Branch Retinal Vein Occlusion
Introduction:
Branch retinal vein occlusion (BRVO) is characterized by retinal hemorrhages in the territory of the obstructed vein. Macular edema, retinal ischemia and neovascularization can result, producing visual reduction.
Epidemiology:
BRVO usually occurs in patients in their fifth or sixth decades of life. The prevalence of BRVO in developed countries is estimated at just below 1%. There does not appear to be any racial or ethnic predilection. Systemic arterial hypertension is the most common systemic risk factor, present in about 75% of affected patients. The pathogenesis is believed to be disease of the adjacent arterial wall leading to venous compressesion at an arterovenous crossing point.
Clinical Features:
Patients may complain of visual blurring, distortion or metamorphopsia. On examination, intraretinal flame and blot shaped hemorrhages as seen in the territory of a dilated, tortuous retinal vein are present (Fig. 14.1.1). Given the distribution of retinal veins the accompanying pathology of BRVO almost never crosses the horizontal raphe. Cotton wool spots, retinal edema in the area drained by the occluded branch, collateral vessels and occasionally retinal neovascularization and vitreous hemorrhage may be seen. Vision loss is largely due to of retinal edema and may sometimes be secondary to retinal ischemia.

OCT Features:
OCT shows retinal thickening and edema limited to the retinal area drained by the obstructed vein (Figs 14.1.2 and 14.1.3). Macular thickness scans will show retinal thickening, usually confined to half the macula. Line scans through the macula show diffuse retinal edema and cystic (hyporeflective) spaces in the outer retina. Subretinal fluid may also be observed in severe cases. Hard exudates can be seen as small hyper-reflective intraretinal spots. Macular thickness scans are particularly valuable in monitoring edema over time and assessing the effects of treatment.
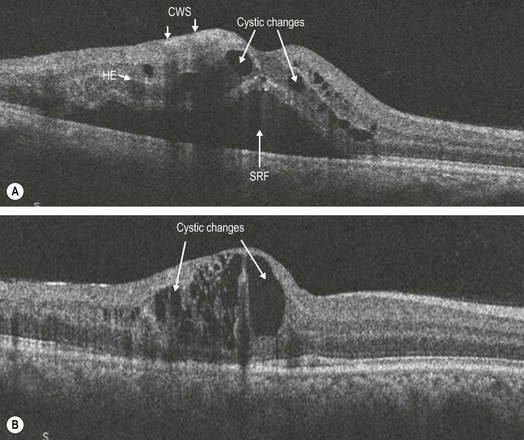
Figure 14.1.2 OCT scans through the macula of the patient (A) with diffuse retinal thickening and cystic changes (arrows). Note the cotton wool spots (CWS) (arrows) in the nerve fiber layer that cause shadowing of the layers beneath them. Some hard exudates (HE) are noted (arrow) as hyper-reflective clusters deeper within the retina and spanning several layers. SRF is also seen (arrow). (B) Note that only part of the retina is thickened unlike in CRVO.
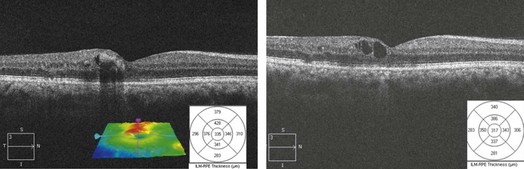
Figure 14.1.3 Successive OCT scans in the same patient after treatment with laser and anti-vascular endothelial growth factor therapy, with thinning of the retina seen on the line and macular thickness scans as well as a smaller geographic spread of the thickening seen on the retinal pigment membrane–internal limiting membrane overlay.
Ancillary Testing:
Fluorescein angiography is of value when the hemorrhages start clearing to assess perfusion. It may also be employed earlier to check for retinal neovascularization.
Treatment:
Primary treatment of macular edema in a BRVO is intravitreal anti-vascular endothelial growth factor injections. Both intravitreal corticosteroids and grid laser can also be employed, but are second-line therapies. Sector panretinal photocoagulation to reduce the risk of vitreous hemorrhage in the setting of retinal neovascularization is effective.