Care of the Patient With a Urinary Disorder
Objectives
Anatomy and Physiology
1. Describe the structures of the urinary system, including functions.
2. List the three processes involved in urine formation.
3. Name three hormones and their influence on nephron function.
4. Compare the normal components of urine with the abnormal components.
Medical-Surgical
5. Identify the effects of aging on urinary system function.
6. Describe the changes in body image created when the patient experiences an alteration in urinary function.
7. Incorporate pharmacotherapeutic and nutritional considerations into the nursing care plan of the patient with a urinary disorder.
8. Prioritize the special needs of the patient with urinary dysfunction.
9. Describe the alterations in kidney function associated with disorders of the urinary tract.
10. Address patient concerns in teaching about altered sexuality secondary to urinary disorders and treatments.
11. Investigate community resources for support for the patient and significant others as they face lifestyle changes from chronic urinary disorders and treatments.
12. Select nursing diagnoses related to alterations in urinary function.
Key Terms
http://evolve.elsevier.com/Cooper/foundationsadult/
Anatomy and Physiology of the Urinary System
Each day, the cells throughout the body metabolize ingested nutrients. This process provides energy for the body and produces waste products. As proteins break down, nitrogenous waste—urea, ammonia, and creatinine (a nitrogenous compound produced by metabolic processes in the body)—is produced. The urinary system is largely responsible for maintenance of homeostasis in the body. The primary function of the kidneys is excretion of these waste products. The kidneys also assist in regulating the body's water, electrolytes, secretion of erythropoietin (which stimulates red blood cell production), and acid-base balance.
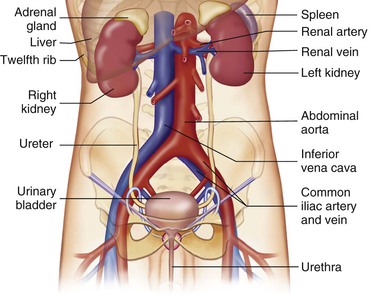
The urinary system consists of two kidneys, two ureters, the bladder, and the urethra. The kidneys remove waste, excess water, and electrolytes from the blood and concentrate them into urine. The ureters transport urine from the kidneys to the bladder The bladder collects and stores urine. The urethra transports urine from the bladder to the outside of the body during elimination (Figure 49-1). This chapter explores the filtering process of the kidneys, the composition of urine, and the how urine is removed from the body.
Kidneys
The kidneys lie behind the parietal peritoneum (retroperitoneal), just below the diaphragm, on each side of the vertebral column. Kidneys are dark red, bean-shaped organs that are 4 to 5 inches (10 to 12 cm) long, 2 to 3 inches (5 to 7.5 cm) wide, and about 1 inch (2.5 cm) thick. Because of the position of the liver, the right kidney lies slightly lower than the left. The kidneys are surrounded and anchored in place by a layer of adipose tissue. Near the center of each kidney's medial border is a notch or indentation called the hilus, where the renal artery enters and the renal vein and the ureter exit the kidney.
The adrenal glands, a part of the endocrine system, sit near the top of each kidney. The adrenal glands secrete hormones that help control blood pressure and heart rate, among other functions. The primary substance secreted by the adrenal cortex is a mineralocorticoid hormone called aldosterone. The level of potassium concentration in the plasma is the primary regulator of aldosterone. Changes evoked through the adrenal glands produce changes in kidney function (see Chapter 50).
Gross Anatomical Structure
The outer covering of the kidney is a strong layer of connective tissue called the renal capsule. Directly beneath the renal capsule is the renal cortex. It contains 1.25 million renal tubules, which are part of the microscopic filtration system. Immediately beneath the cortex is the medulla, which is a darker color. The medulla contains the triangular pyramids. Continuing inward, the narrow points of the pyramids (papillae) empty urine into the calyces. The calyces (singular, calyx) are cuplike extensions of the renal pelvis that guide urine into the main part of the renal pelvis. The renal pelvis is an expansion of the upper end of the ureter; the ureter in turn drains the finished product, urine, into the bladder (Figure 49-2).

Microscopic Structure
Nephron.
Each kidney contains more than 1 million nephrons. The nephron resembles a microscopic funnel with a long stem and two convoluted sections (Figure 49-3). It filters the blood and processes the urine by: (1) controlling body fluid levels by selectively removing or retaining water, (2) helping to regulate the pH of the blood, and (3) removing toxic waste from the blood. Approximately 60 times a day, the body's entire volume of blood is filtered through the kidneys.
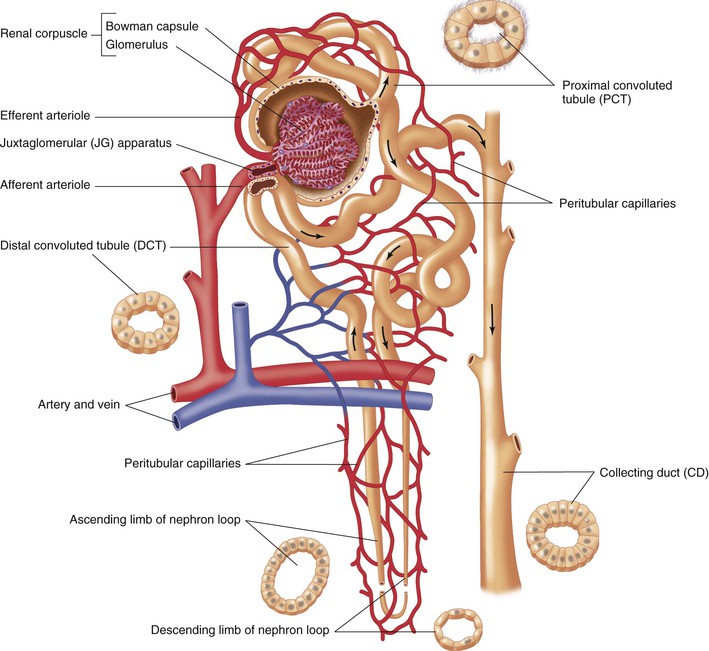
A nephron has two main structures: the renal corpuscle and renal tubule. The renal corpuscle is a tightly bound network of capillaries called glomeruli (singular, glomerulus) that are held inside a cuplike structure, the Bowman's capsule. The renal arteries (right and left) branch off the abdominal aorta and enter each kidney at the hilus. The renal arteries continue branching inside the kidney until blood is delivered to the glomerulus by an afferent arteriole. The filtered blood leaves the glomerulus through an efferent arteriole and flows to a peritubular capillary. The cleansed blood finally reaches the renal veins and flows into the inferior vena cava.
The renal tubule becomes tightly coiled (at the proximal convoluted tubule), makes a sudden straight drop, and curves back upward like a hairpin (at Henle's loop, or nephron loop) and becomes tightly coiled again (at the distal convoluted tubule). The convoluted tubule terminates at the collecting tubule or duct. Several collecting ducts unite in a pyramid and open at the papilla to empty urine into the associated calyx.
The juxtaglomerular apparatus is a microscopic structure in the kidney that regulates the function of each nephron. The juxtaglomerular apparatus is named for its proximity to the glomerulus; it is found between the vascular pole of the renal corpuscle and the returning distal convoluted tubule of the same nephron. This location is critical to its function in regulating renal blood flow and the glomerular filtration rate. The juxtaglomerular apparatus is where the afferent arterioles come into direct contact with the distal convoluted tubule. The juxtaglomerular apparatus regulates systemic blood pressure and filtrate formation.
The specialized cells of the afferent arteriole at this region are called juxtaglomerular cells. These cells contain the enzyme renin and sense blood pressure.
The specialized cells of the distal convoluted tubule at the point of contact with the afferent arteriole are the macula densa cells. These cells sense changes in the solute concentration and flow rate of the filtrate.
When systemic blood pressure decreases, the juxtaglomerular cells have a decreased stretch, which leads to their release of renin. Renin release activates the renin-angiotensin mechanism, which ultimately leads to increased blood pressure.
Reabsorption begins as soon as the filtrate reaches the tubule system. The filtrate contains important products needed by the body: water, glucose, and ions are absorbed. In fact, 99% of the filtrate returns to the body (Figure 49-3).
In summary, the three phases of urine formation (Table 49-1) and location of the processes are as follows:
1. Filtration of water and blood products occurs in the glomerulus of Bowman's capsule.
2. Reabsorption of water, glucose, and necessary ions back into the blood occurs primarily in the proximal convoluted tubules, Henle's loop, and the distal convoluted tubules.
3. Secretion of certain ions, nitrogenous waste products, and drugs occurs primarily in the distal convoluted tubule. This process is the reverse of reabsorption; the substances move from the blood to the filtrate.
Table 49-1
Functions of the Parts of the Nephron in Urine Formation
| PART OF NEPHRON | PROCESS IN URINE FORMATION | SUBSTANCES MOVED AND DIRECTION OF MOVEMENT |
| Glomerulus | Filtration | Water and solutes (sodium and other ions, nitrogenous wastes [urea, uric acid, creatinine], glucose, and other nutrients) filter through the glomeruli into Bowman's capsule |
| Proximal convoluted tubule | Reabsorption | Water and solutes |
| Loop of Henle | Reabsorption | Sodium and chloride ions |
| Distal convoluted and collecting tubules | Reabsorption | Water, sodium and other ions |
| Secretion | Ammonia, potassium ions, urea, uric acid, creatinine, hydrogen ions, and some drugs |
Hormonal influence on nephron function.
When the body experiences increased fluid loss through hemorrhage, diaphoresis, vomiting, diarrhea, or other means, the blood pressure drops. These events decrease the amount of filtrate produced by the kidneys. The posterior pituitary gland releases antidiuretic hormone (ADH). ADH causes the cells of the distal convoluted tubules to increase their rate of water reabsorption. This action returns the water to the bloodstream, which raises the blood pressure to a more normal level and causes the urine to become concentrated. See Box 49-1 for major functions of kidneys.
Urine Composition and Characteristics
The word urine comes from one of its components, uric acid. Each day, the body forms 1000 to 2000 mL of urine; this amount is influenced by several factors, including mental and physical health, oral intake, and blood pressure. Urine is 95% water; the remainder is nitrogenous waste and salts. It is usually a transparent yellow with a characteristic odor. Normal urine is yellow because of urochrome, a pigment resulting from the body's destruction of hemoglobin. Urine is slightly acidic, with a pH of 4.6 to 8 and a specific gravity of 1.003 to 1.030. Healthy urine is sterile, but at room temperature it rapidly decomposes and smells like ammonia as a result of the breakdown of urea.
Urine Abnormalities
A urinalysis, which examines the physical, chemical, and microscopic properties of urine, can give important diagnostic information. If the body's homeostasis has been compromised, certain substances may spill into the urine. Some of the more common substances include the following:
• Albumin in the urine (albuminuria) indicates possible renal disease, increased blood pressure, or toxicity of the kidney cells from heavy metals.
• Glucose (sugar) in the urine (glycosuria) most often indicates a high blood glucose level. When the blood glucose level rises above the renal threshold (the point at which the renal tubules can no longer reabsorb), the glucose spills into the urine.
• Erythrocytes in the urine (hematuria) may indicate infection, tumors, or renal disease. Occasionally an individual may have a renal calculus (kidney stone; plural, calculi), and irritation produces hematuria.
• Ketone bodies in the urine are called ketoaciduria (or ketonuria). It occurs when too many fatty acids are oxidized. This condition is seen with diabetes mellitus, starvation, or any other metabolic condition in which fats are rapidly catabolized.
• Leukocytes (white blood cells [WBCs]) are found in urine when there is an infection in the urinary tract.
Ureters
Once the urine has been formed in the nephrons, it passes to the paired ureters. Ureters are actually extensions of the renal pelvis and extend downward 10 to 12 inches (25 to 30 cm) to the lower part of the urinary bladder. As the ureters leave the kidneys, they remain in the retroperitoneal space and pass under the urinary bladder before entering it. As the ureters enter the bladder (at the ureterovesical junction), internal mucous membrane folds act as a valve to prevent backflow of urine.
Urinary Bladder
The urinary bladder (Figure 49-4) is a temporary storage pouch for urine. It is composed of collapsible muscle and is located anterior to the small intestine and posterior to the symphysis pubis (where the right and left pelvic bones join, just above the penis in men, and just above the vulva in women). As the bladder fills with urine, it rises into the abdominal cavity and can be palpated. The bladder can hold 750 to 1000 mL of urine. When the bladder contains approximately 250 mL of urine, the individual has a conscious desire to urinate. This is because the stretch receptors become activated and a message is sent to the spinal cord. A moderately full bladder holds 450 mL (1 pint) of urine.
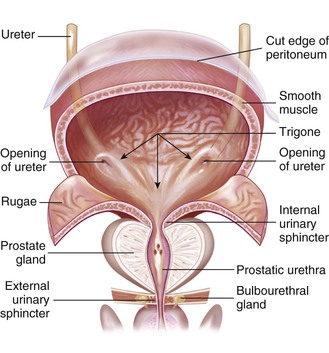
Two sphincters control the release of urine. The internal sphincter, located at the bladder neck, is composed of involuntary muscle. As the bladder becomes full, the stretch receptors cause contractions, pushing the urine past the internal sphincter. The urine then presses on the external sphincter, which is composed of skeletal or voluntary muscle at the terminus of the urethra.
Urethra
The urethra is the terminal portion of the urinary system. It is a small tube that carries urine by peristalsis from the bladder out of its external opening, the urinary meatus. In females it is embedded in the anterior wall of the vagina vestibule and exits between the clitoris and the vaginal opening. The female urethra is approximately  inch in diameter and
inch in diameter and  inches long. In males the urethra is approximately 8 inches long, passing through the prostate gland and extending the length of the glans penis. In the male the urethra serves two functions: as a passageway for urine and semen.
inches long. In males the urethra is approximately 8 inches long, passing through the prostate gland and extending the length of the glans penis. In the male the urethra serves two functions: as a passageway for urine and semen.
Effects of Normal Aging on the Urinary System
With aging the kidneys lose part of their normal functioning capacity. By age 70 the filtering mechanism is only 50% as efficient as at age 40. This occurs because of decreased blood supply and loss of nephrons.
In the aging woman the bladder loses tone and the perineal muscles may relax, resulting in stress incontinence. In the aging man the prostate gland may become enlarged, leading to constriction of the urethra. Incomplete emptying of the bladder in both men and women increases the possibility of urinary tract infection (UTI) (see Life Span Considerations box).
 Life Span Considerations
Life Span Considerations
Older Adults
Urinary Disorder
• Urinary frequency, urgency, nocturia (excessive urination at night), retention, and incontinence are common with aging. These occur because of weakened musculature in the bladder and urethra, diminished neurologic sensation combined with decreased bladder capacity, and the effects of medications such as diuretics.
• Urinary incontinence can lead to a loss of self-esteem and result in decreased participation in social activities.
• Older women are at risk for stress incontinence because of hormonal changes and weakened pelvic musculature.
• Older men are at risk for urinary retention because of prostatic hypertrophy.
• Urinary tract infections in older adults are often associated with invasive procedures such as catheterization, diabetes mellitus, and neurologic disorders.
• Inadequate fluid intake, immobility, and conditions that lead to urinary stasis increase the risk of infection in the older adult.
• Frequent toileting and meticulous skin care can reduce the risk of skin impairment secondary to urinary incontinence.
Laboratory and Diagnostic Examinations
Diagnostic tests for urinary tract conditions include laboratory tests, diagnostic imaging, and endoscopic procedures. Nursing responsibilities vary according to the studies performed. Be aware of specific patient variables that may influence test results: state of hydration, nutritional status, or trauma (see Cultural Considerations box). Prepare patients for diagnostic testing by briefly describing the purpose of the procedure and what the patient can expect to happen.
 Cultural Considerations
Cultural Considerations
Urinary Disorder
A cultural assessment reflects a dynamic process in which the health care team seeks to gain insights concerning the patient's understanding of the meaning of care, health, and well-being. Integral components of a cultural assessment include communication, time orientation, personal space, pain, religious beliefs, taboos, customs, dietary practices, health practices, family roles, and views of death.
Professional discussion of urinary problems requires sensitivity because of the association of the urinary system with the reproductive system and the associated cultural taboos surrounding sexuality. Often the patient's self-image and sexual performance are affected by altered urinary function. Be sensitive to the patient's feelings, guiding the interview to ensure accurate assessment while maintaining the patient's dignity.
Urinalysis
The most common urinary diagnostic study is the urinalysis. Table 49-2 describes normal and abnormal constituents in the urine and possible factors that influence test results. A urinalysis may be done during assessments of other body systems because of the role of the kidneys in maintaining homeostasis. Urine culture and sensitivity may be done to confirm suspected infections, to identify causative organisms, and to determine appropriate antimicrobial therapy. Cultures are also obtained for periodic screening of urine when the threat of a UTI persists. Various reagent strips to test urine for abnormal substances are a quick reference that can be used in a clinical setting or at home. Common substances measured to monitor kidney function include total urine protein, creatinine, urea, uric acid levels, and catecholamines (National Library of Medicine [NLM], 2011). Low levels of protein in the urine are normal. Elevated levels may be noted temporarily with illness. Chronically elevated levels are seen in renal damage and cardiac disease. Creatinine level abnormalities are nonspecific but may be noted with a variety of conditions including kidney failure, urinary obstruction, and infection. Uric acid results from the breakdown of purines. Low levels may be tied to alcohol use and glomerulonephritis. Catecholamines are made by nervous tissue and the adrenal glands. Their levels may be elevated with the ingestion of many medications including tricyclic antidepressants and amphetamines. Levels are reduced with monoamine oxidase (MAO) inhibitors and salicylates. Elevated levels may be associated with metastatic cancers, bone marrow disorders, and gout.
Table 49-2
Urinalysis
| CONSTITUENT | NORMAL RANGE | INFLUENCING FACTORS |
| Color | Pale yellow to amber | Diabetes insipidus, biliary obstruction, medications, diet |
| Turbidity | Clear to slightly cloudy | Phosphates, white blood cells, bacteria |
| Odor | Mildly aromatic | Medication, bacteria, diet |
| pH | 4.6-8 | Stale specimen, food intake, infection, homeostatic imbalance |
| Specific gravity | 1.003-1.030 | State of hydration, medications |
| Glucose | Negative | Diabetes mellitus, medications, diet |
| Protein | Negative | Renal disease, muscle exertion, dehydration |
| Bilirubin | Negative | Liver disease with obstruction or damage, medications |
| Hemoglobin | Negative | Trauma, renal disease |
| Ketones | Negative | Diabetes mellitus, diet, medications |
| Red blood cells | Up to 2 per LPF | Renal or bladder disease, trauma, medications |
| White blood cells | 0-4 per LPF | Renal disease, urinary tract infection |
| Casts | Rare | Renal disease |
| Bacteria | Negative | Urinary tract infection |
LPF, Low-power field.
Urinalysis is performed on sample obtained using clean-catch technique or by catheterization. A sterile urine specimen can be obtained either by inserting a straight catheter into the urinary bladder and removing urine or by obtaining a specimen via the catheter port of an indwelling catheter, using sterile technique. Because the kidneys excrete substances in varying amounts and rates during a 24-hour period, a 24-hour urine sample may be collected. Discard the first voiding and note the time at the beginning of the 24-hour urine collection. For the next 24 hours all urine is collected and placed in a special laboratory container that is opaque to prevent light damage to substances in the urine. The collection container is stored on ice during the collection period.
Urine Specific Gravity
To determine the specific gravity of urine, the density of a urine sample is compared with that of water. It is only an approximation of the concentration of particles (i.e., solutes) in urine, but does indicate a patient's hydration status and gives information about the kidneys' ability to concentrate urine. Urine specific gravity is decreased by high fluid intake, reduced renal concentrating ability, diabetes insipidus (an endocrine disorder in which the kidneys are unable to conserve water when they purify blood), and diuretic use. It is increased in dehydration due to fever, diaphoresis, vomiting, diarrhea, and medical conditions such as diabetic ketoacidosis or hyperglycemic hyperosmolar nonketotic coma (complications of diabetes mellitus in which the kidneys are unable to excrete the high amounts of glucose in the blood) and inappropriate secretion of ADH. The normal value ranges between 1.003 and 1.030, with the lower values suggesting more dilute urine (Pagana and Pagana, 2008).
Blood (Serum) Urea Nitrogen
Blood urea nitrogen (BUN) is a laboratory test used to determine the kidney's ability to rid the blood of nonprotein nitrogenous (NPN) waste and urea, which result from protein breakdown (catabolism). The test may be performed to assess the overall function of the kidneys, to monitor the progression of kidney disease, or to evaluate the effectiveness of prescribed therapies. The acceptable serum range for BUN is 10 to 20 mg/dL. For a more accurate test result, the patient should receive nothing by mouth (NPO) for 8 hours before blood sampling (WebMD, 2010). In addition to renal disease, elevated levels are associated with dehydration, heart disease, and a diet high in protein. If the BUN is elevated, institute preventive nursing measures to protect the patient from possible disorientation or seizures.
Blood (Serum) Creatinine
Creatinine is a catabolic product of creatine, which is used in skeletal muscle contraction. The daily production of creatine, and subsequently creatinine, depends on muscle mass, which fluctuates little. Creatinine, as with BUN, is excreted entirely by the kidneys and is therefore directly proportional to renal excretory function. Thus, with normal renal excretory function, the serum creatinine level should remain constant and normal. Elevated levels may be caused by nonrenal factors such as dehydration, preeclampsia, and muscular dystrophy. Levels may be elevated as a result of renal causes including acute tubular necrosis, glomerulonephritis (inflammation of the glomeruli), pyelonephritis (typically a bacterial infection of the kidneys and upper urinary tract), reduced kidney function, and renal failure. Lower levels may be noted with myasthenia gravis and late-stage muscular dystrophy.
The serum creatinine test, as with BUN, is used to diagnose impaired kidney function. However, unlike BUN, the creatinine level is affected little by dehydration, malnutrition, or hepatic function. The creatinine level is interpreted in conjunction with the BUN. The acceptable serum creatinine range is 0.5 to 1.1 mg/dL (female) and 0.6 to 1.2 mg/dL (male) (Pagana and Pagana, 2008). The level in women is lower because they usually have less muscle mass (PubMed, 2011).
Creatinine Clearance
Creatinine, an NPN substance, is present in the blood and urine. Creatinine is generated during muscle contraction and then excreted by glomerular filtration. Levels are directly related to muscle mass and are usually measured for a 24-hour period. During the testing period, the patient avoids excessive physical activity. A fasting blood sample is drawn at the onset of testing and another at the conclusion. Discard the initial urine specimen and start the 24-hour timing at that point. Collect all urine in the 24-hour period because any deviation will alter test results. An elevated serum level with a decline in urine level indicates renal disease. Normal ranges are as follows: serum, 0.5 to 1.1 mg/dL (female), 0.6 to 1.2 mg/dL (male); urine, 87 to 107 mL/minute (female), 107 to 139 mL/minute (male) (Pagana and Pagana, 2008).
Prostate-Specific Antigen
Prostate-specific antigen (PSA) is an organ-specific glycoprotein produced by normal prostatic tissue. Measurement of PSA has largely replaced that of prostatic acid phosphatase because it is a more accurate test. The normal range is less than 4 ng/mL. Older men normally have levels higher than those of younger men. It may be used to evaluate the prostate health of men being treated for cancer, or as a diagnostic screening. Elevated levels may result from prostate cancer, inflammation or infection, urinary tract infection, or recent cystoscopy or prostatic biopsies. The test is not a specific determination of the presence of prostate cancer. Elevations in levels warrant additional studies.
Urine Osmolality
Assessment of urine osmolality, which directly determines the number of particles (i.e., solute) per volume of water (i.e., solvent), is sometimes more informative than urine specific gravity, but is a more difficult test to perform. Plasma osmolality may be determined in conjunction with the urine sampling when pituitary disorders are suspected. Results provide information on the concentrating ability of the kidneys.
Kidney-Ureter-Bladder Radiography
A kidney-ureter-bladder (KUB) radiograph assesses the general status of the abdomen and the size, structure, and position of the urinary tract structures. No special preparation is necessary. Explain to the patient that the procedure involves changing position on the radiography table, which may be uncomfortably firm. Abnormal findings related to the urinary system may indicate tumors, calculi, glomerulonephritis, cysts, and other conditions.
Intravenous Pyelography or Intravenous Urography
Intravenous pyelography (IVP), also called intravenous urography (IVU), evaluates structures of the urinary tract, filling of the renal pelvis with urine, and transport of urine via the ureters to the bladder. Before performing this procedure it is vital to determine whether the patient has an allergy to iodine (or iodine-containing foods such as iodized salt, saltwater fish, seaweed products, or vegetables grown in iodine-rich soils), because iodine is the basis of the radiopaque dye injected into the patient's vein for this and other radiologic examinations. If the patient is allergic to iodine, the health care provider may order administration of a corticosteroid or an antihistamine before testing or, alternatively, may order ultrasonography.
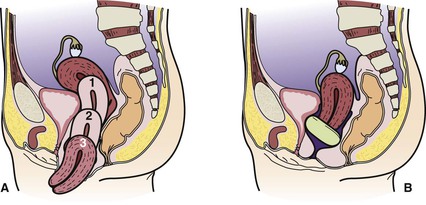
Because kidneys and ureters are positioned in the retroperitoneal space, gas and stool in the intestines interfere with radiographic visualization. Preparation usually includes eating a light evening meal, taking a non–gas-forming laxative, and remaining NPO for 8 hours before the test. If additional tests using barium-based studies are planned, the IVP is scheduled first. When the dye is injected, the patient experiences a warm, flushing sensation and a metallic taste. During the procedure, monitor vital signs frequently. Radiographs are taken at various intervals to monitor movement of the dye. Abnormal findings may indicate structural deviations, hydronephrosis (kidney swelling), calculi within the urinary tract, polycystic renal (kidney) disease (PKD), tumors, and other conditions.
Retrograde Pyelography
Retrograde pyelography involves examination of the lower urinary tract with a cystoscope under aseptic conditions. The urologist injects radiopaque dye directly into the ureters to visualize the upper urinary tract. Urine samples can be obtained directly from the renal pelvis. Additional retrograde studies include the following:
• Retrograde cystography: Radiopaque dye is injected through an indwelling catheter into the urinary bladder to evaluate its structure or to determine the cause of recurrent infections.
• Retrograde urethrography: A catheter is inserted and dye injected as in retrograde cystography to assess the status of the urethral structure.
Voiding Cystourethrography
Voiding cystourethrography is used in conjunction with other diagnostic studies to detect abnormalities of the urinary bladder and the urethra. Preparation includes administering an enema before the test. An indwelling catheter is inserted into the urinary bladder, and dye is injected to outline the lower urinary tract. Radiographs are taken, and the catheter is then removed. The patient is asked to void while radiographs are being taken. Some patients experience embarrassment or anxiety related to the procedure and should be given the opportunity to express their feelings. Structural abnormalities, diverticula, and reflux into the ureter may be detected.
Endoscopic Procedures
Endoscopic procedures are visual examinations of hollow organs, done with a scope (typically a flexible tube equipped with a light and camera). The invasive nature of the procedure makes a signed written consent necessary. The procedure may be done in the surgical suite; if so, the patient requires preoperative preparation (see Chapter 41). The procedure is performed by a urologist.
Cystoscopy is a visual examination done to inspect, treat, or diagnose disorders of the urinary bladder and proximal structures. As with all medical procedures, patient preparation includes a description of what is going to happen. Usually the procedure is carried out with a local anesthetic after the patient has been sedated. Patient safety is paramount when the patient is sedated. The patient is placed in a lithotomy position (i.e., supine, with the legs spread apart and the feet in stirrups) for the procedure, which may produce embarrassment and anxiety. The thought of a scope being inserted while the patient is awake may intensify these feelings. Provide an opportunity for the patient to verbalize feelings.
The scope is inserted under aseptic conditions after a local anesthetic has been instilled into the urethra. The patient experiences a feeling of pressure as the scope enters. Continuous fluid irrigation of the bladder is necessary to facilitate visualization. Care after the procedure is finished includes hydration to dilute the urine. Monitor the first voiding after the procedure, assessing time, amount, color, and any dysuria (painful or difficult urination). The first voiding is occasionally blood tinged due to the trauma of the procedure.
The urologist can perform a brush biopsy via a ureteral catheter during a cystoscopy. A nylon brush is inserted through the catheter to obtain specimens from the renal pelvis or calyces. Nephroscopy (renal endoscopy) done via the percutaneous route (i.e., through the skin) provides direct visualization of the upper urinary structures. The urologist can obtain biopsy or urine specimens or remove calculi.
Renal Angiography
Renal angiography aids in evaluating blood supply to the kidneys, evaluates masses, and detects possible complications after kidney transplantation. Withhold oral intake the night before the procedure. The procedure requires passing a small catheter into an artery (usually the femoral artery) to provide a port for the injection of radiopaque dye. Therefore, when the procedure is completed, have the patient lie flat in bed for several hours to minimize the risk of bleeding. Assess the puncture site for bleeding or hematoma, and maintain the pressure dressing at the site. Assess the circulatory status of the involved extremity every 15 minutes for 1 hour, and then every 2 hours for 24 hours.
Renal Venography
Renal venography provides information about the kidney's venous drainage. The catheter through which a radiopaque dye is injected is inserted into the femoral vein. Care following the procedure includes assessment of vital signs. Monitor the patient for bleeding at the puncture site. Assess for bruising and swelling at the site. Assess pulses distal to the puncture site. Potential complications after the procedure include allergic reaction to the dye, bleeding, clots, or injury to the vein.
Computed Tomography
A computed tomography (CT) scan differentiates masses in the kidney. Images are obtained by a computer-controlled scanner. A radiopaque dye may be injected to enhance the images. Serum urea and creatinine levels are obtained before use of radiopaque dye. The dye is not used if inadequate kidney function is noted. Inform the patient that the table on which he or she is placed and the machine “taking pictures” will move at intervals and that it is important to lie still. The CT body-scanning unit takes multiple cross-sectional pictures at several different sites, creating a three-dimensional map of the renal structure. The adrenal glands, the bladder, and the prostate may also be visualized.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) uses nuclear magnetic resonance as its source of energy to obtain a visual assessment of body tissues. The patient requires no special preparation other than removal of all metal objects that might be attracted by the magnet. Patients with metal prostheses (such as heart valves, orthopedic screws, or cardiac pacemakers) cannot undergo MRI.
Emphasize that the examination area will be confining and that a repetitive “pounding” sound will be heard (somewhat like the sound of a muffled jackhammer). MRI can be used to diagnose pathologic conditions of the renal system.
Renal Scan
A radionuclide tracer substance that will be taken up by renal tubular cells or excreted by the glomerular filtrate is injected intravenously. A series of computer-generated images is then made. The scan provides data related to functional parenchyma (the essential parts of an organ that are concerned with its function). No special patient preparation is needed. Check facility policy concerning the disposal of the patient's urine for the first 24 hours. Pregnant nurses should refrain from caring for patients administered radioactive substances.
Ultrasonography
Ultrasonography is a diagnostic tool that uses the reflection of sound waves to produce images of deep body structures. Inform the patient that a conducting jelly will be applied on the skin over the area to be studied; this improves the transmission of sound waves. The sound waves are high frequency and inaudible to the human ear; the waves are converted into electrical impulses that are photographed for study.
Ultrasonography can visualize size, shape, and position of the kidney and delineate any irregularities in structure. Deviations from normal findings may indicate tumors, congenital anomalies, cysts, or obstructions. No special patient preparation is necessary.
Transrectal Ultrasound
Transrectal ultrasound instrumentation of the prostate gland provides clear images of prostatic tumors that otherwise might go undiagnosed. Transrectal ultrasound–guided biopsy is performed to obtain samples of prostatic tissue from various areas with minimal discomfort to the patient.
Renal Biopsy
The kidney can be biopsied by an open procedure similar to other surgical procedures on the kidney or by the less invasive method of needle biopsy, also called a percutaneous biopsy. Inform the patient that he or she may experience pain during the procedure and should follow instructions, such as holding the breath. Bed rest is instituted for 24 hours after the procedure. Mobility is restricted to bathroom privileges for the next 24 hours, and gradual resumption of activities is allowed after 48 to 72 hours. Potential complications associated with the procedure include infection, damage to the kidney, and bleeding. Teach the patient to report signs of complications including temperature elevations, unrelieved pain, and difficulty voiding.
Urodynamic Studies
Urodynamic studies are indicated when neurologic disease is thought to be the underlying cause of incontinence. These studies evaluate the activity level of the urinary bladder muscle (detrusor). This may cause the patient to be embarrassed and somewhat uncomfortable. A simple urodynamic study is cystometrography, in which a catheter is inserted into the bladder and then connected to a cystometer, which measures bladder capacity and pressure. The examiner asks the patient about sensations of heat, cold, and urge to void, and instructs the patient at times to void and change position.
Cholinergic and anticholinergic medications may be administered during urodynamic studies to determine their effects on bladder function. A cholinergic drug, such as bethanechol (Urecholine), stimulates an atonic bladder; an anticholinergic drug, such as atropine, brings an overactive bladder to a more normal level or function.
Associated testing includes rectal electromyography, which involves placement of an electrode into the anal sphincter; and a urethral pressure profile, in which a special catheter connected to a transducer evaluates urethral pressures.
Medication Considerations
The kidneys filter a wide range of water-soluble products from the blood, including medications. The kidneys' ability to remove certain medications from the blood may be affected by various conditions, such as renal disease, changes in the urine pH, and age. Patients with renal disease are given smaller doses of medications to minimize further damage or drug toxicity. Alteration in urinary pH affects the absorption rate of certain medications. Older patients may have decreased physiologic functioning, diminishing the kidneys' capacity to excrete drugs. Diminished kidney function interferes with the filtration of water-soluble medications.
The medications included in this discussion are representative of those that directly affect kidney function or are used to treat urinary disorders (Table 49-3).
 Table 49-3
Table 49-3
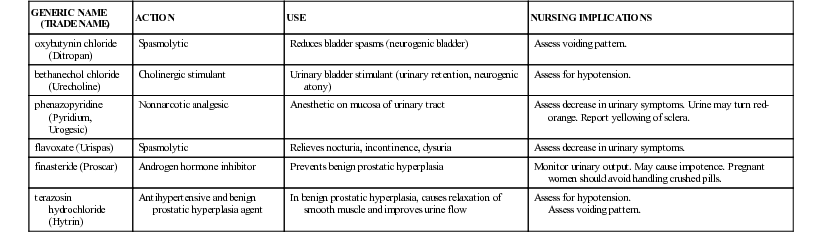
Medications That Affect the Urinary System
| GENERIC NAME (TRADE NAME) | ACTION | USE | NURSING IMPLICATIONS |
| oxybutynin chloride (Ditropan) | Spasmolytic | Reduces bladder spasms (neurogenic bladder) | Assess voiding pattern. |
| bethanechol chloride (Urecholine) | Cholinergic stimulant | Urinary bladder stimulant (urinary retention, neurogenic atony) | Assess for hypotension. |
| phenazopyridine (Pyridium, Urogesic) | Nonnarcotic analgesic | Anesthetic on mucosa of urinary tract | Assess decrease in urinary symptoms. Urine may turn red-orange. Report yellowing of sclera. |
| flavoxate (Urispas) | Spasmolytic | Relieves nocturia, incontinence, dysuria | Assess decrease in urinary symptoms. |
| finasteride (Proscar) | Androgen hormone inhibitor | Prevents benign prostatic hyperplasia | Monitor urinary output. May cause impotence. Pregnant women should avoid handling crushed pills. |
| terazosin hydrochloride (Hytrin) | Antihypertensive and benign prostatic hyperplasia agent | In benign prostatic hyperplasia, causes relaxation of smooth muscle and improves urine flow | Assess for hypotension. Assess voiding pattern. |
Diuretics to Enhance Urinary Output
Diuretics enhance urinary output by increasing the filtration of sodium, chloride, and water at various sites in the kidney. Diuretics are used in the management of a variety of disorders, such as heart failure and hypertension. Diuretics are classified by chemical structure and by the site and type of action in the kidney.
Thiazide Diuretics
Thiazide diuretics such as chlorothiazide (Diuril) act at the distal convoluted tubule to impair sodium and chloride reabsorption, leading to excretion of electrolytes and water. In addition to their intended effects, thiazide diuretics can cause hypokalemia (extreme potassium depletion in blood), hyponatremia (decreased sodium concentration in blood), and/or hypercalcemia (excessive amounts of calcium in blood). Hypochloremic alkalosis occurs from a deficiency of chloride. The primary indication for use is to manage systemic edema and control mild to moderate hypertension. It may take a month to achieve the full antihypertensive effect. Chlorothiazide is contraindicated in anuria (urinary output of less than 100 mL/day).
Loop (or High-Ceiling) Diuretics
Loop, or high-ceiling, diuretics such as furosemide (Lasix) act primarily in the ascending loop of Henle to inhibit tubular reabsorption of sodium and chloride. This group is the most potent of all diuretics and may lead to significant electrolyte depletion. These diuretics are effective for use in patients with impaired kidney function.
In addition to their intended effects, loop diuretics can cause hypokalemia, hypochloremia, hyponatremia, hypocalcemia (abnormally low blood calcium), and/or hypomagnesemia (decreased magnesium in the blood). Their effect on the acid-base balance can lead to the development of hypochloremic alkalosis. Furosemide is used in nephrotic syndrome, heart failure, and pulmonary edema. Side effects are those associated with rapid fluid loss: vertigo, hypotension, and possible circulatory collapse.
Potassium-Sparing Diuretics
Potassium-sparing diuretics act on the distal convoluted tubule to inhibit sodium reabsorption and potassium secretion. Potassium-sparing diuretics decrease the sodium-potassium exchange. Although the actions of these medications vary, they all conserve potassium that is usually lost with sodium in diuresis. But, because they are weak, they are usually used in combination with other diuretics. Potassium-sparing diuretics are contraindicated in patients with hyperkalemia because further retention of potassium could cause a fatal cardiac dysrhythmia. There are two types of potassium-sparing diuretics: aldosterone antagonists and nonaldosterone antagonists. (Note: Cells function and communicate with each other by means of receptors on their surface. Natural ligands bind to these receptors and cause something specific to happen: each receptor type binds to a particular ligand. Agonists and antagonists are drugs that mimic a receptor's natural ligand, but with opposite effects: an antagonist prevents a particular cell response, and an agonist usually prolongs that response.)
The aldosterone antagonist spironolactone (Aldactone) blocks aldosterone in the distal tubule to promote potassium uptake in exchange for sodium secretion. Although it can be used in combination with other diuretics, primarily in the treatment of hypertension and edema, spironolactone is most frequently used for its potassium-sparing quality.
The nonaldosterone antagonist triamterene (Dyrenium) directly reduces ion transportation in the distal tubule, although it has little diuretic effect. Triamterene is instead used to help limit the potassium-wasting effect of other diuretics.
Osmotic Diuretics
Osmotic diuretics act at the proximal convoluted tubule to increase plasma osmotic pressure, causing redistribution of fluid toward the circulatory vessels. Osmotic diuretics are used to manage edema, promote systemic diuresis in cerebral edema, decrease intraocular pressure, and improve kidney function in acute renal failure (ARF). In ARF, osmotics are used to prevent irreversible failure, but they are contraindicated in advanced stages of renal failure.
An example of an osmotic diuretic is mannitol (Osmitrol). It increases the osmolarity of glomerular filtrate; decreases reabsorption of water electrolytes; and increases urinary output, sodium excretion, and chloride excretion, while exerting only a minimal effect on the acid-base balance. Mannitol is used to prevent or treat the oliguric phase of ARF, promote systemic diuresis in cerebral edema, and decrease intraocular pressure. Careful assessment of the cardiovascular system before administering mannitol is essential because of the high risk of inducing heart failure. Avoid extravasation (escape of the medication from the blood vessel into the tissues), which may lead to tissue irritation or necrosis.
Carbonic Anhydrase Inhibitor Diuretics
The enzyme carbonic anhydrase (present in red blood cells) converts water and carbon dioxide to bicarbonate, helping to maintain the acid-base balance in the blood. In the proximal convoluted tubules of the kidneys, acetazolamide (Diamox) inhibits this enzyme, which leads to diuresis; hence acetazolamide is called a carbonic anhydrase inhibitor diuretic. It has limited usefulness as a diuretic, and is also used to lower intraocular pressure.
Nursing Interventions
Because patients receiving diuretics often have complicated disease conditions such as heart failure and pulmonary edema, monitor for signs and symptoms of fluid overload: changes in pulse rate, respirations, cardiac sounds, and lung fields. Record daily morning weights for the patient receiving diuretics. Keep accurate intake and output (I&O) records, and document blood pressure, pulse, and respirations four times a day for the patient on diuretic therapy. Assess BUN, serum electrolytes, and urine as ordered. When instructing the patient and the family about diet, include a warning to avoid overuse of salt in cooking or as a table additive. A number of salt substitutes are currently on the market; however, the long-term effects of those potassium preparations are not known and could further complicate the renal patient's condition. The use of most diuretics, with the exception of the potassium-sparing diuretics, requires adding daily potassium sources (e.g., baked potatoes, raw bananas, apricots, or navel oranges). In some cases the health care provider orders potassium supplements to be taken with the diuretic.
When a diuretic is effective, the serum concentration of other medications may increase as a result. Carefully monitor this potentiating effect to prevent toxicity from other medications. For example, as diuretics effectively decrease the volume of extracellular fluid, the serum level of digoxin may increase proportionately, resulting in digitoxicity. Special care is required in the selection and management of diuretics in the treatment of children, adolescents, and older adults.
Medications for Urinary Tract Infections
Certain antimicrobial agents are administered primarily to treat infections within the urinary tract. Culture and sensitivity testing is used to aid in the selection of the medication that will eradicate the identified pathogen. Urinary antiseptics inhibit bacterial growth and are used to prevent and treat urethritis and cystitis. The health history should include factors such as pregnancy and allergies to ensure the correct medications for the individual are selected.
Urinary antiseptics are divided into four groups: quinolones, nitrofurantoin, methenamine, and fluoroquinolones. Examples of each group follow.
Quinolones
The quinolone nalidixic acid (NegGram) is used to treat UTIs caused by gram-negative microbes (e.g., Escherichia coli and Proteus mirabilis). The common side effects are drowsiness, vertigo, weakness, nausea, and vomiting. The use of nalidixic acid is contraindicated in renal impairment.
Nitrofurantoin
Nitrofurantoin (Macrodantin) is effective against both gram-positive and gram-negative microbes (e.g., Streptococcus faecalis, E. coli, and P. mirabilis) in the urinary tract. Common side effects are loss of appetite, nausea, and vomiting.
Methenamine
Methenamine mandelate (Mandelamine) suppresses fungi and gram-negative and gram-positive organisms (e.g., E. coli, staphylococci, and enterococci). Acidification of the urine by means of an acid-ash diet (such as a diet high in meat, whole grains, eggs, cheese, cranberries, prunes, and plums) or other acidifiers to a pH of less than 5.5 is necessary for effective action. Methenamine mandelate is used for patients with chronic, recurrent UTIs as a preventive measure after antibiotics have cleared the infection. Although side effects are rare, they include nausea, vomiting, skin rash, and urticaria (hives).
Fluoroquinolones
The fluoroquinolone norfloxacin (Noroxin) is a broad-spectrum antibiotic effective against gram-positive and gram-negative organisms (e.g., E. coli, P. mirabilis, Pseudomonas organisms, Staphylococcus aureus, and Staphylococcus epidermidis). It is used in the treatment of UTIs, gonorrhea, and gonococcal urethritis. It is administered with a full glass of water 1 hour before or 2 hours after meals or with antacids.
Nursing Interventions
Before administering antibiotics for UTIs, be certain to check all medications the patient is using for potential negative drug interactions. Instruct the patient to complete the full course of the medication, even though the symptoms may subside quickly. Hydrate the patient to produce a daily urinary output of 2000 mL, unless contraindicated. When indicated, teach the patient to consume an acid-ash diet to help maintain a urine pH of 5.5. Soothe skin irritations with cornstarch or a bath of bicarbonate of soda or dilute vinegar. Report continuing signs of infection.
Observe the patient receiving nalidixic acid for visual disturbances and offer appropriate assistance for ambulation or transfer. Monitor the patient receiving nitrofurantoin for signs of allergic response such as erythema, chills, fever, and dyspnea. If these signs or symptoms develop, discontinue the medication and notify the health care provider (trial doses of this medication may be used to detect a possible allergic reaction before administering the full dose).
Nutritional Considerations
The nutritional needs of the patient with a urinary tract disorder vary with each disease process. Some general guidelines include provision of food choices and number of servings as recommended by the U.S. Department of Agriculture's MyPlate nutrition planning tool (www.choosemyplate.gov) and a daily intake of 2000 mL of water, unless contraindicated. Unique nutritional requirements are discussed with each disorder. Box 49-2 gives an example of dietary modifications to prevent urolithiasis (calculi or stones formed anywhere in the urinary system). Patients with other systemic diseases, such as diabetes mellitus, require strict adherence to those restrictions as well.
Maintaining Adequate Urinary Drainage
Urine clears the body of waste materials and helps balance electrolytes. Conditions that interfere with urinary drainage may create a health crisis. Therefore it is important to reestablish urine flow as soon as possible to prevent the buildup of toxins in the bloodstream. Patients at risk for difficulty with urine elimination include those who have undergone surgical procedures of the bladder, the prostate, or the vagina; patients with primary urologic problems, such as urethral stricture (an abnormal narrowing of the urethra); and those who are critically ill with multisystem problems.
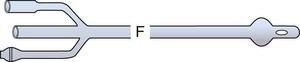
Urinary catheters are used to maintain urine flow, to divert urine flow to facilitate healing postoperatively, to introduce medications by irrigation, and to dilate or prevent narrowing of some portions of the urinary tract. Catheters may be used for intermittent or continuous urinary drainage. Urinary catheters may be introduced into the bladder, the ureter, or the kidney. The type and size of urinary catheter are determined by where it is to be placed, and by the cause of the urinary tract problem. Catheter size is measured by the French (F) system: 1 French (1F) equals a diameter of 0.3 mm. Urethral catheters range from 14F to 24F for adult patients. Ureteral catheters are usually 4F to 6F. The health care provider always inserts ureteral catheters, whereas the nurse usually inserts indwelling urethral catheters.
Types of Catheters
Various types of catheters are used for different purposes (Figure 49-5). The coudé catheter has a tapered tip and is selected for ease of insertion when enlargement of the prostate gland is suspected. The coudé catheter is less traumatic during insertion because it is stiffer and more easily controlled than the straight-tip catheter (Potter and Perry, 2009). The Foley catheter has a balloon near its tip that may be inflated after insertion, holding the catheter in the urinary bladder for continuous drainage. Malecot and de Pezzer, or mushroom, catheters are used to drain urine from the renal pelvis of the kidney. The Robinson catheter has multiple openings in its tip to facilitate intermittent drainage. Ureteral catheters are long and slender to pass into the ureters. The whistle-tip catheter has a slanted, larger orifice at its tip to be used if there is blood in the urine. The cystostomy, vesicostomy, or suprapubic catheter is introduced by the health care provider through the abdominal wall above the symphysis pubis. This catheter diverts urine flow from the urethra as needed to treat injury to the bony pelvis, the urinary tract, or surrounding organs; strictures; or obstruction. The catheter is inserted via surgical incision or puncture of the abdominal and bladder walls with a trocar (a sharp-pointed instrument The catheter is connected to a sterile closed drainage system and secured to avoid accidental removal; the wound is covered with a sterile dressing. When the lower urinary tract has healed, the patient's ability to void is tested by clamping the catheter so that the patient can try to void naturally. When the measured residual urine (the amount left in the bladder after urination) is consistently less than 50 mL, the catheter is usually removed and a sterile dressing is placed over the wound.





An external (Texas or condom) catheter is not actually a catheter but rather a drainage system connected to the external male genitalia. This noninvasive appliance is used for the incontinent male to minimize skin irritation from urine and to reduce risk of infection from an indwelling catheter. The appliance is removed daily for cleansing and inspection of the skin. Use of the external catheter allows the patient to have a more normal lifestyle.
Nursing Interventions and Patient Teaching
Problems of the urinary tract may be indicative of a primary disorder or may be one of multiple symptoms of complex, chronic disease. Therefore it is important to assess urinary elimination at the time of admission. Because of embarrassment and sociocultural taboos, some patients may be reluctant to share information with the nurse. Often the medical system intensifies this discomfort by repeatedly asking the patient to describe the problem to staff in the laboratory, radiology department, and other departments. Discretion during the admission interview and health assessment with strict adherence to Health Insurance Portability and Accountability Act standards enhance patient privacy and comfort.
Nursing interventions for the patient with a urinary drainage system involve a number of principles to prevent and detect infection and trauma:
1. Follow aseptic technique to avoid introducing microorganisms from the environment. Never rest the collecting bag on the floor.
2. Record I&O. For precision monitoring, such as hourly urinary output, add a urometer to the drainage system. If urinary output falls below 50 mL/hour, check the drainage system for proper placement and function before contacting the health care provider.
3. Adequately hydrate the patient to flush the urinary tract.
4. Do not open the drainage system after it is in place except to irrigate the catheter, and then only with health care provider orders. It is important to maintain a closed system to prevent UTIs.
5. Perform catheter care twice daily and as needed, using standard precautions. Each institution has a specific protocol for catheter care. Cleanse the perineum (the region between the thighs, from the anus to the scrotum [in males] or vulva [in females]) with mild soap and warm water, from the front to the back; rinse well; and pat dry. At times an antiseptic solution or ointment may be ordered for use at the catheter incision site.
6. Check the drainage system daily for leaks.
7. Avoid placement of the urinary drainage bag above the level of the catheter insertion, which would cause urine to reenter the drainage system and contaminate the urinary tract.
8. Prevent tension on the system or backflow of urine while transferring the patient.
9. Ambulate the patient if possible to facilitate urine flow. If the patient's activity must be restricted, turn and reposition every  hours.
hours.
10. Avoid kinks or compression of the drainage tube that may cause pooling of the urine within the urinary tract. Gently coil excess tubing, secure with a clamp or pin to avoid dislodging the catheter, and release the tubing before transferring or repositioning the patient.
11. Gently inspect the catheter entry site for blood or exudate that may indicate trauma or infection. Observe the color and composition of the urine for blood or sediment. During drainage of the collection bag, note the presence of odor that is not consistent with the normal smell of urine.
12. Collect specimens from the catheter by cleansing the drainage port with alcohol, and then withdrawing the urine with a sterile adapter and a sterile 10-mL syringe, using standard precautions. Send the urine specimen immediately to the laboratory.
13. Report and record assessment findings and interventions initiated.
After the urinary catheter is removed, the patient may experience difficulty voiding until bladder tone and sensation return. If the patient complains of urinary retention, stimulate urination by running water, placing the patient's hands in water, or pouring water over the perineum. With the last method, subtract the amount of water used in calculating the correct amount voided. If the patient's condition permits, a woman can sit on a bathroom stool or commode, and a male can stand, to void.
The patient may experience some dribbling of urine after voiding as a result of dilation of the sphincter from the catheter. Record the time, amount, and color of the urinary output. Nursing care for the patient who has had their indwelling catheter removed includes assessment of the volume voided, review of intake with consideration to output, and bladder palpation to ensure urinary retention is not occurring.
Nursing diagnoses and interventions for the patient with a urinary catheter include but are not limited to the following.
Instruct the patient about proper transfer from bed, chair, or stretcher and the principles of catheter care. Encourage fluid intake to flush the urinary system.
Self-Catheterization
Self-catheterization may be the intervention of choice for the patient who experiences spinal cord injury or other neurologic disorders that interfere with urinary elimination. Intermittent self-catheterization promotes independent function. At home there is less risk of cross-contamination than in the hospital, so the catheterization procedure can be safely modified as a clean technique. Still, instruct the patient in the use of strict surgical asepsis in the hospital, because of the risk of infection there. Emphasize the need for the patient to be alert for signs and symptoms of infection and to undergo periodic evaluations by the health care provider. Follow institutional guidelines for catheter insertion.
Bladder Training
Bladder training involves developing the muscles of the perineum to improve voluntary control over voiding; bladder training may be modified for different problems. In preparation for removal of a urethral catheter, the health care provider may order a clamp-unclamp routine to improve bladder tone. This method was once widely used but is now less common. A patient with stress incontinence can learn to control leakage by performing Kegel exercises, or pubococcygeal exercises, that tighten the muscles of the perineal floor. The patient can develop awareness of the appropriate muscle group by trying to stop the flow of urine during voiding. Once the patient has identified the correct muscles and the feeling of their contraction, direct her to tighten the muscles of the perineum, hold that tension for 10 seconds, and then relax for 10 seconds. The exercises should be done initially in groups of 10, building to groups of 20, four times a day. Because muscle control develops gradually, it may take 4 to 6 weeks to learn to control leakage.
For habit training, establish a voiding schedule. Monitor the patient's voiding for a few days to identify patterns, or schedule voiding times to correlate with the patient's activities. Typical voiding times are on arising, before each meal, and at bedtime. Help the patient void as scheduled. After a few days, evaluate whether the scheduled voiding pattern keeps the patient continent. Modify the schedule until continence is established. Fluid intake and medications may influence voiding patterns (e.g., the patient may need to void 30 minutes after ingesting coffee or furosemide in response to the diuretic effect). Reduction of fluid intake before bedtime may help keep the patient dry during sleep.
Prognosis
The outcome for patients with urinary disorders depends on many variables: age, preexisting health conditions, general health status, complications, compliance, and available family and community support.
Disorders of the Urinary System
Alterations in Voiding Patterns
Urinary Retention
Etiology and Pathophysiology
Urinary retention is the inability to void even with an urge to void. The patient may not be able to empty the bladder, creating urinary stasis and increasing the possibility of infection. Bladder capacity may be exceeded and the urine may overflow the bladder, causing incontinence. The condition may be acute or chronic. Individuals experiencing acute urinary retention may be completely unable to void despite having a full bladder. Chronic retention is characterized by a sense of the need to void but being unable to completely empty the bladder (National Kidney and Urologic Diseases Information Clearinghouse, 2012a).
Urinary retention has a variety of causes that may be classified as obstructive, infectious/inflammatory, pharmacologic, neurologic, or other (Selius and Subedi, 2008). Obstructions may include calculi or tumor. Infectious/inflammatory processes include urinary tract infections and pyelonephritis. Medications implicated in urinary retention include antiarrhythmics such as disopyramide (Norpace); antihistamines such as fexofenadine (Allegra) and diphenhydramine (Benadryl); antispasmodics/anticholinergics including oxybutynin (Ditropan); and tricyclic antidepressants including imipramine (Tofranil) and amitriptyline (Elavil) (National Kidney and Urologic Diseases Information Clearinghouse, 2012b). Damage to the nerves controlling bladder emptying may be the result of spinal cord injury, stroke, or postoperative complications resulting in interference with the sphincter muscles. Other potential causes may include childbirth or other trauma.
Clinical Manifestations
The signs and symptoms of urinary retention are sometimes vague and easily overlooked. The bladder becomes increasingly distended and may be palpated above the symphysis pubis. Urinary retention may cause the patient considerable discomfort and anxiety.
Assessment
Subjective data include patient complaints of frequency with or without symptoms of burning, urgency, nocturia, and occasionally acute discomfort. Initial symptoms may not seem to be directly associated with urinary retention.
Collection of objective data includes assessing urinary bladder distention (palpable ovoid [egg-shaped] bladder arising suprapubically). The patient may void frequently, void small amounts, and have episodes of incontinence. Patients with diminished sensorium, as from spinal cord injury or organic brain disorder, may be restless and irritable without direct complaints about difficulty voiding.
Medical Management
Diagnostic studies used to confirm diagnosis and potential causes include laboratory studies such as urinalysis, serum blood urea nitrogen, and prostate-specific antigen and imaging studies including renal, bladder, and pelvic ultrasonography, and CT of the abdomen and pelvis.
Mechanical methods, such as the use of urinary catheters or the surgical release of obstructions, may be needed to treat urinary retention. Administer urinary analgesics and antispasmodics as prescribed to enhance patient relaxation and comfort. Continued medical treatments will be focused on alleviating the underlying cause.
Nursing Interventions
The primary goal of nursing interventions is the reinstitution of normal voiding patterns. Regardless of the pathologic findings and medical intervention, the nurse can help the patient achieve adequate voiding by providing a private, relaxed environment. Bladder training approaches may assist the patient in emptying the bladder. Warm showers or sitz baths may promote relaxation of the abdominal, gluteal, and sphincter muscles. Provide warm beverages to help the patient relax. If possible, permit the patient whatever position is preferred for voiding: for women, sitting on a commode or bathroom stool is best; for men, standing may be more natural.
When continence is established, the patient may be catheterized intermittently to determine whether the bladder is emptying. Have the patient void and measure the amount. Catheterize the patient immediately after the voiding and measure the amount retained in the bladder; this is residual urine and should be less than 50 mL. If the underlying pathologic condition remains unchanged, this patient may be at risk for again developing retention. Urinary retention can also be the root cause of repeated urinary tract infections. Teach the patient or primary caretaker to observe for signs and symptoms of urinary retention and to notify the health care provider immediately if they return.
A nursing diagnosis and interventions for the patient with urinary retention include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Impaired urinary elimination, related to: |

Urinary Incontinence
Urinary incontinence (UI) refers to the loss of bladder control. It may range from leaking to full loss of the bladder's contents. An estimated 25 million Americans are affected by urinary continence. Underreporting is likely, given the potential embarrassment related to the condition (National Kidney and Urologic Diseases Information Clearinghouse, 2010).
Etiology and Pathophysiology
UI is the involuntary loss of urine from the bladder. The patient may be totally incontinent, have dribbling, or experience leakage while lifting or sneezing (stress incontinence). Incontinence may arise as a complication of many disorders, such as UTI, loss of sphincter control, or sudden change of pressure within the abdomen. Incontinence may be permanent, as with spinal cord trauma, or temporary, as with pregnancy. Women with weakened structures of the pelvic floor are prone to stress incontinence. Although incontinence may occur at any age, loss of control of urination is a particular problem for older adults.
Physical exertion such as heavy lifting, jobs that require long periods of standing, and high-impact sports may increase an individual's risk for UI. UI may also result from physiologic conditions such as obesity, chronic lung disease, smoking, pelvic floor injury, and surgery. Lack of estrogen in postmenopausal women contributes to atrophy of the vaginal and urethral walls with subsequent loss of muscle tone that may result in postvoiding urine retention and possible prolapse of the bladder.
There are various types of incontinence, which are classified according to their causes. Types of incontinence include the following (Mayo Clinic, 2011):
Stress incontinence: Results from the pressure or stressors on the bladder sphincter by events such as sneezing or heavy lifting
Urge incontinence: Feelings of an urgency to void followed by incontinence. It is associated with conditions such as Parkinson's disease and Alzheimer's disease.
Overflow incontinence: Repeated inability to fully empty the bladder results in an overly full bladder, which leaks out unexpectedly.
Mixed incontinence: A mixture of both stress and urge incontinence
Functional incontinence: The influence of mental and physical impairments resulting in an inability to make it to the toilet in time to void
Clinical Manifestations
The cardinal sign of UI is the involuntary loss of urine, which may or may not be the primary reason the patient seeks treatment.
Assessment
Subjective data include information concerning the patient's inability to control the urine. Determine factors related to the episodes of incontinence. Review voiding patterns and behaviors.
Collection of objective data requires alertness for clues that the patient is experiencing difficulty controlling the flow of urine. Follow the assessment guidelines to clarify the patient's complaints. Although more common in women, UI is a common symptom for men who have benign prostatic hypertrophy (BPH) and should be included in the assessment.
Medical Management
The management of incontinence depends on the underlying cause. If the problem arises from a disorder within the neck of the bladder, surgical repair may be necessary. Incontinence related to sphincter or urethral weakness may be treated with collagen implant injections. Injections promote bladder support by firming up the bladder neck or urethra (NLM, 2012). Temporary or permanent urinary diversion by an indwelling catheter may be indicated.
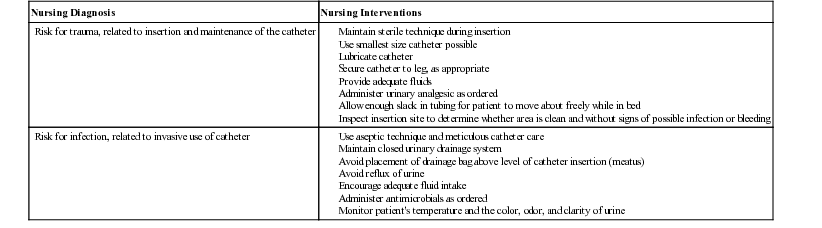
The pessary is a device that can be inserted into the vagina to support the bladder and to reduce pressure on the bladder from the uterus in cases of prolapse (Figure 49-6). This option is beneficial to those patients who are not candidates for surgery or pharmacological management. It may also be the first line of treatment before more aggressive management approaches are attempted.
Management of stress incontinence should include behavior modification, pelvic floor muscle therapies (Kegel exercises), medications, and mechanical devices before resorting to surgical procedures. If these strategies are not effective, surgical interventions offer other treatment options. One procedure is the transvaginal tape sling procedure. The surgeon passes a permanent polypropylene mesh tape, covered by a protective plastic sheath with stainless steel needles attached at each end, through a small incision in the anterior vaginal wall. The U-shaped sling supports the urethra during stress and increased intraabdominal pressure during routine activities. This procedure is not without difficulties. Careful patient teaching is important before any surgical treatment.
Estrogen replacement for the treatment of UI is controversial and its reported effectiveness varies. Topical administration of prednisone and estrogen may help restore turgor and elasticity of the vaginal submucosa. Transdermal oxybutynin (Oxytrol) is effective in reducing the symptoms of an overactive bladder with few side effects. A new self-catheterization system, the Self-Cath Closed System, is available for patients who must maintain intermittent self-catheterization. It is designed for patient convenience and minimization of bacterial contamination. An artificial urinary sphincter is a surgical option to reestablish continence, although there is controversy over its use.
Nursing Interventions
The incontinent patient may reduce fluid intake to decrease voiding, but without adequate fluids, urine may become more concentrated, irritating the bladder mucosa and increasing the urge to urinate. Therapeutic dietary modifications to assist in the management of urinary incontinence include avoidance of alcohol, caffeine, and spicy foods, which may be sources of bladder irritation, resulting in urgency and ultimately incontinence. Discuss timing of intake to avoid late hours just prior to retiring. Bladder training exercises may be implemented to improve the tone of the perineal muscles (Mayo Clinic, 2011). For the female patient, Kegel exercises are helpful; 10 repetitions, 5 to 10 times a day is suggested to improve muscle tone. Establish a 2-hour schedule for the patient to go to the bathroom. Once continence has been achieved, the goal may be raised to 3 hours.
Incontinence pads of various absorbencies are available in most grocery stores and pharmacies. They can increase the patient's confidence to participate in social activities. Use of protective undergarments may help keep the patient and the patient's clothing dry.
Many patients who are incontinent have low self-esteem. Be supportive by listening, encouraging the patient to express feelings, and providing kind reassurances. Never scold.
Neurogenic Bladder
Etiology and Pathophysiology
Neurogenic bladder means the loss of voluntary voiding control, resulting in urinary retention or incontinence. Neurogenic bladder is caused by a lesion of the nervous system that interferes with normal nerve conduction to the urinary bladder. The lesion may be caused by a congenital anomaly (e.g., spina bifida), a neurologic disease (e.g., multiple sclerosis), or trauma (as in spinal cord injury). The two types of neurogenic bladder are spastic and flaccid.
Spastic (reflex or automatic) bladder is caused by an upper motor neuron lesion (above the voiding reflex arc) that results in a loss of the urge to void and a loss of motor control. The bladder wall atrophies, decreasing bladder capacity. Urine is released on reflex, with little or no conscious control.
A flaccid (atonic, nonreflex) bladder, caused by a lower motor neuron lesion (below the voiding reflex arc), continues to fill and distend, with pooling of urine and incomplete emptying. Because of the accompanying loss of sensation, the patient may not experience discomfort that would indicate retention.
Clinical Manifestations
Identification of the disease process is the first step in assessing the potential problem of neurogenic bladder. Prevention of complications is a major concern; infection occurs from urinary stasis and repeated catheterization. Retention of urine may lead to backup of urine (reflux) into the upper urinary tract and to distention of structures of the urinary tract.
Assessment
Subjective data include patient complaints of diaphoresis, flushing, and nausea before reflex incontinence, or infrequent voiding.
Collection of objective data involves investigating the urinary status of the patient at risk for neurogenic bladder; this includes patients with a congenital anomaly, a neurologic disease, or a spinal cord injury. The patient with a spastic bladder experiences UI, whereas the patient with a flaccid bladder describes infrequent voiding.
Diagnostic Tests
To assess the type and extent of damage to the urinary tract, chemistry studies monitor any change in BUN and creatinine levels. Radiographic studies outline structural changes that occur.
Medical Management
Closely monitor patients identified as at risk for neurogenic bladder. Assess urinary function early in the course of treatment, and give antibiotics to treat signs of infection. The patient is aided by the use of parasympathomimetic medication (e.g., bethanechol) to increase the bladder's contractility. The patient may need to use intermittent self-catheterization or a urinary collection system if continence is not achieved.
Sacral nerve modulation (sacral neuromodulation) and stimulation.
A number of electronic devices to modulate nerve impulses are being used experimentally and in clinical practice for treating various bladder problems: urinary frequency, urgency, incontinence, chronic pain, and interstitial cystitis (IC).
Sacral nerve stimulation for urinary urge incontinence involves the use of a permanently implantable electrical stimulation device to change neuronal activity in the sacral efferent and afferent nerves to reduce urinary urge incontinence. The InterStim device, marketed by Medtronic Inc., delivers continuous low-level electrical impulses to the bladder and urethral sphincters via the sacral nerves. It corrects UI by modulating the neural reflexes, reducing stimulation to an overactive bladder, or by boosting stimulation to an underactive one. The mode of action of the impulses is unknown.
Four electrodes are connected to a battery-operated generator. The wire is inserted into the sacral foramen through a 2-cm incision. The end of the wire is tunneled across subcutaneous tissue, exits on the patient's back, and is connected to a temporary generator attached to the outside of the body. The patient tests this temporary implant for 1 to 2 weeks. If the patient achieves 50% continence, a permanent implant is put in place.
Nursing Interventions and Patient Teaching
The management goal for the patient with neurogenic bladder is to establish urinary elimination and prevent complications. Because neurologic function is disturbed, it may not be possible to reinstate normal voiding. The patient with a spastic bladder may be placed on a bladder training program, with self-stimulation used every 2 hours to empty the bladder: The patient tries to initiate voiding using bladder compressions by applying pressure to the abdomen suprapubically or by digital stimulation of the anal sphincter. Residual urine is then measured by catheterization. As the patient becomes more proficient in emptying the bladder, the time between catheterizations is increased until voiding is independent. It is important to educate the patient to be alert for signs of the bladder becoming distended.
Management of the patient with a flaccid bladder is similar. Place the patient on a 2-hour voiding schedule for bladder training. Issues of self-esteem are crucial for this patient to remain in social settings. Provide a supportive, sensitive environment for the patient to discuss ways to adapt to an altered self-image.
Inflammatory and Infectious Disorders of the Urinary System
Urinary Tract Infections
A UTI is caused by the multiplication of microorganisms in any urinary system structure. Infections may result from bacteria, viruses, or fungi. Bacteriuria (bacteria in the urine) is the most common of all nosocomial (hospital-acquired) infections. Escherichia coli is the most common pathogen. Risk factors associated with UTIs include instrumentation (catheterization, surgical manipulation, and invasive diagnostic testing such as a cystoscopy), diaphragm use, condom use, and conditions causing urinary stasis or retention. Immobility, sensory impairment, and multiple organ impairment may increase the chances of infection in older adults. Women are more susceptible to UTIs than men because the urethra is short and proximal to the vagina and rectum.
Etiology and Pathophysiology
UTIs are caused by pathogens that enter the urinary tract, and may or may not cause symptoms. Normally the flushing of the urinary tract with urine is sufficient to wash away pathogens. However, some conditions interfere with this process; urinary obstruction, neurogenic bladder, ureterovesical or urethrovesical reflux, sexual intercourse, and catheterization may introduce bacteria into the urinary system. Many chronic health problems predispose the patient to a UTI: diabetes mellitus, multiple sclerosis, spinal cord injuries, hypertension, and renal diseases.
Changes in urinary tract homeostasis allow the concentration of bacteria and increase the risk of infection. The patient with a compromised immune system does not seem to be predisposed to UTI infections, but once the infection is established, that patient has difficulty recovering. Infections of the lower urinary tract increase the risk of infection of the upper urinary tract, especially if untreated.
Gram-negative microorganisms that commonly infect the urinary tract (e.g., E. coli and Klebsiella, Proteus, or Pseudomonas organisms) are usually from the gastrointestinal tract and ascend through the urinary meatus. Normally the body's defenses keep infections in check and clear them from the system before signs and symptoms appear. If there is incomplete emptying of the bladder or reflux of urine, the retained urine supports growth of bacteria.
Clinical Manifestations
The common signs and symptoms associated with UTI are urgency, frequency, burning on urination, and hematuria that is microscopic to gross (visible without the aid of a microscope). UTIs are identified by the location of the infection: urethritis (urethra), cystitis (urinary bladder), pyelonephritis (kidney), and prostatitis (prostate gland). Infections of the bladder are said to be lower UTIs, whereas infections of the kidneys are upper UTIs.
Assessment
Subjective data include patient complaints of pain or burning on urination, urgency, frequency, and nocturia (excessive urination at night). The patient may also have related asthenia (a general feeling of tiredness and listlessness). Abdominal discomfort, perineal pain, or back pain may be present, depending on the extent of the disease process and site of infection.
Collection of objective data involves palpation of the lower abdomen, which may produce discomfort over the urinary bladder. Urine may be cloudy or blood tinged.
Diagnostic Tests
Urine culture and bacteriologic tests confirm the diagnosis. For patients with recurrent UTIs or systemic disease, more detailed urologic studies, such as an IVP and a voiding cystogram, are completed to assess the extent of involvement and damage to the structures of the urinary tract. Microscopic inspection of the urine often reveals bacteria, hematuria (blood in the urine), and pyuria (pus in the urine). Prostatitis is confirmed by patient history and culture of prostatic fluid or tissue.
Medical Management
The goal of medical management is to eliminate bacteria from the urinary tract, thereby relieving symptoms, preventing damage to renal structures, and preventing spread of infection to other body systems. The primary care provider prescribes antiinfective medications. Medications to treat uncomplicated urinary tract infections often include a 3-day regimen of sulfamethoxazole-trimethoprim (Bactrim, Septra) or ciprofloxacin (Cipro). Longer therapies for 7 to 10 days of amoxicillin or ampicillin, nitrofurantoin (Furadantin, Macrodantin), and levofloxacin (Levaquin) may also be prescribed. Most patients report symptom relief in 2 days (University of Maryland Medical Center, 2009). It is important to instruct patients to complete the full prescribed therapy to aid in the prevention of recurrence (Nickel, 2005). Many patients experience significant discomfort with voiding until the antiinfectives begin to take effect. Phenazopyridine (Pyridium) may be prescribed to manage the discomfort. Its use should be limited to 2 days. It will turn the urine's color to a bright orange hue (NLM, 2010).
Some individuals will experience recurrent infections. They may be placed on longer term prophylactic antibiotic therapies for an additional 6 months. If the infection is complicated by obstruction, that obstruction should be removed. For neurogenic bladder or other retention, intermittent catheterization permits urinary drainage (see Complementary and Alternative Therapies box).
 Complementary and Alternative Therapies
Complementary and Alternative Therapies
Urinary Disorders
• Cranberry (Cranberry Plus, Ultra Cranberry) has been used to prevent urinary tract infections (UTIs), particularly in women prone to recurrent infection. Studies supporting its use are limited. It has also been used to treat acute UTI. Monitor patients for lack of therapeutic effect.
• Echinacea stimulates the immune system and treats UTI. Patients with human immunodeficiency virus infections, including acquired immunodeficiency syndrome, tuberculosis, collagen disease, multiple sclerosis, or other autoimmune disease, should avoid its use. Echinacea should not be used in place of antibiotic therapy.
• Sea holly (Eryngium campestre), specifically the above-ground plant parts, have a mild diuretic effect. The roots have an antispasmodic effect. Above-ground parts are used in UTI and prostatitis; the roots are used to treat kidney and bladder calculi, renal colic, kidney and urinary tract inflammation, and urinary retention.
• Nettle (Urtica dioica) is currently being investigated as an irrigation for the urinary tract and also to treat benign prostatic hypertrophy. Patients with fluid retention caused by reduced cardiac or renal activity should not use this herb.
• Some believe that acupuncture applied to the abdominal meridian may help relieve cystitis.
• Some advocate massage with diluted rosemary, juniper, or lavender to aid in relieving pain associated with cystitis.
Nursing Interventions
Nursing interventions should be supportive, with patient education for adequate hydration and hygiene. Because these infections tend to recur or persist, patient education must include early detection. Comfort measures include a regimen of antiinfective agents, urinary analgesics (e.g., phenazopyridine [Pyridium]), adequate fluid intake, and perineal care. If treatment is effective, the patient should receive relief quickly. Infection may spread from the urinary system to other parts of the body. Urosepsis is septic poisoning due to retention and absorption of urinary products in the tissues.
Because of the high incidence of nosocomial UTIs, it is important that regular staff in service periodically review the basic procedures for catheter insertion and maintenance. Patient education for those who practice self-catheterization should include return demonstration to evaluate the success of maintaining clean technique.
Urethritis
Etiology and Pathophysiology
Urethritis, inflammation of the urethra, is classified by the presence or absence of gonorrhea. Nongonorrheal urethritis is called nonspecific urethritis (NSU). NSU may be caused by bacteria such as Chlamydia or by the protozoan Trichomonas. Viral causes include herpes simplex virus. Sensitivity to contraceptive spermicides may also result in urethritis. Bacteria are normally present in the urethra but do not cause problems unless the integrity of the mucous membrane or tissues is interrupted, as when a catheter is in place or trauma has occurred.
Clinical Manifestations
The clinical manifestations include inflammation of the urethra with pus formation in the mucus-forming glands within the urethral lining. With gonorrheal urethritis, acute infection of the mucous membrane of the urethra causes a purulent exudate from the meatus; the patient feels discomfort, frequency, and burning on urination.
Assessment
Subjective data vary, since the patient may be asymptomatic or may complain of dysuria, urethral pruritus, and urethral discharge. Women may complain of vaginal discharge or vulvar irritation.
Collection of objective data includes light palpation of the lower abdomen, which may produce discomfort over the urinary bladder. Inspection of the urethra may reveal purulent exudates or inflammation. Culture and sensitivity tests may be ordered (to identify the microorganism and the antibiotics to which it is sensitive, respectively); follow the institution's procedure.
Diagnostic Tests
Diagnostic tests are usually limited to a Gram stain of the exudate to identify the pathogen.
Medical Management
The first step in medical management is prevention of injury to the urethra during catheterization or sexual intercourse. Treatment is based on identifying and treating the cause and providing symptomatic relief. Drugs that may be prescribed are sulfamethoxazole-trimethoprim (Bactrim, Septra), metronidazole (Flagyl), clotrimazole (Mycelex), and nystatin (Mycostatin). Comfort measures include antibiotics, adequate fluid intake to flush the system, warm sitz baths, and special care of the perineum using clean technique.
Patients with continuous catheter drainage use either a bedside bag or a leg bag for urine collection. Studies are under way to test a drainage system designed with the bag worn around the waist. This experimental drainage system can be kept closed for 24 hours and offers improvements in ambulation, activities of daily living (ADLs), and social and mental well-being.
Nursing Interventions
Nursing interventions focus on patient education: Avoid sexual activity until the infection clears; take all medications, especially antibiotics, to ensure the infection is resolved; and use condoms for protection from reinfection. Instruct patients with sexually transmitted urethritis to refer their sexual partners for evaluation and testing if they had sexual contact in the 60 days preceding onset of the patient's symptoms or diagnosis.
Cystitis
Etiology and Pathophysiology
Cystitis is an inflammation of the wall of the urinary bladder, usually caused by urethrovesical reflux, introduction of a catheter or similar instrument, or contamination from feces. The most common microorganism causing acute cystitis is E. coli. Cystitis is most common in women because of the ease of entrance of pathogens through the short urethra, even during voiding. Conflicting data exist about the role of bubble baths, clothing, and hygiene in increasing the risk of cystitis in women. Cystitis in men usually occurs secondary to another infection, such as prostatitis or epididymitis (see Patient Teaching box).
 Patient Teaching
Patient Teaching
Cystitis
• Teach the patient to cleanse the perineal area from front to back to prevent contamination by spread of pathogens (especially E. coli) from the rectum to the short urethra.
• Encourage drinking 2000 mL of liquids per day unless contraindicated.
• Instruct the patient to take all prescribed medications even though symptoms may subside quickly.
• Remind the patient to empty the bladder as soon after intercourse as possible
• If UTIs are associated with intercourse, recommend cleansing the genitalia with soap and water prior to having sexual relations.
• Encourage showers instead of tub baths.
• Limit the use of bubble baths.
• Instruct the patient about early detection and testing with a urine test strip such as the Chemstrip 2 LN.
Clinical Manifestations
The common signs and symptoms associated with cystitis are dysuria, urinary frequency, and pyuria.
Assessment
Collection of subjective data includes assessment of the lower abdomen, which may produce discomfort over the urinary bladder. Patient complaints include burning on urination, dysuria, frequency, urgency, and nocturia. The urine may be cloudy, strong-smelling, or reflect hematuria. A low-grade fever may also be present (Mayo Clinic, 2012).
Collection of objective data includes a clean-catch or catheterized urinalysis with culture and sensitivity tests to aid in confirming the diagnosis and in determining the appropriate treatment.
Diagnostic Tests
Microscopic inspection of the urine often reveals bacteria and hematuria. A voiding cystogram may be used to identify reflux of urine into the bladder. Diagnosis is confirmed by a clean-catch, midstream urinalysis that reveals a bacterial count greater than 100,000 organisms/mL.
Medical Management
For cystitis without the complications of obstruction or other underlying pathologic conditions, medical management consists of short-term therapy with an antiinfective agent. If the treatment is effective, the patient should receive relief quickly. A repeat urinalysis 1 to 3 days after initiation of the medication confirms the effectiveness of the intervention.
Nursing Interventions and Patient Teaching
Nursing interventions focus on teaching that these infections tend to recur by either reinfection or persistent infection. Encourage the patient to drink 2000 mL of fluid per day. Record accurate I&O. Include early detection in the teaching. Long-term prophylaxis with low doses of medication may be necessary. A simple urine test, for example, the Chemstrip 2 LN, allows the patient to test the urine at the first sign of infection and to call the health care provider for a prescription.
Prognosis
Successful treatment depends on the patient's ability to adequately flush the urinary tract and complete the course of antibiotics prescribed.
Interstitial Cystitis
Etiology and Pathophysiology
Interstitial cystitis (IC) is a chronic pelvic pain disorder with recurring discomfort or pain in the urinary bladder and surrounding region. Up to an estimated 8 million Americans have interstitial cystitis. It can affect any age and gender, but it most commonly strikes women at age 30 to 40 years. The pathophysiology is unknown. Bacterial infection does not trigger it. It seems to be caused by a breech in the bladder's protective mucosal lining that allows urine to seep through to the bladder wall, resulting in pain, inflammation, and small vessel bleeding. The bladder wall is infiltrated by inflammatory cells, resulting in ulceration and scarring of the mucosa, spasm of the detrusor muscle, hematuria, urgency, frequency, and pain on urination (PubMed, 2012).
Diagnosing the condition may be challenging. It is often mistaken for a urinary tract infection, prostatitis, or overactive bladder. The diagnostic workup will involve ruling out other potential causes. The absence of bacteria in the urinalysis or a negative urine culture provides support to the diagnosis.
ADLs and personal relationships may be disrupted by voiding patterns; some patients report voiding 60 times a day.
Clinical Manifestations
The common signs and symptoms associated with IC are similar to those of cystitis: dysuria, urinary frequency, and microscopic bleeding. IC is characterized by urinary frequency, urgency, suprapubic pain, and dyspareunia (abnormal pain during sexual intercourse); it is often associated with fibromyalgia and irritable bowel syndrome. Autoimmune, allergic, and infectious etiologies are being studied
Assessment
Subjective data include complaints of discomfort over the urinary bladder, dysuria, frequency, urgency, and nocturia.
Collection of objective data includes assessment of the lower abdomen, which may produce discomfort over the urinary bladder and the lower quadrants of the abdomen. A clean-catch midstream sample for urinalysis is used to rule out infection. Cystoscopy and tissue biopsy are used to establish a differential diagnosis.
Medical Management
IC is difficult to treat. Pharmacological therapies are geared at symptom management. Antihistamines such as hydroxyzine pamoate (Vistaril), helps reduce urinary frequency. Amitriptyline (Elavil) and nortriptyline (Aventyl) are two antidepressants that reduce the burning pain and frequency of urination. The only oral medication approved by the U.S. Food and Drug Administration to treat the pain or discomfort of IC is pentosan polysulfate sodium. It improves the bladder's protective mucosal layer and relieves the pain of IC by decreasing the irritating effects of urine on the bladder wall. More invasive medication therapies may include dimethyl sulfoxide (DMA), heparin, or lidocaine instillation directly into the bladder. Nonpharmacological management strategies include biofeedback and physical therapy to manage spasms of the pelvic floor. Dietary therapies have also received some attention. Patients may benefit from diets that avoid foods and beverages known to cause bladder irritation. These foods include aged cheeses, alcohol, artificial sweeteners, chocolate, citrus juices, onions, soy, caffeine, and tomatoes.
Relief of symptoms takes time: it may be 4 weeks to 3 months before significant improvement occurs. For immediate relief, a brief course of opioid analgesics may be prescribed.
Surgical interventions include studies of the effect of sacral nerve root stimulation via implantation of electrodes; cystectomy, with the creation of a urostomy; and urinary diversion. Some patients continue to experience pain even after surgery.
Nursing Interventions and Patient Teaching
Nursing interventions focus on pain control and comfort measures. Because all medications have side effects, patients must consult their health care provider before taking any prescription or over-the-counter medication. Pelvic floor exercise may help decrease urgency and nocturia. Patients may be asked to keep a daily bladder diary; this information can be used to make treatment decisions.
Teaching about dietary choices should be included. A complete IC diet, self-management strategies, and other nonmedical management tools are available from the Interstitial Cystitis Association (www.ichelp.com).
IC is often associated with a reduced quality of life. Embarrassment, pain, and inability to manage elimination may lead to withdrawal from business, social, and intimate relationships. The patient and significant others need psychosocial support to face an uncertain outcome.
Prognosis
Only about half of patients with IC recover fully. Until researchers find a cause and an effective treatment, symptoms will continue.
Prostatitis
Etiology and Pathophysiology
Prostatitis, defined as inflammation and/or infection of the prostate gland, is actually a group of diseases. Bacterial prostatitis is caused by infectious organisms such as Pseudomonas organisms and S. faecalis traveling up the urethra. Nonbacterial prostatitis may result from a variety of conditions related to occlusion of the urethra, such as enlargement of the prostate gland.
Prostatodynia (pain in the prostate gland) manifests with neither inflammation nor infection but demonstrates the other symptoms typical of prostatitis.
Clinical Manifestations
The signs and symptoms vary in number and intensity. The patient may experience fever; chills; malaise; arthralgia; myalgia; perineal prostatic pain; dysuria; obstructive urinary tract symptoms, including frequency, urgency, dysuria, nocturia, hesitancy, weak stream, and incomplete voiding; low back pain; low abdominal pain; spontaneous urethral discharge; ejaculatory pain; and erectile dysfunction. Chronic bacterial prostatitis may be asymptomatic. Edema of the prostate gland may serve as an obstruction, causing urinary retention as a complication to the prostatitis. Pooling of urine may also foster stone formation. Other complications are epididymitis, pyelonephritis, and bacteremia (the presence of bacteria in the blood). The patient may be asymptomatic, but the symptoms of acute bacterial prostatitis are often the same as those of UTI, with pain in the low back, perineum, or rectum. The condition may become chronic.
Diagnostic Tests
Diagnosis is confirmed by patient history and culture of prostatic fluid or tissue. The expressed prostatic secretion (EPS) is considered useful in the diagnosis of prostatitis. EPS is obtained using a premassage and postmassage test. The patient is asked to void into a specimen cup just before and just after a vigorous prostate massage. Prostatic massage (for EPS) should be avoided if acute bacterial prostatitis is suspected, since compression is extremely painful and increases the risk of bacterial spread. Transabdominal ultrasound, MRI, or CT scan may be included in the diagnostic workup. A urinalysis and urine culture, WBC count, and blood cultures may also be performed.
Assessment
Subjective data include complaints of chills and low back and perineal pain. Chronic bacterial prostatitis causes dysuria; urgency; frequency; nocturia; and pain in the lower abdomen or back, perineum, or genitalia.
Collection of objective data involves assessing for elevated temperature and rectal palpation of the prostate gland by the health care provider, which may reveal it to be firm, edematous, and tender.
Medical Management
If the condition is infectious, management focuses on control of the infection and prevention of the complications of abscess formation or bacteremia. Patients with acute prostatitis who have a high fever or other signs consistent with impending sepsis will be hospitalized and prescribed intravenous antibiotics. Patients who are more stable are managed from home. Antibiotics commonly used for acute and chronic bacterial prostatitis include trimethoprim-sulfamethoxazole or fluoroquinolone. The course of therapy ranges from 2 to 4 weeks. Doxycycline or tetracycline may be prescribed for patients with multiple sex partners. Additional pharmacological needs may include antipyretics, urinary analgesics, analgesics, and stool softeners. Antiinflammatories are the most common agents used for pain control in prostatitis, but these provide only moderate pain relief. Opioid analgesics can be given, but cautiously, since this pain can be chronic. The pain resolves as the infection is treated.
Patients with chronic bacterial prostatitis are given oral antibiotic therapy for 4 to 16 weeks.
Nursing Interventions and Patient Teaching
Comfort measures used are analgesics, sitz baths, and stool softeners to reduce pain, edema, spasm, and straining pressure in the pelvis. Education will be needed concerning the medication regimen.
Warn the patient with acute prostatitis to avoid sexual arousal and intercourse so that the prostate can rest; however, intercourse may be beneficial in the treatment of chronic prostatitis. Follow-up with the health care provider is crucial because of the likelihood that the disorder will become chronic.
Prognosis
Prostatitis is difficult to cure and requires long periods of antibiotic treatment. Stress the importance of taking all the antibiotics prescribed, even after the initial symptoms have subsided.
Pyelonephritis
Etiology and Pathophysiology
Pyelonephritis is an inflammation of the structures of the kidney—the renal pelvis, renal tubules, and interstitial tissue. Pyelonephritis is almost always caused by E. coli. The kidney becomes edematous and inflamed, and the blood vessels are congested. The urine may be cloudy and contain pus (pyuria), mucus, and blood. Small abscesses may form in the kidney.
Pyelonephritis is usually seen in association with pregnancy; chronic health problems such as diabetes mellitus, or polycystic or hypertensive renal disease; insult to the urinary tract from catheterization; or infection, obstruction, or trauma. Careful management of these disorders is important to prevent pyelonephritis.
Clinical Manifestations
Acute pyelonephritis may be unilateral or bilateral, causing chills, fever, prostration, and flank pain. Repeated episodes of pyelonephritis lead to a chronic disease pattern, with atrophy of the kidney as the nephrons are destroyed. Azotemia (the retention of excessive amounts of nitrogenous compounds in the blood) develops if enough nephrons are nonfunctional.
Assessment
Subjective data in acute pyelonephritis include a patient who is acutely ill, with malaise and pain in the costovertebral angle (CVA) (the angle formed on either side of the patient's back by the twelfth rib and spinal column; the patient's kidneys lie just under the CVA). CVA tenderness to percussion is a common finding in pyelonephritis. In the chronic phase the patient may show unremarkable symptoms, such as nausea and general malaise.
Collection of objective data includes assessing the patient for signs of infection: elevated temperature, vomiting, and chills. The chronic disease results in systemic signs: elevated blood pressure and gastrointestinal irritation such as vomiting and diarrhea.
Diagnostic Tests
Diagnosis is confirmed by the presence of bacteria and pus in the urine, varying degrees of hematuria, WBCs and WBC casts in the urine (indicating involvement of the renal parenchyma), and leukocytosis. A clean-catch or catheterized urinalysis with culture and sensitivity tests identifies the pathogen and determines appropriate antimicrobial therapy. To prevent spread of infection in the early stages of acute pyelonephritis, imaging examinations, such as an intravenous pyelogram (IVP) or CT scan requiring injection of contrast materials, are usually not performed. Ultrasound of the urinary system is often done to identify anatomical abnormalities such as renal abscesses, obstructing calculus, or hydronephrosis. BUN and creatinine levels of the blood and urine may be assessed to monitor kidney function.
Medical Management
The patient with mild signs and symptoms may be treated on an outpatient basis with antibiotics for 14 to 21 days. Parenteral (intravenous) antibiotics are often given initially in the hospital to establish high serum and urinary medication levels. When initial treatment resolves the acute symptoms and the patient is able to tolerate oral fluids and medications, he or she may be discharged on a regimen of oral antibiotics for an additional 14 to 21 days. Antibiotics are selected according to results of urine culture and sensitivity tests and may include broad-spectrum medications such as ampicillin or vancomycin combined with an aminoglycoside (e.g., tobramycin [Nebcin], gentamicin [Garamycin]); other treatment options include trimethoprim-sulfamethoxazole and fluoroquinolones such as ciprofloxacin and ofloxacin.
Adequate fluids (at least eight 8-ounce glasses per day) are encouraged. Urinary analgesics such as phenazopyridine are helpful. Follow-up urine culture is indicated.
Nursing Interventions and Patient Teaching
Nursing diagnoses and interventions for the patient with pyelonephritis include but are not limited to the following.
| Nursing Diagnosis | Nursing Interventions |
| Risk for infection, related to bacteria in the urinary tract | |
| Health-seeking behaviors, related to desire for prevention of further renal disease |

Teach the patient to identify the signs and symptoms of infection: elevated temperature, flank pain, chills, fever, nausea and vomiting, urgency, fatigue, and general malaise. Also teach the patient indications, dose, length of course, and side effects of the medications. Emphasize the importance of follow-up care with the health care provider on a routine basis and when signs of infection arise.
Prognosis
Prognosis depends on early detection and successful treatment. Baseline assessment for every patient must include urinary assessment because pyelonephritis can occur as a primary or secondary disorder (a condition resulting from complications of another disorder).
Obstructive Disorders of the Urinary Tract
Urinary Obstruction
Etiology and Pathophysiology
Obstruction at any point within the urinary tract can adversely affect function and alter structure. Causes of obstruction include strictures, kinks, cysts, tumors, calculi, and prostatic hypertrophy. Obstruction may lead to alterations in blood chemistry; infection, which thrives as a result of urine stasis; ischemia due to compression; or atrophy of renal tissue.
Clinical Manifestations
The patient may be unaware of any problems at first if the obstruction is partial, allowing urine to drain and kidney function to remain within normal limits. With prostatic hypertrophy the obstructive process may be so gradual that the patient ignores the vague symptom of dull flank pain and seeks medical attention only when urination becomes acutely difficult. Acute pain occurs as the musculature is stretched by increasing pressure from urine accumulation and as muscular contractions increase in an attempt to move urine past the obstruction. This acute pain is called renal colic and is a classic symptom of renal calculi.
Assessment
Subjective data include the patient's cardinal complaint of a sensation of needing to void but only being able to void small amounts. Pain may range from dull flank pain to acute, incapacitating pain. Nausea often accompanies acute pain.
Collection of objective data includes noting on physical assessment whether the bladder is palpable suprapubically because of urine retention. The affected kidney may also be palpable. Retention with overflow occurs when the patient is unable to completely empty the urinary bladder and it quickly refills, causing the urge to void again. Assess time and amount of voidings.
Diagnostic Tests
As a quick evaluation, the health care provider may order a KUB radiograph. Renal ultrasonography or IVP provides definitive information about structural changes. Other diagnostic tests may include visual examinations with the aid of endoscopy, and a blood chemistry profile.
Medical Management
Initial intervention is aimed at establishing urine drainage and relieving discomfort. Conservative measures include inserting an indwelling catheter and administering an analgesic (usually opioid) and an anticholinergic agent (atropine) to decrease smooth muscle motility. It may be necessary to establish urine drainage surgically by inserting a catheter directly into the bladder through the abdominal wall (suprapubic cystostomy), into a ureter (ureterostomy), or into the kidney (nephrostomy).
Surgical correction of an obstruction in the urinary system may involve a tube, called a stent. Stent insertion is used for patients who are poor operative risks. A meshlike tube or coil-shaped device is inserted through an endoscope into the ureter. The stent holds the tubular structure open to facilitate drainage. Stents may be permanent or temporary. Closely monitor the patient for signs of infection, obstruction, and pain.
Nursing Interventions
After surgery, observe the patient for hemorrhage, provide aseptic care of the surgical site, and provide a safe environment to prevent injury and infection.
Prognosis
The prognosis varies, depending on the cause of the obstruction. If surgical correction is successful, the prognosis is excellent.
Hydronephrosis
Etiology and Pathophysiology
Hydronephrosis (dilation of the renal pelvis and calyces) may be congenital or may develop at any time. It can occur unilaterally or bilaterally. Hydronephrosis is caused by obstructions in the lower urinary tract, the ureters, or the kidneys. The location of the obstruction determines whether one or both kidneys are affected. Potential causes may include renal calculi, tumors, strictures, vesicoureteric reflux, and scarring (Figure 49-7).
An obstruction generates pressure from accumulated urine that cannot flow past it. This pressure may cause functional and anatomical damage to the renal system. The renal pelvis and ureters dilate and hypertrophy. This pressure, if prolonged, causes fibrosis and loss of function in affected nephrons. If the condition is left untreated, the kidney may be destroyed.
Clinical Manifestations
Hydronephrosis can occur without any symptoms as long as kidney function is adequate and urine can drain. The amount of pain is proportional to the rate of stretching of urinary tract structures. Slowly developing hydronephrosis may cause only a dull flank pain, whereas a sudden occlusion of the ureter, such as from a calculus, causes a severe stabbing (colicky) pain in the flank. Nausea and vomiting, which often accompany hydronephrosis, are a reflex reaction to the pain and usually subside when the pain is controlled.
Assessment
Subjective data include patient reports of pain, including location, intensity, and character, and nausea. Discuss the patient's voiding pattern: frequency, difficulty starting a stream of urine, dribbling at the end of micturition (voiding), nocturia, and burning on urination. Note any history of obstructive disorders.
Collection of objective data includes assessing the patient suspected of having hydronephrosis for vomiting, hematuria, urinary output, edema, a palpable mass in the abdomen, bladder distention (detected on palpation), and tenderness over the kidneys or bladder.
Diagnostic Tests
A urinalysis and serum kidney function studies that include measurement of urea and creatinine are obtained. Cystoscopy may be performed with or without retrograde pyelogram. Radiographic examinations may include IVP or IVU, KUB radiograph, CT scan, or ultrasound evaluation. Sometimes a renal biopsy is performed.
Medical Management
Management is usually conservative if the condition is not severe. Surgery relieves the obstruction and preserves kidney function. If the kidney is severely damaged, a nephrectomy may be necessary. If infection is present, antiinfective medications are administered: penicillin in combination with sulfisoxazole (Gantrisin) or sulfamethoxazole-trimethoprim (Bactrim). Opioids, such as morphine and meperidine, in combination with antispasmodic drugs, such as propantheline (Pro-Banthine) and belladonna preparations, are usually necessary to relieve severe, colicky pain.
Nursing Interventions and Patient Teaching
Nursing interventions for the patient with hydronephrosis include administering medications as ordered, monitoring I&O, observing for signs and symptoms of infection, and monitoring vital signs. Encourage the patient to take fluids, and assess the patient for pain. Keep any drainage tubes open and anchored to avoid inadvertent displacement. If a catheter is present, provide catheter care. If surgery has been performed, observe the dressing because drainage of urine may continue for some time. Keep the area clean and dry to avoid excoriation of the skin. Explain all procedures to the patient and the family.
Patient teaching includes explaining the abnormality and the signs and symptoms of infection or obstruction. Describe measures to prevent infection, such as adequate fluid intake, perineal hygiene daily with mild soap and water (drying thoroughly), and regular emptying of the bladder.
Prognosis
Prognosis depends on the degree of urinary system destruction and the need for surgical intervention.
Urolithiasis
Urolithiasis (formation of urinary calculi) can develop in any area of the urinary tract. Urolithiasis is a general term that encompasses all urinary calculi, but specific names are also used to indicate where they are located or formed: nephrolithiasis (formation of a kidney stone, or nephrolith), ureterolithiasis (formation of a stone in the ureter, or ureterolith), and cystolithiasis (a bladder stone, or cystolith). Another descriptive term is lithogenesis (the formation of stones).
Etiology and Pathophysiology
Urolithiasis occurs when minerals precipitate out of solution and adhere, forming stones that vary in size and shape. The event that initiates stone formation remains unknown. Factors predisposing individuals to urolithiasis include immobility, hyperparathyroidism (in which calcium leaves the bones and accumulates in the bloodstream), or have recurrent UTIs. Dietary influences may contribute to stone development. Thorough assessment and analysis of the composition of the stones guide medical and nursing management.
Clinical Manifestations
Symptoms depend on the stones' size and degree of mobility. The patient with renal colic seeks care immediately, whereas a person with a less mobile stone may not seek assistance until signs of infection or hydronephrosis occur.
Assessment
Subjective data include the patient with mobile calculi complaining of intractable pain (pain that is unrelieved by ordinary medical measures and is usually accompanied by nausea and vomiting). The patient describes the pain as starting in the flank and radiating into the groin, the genitalia, and the inner thigh. The patient with a less mobile stone may develop signs and symptoms associated with UTI secondary to hydronephrosis.
Collection of objective data includes assessing for hematuria and vomiting.
Diagnostic Tests
Diagnostic tests include KUB and IVP or IVU radiography, ultrasound, cystoscopy, and urinalysis. Other tests may be ordered to determine stone content, presence of infection, and alterations in blood chemistry that influence stone formation. Twenty-four-hour urine examination may be done to detect abnormal excretion of calcium oxalate, phosphorus, or uric acid.
Medical Management
Stone removal and pain management are the primary goals of treatment. Antiinfective agents may be administered to treat infection or prophylactically. If stones are not passed, invasive techniques may be indicated (Figure 49-8). Stones in the lower tract can be removed by cystoscopy with stone manipulation or by surgical incision. Terminology describes the location: ureterolithotomy, pyelolithotomy, and nephrolithotomy. Chemolytic agents, either alkylating or acidifying agents, may be instilled to dissolve stones.
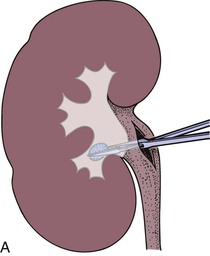
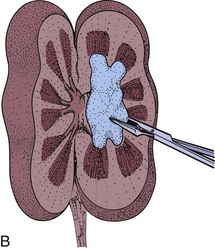
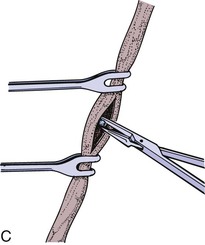
Extracorporeal shock wave lithotripsy is an alternative to surgery. The patient is submerged in a special tank of water, and ultrasonic shock waves are used to pulverize the stone. Urine must still be strained, even if a catheter is in place. Renal colic may occur as the patient passes the stone fragments.
Long-term management may include dietary adjustments to alter urine pH or to decrease the availability of certain substances that cause stone formation. Moderate reduction of foods containing calcium, phosphorus, and purine may help when stones are caused by metabolic abnormalities. Foods to avoid include cheese, greens, whole grains, carbonated beverages, nuts, chocolate, shellfish, and organ meat. Daily fluid intake of 2000 mL (unless clinically contraindicated) helps cleanse the urinary tract.
Drug therapy depends on stone composition. To prevent calcium stone formation, sodium cellulose phosphate is taken; it binds with ingested calcium and prevents its absorption. Aluminum hydroxide gel binds with excess phosphorus, allowing intestinal excretion rather than urinary excretion; and allopurinol (Zyloprim) reduces serum urate levels, thereby facilitating reabsorption of urate crystals.
Nursing Interventions and Patient Teaching
Physical activity and hydration will facilitate stone passage. The patient may require opioid medications to manage the pain. If analgesics are given, provide assistance with ambulation. If the patient is unable to tolerate sufficient oral intake, intravenous fluids may be prescribed. All urine is strained. Any stones or “gravel” noted must be sent to the laboratory for analysis. Assess urine for possible hematuria. Monitor BUN and creatinine for indications of continuing urinary tract obstruction.
Nursing diagnoses and interventions for the patient with urolithiasis include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Risk for infection, related to bacteria in the urinary tract | |
| Health-seeking behaviors, related to desire for prevention of further renal disease |

Discuss the prescribed diet, including fluid intake, and home medications (their purpose, dosage, refills, and side effects). The patient should avoid inactivity by walking frequently. Emphasize the need for follow-up with the health care provider, including keeping scheduled appointments and reporting difficulty with urination.
Although opinions vary greatly as to benefits of dietary restrictions, the nurse may be responsible for clarifying diet instructions. Encourage a fluid intake of at least 2000 mL in 24 hours, unless contraindicated. People who are calcium stone formers may need to curtail their intake of dietary calcium (dairy products, antacids) to within minimum recommended dietary allowance guidelines. New research on the impact of diet on the development of calcium oxalate kidney stones concludes that restricting consumption of animal protein and salt in combination with normal calcium intake reduces the risk of kidney stones better than the traditional low-calcium diet.