Glenohumeral Joint Imaging*
Kenneth Lindell, Timothy G. Sanders
Conventional Radiography
Conventional radiography is and should be the initial imaging examination performed for a patient presenting with shoulder pain. Although radiographs provide limited evaluation of the rotator cuff and glenoid labrum, they can offer important information about the source of the patient's symptoms. Radiographs depict an assortment of osseous abnormalities, including fracture, arthritis, postsurgical changes, and tumor, and they are frequently complementary to more advanced imaging modalities, such as computed tomography (CT) and magnetic resonance imaging (MRI). A wide variety of radiographic views are available to aid in the evaluation of the glenohumeral joint. Knowledge about the advantages and disadvantages of each view will assist in optimizing imaging protocols, depending on the clinical presentation (Box 44-1).1,2
Anteroposterior View
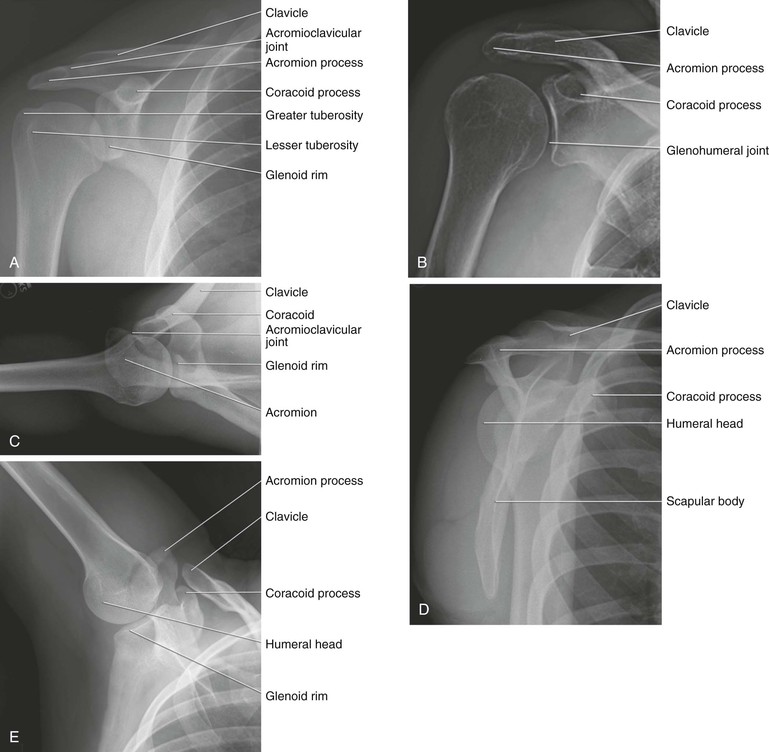
The anteroposterior (AP) view (Fig. 44-1, A) is obtained with the patient in either the upright or supine position. The beam is directed in a true AP direction relative to the body. The glenoid rim is normally tilted anteriorly about 40 degrees, which results in overlap of the humeral head and glenoid rim in the AP view. This view can be obtained with the humeral head in neutral position, internal rotation, or external rotation. When compared with other radiographic views of the shoulder, the AP view provides the best overview of the osseous structures of the shoulder girdle because the projection allows for relatively uniform distribution of soft tissue density across the entire shoulder. As a result, one or more of the AP views is nearly always included in the standard radiographic evaluation of the shoulder. These projections allow for adequate evaluation of the humeral head, glenoid, and body of the scapula, as well as the acromioclavicular (AC) joint and coracoid process. The AP projection is very helpful in the evaluation after acute trauma for evidence of fracture or dislocation and is also of value in assessing the cause of chronic pain from arthritis, impingement, calcific bursitis, tumor, or infection.
Glenohumeral “True” AP (Grashey) View
The true AP view, or Grashey view (Fig. 44-1, B), differs from the standard AP view in that the patient is rotated posteriorly 35 to 40 degrees, thus providing a tangential view of the glenohumeral joint. The advantage of the Grashey view is that it provides a superior evaluation of the glenohumeral joint. This view can demonstrate subtle subluxation in the superior or inferior direction and also will show subtle joint space narrowing associated with glenohumeral arthritis. The disadvantage of this view is that a rapid change in soft tissue density occurs from medial to lateral, and as a result, the lateral aspect of the shoulder, including the acromion and AC joint, is difficult to evaluate because of a rapid change in density on the radiograph and loss of anatomic detail laterally. This loss can be decreased with use of a boomerang-shaped filter draped along the lateral shoulder.
Axillary Lateral View
Variations of the axillary lateral view exist, but the projection is most commonly obtained with the patient supine and with the arm abducted 90 degrees (Fig. 44-1, C). The beam is then directed from distal to proximal while tilted 15 to 30 degrees toward the spine. This projection is best suited for evaluation of subtle anterior or posterior subluxation or dislocation and can also help detect subtle Bankart fractures of the anterior glenoid rim. The osseous detail on this projection, however, is often quite poor, and its main benefit is in identifying anterior or posterior dislocation. Numerous variations of this projection have been developed, some with the goal of decreasing movement of the arm in the setting of acute trauma, and others with the intention of accentuating certain anatomic features. The West Point view is a variation of the axillary view developed to optimize visualization of an osseous Bankart lesion of the anterior glenoid rim. It is obtained by placing the patient in the prone position on the x-ray table with the arm abducted 90 degrees from the long axis of the body and with the forearm draped over the edge of the top of the table. The beam is directed 15 to 20 degrees in an inferior-to-superior direction and tilted 25 degrees toward the spine. This projection improves the detection of osseous Bankart lesions but is very difficult to obtain in the setting of acute trauma and is best reserved for the patient in the setting of subacute or chronic instability.3
Scapular Y View
The scapular Y view is easily obtained in the setting of acute trauma because it can be obtained with the arm immobilized by the side, and little or no movement of the arm is required (Fig. 44-1, D). This view can be very helpful in the setting of acute trauma to evaluate for anterior or posterior dislocation. The projection is obtained with the patient upright or prone and rotated approximately 30 to 45 degrees toward the cassette. The beam is directed down the body of the scapula and results in a projection in which the body of the scapula is seen in tangent and the glenoid fossa en face as a Y-shaped intersection of the scapular body, coracoid process, and acromion process. It is also the projection commonly used when “typing” the undersurface of the acromion.
Stryker Notch View
The Stryker notch view is best suited for viewing the posterolateral aspect of the humeral head and is an excellent radiographic view for detecting flattening of the posterior humeral head or a Hill-Sachs deformity (Fig. 44-1, E). It is very limited, however, in its evaluation of the glenoid rim for osseous Bankart lesions. The Stryker notch view is obtained with the patient in either the upright or supine position. The arm is positioned vertically overhead with the elbow flexed and the hand supported on the back of the head. The beam is directed toward the mid axilla and is tilted about 10 degrees cephalad.
Acromioclavicular Articulation Views
The AC joints are best evaluated with the patient either sitting or standing with the back flat against the cassette. The arms are usually freely hanging by the sides of the body. The patient is sometimes asked to hold weights or sandbags to accentuate AC joint separation, but the value of this measure is questioned.4 The beam is directed toward the midline of the body and centered over the AC joints. This view is useful in evaluating for pathologic features of the AC joint, including fracture, AC joint separation, arthritis, and osteolysis of the distal clavicle. Comparison with the contralateral AC joint can be helpful in detecting subtle abnormalities.
Shoulder Arthrography
In the past, conventional arthrography of the shoulder (Fig. 44-2) was considered the gold standard for diagnosis of tears of the rotator cuff.5 Partial-thickness articular-sided rotator cuff tears, as well as adhesive capsulitis, are also accurately depicted with use of this method. However, partial-thickness rotator cuff tears involving the bursal surface and intrasubstance tears are not demonstrated by conventional shoulder arthrography, and its usefulness in the evaluation of glenohumeral instability is limited. This procedure is no longer widely performed.
Conventional arthrography was replaced by early CT with arthrography (CTA) performed on single-slice scanners, and films were printed in several viewing windows for review. This technique resulted in an effective tool for assessing labral injuries associated with instability, with a similar performance for cuff tears.6 However, CTA was subsequently replaced by MRI and magnetic resonance arthrography (MRA).
MRI largely replaced CTA as the advanced imaging modality for evaluation of the shoulder, and MRA has become the modality of choice for the evaluation of glenohumeral instability. The primary factors contributing to the shift from conventional arthrography and CTA to MRI are the superb soft tissue contrast, multiplanar capabilities provided by MRI, and lack of exposure to ionizing radiation. MRI allows a global assessment of the painful shoulder, including the rotator cuff, labrum and capsular structures, osseous outlet, acromion, and articular surfaces. Bone marrow edema, muscle edema, and muscle atrophy are all readily evaluated with MRI without exposure to ionizing radiation. However, CTA is effective for patients who cannot be placed in an MRI scanner because of metallic implants or shrapnel. CTA is also very fast, lasting just a few minutes, compared with the time required for an MRI scan.
Use of CTA may become more prevalent in the future as newer reconstruction algorithms decrease the amount of radiation exposure, possibly leading to increased CTA utilization. Current studies favorably compare CTA with MRI for labral imaging and imaging of rotator cuff tears.7-9 The improved performance of CTA is due to advances in imaging technologies. Picture archive and communication systems allow review of images on workstations at variable window and level settings. CT scanner technology has also advanced with multidetector scanners, which permit submillimeter-thick scan slices that can be reformatted in any plane.
Arthrography Technique
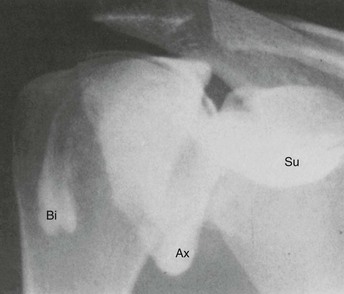
Although many variations in technique exist, a method for performing arthrography prior to MRI or CT typically begins with a review of prior radiographs or the appropriate scout films of the affected shoulder. This review ensures identification of abnormalities such as soft tissue calcifications, postsurgical changes, and possible evidence of trauma or instability. Standard scout films include AP projections of the shoulder in internal and external rotation and an axillary lateral projection. The patient is then placed supine on the fluoroscopic table with the arm positioned next to the body in slight external rotation. The anterior skin is prepared and draped in a sterile manner, and the site of joint puncture is determined fluoroscopically. A point is chosen overlying the lower third of the humeral head about 0.5 cm lateral to the medial cortex of the humeral head. An alternative anterior approach is through the rotator interval10 or a posterior approach.11 The experience of the arthrographer often dictates the approach. Knowledge of all three approaches allows for tailored techniques based on the clinical situation. Although not directly proven in the literature, a posterior approach may permit more consistent visualization of the anterior capsule structures. The skin is anesthetized with 1% lidocaine (Xylocaine) with a 25-gauge, 0.75-inch needle or ethyl chloride spray. A 22-gauge, 3.5-inch or 1.5-inch spinal needle is then used to enter the joint. The correct position is verified fluoroscopically by injecting a small amount of radiopaque contrast material. If the needle is correctly positioned within the joint, the contrast material will outline the medial surface of the humeral head and spill into the subscapularis recess and axillary pouch (Fig. 44-3).

A total injection volume of 12 to 14 mL of material provides adequate distention of the shoulder joint without undue discomfort. Injection of a larger volume often leads to decompression of the joint through a weak point of the capsular insertion along the medial aspect of the subscapularis recess, resulting in leakage of contrast material into the adjacent soft tissues. This phenomenon degrades the quality of the examination and should be avoided. The diagnosis of adhesive capsulitis is made by identifying increasing resistance to the contrast material with a small injected volume, as well as by noting an abnormally small axillary pouch and a small or absent subscapularis recess. If increased pressure is encountered during injection of the contrast agent, fluoroscopic observation should be performed to ensure that the needle tip remains intraarticular. If the contrast agent is intraarticular, the diagnosis of adhesive capsulitis is made, injection of contrast material is ceased, and the needle is withdrawn. Most practices use an iodinated contrast agent for CTA and a dilute gadolinium solution for MRA. The contrast agent can be mixed with 0.1 to 0.3 mL of 1 : 1000 epinephrine to prolong retention of the contrast agent within the joint, thus allowing adequate time for transportation of the patient to the CT or MRI scanner and for imaging. Imaging should be performed as soon as possible after injection of the contrast agent to minimize resorption of contrast material.
Computed Tomography
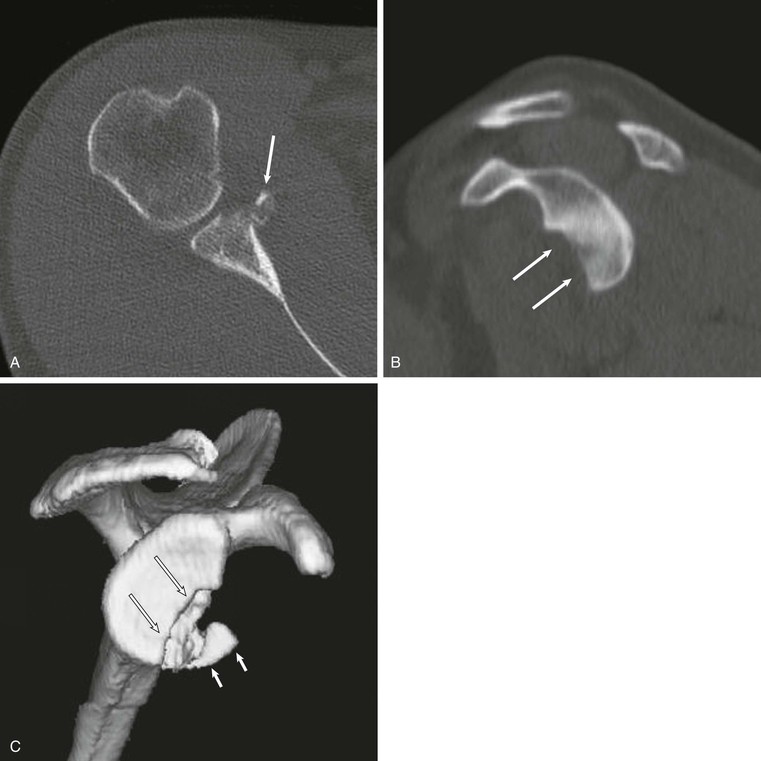
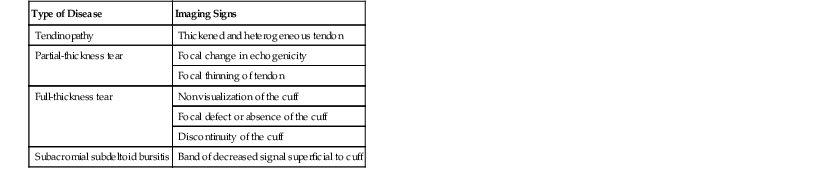
CT of the shoulder is performed primarily as a means of evaluating the osseous structures after trauma.12,13 Multidetector CT examinations with oblique sagittal and oblique coronal reconstructions can accurately detect the extent of humeral head and neck fractures. The precise number of fracture fragments, as well as the extent of displacement and angulation of fracture fragments, is accurately depicted. The scapula is a complex anatomic structure composed of the body, coracoid and acromion processes, and the glenohumeral articular surface. As a result, the full extent of scapular fractures is difficult to describe fully using conventional radiography, whereas the multiplanar capabilities of CT make it ideal for evaluation of complex scapular fractures. After glenohumeral dislocation, CT examination is the best modality to depict the size and position of a glenoid rim fracture fragment, which can be an important part of presurgical planning (Fig. 44-4). CT with three-dimensional reformations and subtraction of the humeral head is also the modality of choice for preoperative assessment of glenoid bone loss after anterior dislocations.14-16
Computed Arthrotomography
Computed arthrotomography of the shoulder was widely used prior to the development of MRI and for years was considered the gold standard in the imaging of labral abnormalities.17-19 The combination of CT with intraarticular injection of contrast material provides a highly sensitive method of evaluating the glenoid labra and articular cartilage.20,21 During the past two decades, MRI and MRA largely replaced CTA in the evaluation of rotator cuff abnormalities and glenohumeral instability.22,23 Recent reports of CTA performed with use of multidetector CT (MDCT) demonstrated accuracy equivalent to or better than MRA for proximal biceps tendon,24 anterior labral injury, and superior labral anterior to posterior (SLAP) lesions.8,25 It is especially useful in the evaluation of the shoulder in a patient with a contraindication to MRI. Axial, oblique sagittal, and oblique coronal reformatted images are obtained to provide a better evaluation of the rotator cuff and labrum and to provide the same reconstruction planes as MRI (Fig. 44-5).
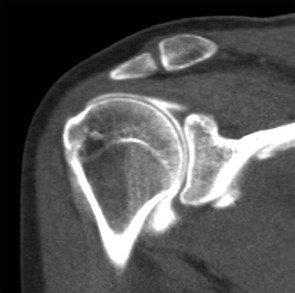
Although MDCT arthrography clearly depicts full-thickness rotator cuff abnormalities and many of the lesions associated with glenohumeral instability, MRI and MRA improve sensitivity in the detection of interstitial and bursal-sided tears, tendinopathy, and bone marrow edema without using ionizing radiation. Relative to CTA, MRI and MRA provide superior soft tissue contrast. However, MDCT arthrography with submillimeter-thick source slices allows exceptional spatial resolution, which assists in the detection of labral tears and the visualization of cartilage lesions.
Ultrasonography
Sonography of the rotator cuff (Fig. 44-6) was first popularized in the 1980s as a simple and noninvasive method of evaluating the rotator cuff,26-30 and in recent years it has been repopularized as an accurate and cost-effective method for evaluation of the rotator cuff.31-35 Ultrasound examination of the shoulder requires a high-resolution transducer (7.5 to 10 MHz). Evaluation of the shoulder is performed with the patient in the sitting position. The examination begins with the arm in the neutral (thumb up) position. In this position, the bicipital tendon (see Fig. 44-6, A) is clearly visualized at the superolateral margin of the shoulder, and the presence or absence of fluid can be noted in the subacromial-subdeltoid bursa. Before evaluation of the rotator cuff, the shoulder is rotated internally, and the arm is placed behind the back. This maneuver results in retraction of the critical portion of the supraspinatus tendon from beneath the acromion, allowing maximal visualization of this portion of the rotator cuff.36 The rotator cuff should be evaluated in both the sagittal and coronal planes.
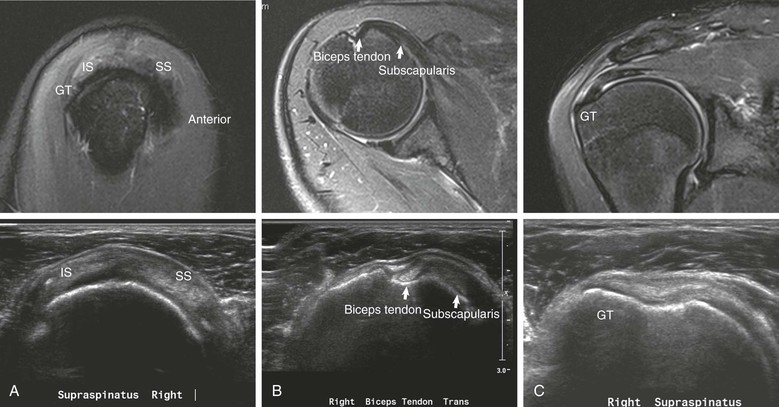
The normal rotator cuff (see Fig. 44-6) is sharply defined, uniform in thickness, and homogeneous in echo texture; it measures 4 to 6 mm in thickness anteriorly, and is normally somewhat thinner posteriorly.27 A thin echogenic band paralleling the upper surface of the cuff characterizes the subacromial-subdeltoid bursa.37 The overlying deltoid muscle is characterized by a speckled appearance that is distinct from the normal overlying cuff (Table 44-1).
TABLE 44-1
SONOGRAPHIC IMAGING SIGNS OF ROTATOR CUFF DISEASE
| Type of Disease | Imaging Signs |
| Tendinopathy | Thickened and heterogeneous tendon |
| Partial-thickness tear | Focal change in echogenicity |
| Focal thinning of tendon | |
| Full-thickness tear | Nonvisualization of the cuff |
| Focal defect or absence of the cuff | |
| Discontinuity of the cuff | |
| Subacromial subdeltoid bursitis | Band of decreased signal superficial to cuff |
Although sonography of the rotator cuff has been shown to be as accurate as MRI in the evaluation of the rotator cuff tendons,38-40 it is clear that sonographic evaluation of the shoulder has a steep learning curve and is operator dependent. Thus MRI provides a more global evaluation of the shoulder, including the labrum and osseous structures, which has led to the use of MRI in most practices.
Magnetic Resonance Imaging
MRI has evolved into the imaging modality of choice for the evaluation of shoulder impingement.23,41-49 It offers consistent soft tissue contrast superior to any other imaging modality and provides an excellent overall assessment of the osseous outlet and acromion, tendons, muscles, capsular structures, and labrum. The addition of intraarticular contrast material has also been shown to increase sensitivity in the detection of undersurface partial-thickness tears of the rotator cuff23,43,50 and abnormalities of the labrum.22,23 A 2009 metaanalysis concluded that MRA is the most sensitive and specific technique for diagnosing rotator cuff tears when compared with MRI and ultrasound.40
The type of magnet and various pulse sequences that are used to evaluate the shoulder differ according to equipment availability and the preference of the imager. Numerous commercial coils are suitable for MRI of the shoulder. Surface coils come in a variety of configurations and are generally adequate for most clinical applications. Quadrature and phased-array coils offer the highest signal/noise ratio and the best overall image quality. The arm is typically positioned next to the side to minimize respiratory artifact. For specialized views, it may be placed over the head. The arm should be placed in the neutral position with the thumb up to provide the most comfort for the patient, thus limiting motion artifact. External rotation tends to be uncomfortable for the patient and tightens the anterior capsule, resulting in poor visualization of the anterior labrum.51,52 Internal rotation may obscure the posterior labrum. Internal rotation can also result in pseudo thickening of the subscapularis tendon.53 The abduction and external rotation (ABER) position reportedly improves visualization of the undersurface of the rotator cuff, as well as of the anterior band of the inferior glenohumeral ligament and the anterior labroligamentous complex.52,54,55 The shoulder is usually imaged in three planes: the axial, oblique sagittal, and oblique coronal planes. A typical imaging protocol includes a T1-weighted sequence in the oblique coronal or sagittal plane (Table 44-2). The T1-weighted images provide the best overall signal/noise ratio and are thus excellent for depicting anatomy. T1-weighted images also nicely demonstrate the osseous anatomy of the shoulder, and because fat is bright, this sequence will demonstrate fatty atrophy of the rotator cuff. Fast spin-echo T2-weighted images with frequency-selective fat saturation are commonly obtained in the oblique coronal and oblique sagittal planes. Fluid is bright on T2-weighted images, thus allowing the most accurate detection of shoulder disease, including rotator cuff abnormalities, labral tears, bone marrow edema, and paralabral cysts. Axial imaging may be performed with use of either fast spin-echo T2-weighted or gradient-echo sequences and typically provides the best opportunity for evaluation of the anterior and posterior labra, as well as of the glenohumeral ligaments and subscapularis tendon.
TABLE 44-2
MAGNETIC RESONANCE IMAGING PULSE SEQUENCE CHARACTERISTICS
| Sequence | Image | Characteristics |
| T1-weighted image | ||
| T2-weighted image |

The use of low field strength magnets has been steadily gaining acceptance in the orthopaedic community as a cost-effective means of performing MRI of the extremities and in particular the shoulder. The advantages of a low field strength magnet include a large-bore opening of the magnet, resulting in better patient acceptance and less difficulty with claustrophobia. As a result, the low field strength systems are less constrained by patient size and body part. The lower strength of the magnet, however, results in decreased signal/noise ratio and longer scan times. The images obtained on a low field strength system are generally considered “less pretty” than the images obtained on a high field strength system, but several studies have demonstrated comparable accuracy for the depiction of rotator cuff disease (see Table 44-2). High field strength systems, however, are still considered superior and provide higher diagnostic accuracy for the detection of cartilage and labral lesions in the shoulder56 and are the most accurate for diagnosing rotator cuff tears.57
Magnetic Resonance Arthrography
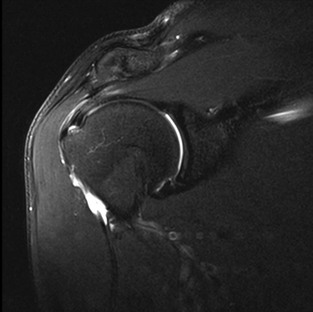
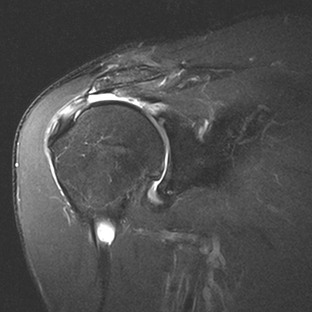
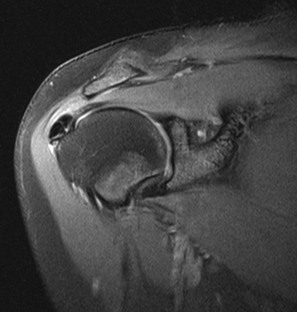
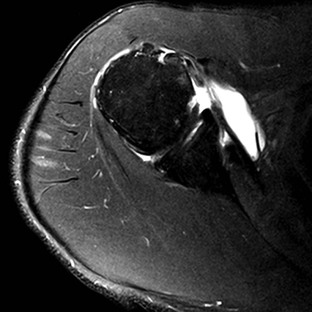
Although conventional MRI is established as the imaging modality of choice in the evaluation of shoulder impingement syndrome, MRA is accepted as the method of choice for the evaluation of glenohumeral instability.22,23 Many of the lesions associated with instability are subtle and may undergo partial healing. This situation, coupled with the fact that the normal anatomic structures of the shoulder lie in close proximity, can make the diagnosis of these lesions difficult even with high-quality conventional MRI.58-62 MRA, on the other hand, is performed by distending the joint with fluid (saline solution or dilute gadolinium), which more accurately depicts subtle labral tears, cartilage and ligamentous abnormalities, and partial-thickness tears of the undersurface of the rotator cuff. The standard injection technique for MRA of the shoulder is described in previous sections. About 12 to 14 mL of gadolinium diluted 1 : 200 with normal saline solution or 1% lidocaine is injected. Imaging protocols vary, but a standard set of imaging sequences typically includes T1-weighted images with frequency-selective fat saturation in the axial, oblique sagittal, and oblique coronal planes. The T1-weighted images have a high signal/noise ratio, resulting in the anatomic detail that is critical in detecting the subtle lesions associated with glenohumeral instability. A T2-weighted sequence performed in the oblique coronal plane is the most important sequence for depicting rotator cuff abnormalities. A T2-weighted sequence may also be helpful in detecting other pathologic processes, such as a paralabral cyst or bone marrow edema (Fig. 44-7, A and B). The ABER view may be added to the standard imaging protocol for any patient thought to have an anterior labral pathologic process.54
Imaging of Specific Shoulder Abnormalities
Interpretation of a shoulder MRI examination requires the evaluation of images obtained in several imaging planes and with various pulse sequences. The following sections provide a systematic approach for MRI evaluation as the imaging basis for recognizing common pathologic processes; when appropriate, complementary imaging modalities are discussed. The important structures that must be thoroughly evaluated on each MRI examination include osseous structures (outlet and acromion); rotator cuff muscles and tendons; the biceps tendon and rotator interval; and the labrum (capsular structures and articular surfaces).
Osseous Outlet and Acromion
The clinical syndrome of shoulder impingement refers to a painful compression of the soft tissues of the anterior shoulder (i.e., the rotator cuff, subacromial bursa, and bicipital tendon) between the humeral head and the coracoacromial arch (i.e., the coracoid process, acromion, coracoacromial ligament, and AC joint).63-65 Pain occurs when the arm is elevated forward and internally rotated or placed in the position of abduction and external rotation.64
In the normal shoulder, the upward pull of the deltoid on the proximal humerus is resisted by an intact rotator cuff so that the humeral head remains centered on the glenoid in all arm positions. If this stabilizing mechanism becomes weakened as a result of trauma, overuse, or age, the humeral head is pulled upward under the structures of the coracoacromial arch. Impingement is initially followed by subacromial bursitis and rotator cuff tendinopathy. Over time, irreversible cuff trauma occurs with fibrosis and degeneration. In the latter stages, a bony excrescence (subacromial enthesophyte) tends to form at the anteroinferior margin of the acromion where the coracoacromial ligament inserts. Tears of the rotator cuff are frequent in this stage, undoubtedly in part because of direct cuff trauma from the spur. After massive tears of the rotator cuff, bone-to-bone contact may result between the humeral head and the undersurface of the anterior third of the acromion, causing sclerosis and proliferative changes in this area.
Neer65 introduced the term impingement syndrome and described three stages with the rotator cuff disorder. For more detailed information, see Chapter 52.
The diagnosis of impingement syndrome is usually made clinically on the basis of appropriate historical and physical examination findings. A thorough history and physical examination by an experienced physician have an 84% to 90% sensitivity and a 75% to 95% specificity for diagnosis of a tear of the rotator cuff.49,66,67 Many imaging modalities are available to assist in the evaluation of the progressively painful shoulder, and their role is both to assess the extent of abnormality of the rotator cuff and to identify configurations of the osseous outlet that may predispose to rotator cuff impingement.
The osseous changes that occur with impingement are seen late and thus offer little in establishing an early diagnosis and preventing progression of the associated soft tissue injuries. The following osseous abnormalities may be associated with the clinical syndrome of impingement64,68-70:
• Enthesophyte formation on the anteroinferior aspect of the acromion
• A long anterior portion of the acromion with anterior or lateral downward sloping of the acromion
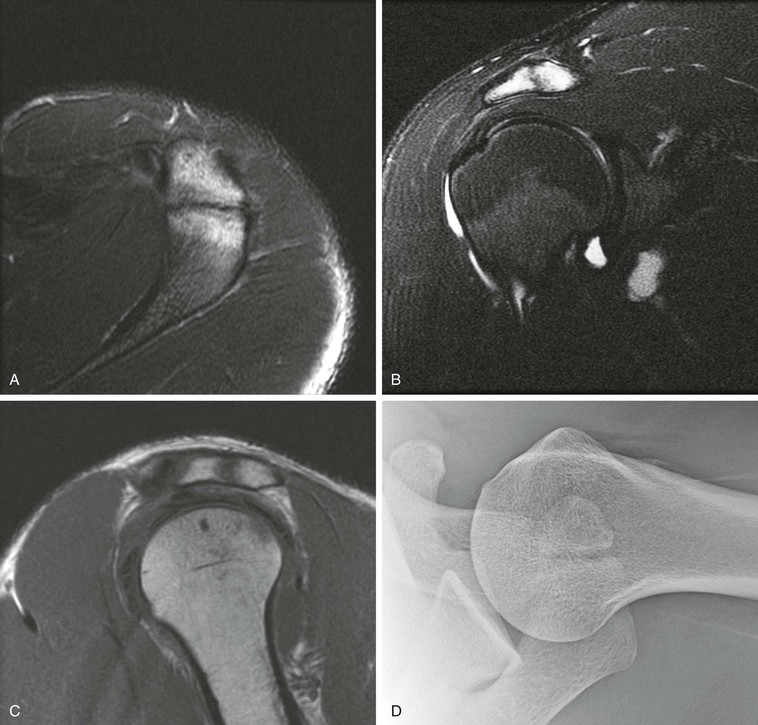
Optimal conventional radiographic views have been described for identifying these variations of the osseous outlet.71-74 The AP radiograph at a 30-degree caudal angle (Fig. 44-8) is helpful in visualizing the anterior aspect of the acromion and in detecting inferiorly directed enthesophytes.72 A modified transcapular lateral view obtained with 10 to 15 degrees of caudal angulation (the supraspinatus outlet view) helps further identify the anteroinferior aspect of the acromion.75 A high-riding humeral head with remodeling of the undersurface of the acromion and sclerosis of the greater tuberosity are conventional radiographic findings (Fig. 44-9) that are pathognomonic of a chronic rotator cuff tear. Although conventional arthrography, ultrasonography, and CT offer improved visualization of the rotator cuff relative to conventional radiography, they add little in the direct evaluation of the osseous outlet.

Magnetic Resonance Imaging of the Osseous Outlet and Acromion
The multiplanar capabilities of MRI and its ability to demonstrate the relationship of the entire osseous outlet to the underlying rotator cuff allow excellent assessment of the outlet. Bigliani68 described three different radiographic acromial shapes (Fig. 44-10) and related the configuration of the undersurface of the acromion to the presence of rotator cuff tears. A type I acromion (see Fig. 44-10, A) has a flat undersurface, a type II acromion (see Fig. 44-10, B) has a curved undersurface, and a type III acromion (see Fig. 44-10, C) has an anterior hook. The acromial types II and III have an increased association with rotator cuff tears.68,70 A type IV acromion with a convex undersurface has subsequently been described, but no definite correlation has been shown to exist between type IV acromion and impingement.76 On MRI, the shape of the acromion (see Fig. 44-10) is best assessed on the oblique sagittal view just lateral to the AC joint. One study, however, suggests poor correlation of acromial arch shape between conventional radiography and MRI.77 Another study found no association between rotator cuff tears and the acromial structure.78 A third study reported poor interobserver agreement between radiographs and MRI scans at categorization of acromial shape.79
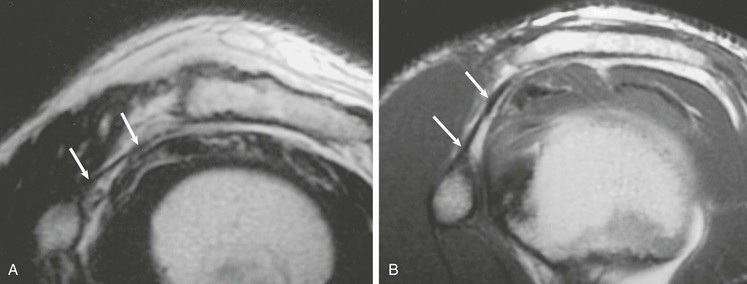
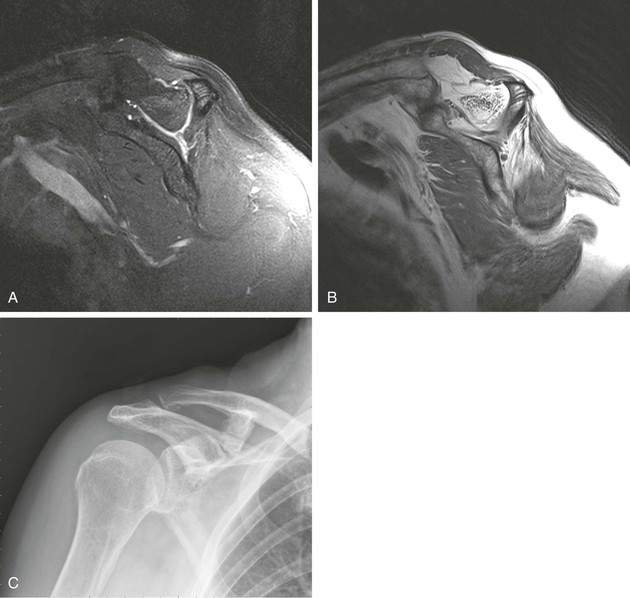
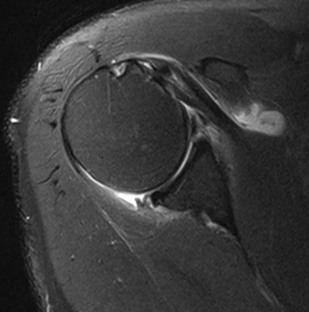
Anterior and lateral downward sloping of the anterior acromion can also narrow the supraspinatus outlet and potentially result in impingement.80,81 Anterior downward sloping (see Fig. 44-11, B) is demonstrated on oblique sagittal MRI; lateral downward sloping (see Fig. 44-11, C) is best seen on the oblique coronal images. An enthesophyte (Fig. 44-12) extending off the anteroinferior aspect of the acromion can also be clearly demonstrated on MRI. It typically appears as a marrow-containing osseous excrescence, which should have MRI signal characteristics similar to those of the adjacent acromion marrow (bright on T1-weighted images). Potential pitfalls include the attachment of the coracoacromial ligament and the deltoid tendon insertion (see Fig. 44-11, A and C) on the anterior acromion. These structures may mimic an osseous excrescence, but they can be differentiated from enthesophytes because they lack marrow signal and appear dark on all pulse sequences. The acromion should also be evaluated for os acromiale (Fig. 44-13), which is an accessory ossification center along the outer edge of the anterior acromion. It is normally fused by 25 years of age. An association exists between persistent os acromiale and impingement of the rotator cuff.82-86 The deltoid muscle attaches to the inferior aspect of the accessory ossicle, and contraction of the deltoid results in a downward motion of the unstable segment, potentially leading to impingement of the underlying rotator cuff. Os acromiale is demonstrated best on axial images (see Fig. 44-7, A), but it can also be seen on oblique sagittal or oblique coronal images (see Fig. 44-7, B),85 on which it should not be confused with the adjacent AC joint. MRI signs of instability of the os acromiale include fluid signal within the synchondrosis or sclerosis, cystic change, or marrow edema on either side of the synchondrosis (Box 44-2).
Hypertrophic changes of the capsule and inferiorly directed osteophyte formation of the AC joint (see Fig. 44-13) can also be associated with impingement.64 MRI demonstrates these changes, as well as associated mass effect on the underlying rotator cuff. The coracoacromial ligament (Fig. 44-14) is a soft tissue structure that forms part of the coracoacromial arch. It extends from the coracoid to the acromion and is well seen on oblique sagittal MRI. It normally measures less than 2 mm in thickness and extends across the rotator interval and anterior aspect of the supraspinatus tendon. The role of the coracoacromial ligament in impingement remains controversial; some persons believe that thickening or ossification (see Fig. 44-14, B) of the ligament may be a potential cause of impingement, whereas others believe that thickening results from impingement.87,88
Coracohumeral impingement, also referred to as subcoracoid impingement, is an uncommon cause of extrinsic impingement that results from a narrowed distance between the coracoid process and the underlying humeral head (Fig. 44-15). Lo and Burkhart89 suggested using an interval less than 6 mm to make the diagnosis at arthroscopy. On axial images the normal interval is approximately 10 mm. A narrowed coracohumeral distance may result in entrapment of the subscapularis tendon between the coracoid process and the humeral head and can lead to isolated tendinosis and disruption of the subscapularis tendon. Abnormalities isolated to the subscapularis tendon should prompt an investigation of the coracohumeral distance and consideration of this diagnosis.90,91 However, after reporting on a small series of patients with subcoracoid impingement at arthroscopy and control subjects, Giaroli et al.90 concluded that subcoracoid impingement is primarily a clinical diagnosis that may be supported with imaging.
Glenoid Dysplasia
Glenoid dysplasia occurs along a spectrum.92 The most severe cases can be appreciated on shoulder radiographs, with a hypoplastic glenoid visible on frontal or oblique views of the shoulder (Fig. 44-16).93 More subtle cases will be seen on MRI as retroversion of the glenoid fossa relative to the scapula or deficiency of the posterior inferior glenoid resulting in a rounded or “S” shape of the posterior inferior glenoid.94,95 Harper et al.94 reported an incidence of 14% in their series of 103 consecutive MRI examinations, as well as an association with posterior labral tears. Weishaupt and collegues95 reported an association between posterior shoulder instability and glenoid rim deficiency. Although severe cases may be seen with radiographs, milder cases should be sought on lower axial images and by assessing the sagittal images of the posterior inferior glenoid rim (see Fig. 44-16). Glenoid dysplasia is associated with increased risk of posterior instability and a posterior labral tear.

Rotator Cuff
The rotator cuff is composed of four tendons: the supraspinatus superiorly, the subscapularis anteriorly, and the infraspinatus and teres minor posteriorly. These tendons are important dynamic stabilizers of the glenohumeral joint, and any review of rotator cuff disease will rapidly expose the supraspinatus tendon as the weak link of the rotator cuff. Most cuff failures originate in the supraspinatus tendon at or near its insertion onto the greater tuberosity of the humeral head. Some investigators attribute this propensity for cuff failure within the supraspinatus tendon to its blood supply.96 The supraspinatus tendon receives its arterial supply from the anterior humeral circumflex, subscapular, suprascapular, and posterior humeral circumflex arteries.97,98 A zone of relative avascularity has been described in the tendon proximal to its attachment site and may represent a “critical zone” for cuff failure.97 Other authors have found this zone to be vascularized by anastomosing vessels from the tendon and humeral tuberosity.99 Arterial filling of the cuff vessels in the critical zone depends on the position of the arm; poor filling is present when the arm is adducted.97 A high correlation has also been shown to exist between rotator cuff tears and subacromial impingement.65 It is probably a combination of avascularity and subacromial impingement that leads to most rotator cuff abnormalities originating in the critical zone of the supraspinatus tendon.
Conventional radiography plays only a limited role in the direct evaluation of the rotator cuff, although it is frequently the initial imaging study performed for patients with the clinical syndrome of impingement. Radiographs allow identification of associated pathologic change, especially of the osseous outlet and acromion. Conventional radiography findings associated with cuff pathology include the following2,100,101:
• A high-riding humeral head (<7 mm between the humeral head and the undersurface of the acromion) is associated with a chronic rotator cuff tear
• Scalloping and loss of normal acromion undersurface convexity (see Fig. 44-9)
Magnetic Resonance Evaluation of the Rotator Cuff
The normal anatomy of the rotator cuff is accurately depicted with MRI. The supraspinatus muscle originates along the posterosuperior portion of the scapula above the level of the scapular spine. A single tendon arises out of the muscle and extends superiorly above the humeral head to insert onto the greater tuberosity of the humeral head. The supraspinatus tendon is best evaluated in the oblique coronal and oblique sagittal MRI planes. The subscapularis is located anteriorly and has multiple tendon slips. It has a broad origin along the anterior aspect of the scapula and attaches to the lesser tuberosity on the anterior aspect of the humeral head. An extension of the subscapularis tendon known as the transverse ligament extends across the intertubercular groove and helps to stabilize the long head of the biceps tendon within the intertubercular groove. The subscapularis muscle and tendon are best evaluated on axial and oblique sagittal MRI. The infraspinatus is located posterosuperiorly and has a broad origin along the posterior aspect of the scapula inferior to the scapular spine. The teres minor is located posteroinferiorly, below the level of the infraspinatus, originating along the axillary surface of the scapula and inserting on the most inferior aspect of the greater tuberosity of the humeral head. The infraspinatus and teres minor are best evaluated on oblique coronal and oblique sagittal images.
The normal tendons demonstrate uniformly dark signal intensity on all pulse sequences; increased signal on T1-weighted images is a nonspecific finding that may represent a wide array of conditions ranging from artifact to a complete tear. T2-weighted images with fat suppression have a lower signal/noise ratio and provide less anatomic detail, but they are both sensitive and specific for depicting the full range of rotator cuff abnormalities.
Increased signal within the rotator cuff tendons on T1-weighted images has many causes. When increased signal is noted on T1-weighted images, the morphologic features of the tendon and the T2-weighted images should be evaluated.67 A normal appearance of the tendon and normal signal intensity on T2-weighted images suggest that the tendon is probably normal. Potential causes of increased signal within a normal tendon on T1-weighted images include partial volume averaging and the “magic angle” phenomenon. This MRI artifact results in increased signal in normal tendons that are angled 55 degrees relative to the direction of the main magnetic field. It occurs primarily on T1-weighted images, and as echo time lengthens, as occurs with T2 weighting, the signal intensity again decreases. This MRI artifact is particularly likely to occur in the critical zone of the supraspinatus tendon and therefore occasionally causes confusion about the integrity of the cuff.
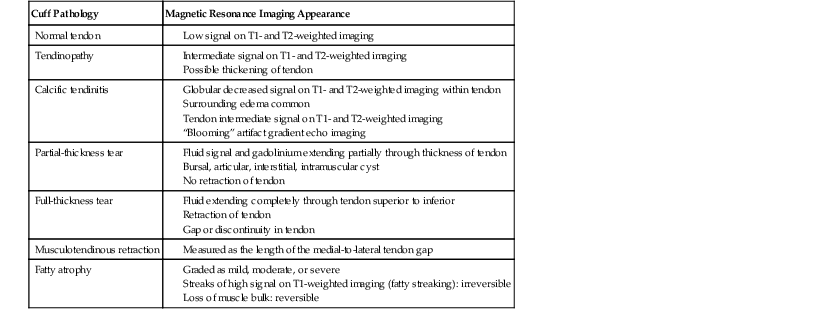
A wide spectrum of rotator cuff pathology can be accurately depicted on MRI, ranging from tendinosis to a full-thickness tear of the rotator cuff (Table 44-3). Tendinosis (Fig. 44-17) is noted as intermediate signal on T1-weighted MRI that persists on T2-weighted MRI. The signal abnormality does not reach the same brightness as fluid on T2-weighted images (see Fig. 44-17, B). The tendon may also demonstrate diffuse or focal thickening, but no evidence of tendon disruption will be seen. Tendinosis represents a degenerative process of the tendon, which histologically represents a combination of inflammation and mucoid degeneration.102 On arthroscopic examination, the tendon may appear to be edematous and hyperemic, with occasional fraying, roughening, or degeneration of the surface of the tendon, and it may be difficult at times to differentiate tendinosis from early partial-thickness tearing both at arthroscopy and on MRI.103
TABLE 44-3
MAGNETIC RESONANCE IMAGING APPEARANCE OF ROTATOR CUFF PATHOLOGY
| Cuff Pathology | Magnetic Resonance Imaging Appearance |
| Normal tendon | |
| Tendinopathy | |
| Calcific tendinitis | |
| Partial-thickness tear | |
| Full-thickness tear | |
| Musculotendinous retraction | |
| Fatty atrophy |
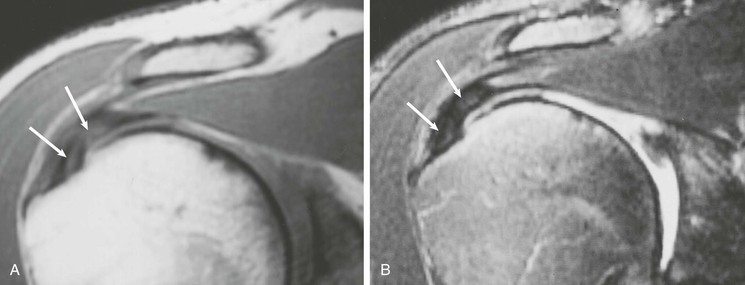
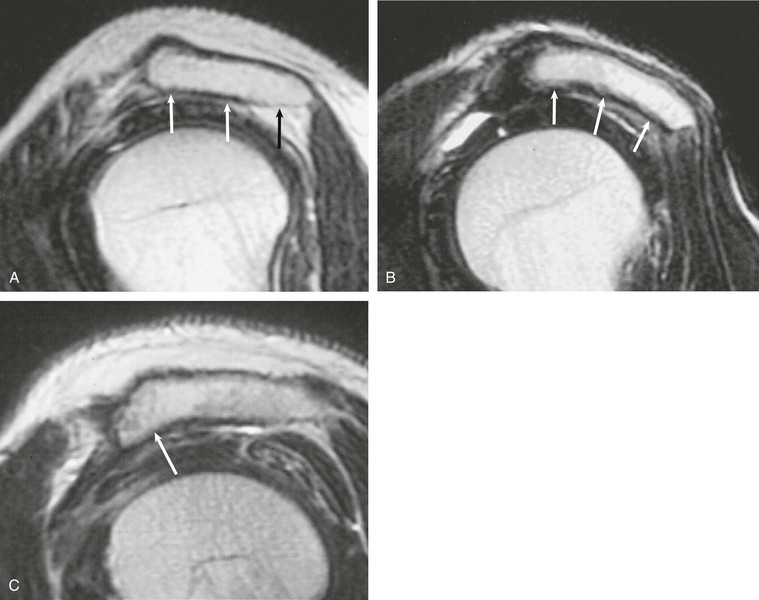
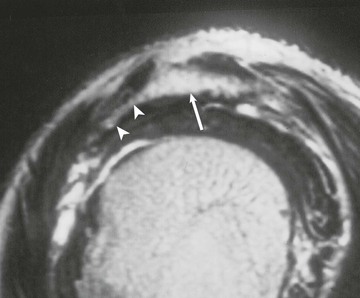
Partial-thickness tears (Figs. 44-18, 44-19, and 44-20) can occur on either the articular surface or the bursal surface or within the substance of the tendon. Articular surface tears are the most common type to occur (see Fig. 44-18). A partial-thickness tear is seen on MRI as an area of increased signal on T1-weighted images that increases to fluid signal intensity on T2-weighted images. The fluid signal intensity extends only partially through the thickness of the tendon from superior to inferior. These tears may partially heal with granulation tissue, making them difficult to distinguish from tendinopathy on MRI. MRA is more sensitive than conventional MRI in detecting articular surface tears; however, it does not increase sensitivity for detecting partial-thickness tears of the bursal surface. It has been suggested that the sensitivity for detecting partial-thickness undersurface tears can be further improved by adding the ABER view to the MRA protocol.55,104,105
Interstitial tears of the rotator cuff represent tears that occur within the substance of the tendon but do not involve the bursal or the articular surface (Fig. 44-19). These tears are demonstrated on MRI as a focal linear area of fluid signal that is contained within the substance of the tendon, and they typically occur at the footprint of the supraspinatus tendon as it attaches to the greater tuberosity of the humeral head.
A partial articular-sided supraspinatus tendon avulsion lesion is a subset of partial-thickness tears.106,107 The tear represents a partial-thickness articular-sided avulsion of the supraspinatus tendon at its most anterior attachment site. This type of tear deserves special attention and should be accurately described on MRI because the recommended treatment for this subset of tendon tears differs from the standard partial-thickness tears described previously. On MRI, a small articular-sided avulsion is seen as fluid signal extending into the articular surface of the supraspinatus tendon at its anterior attachment site with partial avulsion of the tendon at this level, and this lesion represents a subset of the articular surface partial-thickness tears (Fig. 44-20).
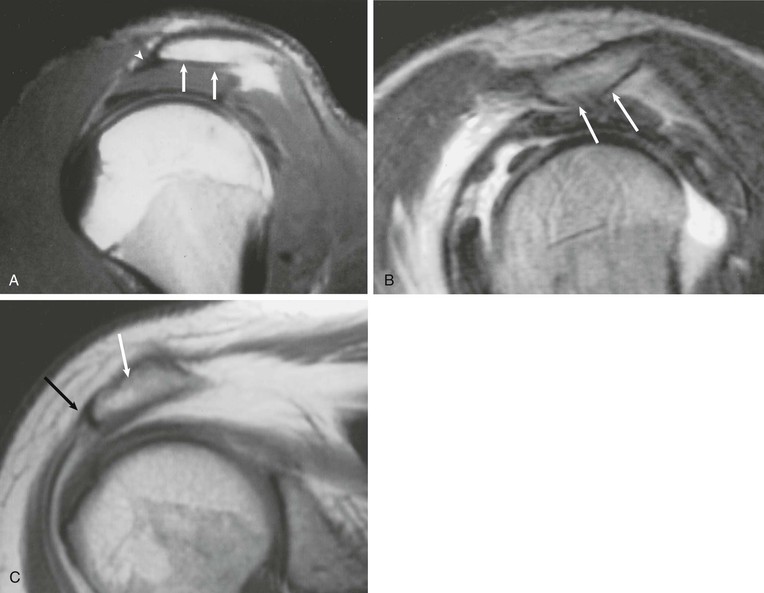
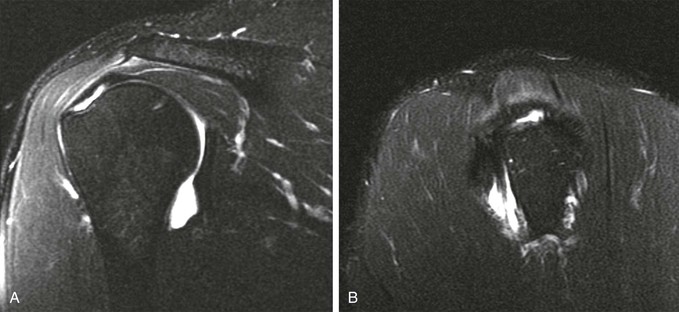
A full-thickness tear of the rotator cuff tendon is defined as a tear that extends through the complete thickness of the tendon from superior to inferior. This tear allows communication between the joint space and the subacromial-subdeltoid bursa. MRI criteria for establishing the diagnosis of a full-thickness tear include high (fluid) signal completely traversing the tendon from superior to inferior on T2-weighted images, a gap or absence of the tendon, and retraction of the musculotendinous junction (Fig. 44-21).
Rotator cuff muscles can undergo atrophy after tendon tears or after denervation. Denervation results in muscle edema followed by progressive fatty infiltration. Chronic rotator cuff tendon tears also result in muscle atrophy even if no nerve injury is present. The terminology with regard to atrophy of the rotator cuff musculature is confusing. The term fatty infiltration is typically used to describe actual fatty infiltration or replacement of the muscle, whereas muscle atrophy is used to describe a loss of muscle bulk. Muscle atrophy is seen on MRI as loss of muscle bulk (best depicted on sagittal images through the cuff musculature), whereas fatty infiltration is seen as streaks of high T1-weighted signal within the substance of the muscle (Fig. 44-22). When they are normal, the four muscles of the rotator cuff demonstrate symmetric bulk and signal characteristics. Loss of bulk indicates muscle atrophy, whereas streaks of high T1-weighted signal within the substance of the muscle indicate fatty infiltration. Goutallier and colleagues reported a system for grading fatty infiltration of the cuff musculature on the basis of CT imaging,108,109 and although this system has been widely adapted for use with MRI, a study by Fuchs and associates110 demonstrated poor correlation between CT and MRI with regard to grading fatty infiltration. Fatty infiltration is typically graded as mild, moderate, or severe based on the extent of fatty infiltration (high T1-weighted signal) with the belly of the muscle. Muscle atrophy can be graded separately as mild, moderate, or severe on the basis of muscle bulk depicted on sagittal images at the level of the supraspinatus fossa. Regardless of the terms used to describe muscle atrophy and fatty infiltration, they are associated with poor functional outcomes after rotator cuff tendon repair and increased risk of a repeat tear.111 Assessment of preoperative MRI scans should include evaluation of muscle atrophy.
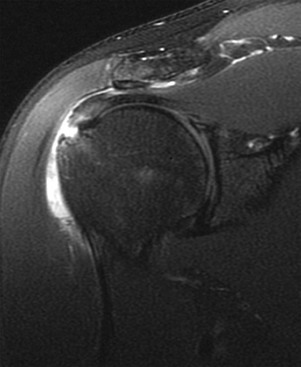
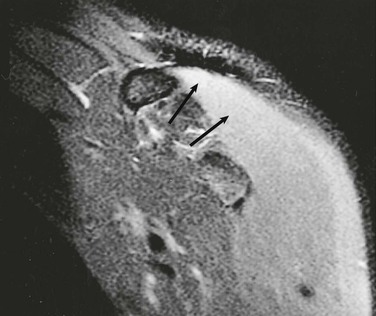
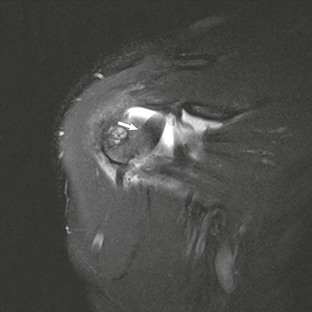
Calcific tendinitis (hydroxyapatite crystal deposition disease) can also be diagnosed with MRI (Fig. 44-23). The crystalline deposits are typically within the critical zone of the rotator cuff and appear as areas of low signal intensity on both T1- and T2-weighted images. Calcific deposits within the rotator cuff may be difficult to identify on MRI because both the tendon and the calcific deposit appear dark on all pulse sequences. Ancillary MRI findings that may aid in the identification of calcific tendinitis include globular thickening of the involved tendon and high signal within the tendon and surrounding tissues as a result of associated inflammation. Gradient-echo imaging may improve conspicuity of the deposits as a result of the “blooming” artifact associated with local magnetic field heterogeneity. Use of gradient-echo imaging and comparison with conventional radiographs improve the likelihood of detecting calcific tendinitis.
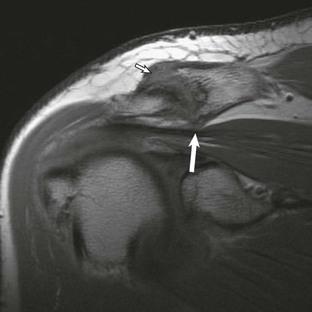
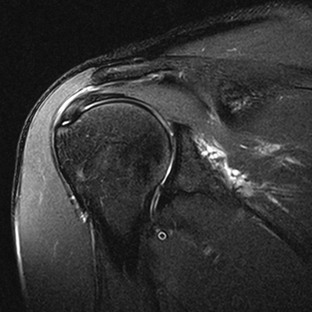
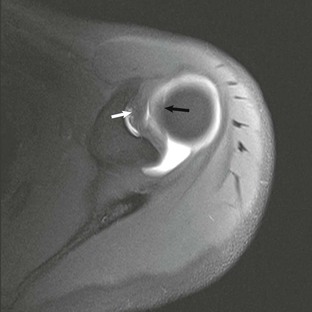
Most cuff tears originate in the supraspinatus tendon; however, large tears may extend into either the infraspinatus or subscapularis tendon. Isolated tears, although less common, occasionally occur in either the infraspinatus or subscapularis (Fig. 44-24) tendon. An isolated tear of the infraspinatus tendon is usually associated with the internal impingement syndrome (discussed further in the section on glenohumeral instability).104 An isolated tear of the subscapularis tendon may result from shoulder dislocation or in association with coracohumeral impingement112 and is best demonstrated on axial MRI as high signal traversing the tendon with retraction of the tendon away from its normal attachment site on the lesser tuberosity. An extension of the subscapularis tendon known as the transverse ligament holds the long head of the biceps tendon in the intertubercular groove, and a tear of the subscapularis tendon may result in disruption of the transverse ligament, leading to medial subluxation or dislocation of the long head of the biceps tendon.113 Axial MRI is well suited not only for evaluating the integrity of the subscapularis tendon but also for demonstrating medial subluxation of the biceps tendon out of the intertubercular groove. The biceps tendon may be displaced superficial to the subscapularis tendon, into the subscapularis tendon (Fig. 44-25) or intraarticular (Fig. 44-26).
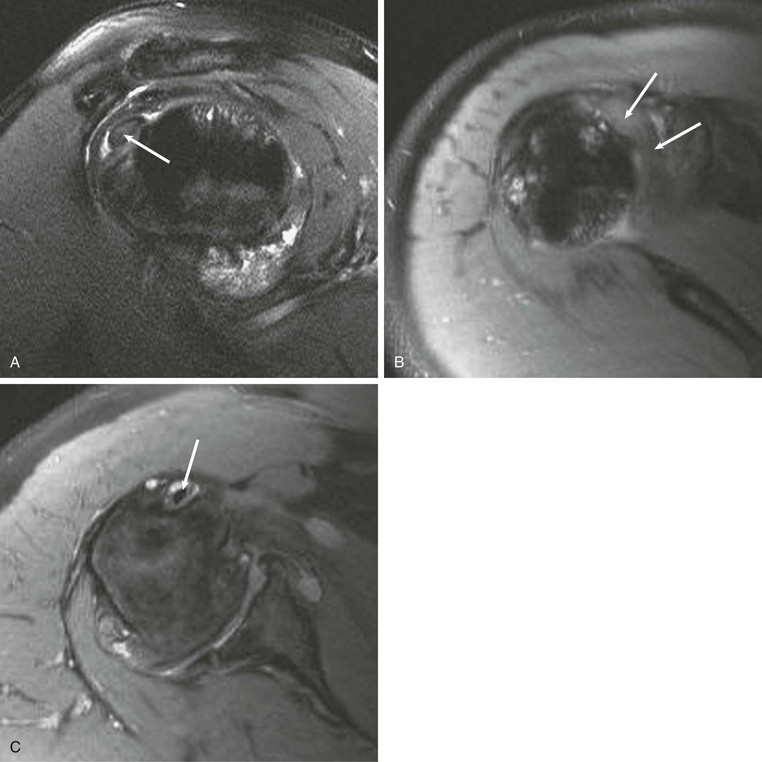
An intramuscular cyst within the rotator cuff (Fig. 44-27, A and B) has been described as a finding associated with small full-thickness tears or partial-thickness articular-sided tears of the rotator cuff.114 Intramuscular cysts are similar to paralabral cysts of the shoulder or meniscal cysts of the knee. Fluid leaks through a defect in the cuff and tracks in a delaminating fashion along the fibers of the tendon, resulting in a fluid collection contained within either the muscle or fascia of the rotator cuff. These cysts have been reported in the supraspinatus, infraspinatus, and subscapularis muscles and appear as oval lobulated collections of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images. Identification of an intramuscular cyst of the rotator cuff should prompt a thorough search for a small associated cuff tear.
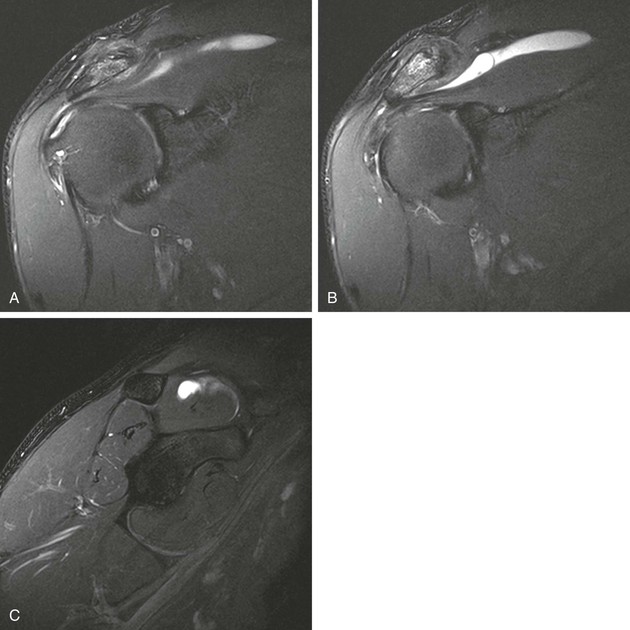
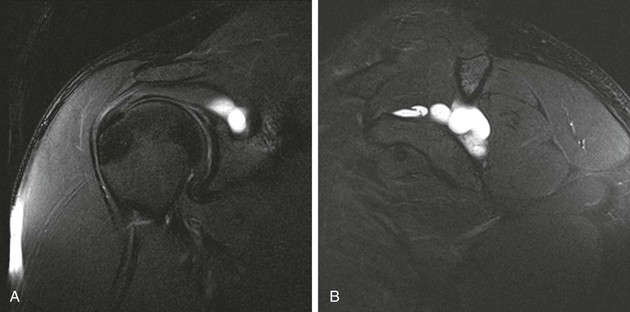
Denervation of a rotator cuff muscle can result from either a compressive neuropathy or an acute traumatic injury of a nerve. Compressive neuropathies most commonly result from a paralabral cyst associated with a labral tear, but they can also be caused by fractures or other masses in the area of the shoulder (see Fig. 44-23, A and C). Paralabral cysts (Fig. 44-28) most commonly arise in association with a SLAP tear or a posterior labral tear. These cysts may extend into either the suprascapular notch or the spinoglenoid notch and can result in entrapment of the suprascapular nerve, which innervates the supraspinatus and infraspinatus muscles.115 Paralabral cysts arising from an anteroinferior labral tear are less common, but they may compress the axillary nerve as it traverses the quadrilateral space.116 Compression of the axillary nerve can also result from adhesive bands in the quadrilateral space in athletes, such as pitchers, who participate in repetitive overhead activities.117 The axillary nerve innervates both the teres minor and deltoid muscles. Anterior dislocation can result in a stretching injury of the axillary nerve and give rise to a temporary or permanent denervation of the teres minor and deltoid muscles and can occasionally mimic a rotator cuff tear on clinical examination in a person with previous anterior dislocation. Denervation atrophy initially results in edema of the affected muscles and over time will progress to an irreversible fatty replacement. On MRI, acute denervation edema appears as a high T2-weighted signal within the affected muscle and is associated with reversible muscle atrophy (Fig. 44-29). The more chronic and irreversible form of fatty atrophy appears as decreased muscle bulk and bright streaks (representing the fat) within the muscles on T1-weighted images (see Fig. 44-23).
Rotator Interval, Biceps, and the Biceps Pulley
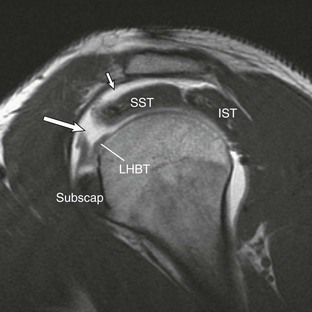
The rotator interval is a triangular space in the anterosuperior aspect of the rotator cuff that is bordered by the anterior margin of the supraspinatus and the superior margin of the subscapularis muscle. The interval allows passage of the long head of the biceps tendon from an intraarticular to an extraarticular location and plays an important role in glenohumeral stability; it also facilitates normal function of the biceps tendon. The biceps pulley refers to the sling formed by the coracohumeral ligament and superior glenohumeral ligament in the lateral aspect of the rotator interval where the biceps tendon exits the joint.118 Injury or disease of the interval can be associated with altered range of motion of the glenohumeral joint, adhesive capsulitis, and signs of anterior superior impingement119 or degenerative arthropathy. Isolated injuries of the interval can occur or may be associated with tears of the most anterior aspect of the supraspinatus tendon or the superior leading edge of the subscapularis tendon. Baumann et al.120 suggest that isolated lesions to the pulley are more common than originally believed and that progression to involvement of adjacent rotator cuff tendons occurs.
Rotator Interval and Biceps Pulley Anatomy
The rotator interval is the gap between the anterior supraspinatus and upper subscapularis tendons. The roof of the rotator interval is formed by the coracohumeral ligament along the bursal surface and the superior glenohumeral ligament along the articular surface. The coracohumeral and superior glenohumeral merge anteriorly and laterally to form the biceps tendon “sling” that is primarily responsible for stability of the long head of the biceps tendon as it transitions from its intraarticular position within the rotator interval to its extraarticular position within the intertubercular groove.121-124
The coracohumeral ligament arises from the base of the coracoid process, extending across the anterior aspect of the glenohumeral joint to insert onto the lesser and greater tuberosities of the humeral head, forming the bursal lining of the rotator interval roof. The coracohumeral ligament is composed of the medial limb (which courses inferiorly from its origin on the coracoid process to insert onto the superior margin of the subscapularis tendon and the lesser tuberosity) and the lateral limb (which courses in a more horizontal fashion to its insertion on the anterior edge of the supraspinatus tendon and the adjacent greater tuberosity). The medial limb is primarily responsible for preventing medial subluxation of the long head of the biceps tendon, and the lateral limb resists superior migration of the humeral head.
The superior glenohumeral ligament arises from the superior glenoid tubercle adjacent to the origin of the long head of the biceps tendon and courses deep to the coracoid process and the coracohumeral ligament to insert onto the lesser tuberosity of the humeral head and comprises the articular lining of the roof of the rotator interval. A second portion of the superior humeral ligament extending from the anterior superior labrum to the lesser tubercle and the transverse humeral ligament was described by Kask et al.125 Together the coracohumeral and superior glenohumeral ligaments surround and merge anteriorly around the intraarticular biceps tendon. The long head of the biceps tendon originates from the superior glenoid tubercle and then crosses the joint in an oblique fashion, sitting within the rotator interval, and is covered by the coracohumeral and superior glenohumeral ligaments. The long head of the biceps tendon exits the joint at the level of the intertubercular groove where it is completely covered and stabilized by these two ligaments. At this point, the combination of the medial limb of the coracohumeral ligament and superior glenohumeral ligament acts as a sling to prevent medial subluxation of the long head of the biceps tendon as it exits the joint. The rotator interval is best visualized and evaluated for disease in the oblique sagittal plane, especially when the joint is distended either by a joint effusion or by intraarticular contrast. Schaeffeler et al.126 reported improved sensitivity for biceps pulley lesions by evaluating the biceps tendon for displacement relative to the subscapularis tendon with MRA.
The rotator interval plays an important role with regard to static glenohumeral stability. The coracohumeral ligament and the superior glenohumeral ligament combine to limit external rotation of the humeral head. The superior glenohumeral ligament also contributes the least to glenohumeral stability by limiting inferior subluxation of the humeral head while the arm is in 0 degrees of abduction. The coracohumeral ligament limits superior migration of the humeral head. Disease processes that affect the rotator interval can limit external rotation of the humeral head, whereas injury to the rotator interval can contribute to anterior, superior, and inferior instability of the glenohumeral joint, thus leading to progressive degenerative arthropathy. The biceps pulley and rotator interval also play an important role with regard to the stability of the long head of the biceps tendon (Box 44-3).125
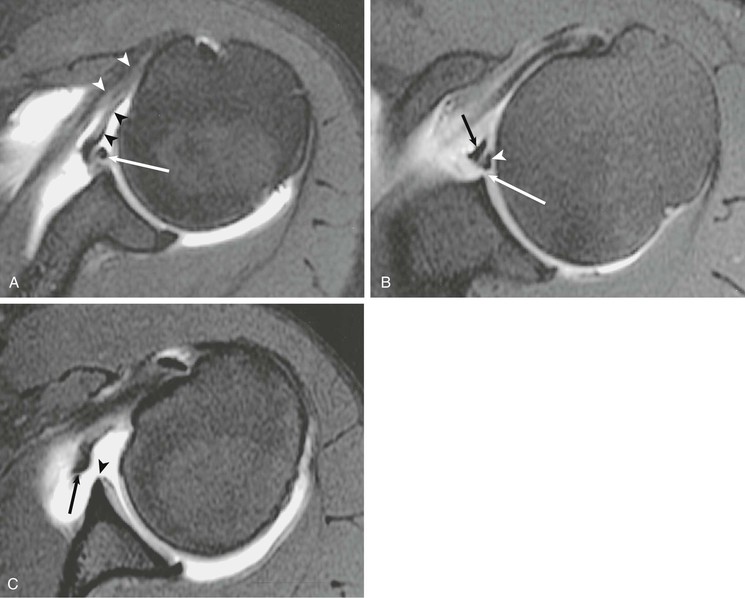
A tear of the rotator interval can result from an acute traumatic event or from repetitive microtrauma isolated tears of the rotator interval; they most commonly are diagnosed in conjunction with a tear of the anterior portion of the supraspinatus tendon and/or the upper subscapularis tendon. Disruption of the rotator interval can result in shoulder pain and allow superior migration of the humeral head (microinstability). MRI findings of an isolated rotator interval tear include a high T2-weighted signal isolated to the rotator interval or disruption of the capsule of the rotator interval.124 Direct MRA improves detection of the disrupted capsule at the level of the interval and may actually demonstrate leakage of contrast material through a defect into the subacromial-subdeltoid bursa or extension of contrast to the posterior surface of the coracoid process as reported by Vinson et al.124 (Fig. 44-30). Schaeffeler et al.126 recommended caudal or anterior displacement of the biceps tendon because they are more sensitive than previously proposed criteria for pulley lesions.
Long Head of the Biceps Tendon
The tendon of the long head of the biceps is an important stabilizing structure of the glenohumeral joint, contributing to both superior and anterior stability.127 Like any other tendon, the long head of the biceps tendon can be involved in a broad array of injuries ranging from tenosynovitis and tendinosis to partial or complete tears. Because of the unique anatomic configuration of the biceps tendon, subluxation or dislocation can occur in conjunction with tears of the rotator cuff or isolated injuries of the subscapularis tendon.113 SLAP tears, which can also be associated with injuries of the proximal biceps tendon, are discussed in another section and are not addressed here. The course and morphologic appearance of the long bicipital tendon can be evaluated with sonography, CT, MRI, or MRA; however, the superior soft tissue contrast and multiplanar capabilities afforded by MRI make it the imaging modality of choice. A thorough evaluation by any shoulder imaging study should include an assessment of the course and appearance of the long bicipital tendon.
The normal course of the tendon begins as the tendon arises from the long head of the biceps muscle in the upper arm. The tendon then courses through the intertubercular sulcus, located between the lesser and greater tuberosities. As it passes through the intertubercular sulcus, it is held in place inferiorly by the tendon of the pectoralis major muscle as it attaches to the proximal humeral shaft. At the intertubercular groove, it is held in place by the transverse ligament, which is an extension of the subscapularis tendon. Superiorly, it becomes intraarticular, being located in the rotator interval and covered by the coracohumeral ligament and finally by the superior glenohumeral ligament. These two ligaments form the “sling” or pulley mechanism responsible for the stability of the biceps tendon as it transitions from its intraarticular to its extraarticular location.121,128 It then has a broad triangular attachment to the superior labrum at or near the superior glenoid tubercle.
Conventional MRI accurately depicts both the location and the morphologic features of the extraarticular portion of the tendon, whereas MRA improves detection of subtle intraarticular abnormalities of the tendon at or near its proximal attachment site. Tenosynovitis can result from repetitive trauma or from an inflammatory process such as rheumatoid arthritis, and it is usually depicted on MRI as increased fluid, sometimes containing complex debris or bodies within the bicipital tendon sheath. The tendon sheath normally communicates with the shoulder joint; therefore, only significant amounts of fluid isolated to the bicipital tendon sheath or fluid quantities out of proportion to associated joint effusions are suggestive of this diagnosis. Tendinosis is a little farther along the spectrum of injury and includes degeneration of the bicipital tendon, which is depicted on MRI as thickening and increased signal within the substance of the tendon (Fig. 44-31).129,130 A partial or complete tear of the long bicipital tendon may result from repetitive microtrauma or from an isolated traumatic injury. It most commonly occurs in middle-aged men as a result of impingement, with rupture usually occurring near the proximal aspect of the intertubercular sulcus. Partial tears may be seen as attenuation of the tendon or thickening with markedly increased T2 signal (Fig. 44-32). Complete tears result in nonvisualization of the tendon in the bicipital groove.

The “hourglass” biceps tendon describes a condition featuring marked tendinosis and hypertrophy isolated to the intraarticular portion of the long bicipital tendon, which prevents the tendon from sliding into the bicipital groove during elevation of the arm.131 Entrapment of the long bicipital tendon causes a mechanical block and pain. This condition occurs most often in association with a full-thickness tear of the rotator cuff, although entrapment occurring in association with partial-thickness rotator cuff tears has been described in case reports as well. Patients present with anterior arm pain and loss of passive elevation of the arm averaging about 10 to 20 degrees. The condition is treated with resection of the abnormal segment and tenodesis of the biceps tendon followed by appropriate treatment of any concomitant injury of the rotator cuff. MRI will show marked tendinosis and thickening limited to the intraarticular portion of the biceps tendon (Fig. 44-33) and is often associated with either a partial- or full-thickness rotator cuff tear.
Subluxation or dislocation of the tendon out of the intertubercular sulcus can result from injury to the overlying stabilizing structures.113 A tear of the coracohumeral ligament will result in medial subluxation of the long bicipital tendon, and three patterns of subluxation have been described that are related to the status of the subscapularis tendon and the coracohumeral ligament (Table 44-4). First, disruption of the coracohumeral ligament in conjunction with a complete tear or avulsion of the subscapularis tendon off of the lesser tuberosity will result in an intraarticular subluxation or dislocation. The long bicipital tendon will sublux medially into the anterior aspect of the glenohumeral joint, medial to the intertubercular groove. Second, a tear of the coracohumeral ligament in conjunction with a tear of the transverse humeral ligament (superficial fibers of the subscapularis tendon) will result in extraarticular subluxation of the long bicipital tendon, and the tendon will be located medial to the intertubercular groove but superficial to the intact fibers of the subscapularis tendon. Finally, an isolated tear of the coracohumeral ligament with an intact subscapularis tendon and transverse humeral ligament will allow medial migration of the long bicipital tendon into the substance of the subscapularis tendon, resulting in interstitial tearing of the tendon. This lesion is the so-called hidden lesion because the abnormal position of the tendon may not be visible to the arthroscopist. Preoperative MRI can alert the surgeon to the abnormal position of the long bicipital tendon because axial MRI nicely depicts the location of the long bicipital tendon medial to the intertubercular groove (see Fig. 44-26).
TABLE 44-4
PATTERNS OF MEDIAL SUBLUXATION: LONG BICIPITAL TENDON
| Torn Structures | Location of Medially Subluxed Tendon |
| Coracohumeral ligament Subscapularis tendon | Intraarticular |
| Coracohumeral ligament Transverse humeral ligament | Extraarticular (superficial to subscapularis) |
| Isolated coracohumeral ligament tear | Within substance of subscapularis tendon or muscle (“hidden lesion”) |
The rotator interval is an unsupported part of the glenohumeral joint capsule and as such is prone to disorders that affect the synovium, including inflammatory arthritides and adhesive capsulitis. Evaluation of the rotator interval in these disorders is best performed with either direct or indirect MRA using the oblique sagittal images.
Adhesive Capsulitis (Frozen Shoulder)
Adhesive capsulitis is a pathologic entity unique to the shoulder that is characterized by inflammation and thickening of the synovium. The inflammatory changes are most prominent in the areas of the capsule that lack reinforcement by the rotator cuff tendons, most notably the rotator interval and axillary recess. Women 40 to 70 years of age are most often affected; patients present clinically with the insidious onset of shoulder pain followed by progressive stiffness and weakness of the glenohumeral joint. The onset of symptoms is often related to a previous episode of minor trauma, but it may be idiopathic or associated with preexisting rheumatologic disorders or diabetes. At the time of clinical presentation, patients are often misdiagnosed with impingement syndrome or rotator cuff disease because the signs and symptoms broadly overlap with those of adhesive capsulitis. Physical examination demonstrates a painful restriction of motion of the shoulder in all directions, but the most pronounced restriction of motion usually involves external rotation of the humeral head (Box 44-4).
The clinical presentation and age distribution of patients with adhesive capsulitis overlap with those of rotator cuff disease, and as a result, imaging can play an important diagnostic role. No conventional radiographic signs are diagnostic of adhesive capsulitis, although radiographs may be helpful in excluding other sources of pain and decreased range of motion. Conventional arthrography demonstrates a small contracted joint capsule with a decreased joint volume of less than 10 mL. The axillary pouch appears small and contracted, and there is a lack of contrast material filling the long head of the biceps tendon sheath.
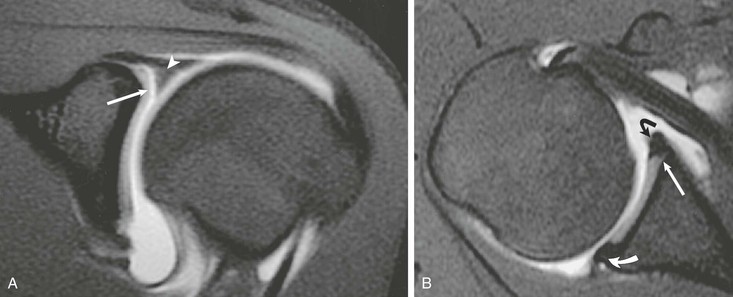
MRI findings include abnormal soft tissue in the rotator interval, obliteration of the subcoracoid fat triangle, and thickening of the coracohumeral ligament. Thickening of the joint capsule (normal is <4 mm) may also be seen in the region of the axillary pouch (Fig. 44-34). Inflammatory changes of the capsule may also be seen as increased T2-weighted signal adjacent to the capsule of the axillary pouch. The use of MRA may be helpful in establishing the correct diagnosis in two ways. First, a decreased joint volume of less than 10 mL will be noted, similar to conventional arthrography. Second, the contrast material will help outline and define the abnormal soft tissue in the rotator interval. Indirect MRA, however, appears to be most specific for establishing the diagnosis of adhesive capsulitis on the basis of imaging. Findings include enhancement of the abnormal soft tissues within the rotator interval combined with enhancement of the capsule and adjacent soft tissues in the region of the axillary pouch (see Box 44-4).132-134 However, Gondim Teixeira et al.135 recently reported high sensitivity and specificity with use of increased T2-weighted signal on fat-suppressed images in the capsule without the use of contrast material.

Labrum and Capsular Structures
Glenohumeral instability is a complex topic in terms of diagnosis and treatment of shoulder injuries. The anatomic configuration of the shoulder allows extensive range of motion, but it also predisposes the shoulder to instability. Instability can be the result of insult to any of the static or dynamic stabilizers of the joint. The clinical definition of shoulder instability is the symptomatic displacement of the humeral head out of the glenoid fossa, and various schemes have been developed to classify shoulder instability. These schemes include the temporal relationship of the instability to previous trauma (first time vs. recurrent), the degree of instability (subluxation vs. dislocation), and the direction of instability (anterior inferior, posterior, inferior, anterior superior, posterior superior, or multidirectional). Instability can also be related to congenital factors including glenoid dysplasia. For more details on the diagnosis and classification of instability, see Chapters 46, 47, and 48.
Although the initial imaging study after suspected shoulder dislocation or recurrent glenohumeral instability is usually conventional radiography, it provides only a limited evaluation of the shoulder, with detection of such abnormalities as fractures, persistent dislocation, and abnormal soft tissue calcifications. MRA is considered the most accurate way to study the labrum and capsule structures. As described earlier, MDCT arthrography has been reported to be comparable to MRA for evaluating the labrum and capsule.8,25
Conventional radiography is often complementary to more sophisticated imaging techniques in the evaluation of glenohumeral instability. The imaging protocol for conventional radiography varies, depending on personal preference, but it should include the basic views, which will enhance the detection of osseous abnormalities. For patients with a history of antecedent trauma, views should be selected that optimize visualization of the Hill-Sachs deformity, anterior trough defect, and Bankart lesion.136 The Garth view,137 the AP view with the shoulder in internal rotation, the axillary view, and the Stryker notch view improve detection of the posterior Hill-Sachs deformity and of the anterior trough defect (see Fig. 44-35). The anterior and posterior glenoid rim is best imaged on the axillary view or one of its many variations. An osseous Bankart lesion involving the anteroinferior glenoid rim is best visualized on the Garth view or the West Point view.3 The patient's condition should also be taken into consideration in selecting radiographic views because the standard axillary view may be difficult to obtain in the setting of acute trauma. In these situations, one of the many axillary variants may be easier to obtain. In the setting of recurrent subluxation with no antecedent trauma, it is recommended that two tangential views be obtained to identify subtle subluxation of the humeral head. A true anteroposterior glenohumeral (Grashey) view will aid in the detection of inferior subluxation, and one of the axillary view variants will demonstrate anterior or posterior subluxation.

The radiographic findings associated with glenohumeral instability include the Hill-Sachs and Bankart osseous abnormalities, which occur when the posterior aspect of the humeral head has an impact on the anteroinferior glenoid rim at the time of anterior dislocation. The Hill-Sachs lesion is seen as flattening or a wedge-shaped defect involving the posterosuperior aspect of the humeral head; the bony Bankart lesion is seen as a small fracture or area of cortical irregularity involving the anteroinferior glenoid rim. Although these radiographic findings lack sensitivity, they are specific for previous anterior dislocation and indicate that injury has occurred to the labroligamentous complex, which may predispose the patient to recurrent glenohumeral instability. At the time of posterior dislocation, the anterior aspect of the humeral head has an impact on the posterior glenoid rim, creating an anterior trough defect in the anterior aspect of the humeral head and a “reverse Bankart” lesion involving the posterior glenoid rim. Subluxation can be a subtle radiographic finding that may indicate glenohumeral instability, and it is best detected on tangential views of the glenohumeral joint. The center of the humeral head should be centered within the glenoid fossa, and any asymmetry may indicate subluxation or persistent dislocation (Box 44-5).
MRI and MRA are the main imaging modalities used in the evaluation of a patient with glenohumeral instability.22,23 Even with 3-tesla magnets, MRA demonstrated superior sensitivity compared with routine MRI in a study of 150 consecutive examinations for detecting SLAP lesions and labral tears.138 Joint distention with fluid outlines and separates the normal anatomic structures, allowing more accurate depiction of subtle lesions (Fig. 44-36). CT imaging with sagittal and coronal reconstructions remains the study of choice for detecting and depicting the size and location of a fracture fragment of the anteroinferior glenoid rim (see Fig. 44-4), which can be useful in presurgical planning in patients with large osseous Bankart lesions. As previously stated, MDCT arthrography is accurate for detecting instability lesions and very useful for patients who cannot undergo MRA or lack access to MRI services. The addition of MRI stress views, such as the ABER view (see Fig. 44-37, C), may improve visualization of a nondisplaced tear in the anterior inferior labrum.54
MRA of Glenohumeral Instability
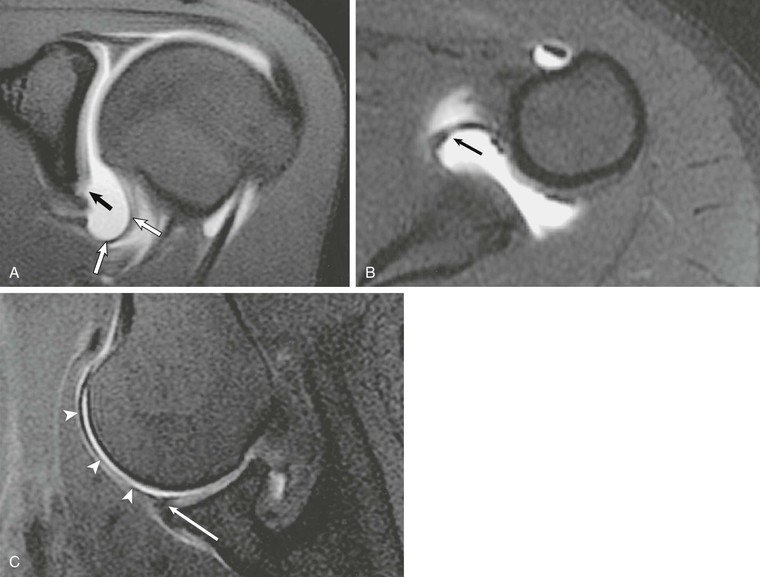
Articulation of the large surface area of the humeral head with the small surface area of the glenoid fossa allows extensive range of motion of the shoulder but also predisposes it to instability. The various soft tissue structures in the area of the shoulder improve joint stability. The glenoid labrum and capsular structures act as static stabilizers, whereas the rotator cuff provides dynamic stabilization of the glenohumeral joint. The glenoid labrum is a thickening of the joint capsule that inserts into the periphery of the osseous glenoid and functions to deepen the shallow glenoid fossa, providing extended coverage of the humeral head.139-141 The superior labrum (Fig. 44-38) is best visualized on coronal MRI and appears as a dark triangular structure extending off of the superior glenoid rim. The anterior and posterior labra (see Fig. 44-36, B) are best seen on axial and coronal images, typically appearing as dark triangular structures; on occasion, however, the normal labrum may appear rounded, blunted, or flattened.140,142 Three glenohumeral ligaments, which represent thickenings of the capsule, also serve to improve stability of the shoulder.
The inferior glenohumeral ligament (see Fig. 44-37, A) is the most important of the three thickenings and functions primarily to improve glenohumeral stability with the arm in abduction and external rotation.143 It is composed of three separate components: the anterior band, posterior band, and axillary pouch.144,145 The origin of the inferior glenohumeral ligament is somewhat variable; it arises from either the inferior glenoid labrum or adjacent osseous glenoid. It then inserts in a collarlike fashion along the medial aspect of the humeral neck. It is lax when the arm is in neutral position and appears redundant when the arm is imaged in the standard planes on MRA (see Fig. 44-37, A and B). The middle glenohumeral ligament (Fig. 44-39) is less important as a stabilizer, but it is responsible for preventing external rotation of the arm during abduction between 60 and 90 degrees.146 In terms of size, it is the most variable of the three ligaments, ranging from a thick cordlike ligament to complete absence.147 It arises from the superior glenoid tubercle adjacent to the origin of the biceps tendon and superior glenohumeral ligament and then courses obliquely in an inferolateral direction to merge with the deep fibers of the subscapularis tendon just before attaching to the humeral neck. It is typically seen on axial MRI deep to the subscapularis muscle and superficial to the anterior labrum, occasionally mimicking an avulsed fragment of the anterior labrum.
The superior glenohumeral ligament (see Fig. 44-38) contributes to shoulder stability, although a report suggests that it provides some degree of restraint, preventing inferior subluxation of the humeral head when the arm is in 0 degrees of abduction.148,149 It arises from the superior glenoid tubercle adjacent to the attachment of the biceps tendon and then courses obliquely and anteriorly to merge with the coracohumeral ligament before its attachment on the humeral head. The superior glenohumeral ligament forms the floor of the rotator interval and also plays a role in stability of the long head of the biceps tendon, merging with the coracohumeral ligament to form the biceps pulley.124,125,127 It is consistently visualized on axial MRA images as a thick bandlike structure arising from the glenoid tubercle and paralleling the coracoid process.145
Several normal anatomic variations have been described that, on MRA, can mimic a labral tear.150 Most of these occur in the anterior superior quadrant of the labrum and include the following variations:
• Cartilage undermining—smooth, tapering, intermediate-signal hyaline cartilage that partially undermines the superior labrum (see Fig. 44-36, B)136,139,151
• Sublabral recess—a potential space between the labrum and underlying glenoid that appears as a smooth tapering fluid collection that only partially undermines the superior labrum with no labral displacement (see Fig. 44-36, A)152; a tear differs in that it will show an irregular surface of the labrum with possible labral detachment or displacement (see Fig. 44-40, A)
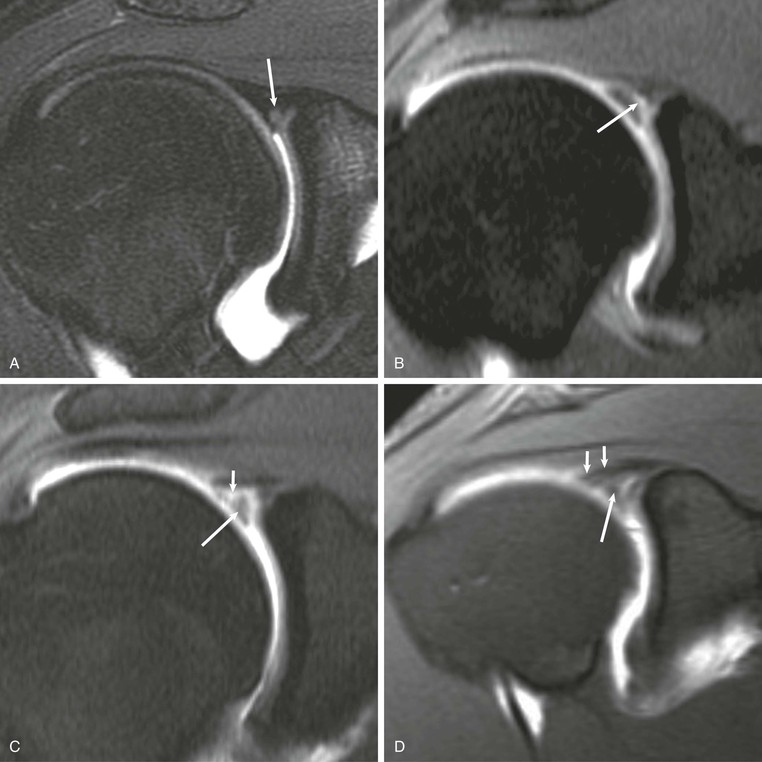
• Sublabral foramen—complete detachment of the superior labrum that occurs only in the anterosuperior quadrant147,153; it appears on MRI as a fluid-filled gap between the labrum and the osseous glenoid (see Fig. 44-39, B)
• Buford complex—absent or diminutive anterosuperior labrum associated with a thick, cordlike middle glenohumeral ligament that can mimic a displaced tear of the anterior labrum on MRI (see Fig. 44-39, C)142,145,147,153
MRA of Multidirectional Glenohumeral Instability
The diagnosis of multidirectional instability is usually established solely on the basis of history and physical examination findings; MRI adds little to the evaluation. No specific MRI findings confirm the diagnosis of multidirectional glenohumeral instability, but in the atypical case, it may help to exclude a concurrent Bankart or other labral lesion.154
MRA of Posttraumatic Anterior Glenohumeral Instability
A wide variety of glenolabral lesions exist, and in a given patient, the specific lesion depends on the mechanism of injury that led to the labral abnormality. Unidirectional instability may be further classified as anterior or posterior in direction. Anterior glenohumeral instability usually results from a fall on the outstretched arm or stress while in abduction and external rotation. In patients younger than 35 years, the typical lesion resulting from an anterior dislocation is either a Bankart lesion or a Bankart variant. In the patient older than 35 years with a first-time anterior shoulder dislocation, the resulting lesion is usually either a tear of the supraspinatus tendon, a tear of the subscapularis tendon, or an avulsion injury of the greater tuberosity of the humeral head. Posterior instability occurs less commonly than anterior instability and can result either from a single traumatic event resulting in posterior dislocation of the humeral head or from repetitive microtrauma as occurs in weight lifters, football linemen, and swimmers. Finally, a miscellaneous category of lesions includes the SLAP tear and internal impingement syndrome.
Acute anterior dislocation of the humeral head in the young patient typically results in disruption of the anterior labroligamentous complex, and Bankart is generally credited with the first description of this lesion in 1923. The classic Bankart lesion (Fig. 44-41) is composed of an avulsion of the anterior labroligamentous complex from the glenoid with disruption of the medial scapular periosteum. The MRI appearance of a Bankart lesion varies, depending on the age of the lesion, but the anteroinferior labrum typically loses its normal triangular configuration and becomes irregular or amorphous in appearance. A discrete tear may be seen as an irregular collection of contrast material extending into the labrum. In the acute lesion, the anterior labrum may be displaced away from the adjacent glenoid, whereas in the more chronic injury, the labrum may scar back down to the glenoid and demonstrate minimal displacement, making it more difficult to identify at the time of imaging or at arthroscopy. On occasion, an associated fracture of the inferior glenoid rim (an osseous Bankart lesion) or of the posterosuperior humeral head (a Hill-Sachs deformity; Fig. 44-42) may result from an impaction injury at the time of dislocation. Although both of these osseous abnormalities are accurately depicted on MRI, CT examination with sagittal reconstructions is often considered the imaging modality of choice for detecting and depicting the size and appearance of the osseous Bankart lesion (see Fig. 44-5).14
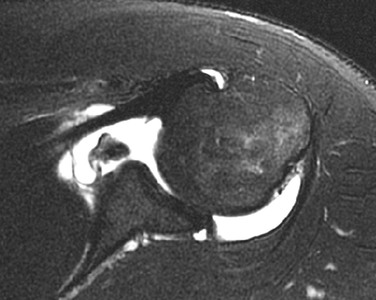
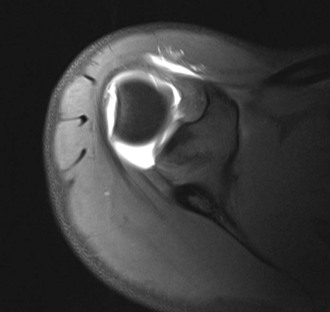
Two Bankart variants that have potential therapeutic and diagnostic ramifications have been described (Table 44-5). The classic Bankart lesion is composed of a tear of the anterior labrum coupled with disruption of the medial scapular periosteum, resulting in displacement of the anterior labroligamentous complex. Both Bankart variants differ from the classic Bankart lesion in that the medial scapular periosteum remains intact, preventing complete separation of the labrum from the adjacent osseous glenoid.
TABLE 44-5
BANKART VARIANTS
| Lesion | Description |
| Bankart | Anteroinferior labral tear with disrupted medial scapular periosteum |
| Osseous Bankart | Anteroinferior labral tear with adjacent glenoid rim fracture |
| Perthes (nondisplaced Bankart) | Nondisplaced anterior inferior labral tear with an intact medial scapular periosteum |
| Anterior labroligamentous periosteal sleeve avulsion (ALPSA; medialized Bankart) | Medial anteroinferior labral tear; torn labrum displaced medially by an intact medial scapular periosteum |
| Reverse Bankart | Posteroinferior labral tear |
The first of these variations was initially described by Perthes in 1906 and has subsequently been referred to as the Perthes lesion.61,154 This Bankart variant consists of a nondisplaced tear of the anteroinferior labrum held in nearly anatomic position by an intact medial scapular periosteum (Fig. 44-43). The tear may eventually resynovialize, making identification of the labral tear difficult at arthroscopy or on MRI. The clinical importance of the Perthes lesion is that glenohumeral instability may persist in the face of a resynovialized nondisplaced tear, and at arthroscopy, the surgeon must probe the anterior labrum to determine whether it is incompetent. Identification of a nondisplaced anterior labral tear may be difficult with MRA, but it may be aided by applying stress to the anterior labroligamentous complex. The application of stress is accomplished by positioning the arm in the ABER position (see Fig. 44-37, C), which places traction on the anterior band of the inferior glenohumeral ligament, thereby pulling the partially detached labrum away from the glenoid and allowing the tear to fill with contrast material. When a nondisplaced tear of the anterior labrum is identified at MRA, the surgeon should be alerted so that the anterior labrum is adequately probed to avoid inadvertently missing the nondisplaced tear.
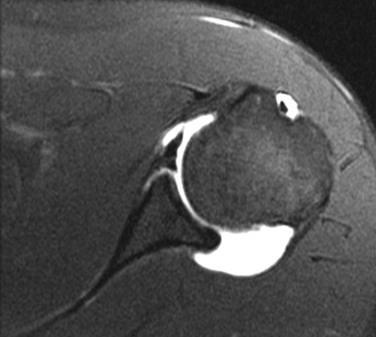
Neviaser60 described a second variation of the Bankart lesion, which he referred to as the anterior labroligamentous periosteal sleeve avulsion (ALPSA) lesion. The ALPSA lesion is similar to the Perthes lesion in that the medial scapular periosteum remains intact. In the ALPSA lesion, however, the labrum is displaced medially and rolls up on itself like a sleeve is rolled up the arm. The labrum then heals in this abnormal medialized position. The ALPSA lesion is sometimes referred to as the medialized Bankart (Fig. 44-44). MRA accurately depicts the position of the labrum and demonstrates its medial displacement.154 The ALPSA lesion is treated arthroscopically by releasing the labrum from its abnormal position followed by anatomic restoration of the Bankart lesion, thereby securing the labrum in its normal anatomic position.60
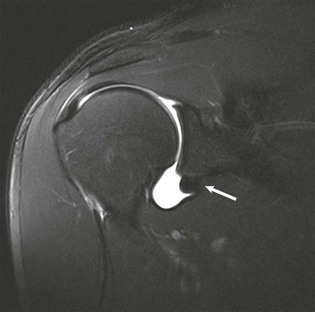
First-time dislocation in patients older than 35 to 40 years sometimes leads to a set of lesions different from those seen in the younger patient. As a patient ages, the rotator cuff tendons gradually degenerate and over time become the weak link among the various anatomic structures responsible for anterior shoulder stability.60,112,143 First-time dislocation after age 35 years therefore uncommonly results in a Bankart lesion but usually results in one of the following three lesions:
• Tear of the supraspinatus tendon (Fig. 44-45, A)
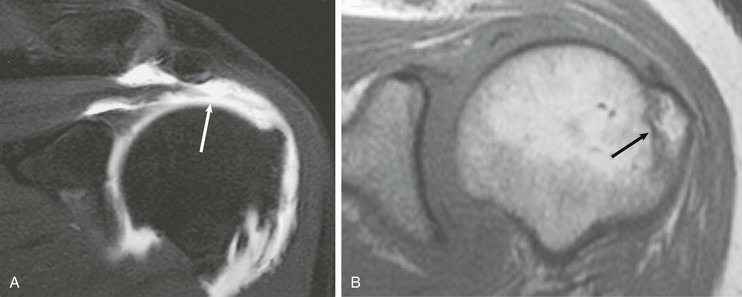
• Avulsion fracture of the greater tuberosity of the humeral head (see Fig. 44-45, B)
• Avulsion or tear of the subscapularis tendon and anterior capsular structures (see Fig. 44-25)
MRA can play a pivotal role in directing the appropriate therapy in the older patient after a first-time anterior dislocation of the shoulder. The patient with rotator cuff rupture will have weakness on abduction and may be incorrectly diagnosed with an axillary nerve injury.112,155 This group of patients may benefit from surgical repair, depending on the extent of the rotator cuff tear. The patient with a greater tuberosity avulsion fracture is usually treated conservatively, whereas the patient with an avulsion of the subscapularis and anterior capsule is likely to have recurrent instability and persistent pain and will require surgical repair to regain stability.156 MRA can accurately differentiate these lesions, thereby directing clinical management by correctly identifying patients who would benefit most from surgical intervention. MRA clearly depicts a rotator cuff rupture as high signal contrast extending through the rotator cuff defect and retraction of the musculotendinous junction. Axillary nerve palsy, which initially results in denervation edema, is seen on MRI as high signal within the muscle on T2-weighted images (see Fig. 44-29). Chronic denervation of the rotator cuff eventually leads to fatty atrophy, which is characterized by increased signal on T1-weighted images.116,117,157,158 An avulsion fracture of the greater tuberosity is depicted as a dark fracture line extending through the greater tuberosity on all MRI pulse sequences. Surrounding bone marrow edema in the acute fracture is depicted as increased signal on T2-weighted images or decreased signal intensity on T1-weighted images. Finally, an avulsion injury of the subscapularis and anterior capsular structures is best depicted on axial images using MRA. Extension of contrast material will be seen between the subscapularis tendon and the lesser tuberosity. Retraction of the musculotendinous junction may also be noted.147,159-161
MRA of Posterior Glenohumeral Instability
Posterior shoulder instability is less common than anterior instability, and a full description is included in Chapter 47. It typically results from either a single traumatic event or repetitive microtrauma as in weight lifters or swimmers and can be a difficult entity to diagnose and treat.162,163 Traumatic posterior dislocation usually results from a fall on the outstretched arm with the arm positioned in adduction and internal rotation. In this position, the posterior capsule becomes taut, and any force directing the humeral head posteriorly can result in disruption of the posterior capsule or labrum (see Fig. 44-46, A). Similar lesions are seen in anterior and posterior glenohumeral instability, but the term “reverse” is typically applied to the lesions associated with posterior instability (e.g., a reverse Bankart or reverse Hill-Sachs lesion). MRA accurately depicts a posterior labral tear as high signal contrast extending into the tear with displacement and abnormal morphologic features of the labrum (see Fig. 44-46, B). Osseous injuries, including a reverse Hill-Sachs lesion or a reverse osseous Bankart abnormality, are also depicted (Fig. 44-47).22,164
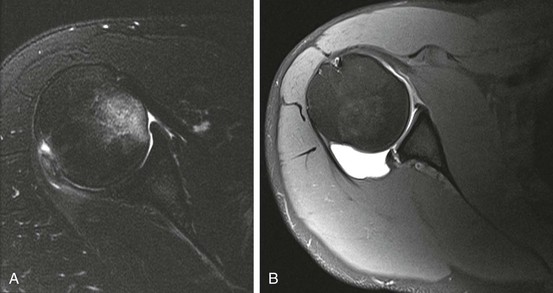

SLAP Lesion
The acronym SLAP was coined by Steve Snyder and colleagues in 1990 to describe a tear of the superior labrum.165 Two different mechanisms have been proposed as potentially leading to the SLAP lesion. The first is a fall on the outstretched arm that results in compressive forces on the superior labrum; the second is traction from a traumatic pull or repetitive microtrauma from recurrent overhead activity, such as throwing or swimming. Patients with a SLAP injury typically present with shoulder pain, aggravated by overhead activities, and may also report a catching or popping sensation. Physical examination is often unreliable in establishing the diagnosis of a SLAP tear, although stress maneuvers may indicate that an abnormality involves the biceps anchor. For a more detailed description including treatment options, see Chapter 49.
Treatment varies, depending on the type of SLAP tear, but generally involves arthroscopic debridement or arthroscopic repair if conservative therapy fails.166-168
Since the original report of the SLAP lesion, numerous articles have described the conventional MRI and MRA findings.169-173 MRA is both sensitive and accurate as a technique for diagnosis of SLAP tears. The SLAP lesion is usually best seen on oblique coronal MRI (see Fig. 44-40). Contrast material extends into the normally dark triangle of the superior labrum, representing either marked fraying or detachment from the glenoid. The SLAP lesion can easily be confused with several normal anatomic variants that occur in the anterosuperior quadrant of the labrum. These variants are the superior labral recess (see Fig. 44-36, A), the sublabral foramen (see Fig. 44-39, B), and potentially the Buford complex (see Fig. 44-39, C). A tear can often be differentiated from these normal variations because abnormal signal extends into the tear, which is usually irregular in appearance, and the labrum may actually pull away from the glenoid. In type III and type IV SLAP lesions, a labral fragment is often seen dangling from the superior labrum and is outlined by intraarticular contrast material. Contrast material seen extending into the substance of the superior labrum or biceps anchor is abnormal and is diagnostic of a SLAP tear (see Box 44-5). In addition to identifying the abnormality of the superior labrum, it is important to detect any extension of the SLAP tear to adjacent structures because involvement of adjacent structures can have an impact on proper surgical treatment. SLAP lesions can extend to involve the inferior labrum in either the anterior or posterior quadrants. SLAP lesions can also extend to involve the superior or middle glenohumeral ligaments and can also be associated with rotator cuff disease.
GLAD Lesion
Neviaser59 first described the glenolabral articular disruption (GLAD) lesion as a superficial tear of the anteroinferior labrum associated with an injury of the adjacent articular cartilage. It is caused by a forced adduction injury to the shoulder with the arm positioned in abduction and external rotation. The injury results from an impaction of the humeral head against the glenoid fossa without anterior subluxation or dislocation. The patient presents clinically with persistent shoulder pain but demonstrates no evidence of instability on physical examination. This lesion is probably the first along the spectrum of instability lesions resulting from a fall on an outstretched arm. The labral tear is superficial and nondisplaced; as a result, it does not lead to clinically identifiable instability. The pain is most likely due to catching of the cartilage flap as it contacts the moving humeral head.67
The abnormalities associated with the GLAD lesion are subtle and may be undetectable on routine MRI of the shoulder. MRA, however, has been shown to increase the sensitivity of detecting subtle labral lesions.22,42 The following findings are noted on MRA in a patient with the GLAD lesion (Fig. 44-48):
• Flap tears of the articular cartilage, usually in the anteroinferior quadrant
• A superficial, nondisplaced tear of the anteroinferior labrum
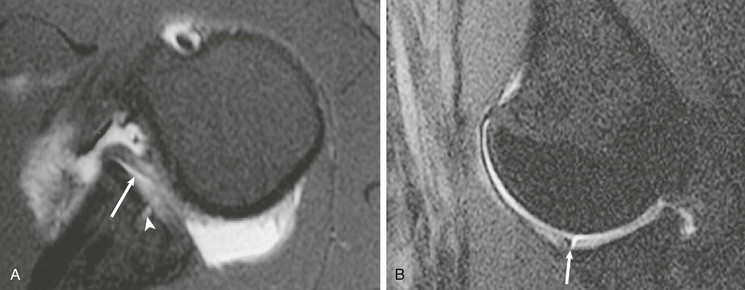
The anterior band of the inferior glenohumeral ligament and the medial scapular periosteum remain intact. These abnormalities noted on MRA could mimic findings seen in the chronic Bankart lesion with an adjacent chondral injury resulting from recurrent glenohumeral instability. However, the GLAD lesion can be differentiated from the Bankart lesion on the basis of the mechanism of injury, as well as by the absence of instability on physical examination.
HAGL Lesion
The Bankart lesion results from a tear or avulsion of the anterior labroligamentous complex at its insertion site on the osseous glenoid, whereas a lesser known entity is the humeral avulsion of the glenohumeral ligament (HAGL). Cadaveric studies have demonstrated failure of the anterior labroligamentous complex under tension at the glenoid attachment in 40%, in the midsubstance in 35%, and at the humeral attachment in 25% of the specimens.143 Although disruption of the anterior labroligamentous complex may occur at the glenoid attachment site, reports have also shown that the inferior glenohumeral ligament may fail in the midsubstance or at the humeral attachment site.174-176 In a single series, the HAGL lesion was found as an isolated abnormality in 35% of shoulders with recurrent anterior instability. It was suggested that many cases of recurrent shoulder instability that in the past were thought to result from capsular laxity may actually be the result of a missed HAGL lesion175 The HAGL lesion has been associated with anterior dislocation of the shoulder.177
Findings of the HAGL lesion on MRA include disruption of the anterior band of the inferior glenohumeral ligament either in its midsubstance or near its humeral attachment (Fig. 44-49). Extravasation of contrast material is seen through the defect in the ligament; associated disruption of the adjacent subscapularis may or may not be present. Identification of this lesion at MRA may be helpful to the arthroscopist because this lesion may be difficult to detect with use of the standard arthroscopic portals, and a miniarthrotomy may be required to identify the lesion and adequately repair it. Melvin et al.178 reported a small series of false-positive diagnoses of the HAGL lesion and recommend describing the lesion at imaging as injury to the inferior glenohumeral complex and leaving more specific characterization to arthroscopy. Bui-Mansfield et al.179 proposed use of a classification system for describing injuries to the inferior glenohumeral complex that illustrates the potential complexity of injury to the axillary pouch.
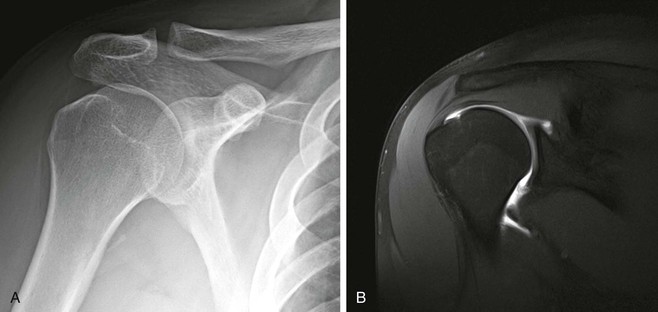
Posterosuperior Glenoid Impingement
Posterosuperior glenoid (or internal) impingement is a condition that occurs in athletes who participate in overhead activities, such as throwing. The injury occurs during the late cocking phase of throwing and is characterized by repeated impingement of the undersurface of the posterior aspect of the rotator cuff on the posterosuperior labrum and glenoid. It has been suggested that anterior instability is associated with internal impingement and may be contributory.180-183 This form of internal impingement may lead to undersurface tearing of the posterior aspect of the rotator cuff, as well as fraying and degeneration of the posterosuperior labrum. Associated injuries may include bony changes in the greater tuberosity of the humeral head as a result of recurrent impaction of the humeral head against the posterior glenoid. If anterior instability is also present, a lesion of the anterior labroligamentous complex may also be noted. Because the initial recommended treatment is conservative, accurate diagnosis with MRI may eliminate the need for diagnostic shoulder arthroscopy and the associated recuperation time. The constellation of MRI findings in a patient with posterosuperior glenoid impingement includes the following findings (Fig. 44-50):
• A partial-thickness articular-sided tear or fraying of the posterior aspect of the rotator cuff (infraspinatus tendon or the posterior aspect of the supraspinatus tendon)
• Degenerative fraying or a discrete tear of the posterior aspect of the superior labrum
• Subcortical cystic changes in the greater tuberosity of the humeral head
• Impingement of the posterior rotator cuff between the humeral head and the posterior glenoid seen on ABER imaging
• A possible tear, stretching, or laxity of the anteroinferior labroligamentous complex104
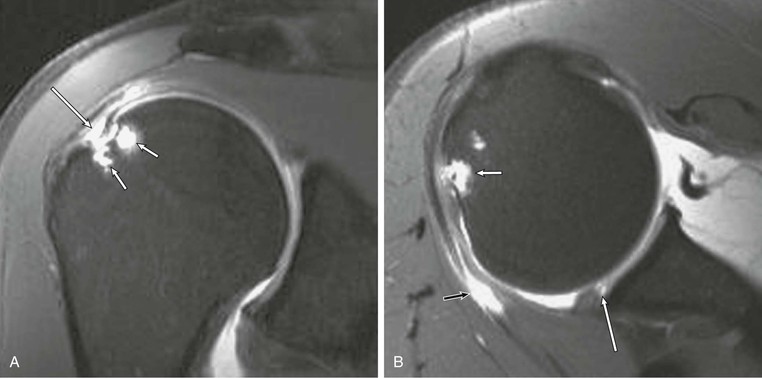
Glenohumeral Internal Rotation Deficit Disorder
For years it was believed that the primary pathophysiologic feature of internal impingement is microtrauma to the anterior capsule, resulting in anterior capsular laxity and allowing excessive external rotation of the humeral head. This mechanism leads to subtle posterior subluxation of the humeral head during maximal abduction and external rotation, which results in impingement of the posterior cuff. Burkhart and associates184 questioned the long-standing theory that microinstability is the universal cause of internal impingement in the disabled throwing athlete. These investigators proposed that, in many cases, the primary lesion in athletes whose sport involves throwing is posterior capsular contraction or scarring and posterior muscular tightness, leading to an acquired loss of internal rotation with secondary increased external rotation and tertiary anterior capsular stretching.184 This lesion has been referred to as glenohumeral internal rotation deficit disorder, indicating that the internal impingement results from posteroinferior capsular contracture that leads to the subtle posterior subluxation of the humeral head during maximal abduction and external rotation and thus to superior instability and SLAP lesions. The theory is important because appropriate treatment will differ depending on whether the primary lesion is anterior capsular stretching or posterior capsular contracture and scarring. MRI is supportive of the glenohumeral internal rotation deficit theory in many cases of internal impingement with posterior capsular thickening and scarring accompanying the previously described lesions of internal impingement (Fig. 44-51).

Labral Cysts
The glenoid labral cyst is the final lesion of the glenoid labrum to be discussed that is associated with glenohumeral instability. These cysts arise adjacent to the glenoid labrum as a result of either a tear or degeneration of the labrum and are analogous to cysts that arise adjacent to other joints, such as the meniscal cysts of the knee or labral cysts of the hip. They have a high association with labral tears and glenohumeral instability, and it has been hypothesized that fluid extrudes through a labral defect and collects in the adjacent soft tissues, thus forming a labral cyst.185 They commonly occur superiorly in association with SLAP lesions or posteriorly in association with posterior labral tears, but they have also been reported inferiorly in association with anteroinferior labral tears. Glenoid labral cysts have been implicated as the cause of compression neuropathies of both the suprascapular and axillary nerves.116,186
A glenoid labral cyst is depicted on MRI as a fluid-filled structure adjacent to the labrum (see Fig. 44-28). Glenoid labral cysts are variable in size, ranging from a few millimeters to several centimeters. They are frequently lobulated and may contain internal septations. They are bright on T2-weighted images and have an intermediate signal on T1-weighted images. They may communicate with the joint space or may be isolated from the joint space as a result of partial resynovialization of the adjacent labral tear. Thus after the intraarticular injection of a contrast agent during MRA, the cyst may continue to demonstrate fluid signal or may demonstrate a high signal on T1-weighted images as a result of the presence of contrast material. Because labral cysts have a high association with labral tears, identification of a cyst on MRI should prompt a thorough search for an associated labral tear.
A cyst that extends into the suprascapular or spinoglenoid notch may result in a compressive neuropathy of the suprascapular nerve; a cyst dissecting inferiorly into the quadrilateral space may produce a compressive neuropathy of the axillary nerve (Table 44-6).115-117,157,187,188 Compressive neuropathy initially results in diffuse edema and eventually leads to fatty replacement of the involved muscles in the chronic irreversible stages of the disease. On MRI, denervation edema appears as diffuse increased signal intensity within the affected muscle on T2-weighted images (see Fig. 44-29). The more chronic form of fatty atrophy demonstrates streaks of increased signal intensity within the involved muscle on T1-weighted images coupled with loss of the normal muscle bulk (see Fig. 44-23).
TABLE 44-6
COMPRESSIVE NEUROPATHIES CAUSED BY PARALABRAL CYSTS
| Location of Entrapment | Associated Labral Tear | Nerve Entrapped | Affected Muscles |
| Suprascapular notch | Superior | Suprascapular | Supraspinatus Infraspinatus |
| Spinoglenoid notch | Superior Posterior | Suprascapular | Infraspinatus |
| Quadrilateral space | Anteroinferior | Axillary | Teres minor Deltoid |

Articular Surfaces
The articular cartilage of the shoulder can be evaluated by CTA or MRI. CTA has high spatial resolution and can be reformatted in any plane (see Fig. 44-5). MRI using T2-weighted imaging with fat-suppression sequences with or without use of contrast material can also be used to evaluate the articular surface. In all cases, careful inspection of the cartilage is indicated as part of the imaging review. In the absence of trauma and bone marrow edema or subchondral cystic changes, cartilage injuries can be difficult to appreciate but remain clinically significant (Fig. 44-52).
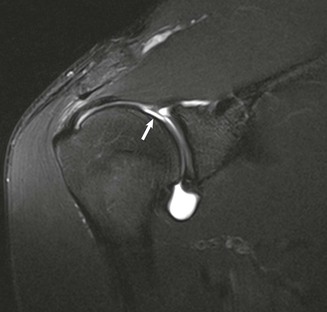
For a complete list of references, go to expertconsult.com.