Care of the Patient With an Endocrine Disorder
Objectives
Anatomy and Physiology
1. List and describe the endocrine glands and their hormones.
3. Explain the action of hormones on their target organs.
4. Describe how the hypothalamus controls the anterior and posterior lobes of the pituitary gland.
Medical-Surgical
5. Discuss the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, nursing interventions, patient teaching, and prognosis for patients with acromegaly, gigantism, dwarfism, diabetes insipidus, syndrome of inappropriate antidiuretic hormone, hyperthyroidism, hypothyroidism, goiter, thyroid cancer, hyperparathyroidism, hypoparathyroidism, Cushing's syndrome, and Addison's disease.
6. Explain how to test for Chvostek's sign, Trousseau's sign, and carpopedal spasms.
7. List two significant complications that may occur after thyroidectomy.
8. Describe the etiology and pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, nursing interventions, patient teaching, and prognosis for the patient with diabetes mellitus.
9. Differentiate between the signs and symptoms of hyperglycemia and hypoglycemia.
10. Differentiate among the signs and symptoms of diabetic ketoacidosis, hyperglycemic hyperosmolar nonketotic coma, and hypoglycemic reaction.
11. Explain the roles of nutrition, exercise, and medication in the control of diabetes mellitus.
12. Discuss how the various classes of oral hypoglycemic medications work to improve the mechanisms by which insulin and glucose are produced and used by the body.
13. Discuss the various insulin types and their characteristics.
14. Describe the correct way to draw up and administer insulin.
15. Discuss the acute and long-term complications of diabetes mellitus.
Key Terms
http://evolve.elsevier.com/Cooper/foundationsadult/
Anatomy and Physiology of the Endocrine System
Endocrine Glands and Hormones
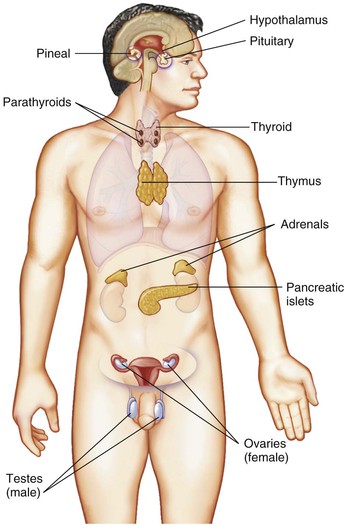
A gland is a specialized group of cells and tissues that work together to produce and secrete substances such as hormones, enzymes, or other bodily components. Glands can be divided into two broad categories: exocrine and endocrine. Exocrine glands secrete through a series of ducts (sebaceous and sudoriferous glands of the skin). Their secretions are protective and functional. Endocrine glands are ductless, as they release their secretions directly into the bloodstream. Their secretions have a regulatory function. Both endocrine and exocrine glands control homeostasis by communicating with and regulating their assigned body functions. The hormones secreted by the endocrine system work closely with the nervous system. Hormones are chemical messengers that travel through the bloodstream to their target organs. Metabolic changes occur in response to the actions of hormones.
The total weight of all the endocrine glands is less than half a pound, yet they have a powerful influence. The slightest change in hormonal levels can upset the metabolic balance of the entire body. Hormones can increase or decrease a normal body process by affecting a target organ. Actions of hormones are interrelated. Increases or decreases in a single hormone can significantly impact the actions of other hormones. The endocrine glands (Figure 50-1) have a generalized effect on the patient's metabolism, growth, development, reproduction, and many other bodily activities such as temperature, fluid balance, and emotional responses.
The amount of hormone released is controlled by negative feedback inhibition (in which a gland releases a hormone, which stimulates target cells to release a second hormone; the gland slows the release of its hormone as it senses the amount of the second hormone increasing). Information is constantly being exchanged via the bloodstream between target organs and endocrine glands such as the pituitary gland.
Pituitary Gland
The pea-sized pituitary gland (hypophysis) is one of the most powerful glands in the body. It has been called the “master gland” because, through negative feedback, it controls the other endocrine glands. It works closely with the hypothalamus of the brain and is located in a cranial cavity in a small saddle-like depression in the sphenoid bone. It is divided into two segments: the anterior pituitary (adenohypophysis) and the posterior pituitary (neurohypophysis). Each segment produces specialized hormones. The hypothalamus actually produces the hormones of the posterior pituitary and releases them for storage in the posterior pituitary gland; they are released from there as a result of nerve impulses received from the hypothalamus.
Anterior pituitary gland.
Six major hormones are secreted by the anterior pituitary gland:
1. Somatotropin, or growth hormone (GH)
2. Adrenocorticotropic hormone (ACTH)
3. Thyroid-stimulating hormone (TSH)
4 and 5. Gonadotropic hormones: Follicle-stimulating hormone (FSH) and luteinizing hormone (LH)
These hormones make up about 75% of the gland's total weight. The first five hormones in the list are called tropic hormones, because they are responsible for the stimulation of other endocrine glands. Prolactin, the remaining hormone, has a more direct effect: it causes the mammary glands to produce milk. These hormones and their functions are shown in Figure 50-2.
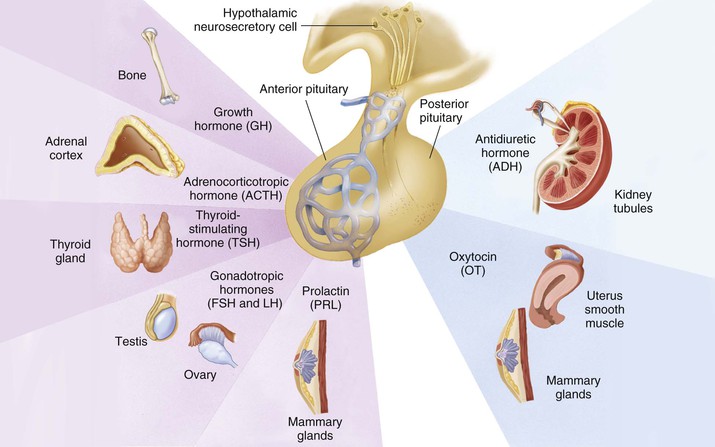
Posterior pituitary gland.
Two hormones are released by the posterior pituitary when the hypothalamus stimulates their release. They are oxytocin and antidiuretic hormone (ADH) (see Figure 50-2). Oxytocin promotes the release of milk and stimulates uterine contractions during labor. ADH, also called vasopressin, causes the kidneys to conserve water by decreasing the amount of urine produced. ADH/vasopressin also causes constriction of the arterioles in the body and a pressor effect, which results in increased blood pressure.
Thyroid Gland
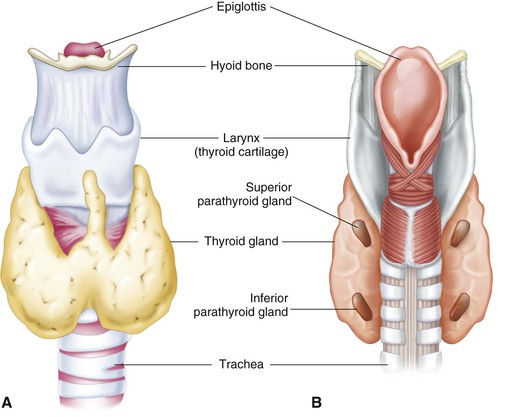
The thyroid gland is butterfly shaped, with one lobe lying on either side of the trachea just below the larynx (Figure 50-3). The lobes are connected by the isthmus. The gland is very vascular and receives approximately 80 to 120 mL of blood per minute.
The thyroid gland secretes the hormones thyroxine (T4) and triiodothyronine (T3). Adequate oral intake of iodine is necessary for the formation of thyroid hormones. These hormones regulate three main functions: (1) growth and development, (2) metabolism, and (3) activity of the nervous system. Their function is controlled by the release of thyroid-stimulating hormone (TSH) from the pituitary gland.
Calcitonin is a hormone also released by the thyroid gland. It decreases blood calcium levels by causing calcium to be stored in the bones.
Parathyroid Glands
The four parathyroid glands are located on the posterior surface of the thyroid gland (see Figure 50-3) and secrete parathyroid hormone (PTH, parathormone). As an antagonist to calcitonin from the thyroid, PTH tends to increase the concentration of calcium in the blood. It also regulates the amount of phosphorus in the blood.
The delicate balance of calcium in the blood is extremely important for normal body function. When calcium blood levels are low, the nerve cells become excited and stimulate the muscles with too many impulses, resulting in spasms (tetany). When blood calcium levels are abnormally high, heart function becomes impaired; this can result in death. Under the influence of PTH, two changes occur in the kidneys: It increases the reabsorption of calcium and magnesium from the kidney tubules and accelerates the elimination of phosphorus in the urine.
 Adrenal Glands
Adrenal Glands
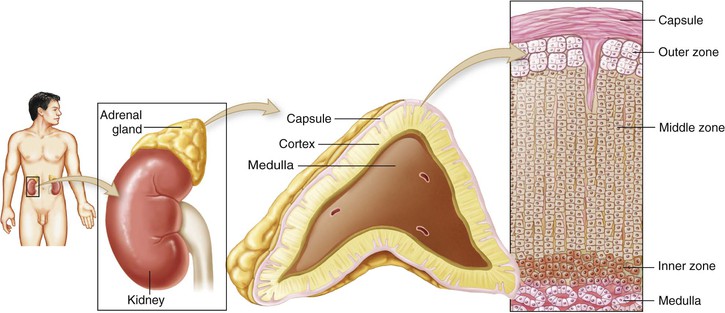
The adrenal glands (suprarenal glands) are small, yellow masses that lie atop the kidneys. Both glands contain an outer section, the adrenal cortex, and a smaller inner section, the adrenal medulla (Figure 50-4).
Adrenal cortex.
The adrenal cortex is divided into three separate layers. Each layer secretes a particular hormone, called a steroid:
• Mineralocorticoids are secreted by the outer zone (zona glomerulosa): These are primarily involved in water and electrolyte balance and indirectly manage blood pressure. Aldosterone, the principal mineralocorticoid, regulates sodium and potassium levels by affecting the renal tubules. It decreases the level of potassium and increases the level of sodium in the bloodstream. The retention of sodium causes retention of water, which leads to an increase in blood volume and blood pressure.
• Glucocorticoids are secreted by the middle zone (zona fasciculata): The most important of these is cortisol, which is involved in glucose metabolism and provides extra reserve energy in times of stress. Glucocorticoids also exhibit antiinflammatory properties.
• Sex hormones are secreted by the inner zone (zona reticularis): Androgens are male hormones and estrogens are female hormones. In the adult the adrenal glands release a relatively small amount of these hormones, which have an insignificant impact on the system.
Adrenal medulla.
The cells composing the adrenal medulla arise from the same type of cells as the sympathetic nervous system. Two hormones are released during times of stress: (1) epinephrine (adrenaline), and (2) norepinephrine. They cause the heart rate and blood pressure to increase, the blood vessels to constrict, and the liver to release glucose reserves for immediate energy. This is a systemic preparation of the body for a “fight-or-flight” response needed in times of crisis.
Pancreas
The pancreas is an elongated gland that lies posterior to the stomach. It is an active organ, composed of both exocrine and endocrine tissue. The endocrine tissue of the pancreas contains more than a million tiny clusters of cells known collectively as the islets of Langerhans. These cells secrete two major hormones. The first, insulin, is secreted by the beta cells in response to increased levels of glucose in the blood. Insulin's secretion pattern is a physiologic example of negative feedback between insulin and glucose. Elevated blood glucose levels stimulate the pancreas to secrete insulin. The stimulus for insulin secretion decreases as blood glucose levels decrease. The homeostatic mechanism is considered negative feedback because it reverses the change in blood glucose level. The second pancreatic hormone is glucagon, which is secreted by the alpha cells in response to decreased levels of glucose in the blood. Insulin and glucagon play a major role in carbohydrate, fat, and protein metabolism.
Female Sex Glands
Deep in the lower abdominal region, lying to the left and right of the uterus, are two almond-shaped ovaries, the major female sex glands. At puberty the ovaries begin producing two hormones: estrogen (responsible for the development of secondary sex characteristics, such as axillary hair and pubic hair, and for maturation of the reproductive organs) and progesterone (continues the preparation of the reproductive organs that was initiated by estrogen). (See Chapter 51 for more information.)
The placenta is a temporary endocrine gland that forms and functions during pregnancy. During this time the ovaries become inactive and the placenta releases the estrogen and progesterone needed to maintain the pregnancy. (For a more in-depth discussion, refer to Chapter 51.)
Male Sex Glands
Suspended outside the body in the scrotum, a saclike structure, are the two oval sex glands called the testes. They release the hormone testosterone, which is responsible for the development of the male secondary sex characteristics, including axillary, pubic, and facial hair; maturation of the reproductive organs; deepening of the voice; and development of muscle and bone mass. Testosterone is necessary for sperm formation.
Thymus Gland
The thymus gland lies in the upper thorax, posterior to the sternum (see Figure 50-1). It produces the hormone thymosin, which plays an active role in the immune system. T lymphocytes (a type of white blood cell) are stimulated to carry out immune reactions to certain types of antigens. The thymus gland programs this information into the T lymphocytes in utero and during the first few months of life.
Pineal Gland
The pineal gland is a small, cone-shaped gland located in the roof of the third ventricle of the brain (see Figure 50-1). It secretes the hormone melatonin, which seems to inhibit reproductive activities by inhibiting the gonadotropic hormones. This is particularly important in preventing the sexual maturation of the child's body until adulthood. It is thought to induce sleep, may affect mood, and has an impact on menstrual cycles.
Disorders of the Pituitary Gland (Hypophysis)
Acromegaly
Etiology and Pathophysiology
An overproduction of somatotropin (growth hormone [GH]) after the onset of puberty causes acromegaly, a condition that affects an estimated 6 people per 100,000 (National Library of Medicine [NLM], 2011a). The cause may be either (1) idiopathic hyperplasia (an increase in the number of cells, without a known cause) of the anterior lobe of the pituitary gland or (2) tumor growth. Unfortunately, growth changes that occur in acromegaly are irreversible, even with adequate medical or surgical intervention.
Clinical Manifestations
Manifestations of acromegaly begin gradually, usually in the third or fourth decade of life. Typically an average of 7 to 9 years passes between the initial onset of signs and symptoms and final diagnosis. The subsequent overabundance of GH produces many changes throughout the patient's body, including enlarged cranium and lower jaw, separated and maloccluded teeth, bulging forehead, bulbous nose, thick lips, enlarged tongue, and generalized coarsening of the facial features (Figure 50-5). Enlargement of the tongue results in speech difficulties, and the voice deepens as a result of hypertrophy of the vocal cords. The hands and feet grow larger; the fingertips develop a tufted or clubbed appearance. There is enlargement of the heart, liver, and spleen. Muscle weakness usually develops. Joints may hypertrophy and become painful and stiff. Male patients may become impotent, and female patients may develop a deepened voice, increased facial hair, and amenorrhea (lack of menstrual cycles). If a tumor is present, pressure on the optic nerve may cause partial or complete blindness. Visual disturbances are often a first sign of acromegaly. Severe headaches are common.


Assessment
Subjective data include headaches or visual disturbances and painful, stiff joints. Evaluate muscle weakness and its effect on the patient's ability to perform activities. Encourage patients to share their emotional responses to sexual problems (such as impotence in men and masculinization in women). Particular attention should be given to the emotional distress associated with the physical changes often assessed with the development of acromegaly.
Collection of objective data includes ongoing assessment of bone enlargement and joint involvement, as evidenced by gait changes and decreasing ability to perform activities. Changes in vital signs that may herald the onset of early heart failure include dyspnea, tachycardia, weak pulse, and hypotension. The patient's fluid volume status should be assessed with each interaction. After surgical removal of the pituitary tumor, the patient is at risk for diabetes insipidus. If the posterior pituitary gland was damaged during surgery, it may cause a lack of ADH; diabetes insipidus is a condition in which the kidneys do not conserve water properly. Hypertension, heart failure, and cardiomyopathy are possible complications secondary to enlargement of the heart and other organs.
Diagnostic Tests
Diagnosis of acromegaly is based on the history and clinical manifestations, computed tomography (CT) scan, magnetic resonance imaging (MRI), and cranial radiographic evaluation. A complete ophthalmologic examination, including visual fields, is usually performed because a large tumor of the pituitary gland potentially causes pressure on the optic nerves or optic chiasm (where the optic nerves cross, just in front of the pituitary gland). Laboratory tests confirm elevated levels of serum GH and plasma insulin-like growth factor-1. The definitive test for acromegaly is the growth hormone suppression test (Mayo Clinic, 2013). The GH concentration normally falls during this challenge test, but in acromegaly these levels do not fall. Note: Restrict the patient's oral intake for 10 to 12 hours before this test (NLM, 2011b).
Medical Management
Medical treatments include dopamine agonists such as cabergoline (Dostinex) and somatostatin analogs (which inhibit GH), such as octreotide (Sandostatin, Sandostatin LAR Depot) (Table 50-1), especially in patients who are not candidates for surgery or radiation therapy. These drugs are used in an attempt to suppress GH secretion. Surgical treatment to remove pituitary tumors associated with acromegaly is accomplished with the transsphenoidal removal of tumor tissue. The goal of transsphenoidal surgery is to remove only the tumor that is causing GH secretion. Irradiation procedures using proton beam therapy have been used to destroy GH-secreting tumors. Proton beam treatment uses very low doses of radiation and therefore is much less destructive to adjacent tissues, such as the hypothalamus and temporal lobes, than conventional radiation therapy.
 Table 50-1
Table 50-1
Medications for Endocrine Disorders
| GENERIC NAME (TRADE NAME) | ACTION | SIDE EFFECTS | NURSING IMPLICATIONS |
| bromocriptine (Parlodel) | Inhibits prolactin secretion; lowers serum levels of growth hormone, dopamine receptor agonist | Nausea, headache, dizziness, abdominal cramping, orthostatic hypotension | Give with meals to prevent GI effects; change positions carefully to prevent orthostatic hypotension; contraindicated with hypersensitivity to ergot derivatives |
| Calcium salts (gluconate, lactate, chloride gluceptate) | Calcium electrolyte replacement | Hypercalcemia, phlebitis, necrosis, and burning at IV site; bradycardia, hypotension, and dysrhythmias with rapid IV administration | Monitor cardiac status and blood pressure and for extravasation when giving intravenously |
| fludrocortisone (Florinef) | Adrenal corticosteroid with mineralocorticoid activity; promotes sodium and water retention | Hypertension, edema, sweating, rash, hypokalemia | Monitor for hypokalemia and fluid retention or depletion; do not discontinue abruptly; patient should carry identification signaling use |
| levothyroxine (Eltroxin, Synthroid, Levothroid) liothyronine (Cytomel) liotrix (Thyrolar) thyroid (Thyrar, Armour Thyroid) | Thyroid hormone replacement | Most side effects due to therapeutic overdose; include anxiety, insomnia, headache, hypertension, tremors, angina, dysrhythmias, tachycardia, menstrual irregularities | Give in morning to minimize insomnia; use caution in older adults or patients with coronary artery disease; monitor for signs of overdose; do not switch brands unless instructed |
| mitotane (Lysodren) | Adrenal cytotoxic agent; reduces production of adrenal steroids | Anorexia, nausea, vomiting, diarrhea, lethargy, somnolence, vertigo, rash | Tell patient to use contraception; instruct patient to use caution when driving or performing tasks requiring alertness; monitor for dehydration |
| Potassium iodide (SSKI) | Blocks release of thyroid hormone in thyroid storm and hyperthyroidism; also used as an expectorant | Hypersensitivity reactions, rash, metallic taste, burning in mouth or throat, GI irritation, headache, parotitis, hyperkalemia | Do not use in pregnant women; mix with fruit juice to mask taste |
| Somatostatin analogs: octreotide (Sandostatin) | Inhibits growth hormone secretion; suppresses secretion of serotonin, gastroenteropancreatic peptides; enhances fluid and electrolyte absorption from the GI tract; used to treat carcinoid tumors, VIPomas,* and high-output fistulas† | Nausea, diarrhea, abdominal pain, headache, injection site discomfort, hyperglycemia, hypoglycemia | SubQ route of administration is preferred, but may also be given IV |
| Antidiuretic hormone: vasopressin (Pitressin) | Synthetic pituitary hormone with antidiuretic effects on the kidney (used to treat diabetes insipidus); also a potent vasoconstrictor (used to treat bleeding esophageal varices) | Nasal irritation and congestion with nasal preparations; hypertension; ischemia of heart, mesenteric organs, and kidneys; angina; myocardial infarction; water retention; hyponatremia | Use with caution in older adults or patients with coronary artery disease or heart failure; discontinue if chest pain develops; monitor urinary output and serum sodium |
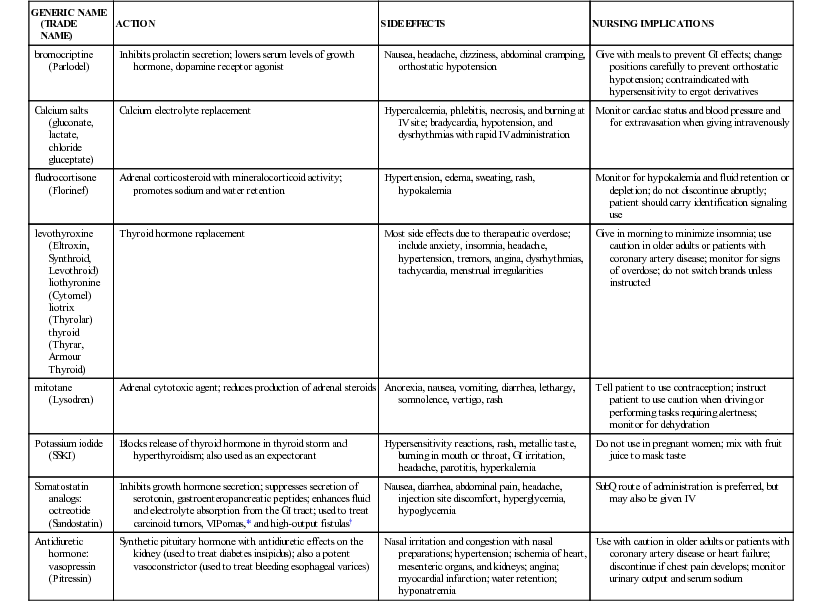
* VIPomas are neuroendocrine tumors of the pancreas that secrete vasoactive intestinal polypeptide (VIP) autonomously.
† A fistula is an abnormal passage from an internal organ through the skin to the outside of the body, and through which internal secretions and water pass. They are often triggered by surgery. A high-output fistula produces 500 mL/day or more.
GI, Gastrointestinal; IV, intravenous; subQ, subcutaneous.
Nursing Interventions and Patient Teaching
Nursing interventions are primarily supportive and are geared toward relieving the discomforts of the patient. Muscle weakness, joint pain, and stiffness warrant assessment of the ability to perform activities of daily living (ADLs). Joint pain/discomfort should be assessed frequently. Headache may impair the patient's ability to socialize and may also impede education and employment. Worsening headaches may indicate tumor progression. Jaw muscles and the temporomandibular joint may be involved. The diet should be soft and easy to chew. Encourage the patient to chew thoroughly, and allow adequate time during meals, assisting when necessary. Nonopioid analgesics may be given for pain relief. Visual impairment may increase the risk of injury for these patients, so take care to prevent them from stumbling into furniture or dropping objects.
As the body changes, the patient may develop problems with self-esteem and may feel physically unattractive. He or she may have difficulty communicating with significant others, which can disrupt individual or family coping methods. Other complications of acromegaly are related to enlargement of the liver, spleen, and heart. Cardiac dysrhythmias may develop, and the patient may experience heart failure. Abdominal girth may increase as a result of weight gain and inactivity, and respiratory difficulty may occur.
Nursing diagnoses and interventions for the patient with acromegaly include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Disturbed body image, related to physical manifestations of the condition (may include enlargement of hands, feet, tongue, jaw, and soft tissue) |

The patient should remain under the supervision of a health care provider so that any complications can be promptly diagnosed and adequately treated. Teach the patient exercises that can be performed at home, such as active range-of-motion of joints of the extremities and of the neck, to help prevent muscle atrophy and loss of movement.
Prognosis
Even with adequate medical or surgical treatment, the physical changes are irreversible, and the patient is prone to developing complications such as diabetes, heart failure, hypertension, osteoarthritis, colon polyps, sleep apnea, and vision loss (Mayo Clinic, 2013).
Gigantism
Etiology and Pathophysiology
Gigantism usually results from an oversecretion of GH before the onset of puberty, as a result of hyperplasia of the anterior pituitary. The hyperplastic tissue may develop into a tumor. Another possible cause is a defect in the hypothalamus that directs the anterior pituitary to release excessive amounts of GH.
Clinical Manifestations
When overproduction of GH occurs in a child before the epiphyses (growth plates at each end of the bones) close, there is an overgrowth of the long bones. This causes the individual to grow abnormally tall and have increased muscle and visceral development. Weight increases, but body proportions are usually normal. Despite their size, these patients are usually weak. Other kinds of gigantism may be caused by certain genetic disorders or by disturbances in sex hormone production. Once identified, these children should be referred for further medical evaluation and follow-up.
Assessment
Collection of subjective data includes assessment of the patient's understanding of the disease process and his or her ability to verbalize emotional responses.
Collection of objective data requires frequent measurement of height. Assess the patient's use of adaptive coping measures and family interactions.
Diagnostic Tests
A growth hormone suppression test may be done to evaluate GH levels (Mayo Clinic, 2013). In the patient with gigantism, baseline levels of GH are high. Blood levels of growth hormone are also evaluated for diagnosis of gigantism.
Medical Management
Medical management of children with gigantism may include surgical removal of tumor tissue or irradiation of the anterior pituitary gland, with subsequent replacement of pituitary hormones as indicated. The health care provider then observes the child for the development of related complications, such as hypertension, heart failure, osteoporosis, thickened bones, and delayed sexual development.
Nursing Interventions and Patient Teaching
Nursing interventions primarily include early identification of children who are experiencing increased growth rates compared with other children their age. The child's height is recorded at each visit to the primary health care provider and a deviation of two or more percentile levels from the median should be reported. The condition causes potential problems with self-image, especially if the child is a preteen who is a great deal taller than peers. Girls usually experience more emotional trauma in this situation than boys do. Be understanding and compassionate regarding the emotional and physical aspects of being taller than their peers.
Early diagnosis of these patients is essential, since proper medical management can hinder the height a child will reach. Stress to the parents the importance of regular visits to the pediatrician or pediatric endocrinologist (a health care provider who specializes in endocrinology).
Prognosis
With new medical and surgical advances, the expected life span of these patients is longer than it was previously. However, their life expectancy is still less than that of the average individual, primarily because of cardiovascular and joint disorders.
Dwarfism
Etiology and Pathophysiology
There are differing types of dwarfism or short stature. The condition may be caused by genetic mutations; growth hormone deficiency; and other, unknown causes. Individuals affected by hypopituitarism are in the minority of cases. Hypopituitary dwarfism is a condition caused by deficiency in GH. Most cases are idiopathic, but a small number can be attributed to an autosomal recessive trait. In some cases the patients also lack adrenocorticotropic hormone (ACTH), TSH, and the gonadotropins.
Clinical Manifestations
Short stature is the most obvious clue to a potential deficiency in growth hormone. These patients are usually well proportioned and well nourished but appear younger than their chronologic age. If a child's height is below the third percentile, there is cause for follow-up. They may have problems with dentition as the permanent teeth erupt, since the jaws are underdeveloped (Mayo Clinic, 2011a). Sexual development is usually normal but delayed. Many people with hypopituitary dwarfism are able to reproduce offspring of average height unless there is an accompanying deficiency in gonadotropins. Because only a small number of children with short stature or delayed growth have dwarfism, a thorough diagnostic workup is crucial.
Assessment
Subjective data include the patient's understanding of the disease process and emotional responses to it. A family history of dwarfism may reveal previously successful coping strategies. Encourage the patient to verbalize feelings. Affected children typically have normal intelligence. The child's history usually reveals a normal birth weight. It is important to determine when the child's growth retardation was first noted.
Collection of objective data includes regular measurement of height and weight to determine responses to GH and other hormones that may be administered. Review birth weight and length. Compare current height and weight with standard growth charts, and compare the child's growth pattern with that of siblings and other relatives at a comparable age.
Diagnostic Tests
Diagnostic tests include radiographic evaluation of the wrist to determine any difference between the patient's bone age and his or her chronological age, which might indicate a growth problem; and an MRI or a CT scan to rule out a pituitary tumor. Definitive diagnosis is based on decreased plasma levels of GH. Note: Restrict the patient's oral intake after midnight for this test. Additional genetic testing may be indicated to distinguish specific types of dwarfism and to help in future family planning decisions (Mayo Clinic, 2011a).
Medical Management
Medical treatment involves replacement of GH by injection and the addition of other hormones as needed to correct deficiencies. If a tumor is the cause of dwarfism, surgery is usually indicated. Nurses should be aware that replacement of GH by injection is expensive and may impede uninsured or underinsured parents from pursuing this treatment option.
Nursing Interventions and Patient Teaching
Exercise particular care to identify children with growth problems. The health care provider correlates the onset of growth retardation with symptoms of headache, visual disturbances, or behavior changes that might indicate a tumor, so be alert for these symptoms. The nurse should avoid making the parents feel guilty about any delay in seeking medical attention for their child.
Encourage the child to wear age-appropriate clothing and engage in activities with peers, since significant problems with self-esteem can occur in dwarfism. Emphasize the child's abilities and strengths instead of his or her physical size. Ensuring that older children and young adults have clothing that is consistent with their peers, fashionable, and age appropriate will contribute to their emotional well-being.
Prognosis
Most of these patients lead fairly average lives, and many become parents of average-height children. Complications experienced are often of the musculoskeletal and cardiovascular systems. The life span of a patient with dwarfism is typically normal, depending on the management of complications.
Diabetes Insipidus
Etiology and Pathophysiology
Diabetes insipidus, a metabolic disorder of the pituitary gland, occurs when the posterior pituitary does not produce sufficient ADH or the action of ADH is diminished. The condition may be transient or permanent. A decrease in ADH causes increased urinary output, which in turn results in dehydration and increased plasma osmolality—that is, a state of imbalance between the electrolyte and fluid components of the plasma.
The condition may be either primary or secondary to other conditions such as head injury, intracranial tumor, intracranial aneurysm, infarct, or if the pituitary gland is damaged during surgery. Infections such as encephalitis or meningitis are associated with secondary diabetes insipidus.
Clinical Manifestations
Diabetes insipidus is characterized by significant polyuria (excretion of an abnormally large quantity of urine) and intense polydipsia (excessive thirst). The urine is very dilute, looking much like water. Associated urine specific gravity (the density of urine compared with that of water) (see Chapter 49) is 1.001 to 1.005 (the normal range is 1.003 to 1.030). Normal urinary output is 1.5 L/24 hours; patients with diabetes insipidus may have a urinary output exceeding 5 to 20 L/24 hours. The patient craves fluids and may drink 4 to 20 L of fluid daily, yet may still become severely dehydrated and have increased levels of sodium in the blood (hypernatremia) due to excess urine output. These patients continue to produce copious quantities of urine when unconscious after surgery or head trauma; if not prevented, diabetes insipidus under these circumstances can lead to hypovolemic shock (failure to adequately perfuse vital organs as a result of insufficient blood volume). Manifestations of this complication include changes in level of consciousness, tachycardia, tachypnea, and hypotension. Hypovolemic shock usually follows trauma and consequent blood loss; in these cases the body increases its release of ADH in an effort to maintain blood volume; in diabetes insipidus–related hypovolemic shock, urinary output remains high rather than decreases.
Assessment
Subjective data include the patient's understanding of the relationship of symptoms (such as thirst and polyuria) to the underlying cause. The patient should be able to state the importance of not restricting oral fluids. Assess the severity of thirst. The patient may be embarrassed about the constant need to drink and then empty the bladder and may voluntarily restrict social contacts and work activities. The patient is weak, tired, and lethargic. Assessment of the patient should include symptoms indicating an electrolyte imbalance.
Collection of objective data includes assessment of skin turgor (the normal resiliency of the skin) and color and specific gravity of the urine and vital signs. Carefully monitor intake and output (I&O). The skin is dry, turgor is poor, and body weight is lost. Constipation may occur. Weigh the patient daily in the early morning, before breakfast. Determine whether the patient has nocturia.
Diagnostic Tests
Diagnosis is based on clinical manifestations, urine specific gravity, and urine ADH measurement. The urine specific gravity often drops below 1.003, and the serum sodium level increases to more than 145 mEq/L (normal serum sodium level is 135 to 145 mEq/L). Due to hemoconcentration the serum osmolality may be greater than 300 mOsm/kg (normal is 280 to 300 mOsm/kg). The fluid deprivation (water deprivation) test may be ordered to determine how well the pituitary is producing ADH and to help rule out other causes. This test involves withholding fluids for a period of up to 12 hours. During the testing period, urine specific gravity and serum osmolality are frequently measured, as well as orthostatic vital signs. Beginning and ending weights are also obtained for comparison. A CT scan and radiographic evaluation of the sella turcica (the “Turkish saddle”–shaped depression in the sphenoid bone that houses the pituitary gland) may be done to help evaluate the pituitary structures.
Medical Management
Medical treatment involves intravenous (IV), subcutaneous, intranasal, or oral administration of ADH preparations in the form of desmopressin acetate (1-deamino-8-d-arginine vasopressin, or DDAVP). Several other drugs are available for ADH replacement, including aqueous vasopressin (Pitressin intramuscular [IM] or intranasal), vasopressin tannate IM, and lypressin (Diapid intranasal). Coffee, tea, and other beverages containing caffeine are usually eliminated from the diet because of their possible diuretic effect. If the patient cannot match the urinary losses through oral intake, he or she is at risk for dehydration and severe hypernatremia. IV fluids of hypotonic saline or dextrose 5% in water are needed.
Nursing Interventions and Patient Teaching
Specific nursing interventions are aimed at protecting the patient from injury. The patient is likely fatigued from frequently ambulation to the bathroom to void and impaired sleep pattern. The patient may be at risk for injury or falls secondary to fatigue, exhaustion, and electrolyte imbalances. Carefully monitor the patient's intake and output and document. Assess skin turgor frequently, along with the condition of oral mucous membranes. Weigh the patient and record I&O daily. Do not limit oral fluids in an effort to reduce urinary output.
Nursing diagnoses and interventions for the patient with diabetes insipidus include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Deficient body fluid volume, risk for, related to excessive urine production |

Instruct the patient to wear some form of medical-alert identification, such as a necklace or bracelet, stating the diagnosis of diabetes insipidus. Stress that the patient must remain under medical supervision for monitoring of the metabolic state, since the condition may worsen with time.
Prognosis
The prognosis depends on the etiology. Patients who survive usually are dependent on medication for the rest of their lives. With proper treatment, most patients can expect to live a relatively normal life.
Syndrome of Inappropriate Antidiuretic Hormone
Syndrome of inappropriate ADH (SIADH) occurs when the pituitary gland releases too much ADH. In response to ADH, the kidneys reabsorb more water, decreasing urinary output and expanding the body's fluid volume. The patient experiences hyponatremia, hemodilution, and fluid overload without peripheral edema.
Etiology and Pathophysiology
ADH regulates the body's water balance. Synthesized in the hypothalamus, ADH is stored in the posterior pituitary gland. When released into the circulation, it acts on the kidneys' distal tubules and collecting ducts, increasing their permeability to water. This decreases urine volume, since more water is reabsorbed and returned to the circulation, which increases blood volume.
When the body's system of checks and balances malfunctions—whether from a tumor, medication, unrelated disease process, or some other cause—ADH may be released continuously, causing SIADH, which occurs more commonly in older adults.
ADH is released in response to stress. Be alert to patients who have the following risk factors and who are also in pain or undergoing stressful procedures:
• Medications including anesthetics, opiates, barbiturates, thiazide diuretics, and oral hypoglycemics
• Malignancies (the most common cause of SIADH; cancerous cells are capable of producing, storing, and releasing ADH)
• Nonmalignant pulmonary diseases including chronic obstructive pulmonary disease, tuberculosis, lung abscesses, and pneumonia
• Nervous system disorders including head trauma, cerebral vascular accident, encephalitis, meningitis, and Guillain-Barré syndrome
• Miscellaneous causes including lupus erythematous, adrenal insufficiency, and thyroid and parathyroid deficiencies
Clinical Manifestations
Clinically, SIADH is characterized by hyponatremia and water retention that progresses to water intoxication. The severity of the patient's condition is largely linked to the sodium levels and the location of fluid accumulation. Most signs and symptoms appear when serum sodium levels fall below 125 mEq/L. Signs and symptoms include nausea, vomiting, irritability, confusion, tremors, seizures, stupor, coma, and pathologic reflexes.
Assessment
Subjective data include vague complaints. Hyponatremia triggers the earliest symptoms, which are nonspecific and could indicate other disorders. The nurse should assess for complaints or reports of cramping, anorexia, nausea, and headaches.
Collection of objective data includes assessment for hyponatremia. Fluid intake exceeds urinary output. The patient does not develop peripheral edema because excess fluid is accumulating in the vascular system, not in the interstitial spaces and therefore weight gain is not always noted with SIADH.
As water intoxication progresses and the patient's serum becomes more hypotonic, brain cells expand (become edematous), and therefore the later signs of SIADH are neurologic. The patient becomes progressively lethargic, with marked personality changes. The patient has seizures, and the deep tendon reflexes diminish or disappear altogether.
All electrolyte levels should be monitored and the patient assessed often for signs and symptoms of increases and decreases in electrolytes, either from the disease process or the implementing of treatments for correction.
Diagnostic Tests
The diagnosis of SIADH is made by simultaneous measurements of urine and serum osmolality. Serum osmolality is less than 280 mmol/kg (normal is 285 to 295 mOsm/kg). Laboratory tests show hyponatremia (sodium less than 134 mEq/L). The serum is diluted and the urine is concentrated. Urine specific gravity is greater than 1.032, and urine sodium is elevated due to concentration.
Medical Management
The health care provider orders fluid restriction, initially 800 to 1000 mL/day. However, with severe hyponatremia fluids may be restricted to 500 mL/day. Daily fluid intake should equal fluid output. If fluid restriction is adequate, tests show a gradual increase in serum sodium along with a decrease in body weight.
A hypertonic saline solution (3% to 5%) may be ordered via IV infusion pump at a very slow rate to avoid too rapid a rise in sodium. This is necessary to correct sodium imbalance and to pull water out of edematous brain cells.
The health care provider may order medications such as demeclocycline (Declomycin), a tetracycline derivative, at a dosage of 300 mg orally four times daily. The health care provider may also prescribe lithium carbonate. Both drugs interfere with the antidiuretic action of ADH and cause polyuria. Diuretics such as furosemide (Lasix)—40 to 80 mg/day orally in divided doses or 20 to 40 mg IV daily—may be prescribed, to eliminate excess fluid, but only if the serum sodium is at least 125 mEq/L, or the drug may promote more loss of sodium. Taking furosemide increases losses of potassium, magnesium, and calcium; supplements may be needed.
Treatment must also be directed at eliminating the underlying problem. Surgical resection, radiation, or chemotherapy may be indicated for malignant neoplasms. If the causative factor is a medication, it is discontinued.
Monitoring the patient for signs and symptoms of further electrolyte imbalances is a priority nursing assessment. Intake and output should also be monitored closely to ensure intake and output are comparable.
Nursing Interventions and Patient Teaching
The goals of nursing care are focused on assessment of the condition with documentation and reporting of changes. Timing of the assessment frequency is based on the patient's condition. The nurse performs a neurologic examination and assesses the patient's hydration status frequently. Auscultate lung sounds; crackles indicate fluid overload. Monitor the patient's oxygen saturation frequently. Carefully observe serum electrolytes, urine sodium, and urine specific gravity because overcorrection can cause hypernatremia. Weigh the patient daily. Closely monitor I&O; output is the guide to regulating intake.
Restriction of fluid intake is done to prevent fluid overload. Provide and frequently reinforce education. Solicit patient input in scheduling fluid allotments and types of fluids. Patients on diuretic therapy may require supplementation of sodium and potassium. Instruct patients to avoid foods high in sodium content, which may promote thirstiness.
The nurse should use simple explanations when detailing the plan of care because anxiety can aggravate SIADH. If the patient reports nausea, the nurse should obtain an order for an antiemetic before administration.
Nursing diagnoses and interventions for the patient with SIADH include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Excess fluid volume, related to decreased urinary output | |
| Risk for impaired oral mucous membranes, related to fluid restrictions of 500 mL/day |

Patient teaching should be an ongoing part of nursing care. Be certain the patient understands the treatment plan, the rationale behind it, and the expected outcome. Provide information about signs and symptoms of SIADH, and tell the patient to alert the health care provider if any changes are noted. SIADH can recur after discharge.
Prognosis
SIADH resulting from an adverse reaction to medication, or secondary to a head trauma, is self-limiting. The ability to manage metabolic conditions will determine the chronicity of the disease. SIADH is potentially dangerous but treatable. Early diagnosis and medical management improve the prognosis.
Disorders of the Thyroid and Parathyroid Glands
Hyperthyroidism
Etiology and Pathophysiology
Hyperthyroidism—also called Graves' disease, exophthalmic goiter, and thyrotoxicosis—is a condition in which there is increased activity of the thyroid gland, with overproduction of the thyroid hormones T4 and T3, resulting in an exaggeration of metabolic processes. Graves' disease (the most common cause of hyperthyroidism) occurs most frequently in women in the 20- to 40-year-old age group. Two percent of the female population is affected by Graves' disease, compared with 0.2% of the male population. Graves' disease is an autoimmune disorder of unknown etiology.
Clinical Manifestations
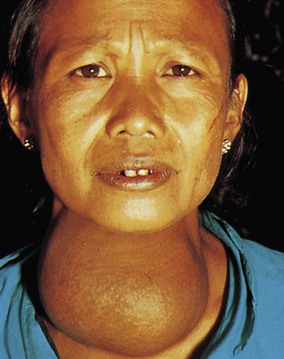
Clinical manifestations are numerous and varied, from mild to severe. The patient usually has visible edema of the anterior portion of the neck as a result of enlargement of the thyroid. In severe cases, exophthalmos (bulging of the eyeballs) may occur, usually attributable to periorbital edema (Figure 50-6). Twenty percent to 40% of patients with Graves' disease manifest the classic finding of exophthalmos. The eyeballs are forced outward, resulting in incomplete closure of the eyelids; the exposed corneas become dry with subsequent development of corneal ulcers and loss of vision.

Assessment
Subjective data include the patient's description of an inability to concentrate and memory loss. The patient may complain of dysphagia or may be hoarse. There is usually weight loss, even with a voracious appetite. The patient reports feeling nervous, jittery, and excitable and may experience insomnia. The nurse would assess the patient for complaints of “heart palpitations” or other cardiac concerns, such as shortness of breath. These patients are emotionally labile and may overreact to stressful situations.
Objective data include changes in vital signs. The pulse is usually rapid, blood pressure is elevated, with cardiac arrhythmias noted. A bruit may be auscultated over the thyroid. The skin is warm and flushed, and the hair becomes fine and brittle. Female patients may cease to menstruate. Elevated body temperature may be accompanied by intolerance to heat, with profuse diaphoresis. The patient may have an increase in bowel movements. Note tremors of the hands. Behavior changes may include hyperactivity and clumsiness. Daily weighing usually shows weight loss.
Diagnostic Tests
The thyroid is controlled by the hypothalamus. Under normal conditions the thyroid secretes T3 and T4 in response to TSH released by the pituitary. As the T3 and T4 levels in the blood increase, the pituitary stops secreting TSH—an example of the negative feedback loop described earlier in this chapter.
If the thyroid becomes impaired, its hormone secretion may not respond normally to TSH. It may secrete too much (hyperthyroidism) or too little (hypothyroidism) T3 and T4. Hyperthyroidism is confirmed by a decrease in TSH level (because the overactive thyroid is releasing high amounts of T3 and T4, which exert negative feedback on the pituitary gland, causing it to stop secreting TSH) and an elevation of the level of free T4 (FT4). Total T3 and T4 levels may be evaluated but are not as helpful in the diagnosis. Additional diagnostic tests include radioactive iodine uptake scans and thyroid scans, typically performed in an outpatient setting (Box 50-1).
Medical Management
Ablation therapy using radioactive iodine is the gold standard for treating hyperthyroidism. The goal is to destroy enough of the hypertrophied thyroid tissue to produce a normally functioning thyroid gland. Dosing is patient specific and often results in the development of hypothyroidism. The therapeutic dose of radioactive iodine is low, so no radiation safety precautions are necessary, with the exception of danger to pregnant women providing care.
Medical management for hyperthyroidism may include daily administration of drugs that block the production of thyroid hormones, such as propylthiouracil (PTU) or methimazole (Tapazole) (Table 50-2). The patient usually begins to notice a decrease in symptoms within 6 to 8 weeks after starting drug therapy. This may be followed after the acute stage by ablation therapy using a therapeutic dose of radioactive iodine (Na131I or Na125I), based on the patient's age, clinical manifestations, and estimated weight of the thyroid.
Table 50-2
Medications Commonly Used to Treat Hyperthyroidism and Hypothyroidism
| MEDICATIONS | COMMON SIDE EFFECTS |
| Hyperthyroidism | |
| Iodine or iodine products (potassium or sodium iodide with strong iodine solution, potassium iodide, Lugol's solution) | Nausea, vomiting, diarrhea, abdominal pain |
| Radioactive iodine (131I or 125I) | Sore throat, edema or pain in neck, temporary loss of taste, nausea, vomiting, painful salivary glands |
| methimazole (Tapazole), propylthiouracil (PTU) | Rash or pruritus, vertigo, nausea, vomiting, loss of taste, paresthesias, abdominal pain |
| Hypothyroidism | |
| levothyroxine (Levothroid, Synthroid, Eltroxin, Levo-T, Unithroid) liothyronine (Cytomel) liotrix (Thyrolar) thyroid (Armour Thyroid, Thyrar) | Nervousness, irritability, tremors, insomnia, tachycardia, hypertension, palpitations, cardiac dysrhythmias, vomiting, diarrhea, nausea, appetite changes, weight loss, menstrual irregularities, leg cramps, fever |
Because of the possible development of hypothyroidism following this treatment, the patient must have adequate follow-up medical supervision. If a patient develops hypothyroidism after treatment, levothyroxine therapy will be needed. Note: 131I is not a radiation hazard to the nonpregnant patient but is absolutely contraindicated during pregnancy. Pregnant health care professionals should not care for this patient for several days after treatment.
Surgery has fallen out of favor because of possible serious complications, such as hemorrhage, hypoparathyroidism, and vocal cord paralysis. Surgery may still be indicated for patients who cannot tolerate antithyroid drugs, are not good candidates for radioactive iodine therapy, have a possible malignancy, or have large goiters causing tracheal compression.
Surgical treatment for hyperthyroidism is subtotal thyroidectomy, a procedure in which approximately five sixths of the thyroid is removed. If too much tissue is taken, the gland will not regenerate after surgery and hypothyroidism will result. Surgery is usually delayed, if possible, until the patient is in a normal thyroid (euthyroid) state because of the risk of excessive bleeding during thyroidectomy and postoperative thyroid crisis.
Patients who have only mild hyperthyroidism are rarely admitted to the acute care hospital. They are treated by the health care provider in an office or clinic setting. However, the hospital nurse may come in contact with the hyperthyroid patient admitted for a different condition and may also care for these patients before and after thyroidectomy.
Nursing Interventions and Patient Teaching
The hyperthyroid patient needs more nutrients because of increased metabolism. Diet therapy usually consists of food high in protein. Increased vitamins (especially the B vitamins), minerals, and carbohydrates are also indicated. Losses in bone density may be attributed to hyperthyroidism. Supplementation with calcium and vitamin D is indicated to avoid the development of osteoporosis. Offer between-meal snacks. Food should be soft and easily swallowed if the patient has dysphagia (difficulty swallowing). Coffee, tea, and colas should be avoided because of their stimulant effect.
Preoperative teaching is extremely important for the patient who is scheduled for a thyroidectomy. Keep the environment as stable as possible to prevent increased hyperstimulation. Include instructions on how to properly support the head while turning in bed or rising to a sitting or standing position. The nurse (or patient) places both hands behind the head and maintains anatomical position while the rest of the body is being moved. Also teach the patient to deep breathe, but the health care provider will determine whether coughing is to be done postoperatively, since it strains the suture line. Inform the patient that a period of “voice rest” may be enforced for 48 hours postoperatively and that pencil and paper will be provided for writing notes instead of talking. Do voice checks every 2 to 4 hours, as ordered by the health care provider, to rule out damage to the laryngeal nerve resulting in inability to speak. Ask the patient to say “ah” and check for excessive hoarseness or voice change. Slight hoarseness is expected and should not cause alarm. Damage to the laryngeal nerve during surgery occurs in approximately 12.4% of cases, but the damage is not always permanent.
Postoperative management includes keeping the patient in a semi-Fowler's position, to decrease edema at the operative site and to enhance respiratory status, with pillows supporting the head and shoulders. Caution the patient to avoid hyperextending the head to prevent excess tension on the incision, which is usually made in a horizontal crease in the anterior neck. Have a suction apparatus and tracheotomy tray available for emergency use. A cool-mist humidifier at the bedside may help soothe the throat and prevent coughing. Check vital signs frequently, with special attention paid to the rate and depth of respirations and observations for any dyspnea (shortness of breath or difficulty breathing) related to edema in the operative site. Before giving any liquid orally, be sure the swallowing and cough reflexes have returned. Be alert for signs of internal or external bleeding; early signs of internal bleeding include restlessness, apprehension, increased pulse rate, decreased blood pressure, and a feeling of fullness in the neck. Later, cyanosis may develop, signaling an obstructed airway; provide for adequate airway management and notify the surgeon immediately. Inspect the dressing on the neck frequently for obvious external bleeding. Also check for bleeding at the sides and back of the neck and on top of the patient's shoulders, since oozing blood may pool there as a result of gravity. Most surgeons allow a dressing to be reinforced as needed and loosened slightly if the patient complains that it is too tight.
Postoperatively, the diet initially consists of clear, cool liquids, progressing to soft food as tolerated. This is followed by a regular diet as soon as possible to help the patient regain lost weight and correct any nutritional deficiencies.
Another significant postoperative complication after thyroidectomy is tetany. One possible cause of tetany is the inadvertent removal of one or more of the parathyroid glands during surgery. Another is edema in the operative area, which occludes release of PTH into the bloodstream, resulting in a low serum calcium level (normal serum calcium is 9.0 to 10.5 mg/dL). The symptoms include numbness and tingling in the fingertips and toes and around the mouth. The patient may also have carpopedal spasms (muscle spasms in the wrists and feet) and increased pulse, respirations, and blood pressure, accompanied by anxiety and agitation. Laryngeal spasm and stridor may occur. Chvostek's sign (an abnormal spasm of the facial muscles elicited by light taps on the facial nerve in patients who are hypocalcemic) is positive, and Trousseau's sign (assesses for latent tetany) may also be positive; carpal spasm is induced by inflating a sphygmomanometer cuff on the upper arm to a pressure exceeding systolic blood pressure for 3 minutes; a positive result may be seen in hypocalcemia (a deficiency of calcium in the blood serum) and hypomagnesemia. If untreated, the condition may progress to convulsions or lethal cardiac dysrhythmias. Emergency treatment of tetany is the IV administration of calcium gluconate, which should always be available postoperatively.
The other serious complication after thyroidectomy is thyroid crisis, or thyroid storm. Fortunately, it occurs rarely and can usually be attributed to manipulation of the thyroid during surgery, which causes the release of large amounts of thyroid hormones into the bloodstream. If thyroid crisis occurs, it usually does so within the first 12 hours postoperatively. In thyroid crisis, all the signs and symptoms of hyperthyroidism are exaggerated. In addition, the patient may develop nausea, vomiting, severe tachycardia, severe hypertension, and occasionally hyperthermia up to 106° F (41° C). Extreme restlessness, cardiac dysrhythmia, and delirium may also occur. The patient may develop heart failure as evidenced by decreased cardiac output secondary to cardiac strain and tachycardia. Diagnostic tests indicate increased FT4 and decreased TSH.
The three goals of thyroid storm management are (1) to induce a normal thyroid state, (2) prevent cardiovascular collapse, and (3) prevent excessive hyperthermia. Emergency treatment of thyroid crisis includes administration of IV fluids, sodium iodide, corticosteroids, antipyretics, an antithyroid drug (such as PTU or methimazole), and oxygen as needed. Prompt, adequate treatment usually results in dramatic improvement within 12 to 24 hours.
Nursing diagnoses and interventions for the patient having a thyroidectomy include but are not limited to the following.
| Nursing Diagnosis | Nursing Interventions |
| Preoperative | |
| Risk for hyperthermia, related to increased metabolism | |
| Imbalanced nutrition: Less than body requirements, related to increased metabolism | |
| Postoperative | |
| Impaired swallowing, related to postoperative edema | |
| Ineffective breathing pattern, risk for, related to: | |
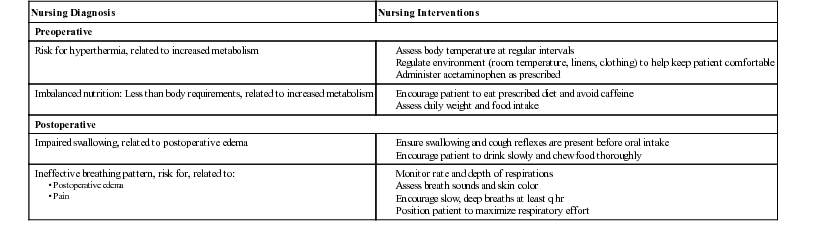
Patient education after thyroidectomy includes stressing the importance of follow-up medical supervision. Thyroid function tests are done periodically to check for both hyperthyroidism and hypothyroidism, which occurs in approximately 43% of surgical cases. Before discharge, teach the patient proper care of the incision site and symptoms that might indicate development of an infection, in which case he or she should notify the surgeon immediately. Discuss with the patient the need for a high-calorie, high-protein, high-carbohydrate diet until weight is stable.
Prognosis
With adequate, appropriate medical or surgical treatment, these patients usually have a normal life expectancy. However, exophthalmos, if present, may remain to a lesser degree in some patients.
Hypothyroidism
Etiology and Pathophysiology
Hypothyroidism is one of the most common medical disorders in the United States. It occurs most often in women 30 to 60 years of age and is more common in older adults than previously thought. Hypothyroidism occurs when the thyroid fails to secrete sufficient hormones, slowing all of the body's metabolic processes. Causes include an autoimmune response, radiation therapy, pituitary disorders, or iodine deficiency. It sometimes results from medical or surgical treatment of hyperthyroidism (Mayo Clinic, 2012). Severe hypothyroidism in adults is called myxedema. It is characterized by edema of the hands, face, feet, and periorbital tissues. Congenital hypothyroidism is called cretinism and is estimated to occur in 1 of every 4000 births (Daniel and Postellon, 2013). All infants in the United States are screened for decreased thyroid function at birth.
Clinical Manifestations
Clinical manifestations range from mild to severe and depend on the degree of thyroid hormone deficiency present. All the body's metabolic processes slow, resulting in decreased production of body heat, intolerance to cold, and weight gain. Atherosclerotic changes may result in coronary artery disease. Hypothyroidism may have adverse effects on the heart, with decreased cardiac output and contractility; the patient experiences decreased exercise tolerance and dyspnea on exertion. Early signs are weight gain, difficulty concentrating, constipation, and fluid/weight gain. Late signs include mood swings, infertility (in women), acute fatigue syndrome, and depression.
Assessment
Subjective data include the patient's mental and emotional status, which may include depression, paranoia, impaired memory, and general slowing of thought processes. Speech and hearing may be deficient. The patient is lethargic, forgetful, and irritable. Because of the body's slowed metabolism, cold intolerance, anorexia, and constipation may develop. Both sexes may experience decreased libido and reproductive difficulty. Assess the patient's adaptive coping methods.
Collection of objective data includes assessment of the skin and hair. The hair thins and may fall out; the skin becomes thickened and dry. Facial features may enlarge to give the patient an edematous appearance with a masklike facial expression. The voice is characteristically low and hoarse. Decreased metabolism usually causes bradycardia, decreased blood pressure and respirations, and exercise intolerance. The patient has decreased ability to perform activities because of weakness, clumsiness, and ataxia. Assess the respiratory rate after administration of any central nervous system depressant. Evaluate the abdomen for distention, since myxedema ileus (intestinal obstruction) may occur. Menorrhagia (excessive menstrual flow) is a frequent complaint of women with hypothyroidism. Also, inhibition of ovulation with subsequent infertility may occur (Lewis et al., 2011).
Diagnostic Tests
Diagnosis of hypothyroidism is based on the physical examination and history and on appropriate laboratory tests, such as TSH, T3, T4, and FT4 levels. Low levels of T3, T4, and FT4 are the underlying stimuli for TSH secretion. Therefore, a compensatory elevation of TSH occurs in patients with primary hypothyroid states, and low levels of T3, T4, and FT4 are present. Subclinical cases may go undiagnosed for years, so be aware of subtle clues while interviewing and caring for the patient.
Medical Management
Hypothyroidism is treated with hormone replacement therapy using desiccated animal thyroid (Armour Thyroid), T4, or synthetic products such as levothyroxine (Levothroid, Synthroid, Levo-T, Eltroxin) (see Table 50-2). Synthetic products are typically preferred over biologic agents to treat hypothyroidism. The drugs are usually given in the morning to enhance metabolization of nutrients ingested during the daily meals. The nurse should teach the patient to take levothyroxine on an empty stomach. The patient initially is given a small dose, with increases as necessary until the desired effect is achieved. A maintenance dosage is then established. Early in treatment, the hormone level should be monitored about every 6 to 8 weeks until the patient's TSH level is normal and then tested at least annually. Watch the patient for adverse effects of drug therapy, which mimic the signs and symptoms of hyperthyroidism. There is usually a dramatic change in the patient after replacement therapy begins. Lifelong thyroid replacement therapy is usually required, as well as laboratory monitoring of T3, T4, and TSH levels to adjust the dosage and minimize the effects of hypothyroidism or hyperthyroidism as a result of a too-high dosage.
Nursing Interventions and Patient Teaching
Nursing interventions for the hospitalized patient with severe hypothyroidism center mainly on symptomatic relief. Keep the room at least 70° to 74° F (21° to 23° C), and be certain the patient does not become chilled during bathing or other procedures. Allow extra time for physical care so the patient does not feel rushed. Keep accurate records of bowel elimination because constipation may be severe. Stool softeners and bulk laxatives may be ordered. Provide a high-protein, high-fiber, low-calorie diet, and encourage increased fluid intake. The patient should avoid concentrated carbohydrates, such as sweets, to help prevent excessive weight gain. Watch for chest pain or dyspnea accompanied by changes in the rate or rhythm of the heart; this may indicate cardiac involvement. Caution the patient to not stop taking the thyroid hormone without consulting a health care provider. This medication must be taken for the rest of the patient's life. Because most patients with hypothyroidism are more susceptible to the effects of sedatives, hypnotics, and anesthetics, be alert for possible adverse effects if these agents are given.
Teach the patient to take the thyroid hormone on a consistent schedule, typically in the morning on an empty stomach. Taking the medication with food, vitamins, and minerals can impair absorption. In addition, the patient should inform the health care provider if the diet typically contains soybean flour, cottonseed oil, or walnuts, which can adversely impair absorption.
Nursing diagnoses and interventions for the patient with hypothyroidism include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Decreased cardiac output, related to decreased metabolism | |
| Constipation, related to decreased peristaltic action |

Regular checkups are essential because the drug dosage may need to be adjusted periodically. The patient and significant other should understand the desired effects and major adverse effects of the medication. Instruct the patient to eat well-balanced meals of high-fiber foods such as fruits, vegetables, and whole-grain cereals and breads. The patient also needs an adequate intake of iodine, found in foods such as saltwater fish, milk, and eggs. Increased fluid intake will help prevent constipation. Tell the patient and the family that mental and physical slowness may still be present but should improve with thyroid replacement therapy.
Prognosis
Most patients with hypothyroidism do well with proper medical supervision, although they will probably have to take medication for the rest of their lives. In children, when T4 replacement begins before epiphyseal fusion, the chance for normal growth is greatly improved.
Simple (Colloid) Goiter
Etiology and Pathophysiology
A simple, or colloid, goiter develops when the thyroid gland enlarges in response to low iodine levels in the bloodstream or when it is unable to use iodine properly. When the blood level of T3 is too low to signal the pituitary to decrease TSH secretion, the thyroid gland responds by increasing the formation of thyroglobulin (colloid), which accumulates in the thyroid follicles and causes the gland to enlarge (Figure 50-7). Most cases of simple goiter can be attributed to insufficient dietary intake of iodine, leading to this overgrowth of thyroid tissue.
Clinical Manifestations
The patient usually has no manifestations of overt thyroid dysfunction, and the diagnosis is essentially based on the patient's physical appearance.
Assessment
Subjective data include the patient's emotional response to the unsightly enlargement of the thyroid. Encourage the patient to talk about his or her feelings. The patient may complain only of symptoms of dysphagia, hoarseness, or dyspnea related to the pressure of the enlarged gland against the esophagus and trachea. Dysphagia may make it difficult to eat and drink adequate amounts. Assess the patient for increasing dyspnea. Determine the patient's understanding of the need for medication, diet therapy, and medical follow-up.
Collection of objective data includes assessment of increased goiter size, voice changes, and adequacy of food and fluid intake.
Diagnostic Testing
Diagnostic testing includes a thyroid scan or an ultrasound of the thyroid gland to determine function and structure. Serum tests to evaluate T3, T4, and TSH levels are also completed.
Medical Management
The thyroid may be only slightly enlarged, or it may be so enlarged that surgery must be done to improve respiration or swallowing. Surgery also is sometimes performed for cosmetic effect, since this type of goiter can be unsightly and damage the patient's self-image and self-esteem. Lugol's solution is one antihyperthyroid agent used in conjunction with other antihyperthyroid medications, to decrease or shrink the thyroid gland, typically before surgery. It is also used in cases where surgical removal of the thyroid gland is not feasible or must be delayed (NLM, 2013).
If thyroidectomy is done, most of the gland is removed. Medical treatment consists of oral administration of potassium iodide and foods high in iodine (such as seafood, seaweed, dairy, grains, iodized salt, and eggs) (Office of Dietary Supplements, n.d.).
Nursing Interventions and Patient Teaching
Nursing interventions after thyroidectomy (previously discussed) are aimed at prevention of complications such as bleeding, tetany, and thyroid crisis.
Nursing diagnoses and interventions for the patient with simple (colloid) goiter include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Risk for noncompliance, related to therapeutic regimen | |
| Risk for disturbed body image, related to altered physical appearance |

Stress the importance of adequate dietary intake of iodine by the patient. Medical supervision is recommended at regular intervals.
Prognosis
Most patients can expect to live a normal life after adequate treatment of goiter. If the thyroid becomes inactive, a diagnosis of hypothyroidism is made and the patient is treated with conventional replacement therapy medications.
Cancer of the Thyroid
Etiology and Pathophysiology
Cancer of the thyroid is a relatively rare malignancy, affecting approximately 25 per 1 million people in the United States each year. Risk factors include diets low in iodine (not common in the United States) and radiation exposure; women in their 40s and 50s are at greater risk as well. In the late 1940s and up into the 1960s, radiation was used more frequently than it is today for medical procedures. At one time, radiation was used to treat acne, enlarged thymus tissue, and tonsils/adenoids in children and teens (American Cancer Society [ACS], 2013). Cancer of the thyroid occurs more frequently in females and in whites. The incidence rises as age increases (Norman, 2012). About 75% of malignancies of the thyroid are papillary, well-differentiated adenocarcinomas, a type of cancer that grows slowly, is usually contained, and does not spread beyond the adjacent lymph nodes. Cure rates after thyroidectomy in these cases are excellent. Other cancers, follicular and anaplastic, are rarer and have extremely low cure rates.
Clinical Manifestations
The principal clinical manifestation of thyroid cancer is a firm, fixed, small, rounded, painless mass or nodule that is felt during palpation of the gland. Only in rare instances are the symptoms of hyperthyroidism seen.
Assessment
Subjective data include the patient's use of adaptive coping methods to deal with the diagnosis. Also observe the support system provided by the patient's significant others. Assess the patient's understanding of the importance of medical follow-up, and for reports of trouble breathing, hoarseness, or difficulty in swallowing.
Objective data include progressive enlargement of the tumor area preoperatively, response to 131I therapy, and skin involvement in the neck and torso after radiation therapy. Assess for trachea and vocal cord involvement as well.
Diagnostic Tests
Papillary thyroid cancer is suspected when a thyroid scan shows a “cold” nodule, indicating decreased uptake of 131I. Benign adenomas and follicular cancers are usually visualized as “hot” nodules because of their increased uptake of the isotope. Thyroid function tests usually yield normal results. The health care provider uses ultrasound and CT scans of the thyroid to further investigate the thyroid and surrounding tissue. If the parathyroid gland is involved, the serum calcium level may be elevated as well. To confirm the diagnosis, a thyroid needle biopsy may be done, but only by a skilled health care provider to avoid seeding of adjacent tissues. Metastasis could result, with the prognosis becoming much more grave.
Medical Management
Treatment of thyroid cancer is a total thyroidectomy, with subsequent lifelong thyroid hormone replacement therapy. If metastasis is present at the time of the initial surgery, a radical neck dissection may be performed. In addition, radiation therapy, chemotherapy, and administration of radioactive 131I may be done.
Nursing Interventions and Patient Teaching
Nursing interventions are like those for the patient who has undergone thyroidectomy (see the previous section “Hyperthyroidism”). As with a thyroidectomy for noncancerous lesions, the major postoperative complications are respiratory distress, recurrent laryngeal damage, hemorrhage, and hypoparathyroidism. The nurse assesses the patient's oxygen saturation, voice tone and presence, and surgical site and monitors for signs and symptoms of hypothyroidism and hypoparathyroidism, including serum calcium levels. The nurse should take caution to assess the posterior neck area as well. The drainage from the incision may pool at the posterior neck and not be obvious from the anterior view.
Nursing diagnoses and interventions for the patient with cancer of the thyroid include but are not limited to the following.
| Nursing Diagnosis | Nursing Interventions |
| Anxiety, related to situational crisis | |
| Risk for injury, related to increased metabolic action of thyroid hormone and decreased calcium serum levels | |
| Risk for fluid volume deficiency, related to postoperative hemorrhage |
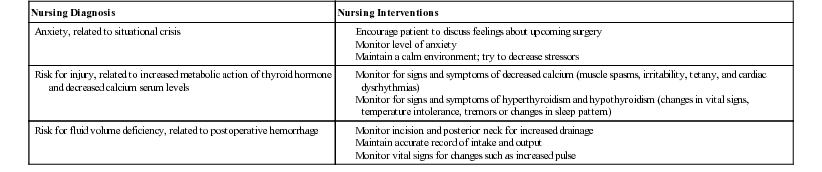
Stress the importance of proper medical follow-up to monitor thyroid hormone replacement therapy and to help ensure prompt diagnosis of any metastatic lesions. Before discharge from the hospital, teach the patient proper care of the surgical incision. Include teaching on the possibility of surgically induced hypothyroidism (depending on the amount of thyroid gland removed) including the need to take thyroid replacement therapy correctly, and signs and symptoms of hyperthyroidism (if the dosage is too high).
Prognosis
The prognosis after treatment for thyroid cancer depends on the type of tumor. For papillary carcinoma the prognosis is excellent, and the 5-year survival rate for stage I and II is nearly 100%. For stages III and IV the rate is 93% and 51%; for follicular and anaplastic carcinomas, the prognosis is much less favorable (ACS, 2013).
Hyperparathyroidism
Etiology and Pathophysiology
Hyperparathyroidism involves overactivity of the parathyroid glands, with increased production of PTH. The cause of this condition may be a primary hypertrophy of one or more of the tiny parathyroid glands, usually in the form of an adenoma (benign growths that may evolve into adenocarcinomas). It may also result from chronic renal failure, pyelonephritis, or glomerulonephritis. Parathyroid carcinoma may in rare cases result in hyperparathyroidism with rapid progress and a grave prognosis. Hyperparathyroidism usually occurs in adults between 30 and 70 years of age, and it occurs twice as often in women. Risk factors include postmenopausal status, prolonged or severe calcium or vitamin D deficiency, lithium use, and radiation to the neck (Mayo Clinic, 2011b).
Clinical Manifestations
The primary clinical manifestation is hypercalcemia. This occurs as calcium leaves the bones and accumulates in the bloodstream. As a result, the bones become demineralized, causing skeletal pain, pain on weight bearing, and pathologic fractures (fractures that result from slight or no trauma to diseased bone). The first presentation of the illness may be a patient seen for a fractured bone that is unrelated to trauma. The high level of calcium in the blood may lead to the formation of kidney stones.
Assessment
Collection of subjective data includes assessment of the severity of skeletal pain, the degree of muscle weakness, and the effectiveness of analgesics. It is important to determine nursing measures that contribute to the patient's comfort and mobility. As neuromuscular function decreases, the patient has generalized fatigue, drowsiness, apathy, nausea, and anorexia; assess the degree of anorexia and nausea. There may be constipation, personality changes, disorientation, and even paranoia. Renal colic and dull back pain may indicate calculus (kidney stone) formation.
Collection of objective data includes careful observation for any skeletal deformity or abnormal movement of bone that might indicate a pathologic fracture. Observe the urine for quantity and the presence of hematuria and stones. There may be vomiting and weight loss. Hypertension and cardiac dysrhythmias may present significant problems. Changes in the serum calcium level may cause bradycardia and other cardiac irregularities. The level of consciousness may decrease to the level of stupor or coma.
Diagnostic Tests
Radiographic examination may reveal skeletal decalcification. Blood PTH levels are increased, as are alkaline phosphate levels. The patient should receive nothing by mouth for 8 to 12 hours before these tests. The serum calcium level is elevated, whereas the serum phosphorus level is decreased. Bone density measurements may also be used to detect bone loss. Imaging, such as MRI, CT, and ultrasound, may be used to localize the adenoma. A sestamibi scan is useful in determining the location of a parathyroid tumor. In this diagnostic test, a radioactive dye is injected into the patient's vein and the parathyroid gland absorbs the agent, which is then detectable on imaging (Parathyroid.com, 2012). The primary health care provider may also request 24-hour urine collection to determine calcium levels. An elevated urine calcium level is indicative of increased parathyroid hormone levels (NLM, 2011c). A differential diagnosis should be made to rule out multiple myeloma, Cushing's syndrome, vitamin D excess, and other causes of hypercalcemia.
Medical Management
The treatment for hyperparathyroidism is surgical removal of an existing tumor or of one or more parathyroid glands. Normal parathyroid tissue taken from the patient is transplanted in the forearm or near the sternocleidomastoid muscle (a muscle in the side of the neck). This autotransplantation allows the parathyroid tissue to continue to secrete PTH to regulate the concentration of calcium and phosphorus in the blood. If autotransplantation is not possible, or if it fails, the patient needs to take calcium replacement for life (Lundström et al., 1978).
Nursing Interventions and Patient Teaching
Preoperative nursing interventions include helping restore fluid and electrolyte balance by encouraging increased oral fluid intake and by carefully monitoring IV fluid therapy. Monitor the patient's I&O because diuretics may be used to encourage elimination of serum calcium. Furosemide is the diuretic of choice. Thiazide diuretics are not used because they decrease renal excretion of calcium and thus increase the hypercalcemic state. Urine may be strained if the patient exhibits signs of kidney calculi. Daily serum calcium levels may be ordered. The diet should be low in calcium, eliminating milk and other dairy products. Antacids are high in calcium and should not be used. Accurately assess the patient's pain and administer prescribed analgesics as needed. Postoperatively, care for the patient in the same manner as after a thyroidectomy, with careful monitoring of I&O. These patients commonly retain fluid in the tissues after surgery and often have decreased urinary output. It is important to avoid overhydration at this point. Assess the patient frequently for signs of hypocalcemia, such as tetany, cardiac dysrhythmias, and carpopedal spasms (i.e., spasms of the hands or feet). If tetany does occur, administer calcium gluconate intravenously.
Nursing diagnoses and interventions for the patient with hyperparathyroidism include but are not limited to the following.
| Nursing Diagnosis | Nursing Interventions |
| Activity intolerance, related to neuromuscular dysfunction | |
| Acute skeletal, joint pain related to hormonal imbalances | |
| Renal colic, related to physiologic variables |

Teach the patient the principles of good body mechanics to prevent pathologic fractures during ambulation. Reassure the patient that bone pain should gradually decrease as electrolyte balance is restored and the condition is alleviated. Encourage the patient to participate in mild exercise as prescribed by the health care provider to regain muscle strength and promote bone health. Encourage the patient to consume plenty of water, monitor the amount of dietary calcium and vitamin D, and avoid smoking. Teach the patient that certain medications such as some diuretics and lithium can elevate the serum calcium level. Evaluate the home environment and develop a plan of changes necessary to prevent accidents, such as eliminating tripping hazards.
Prognosis
With proper medical or surgical treatment, the patient can maintain an average life expectancy. In patients with parathyroid carcinoma, the prognosis is grave.
Hypoparathyroidism
Etiology and Pathophysiology
Hypoparathyroidism occurs when there is decreased PTH, resulting in decreased levels of serum calcium. Idiopathic hypoparathyroidism is a rare condition, thought to be either autoimmune or familial in origin. The most common cause is the inadvertent removal or destruction of one or more of the tiny parathyroid glands during thyroidectomy. Other causes include previous radiation treatments to the neck area, an overdose of vitamin D or calcium, cancer (lymphoma or multiple myeloma), and a low magnesium level.
Clinical Manifestations
Decreased PTH levels in the bloodstream cause an increased serum phosphorus level and a decreased serum calcium level, resulting in neuromuscular hyperexcitability, involuntary and uncontrollable muscle spasms, and hypocalcemic tetany. Severe hypocalcemia may result in laryngeal spasm, stridor, cyanosis, and an increased possibility of asphyxia. Some patients have calcification of the basal ganglia in the brain, causing a parkinsonian syndrome with bizarre posturing and spastic movements.
Assessment
Collection of subjective data includes assessment of neuromuscular activity for symptoms such as dysphagia and numbness or tingling of the lips, fingertips, and occasionally feet and increased muscle tension leading to paresthesias (burning or prickling sensations) and stiffness. The patient may feel anxious, irritable, or depressed. The patient may experience headaches and nausea. Abdominal or flank pain may occur if a renal calculus attempts to pass down the ureter into the bladder. Assess the effectiveness of narcotics used to relieve renal colic.
Objective data include a positive Chvostek sign or Trousseau sign. If laryngeal spasm and stridor occur, cyanosis may appear. Cardiac output may decrease as a result of hypocalcemia, and the patient may develop dysrhythmias. Tetanic spasms of the extremities may be observed. The magnesium level should be monitored closely.
Diagnostic Tests
Diagnostic laboratory studies confirm the decreased serum calcium and PTH with increased urinary calcium, and increased serum phosphorus with decreased urinary phosphorus. Rule out other possible causes of hypocalcemia, such as vitamin D deficiency, kidney failure, and acute pancreatitis. Additional diagnostic testing includes electrocardiography, x-rays, and bone density scans.
Medical Management
The immediate treatment of hypoparathyroid tetany is IV administration of calcium gluconate or calcium chloride (10%). This drug irritates the vessel wall and should always be given slowly, at a rate not to exceed 1 mL/minute. The patient may complain of a hot feeling of the skin or tongue. If given too rapidly, IV calcium can precipitate hypotension, serious cardiac dysrhythmias, or cardiac arrest. Thus, electrocardiographic monitoring is indicated when administering calcium. Take care that none of the drug escapes the vein (extravasates) and moves into the tissues, since sloughing may occur. After the initial IV dose, calcium may be continued in a slow IV infusion until tetany is controlled; then it is given orally. Vitamin D is usually also given orally to increase the absorption and blood level of calcium.
Nursing Interventions and Patient Teaching
Monitor any patient receiving calcium, especially intravenously, for signs of hypercalcemia. The most common clinical manifestations of this are vomiting, disorientation, anorexia, abdominal pain, and weakness. Assess the patient for respiratory distress; renal involvement; and adverse reactions to calcium therapy, such as bradycardia, syncope, and hypotension. Use calcium cautiously in digitalized patients, since it may cause digitalis toxicity. Cimetidine (Tagamet) interferes with normal parathyroid functioning and should be used carefully in these patients. Vitamin D supplements are prescribed to improve the absorption of calcium in the intestinal tract and improve bone resorption in patients with chronic and resistant hypocalcemia. Dihydrotachysterol (Hytakerol) and calcitriol (Rocaltrol) are the preferred medications (NLM, 2010). The diet should contain foods high in calcium, such as low-fat dairy products, dark green vegetables, soybeans, tofu, and canned fish with the bones included. Offer high-calcium snacks. Patients should be encouraged to consume adequate amounts of calcium (1200 mg/day in divided doses for adults) via their diet. If this is not likely, calcium supplements should be considered. A diet low in phosphorus is also important. Foods low in phosphorus include soy milk, white rice, jam, honey, lemon-lime soda, cucumbers, lettuce, peppers, tomatoes, and non-organ meats (Rail, 2011).
Nursing diagnoses and interventions for the patient with hypoparathyroidism include but are not limited to the following:
| Nursing Diagnosis | Nursing Interventions |
| Risk for injury, related to postoperative hypocalcemia |

Teach the patient the early symptoms of hypocalcemia, with instructions to notify the nurse or health care provider if they occur. Draw blood levels of calcium and phosphorus periodically while the patient is hospitalized. Teach the patient to monitor the pulse for changes, maintain fluid balance, and use calcium supplements at home. Stress the need for life-long treatment and follow-up care, including monitoring calcium levels three or four times a year.
Prognosis
For most patients, treatment keeps the symptoms under control, and those affected have a normal life expectancy.