Capillary collection
Objectives
After completing this chapter, you should be able to:
1. List situations in which a capillary collection might be preferred.
2. Explain why it is necessary to inform the physician when capillary blood is collected.
3. Describe the common skin puncture devices.
4. Discuss containers that may be used to collect capillary blood.
5. Explain how circulation may be increased at the puncture site.
6. Discuss proper capillary collection site selection.
7. Explain why it is important to control the depth of the puncture.
8. List, in order, the steps for capillary collection.
9. Describe how the cut should be made when a finger is used as the puncture site.
10. Explain why the first drop of blood is discarded.
11. List precautions to be observed when collecting capillary blood.
12. State the order of the draw in collecting capillary blood.
13. List, in order, the steps for performing a bleeding time (BT) test.
Key terms
ancillary blood glucose test
bleeding time (BT) test
bilirubin, uric acid, phosphorus, and potassium (BURPP)
calcaneus
capillary tubes
Caraway or Natelson pipets
iatrogenic anemia
microcollection containers
microcollection tubes
microhematocrit tubes
osteochondritis
osteomyelitis
venous thrombosis
Capillary collection, also called dermal puncture or skin puncture, is the usual collection procedure for infants. In adults, it is an alternative collection procedure when minute amounts of blood are needed for testing, or for patients for whom venipuncture is inadvisable or impossible. In addition, it is typically used when collecting blood from infants and point-of-care testing. The depth of puncture must be carefully controlled to produce adequate flow while avoiding contact with underlying bone. Skin puncture devices deliver a precise incision, and microsample containers, sized to fit the desired sample, collect the blood from the puncture site.
Abbreviations
BURPP bilirubin, uric acid, phosphorus, and potassium
Reasons for performing capillary collection
Although venipuncture is the most common way to obtain a blood sample, at times it is impossible or inadvisable to do so. In these situations, capillary collection (also called skin puncture or dermal puncture) offers a valuable alternative. Capillary collection is the preferred method for obtaining blood from newborns and infants for neonatal bilirubin, newborn screening, and point-of-care testing. Capillary collection is also used for ancillary blood glucose testing.
A requisition form generally does not state that a capillary collection should be performed, and it is up to the phlebotomist to choose the best collection method for the tests ordered. For this reason, you must be familiar with the advantages, limitations, and appropriate uses of capillary collection. Knowing how and when to perform a capillary collection is a vital skill for a phlebotomist.
Capillary collection is preferred in several situations and for several types of patients (Box 10-1). Adult patients undergoing frequent glucose monitoring are excellent candidates for capillary collection, because the test requires only a small amount of blood, which must be taken frequently. Access to venipuncture sites may be difficult with obese patients, whose veins are often hard to find, and with geriatric patients, who often have small or fragile veins that can make obtaining venous blood difficult. Venipuncture may be contraindicated for patients with burns or scars over venipuncture sites or for those at risk for venous thrombosis (caused when clots form within the veins), because venipuncture increases the risk of venous thrombosis. Other patients may be at risk for serious complications associated with deep venipuncture, including iatrogenic anemia, hemorrhage, infection, organ or tissue damage, arteriospasm, or cardiac arrest. Iatrogenic anemia is anemia caused by excessive blood draws.
Capillary collection is usually the preferred method of collection for newborns, infants, and children younger than 2 years. Young children’s smaller veins and lower blood volume make venipuncture both difficult and potentially dangerous. Reducing blood volume through venipuncture is a concern for newborns and infants. It may lead to anemia and even cardiac arrest and death.
In addition to serving as a substitute for venipuncture, capillary blood gas (CBG) determination can be used as an alternative to arterial puncture for arterial blood gas (ABG) determination in infants.
FLASH FORWARD

Special considerations for collection from pediatric and geriatric patients are discussed in Chapter 12.
However, some tests cannot be performed on blood from a capillary collection. These include blood cultures and most routine coagulation tests. Capillary collection may not be appropriate for severely dehydrated patients, because test results may not be accurate. (This may also be a concern with venipuncture for such patients.) Capillary collection should not be used at sites that are swollen or where circulation or lymphatic drainage is compromised (such as a limb on the same side as a mastectomy).
Differences between venous and capillary blood
A capillary puncture collects blood from capillaries. Because capillaries are the bridges between arteries and veins, blood collected by capillary puncture is a mixture of venous blood and arterial blood. The arterial proportion in the sample is increased when the collection site is warmed, as may be done to help increase blood flow before collection. Small amounts of tissue fluid from the puncture site may also be in the sample, especially in the first drop.
The levels of many substances are the same in both capillary and venous blood, but this is not the case for all substances, as indicated in Table 10-1. For instance, the normal potassium reading obtained by capillary collection is lower than that in a plasma sample obtained by venipuncture, but higher than that in a serum sample obtained by venipuncture. Because of these differences, results obtained by the two techniques cannot be compared. For this reason as well, it is important to record that the sample was obtained by capillary collection.
TABLE 10-1
Reference Values in Capillary and Venous Blood
| Higher in Capillary Blood | Higher in Venous Blood |
| • Glucose | • Calcium |
| • Hemoglobin | • Total protein |
| • Potassium (serum sample) | • Potassium (plasma sample) |

Equipment for capillary collection
Capillary collection equipment allows the phlebotomist to puncture the skin safely and collect the sample quickly and efficiently, with a minimum of discomfort for the patient.
Skin puncture devices
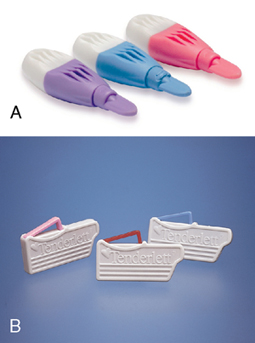
Skin puncture devices in the modern health care environment are designed with a retractable blade per Occupational Safety and Health Administration (OSHA) safety regulations. Some devices are contact activated, whereas others require the phlebotomist to depress a trigger to release the blade. Automatic puncture devices (Figure 10-1) deliver a swift puncture to a predetermined depth, which can be a significant advantage at sites where the bone is close to the skin (see “Site Selection”). The dimensions of the puncture are controlled by the width and depth of the point. Some automatic puncture devices have a platform that is positioned over the puncture site and color coded for different depths. (The automatic devices designed for home glucose testing make a cut that is too small for multiple tests or for filling several microsample containers and are not used in clinical practice.) Safety features include retractable blades and locks that keep a blade from being used a second time and prevent accidental sticks to the phlebotomist.
The Lasette laser lancing device is unique in that it uses a laser, rather than a sharp instrument, to pierce the skin, which causes less pain and bruising at the sample site. Cross-contamination between patients is avoided by disposing of the single-use lens cover between uses. The device is approved for patients 5 years and older.
Microsample containers
Microsample containers come in different sizes to accommodate different volumes of blood.
Microcollection tubes (also called “bullets”) hold up to 750 μL of blood. They are made of plastic and are available with a variety of anticoagulants and additives (Figure 10-2). The tubes are color coded by additive to match the coding of evacuated containers. Microcollection tubes are used for all types of dermal puncture collections and are the most common type of collection containers used for dermal puncture samples. They are also available with a plastic capillary tube that is fitted inside the container to aid in the collection of the sample.

FLASH FORWARD
See Appendix A to review metric symbols.
Capillary tubes come in either plastic or glass, and in a range of sizes. These tubes are used primarily for the collection of samples for CBG determinations. Caraway or Natelson pipets are narrow glass tubes with capacities up to about 470 μL. The use of these tubes has declined in recent years because of heightened attention to sharps injury prevention, and OSHA recommends against using glass tubes of this sort. Plastic capillary tubes are increasingly being used instead.
Capillary tubes are available either plain, with a blue band, or heparin coated, with a red, yellow, or green band (colors may vary with the manufacturer). Once the sample is in the tube, one or both ends are sealed. Sealing used to be done by pushing the ends into soft clay. New, safer sealing methods are recommended that instead fit the ends with small plastic caps. Both ends must be sealed for a CBG determination. In the laboratory, the sample may be centrifuged to separate cells from plasma or serum. The sample can be removed with a syringe.
FLASH FORWARD
You will learn about collecting blood gas samples in Chapter 13.
Microhematocrit tubes are small tubes, either plastic or glass, with a volume up to 75 μL. These tubes are used infrequently and have been largely replaced by microcollection containers. However when a spun hematocrit is requested, a plastic capillary tube can be used.
Finally, capillary collection is also used in neonatal screening for a variety of inherited diseases. In this situation, no collection container is used. Instead, drops of blood are applied directly to specially prepared filter paper.
FLASH FORWARD
You will learn about neonatal screening collection in Chapter 12.
Additional supplies
As in venipuncture, alcohol pads are used to prepare the site, and gauze pads are used to help stop the bleeding. A sharps disposal container is needed for the lancet.
Warming devices increase circulation. Simple towels or washcloths may be soaked in warm water and applied to the site. Be sure that the site is completely dry before puncture, however, as residual water will cause hemolysis and dilution of the specimen. Commercial warming packs are also available. The pack is first wrapped in a dry towel and then activated by squeezing. Such “heel warmers” are often used when blood must be collected from infants. The temperature of the device should not exceed 42° C, and it should be applied for 3 to 5 minutes. Glass slides are used to prepare blood smears for microscopic examination of blood cells.
FLASH FORWARD
You will learn how to prepare a blood smear in Chapter 14.
Site selection
General considerations
Capillary collection should be performed on warm, healthy skin that is free of scars, cuts, bruises, and rashes. The site must be easily accessible and have good capillary flow near the skin surface, but there must be enough clearance above the underlying bone to prevent the lancet from accidentally contacting it. Bone puncture can lead to osteochondritis, a painful inflammation of the bone or cartilage, or osteomyelitis, a potentially serious, sometimes fatal, bone infection.
You should also avoid skin that has been damaged or compromised in any way. Specific areas to avoid include skin that is callused, scarred, burned, infected, bruised, edematous, or bluish. Also avoid previous puncture sites as well as sites where circulation or lymphatic drainage is compromised.
Puncture depth and width
The depth of the puncture depends on the site and the patient (Table 10-2). To minimize the risk of inflammation and infection, the lancet should never penetrate more than 3.0 mm. For a heel puncture, the maximum depth is 2.0 mm, because the calcaneus, or heel bone, can lie very close to the surface. For premature babies, the recommended depth is 0.65 to 0.85 mm.
TABLE 10-2
Puncture Depth
| Use | Depth |
| Finger stick | 3.0 mm |
| Heel stick | 2.0 mm |
| Heel stick (premature infants or neonates) | 0.65–0.85 mm |
| Bleeding time | 1.0 mm |
Puncture width should not exceed 2.4 mm (Figure 10-3). At the right site, this achieves adequate blood flow but remains well above the bone. Puncture width is actually more important than depth in determining blood flow, because capillary beds may lie close to the skin, especially for newborns. A wider cut severs more capillaries and produces greater flow.
Capillary collection sites for adults and older children
For adults and for children older than 1 year, dermal punctures are almost always performed on the fingertips of the nondominant hand. The best sites are the palmar surface of the distal segments of the third (middle) and fourth (ring) fingers (Figure 10-4). The thumb is likely to be callused, and the index finger’s extra nerve endings make punctures more painful. The little finger (pinky) has too little tissue for safe puncture. If the fingers cannot be used, the big toe may be an option—check the policy at your workplace. Earlobes are never used for dermal puncture.

 FLASHBACK
FLASHBACK
Anatomic terminology was discussed in Chapter 6.
The puncture should be made near the fleshy center of the chosen finger. Avoid the edge of the finger, as the underlying bone is too close to the surface. As indicated in Figure 10-4, the puncture should be made perpendicular to (across) the ridges of the fingerprint, which lessens the flow of blood into the grooves.
Capillary collection sites for infants
For children younger than 1 year, there is too little tissue available in any of the fingers. For this reason, dermal puncture is performed in the heel (Figure 10-5). As shown in Figure 10-6, only the medial and lateral borders of the plantar (bottom) surface can be used. The center of the plantar surface is too close to the calcaneus, as is the posterior (back) surface. The arch is too close to nerves and tendons. For older infants, the big toe may be used if the heel is unacceptable. Be aware that the heel may be callused on young children who have begun to walk.


 AVOID THAT ERROR!
AVOID THAT ERROR!
When phlebotomist Brandon Mayhew entered the waiting room and saw his next draw, 1-month-old Derek Stevens, he knew he would need to be especially careful to make this dermal collection as smooth as possible for both the infant and the nervous mother. He greeted them warmly, smiled at Derek, and quickly cleansed the infant’s big toe, which Brandon had chosen as the puncture site. Once it was dry, he collected the sample without delay, applied a bandage, labeled the tubes, and thanked the patient. Two weeks later, Derek was admitted to the hospital with a bone infection, and Brandon was named in a lawsuit for injuring Derek. What did Brandon do wrong? What should he have done? And what should he do now?
Capillary collection
Procedure 10-1 outlines the steps for a capillary collection. In addition to these specific steps, you should always greet the patient, identify the patient, and obtain consent, as you would for a routine venipuncture.
PROCEDURE 10-1




Capillary Collection
|
1. After documenting on the requisition that you are performing a capillary collection, sanitize your hands and put on gloves.
Proper hand sanitation and gloving techniques were covered in Procedures 4-1 and 4-2. | |
 | |
|
Warm the area first, if necessary. If the site feels cold, it should be warmed for at least 3 minutes at a temperature no greater than 42° C. If a wet washcloth is used, be sure to remove any residual water, as residual water will cause hemolysis and dilution of the specimen. Use 70% isopropyl alcohol to clean the site. Allow the site to dry completely. In addition to causing stinging, contamination, and hemolysis, residual alcohol interferes with the formation of rounded drops of blood on the skin surface. (Use of povidone–iodine is not recommended for dermal punctures, because it may elevate test results for bilirubin, uric acid, phosphorus, and potassium. Remember the acronym BURPP to help you learn this group of tests.) Massaging the finger proximal to the puncture site (closer to the palm) can help increase blood flow. To avoid hemolysis, massage gently, and do not squeeze. |

 |
|
4. Position and hold the area. Hold the finger or heel firmly. This prevents it from moving during the puncture and reassures the patient. Grasp the patient’s finger with its palmar surface up, holding it between your thumb and index finger. To hold the patient’s heel, place your thumb in the arch, wrap your hand over the top of the foot, and place your index finger behind the heel. |
 |
|
5. Make the puncture, and dispose of the blade properly. Align the device so the cut is made across the fingerprint ridges or heel lines. This allows the blood to flow out and make a rounded drop, rather than run into the grooves. Puncture the skin slightly lateral to the center of the finger (that is, slightly toward the pinky finger), so that the hand can be tilted for easier blood flow into the container. Do not lift the device immediately after the puncture is complete. Count to two before lifting the device to ensure that the blade has made the puncture to the full depth and then fully retracted. Scraping of the skin may occur if the blade is not retracted. Dispose of the used blade immediately in an appropriate collection container. Failure to obtain blood: If you are unable to obtain sufficient blood with the first puncture, the policy at most institutions is to attempt one more puncture. You must use a sterile lancet to make the new puncture. After two unsuccessful punctures, notify the nursing station and contact a different phlebotomist to complete the procedure. |


 |
|
6. Prepare to collect the sample. Wipe away the first drop of blood with a clean gauze pad to prevent contaminating the sample with tissue fluid. Keep the finger in a downward position to help encourage blood flow. You can alternate applying and releasing firm pressure proximal to the site to increase flow, but avoid constant massaging, as this will cut off flow, cause hemolysis, and introduce tissue fluid back into the sample. |

 |
|
Once blood is flowing freely, position the container for collection. Microcollection tubes should be slanted downward. Lightly touch the scoop of the tube to the blood drop, and allow the blood to run into the tube. Do not scrape the skin with the container. This causes hemolysis, activates platelets, and contaminates the sample with epithelial skin cells. Tap the container lightly to move blood to the bottom. Close the lid after the sample has been collected. Invert the tube 8 to 10 times after filling if additives are present. Be careful not to overfill the microcollection tube containing anticoagulant because the ratio of anticoagulant to blood will be exceeded and microclots will form. The collection will need to be repeated due to inaccurate test results. Order of collection: Platelet counts, complete blood counts (CBCs) and other hematology tests are collected first, followed by chemistry tests. Be mindful of specimens that require special handling before transport. |
 |
|
Apply pressure to the puncture site using a clean gauze square. Once bleeding has stopped, you can bandage the site for older children and adults. Do not use a bandage on children younger than age 2, as they may remove the bandage and choke on it. When drawing blood from children and infants, be especially careful that all equipment has been picked up and bed rails have been placed back in position. Label the microsample container, and place it in a larger holder for transport to the laboratory. |
 |
Other uses of capillary puncture
Capillary puncture is used for bleeding time tests and ancillary blood glucose testing (also called bedside glucose testing). It can also be used as an alternative to arterial puncture for ABG determination.
Bleeding time test
A bleeding time (BT) test measures the length of time required for bleeding to stop after an incision is made. In the past, this test was used before surgery to help assess the overall integrity of primary hemostasis. Inconsistencies in the test have led to its replacement by the platelet function assay (PFA) or other tests. These are performed not on dermal puncture samples but on venous blood. The procedure is included here because you may be called upon to perform it nonetheless. To perform a BT test, an automated incision device is used, with the depth set at 1 mm, and length at 5 mm. Some devices make one incision; others make two incisions at the same time. The steps of the BT test are shown in Procedure 10-2.
PROCEDURE 10-2
Bleeding Time Test








FLASHBACK
Hemostasis was discussed in Chapter 7.
Results and complications
Normal BT is 2 to 10 minutes and depends somewhat on the device used. Bleeding that does not stop within 15 to 20 minutes means one of two things: (1) either the patient has a condition that is interfering with normal platelet plug formation or (2) the test was performed incorrectly—a capillary was scratched, the incision was too deep, the filter paper touched the incision site, or some technical error was made. If only one incision was made, the test may have to be repeated on the other arm. If two incisions were made and the two BTs are within several minutes of each other, it is unnecessary to repeat the test. Be sure to learn the exact protocol for your laboratory before this situation occurs. Abnormally short BTs are probably caused by a test error—for instance, the incision may have been too shallow, the device may have been lifted too soon, or there may have been hair at the incision site.
Review for certification
Capillary collection is used for a variety of patients with compromised or otherwise inaccessible veins, including infants, or when only a small sample is needed. A calibrated puncture device delivers a precise, carefully controlled puncture, avoiding contact with the bone and reducing the risk of osteomyelitis or osteochondritis. The size and purpose of the sample dictate the collection container used, although microcollection tubes are increasingly used for most collections. The BT test assesses the integrity of primary hemostasis by measuring the time required to stop bleeding after a standard incision is made.
AVOID THAT ERROR!
Brandon chose an inappropriate site for dermal collection. In newborns, the bone in the toe is too close to the surface for safe dermal puncture. Brandon should have collected from the medial or lateral border of the plantar surface of the heel. Brandon also applied a bandage, which should not be used in children this young. At this point, Brandon will need to consult a lawyer to defend against the suit.
Study questions
See answers in Appendix F.
1. Name two sites commonly used for adult capillary collection.
2. Explain why it is best to perform a capillary collection rather than a venipuncture on children.
3. List six types of patients, other than infants, for whom capillary collection may be advisable.
4. Explain why, in a capillary collection, the first drop of blood is wiped away with clean gauze.
5. Describe what microcollection containers are used for.
6. What can be used to stimulate blood flow to the capillaries?
7. List six specific areas of the skin to avoid when performing a capillary collection.
8. At what age are heel sticks preferred to finger sticks?
9. List four reasons alcohol must air-dry before a capillary stick.
10. Explain why povidone–iodine should not be used for capillary collection procedures.
11. Which fingers are acceptable to use for capillary collection?
12. Describe the order of collection for a capillary collection.
13. Explain the purpose of the BT test.
14. Why should bandages not be placed on young children following a dermal puncture?
Certification examination preparation
See answers in Appendix F.
1. Capillary collections are performed on
2. Which of the following has a higher value in a capillary sample as opposed to a venous serum sample?
3. Good candidates for dermal collection include patients who
4. Capillary collection may be appropriate in geriatric patients because
a. tourniquets are hard to place in this patient group.
b. their veins tend to be small and fragile.
5. An infant heel-warming device should be applied for approximately
6. The depth of a heel puncture should not be more than
7. Which finger is most widely used for capillary collection?
8. In performing a dermal puncture, the puncture should be
9. The location for heel sticks is the
10. Which sample(s) is/are collected first in a capillary collection?
11. Which medication does not interfere with the BT test?
12. At what level does the blood pressure cuff remain during a BT test?