportunistic invaders.”22 Microorganisms that colonize the periodontal abscess have been reported to be primarily gram-negative anaerobic rods.51
Lateral Periodontal Cyst
The periodontal cyst, which is also called lateral periodontal cyst, is an uncommon lesion that produces localized destruction of the periodontal tissues along a lateral root surface, most often in the mandibular canine–premolar area.23,70 It is considered to be derived from the rests of Malassez or other proliferating odontogenic rests.69
A periodontal cyst is usually asymptomatic, without grossly detectable changes, but it may present as a localized, tender swelling. Radiographically, an interproximal periodontal cyst appears on the side of the root as a radiolucent area bordered by a radiopaque line. Its radiographic appearance cannot be differentiated from that of a periodontal abscess.