Asepsis and Infection Control
Objectives
1. Explain the difference between medical and surgical asepsis.
2. Explain how each element of the chain of infection contributes to infection.
3. List five major classifications of pathogens.
4. Identify the body's normal defenses against infections.
5. Discuss nursing interventions used to interrupt the chain of infection.
6. Describe the signs and symptoms of a localized infection and those of a systemic infection.
7. Discuss the events in the inflammatory response.
8. Discuss standard precautions.
9. Demonstrate the proper procedure for hand hygiene.
10. Demonstrate technique for gowning and gloving.
11. Identify principles of surgical asepsis.
12. Describe the accepted techniques of preparation for disinfection and sterilization.
13. Discuss patient teaching for infection prevention and control as an element of health promotion.
14. Discuss infection prevention and control measures in the home.
Key Terms
http://evolve.elsevier.com/Cooper/foundationsadult/
With the discovery that microorganisms cause infection came the realization that illness or disease caused by infection is prevented by inhibiting or stopping growth and reproduction. Aseptic technique is a method developed by Joseph Lister (1827–1912) to reduce morbidity and mortality from infection. Lister is known as the father of aseptic technique, although many researchers contributed to its development.
In today's health care environment, nurses and other health care workers must practice effective infection prevention and control measures to protect patients from drug-resistant microorganisms and prevent occupational exposure to infectious material, which helps reduce health care delivery costs.
Asepsis
The increase of transmissible infections, not only in health care facilities but also in the home, is an issue of great societal concern. Microorganisms (tiny, usually microscopic, entities capable of carrying on living processes) are naturally present on and in the human body and in the environment. Many of these microorganisms are harmless (nonpathogenic) and in most individuals do not produce disease. Some are even helpful. If an individual is highly susceptible to infection, the nonpathogenic microorganisms can be dangerous.
Any patient who enters a health care facility has a greater risk of an infection developing because of reduced immunologic function. Increased stressors on the patient's immune system are caused by the presenting illness, exposure to disease-causing microorganisms, and portals created by invasive procedures. In addition, health care facilities are an environment conducive to the spread of these microorganisms because of the many ill carriers within their walls. The nurse's knowledge about infection and the application of infection prevention and control principles help protect patients from infection. With each patient care activity, the nurse should ensure that infection prevention and control is part of the routine.
Infection prevention and control consists of the implementation of policies and procedures in hospitals and other health care facilities to minimize the spread of health care–associated or community-acquired infections to patients and other staff members. During patient care activities, the nurse may be exposed to pathogenic microorganisms. The nurse is a chief player in the prevention of the spread of infection, which is accomplished with learning and continued observation of both routine and specialized practices of cleanliness and disinfection. These techniques aid in accomplishing asepsis (the absence of pathogenic microorganisms). Asepsis is divided into the following two categories:
1. Medical asepsis consists of techniques that inhibit the growth and transmission of pathogenic microorganisms. Medical asepsis is also known as clean technique and is used in many daily activities, such as hand hygiene and changing of patient bed linens.
2. Surgical asepsis consists of techniques designed to destroy all microorganisms and their spores (the reproductive cell of some microorganisms, such as fungi or protozoa). Surgical asepsis is known as sterile technique and is used in specialized areas, such as the operating room, or during invasive procedures, such as urinary catheter insertion.
Infection
For an infection to develop, a specific cycle or chain of events must occur. The following six elements are necessary for infection and are referred to as the chain of infection (Figure 7-1):
1. Infectious agent: A pathogen
2. Reservoir: Where the pathogen can grow
3. Portal of exit: Exit route from the reservoir
4. Mode of transmission: Method or vehicle of transportation, such as exudate, feces, air droplets, hands, and needles
5. Portal of entry: Entrance through skin, mucous lining, or mouth
6. Host: Another person or animal that is susceptible to the pathogen

For prevention of the transmission of an infection, the cycle must be interrupted. Medical asepsis is an effective way to disrupt the chain of infection. This practice helps to inhibit (to stop or slow a process) the growth and reduce the number of microorganisms.
Infectious Agent
Pathogenic microorganisms are infectious agents. Pathogens can be bacteria, viruses, yeasts, fungi, and protozoa. All these microorganisms need food for growth and a suitable environment in which to live. Unwashed hands, wound drainage, soiled linen, and decaying teeth provide ideal areas for pathogenic growth. The microorganism strength, the number of microorganisms present, the effectiveness of a person's immune system, and the length of exposure to the microorganisms determine the ability to produce disease. The role of the nurse is to provide a safe environment by working to prevent the transmission of infection.
Health care workers have several ways to help their patients remain free of infection. Proper disinfection (the use of a chemical that can be applied to objects to destroy microorganisms), appropriate use of an antiseptic (a substance that tends to inhibit the growth and reproduction of microorganisms and may be used on humans), and use of surgical asepsis when indicated are all important ways to help reduce the presence of microorganisms.
 Bacteria
Bacteria
Bacteria have many different characteristics. In addition to their three basic shapes (round, oblong, and spiral), there are many variations. Some are elongated or have pointed ends, and some are flattened on one side. Some are shaped like commas, and others appear square. Spirilla are often tightly coiled, like a corkscrew. During cell division, some bacteria remain together to form pairs, whereas others form long chains. Diagnostic testing focuses on the unique characteristics for identification of specific types of bacteria.
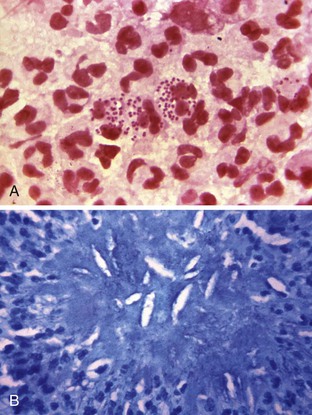
Bacteria can also be differentiated by their chemical compositions, the nutrients that they need to grow, and the waste products that the bacteria form. Aerobic bacteria grow only in the presence of oxygen, whereas anaerobic bacteria grow only in the absence of oxygen (Figure 7-2, A and B). Some bacteria are capable of movement. Motility is possible because of fine, hair-like projections—flagella—that extend from the bacterial cell. These projections move in a wavelike fashion to propel the cell. Some bacteria have only one flagellum attached to one end of the cell, and others have many flagella surrounding the cell. Locomotion of the spirochete is achieved with a wiggling motion that involves the entire cell body.
Some bacteria form a specialized structure called a spore. The spore is a round body that is formed by the bacterium when conditions are unfavorable for growth of the bacterium. The spore enlarges until it is as large as the bacterial cell and is surrounded by a capsule. Eventually, the portion of the cell that surrounds the spore disintegrates. The spore remains dormant until environmental conditions become favorable for growth. Then, the spore germinates and begins reproducing. Characteristically, spores have a high degree of resistance to heat and disinfectants. Some bacteria have the ability to form capsules around the cell wall. These mucilaginous (of a thick, sticky, slimy substance) envelopes form when the bacterial environment is hostile. The formation of the capsule is a defense mechanism to help protect the bacteria. As with spores, staining in the laboratory usually requires special procedures. Capsule formation also contributes to the development of multidrug resistance. When capsules are present, antibiotic therapy is sometimes ineffective because the capsule prevents the drug from reaching the bacteria within the capsule.
Identification of the specific organism is vital to the development of the appropriate plan of treatment. Antimicrobial therapies provide a system of attack that is individualized to specific microorganisms. Specially trained laboratory personnel perform this identification. In some instances, they examine a specimen before staining it, but this method is usually less satisfactory. Most bacteria are not visible without a special staining process, in which a dye is applied to a specially prepared glass slide that contains a small amount of the material to be examined. Identification of most bacteria is possible with this simple process; however, other bacteria necessitate additional staining.
Depending on whether a color can be removed with a solvent or the color is retained after the use of the solvent, the organism is identified as gram positive or gram negative. Special staining techniques are required for bacteria that have flagella, spores, or capsules.
The nurse collects specimens of body fluids and secretions suspected of containing pathogenic organisms in sterile containers and sends them to the laboratory for culture and sensitivity testing. Laboratory personnel transfer the specimen to a special culture medium that promotes growth. They then study the culture and identify the pathogens. The results of the sensitivity tests assist the practitioner in determining which antimicrobial (antibiotic) medication will effectively inhibit the pathogens' growth. The practitioner then orders appropriate antimicrobial agents on the basis of these tests, which typically take 48 to 72 hours to complete. Different organisms require different antibiotics to be effectively destroyed.
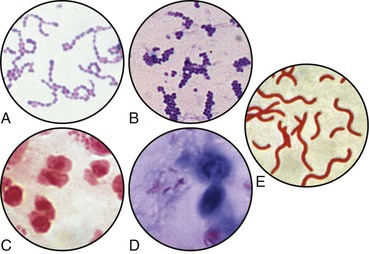
Bacterial infections are transmitted from person to person by direct contact, by inhalation, and by indirect contact with articles contaminated with the pathogen. Some are also transmitted through the ingestion of contaminated food and drink (Figure 7-3).
The Streptococcus bacterium is responsible for more diseases than any other organism, but methicillin-resistant Staphylococcus aureus (MRSA) has been found to be responsible for a number of serious and sometimes fatal infections. Patients with immunocompromised conditions who are admitted to health care facilities have an increased risk of exposure to strains of MRSA that are multidrug resistant and therefore more difficult to treat.
Rocky Mountain spotted fever has been found in almost every area of the United States, and its prevalence continues to increase. It is transmitted to humans through the bite of an infected tick. Several varieties of ticks carry the disease. The ticks live on many different kinds of animals found in rural and wooded areas. They are also able to live on common house pets, such as cats and dogs. People who work in areas where ticks are known to be abundant are more likely to become infected. The tick attaches itself to the skin, and the longer it remains attached, the more likely the person is to become infected. Great care must be taken not to crush or squeeze the tick on removal from the skin.
The spore-forming bacterium Bacillus anthracis causes the acute infectious disease of anthrax. Anthrax infection occurs in three forms:
• Cutaneous (skin) (Figure 7-4)

Anthrax occurs more commonly in animals, but it also has the ability to infect humans. It is seen more often in agricultural regions of South and Central America, southern and eastern Europe, Asia, Africa, the Caribbean, and the Middle East, where it is found in animals. It rarely infects domesticated animals in the United States.
B. anthracis spores are able to live in the soil for many years. Casual contact from person to person does not spread anthrax. In cases of intentional exposure (e.g., during a biologic terrorism event), the most likely routes of infection are inhalation of the spores and spore contact with skin. B. anthracis is considered by the Centers for Disease Control and Prevention (2006) to be one of a number of potential agents that may be used during a biologic terrorism event (see Chapter 10).
Anthrax infection is diagnosed when B. anthracis is detected in blood, skin lesions, or respiratory secretions by means of a laboratory culture or measurement of specific antibodies in the blood of infected people.
Treatment consists of antibiotics such as ciprofloxacin (Cipro) or doxycycline (Vibramycin). A vaccine is available for prevention of anthrax infection. Vaccination is recommended for those at high risk of exposure, such as laboratory personnel who handle the bacterium or members of the armed forces. If left untreated, anthrax can be fatal.
Viruses
Viruses are the smallest known agents to cause disease. They are not complete cells but are composed of either RNA or DNA. They consist of a protein coat around a nucleic acid core and depend on the metabolic processes of the cell they enter. Before 1900, scientists discovered that certain agents, unlike bacteria, have the ability to pass through a laboratory filter. In addition, they were unable to observe these tiny bodies with the ordinary microscope. In 1898, Martinus W. Beijerinck called these small bodies viruses, and they became known as filterable viruses.
For years, scientists knew little about viruses, even though they were able to observe their effect on humans and animals. In 1941, the electron microscope became available. With this advancement, the science of virology was born, and a whole new era in the study of human disease was opened. In addition, the development of other tools and techniques has resulted in rapid advances in the study of viruses: the use of certain dyes that become luminous when exposed to ultraviolet light (fluorescent microscopy), tissue culture methods, ultracentrifuge, cytochemistry, and the development of other technical laboratory aids.
Viruses gain entrance to the body through various portals such as the respiratory tract, the gastrointestinal tract, and broken skin. Sometimes a virus can infect a susceptible host through a mosquito bite or during an accidental needle stick with a contaminated needle. Viruses are selective in the type of body cells they attack, but once they have found cells for which they have an affinity, they enter the cell and reproduce rapidly. As they multiply, they interrupt the cell activities and use the cell material to produce new virus material.
Viral infections are usually self-limiting. They run a given course, and recovery usually occurs. One exception is acquired immunodeficiency syndrome (AIDS). Without adequate treatment with specific types of medication, the human immunodeficiency virus (HIV) reproduces and the immune system continues to be stressed to the point where it can no longer fight off even the most common infection; the patient then receives the diagnosis of AIDS. Other viral diseases have the capacity to cause death if complications occur or if they attack individuals with extremely weak or debilitated conditions. People who are at either end of the age spectrum are also at increased risk for complications. The common cold is caused by a virus. Symptoms of the common cold are usually relieved with the patient staying in bed and taking certain over-the-counter remedies. No medicine cures the cold; medicine only relieves the discomfort. Antibiotics do not alter the course of the vast majority of viral diseases.
Viruses are classified in various ways, either according to the diseases they cause or by the characteristics of a specific group. In the latter classification system, each subgroup often has many types or strains (Table 7-1).
Table 7-1
Common Pathogens, Reservoirs, and Infections or Diseases
| ORGANISM | PRIMARY RESERVOIR | INFECTION OR DISEASE |
| Bacteria | ||
| Staphylococcus aureus | Skin, hair, anterior nares | Wound infection, pneumonia, food poisoning |
| β-Hemolytic group A streptococci | Oropharynx, skin, perineal care | Strep throat, rheumatic fever, scarlet fever, impetigo |
| β-Hemolytic group B streptococci | Adult genitals | Urinary tract infection, wound infection, neonatal sepsis |
| Escherichia coli | Colon | Enteritis |
| E. coli serotype O157:H7 | Colon—food and water | Hemolytic-uremic syndrome (HUS) |
| Neisseria gonorrhoeae | Genitourinary tract, rectum, mouth, eye | Gonorrhea, pelvic inflammatory disease, conjunctivitis |
| Staphylococcus epidermidis | Skin | IV line infection, bacteremia, endocarditis |
| Tubercle bacillus (Mycobacterium tuberculosis) | Lungs | Tuberculosis infection Tuberculosis disease |
| Bacillus anthracis | Infected animals or their products; bioterrorist release | Cutaneous anthrax Inhalation anthrax Gastrointestinal anthrax |
| Rickettsia rickettsii | Wood tick | Rocky Mountain spotted fever |
| Viruses | ||
| Herpes simplex virus I and II | Lesions of the mouth, skin, adult genitals | Cold sores, sexually transmitted infections |
| Hepatitis A and E | Food or water, feces | Hepatitis A and E |
| Hepatitis B, C, D, and G | Blood, body fluids, and excretions | Hepatitis B |
| Human immunodeficiency virus (HIV) | Blood, semen, vaginal secretions, breast milk | HIV-positive status, HIV infection |
| Varicella zoster virus | Vesicle fluid, respiratory tract infections | HIV disease Varicella (chickenpox) primary infection, herpes zoster (shingles) reactivation |
| Fungi | ||
| Pneumocystis jiroveci (carinii) | Intestinal tract, genitourinary tract, respiratory tract, and circulatory system of humans and animals | Pneumonia referred to as an opportunistic infection in acquired immunodeficiency syndrome (AIDS) |
| Candida albicans | Mouth, skin, colon, genital tract | Thrush, dermatitis, sexually transmitted diseases |
| Cryptococcus species | Bird feces | Pneumonia-like illness, meningoencephalitis |
| Protozoa | ||
| Plasmodium falciparum | Mosquito | Malaria |
| Entamoeba histolytica | Intestinal tract (specifically the large intestine) | Diarrhea, colitis |
IV, Intravenous.
Fungi
Fungal (mycotic) infections are among the most common diseases found in humans. Fungi are among the most plentiful forms of life. They belong to the plant kingdom, and although many of them are harmless, some are responsible for infections. Fungus types that many people are familiar with include the fuzzy black, green, or white growth on stale bread. Mycotic infections are diseases caused by yeasts and molds. Some are superficial and involve the skin and the mucous membranes. Most frequently, the infections involve the external layers of the skin, the hair, and the nails.
Fungi may also invade the deeper tissues of the body. These types of infections may produce no signs or symptoms; however, some become serious and potentially fatal, especially in a patient with severe immunocompromise. Coccidioidomycosis (valley fever) and histoplasmosis (a systemic fungal respiratory disease) are examples of systemic fungal infections.
Protozoa
The protozoa are single-celled animals; in some form, they exist everywhere in nature. Some of the parasitic forms of protozoa are found in the intestinal tract, the genitourinary tract, the respiratory tract, and the circulatory system of humans and other animals. Protozoa are responsible for malaria, amebic dysentery, and African sleeping sickness (see Table 7-1).
Reservoir
To thrive, organisms need a proper atmosphere. Characteristics of an environment that supports organism growth include an available food source, oxygen, water, light, and desirable temperatures and levels of acidity or alkalinity. Any natural habitat of a microorganism that promotes growth and reproduction is a reservoir. Many areas of the body typically host a variety of microorganisms, but the presence of these microorganisms does not always cause illness. Reservoirs include humans, animals, and environmental sources. Within the health care environment, infection may breed and thrive in soiled dressings and medical equipment, including stethoscopes, bedside tables, and overbed tables.
A carrier, or vector, is a person or animal that does not become ill but harbors and spreads an organism, causing disease in others.
The nurse must be aware of the potential risk presented within the health care environment. Ensuring cleaning between patient use, prompt changing of soiled materials, and proper disposal of contaminated materials is helpful in this mission (Box 7-1).
Portal of Exit
A microorganism does not have the capacity to cause disease in another host without finding a point of escape from the reservoir. Examples of exit routes in humans are any body fluids produced from the patient, such as those from the gastrointestinal, respiratory, and genitourinary systems or from an open area on the patient's body.
With hand hygiene, the nurse can help prevent the spread of microorganisms. Also, the nurse should teach the patient to cover the nose and mouth when coughing or sneezing.
Mode of Transmission
A contaminated vehicle is the means by which microorganisms are carried about and transported to the next host, once they have left the reservoir. Contamination means a condition of being soiled, stained, touched by, or otherwise exposed to harmful agents (e.g., the entry of infectious materials into a previously clean or sterile environment), which makes an object potentially unsafe for use. If the vehicle is a living carrier, it is called a vector. If the vehicle is an inanimate (nonliving) object, it is called a fomite. Some examples of fomites found in health care facilities are computers (many people touch the computer throughout the day), medical records and charts, stethoscopes, thermometers, bandage scissors, used tissues, drinking glasses, needles, and soiled dressings.
Transmission via this kind of common contact with a fomite or vector is known as the indirect method of transmission. Transmission through direct contact is also possible, such as when the nurse uses poor hand hygiene technique and then turns or bathes a patient.
Air currents can carry microorganisms. To help reduce the number of microorganisms in the air, the nurse should not shake the linens when making a bed. Use of a dampened or treated cloth when dusting can help prevent circulation of dust particles.
The floor is one of the dirtiest areas in any building. The nurse should not use anything that has been dropped on the floor. Linens that have been dropped on the floor should be treated as soiled and placed in the appropriate container to be sent for laundering. Supplies (such as dressings) should be discarded. Feet and furniture are the only items that belong on the floor.
Because so many factors can promote the spread of infection to a patient, all health care workers who provide direct care (physical therapists, physicians, nurses) and those who perform diagnostic and support services (laboratory technicians, respiratory therapists, dietary workers) must follow infection prevention and control practices to prevent or minimize the spread of infection.
Portal of Entry
Once the microorganism has exited the reservoir and has been transmitted to a susceptible host, it has to find a way to enter the host. When the host's defense mechanisms are reduced (see the section “Host”), the microorganism has a greater chance to gain entry to the host and produce infection. If the patient's skin is punctured with a contaminated needle, microorganisms are able to enter into the bloodstream. If the nurse is not careful when changing a wound dressing, contamination of the new dressing or the wound could occur and could introduce possibly pathogenic microorganisms into the open wound and cause an infection.
Many of the entrance and exit routes microorganisms take are the same, and methods used to prevent or control both processes are also similar. The skin is the first line of defense. It should be kept intact, lubricated, and clean. The nurse should closely observe the patient's skin for any open areas and treat them accordingly (see Chapter 9).
Accidental needle sticks are a potential hazard for all personnel who work in a health care facility. Any injury caused by a sharp piece of possibly dirty equipment (such as a used needle or scalpel) should be reported immediately so that procedures can be started to help prevent development of specific types of infections (such as hepatitis B and HIV). Available and appropriate waste containers are essential for safe disposal of sharp instruments. Needles should never be recapped.
A Foley catheter or another type of drainage equipment often provides an entrance for microorganisms. The nurse should ensure that tubes remain connected and intact. The nurse should take care when turning, positioning, or transferring a patient to prevent any tubes from becoming tangled or pulling apart.
In the care of open areas, specific techniques can be used to prevent the entrance of microorganisms. The nurse should wear gloves when handling soiled dressings and place the dressings in the appropriate type of waste container for disposal per facility policy.
Host
A host is an organism in which another organism is nourished and harbored.
Susceptibility to an infection is defined by the amount of resistance that the host can exhibit against the pathogen. Microorganisms are constantly in contact with people, but an infection does not develop unless a person is susceptible to the microorganism's strength and numbers. As the pathogen's strength and numbers increase, the person becomes more susceptible. Factors that affect a person's immunologic defense mechanisms are described in Box 7-2.
Immunizations have proven effective in reducing susceptibility to some types of infectious diseases. These are given before a person has been exposed to a disease (to provide protection before contact) or after exposure (if the person's history indicates possible contact with an infectious microorganism). Table 7-2 lists the normal defense mechanisms against infection.
Table 7-2
Normal Defense Mechanisms Against Infection
| DEFENSE MECHANISMS | ACTION | FACTORS THAT MAY ALTER DISEASE |
| Skin | ||
| Intact multilayered surface (body's first line of defense against infection) | Provides barrier to microorganisms | Cuts, abrasions, puncture wounds, areas of maceration |
| Shedding of outer layer of skin cells | Removes organisms that adhere to skin's outer layers | Failure to bathe regularly |
| Sebum | Contains fatty acid that kills some bacteria | Excessive bathing |
| Mouth | ||
| Intact multilayered mucosa | Provides mechanical barrier to microorganisms | Lacerations, trauma, extracted teeth |
| Saliva | Washes away particles that contain microorganisms Contains microbial inhibitors (e.g., lysozyme) | Poor oral hygiene, dehydration |
| Eye tearing and blinking | Provides mechanisms to reduce entry (blinking) or to assist in washing away (tearing) particles that contain pathogens, thus reducing number (dose) of organisms | Injury, exposure—splash or splatter of blood or other potentially infectious material into the eye |
| Respiratory Tract | ||
| Cilia lining upper airway coated by mucus | Trap inhaled microbes and sweep them outward in mucus to be expectorated or swallowed Engulf and destroy microorganisms that reach lungs' alveoli | Smoking, high concentration of oxygen and carbon dioxide, decreased humidity, cold air |
| Urinary Tract | ||
| Flushing action of urine flow | Washes away microorganisms on lining of bladder and urethra | Obstruction to normal flow by urinary catheter placement, obstruction from growth or tumor, delayed micturition Introduction of urinary catheter, continual movement of catheter in urethra |
| Gastrointestinal Tract | ||
| Acidity of gastric secretions | Chemically destroys microorganisms incapable of surviving low pH | Use of antacids |
| Rapid peristalsis in small intestine | Prevents retention of bacterial contents | Delayed motility resulting from impaction of fecal contents in large bowel or mechanical obstruction by masses |
| Vagina | ||
| At puberty, normal flora cause vaginal secretions to achieve low pH | Inhibit growth of many microorganisms | Antibiotics, excessive douching, and oral contraceptives disrupting normal flora |
Health care facility policies mandate that workers be current with immunizations. Many facilities also require preventative medications and vaccines. As role models, nurses should provide teaching and encouragement to their patients concerning the benefits of these practices.
Infectious Process
When the nurse understands the chain of infection, the nurse gains the ability to intervene to prevent infections from developing. When the patient acquires an infection, the nurse can observe certain signs and symptoms and take appropriate actions to prevent its spread. Infections follow a progressive course (Box 7-3). The severity of the patient's illness depends on the extent of the infection, the virulence (disease-causing power) of the microorganisms, and the susceptibility of the host.
If infection is localized (e.g., a superficial wound infection), proper care helps control its spread and minimizes the illness (Figure 7-5). The patient usually experiences localized symptoms such as pain and tenderness at the wound site. An infection that affects the entire body instead of just a single organ or part is systemic and has potential to be fatal.

The course of an infection influences the level of nursing care that must be provided. The nurse is responsible for the administration of prescribed antimicrobial agents (antibiotics or antivirals). Monitoring of activities to assess response to the therapies includes the objective nursing assessment and vital signs, laboratory studies (e.g., white blood cell levels and albumin values), and subjective reports from the patient. Supportive therapy includes providing adequate nutrition and rest to bolster the body's defense against the infectious process. The complexity of care further depends on body systems affected by the infection.
Regardless of whether infection is localized or systemic, the nurse plays a critical role in minimizing its spread. For example, the organism that causes a simple wound infection often spreads to involve an incisional wound site if the nurse uses improper technique during the dressing change. If nurses have a break in their own skin, they may acquire infections from patients if the technique for controlling infection transmission is inadequate.
Inflammatory Response
Inflammation is the body's response to injury or infection at the cellular level. Inflammation is a protective vascular reaction that delivers fluid, blood products, and nutrients to interstitial tissues in the area of an injury. The process neutralizes and eliminates pathogens or necrotic (dead) tissues and establishes a means of repairing body cells and tissues. Signs of inflammation frequently include edema (swelling), rubor (redness), heat, pain or tenderness, and loss of function in the affected body part. When inflammation becomes systemic, other signs and symptoms develop, including fever, leukocytosis (increased white blood cell count), malaise (generalized discomfort), anorexia, nausea, vomiting, and lymph node enlargement.
The inflammatory response is triggered by physical agents, chemical agents, or microorganisms. Mechanical trauma, temperature extremes, and radiation are examples of physical agents. Chemical agents include external and internal irritants, such as harsh poisons or gastric acid. Microorganisms trigger this response as well, as previously discussed. The inflammatory response sometimes occurs in the absence of an infectious process.
Health Care–Associated Infections
One in every 20 patients admitted to the hospital has development of a health care–associated infection (HAI) (Centers for Disease Control, 2010). These infections were previously referred to as nosocomial infections. To be classified as an HAI, the infection develops at least 48 hours after hospitalization or contact with another type of health care facility. These infections pose a far-reaching and serious problem. Hospitals harbor microorganisms that are often highly virulent (exceedingly pathogenic), which makes them more likely places for infection. The hospitalized patient's immune system is probably already weakened from disease or invasive procedures, which makes the patient more susceptible to pathogens. HAIs not only necessitate longer hospital stays for the patient but also increase costs for both the patient and the hospital.
An exogenous (growing outside the body) infection is caused by microorganisms from another person (e.g., an infection transmitted to the patient by a health care worker). An endogenous (growing within the body) infection is caused by the patient's own normal microorganisms, which become altered and overgrow or are transferred from one body site to another (e.g., microorganisms in fecal material are transferred to skin by hands and infect a wound).
HAIs are most commonly transmitted via direct contact between health care workers and patients or from patient to patient. For this reason, a strong emphasis must be placed on the prevention of transmission with measures such as hand hygiene and environmental cleaning.
The nurse is responsible for providing the patient with a clean and safe environment. The nurse must be conscientious and thorough while performing clean and aseptic procedures to reduce the transmission of infection. To decrease the occurrence or duration of HAIs, many facilities have an infection prevention and control department, which investigates and establishes policies to ensure that all personnel maintain aseptic techniques while performing a procedure on a patient. These procedures include clean technique, which is used in all areas, and sterile technique, which is used in invasive procedures.
HAIs significantly increase health care costs. Extended lengths of stay in health care facilities increase disability, and prolonged recovery times add to the expenses the patient has to bear, and to those of the health care facility and any funding bodies (e.g., health insurance companies, Medicare, and Medicaid). In 2008, the Centers for Medicare and Medicaid Services (CMMS) took a stance against hospital acquired infections by discontinuing reimbursement for conditions such as catheter-associated urinary tract infections (UTIs) and bloodstream infections. This position encourages facilities to focus on activities that prevent hospital-acquired infections to avoid financial penalties.
Infection Prevention and Control Team
Infection prevention and control is a valuable discipline in the health care arena. The Occupational Safety and Health Administration (OSHA), hospital accrediting agencies, and hospital administration place a strong emphasis on infection prevention and control. Administratively, infection control nurses and other members of the infection prevention and control team function within the hospital via the infection prevention and control committee.
Infection Control Nurse
Many facilities employ nurses or other professionals who are specially trained in infection prevention and control. They are responsible for advising hospital personnel on the development and implementation of safe patient care delivery practices and for monitoring infection within the health care agency. Duties of an infection control nurse are as follows.
• Providing staff education on infection prevention and control.
• Reviewing and revising infection prevention and control policies and procedures to ensure they are in compliance with local, state, and federal regulations and with hospital accrediting agencies.
• Reviewing patient medical records and laboratory reports and recommending appropriate transmission-based isolation procedures.
• Screening patient records for community-acquired infections (those that are acquired outside of the health care setting). These infections often are distinguished from health care–associated infections by the type of organisms that affect patients who are recovering from a disease or injury.
• Consulting with occupational health departments concerning recommendations to prevent and control the spread of infection among health care personnel, such as testing for tuberculosis.
• Compiling data and analyzing the results regarding the epidemiology of health care–associated (or health care–acquired) infections.
• Notifying the local public health department of incidences of specific reportable communicable diseases.
• Conferring with various hospital departments and other resources to investigate unusual events or clusters of infection.
• Educating patients and families in the prevention and control of infection.
• Identifying infection control problems associated with medical or patient equipment.
• Assessing microorganism sensitivity to antibiotics presently in use and communicating with medical staff regarding current sensitivity and resistance patterns.
An infection control nurse is a valuable resource in the prevention and control of HAIs.
Occupational Health Service
The occupational health service plays an important role in the prevention or the control of an infection in a health care setting by taking measures to protect the health care worker and patients from certain infections. Federal law requires that health care employers make available the hepatitis B vaccine and vaccination series to all employees who have the risk for occupational exposure.
When any needle stick occurs, the health care worker must report it immediately. Hepatitis B, or serum hepatitis, is the most commonly transmitted infection from contaminated needles. Health care agencies require workers who have had a needle stick to complete an injury report and seek appropriate treatment (Box 7-4).
Many facilities mandate that all workers and students obtain titers as proof of immunity against varicella, measles, mumps, and rubella. Titers are laboratory tests that measure the amount of an antibody in the bloodstream. If the amount of the antibody is not high enough, the health care agency often requires personnel to receive a vaccination or be revaccinated to prevent the disease.
Standard Precautions
With the understanding that exposure to blood-borne pathogens (e.g., hepatitis B virus, HIV) can produce illness and infection came the realization that specific precautions can be used to help prevent infections.
The Centers for Disease Control and Prevention (CDC), part of the U.S. Department of Health and Human Services, provides facilities and services for investigation, prevention, and control of disease. The CDC has conducted studies on health care workers with documented skin or mucous membrane exposure to blood or body fluids of infected patients (Siegel et al., 2007). The studies show that infection is much more likely to occur when health care workers do not use appropriate protective measures.
Accurate identification of all patients infected with blood-borne pathogens is difficult. In the past, the CDC recommended that health care workers use “universal blood and body fluid precautions,” or “universal precautions,” and body substance isolation when caring for all patients. These two sets of precautions have now been incorporated into one standard set of guidelines, called standard precautions (Box 7-5).
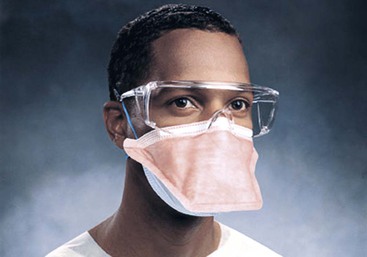
The increased incidence of tuberculosis (TB) has led to a heightened stress, along with these precautions, on wearing the particulate respirator mask (Figure 7-6) to protect against airborne pathogens.
The CDC guidelines for transmission-based precautions in hospitals, revised in 2007, have been adopted by many health care facilities (Siegel et al., 2007). The goal of these guidelines is to interrupt the chain of infection and reduce transmission of blood-borne pathogens and other potentially infectious materials. The guidelines apply to: (1) blood; (2) all body fluids, secretions, and excretions except sweat, regardless of whether or not they contain visible blood; (3) nonintact skin; and (4) mucous membranes. Standard precautions are designed to reduce the risk of transmission of microorganisms from both recognized and unrecognized sources of infections.
These precautions promote hand hygiene and use of gloves, masks, eye protection, and gowns when appropriate for patient contact.
Hand Hygiene
Hand hygiene is the single most important and basic preventive technique that health care workers can use to interrupt the infectious process. Box 7-6 indicates when initiation of hand hygiene is essential.
Performing hand hygiene (Skill 7-1) provides the necessary protection before the nurse cares for a patient. For effective cleansing of hands soiled with dirt or organic matter, or if the nurse has handled a contaminated item, soap or detergents that contain antiseptic and water are required. The standard is to wash for 15 to 30 seconds with facility-approved soap, running hands under warm water (very hot water increases the risk of drying and chapping the skin). Box 7-7 contains an overview of the CDC hand hygiene guidelines, and Box 7-8 addresses the use of alcohol-based waterless antiseptics for hand hygiene. All forms of health care–associated infections can result from improper hand hygiene and use of contaminated equipment.
Skill 7-1
Performing Hand Hygiene With Soap and Water








Nursing Action (Rationale)
1. Inspect hands, observing for visible soiling, breaks, or cuts in the skin and cuticles. (Poor personal hygiene and an open area of the skin provide areas in which microorganisms are able to grow.)
2. Determine amount of contaminant on hands. (Determines the type of hand hygiene needed.)
3. Assess areas around the skin that are contaminated. (Prevents contamination of hands during and after hand hygiene procedure.)
4. Adjust the water to appropriate temperature and force. (Water that is too hot can chap skin, and too much force causes splashing and may spread microorganisms to other areas, especially your clothing.)
5. Wet hands and wrists under the running water, always keeping hands lower than elbows. (Hands are the most contaminated part of the upper extremities; water should flow from the wrists [least contaminated area] over the hands, and then down the drain.)
6. Lather hands with liquid soap (about 1 teaspoon). (Soap lather emulsifies fat and aids in cleansing.)
7. Wash hands thoroughly with a firm, circular motion and friction on back of hands, palms, and wrists. Wash each finger individually, paying special attention to areas between fingers and knuckles by interlacing fingers and thumbs and moving hands back and forth, causing friction. (Helps to loosen soil and microorganisms, both resident [normally present] and transient [acquired from contamination].)

8. Wash for 15 to 30 seconds. (The greater the contamination, the more need for longer washing.)
9. Rinse wrists and hands completely, again keeping hands lower than elbows. (Water should run from cleaner area [the wrists] over the hands, and then down the drain, rinsing the dirt and microorganisms away.)

10. Dry hands thoroughly with paper towels. Start by patting at fingertips, then hands, and then wrists and forearms. (Prevents chapping. Drying should progress from clean to less clean, and the cleanest areas are now your fingers and hands.)
11. If it is necessary to turn off faucets manually, use a dry paper towel. (Keeps clean hands from touching contaminated handles.)
12. Use hospital-approved hand lotion if desired. (Keeps skin soft and lubricated so it does not crack easily.)
13. Inspect hands and nails for cleanliness. (Ensures cleanliness of hands and nails.)
14. If hands are not visibly soiled, use an alcohol-based waterless antiseptic for routine decontamination of hands in all clinical situations, unless you are caring for a patient with Clostridium difficile or Candida infection. The spores are unaffected by alcohol, so soap and water must be used in this instance (see Box 7-8).


15. Provide patient teaching (see Patient Teaching box on infection prevention and control).
16. Explain to the patient the importance of hand hygiene. (Helps the patient understand that hand hygiene slows down the spread of infection.)
17. If contamination occurs, it is necessary to reassess technique.
Box 7-7
Overview of CDC Hand Hygiene Guidelines
The Centers for Disease Control and Prevention (CDC) makes recommendations for hand hygiene in health care settings. Hand hygiene is a term that applies to hand washing, use of an antiseptic hand sanitizer, and surgical hand antisepsis. Evidence suggests that hand antisepsis, the cleansing of hands with an antiseptic hand sanitizer, is more effective in reducing health care–associated infections than is plain hand washing.
Follow These Guidelines in the Care of All Patients
• Continue practice of washing hands with either facility-approved soap or antimicrobial soap and water whenever hands are visibly soiled.
• Use an alcohol-based hand sanitizer to routinely decontaminate the hands in the following clinical situations: (Note: If alcohol-based hand sanitizers are not available, the only alternative is hand washing. See Skill 7-1, step 16.)
• Before and after patient contact.
• Before donning sterile gloves when inserting central intravascular catheters.
• Before performing nonsurgical invasive procedures (e.g., urinary catheter insertion, nasotracheal suctioning).
• After contact with body fluids or excretions, mucous membranes, nonintact skin, and wound dressings.
• If moving from a contaminated body site (rectal area or mouth) to a clean body site (surgical wound, urinary meatus) during patient care.
• After contact with inanimate objects (including medical equipment) in the immediate vicinity of the patient.
• Before eating and after using a restroom, wash hands with facility-approved soap and water.
• Antimicrobial-impregnated wipes (i.e., towelettes) are not a substitute for using an alcohol-based hand sanitizer or antimicrobial soap.
• If exposure to Bacillus anthracis is suspected or proven, wash hands with facility-approved soap and water. The physical action of washing and rinsing hands is recommended because alcohols, chlorhexidine, iodophors, and other antiseptic agents have poor activity against spores.
Follow These Guidelines for Surgical Hand Antisepsis (see Skill 7-6)
• Surgical hand antisepsis reduces the resident microbial count on the hands to a minimum.
• The CDC recommends using an antimicrobial soap to scrub hands and forearms for the length of time recommended by the manufacturer. Refer to agency policy for time required.
• When using an alcohol-based surgical hand-scrub product with persistent activity, follow the manufacturer instructions. Before applying the alcohol solution, prewash hands and forearms with a non-antimicrobial soap and dry hands and forearms completely. After application of the alcohol-based product as recommended, allow hands and forearms to dry thoroughly before donning sterile gloves.
General Recommendations for Hand Hygiene
• Use facility-approved hand lotions or creams to minimize the occurrence of irritant contact dermatitis associated with hand antisepsis or hand washing.
• Do not wear artificial fingernails or nail polish when having direct contact with patients at high risk (e.g., those in intensive care units or operating rooms).
• Keep natural nail tips less than  inch long.
inch long.
• Wear gloves when contact with blood or other potentially infectious materials, mucous membranes, and nonintact skin could occur.
• Remove gloves after caring for a patient. Do not wear the same pair of gloves for the care of more than one patient, and do not wash gloves between uses with different patients.
• Change gloves during patient care if moving from a contaminated body site to a clean body site.
Modified from Boyce JM, Pittet D: HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force and the CDC Healthcare Control Practices Advisory Committee draft guidelines for hand hygiene in healthcare settings. Infection Control and Hospital Epidemiology, 23(12 Suppl):S3-S40.
An increase in the wearing of artificial fingernails and nail polish has prompted several research studies. A series of regulatory agencies, including the CDC, The Joint Commission, and the Association of Perioperative Registered Nurses (AORN), has adopted position statements concerning their use. Only natural nails should be worn in the health care setting; these should be no longer than  inch. The use of artificial and acrylic nails should be avoided because of their potential status as carriers of harmful microorganisms.
inch. The use of artificial and acrylic nails should be avoided because of their potential status as carriers of harmful microorganisms.
In addition to hand hygiene, other actions can be taken to reduce the chance of transmitting microorganisms. The nurse should teach patients and visitors about appropriate times for hand hygiene (see Patient Teaching box on infection prevention and control). The nurse should provide patients with their own set of personal care articles, such as a bedpan, urinal, bath basin, water pitcher, and drinking glass, to prevent cross contamination. Because microorganisms are also transmitted by indirect contact with contaminated equipment and soiled linen, these articles should be placed in special waste containers or laundry bags. These items should be kept away from the nurse's uniform. The risk of transmitting health care–acquired infections or infectious diseases among patients is high when standard precautions are not followed. Health care workers need to stay informed about patients who have a known source of infection and communicate the information with other health care workers as appropriate. By following recommendations for infection prevention and control practices, health care workers experience more protection from exposure and reduce the patient's risk for acquiring a health care–associated infection.
 Patient Teaching
Patient Teaching
Infection Prevention and Control
• Teach the patient about the infection process, especially how an infection is transmitted, and stress the importance of interrupting the process. Use a simple diagram to illustrate this (see Figure 7-1). Teaching caregivers is extremely important as well.
• Use an example for each step that is familiar to the patient.
• Provide a simple explanation of clean as opposed to contaminated items.
• Although hand hygiene is a basic hygiene technique, emphasize when and how the procedure should be performed to be effective in preventing infection. Demonstrate hand hygiene within sight of the patient whenever possible.
• Instruct the patient about the signs and symptoms of infection.
• Teach the applications of aseptic principles to self-care activities, such as wound care and medication administration.
• When isolation apparel (such as mask, gown, or gloves) is to be used, demonstrate the procedures for the patient and visitors.
• Instruct the patient to place contaminated dressings and other disposable items that contain infectious body fluids in a leak-resistant bag. At home, needles should be placed in bleach bottles with the cap taped or glued on or placed in a sharps container and taken to a local hospital for disposal.
Always allow a question-and-answer session for the patient (some patients need special assistance in understanding the precautions).
 Gloving
Gloving
Nurses and other health care personnel should don gloves if any possibility exists of contact with infectious material with their hands. The CDC (Boyce and Pittet, 2002) gives the following advice regarding gloves:
• Wear gloves only once, and then place them into the appropriate waste containers for safe disposal.
• If you have not completed the patient's care but have come into contact with infectious material, change the gloves before continuing the patient's care.
• Because of the risk of perforating the gloves during use, perform hand hygiene after removing the gloves (Skill 7-2).
Skill 7-2
Gloving
Nursing Action (Rationale)
1. Remove gloves from dispenser. (Keeps gloves handy and ready for use.)
2. Inspect gloves for perforations. (Prevents pathogenic microorganisms from entering through perforation in gloves.)
3. Don gloves when ready to begin patient care. Wearing gloves with a gown does not necessitate any special technique for putting them on; wear them pulled over cuffs of gown. (Ensures full coverage of your wrists.)
4. Change gloves after direct handling of infectious material such as wound drainage. (Prevents cross contamination.)
5. Do not touch side rails, tables, or bed stands with contaminated gloves. (Prevents spread of microorganisms throughout environment.)
Removing Gloves
6. Remove first glove by grasping outer surface at palm with other gloved hand and pulling glove inside out and off. Place this glove in the hand that is still gloved. (Prevents you from touching your own skin with contaminated glove.)

7. Remove second glove by placing finger under cuff and turning glove inside out and over other glove. Drop gloves into waste container. (Prevents you from touching contaminated glove. Wraps contamination inside gloves to help protect others.)

8. Perform hand hygiene. (Helps prevent cross contamination.)
9. Provide patient teaching (see Patient Teaching box on gloving technique).
10. If contamination occurs, it is necessary to reassess technique.
Family members need to understand the importance of the use of gloves. Explain that gloves become contaminated if they touch infected material or a contaminated object (see Patient Teaching box on gloving technique).
Patient Teaching
Gloving Technique
• The nurse should ensure that the patient understands the rationale for the use of gloves.
• Some patients need special assistance in understanding the precautions.
The nurse should demonstrate to the patient how to don gloves.
Latex Allergy
Latex allergy causes an individual to have a reaction to certain proteins found in natural rubber latex, a product manufactured from a milky fluid derived from the rubber tree found in Africa and Southeast Asia. The latex proteins are able to enter the body through the skin and mucous membranes, intravascularly, and by inhalation. The nurse should suspect the presence of a latex allergy and obtain an evaluation by a physician when anyone has development of red, watery, itchy eyes; sinus or nasal congestion; tachycardia; or hypotension after exposure to latex. Anaphylaxis is a potentially life-threatening condition that can develop when someone is exposed to latex and has a severe latex allergy.
Some medical products contain latex. Synthetic versions of many products are available. Even though an individual product is “latex free,” an environment is “latex safe” only when all items of latex that have the potential to come in contact with the allergic individual are removed (Box 7-9).
Gowning
The nurse should don a gown when preparing to provide care for a patient in isolation to help protect the nurse's clothing from becoming soiled. The gown also provides protection against unknown infectious microorganisms. Recommendations are that the nurse discards the gown when leaving the patient's room rather than reuse it. This aids in preventing the spread of pathogens to other patients or personnel. This procedure also applies to visitors.
Another rationale for use of a gown is protection of a patient whose immune system is inadequate. In this situation, health care workers and visitors wear a gown to prevent the transfer of microorganisms from themselves to the patient.
There are several types of isolation. Some necessitate the wearing of a gown, whereas others do not. Donning of an isolation gown is indicated in the care of patients with diseases characterized by heavy drainage or exudate, infectious and acute diarrhea, other gastrointestinal disorders, respiratory disorders, skin wounds or burns, and urinary disorders.
Isolation gowns open at the back and have ties at the neck and the waist to keep the gown securely closed, protecting the back and the front of the nurse's uniform. The gown must be long enough to cover the uniform and, for added protection, have long sleeves with cuffs.
To don gowns correctly, follow the procedure listed in Skill 7-3.
Skill 7-3
Gowning for Isolation
Nursing Action (Rationale)
1. Push up long sleeves, if you have them. (Ensures that uniform sleeve is under gown sleeve for protection.)
2. Perform hand hygiene. (Reduces spread of microorganisms.)
3. Don gown and tie it securely at neck and waist. (Provides protective covering of the entire uniform.)

4. Remove gown after providing necessary patient care. (Has protected the nurse.)

5. Discard soiled gown appropriately. (Prevents contamination.)

6. Perform hand hygiene. (Prevents spread of microorganisms.)
7. Record use of gown in isolation procedure if required by the health care agency. (Provides proof that appropriate procedure was followed.) Some agencies charge a daily rate for isolation precautions. This is noted on a daily basis in the patient's record. Therefore, repeated notations throughout the 24 hours are not necessary.
8. Provide patient teaching (see Patient Teaching box on infection prevention and control).
9. If contamination occurs, it is necessary to reassess technique.
Step 3 figure from Potter PA, Perry AG: Fundamentals of nursing: Concepts, process, and practice, ed 8, St. Louis, 2013, Mosby. Steps 4 and 5 figures from Elkin MK, Perry AG, Potter PA: Nursing interventions and clinical skills, ed 4, St. Louis, 2008, Mosby.
Mask and Protective Eyewear
When a mask is correctly applied, it fits snugly below the health care worker's chin and securely over the nose and mouth; the top edge fits below eyeglasses, if worn (this prevents fogging of glasses). Masks are available with eye shields to cover the wearer's eyes (or glasses). Goggles are another possible way to protect eyes (see Figure 7-5, A). Nurses should change the mask at least every 20 to 30 minutes and when it becomes moist. Nurses should not reuse the mask or allow it to dangle around their neck and then reuse it (Skill 7-4). Masks and protective eye wear protect members of the health care team in the following ways:
• They protect the wearer from inhaling microorganisms that travel on airborne droplets for short distances or that remain suspended in the air for longer periods and from splashing if it should occur. Masks also prevent the mucous membranes of the nose and mouth from coming into contact with contaminants.
• They prevent the patient from inhaling pathogens if resistance is reduced or if a patient with an airborne respiratory infection is being transported to another care area.
• Eyewear shields protect the membranes and conjunctiva of the eye.
Skill 7-4
Donning a Mask
Nursing Action (Rationale)
The nurse should perform the following steps when donning a mask:
1. Remove mask from container. (Mask is readily available for use.)
2. Don mask when ready to begin patient care by covering your nose, mouth, and eyes (or glasses) with the device. Wear a mask with a protective eye shield when there is risk of splashing. Secure mask in place with elastic band or by tying the strings behind your head. (Provides protection from microorganisms.)

3. Wear mask until it becomes moist, but no longer than 20 to 30 minutes. (Moisture renders a mask ineffective.)
4. Remove mask by untying the strings or moving the elastic. Be certain not to touch contaminated area. (Prevents your coming into contact with contaminated mask.)

5. Dispose of soiled mask in appropriate container. (Protects other health care workers.)
6. Wash hands thoroughly. (Removes microorganisms.)
7. Record use of mask during patient care (some agencies require documentation of specific barriers used). (Provides proof of wearing mask for protection of patient and nurse.)
8. If contamination occurs, it is necessary to reassess technique.
9. Provide patient teaching (see Patient Teaching box on infection prevention and control).
Figures from Potter PA, Perry AG: Fundamentals of nursing: Concepts, process, and practice, ed 8, St Louis, 2013, Mosby.
Disposing of Contaminated Equipment
Health care facilities generate immense quantities of contaminated materials, some of which are disposable and some of which are reusable. It is essential to design and implement an effective mechanism to handle this material within the facility. The process for the disposal of contaminated materials is reviewed by the infection control nurse and the infection prevention and control committee. Some facilities manage the waste onsite, and other facilities rely on waste haulers to remove the waste. A major risk to health care workers and facility personnel is in the improper disposal of sharps (needles, scalpels), which are often contaminated by blood or bodily fluid. When left in linens, these sharp items have the potential to injure workers cleaning patient care areas. For prevention of this problem, all patient care areas in which sharps are ever used must be provided with puncture-proof containers into which health care workers place used disposable sharp items.
Handling Linen
The CDC recommends the following guidelines for handling linen:
Note that double bagging (placing a plastic bag that contains contaminated linen into another clean plastic bag) is no longer recommended as a universal practice, unless a cloth bag is being placed in a plastic bag. In most cases, a single bag is adequate if it is possible to place the contaminated articles in the bag without contamination of the outside of the bag.
Isolation Technique
The CDC issued isolation guidelines, in addition to standard precautions, that contain two tiers of approach (Siegel et al., 2007). The first tier contains precautions designed for health care workers to use when caring for all patients in health care facilities regardless of their diagnosis or presumed infectiousness. This first tier is called standard precautions.
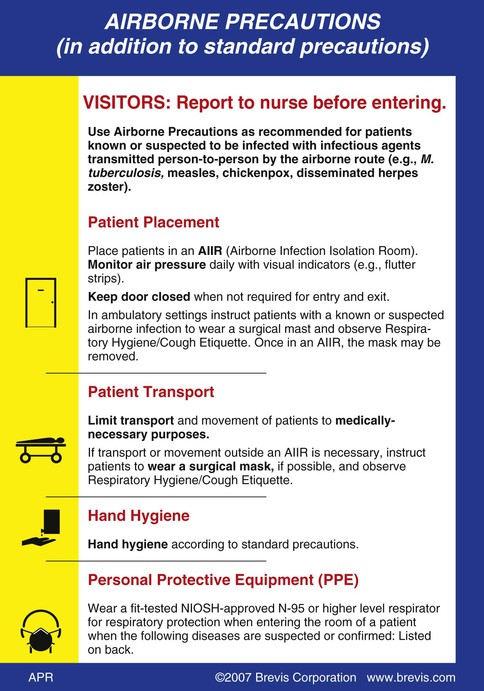
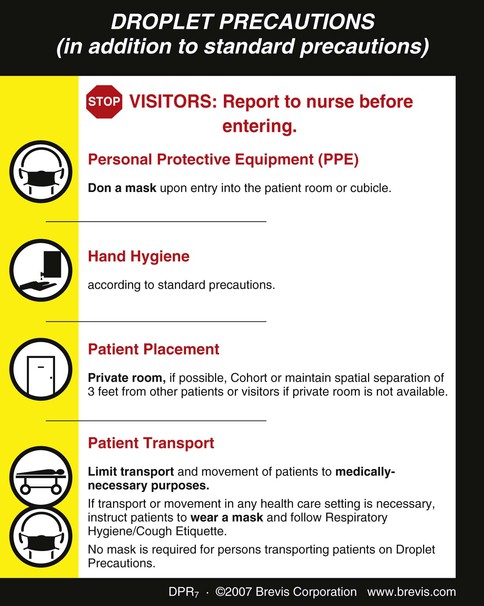
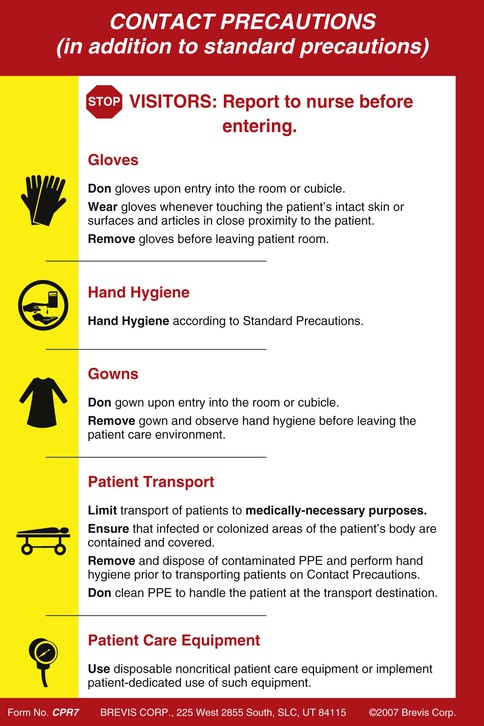
The second tier condenses the disease-specific approach to isolation into transmission categories: airborne, droplet, and contact precautions. These precautions are designed to be used in the care of patients with a specific type of confirmed or suspected infection (Box 7-10 and Figures 7-7 to 7-9).
The type of isolation techniques followed for a given patient depends on how transmissible the pathogen in question is. The nurse should follow some basic principles regardless of which technique is used:
• The nurse should perform thorough hand hygiene before and after caring for a patient.
• The nurse should have an adequate understanding of the disease process and the method of transmission of the infectious microorganism to help determine which protective barriers to use.
• The nurse should dispose of contaminated equipment and articles in a safe and effective manner to prevent transmission of pathogens to other individuals.
• If the patient is to be transported to other areas in the agency (away from the isolation room), the nurse should take necessary measures to protect those who will potentially be exposed. The patient should be transported in accordance with hospital protocol.
Environmental barriers keep pathogens in a confined area. Examples of such barriers are placing a patient in a private or isolation room, closing the patient's door, and wearing personal protective equipment (such as a gown, mask, goggles, and gloves).
The patient with an infectious disease should be placed in a private or isolation room equipped with the appropriate hand hygiene and toilet facilities. Private rooms used for airborne illness isolation have negative-pressure airflow that prevents infectious particulates from flowing out of the closed environment. Special rooms with positive-pressure airflow are also used for patients with immunocompromised conditions, such as transplant recipients or patients who are receiving certain kinds of chemotherapy. In this case, a reduced number of microorganisms are able to enter the room. All articles that come into contact with the patient are contaminated, and these items should be handled appropriately to help reduce the transmission of microorganisms. Dedicated equipment for assessment of vital signs remains in the room if possible. Otherwise it is mandatory for the health care worker to disinfect the equipment when it must be removed from the room to use on another patient.
The psychologic or emotional deprivation that may result with use of these transmission-based isolation precautions must be considered in the care of the patient. The patient is forced into solitude and deprived of normal social contacts. If possible, the nurse may wish to spend extra time with the patient to reduce feelings of isolation. Keep the room clean and pleasant. Provide instruction about the rationale for the precautions to the patient and family members. Teach the family and visitors how to apply and dispose of any personal protective equipment that they may need to wear and ensure that the procedure is followed (Skill 7-5).
Skill 7-5
Isolation Precautions
Nursing Action (Rationale)
1. Determine causative microorganism and patient's immune system status. (Determines virulence of causative pathogen and how well the patient's immune system is working.)
2. Recognize mode of transmission and how the microorganism may exit the body. (Determines the category or type of isolation to use.)
3. Follow agency policy for specific type of transmission-based precautions used. (Increases awareness of isolation categories available in the agency.)
4. Ensure that the environment has the equipment and supplies for the type of isolation:
a. Private or isolation room with anteroom. (Reduces spread of pathogens.)
b. Adequate hand hygiene facilities. (All workers and visitors are to perform hand hygiene before entering and leaving the area.)
c. Containers for trash, soiled linen, and sharp instruments (such as needles.) (Ensures safe disposal of contaminated articles.)
5. Provide explanation of isolation precautions to patient, family, and visitors. (Relieves apprehension and promotes cooperation of those involved.)
6. Post sign on door of patient's room or wall outside room stating the type of protective measures in use for patient care. (Informs personnel, patient, family, and visitors entering room of precautions to be followed and encourages cooperation.)
7. Be certain to supply the room with lined containers designated for soiled linens and for trash. (Prevents transmission of pathogens from seepage through container.)
8. Assess vital signs with designated equipment if possible, administer medications, administer hygiene, and collect specimens (Table 7-3). (Administers patient care.)
Table 7-3
Specimen Collection Techniques for the Patient in Isolation
| AMOUNT NEEDED* | COLLECTION DEVICE* | SPECIMEN COLLECTION AND TRANSFER |
| Wound (Culture) Specimen | ||
| As much as possible (after cleaning surface of skin or wound bed to remove flora or debris) | Sterile cotton-tipped swab or syringe | Clean site with sterile water or saline solution before wound specimen collection. Don gloves and place clean test tube or culturette tube on clean paper towel. After swabbing center of wound site, grasp collection tube by holding it with paper towel. Carefully insert swab without touching outside of tube. After removing gloves, washing hands, and securing tube's top, transfer labeled tube into bag for transport to laboratory. Document that procedure was performed. |
| Blood (Culture) Specimen | ||
| This specimen is usually obtained by the laboratory technician 10 mL per culture bottle, from two different venipuncture sites (volume may differ based on collection containers and age of patient) | Syringes, needles, and culture media bottles | Don gloves and perform venipuncture per hospital protocol at two different sites to decrease likelihood of both specimens being contaminated by skin flora. Inject 10 mL of blood into each bottle. Remove gloves and wash hands. Secure tops of bottles, label specimens, complete requisition, and send to laboratory. Document that procedure was performed. |
| Stool (Culture) Specimen | ||
| Small amount, approximately size of a walnut | Clean specimen cup with seal top (not necessary to be sterile) and sterile tongue blade | Don gloves and place cup on clean paper towel in patient's bathroom. With tongue blade, collect needed amount of feces from bedpan, not the toilet. Transfer feces to specimen cup without touching cup's outside surface; cover with lid provided. Remove gloves, wash hands, and place seal on cup. Repeat hand washing. Transfer specimen cup into clean bag for transport to laboratory after ensuring cup is correctly labeled. Document procedure was performed. |
| Urine (Culture) Specimen | ||
| 5-15 mL for adults | Syringe and sterile cup | Don gloves and place cup or tube on clean towel in patient's bathroom. Use alcohol swab pad, syringe, and needle to collect specimen if patient has Foley catheter. (All Foley catheters are equipped with needleless ports, which have to be cleaned per manufacturer guidelines; alcohol swabs are not sufficient.) Otherwise, have patient follow procedure to obtain clean-voided specimen (see Chapter 19). Transfer urine into sterile container by injecting urine from syringe or pouring it from container. Secure top of labeled container, remove gloves, and wash hands. Transfer labeled specimen into clean bag for transport to laboratory, after ensuring container is labeled correctly. Document procedure was completed. |
* Agency policies may differ on type of container. Ensure that all specimen containers used have the biohazard symbol on the outside and amount of specimen required and are bagged for transport to a laboratory.
From Pagana KD, Pagana TJ: Mosby's diagnostic and laboratory test reference, ed 7, St Louis, 2005, Mosby.
9. Report any changes in patient's health status to primary health care provider or supervisor. (Ensures continuity of care and helps determine patient progress.)
10. Record assessments and performance of transmission-based precautions. (Provides proof of appropriate patient care.) Document per agency policy.
11. Determine patient's understanding of activities in room. (Increases patient's comfort and feeling of well-being.)
12. Provide patient teaching (see Patient Teaching box on infection prevention and control).
13. Additional techniques for acid-fast bacillus (AFB) isolation (airborne precautions):
a. Before entering room, don N-95 respirator mask that you have undergone a fit-test for. (Reduces transmission of airborne droplet nuclei.)
b. Educate patient, family, and other visitors about how AFB is transmitted. (Improves ability of patient to participate in care. TB cannot be transmitted through contact with clothing, bedding, food, or eating utensils.)
c. Explain to patient that TB is transmitted by inhalation of droplets that remain suspended in the air when patient coughs, sneezes, or speaks (CDC, 2006). Offer opportunity for questions. (Improves ability of patient to participate in care.)
d. Instruct patient to cover mouth with tissue when coughing, educate patient about when to perform hand hygiene, and educate about the importance of wearing a regular disposable surgical mask while out of the room. (Reduces spread of droplet nuclei.)
e. Record assessments and performance of patient care. (Promotes continuity of care.)
Pulmonary Tuberculosis Precautions
Pulmonary tuberculosis (TB) infections continue to concern health care workers. Some strains of these bacteria are multidrug-resistant, which makes treatment of the infection very difficult. The best way to prevent the transmission of pulmonary TB is to quickly identify, isolate, and treat patients with TB. The nurse should suspect a patient has pulmonary TB if the patient has respiratory symptoms that last longer than 2 weeks. Other suspicious symptoms include fatigue, unexplained weight loss, dyspnea, fever, night sweats, and hemoptysis (a cough that can be productive of blood). Good assessment skills hasten the possibility of a diagnosis, which is essential because the risk of exposure is greatest before a diagnosis is made and isolation precautions are implemented. Isolation for patients with known or suspected TB includes a negative-pressure isolation room (see Box 7-10). Such rooms have negative pressure in relation to surrounding areas in the facility so that room air is exhausted directly to the outside or through special high-efficiency particulate air (HEPA) filters, if recirculation is unavoidable. High-risk procedures on patients with suspected or confirmed infectious TB must be performed in negative-pressure rooms.
OSHA and CDC guidelines require health care workers who care for patients with known or suspected TB to wear HEPA respirators (Jensen et al., 2005; U.S. Department of Labor, 2009). The respirators have the capacity to filter particles smaller than 5 µm in size with a filter efficiency of 95% or higher. The masks of health care employees who work with TB cases must undergo a fit-test to obtain a face-seal leakage of 10% or less. To ensure correct fit and efficiency, workers who experience a significant weight loss or weight gain should repeat the fitting process. Under National Institute for Occupational Safety and Health (NIOSH) criteria, the minimally acceptable level of respiratory protection for TB is the N-95 respirator (see Skill 7-5). Training in the wearing and storage of the respirator is required for hospital staff. OSHA also requires employers to provide training concerning transmission of TB, especially in areas where risk of exposure is high, such as areas where bronchoscopies are performed. Other requirements include annual TB skin testing for health care workers and appropriate follow-up when a previously negative skin test becomes positive.
Another option for health care workers who work around patients with known or suspected airborne infections such as TB is called a powered air purifying respirator (PAPR). A PAPR may be selected instead of an N-95 respirator if an N-95 respirator does not fit adequately. Facial hair and facial deformities may interfere with the face seal of an N-95. A PAPR may also be worn if an N-95 respirator is unavailable.
Surgical Asepsis
Surgical asepsis, or sterile technique, requires that the nurse use different precautions from those of medical asepsis. Surgical asepsis is the complete removal of all microorganisms, including spores, from an object. The nurse must understand that the slightest break in technique, when working with a sterile field or with sterile equipment, results in contamination. The nurse must practice surgical asepsis during the period of care to keep microorganisms away from the area.
Although surgical asepsis is practiced in the operating room, the labor and delivery area, and major diagnostic or procedure areas, the nurse also sometimes uses surgical aseptic techniques at the patient's bedside. This includes, for example, when the nurse inserts intravenous (IV) lines or urinary catheters, suctions the patient's lower airway, and applies sterile dressings. In an operating room, the nurse follows a series of steps to maintain sterile techniques, including donning a mask, protective eyewear, and a cap; performing surgical hand hygiene; and donning a sterile gown and gloves. In contrast, when the nurse is changing a dressing at a patient's bedside, the nurse often only performs hand hygiene, dons sterile gloves, and maintains a sterile area during the procedure.
Because surgical asepsis requires exact techniques, the nurse needs the patient's cooperation. For this reason, the nurse should prepare the patient before any procedure. Some patients may fear moving or touching objects during a sterile procedure, whereas other patients may try to assist. The nurse should explain how a procedure is to be performed and instruct the patient how to avoid contaminating sterile items, including the following measures:
• The patient should try not to make sudden movements of body parts covered by sterile drapes.
• The patient should refrain from touching sterile supplies, drapes, and the nurse's gloves and gown.
• The patient should avoid coughing, sneezing, or talking over a sterile area.
Principles of Sterile Technique
When beginning a surgically aseptic procedure, the nurse should follow the principles listed in Box 7-11 to ensure maintenance of surgical asepsis. Failure to follow each principle conscientiously endangers patients by placing them at risk for infection.
Assemble all the equipment necessary for a sterile procedure before the procedure begins. By doing so, the nurse avoids the need to leave a sterile area unattended to locate missing equipment or supplies. The nurse should have a few extra supplies available in case something accidentally becomes contaminated. If an object becomes contaminated during the procedure, it should be discarded immediately per facility policy.
Surgical Hand Scrub
In the operating room setting, effective hand washing or use of appropriate surgical hand rub to achieve surgical hand hygiene is imperative. To reduce patients' risk of postoperative infection, the nurses and other surgical personnel use an antimicrobial solution for hand hygiene as an integral part of the presurgical scrubbing procedure. Although sterilizing the skin is not possible the number of microorganisms can be greatly reduced by chemical, physical, and mechanical means.
The surgical hand scrub (Skill 7-6) is the traditional method for surgical asepsis. With the use of an antimicrobial agent and sterile brushes, the surgical hand scrub removes debris and transient microorganisms from the nails, the hands, and the forearms. This technique also reduces the resident microbial count to a minimum and inhibits rapid or rebound growth of microorganisms. Use of an alcohol-based surgical hand rub is also acceptable as long it has met U.S. Food and Drug Administration requirements to be used for this purpose. Both hand antiseptic methods are currently used in operating room settings. Skill 7-6 addresses both techniques. Surgical personnel wear surgical attire (i.e., scrubs) in the operating room to reduce the chance for contamination from themselves to patients and vice versa. Fingernails should be short, clean, and natural. The nurse must not wear artificial nails. Artificial nails harbor microorganisms and fungus. The nurse should remove all rings, watches, and bracelets before the surgical scrub and while assisting with procedures that require surgical asepsis.
Skill 7-6
Surgical Hand Hygiene
Nursing Action (Rationale)
1. Inspect hands for presence of abrasions, cuts, or open lesions. (These conditions increase likelihood of more microorganisms residing on skin surfaces.)
2. Apply surgical shoe covers, cap or hood, face mask, and protective eyewear. (Mask prevents escape into air of microorganisms that can contaminate hands. Other protective wear prevents exposure to blood and body fluid splashes during the procedure.)
3. Perform surgical hand hygiene (traditional method):
a. Turn on water using knee or foot controls and adjust to comfortable temperature.
b. Wet hands and arms under running lukewarm water and lather with detergent to 5 cm (2 inches) above elbows. (Keep hands above elbows at all times.) (Hands become cleanest part of upper extremity. Keeping hands elevated allows water to flow from least to most contaminated areas because water runs by gravity from fingertips to elbows. Washing a wide area reduces risk of contaminating gown that you will don later.)
c. Rinse hands and arms thoroughly under running water. Remember to keep hands above elbows. (Rinsing removes transient microorganisms from fingers, hands, and forearms.)
d. Under running water, clean under nails of both hands with nail pick. Discard after use. (Removes dirt and organic material that harbor large numbers of microorganisms.)

e. (1)Wet clean sponge and apply antimicrobial detergent. Scrub nails of one hand with 15 strokes. Holding sponge perpendicular to hand, scrub palm, each side of thumb and fingers, and posterior side of hand with 10 strokes each.

(2) Mentally divide your arm into thirds, and scrub each third 10 times. Entire scrub should last 5 to 10 minutes. Rinse sponge and repeat sequence for other arm. It is permitted to substitute with a two-sponge method. Check agency policy. (Friction loosens resident bacteria that adhere to skin surfaces. Ensures coverage of all surfaces. Scrubbing is performed from cleanest area [hands] to marginal area [upper arms.])

f. Discard sponge and rinse hands and arms thoroughly. Turn off water with foot or knee control and back into room entrance with hands elevated in front of and away from the body. (After touching skin, consider sponge contaminated. Rinsing removes resident bacteria. Prevents accidental contamination.)

g. (1) Walk up to sterile tray and lean forward slightly to pick up a sterile towel.

(2) Dry one hand thoroughly, moving in sequence from fingers to elbow. Dry in a rotating motion. Dry from cleanest to least clean area. (Drying prevents chapping and facilitates donning of gloves. Leaning forward prevents accidental contact of arms with scrub attire.)

h. Repeat drying method for other hand by carefully reversing towel or using a new sterile towel. (Prevents accidental contamination.)
i. Discard towel. (Prevents accidental contamination.)
j. Proceed with sterile gowning.
4. Alternate method of surgical hand hygiene using alcohol-based antiseptic:
a. Wash hands with soap and water for 15 to 30 seconds to remove soil. (Removes dirt and organic material that harbor large numbers of microorganisms.)
b. Under running water, clean under nails of both hands with nail pick. Discard after use and dry hands with a paper towel. (Removes dirt and organic material that harbor large numbers of microorganisms.)
c. Apply enough alcohol-based waterless antiseptic to one palm to cover both hands thoroughly. Spread the antiseptic over all surfaces of the hands and the fingernails. Follow product instructions for length of time to rub over hand surfaces. Allow to air-dry. (Ensures coverage of all surfaces. Air-drying ensures complete antisepsis.)
d. Repeat the process and allow hands to air-dry before applying sterile gloves.
Figures from Potter PA, Perry AG: Fundamentals of nursing: Concepts, process, and practice, ed 8, St Louis, 2013, Mosby.
The Association of Perioperative Registered Nurses (AORN, 2013) has a revised set of policies and procedures; also, refer to agency policy on surgical hand hygiene (see Chapter 41).
Managing Sterile Packages
Sterile items such as syringes, gauze dressings, and catheters are packaged in paper or plastic containers that are impervious to (unable to be penetrated by) microorganisms as long as the items remain dry and intact. Paper packages are permeable to steam and thus allow for steam autoclaving. A disadvantage of paper wrappers is that they tear or puncture relatively easily. Sterile items should be placed in clean enclosed storage cabinets and never kept in the same room as dirty equipment.
Sterile supplies have dated labels or chemical tapes that indicate the date when the sterilization expires. The tapes change color during the sterilization process. Failure of the tapes to change color means the item is not sterile. Never use or allow use of a sterile item or piece of equipment after the expiration date. Some agencies use the “event-related” contamination rule. If the integrity of the sterile package is questionable (i.e., wet, torn, discolored), the item is discarded or resterilized per policy. If the nurse finds moisture present after a sterile tray is opened, the item is either discarded or returned to the institution's supply area for resterilization.
Before the nurse opens a sterile item, thorough hand hygiene is performed. The supplies are assembled at the work area, such as the bedside table or in the treatment room, before packages are opened. A bedside table or countertop provides a large, clean working area for opening of items. The nurse should ensure that the work area is above the nurse's waist level. Sterile supplies should not be opened in a space where a dirty object may fall on or come into contact with them.
Sterile packaged items can be opened without contamination of the contents even when the nurse is not wearing sterile gloves. Commercially packaged items are usually designed so that the nurse only has to tear away or separate the paper or plastic cover from the rest of the tray or kit. The nurse holds the item in one hand while pulling the wrapper with the other (Figure 7-10). The nurse should be careful after opening to keep the inner contents sterile before use. When opening items packed in linen and some commercially prepackaged items, use the steps described in Box 7-12 and illustrated in Figure 7-10 and Figure 7-11.


Preparing a Sterile Field
When performing sterile procedures, the nurse needs a sterile work area that provides room for handling and placing sterile items. A sterile field is an area that is free of microorganisms and has been prepared to receive sterile items. The nurse should prepare the field by using the inner surface of a sterile wrapper as the work surface or by using a sterile drape (Skill 7-7).
Skill 7-7
Preparing a Sterile Field
Nursing Action (Rationale)
1. Prepare sterile field just before planned procedure. (Prevents exposure of sterile field and supplies to air contamination.) Be sure to use supplies immediately.
2. Select clean work surface that is above waist level. (Consider sterile objects held below waist contaminated.)
3. Assemble necessary equipment. (Preparing equipment in advance prevents breaks in technique.)
4. Check dates, labels, and condition of package for sterility of equipment. (Consider equipment stored beyond expiration date, or a package that is damaged, unsterile.)
5. Wash hands thoroughly. (Prevents spread of microorganisms.)
6. Place package containing sterile drape on work surface and open. (Ensures sterility of packaged drape.)
7. With fingertips of one hand, pick up folded top edge of sterile drape. (Up to the 1-inch border around drape is unsterile and permitted to be touched.)
8. Gently lift drape up from its outer cover and let it unfold by itself without touching any object. Discard outer cover with your other hand. (If sterile object touches any unsterile object, it becomes contaminated.)
9. With other hand, grasp adjacent corner of drape and hold the entire edge straight up and away from your body. Now, properly place drape while using two hands and being sure to keep the drape away from unsterile surfaces. (Prevents contamination.)
a. Holding drape, first position the bottom half over intended work surface. (Prevents from reaching over sterile field.)
b. Allow top half of drape to be placed over work surface last. (Creates a flat, sterile work surface.)
10. Perform procedure using sterile technique. (Prevents contamination.)
Sometimes the nurse chooses to wear sterile gloves while preparing items on the field. The nurse is then able to touch the entire drape, but an assistant has to open and pass sterile items to the nurse unless the nurse applies new sterile gloves to prevent contamination of the sterile items. The nurse should not allow the gloves to touch the outside wrappers of the package that contains the sterile items.
Pouring Sterile Solutions
The nurse may be required to pour sterile solutions into sterile containers. A bottle that contains a sterile solution is sterile on the inside and contaminated on the outside. The bottle's neck is also contaminated, but the inside of the bottle cap is sterile. After opening a cap or lid, the nurse can hold it in the hand or place it, sterile side (inside) up, on a clean surface. Thus, the nurse can see the inside of the lid as it rests on the table surface. The nurse can never allow a bottle's cap or lid to rest sterile side down on a sterile surface because the cap's outer edge is unsterile and will contaminate the surface. Likewise, placement of a sterile cap down on an unsterile surface increases the chances of the inside of the cap becoming contaminated.
The nurse should hold the bottle with its label in the palm of the hand to prevent the solution from wetting the label. If the solution is allowed to wet the label, it may cause it to fade and reduce its legibility. The nurse should keep the edge of the bottle from touching the edge or the inside of the receiving container, which is unsterile. The solution should be poured slowly to avoid splashing the underlying drape or field. The bottle should never be held so high above the recipient container that even slow pouring causes splashing. The bottle should be held over the outside of the edge of the sterile field (Figure 7-12).

Donning a Sterile Gown
A nurse must don a sterile gown (Skill 7-8) before working in the operating room and before assisting with certain sterile procedures or working in special treatment areas. The sterile gown decreases the risk of contaminating sterile objects when the nurse handles them. In addition, the sterile gown prevents contamination of sterile objects or sterile fields by microorganisms shed from the nurse's skin (Potter and Perry, 2007).
Skill 7-8
Donning a Sterile Gown
Nursing Action (Rationale)
The nurse should perform the following steps when applying a sterile gown:
1. Don surgical cap, shoe covers, protective eyewear, and mask, and then perform surgical hand hygiene. (Prevents contamination of the surgical field and protects the nurse from blood and body fluid exposure.)
2. Ask the circulating nurse to open the sterile gown package and the sterile glove package. (Prevents contamination of the hands after the surgical hand wash because the outer wraps are not sterile.)
a. If available, the scrub nurse assists by pulling the gown over your extended hands and arms. If no assistance from a scrub nurse is available:
(1) Pick up the gown touching only the inner surface below the neck. (Touching the outer, sterile surface causes the gown to become contaminated because the hands are not yet gloved and thus unsterile.)
(2) Maintain constant control of the folded layers of the gown. (Prevents the gown from brushing against unsterile surfaces.)
(3) While holding the gown at arm's length, allow the gown to unfold from top to bottom. Be sure that the gown does not touch the floor. (Prevents contamination.)

(4) While holding the inside of the gown near the shoulders and below the neckband, slide hands and arms into the sleeves with your fingers stopping at the end of the cuffs. (The fingers remain inside the sleeves in order to don the sterile gloves by means of closed gloving.)

(5) Ask another staff member to grasp the cord that is attached to the ties of the gown to draw the ties around to the back with the gown overlapping itself. The staff member should now tie the gown, avoiding touching any part of the gown except the ties. (Do not allow the front or the sides of the gown to be touched by the staff member because these areas are sterile.)
Figures from Elkin MK, Perry AG, Potter PA: Nursing interventions and clinical skills, ed 4, St. Louis, 2008, Mosby.
Donning Sterile Gloves
Sterile gloves are an additional barrier used to prevent the transmission of microorganisms. The two methods of donning gloves are open (Skill 7-9) and closed (Figure 7-13). Nurses who work on general nursing divisions use open gloving before procedures such as dressing changes or urinary catheter insertions. Nurses should use the closed gloving method when donning a sterile gown before procedures in the operating room and special treatment areas.
Skill 7-9
Performing Open Sterile Gloving
Nursing Action (Rationale)
1. Have package of properly sized sterile gloves at treatment area. (Facilitates procedure.)
2. Perform thorough hand hygiene. (Removes bacteria from skin surfaces.)
3. Remove outer glove package wrapper by carefully separating and peeling apart sides. (Prevents inner glove package from accidentally opening and touching contaminated objects.)

4. Grasping inner side of package, lay package on clean flat surface just above waist level. Open package, keeping gloves on wrapper's inside surface. (Inner surface of glove package is sterile. Sterile objects held below the waist are considered contaminated.)

5. Identify right and left gloves. Each glove has a cuff approximately 2 inches (5 cm) deep. (Proper identification of gloves prevents contamination by improper fit.)
6. Glove dominant hand first. With thumb and first two fingers of nondominant hand, grasp edge of cuff of glove for dominant hand. Touch only glove's inside surface. (Gloving of dominant hand first improves dexterity. Touching inside surface is permitted because inner edge of cuff will lie against skin. If glove's outer surface touches hand or wrist, it is contaminated.)

7. Carefully pull glove over dominant hand, leaving cuff; be sure cuff does not roll up wrist. Be sure thumb and fingers are in proper spaces. (If glove's outer surface touches hand or wrist, it is contaminated.)

8. With gloved dominant hand, slip fingers underneath second glove's cuff in such fashion that the cuff will protect the gloved fingers. (Sterile touching sterile prevents glove contamination.)

9. Carefully pull second glove over nondominant hand. Do not allow fingers and thumb of gloved dominant hand to touch any part of exposed nondominant hand. Keep thumb of dominant hand abducted back. (Contact of gloved hand with exposed hand results in contamination.)

10. After second glove is on, interlock hands. Be sure to touch only sterile sides. The cuffs usually fall down after application. (Ensures smooth fit over fingers.)

Glove Removal and Disposal
11. Grasp outside of one cuff with other gloved hand; avoid touching wrist. (Minimizes contamination of underlying skin.)

12. Pull glove off, turning it inside out. Discard in receptacle. (The outside of glove does not touch skin surface.)

13. Take fingers of bare hand and tuck inside remaining glove cuff. Peel glove off, inside out. Discard in receptacle. (Reduces spread of microorganisms.)

Steps 3, 4, 6-9 figures from Elkin MK, Perry AG, Potter PA: Nursing interventions and clinical skills, ed 4, St. Louis, 2008, Mosby. Step 10 figure from Potter PA, Perry AG: Fundamentals of nursing: Concepts, process, and practice, ed 7, St. Louis, 2009, Mosby.
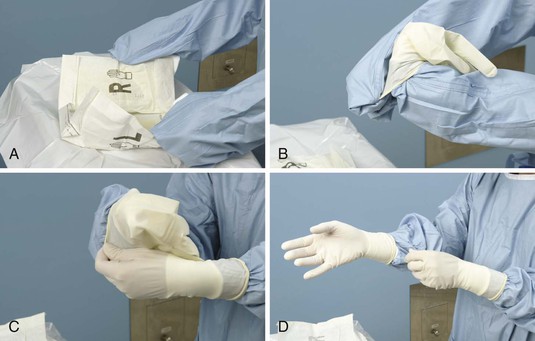
The nurse should select the proper glove size. The glove must be snug enough for the nurse to pick up things easily and yet not so tightly stretched that it tears easily.
Closed Gloving
Closed gloving is practiced when the nurse also needs to wear a sterile gown. With closed gloving, contamination of the sterile gown is prevented. The wearer of a sterile gown and sterile gloves can now safely handle sterile materials and instruments during surgery or other types of sterile procedures.
Cleaning, Disinfection, and Sterilization
Microorganisms are present on items in the home and public areas, including health care agencies. By following basic clean or aseptic technique, the nurse is able to help interrupt the spread of infection. Antiseptics are a means to inhibit the growth of microorganisms, although killing them this way is not possible. Antiseptics are also referred to as bacteriostatic solutions. Bacterio- means “microorganism,” and static means “referring to that which cannot move or grow.” Use of antiseptics (like alcohol or chlorhexidine gluconate) on human tissue is acceptable and is often performed before sterile procedures like surgery and during wound care. Antiseptics can be used for mouth care and when performing hand hygiene.
Cleaning
Cleaning is the removal of foreign materials, such as soil and organic material, from objects. Generally, cleaning involves use of water and mechanical action with or without detergents.
When an object comes in contact with potentially infectious material, the object is contaminated. If the object is disposable, it is discarded per facility policy. Reusable objects must be thoroughly cleaned and then either disinfected or sterilized before reuse, per facility policy.
When cleaning equipment that is soiled by organic material such as blood, fecal matter, mucus, or pus, the nurse should put on a mask and protective eyewear or goggles (or a face shield), a fluid-resistant gown, and waterproof gloves. These barriers provide protection from infectious organisms (as discussed previously). The nurse needs a stiff-bristled brush and detergent or soap for cleaning.
Perform the following steps when cleaning equipment:
1. Rinse a contaminated object or article with cold running water to remove organic material. Hot water causes the protein in organic material to coagulate and stick to objects, making removal difficult.
2. After rinsing, wash the object with soap and warm water. Soap or detergent reduces the surface tension of water and emulsifies dirt and remaining material. Rinse the object thoroughly to remove the emulsified dirt.
3. Use a brush to remove dirt or material present in the equipment's grooves or seams. Friction dislodges contaminated material for easy removal. Open any hinged items for cleaning.
4. Rinse the object in warm water.
5. Dry the object and prepare it for disinfection or sterilization if indicated by the intended use of the item.
6. The brush, the gloves, and the sink in which the equipment is cleaned are considered contaminated and must be cleaned and dried per facility policy.
Disinfection
Disinfection is used to destroy microorganisms. However, it does not destroy spores. The solutions used during disinfection are called disinfectants, or possibly bactericidal solutions (the suffix -cidal is derived from a Latin word meaning “to kill”). These solutions are too strong to use on human skin and are appropriate to use on inanimate objects. If a disinfectant solution comes in contact with human tissue, the tissue may feel “slippery.” This is the first step of tissue breakdown. When using a disinfectant, the nurse should use clean gloves to protect the skin (Skill 7-10).
Skill 7-10
Preparing for Disinfection and Sterilization
Nursing Action (Rationale)
1. Prepare equipment and supplies. (Ensures organization of procedure.)
• Disinfectant to use for cleansing. (Aids in appropriate care of equipment and reusable supplies.)
• Method of sterilization. (Ensures that appropriate method is used.)
• Gloves. (Protects you from contamination.)
• Running water. (Aids in cleansing and rinsing of articles.)
• Scrub brush. (Aids in cleansing grooves.)
• Cloth wrapper. (Provides the means for wrapping articles that require sterilization.)
2. Don gloves. (Protects you from contamination.)
3. Rinse article under cool running water. (Emulsifies or softens soil for removal.)
4. Wash article with detergent. (Emulsifies or softens dirt for easy removal.)
5. Use scrub brush to remove material in grooves. (Friction loosens material in corners and grooves.)
6. Dry article thoroughly. (Prevents the growth of microorganisms.)
7. Prepare article for sterilization by wrapping it in cloth wrapper. (Promotes appropriate sterilization of the article.)
8. Clean work area and put in order. (Prevents the spread of microorganisms.)
9. Perform patient teaching (see Patient Teaching box on disinfection and sterilization at home).
Sterilization
Sterilization refers to methods used to kill all microorganisms, including spores. The two types of sterilization methods are physical and chemical (Box 7-13).
Most health agencies have a central supply department that disinfects and sterilizes reusable equipment and supplies. Although most supplies used today for patient care are disposable, some supplies and equipment still require the use of disinfection and sterilization. The patient and family members should be taught the principles of cleansing and disinfecting in the home environment (see Patient Teaching box on disinfection and sterilization).
There are two accepted methods of disinfection and sterilization (see Box 7-13). One is a physical process that uses heat or radiation; the second process uses chemicals. Both methods destroy microorganisms. The method used depends on the following factors: (1) the type of microorganisms present (spore-forming bacteria are resistant to destruction); (2) how many microorganisms may be present (it takes longer to kill a large number); and (3) the type of item that needs to be disinfected and sterilized (some materials are so sensitive that heat or certain chemicals destroy them). Other determinants of the sterilization method used are: (1) the intended use for the article (e.g., surgery requires that all organisms be destroyed, whereas medical asepsis consists of techniques that inhibit the growth and transmission of pathogenic microorganisms); and (2) the methods of sterilization available.
Liquid and gaseous chemicals are used to sterilize and disinfect equipment. Examples may include iodine, alcohol, dialdehyde, and chlorine bleach compounds. Chlorine bleach is useful for household disinfection and disinfection of water, but it must never be mixed with ammonia because of the resulting emission of toxic fumes. Chlorine bleach has a tendency to corrode some metals. Iodine is a good bactericidal agent (i.e., it kills bacteria but not spores). Iodine leaves behind stains and is not used as widely as it was previously.
Patient Teaching for Infection Prevention and Control
Patients and families often have to learn to use infection prevention and control practices at home. Aseptic technique becomes almost second nature to the nurse, who practices it daily. However, the patient is less aware of the factors that promote the spread of infection and of the ways to prevent its transmission. The nurse should educate patients about the nature of infection and the techniques to use in planning or controlling its spread (see Life Span Considerations for Older Adults and Cultural Considerations boxes regarding infection control).
 Life Span Considerations
Life Span Considerations
Older Adults
Infection Prevention and Control
• The older adult experiences an alteration in integrity of the oral mucosa. Promote careful oral hygiene and emphasize the importance of routine dental care.
• The older adult experiences a decrease in the production of digestive acid. Teach the older patient to carefully wash hands before food preparation, to adequately cook foods, and to refrigerate unused portions promptly.
• The dermal and epidermal skin layers of the older adult become thinner, and elasticity is decreased. Turn the bedridden patient frequently, and carefully observe the skin for impairment.
• The older adult may experience urethral stricture, neurogenic bladder, and prostatic enlargement (in males). In the older patient with an indwelling Foley catheter, assess for adequate drainage and maintain cleanliness of the urethra and the perineal area.
Older adults experience a decrease in ribcage movement during inspiration. In caring for older adults after surgery, elevate the head of the bed (if indicated) and encourage the patient to cough and breathe deeply and to get out of bed as soon as possible to prevent postoperative complications such as pneumonia.
 Cultural Considerations
Cultural Considerations
Infection Prevention and Control
• Cultural heritage affects all dimensions of health. The patient's cultural background must be considered when educating a patient about infection prevention and control measures.
• The way that culture influences behaviors, attitudes, and values depends on many factors and is often not the same for every member of a cultural group.
• Clean water may be a difficult commodity for many Alaskan Eskimos to obtain reliably. In some villages near the ocean, drinking water is brought in as ice from several miles upriver. In this process, the chunks of ice destined for human consumption are often handled by many people and must be melted, boiled, and cooled.
• Some Japanese Americans have a traditional belief that disease is caused by contact with contaminated agents such as blood, corpses, and skin diseases.
• The germ theory can be confusing to individuals with animistic beliefs (a belief in the existence of spirits and demons). They may believe that the supernatural or spirit world causes disease.
• Observant Jews have customs that promote good hygiene or have been proven to be medically sound practices, such as washing the hands on awakening from sleep, after elimination of body wastes, after hair cutting, after touching vermin (insects and small animals), after being close to a dead body, and before eating or drinking.
• In Cajun culture, people may trust faith healers and be less likely to take preventive health measures.
Infection Prevention and Control for Home and Hospice Settings
Patients are now commonly discharged from acute care to their homes faster than in the past. Thus, they often require care from home health personnel. An infection that develops within 30 days after discharge, such as a wound infection at an operative site, may be an outcome of hospitalization, and the acute care facility's infection control department needs to receive a report. As more patients elect to die at home, care for the dying will make similar care and reporting measures necessary more often. The epidemiologic (pertaining to the study of the occurrence, distribution, and causes of disease in humankind) basis of infections that develop in homes is sometimes related to the diseases that affect a community. The patient may have development of influenza, an enteric infection, or a streptococcal pharyngitis as it passes through the community.
As home care and hospice programs continue to expand, questions emerge about infection prevention and control in these settings. The reliability of hospital infection rates depends directly on accurate identification of the source of infection. Such accuracy tends to be problematic when rapid hospital discharges leave the source of an infection unclear. Hospitalized patients need to receive education and instruction at discharge about reporting the occurrence of any signs and symptoms of infection such as pain, erythema (redness), edema (swelling), drainage or exudate, and fever to the appropriate acute care personnel after discharge (Health Promotion box).
 Health Promotion
Health Promotion
Prevention of Infection in the Home Setting
The basic principles of hygiene are bathing; not sharing personal articles such as combs, toothbrushes, razors, and washcloths; and covering one's mouth when coughing and sneezing. These practices are important to help prevent the spread of infection in the home setting. Patient education about the risk of spreading microorganisms responsible for hospital-acquired infections to family or friends is important, especially when family members are assisting at home in changing dressings or managing hygiene for patients with incontinence.
The licensed practical/vocational nurse (LPN/ LVN) helps educate patients and family members about the following activities:
• Hand hygiene. Wash hands after using the bathroom, after contact with any secretions, before eating, and before and after patient care. Use warm water, soap, and friction for 15 to 30 seconds, and dry hands thoroughly.
• Food preparation. Do not allow any person with an infectious gastrointestinal disease to prepare food until symptoms resolve. Do not thaw and then refreeze foods. Be sure cooked foods are stored immediately in clean containers in the refrigerator. Wash hands before food preparation. Using a dishwasher or washing dishes in hot soapy water decreases the risk of contamination.
• Tube feedings. Prepare enough formula for only 8 hours (commercially prepared) or 4 hours (home prepared). Contaminated enteral feeding may cause infections in patients (e.g., Salmonella or staphylococcal infections). The feeding bag and tubing should be cleansed or replaced per manufacturer recommendations.
• Linens. Wash linens that are contaminated with blood or body fluids separately in hot, soapy water with 1 cup of bleach per load, and dry them in a dryer on the hot cycle.
• Waste containers. Keep waste containers available in the patient contact area for the disposal of dressings, diapers, tissues, and other disposable items. Place a sturdy bag inside the waste container to prevent spilling and leakage. Flush body fluids such as urine, vomitus, feces, and blood down the toilet.
• Body fluid spills. Clean up any accidental body fluid spill as soon as possible, while wearing gloves. To disinfect, spray a solution of 1 cup of bleach diluted with 10 cups of water over the spill, and clean up with paper towels. Then, place the paper towels in the plastic-lined waste container.
 Nursing Process
Nursing Process
The role of the licensed LPN/LVN in the nursing process as stated is that the LPN/LVN:
• Participates in planning care for patients based on patient needs
• Reviews patient's plan of care and recommends revisions as needed
• Reviews and follows defined prioritization for patient care
• Uses clinical pathways, care maps, or care plans to guide and review patient care
 Assessment
Assessment
By evaluating signs and symptoms revealed during assessment, the nurse is able to determine whether a patient's clinical condition indicates a risk for infection. Early recognition of infection helps the nurse make a correct nursing diagnosis and thus establish an appropriate treatment plan. Also, the nurse should consider how well the patient is dealing with the disease and whether any resources could benefit the patient. It is important to include the patients: how does the infection affect them?
Prompt assessment of laboratory will provide information about potential infections. Laboratory values such as increased white blood cell count or a positive blood culture often indicate infection. In assessment of laboratory data, the nurse should consider the age of the patient. For example, in the older adult, smaller amounts of bacteria such as Salmonella have the potential to cause gastrointestinal infections because of the decrease in bactericidal gastric acids and deterioration of the mucosal layer of the stomach.
Sometimes positive laboratory results indicate the need to use transmission-based isolation precautions. In this case, the nurse should consult the infection control nurse or refer to the facility's infection prevention and control policy manual.
Nursing Diagnosis
The selection of a nursing diagnosis is based on data collected during the assessment. Possible nursing diagnoses for patients susceptible to or affected by an infection include the following:
• Risk for infection (Nursing Care Plan 7-1)
 Nursing Care Plan 7-1
Nursing Care Plan 7-1
The Patient With an Infection
This care plan has been created for the patient who is at risk for infection. Mr. R. is a 68-year-old man in the nursing unit for 8-hour postoperative care after a bowel resection. He has intravenous fluids infusing and a urethral catheter in place.
Nursing Diagnosis
Risk for infection, related to presence of abdominal incision, intravenous devices, age, presence of indwelling catheter

Critical Thinking Questions
1. Mr. R. has a peripheral IV infusing and reports discomfort at the site of insertion. What should the nurse do?
2. Mr. R. has a urinary catheter connected to continuous drainage. He reports burning at the site of insertion, and the nurse notes dark, concentrated urine in the tubing. What should the nurse do next?
3. The nurse notes on the sheet of laboratory results for the patient that his WBC count is 10,000/mm3. Why is this a concern, and what is recommended as a precautionary measure?
Expected Outcomes and Planning
The plan of care focuses on achieving specific goals and outcomes related to the nursing diagnoses chosen. Interventions are determined with the aid of the patient, the family, the physician, and other members of the health care team. These goals and outcomes possibly include the following:
Implementation
The nurse's role is to prevent the onset and spread of infection and promote healing. By recognizing and assessing a patient's risk factors and implementing appropriate measures, the nurse has the capacity to help reduce the risk of transmitting infections. The nurse should use good hand hygiene techniques, properly use sterile supplies, and wear appropriate personal protective equipment, as indicated.
Evaluation
The success of the nurse who practices infection prevention and control techniques is measured according to the extent to which the goals are achieved for reducing or preventing infection. Evaluation is by nature ongoing because a patient's condition can change at any time. The nurse is then in a position to decide to continue nursing interventions, revise them as necessary, or determine that the problem has been resolved. This is accomplished by referring to the goals and outcomes identified when planning care.
Goal 1: Transmission of infectious organisms is controlled.
Evaluative measures: Assess patient's temperature; observe wound sites for erythema, edema, tenderness, or exudate.
Goal 2: Progression of infection is controlled or decreased.
Evaluative measures: Inspect size of inflamed area over consecutive intervals; gently palpate involved site to note reduction in tenderness.
See the Coordinated Care box for infection prevention and control procedures.
 Coordinated Care
Coordinated Care
Delegation
Infection Prevention and Control
Hand hygiene or antisepsis involves a set of basic procedures that all caregivers are obliged to perform correctly. If the nurse observes other caregivers or family caregivers cleanse their hands incorrectly, the nurse should reinforce the importance of the correct technique and procedural steps.
Observe the Consistency and Thoroughness of Staff in Washing or Disinfecting Hands
Application of disposable gloves is a basic procedure that should be performed correctly by unlicensed assistive personnel (UAP). If the nurse observes UAP failing to use gloves when necessary, reinforce the importance of the procedure.
Clarify for the UAP the Type of Isolation Precautions to Use (see Figures 7-7 to 7-9)
Basic care procedures (e.g., bathing and feeding) that are performed for patients in transmission-based isolation can be delegated to UAP. The nurse is responsible for assessing whether it is more effective to provide direct care or delegate care activities, depending on the patient's clinical status. Procedures such as medication administration and care of IV lines require the application of critical thinking knowledge unique to the nurse.
Clarify for UAP Special Precautions in Use of a Fitted Respirator Mask
Basic care procedures (e.g., bathing and feeding) that are performed under airborne infection isolation (see Skill 7-5) can be delegated to UAP. The nurse is responsible for assessing whether it is more effective to provide direct care or delegate care activities, depending on the patient's clinical status. Procedures such as medication administration and care of IV lines require the critical thinking and knowledge application unique to the nurse.