Internal Derangements of Joints
Upper and Lower Limbs
Robert S.D. Campbell, Andrew J. Dunn, Eugene McNally, Ahmed Daghir
Introduction
Magnetic resonance imaging (MRI) and ultrasound now allow the radiologist to undertake detailed examinations of the soft tissues of joints including tendons, ligaments, cartilage and fibrocartilagenous structures such as the menisci. Injuries that previously had to be inferred from patterns of bone injury shown on conventional radiographs can now be assessed in great detail allowing prognosis for conservative management and planning for surgical decision making. While common features exist in terms of the appearance of tendon and ligament abnormalities, the individual biomechanical properties of the different joints and the varying requirements of these joints strongly influence the patterns of injury seen. Broadly, soft-tissue joint injury falls into two patterns: acute injuries such as an acute ligament tear or osteochondral injury and chronic injury. Chronic injury generally occurs as a result of chronic and repetitive microtrauma to the structure concerned. Examples include tendinopathy and impingement syndromes. In this chapter we have used the term ‘tendinopathy’ (sometimes also known as tendinosis) to refer to chronic degenerative change in tendons. This was previously referred to as tendinitis, but this term has fallen out of use as it implies an inflammatory process which is not a feature of the chronic pattern of tendon injury being described.
The Shoulder
The shoulder is the most mobile joint in the human body. Movement occurs primarily through the gleno-humeral joint, but with a large contribution from the scapulothoracic articulation. The upper limb and scapula articulate with the trunk through the acromioclavicular and sternoclavicular joints. The wide range of movement that can occur at the shoulder is possible because of the shallow cup provided by the glenoid and relatively large humeral head. This configuration has been likened to a golf ball on a golf tee and is inherently unstable. Stability to the glenohumeral joint is provided through the soft tissues of the rotator cuff tendons and ligaments, which are susceptible to injury.
The glenoid fossa of the scapula articulates with the head of the humerus to form the glenohumeral joint (GHJ). The glenoid is shallow, pear shaped and anteverted in both the sagittal and axial planes. The fibrocartilaginous labrum runs circumferentially around the glenoid, increasing the overall surface area and contributing to the stability of the joint.
The GHJ is surrounded by a number of synovial-lined bursae that communicate with each other and provide lubrication for the motion of the rotator cuff tendons. The subscapularis bursa (SSB) lies anteriorly between the subscapularis tendon and the anterior deltoid muscle. The subacromial bursa (SAB) lies between the supraspinatus and infraspinatus tendons and the undersurface of the acromion, ACJ and lateral end of the clavicle. The subdeltoid bursa (SDB) is continuous with the lateral aspects of the SAB and SSB and continues posteriorly beneath the posterior belly of the deltoid muscle.
The rotator cuff muscles and tendons along with the long head of biceps are the dynamic stabilisers of the GHJ. The rotator cuff muscles arise from the scapula, passing laterally, to insert on the proximal humerus. They contribute to abduction as well as internal and external rotation of the humerus. The coracoacromial arch is formed by the coracoid, the acromion and the intervening coracoacromial ligament, under which the supraspinatus tendon (SST) passes. The rotator cuff comprises:
• Subscapularis: inserts on lesser tuberosity
• Supraspinatus: inserts anterior facet of greater tuberosity
• Infraspinatus: inserts middle facet of greater tuberosity
• Teres minor: inserts posterior facet of greater tuberosity.
The long head of biceps (LHB) tendon arises from the supraglenoid tubercle and superior labrum. The intra-articular component passes between the subscapularis and supraspinatus tendons in a region known as the rotator interval, and enters the bicipital groove on the anterior aspect of the humeral head. The LHB is stabilised within the rotator interval by the biceps pulley comprised of coracohumeral and superior glenohumeral ligaments.
The static stabilisers of the GHJ are the glenohumeral (G-H) ligaments which are condensations of the joint capsule. They comprise the superior, middle and inferior glenohumeral ligaments. The IGHL is the most important of the G-H ligaments. It is divided into anterior and posterior components, which act like a hammock to support the humeral head in abduction.
The commonest types of internal derangement of the shoulder relate to:
Rotator Cuff Disease
The commonest cause of rotator cuff tendon tears is external impingement occurring mostly in patients over the age of 40 years. Acute injuries are uncommon in the younger population, except in athletes. Impingement of the rotator cuff tendons occurs between the humeral head and coracoacromial arch during abduction of the upper arm. Initially there is reversible oedema and haemorrhage in the tendons, which may lead to tendinopathy and eventually failure of the tendon.1 The subacromial space may be reduced by bony abnormalities such as AC joint osteophytes and abnormalities of the shape of the acromion. Secondary impingement may occur through abnormal coordination of the rotator cuff muscles and abnormal scapulothoracic movement.
The impingement phenomenon is associated with the development of subacromial bursitis, and acromial bone spur formation. This further limits the subacromial space and aggravates the impingement process.1
Tendinopathy is defined as tendon injury on a cellular level that is most commonly age related and degenerative in nature but may also occur following trauma in younger individuals. The connective tissue that binds and organises the collagen bundles of the tendon undergoes microscopic tearing that leads to activation of inflammatory mediators and disorganised tendon healing. The tendon often thickens and may show features of delamination, mucoid degeneration and eventually partial tearing on imaging.2 Calcific tendinopathy is characterised by intrasubstance deposition of calcium hydroxyapatite crystals of unknown aetiology. The calcific deposits may be asymptomatic but can become painful when they produce focal tendon swelling that may contribute to external impingement. Release of calcium from the tendon into the overlying SAB can produce an acute inflammatory bursal reaction.
Rotator cuff tendon tears are defined as partial or full thickness. A partial thickness tear (PTT) involves either the articular surface (commonest) or the bursal surface (less common), but does not extend all the way through the tendon.2 A full thickness tear (FTT) extends from the articular surface to the bursal surface and creates an abnormal communication between the GHJ and SAB. The term full thickness only indicates that the tear extends through the full thickness of the tendon; it does not imply the tear extends from the anterior edge of the tendon to the posterior edge. However, as the tear size increases, the whole tendon may become torn (anterior to posterior) creating a massive tear with medial tendon retraction. The supraspinatus is most commonly affected, but tears may progress to involve both infraspinatus and subscapularis.
Tears of the LHB pulley and subscapularis tendon may lead to medial subluxation of the LHB tendon from the bicipital groove. The LHB may also show features on tendinopathy or may eventually rupture.
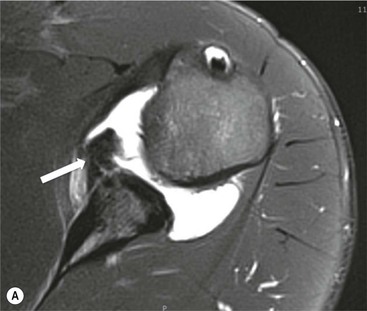
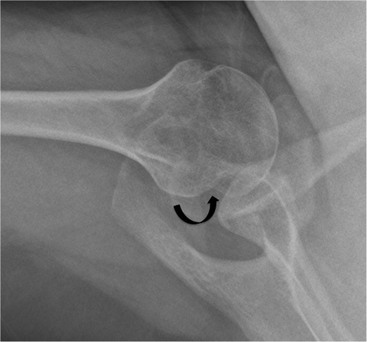
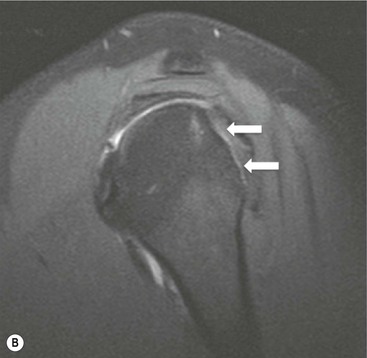
Radiography is useful for demonstrating bony abnormalities of the AC joint and acromion and excluding associated GHJ arthrosis (Fig. 46-1). Marked narrowing of the subacromial space is a specific but insensitive sign of a full thickness rotator cuff tear3 (Fig. 46-2). MRI and ultrasound (US) directly visualise the rotator cuff tendons. Both techniques are capable of diagnosing tendinopathy (Fig. 46-3), and have nearly 100% accuracy rates for FTTs of the rotator cuff.4 MR arthrography is not usually indicated for primary rotator cuff disease. The most important features to describe that help determine management include the following:
• presence of associated rotator cuff muscle atrophy
• dislocation or rupture of the LHB tendon



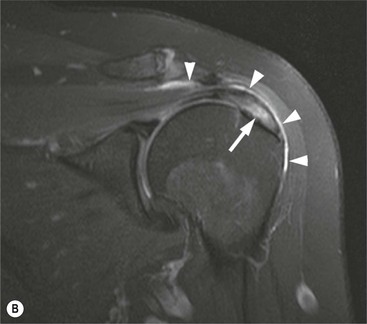
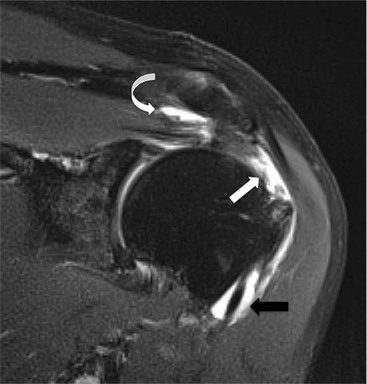
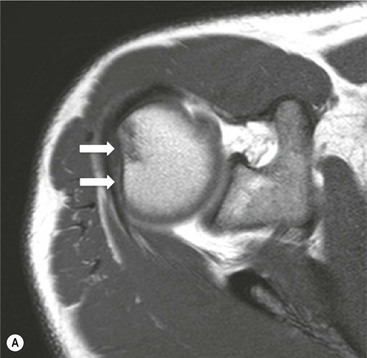
The primary sign of a rotator cuff FTT is a focal deficiency of the tendon (Figs. 46-4 and 46-5). This nearly always occurs at the tendon insertion on the tuberosity. The margins of the tear are best delineated when there is fluid within the tendon defect. Secondary signs of an FTT include the presence of fluid in both the GHJ and SAB, and flattening or concavity of the subacromial fat plane.
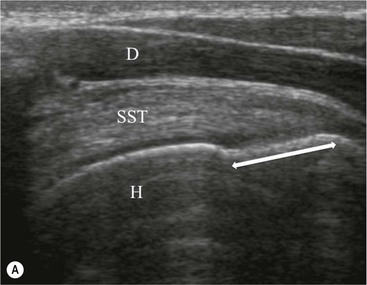
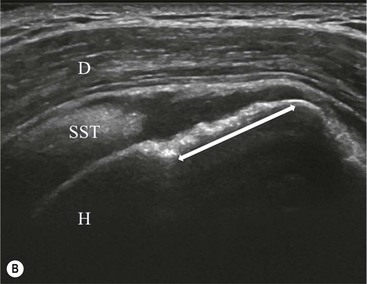
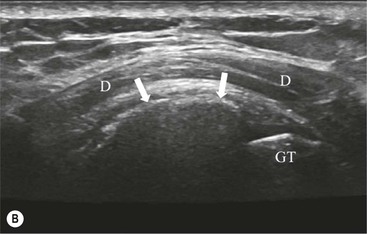
PTTs are less reliably demonstrated by both MRI and US, and it may be difficult to differentiate tendinopathy from partial tears. Focal clefts, tears, or tendon thinning affecting the articular margin of the footprint of the tuberosity are most common (Figs. 46-6 and 46-7). Tendon thickening is not always present. It is important not to mistake magic angle phenomenon on short TE MR sequences or anisotropy on US as evidence of tendinopathy.2

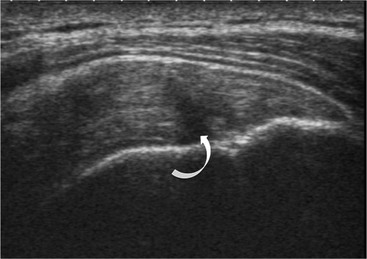
Calcific tendinopathy can be visualised on radiographs as discrete amorphous deposits of calcium density. On US they are echogenic and may or may not cast acoustic shadowing (Fig. 46-8). Small deposits of calcium may be difficult to detect on MRI as both the calcification and surrounding tendon are of low SI.

GHJ Instability
The GHJ is an inherently unstable joint. Injury or abnormality of the static stabilisers renders the joint susceptible to recurrent dislocation, and further injury. Chronic GHJ instability may lead to secondary arthrosis if untreated. Imaging is used to document the extent of internal derangement in order to determine the therapeutic options.5
Instability of the GHJ may be dependent on three factors, referred to as the Bayley triangle:
A combination of these factors may be present in any one patient, but trauma is the commonest cause of instability. Anteroinferior dislocation is the commonest presentation. Posterior dislocation is frequently encountered following epileptic seizures. Inferior dislocation is rare.
Radiographs are the primary imaging technique to confirm GHJ dislocation and establish joint congruity following reduction. Anteroposterior and axial views or a modified caudal angled axial are most appropriate. MRI, MR arthrography or CT arthrography are used in the non-acute setting to assess the static stabilisers.6
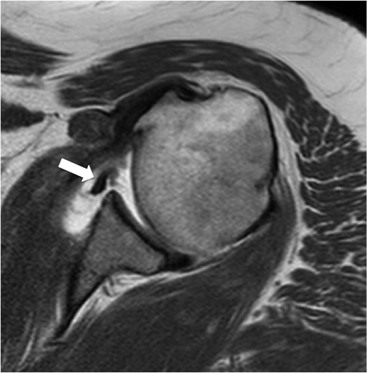
Anterior GHJ dislocation causes tearing and detachment of the anteroinferior glenoid labrum, known as a Bankart lesion. The location of the labral tear is described according to clockface terminology: 12 o'clock represents the biceps anchor, and 3 o'clock is anterior at the equator of the glenoid. Fluid signal intensity or contrast medium extending between the glenoid and labrum is the primary sign of a labral tear (Fig. 46-9). The labrum may become displaced, and it is important to assess the position of the labrum with respect to the face of the glenoid.
More severe injury may be associated with a bony injury of the glenoid rim, usually called a bony Bankart lesion (Fig. 46-10). Non-enhanced CT may occasionally be preferred to assess the size of the bony defect of the glenoid. There is usually associated impaction injury on the posterosuperior aspect of the humeral head called a Hill–Sachs defect (Figs. 46-11 and 46-12).
In posterior dislocation the location of labral and humeral injury is opposite to anterior dislocation, and are termed reverse Bankart lesions and reverse Hill–Sachs defects.
Injury to the joint capsule and glenohumeral ligaments is common. The anterior band of IGHL is the most important joint stabiliser. It may be torn at the humeral insertion or less commonly from its origin on the glenoid. Imaging with the arm in abduction and external rotation (ABER imaging) is sometimes used to assess the integrity of the ligament, to identify the degree of labral displacement and loss of joint congruity.5
The most important features to describe that help determine management include:
Superior Labral Tears
Tears of the superior labrum and biceps anchor are commonly encountered injuries in overhead throwing athletes. Abnormal traction on the biceps anchor and superior labrum results in tears that usually extend posteriorly. They are often referred to as superior labral tears anterior to posterior (SLAP tears).7 MRI, MR arthrography or CT arthrography may assess the glenoid labrum.
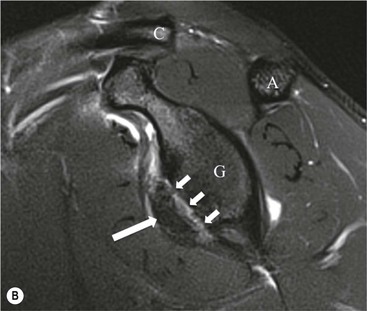
Contrast medium or fluid signal intensity extending into the substance of the labrum or through the chondro-labral junction is the primary sign of a SLAP tear (Fig. 46-13). Tears may be localised to the posterosuperior labrum, or may be more extensive. There may be tear extension into the LHB tendon. There are many grades of SLAP tears described but the extent of the tear and the structures involved are the most important features.8
The most important features to describe that help determine management include:
The Acromioclavicular Joint
The AC joint is a synovial plane joint. All the forces of glenohumeral and scapulothoracic movements are transmitted to the trunk through the ACJ and sternoclavicular joint. Osteoathritis (OA) of the ACJ is common and the associated capsular thickening and osteophyte formation is a contributor to external impingement of the shoulder.
The ACJ has strong capsular ligaments, and is also stabilised by the coracoclavicular (C-C) ligaments. Traumatic disruption and dislocation of the joint is described by the Rockwood classification:
Grade I: undisplaced injury with sprain of acromio-clavicular ligaments.
Grade II: ACJ widening with <50% superior displacement of lateral clavicle.
Grade III and IV injuries are associated with disruption of the C-C ligaments and above are treated surgically. Grade I and II injuries usually resolve spontaneously. However, some patients may present with persistent pain and instability. Ligament reconstruction may be required in the athletic population.9 Weight-bearing radiographs may demonstrate abnormal joint widening, and the C-C ligaments can be visualised directly by MRI (Fig. 46-14).
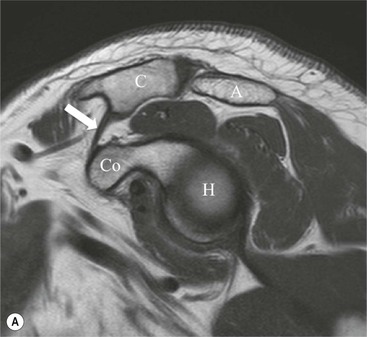
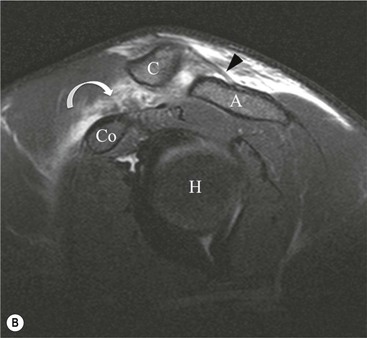
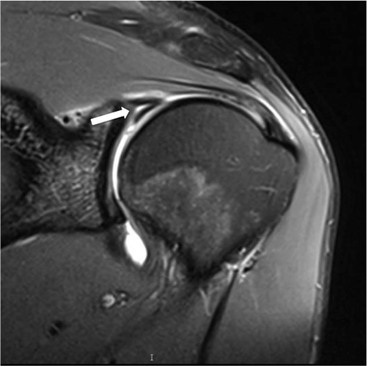
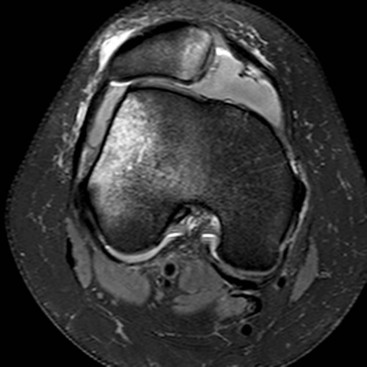
Post-traumatic osteolysis of the lateral clavicle occurs in approximately 6% of ACJ disruptions and may also be seen with repetitive ACJ microtrauma such as weight-lifting (Fig. 46-15).

The Sternoclavicular Joint
The sternoclavicular joint (SCJ) is a synovial saddle joint, with a cartilaginous articular disc. It has limited movement, but like the AC joint transmits the forces of shoulder movement to the trunk. It is very prone to osteoarthritis, which may be associated with chronic anterior subluxation. Radiographic evaluation of the SC joints may be difficult but CT or MRI readily demonstrate the features of arthrosis.10
Traumatic subluxation and dislocation usually occurs anteriorly. Posterior dislocation is a rare but important injury, as the displaced medial clavicle may be associated with vascular injury in the superior mediastinum.11
The Elbow
The elbow is a complex synovial hinge joint. It comprises the ulnotrochlear and radiocapitellar articulations which allow flexion and extension of the elbow. The proximal radioulnar joint (in conjuction with the distal radioulnar joint) enables pronation and supination of the forearm by rotation of the radius around the ulna.12
The primary flexors are biceps brachii, brachialis and brachoradialis. Triceps is the main extensor. Supination of the forearm occurs through the action of biceps and supinator. Pronation is by pronator teres, and pronator quadratus (at the wrist). The common tendon for wrist and hand extension arises from the lateral humeral epicondyle, and the common flexor tendon from the medial epicondyle.
The joint is stabilised by the ulnar collateral and radial collateral ligaments. The radial collateral complex includes the annular ligament which supports the radial head.
Tendons
Insertional tendinopathy around the elbow joint most commonly affects:
The triceps and other tendons are rarely involved.
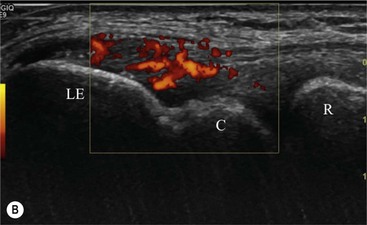
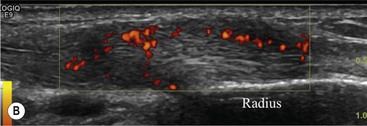
Tendinopathy of the common extensor and flexor tendons presents with localised pain over the distal humeral epicondyles. It is often a clinical diagnosis, although imaging may be performed in refractory cases to confirm the diagnosis and exclude a tear. Ultrasound is frequently used to guide injection therapy.
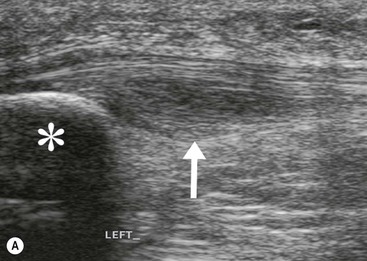
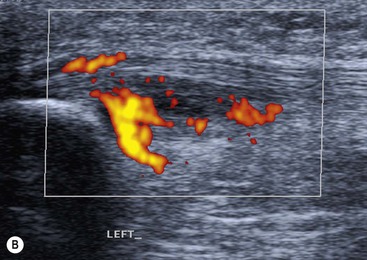
The affected tendon is thickened and hyporeflective on US, with neovascularisation on Doppler imaging (Fig. 46-16). High SI is demonstrated on fluid-sensitive MRI sequences (Fig. 46-17). Tendon tears are demonstrated as focal areas of deficiency.13 In chronic cases, new bone formation may be seen on radiographs at the tendon enthesis. Calcific tendinopathy is much less common than in the rotator cuff of the shoulder.
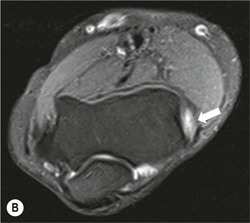

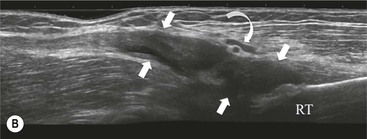
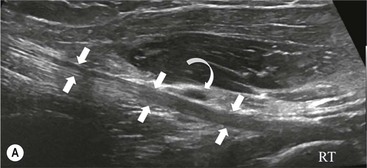
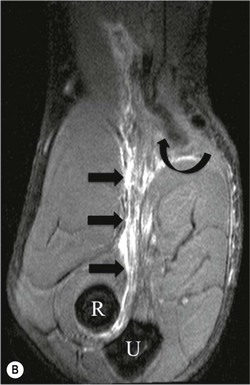
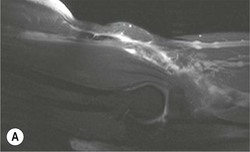
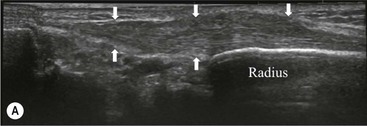
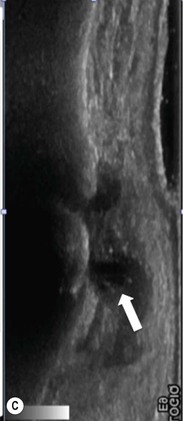
The distal biceps tendon inserts on the tuberosity of the proximal radius. It does not have a tendon sheath, but surrounding connective tissue is known as a paratenon. It is surrounded near the insertion by the bicipitoradial bursa. Distal biceps tears are often clinically unrecognised, but may be amenable to surgery if diagnosed early. In the early stages the tendon is thickened and there may be an effusion in the bicipitoradial bursa (Fig. 46-18). In complete rupture the tendon retracts proximally. MRI and US may be used to confirm the diagnosis and locate the tendon end (Figs. 46-19 and 46-20).

Bone and Cartilage
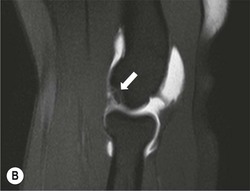
The capitellum is the third most commonly affected site in osteochondritis dissecans (after the knee and ankle). It commonly affects teenagers and young adults. A focal osteochondral fragment or defect may be visualised on radiographs. Cross-sectional imaging with MRI, MR arthrography or CT arthrography is used to detect radiographically occult lesions and for grading osteochondral lesions (Fig. 46-21). The osteochondral fragment may remain in situ or lie remotely within the elbow joint. Fluid SI at the base of the osteochondral lesion on MRI, or contrast medium tracking around the fragment on arthrographic images, is a sign of an unstable lesion. Integrity of the overlying articular cartilage is a good sign of stability.

Reports should include:
• size and location of osteochondral defect;
• stability of the lesion and integrity of overlying cartilage; and
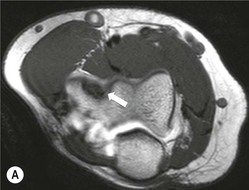
Intra-articular bodies are also frequently encountered in OA of the elbow. They may be calcified, but non-calcified chondral bodies may also occur. CT is often utilised to assess the size and location of osteophytes before surgery, as well as identify small loose bodies. Chondral bodies are not visualised on radiographs or conventional CT. In some cases pre- and post-angiography CT may be performed (Fig. 46-22). Conventional MRI is less sensitive for detection of small intra-articular bodies.


Ligaments
The collateral ligaments of the elbow may be torn as the result of an elbow dislocation, and may require surgical repair. A coronoid process fracture is a sign of an unrecognised elbow dislocation. Chronic tears of the ulnar collateral ligament are infrequently encountered in some throwing sports and in weightlifters.
In acute injuries MRI shows the presence of soft-tissue oedema and haemorrhage around the affected ligament. MR arthrography may be preferred for diagnosis of chronic tears. Acute ulnar collateral ligament (UCL) tears often occur at the proximal origin on the medial humeral epicondyle (Fig. 46-23). In chronic tears the defect is usually at the insertion on the sublime tubercle of the ulna.14

Hand and Wrist
The wrist is a synovial joint, formed from the articulations between the radius and ulna, the eight carpal bones and the metacarpal bones. The distal radioulnar joint allows supination and pronation of the forearm.
The mechanics of the wrist are complex, but movement occurs primarily through the proximal carpal row, comprising the scaphoid, lunate and triquetrum. This acts as a bridge between the forearm bones and the distal carpal row, which is relatively rigid. The proximal carpal row is referred to as the intercalated segment, and the lunate acts as the keystone. Stability between the segments of the proximal row is maintained by the intrinsic scapholunate and lunotriquetral ligaments. Stability between the radius and ulna, the proximal and distal carpal rows is maintained by multiple dorsal and volar extrinsic ligaments. Carpal alignment is assessed on PA radiographs, by identifying continuity of the articular surfaces of the carpal bones (known as the arcs of Gilula).
The first carpometacarpal joint between the trapezium and first metacarpal is more mobile than the other CMC joints to allow for the greater range of movements of the thumb. It has a separate synovial compartment.
The distal radioulnar joint and ulnocarpal joint are stabilised by the triangular fibrocartilage (TFC) complex. The TFC is a cartilaginous disc that arises from the ulnar border of the distal radius and attaches to the fovea of the ulnar styloid. Its margins blend with the dorsal and volar radioulnar ligaments, and the extensor carpi ulnaris (ECU) tendon sheath.
The flexor tendons of the fingers and thumb pass through the carpal tunnel, which is maintained superficially by the flexor retinaculum, which extends from the hook of hamate and pisiform to the scaphoid and trapezium. The median nerve passes through the carpal tunnel to enter the palm. The extensor tendons are stabilised by the extensor retinaculum on the dorsal aspect of the wrist at the level of the first carpal row.
Bone
Fractures around the wrist are common. Waist of scaphoid fractures may be associated with avascular necrosis of the proximal pole. The more proximal the fracture site, the higher the incidence of fracture non-union.
Radiological signs of avascular necrosis (AVN) include sclerosis of the proximal pole, which may progress to articular collapse and bone fragmentation. CT is used to assess the state of fracture union (Fig. 46-24). Signs of AVN on MRI include low SI sclerosis on T1-weighted (T1W) images and short T1 inversion recovery (STIR) images. Marrow oedema on STIR images is an indicator of persistent vascular perfusion in the proximal segment. The absence of enhancement with gadolinium contrast medium on fat-saturated T1W images in areas of sclerosis is a reliable indicator of lack of vascularity15 (Fig. 46-25).







Spontaneous AVN of the lunate is known as Keinböck's disease. The radiographic and MRI features are the same as AVN of the scaphoid (Fig. 46-26). It may be associated with negative ulnar variance (short ulna). Advanced bony collapse in both proximal scaphoid fractures and AVN of the lunate results in late-stage secondary osteroarthritis.


Wrist Ligaments
Tears of the ligaments of the wrist can result in carpal instability. Disruption of the intrinsic ligaments results in intercalated segment instability. This is also termed dissociative carpal instability because there is dissociation between the segments of the proximal carpal row.
The scapholunate ligament is most frequently involved. Radiographs may show scapholunate diastasis (>3 mm). The lunate demonstrates dorsal rotation on lateral views and volar rotation of the scaphoid. This results in an increase in the scapholunate angle (>60°) known as dorsal intercalated segment instability (DISI) (Fig. 46-27). A DISI deformity of the carpus may also be associated with fractures of the scaphoid.


Disruption of the lunotriquetral ligament is less common. In this situation there is volar rotation of the lunate on lateral radiographs, with reduction of the scapholunate angle (<30°). On PA radiographs there may be an obvious step between the distal articular surface of the lunate and triquetrum. This is termed volar intercalated segment instability (VISI).
More subtle degrees of instability may be demonstrated by an instability series of radiographs acquired with radial and ulnar deviation and with a clenched fist view. Video fluoroscopy is also useful for assessing dynamic wrist instability.
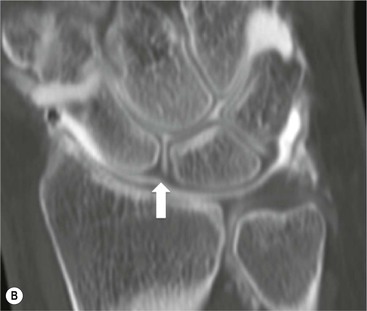
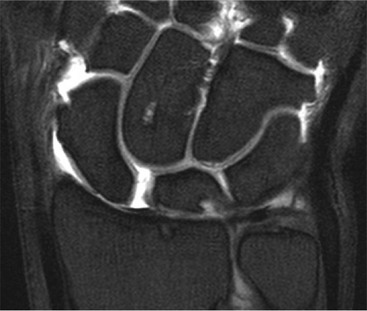
Abnormal communication between the radiocarpal and midcarpal joints may be seen on arthrography (Fig. 46-28), which is usually combined with MRI or CT16 (Figs. 46-29 and 46-30). However, direct visualisation of the ligaments is possible with conventional MRI. The most important features to describe that help determine management include the following:
Injuries to the extrinsic ligaments result in a variety of complex radiocarpal and midcarpal non-dissociative instabilities.

Lunate and perilunate dislocations are important injuries. In lunate dislocation, the lunate dislocates in a volar direction with loss of the articulation of the radius and other carpal bones. In perilunate dislocation, the lunate retains the articulation with the radius and the remainder of the carpus dislocates in a dorsal or volar direction. PA radiographs show an abnormal triangular appearance of the lunate. Differentiation of lunate versus perilunate dislocation is best made on a lateral radiograph. Both injuries may be associated with scaphoid (or other carpal) fractures, which indicates a greater degree of wrist instability.
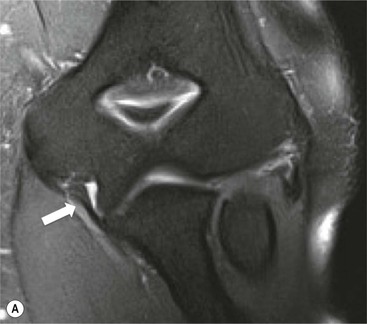
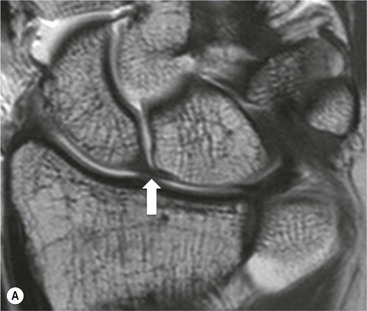
Triangular Fibrocartilage
The TFC is composed of fibrocartilage and is normally low SI on all MRI pulse sequences (Fig. 46-31). Tears of the TFC complex may present as ulnar-sided wrist pain. They occur as either a degenerative phenomenon or as an acute injury. Degenerative tears frequently result in central perforation of the TFC (Fig. 46-32), and are associated with positive ulnar variance (long ulna). This in turn may lead to ulnar abutment on the triquetrum, which is another cause of ulnar-sided wrist pain.


Traumatic TFC tears often affect the ulnar attachments and are associated with ulnar styloid fractures (Fig. 46-33). These injuries may also involve the dorsal and volar radioulnar ligaments and can lead to DRUJ instability.

Wrist Tendons
The tendons of the wrist are divided into extensor and flexor tendons. The extensor tendons form six groups with separate synovial sheaths, numbered from a radial to ulnar direction at the level of the radiocarpal joint.
Extensor tendinopathy is commonly seen in the extensor carpi ulnaris (ECU) tendon as it passes over the ulnar styloid. This is a common site for tenosynovitis in the setting of inflammatory arthropathy that may produce erosion of the ulnar styloid. Another commonly encountered extensor tendinopathy affects the extensor group I tendons of abductor pollicis longus and extensor pollicis brevis.17 This is frequently associated with a stenosing tendosynovitis known as De Quervain's tenosynovitis (Fig. 46-34).
The flexor tendons are grouped within the carpal tunnel, with the exception of the flexor carpi ulnaris and radialis tendons. Isolated flexor tendinopathy is uncommon, though generalised flexor tenosynovitis may occur with rheumatoid arthritis. This increases the pressure within the carpal tunnel and may cause a secondary carpal tunnel syndrome by compression of the median nerve.
Median Nerve
Carpal tunnel syndrome is a neuropathy of the median nerve. It is usually idiopathic, or associated with pregnancy. Direct nerve compression may occur within the carpal tunnel in patients with synovitis of the wrist or flexor tendons. Lesions with mass effect arising from the tendon sheath or peripheral nerve sheath tumours are occasionally encountered.
Diagnosis is often made by a combination of clinical findings and nerve conduction studies. US or MRI may be required in cases with atypical features. Imaging is used to visualise abnormalities of the nerve, and to exclude secondary causes of carpal tunnel syndrome. The changes in the nerve are variable and include flattening of the nerve within the carpal tunnel, and proximal thickening. A cross-sectional area of > 10 mm2 is suggestive of carpal tunnel syndrome. Qualitative changes within the nerve such as loss of normal fascicular pattern on US or increased SI on MRI are unreliable signs in isolation.18
UCL of Thumb
Tears of the ulnar collateral ligament of the thumb are common. They are often referred to as gamekeeper's thumb or skier's thumb. Undisplaced ligament tears can be treated conservatively, but displaced tears will not heal and require surgical repair.
In a displaced tear the ligament is torn from the distal insertion and retracts proximally around the aponeurosis of the adductor pollicis. This is known as a Stener lesion.19 The displaced ligament can be demonstrated on both MRI and US (Fig. 46-35).


The Hip
The hip is a large ball-and-socket joint which allows a wide range of movement while maintaining strong stability such that dislocation is much less frequent than in the shoulder. The cup-shaped acetabulum is formed at the junction of the ilial, ischial and pubic bones. The depth of the acetabulum is increased by the fibrocartilaginous labrum. Stability is further increased by the iliofemoral, ischiofemoral and pubofemoral ligaments which reinforce the joint capsule. The acetabulum and femoral head are lined by hyaline cartilage. The ligamentum teres is a weak ligament attaching to the fovea of the femoral head. It transmits the foveal artery, though in adults most of the blood supply of the femoral head is provided by the circumflex femoral arteries.
Labrum and Cartilage
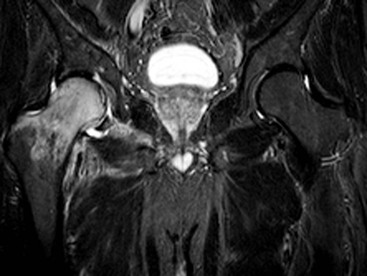
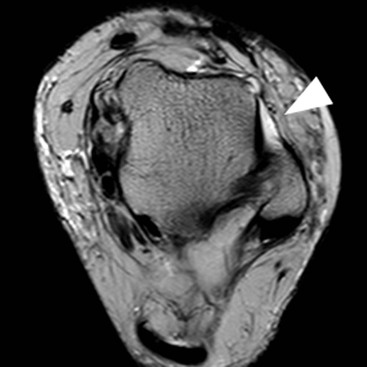
The fibrocartilaginous labrum forms a ring at the margin of the acetabulum, increasing the stability of the joint by deepening the acetabular fossa. Lesions of the acetabular labrum constitute one of the most common internal derangements of the hip. Tears of the labrum may be traumatic or degenerative and are a cause of pain and mechanical symptoms. The gold standard imaging technique is MRI following injection of gadolinium contrast medium into the joint (MR arthrography). However, with modern high field strength systems some centres make use of conventional MRI without arthrographic contrast medium. The torn labrum may appear small, irregular, absent or may demonstrate linear penetration of contrast agent into the tear (Fig. 46-36). The anterosuperior and superior portions of the labrum are most frequently affected. Fluid tracking through the tear may form a paralabral cyst which is a useful indication of an underlying labral tear. Occasionally intra-articular contrast material can be seen communicating with the cyst on MR arthrographic images. Labral tears are often associated with adjacent articular cartilage damage and it is proposed that a labral tear is a precursor to the development of osteoarthritis. However, it is also important to recognise that labral degenerative tears are seen in association with osteoarthritis and the precise relationship between the two entities is as yet unclear.

Traumatic tears may arise from impingement between the femoral head and neck and the acetabular rim. This condition is known as femoroacetabular impingement.
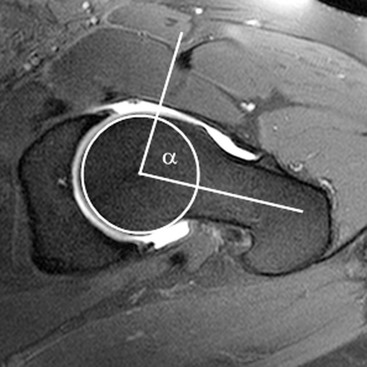
Two kinds of femoroacetabular impingement are described, cam type and pincer type, though these often coexist.20 Cam impingement is caused by the presence of an abnormal osseous ‘bump’ found on the anterior or lateral aspect of the femoral head–neck junction (Fig. 46-36). This produces abnormal contact between femur and acetabular rim in certain positions and typically presents in young athletic men. The α angle can be used to identify this loss of sphericity on a cross-table lateral radiograph or axial oblique MRI (Fig. 46-37). An α angle measuring greater than 50° may be taken as abnormal.21 Repeated contact between the osseous bump and the anterior acetabulum during hip flexion results in a labral tear and/or cartilage damage. CT is an excellent technique for demonstrating the bone morphology in this condition, although MR arthrography is able to show the cartilage and labral damage. Acetabular cartilage delamination (separation of the cartilage from the underlying bone), sometimes termed a ‘carpet lesion’, is common in cam-type impingement and may be detected on MR arthrography.22 The information provided by arthrographic MRI is important, as joint-sparing treatment (such as cam re-contouring) is unlikely to give effective symptom relief if there is established severe cartilage damage.
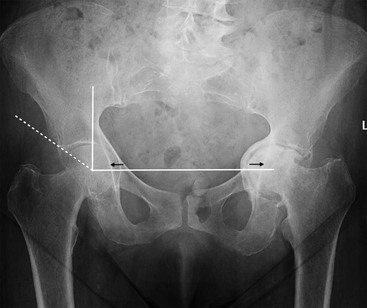
Pincer-type impingement, more common in middle-aged women, results from overcoverage of the femoral head by the acetabulum. This can be due to a deep acetabulum, bone hypertrophy at the acetabular rim or abnormal acetabular retroversion, the latter leading to an effective overcoverage of the femoral head anteriorly. On hip flexion the abnormal morphology results in impingement between the acetabular rim and the femoral neck, leading to labral and cartilage damage. The centre-edge angle is a method to identify acetabular overcoverage on an AP radiograph of the pelvis (Fig. 46-38). A centre-edge angle greater than 40° may be considered abnormal.23 Coxa profunda and protusio acetabuli are two types of deformity that predispose to pincer-type impingement. Coxa profunda is identified on an AP radiograph when the floor of the acetabular fossa overlaps the ilioischial line. Protrusio acetabuli, more severe, is present when the femoral head itself overlaps the ilioischial line (Fig. 46-38).
Muscle and Tendon
Muscle and tendon injury around the hip is common. This may result from acute trauma such as may be sustained in sporting activities or, particularly in the case of tendon injury, from chronic repetitive microtrauma. The hamstring and adductor origins are commonly affected in young athletes while gluteus medius tendon degeneration (tendinopathy) and tears are more common in the elderly. On MRI and ultrasound, the appearances vary depending on the severity of the injury. In the case of muscle injury, findings may range from minor muscle oedema to discontinuity of fibres and muscle retraction. In chronic cases there may be fatty atrophy or muscle ossification. Tendon disease in the form of tears or tendinopathic change may also be demonstrated; the latter is seen as loss of the normal tendon low signal on T1- and T2-weighted MR images along with thickening of the tendon. Ultrasound will also show tendon discontinuities and tendinopathy.
Avulsion of an unfused apophysis at a muscle attachment may occur in children undertaking athletic activities. The anterior superior iliac spine (sartorius muscle), the anterior inferior iliac spine (rectus femoris) and ischial tuberosity (hamstring) are common sites of involvement (Fig. 46-39). Because avulsed apophyses continue to form bone, this can lead to bizarre mass-like appearances on imaging when presentation is delayed. The location of the bone ‘mass’ and the age of the patient are key to making the correct diagnosis.

While mechanical snaps and clicks can arise from within the joint, for instance in the presence of a labral tear or loose body, such mechanical symptoms may also arise from extra-articular causes. The snapping hip describes a snap or clunk felt by the patient when undertaking a particular movement. It may be associated with pain and the snap may be audible. Two of the most common extra-articular varieties are the snapping iliotibial band (external type) and the snapping iliopsoas tendon (internal type). Both can be imaged using ultrasound, which allows continuous visualisation of the relevant structures while the patient reproduces the snapping. In the external type the gluteus maximus muscle can be shown initially lying over the greater trochanter before abruptly moving posteriorly to bring the iliotibial band into contact with the greater trochanter.24 In the internal type the iliopsoas tendon rotates abnormally before abruptly reversing and forcefully striking the superior pubic ramus.25
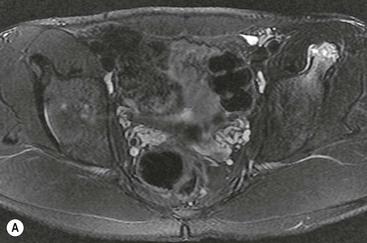
Ischiofemoral impingement is a recently described condition predominantly affecting women associated with narrowing of the space between the ischial tuberosity and lesser trochanter of the femur. It is thought that the quadratus femoris muscle which passes through this space may be impinged during repetitive hip movement, giving rise to pain. MRI reveals narrowing of the space associated with oedema of the quadratus femoris muscle belly and adjacent free fluid (Fig. 46-40).26 However, similar appearances may be found in asymptomatic individuals and the clinical significance of this has not yet been established.

Bone
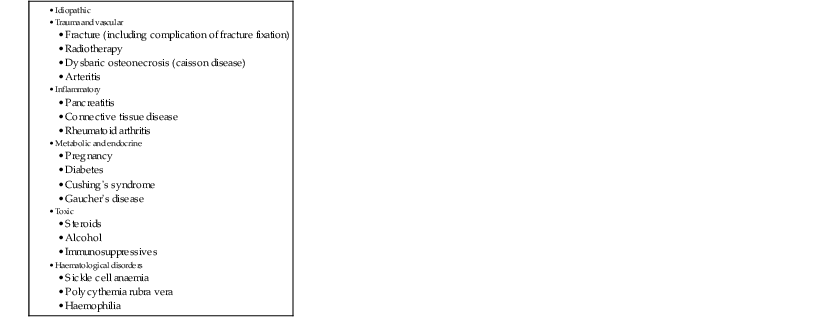
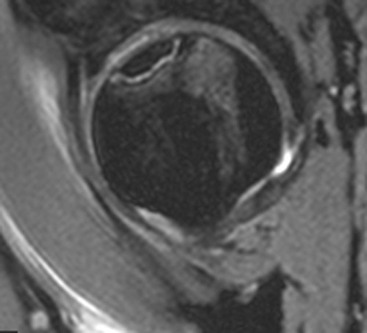
Avascular necrosis of the femoral head has many potential underlying causes (Table 46-1). MRI is the preferred technique, allowing early detection of signal change in the subchondral region of the femoral head. The ‘double line’ sign on fluid-sensitive sequences, characteristic of AVN, describes a low signal sclerotic line next to a high signal hypervascular line which demarcates the extent of the lesion (Fig. 46-41). There may be accompanying bone marrow oedema in the femoral head and neck. The extent of involvement on MRI has prognostic value in determining the outcome after decompressive surgery.27 Conventional radiographs are much less sensitive in the early stages of AVN, but as the process progresses they will typically show a linear subchondral lucency that progresses to articular collapse and sclerosis. Both hips should be imaged together, as bilateral involvement is common.
TABLE 46-1
Potential Causes of Hip AVN
Transient osteoporosis of the hip (TOP), also known as bone marrow oedema syndrome, is a self-limiting painful condition of uncertain aetiology.28 On MRI this appears as extensive bone marrow oedema signal involving the femoral head and/or neck (Fig. 46-42). Conventional radiographs may show reduced bone density but MRI is the most important tool in diagnosis. Following resolution in the hip, the condition may go on to involve other parts of the skeleton, in which case the condition is called regional migratory osteoporosis. Bone marrow high signal (oedema) seen in the femoral head and/or neck raises several possible diagnoses, including transient osteoporosis, that should also be considered (Table 46-2).

Bursae
Bursae are synovial-lined structures found in many sites around the musculoskeletal system, and it is their normal function to facilitate the movement between muscles and adjacent structures. Bursal inflammation, or bursitis, may result from overuse injury or from involvement by systemic inflammatory conditions such as inflammatory arthritis. On imaging, a normal bursa will often be unseen, or appear as a thin layer of fluid between tissues. When inflamed (bursitis), imaging will show the bursa as a more substantial fluid-containing structure. There may be thickening of the bursal walls and adjacent soft-tissue oedema. Several bursae are recognised around the hip, but the most common to be associated with symptoms are the iliopsoas and the greater trochanteric bursae. The trochanteric bursae are a group of bursae found deep to the gluteus maximus, gluteus medius and gluteus minimus muscles.29 ‘Trochanteric bursitis’ is a relatively common condition which may involve one or more of the bursae and typically occurs in middle-aged women. Trochanteric bursitis presents with lateral hip pain and may be associated with tendinopathy of gluteus medius (Fig. 46-43). The iliopsoas bursa is the largest bursa in the body and communicates with the hip joint in approximately 15% of individuals. It lies deep to the iliopsoas muscle and passes directly over the anterior hip joint capsule. Iliopsoas bursitis typically presents with anterior hip pain related to movement or with an anterior groin mass if large.

The Knee
The knee is the largest joint in the body and comprises three compartments, the medial and lateral femorotibial compartments and the patellofemoral compartment. The femoral condyles articulate with the tibial condyles, and the patella articulates with the femoral trochlea. The joint capsule encloses the articular surfaces, menisci and cruciate ligaments. The collateral ligaments and tendons are extra-articular, apart from the popliteus tendon, which has an intra-articular portion. The bony articular surfaces alone are inherently unstable, so these soft-tissue supporting structures are vital to the joint stability and are prone to injury. MRI remains the imaging technique of choice for evaluating most internal knee derangements. It is well suited for demonstrating the menisci, tendons and ligaments. However, ultrasound can be used to demonstrate the peripheral joint structures, showing the medial and lateral collateral ligaments and soft tissues of the extensor mechanism well.
Menisci
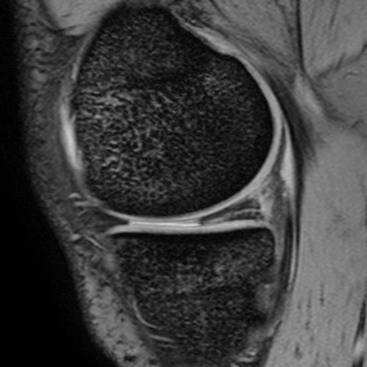
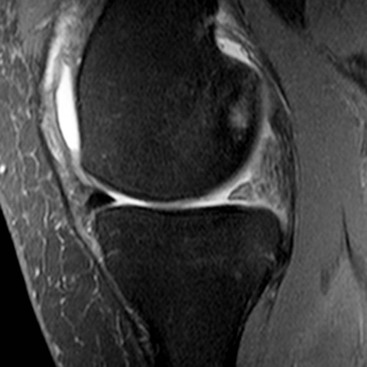
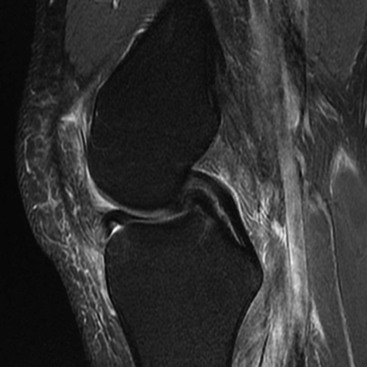
The menisci are two semilunar fibrocartilaginous structures located between the articular cartilage of the femoral and tibial condyles. They each have a crescent shape with an anterior and posterior horn and a body. The tips of the horns are attached to the tibial plateau adjacent to the intercondylar eminence. These attachments are known as the meniscal roots. The medial meniscus is larger than the lateral and has a larger posterior horn than anterior horn. In the case of the lateral meniscus, the horns are of similar size, but in approximately 5% of individuals the lateral meniscus has a discoid morphology. A discoid meniscus is associated with increased incidence of pathology from a young age. Sagittal MRI sequences of the normal meniscus show a bow-tie configuration at the periphery. On progressive images toward the intercondylar fossa the meniscus appears as two triangles representing the anterior and posterior horns. The normal menisci exhibit uniform low signal on all MRI sequences, although in children some increased signal is frequently identified in the posterior third. Degeneration may lead to intrameniscal high signal, or ‘myxoid change’, particularly in the posterior medial meniscus. A tear is diagnosed on MRI when high signal is demonstrated extending to the articular surface of the meniscus. Tears may be horizontal or vertical depending on whether they reach one meniscal surface or two. A complex tear is diagnosed when two or more tear configurations are present. The configuration of a meniscal tear has important implications for management. Horizontal tears are frequently degenerative in nature and may be asymptomatic (Fig. 46-44). Joint fluid may escape through a horizontal tear, forming a parameniscal cyst. Two types of vertical tear are recognised. Longitudinal tears lie within the substance of the meniscus, tracking circumferentially. They often involve the periphery of the meniscus where the blood supply is better and may therefore heal spontaneously. As the name suggests, radial tears extend radially into the meniscus from the free edge; they take several forms. A small oblique slit is a common form and is called a parrot beak tear (Fig. 46-45). If it traverses the full width, a radial tear may split the meniscus, leading to separation of the two parts. A ‘ghost meniscus’ describes the MRI appearance of a complete radial tear where the image section passes through the split (Fig. 46-46). This sign is most often found in tears involving the posterior root of the medial meniscus. Some tears have a fragment which may displace and cause locking; this is particularly common with longitudinal tears, which, in particular, can give rise to a ‘bucket handle’ tear. Here the meniscal fragment remaining attached at both ends flips into the intercondylar notch (Fig. 46-47). The ‘double PCL sign’ describes a sagittal view showing the posterior cruciate ligament (PCL) and a second parallel low signal structure representing the displaced bucket handle fragment of a torn meniscus (Fig. 46-48).


Anterior Cruciate Ligament
The anterior cruciate ligament (ACL) attaches proximally at the posteromedial margin of the lateral femoral condyle in the intercondylar fossa and distally at the anterior aspect of the tibial intercondylar eminence. The ACL acts to restrain anterior translation and, to a lesser extent, internal rotation of the tibia relative to the femur. On MRI, the ligament is best visualised on sagittal images, appearing normally as fan-shaped bundles of taut fibres. Two bundles, the anteromedial and posterolateral, may be differentiated on the coronal and axial sequences. As fluid and loose connective tissue may be interspaced between the bundles, the ACL often appears larger and of more mixed signal intensity than the PCL.
ACL tears are common sporting injuries. On MRI, complete tears appear as discontinuity of the fibres, increased signal and/or laxity (Fig. 46-49). The mid-substance of the ligament is injured more frequently than the proximal or distal portions. Partial tears or sprains of the ACL are recognised on MRI by altered signal and/or laxity in the presence of continuity of some fibres. There are several secondary imaging signs associated with ACL injury. Typically there is microfracture in the posterior aspect of the lateral tibial plateau and the subarticular lateral femoral condyle, reflecting impaction between these sites during subluxation of the knee at the time of the injury (pivot shift injury). ACL tears may be accompanied by anterior translation of the tibia relative to the femur. This can be detected on sagittal images as it will cause buckling of the PCL. The lateral notch sign, which is specific but not very sensitive for ACL injury, describes abnormally deep indentation of the condylopatellar sulcus of the lateral femoral condyle on a lateral conventional radiograph.30 ACL injuries are commonly associated with injury to other structures. O'Donaghue's triad describes tears of the ACL, MCL and medial meniscus. A Segond fracture, which has a high association with ACL injury, describes avulsion of a fracture fragment from the lateral margin of the lateral tibial condyle at the attachment of the joint capsule.

Posterior Cruciate Ligament
The posterior cruciate ligament (PCL) extends from the anterolateral margin of the medial femoral condyle to the posterior aspect of the tibial intercondylar eminence. It normally appears as a thick low signal bundle that is visualised well in all planes on MRI. Tears of the PCL, e.g. from a sporting or dashboard-type injury, may result in instability characterised by posterior translation of the tibia relative to the femur. Partial intrasubstance ruptures of the PCL are more common than complete tears and avulsions. Intrasubstance tears exhibit thickening and altered signal on MRI while usually maintaining the appearance of a continuous structure (Fig. 46-50).31 Microfracture of the anterior aspect of the tibial plateau is typical. Associated soft-tissue injury is common, including tears of the ACL, medial collateral ligament and posterolateral corner.

Medial Collateral Ligament
The medial collateral ligament (MCL) has superficial and deep components; the former are more important for maintaining knee stability in the presence of valgus forces. The posterior oblique ligament is found more posteriorly and is formed by contributions from the superficial and deep MCL. Together with the semimembranosus tendon, it is an important stabiliser of the knee posteromedially. Coronal MRI sequences clearly identify the MCL as a thin low signal band, differentiating the superficial portion from the much shorter deep portion which has attachments to the middle third of the lateral meniscus. Injury to the MCL may be classified according to severity.32 A Grade 1 sprain is a periligamentous injury characterised by oedema around the ligament which maintains low signal. A Grade 2 injury represents a partial tear with focal intraligamentous thickening and altered signal intensity as a result of oedema and/or haemorrhage. A Grade 3, or complete, tear shows complete discontinuity across the ligament. Chronic ossification of the proximal MCL following injury is known as a Pellegrini–Stieda lesion.
Lateral Collateral Ligament Complex and Posterolateral Corner
Lateral joint stability is provided by a number of structures including anteriorly, the iliotibial band, which attaches onto the proximal tibia. The lateral collateral ligament (LCL), or fibular collateral ligament, passes between the lateral femoral condyle and the fibular head. The biceps femoris tendon has a common attachment with the LCL to the fibular head known as the conjoint tendon. LCL tears may arise within the ligamentous substance or from avulsion at the fibular head.
The LCL is a component of the posterolateral corner complex of supporting structures which also includes the popliteus tendon, biceps tendon, arcuate ligament, popliteofibular ligament and posterior joint capsule. Injury to the posterolateral corner is often associated with damage to other ligamentous structures, most commonly tears of the ACL. Posterolateral corner injuries may lead to posterolateral instability which has implications for surgical management, particularly when associated with ACL injuries. While the LCL, biceps tendon and popliteus are seen well on MRI, it is often difficult to reliably evaluate the smaller components of the posterolateral corner individually because of their small size and orientation.
The Extensor Mechanism and Patellofemoral Joint
The patella is a sesamoid bone (the largest in the body) that lies between the quadriceps tendon proximally and the patellar tendon distally. The medial and lateral patellar retinacula also form part of the extensor mechanism. The patella articulates with the trochlea groove, or sulcus, of the femur. This groove is an important component in providing stability to the patella. Trochlea dysplasia describes a shallow sulcus (this can be measured on imaging) that predisposes to patellar dislocation. An abnormally high position of the patella (patella alta) may contribute to patellar maltracking and/or cartilage damage. The Insall–Salvati ratio assesses relative patella height and is given by the ratio of patellar tendon length to the length of the patella itself. It can be calculated from conventional radiographs or sagittal MRI images.33,34 Axial MRI or CT images may be used to measure the tibial tubercle–trochlea groove distance (TTD) which identifies lateralisation of the patellar tendon insertion (which predisposes to lateral dislocation).35 The patella is prone to dislocate laterally due to the valgus force of the quadriceps muscle group, although in the majority of cases this dislocation is transient and by the time of presentation to hospital the patella has reduced. Nevertheless there are characteristic MRI findings in acute patellar dislocation–relocation (Fig. 46-51). These include subcortical bone marrow oedema of the medial patella and lateral femoral condyle reflecting ‘kissing contusions’. There is usually an associated tear of the medial patellar retinaculum and/or an osteochondral fracture of the patella.
Cartilage degeneration in the knee is common as a feature of osteoarthritis. Chondromalacia patellae describes cartilage damage occurring in adolescents and young adults which primarily involves the patellofemoral compartment. This may be associated with patellar misalignment or trauma. Cartilage damage can be graded according to severity. Early damage is demonstrated on MRI as signal abnormality and thinning. Progressive damage appears as full-thickness fissuring or a defect. The presence of subchondral oedema or cyst formation indicates the most severe damage.
Patellar tendinopathy involving the proximal tendon attachment is commonly referred to as ‘jumper’s knee’ because of its association with athletic activities that involve jumping. It can be demonstrated on MRI and ultrasound where it typically appears as focal thickening of the central deep portion of the proximal tendon with increased Doppler vascularity (Fig. 46-52). On ultrasound the tendinopathic tendon shows low reflectivity and on MRI increased intrasubstance signal. Patellar tendinopathy may also involve the more distal tendon. Osgood–Schlatter disease is a common condition in children aged between 8 and 13 years and is characterised by distal patellar tendinopathy, tibial tubercle enlargement or fragmentation and thickening of the overlying soft tissues. The condition is thought to result from repetitive traction injury related to sporting activity. Tears of the patella or quadriceps tendons may occur, typically on the background of tendinopathy. They are readily evaluated with ultrasound or MRI.
Bone and Cartilage
Osteochondritis dissecans is a common condition of uncertain aetiology affecting children and adolescents. It is characterised by focal cartilage and subchondral bone abnormality, and most commonly involves the lateral aspect of the medial femoral condyle. Conventional radiographs may reveal linear subarticular lucency with adjacent sclerosis but they are not sensitive. MRI clearly demonstrates these lesions, allowing measurement and localisation. A rim of fluid signal which undercuts the involved bone implies the lesion has become detached and may go on to displace into the joint space.
Repeated mechanical trauma to the articular surfaces of the knee may lead to subchondral fractures. Often occult on conventional radiographs, these lesions are demonstrated on fluid-sensitive MRI sequences as focal linear subchondral low signal (indicating the fracture line) with intense surrounding oedema-like signal in the bone marrow. Cartilage and meniscal damage may predispose to such injuries. Normal forces in the absence of predisposing abnormality may cause subchondral fracture if the underlying bone is weak (insufficiency fracture). Subchondral insufficiency fracture was sometimes previously referred to as ‘spontaneous osteonecrosis of the knee’, a term that is incorrect and becoming archaic. Recent interest has focused on a condition called ‘bone marrow oedema syndrome’ or ‘transient osteoporosis’ which is believed to predispose to insufficiency fracture in the knee and elsewhere (Fig. 46-53).28

Bursae
There are numerous anatomical bursae around the knee. Inflammation of a bursa, or bursitis, is commonly caused by friction from repetitive movement, though bursae may also be involved in systemic inflammatory conditions such as rheumatoid arthritis. Around the patellar tendon there are the superficial infrapatellar, deep infrapatellar and prepatellar bursae. Bursitis may affect any of these, and involvement of the last is called ‘housemaid’s knee’. Friction between the distal iliotibial band and lateral femoral condyle may give rise to bursitis known as ‘runner’s knee’. Inflammation of the pes anserine bursa gives rise to pain over the anteromedial aspect of the proximal tibia. The most commonly involved bursa in the popliteal region lies between the medial head of gastrocnemius and the semimembranosus tendon, the popliteal bursa. This communicates with the joint and distension of this bursa is called a popliteal or baker's cyst.
The Ankle and Foot
The ankle allows a wide range of movement, but also has to transmit considerable forces. It is the most commonly injured joint, with ligamentous injury in the form of sprains and tears particularly common. Patients typically present with pain and/or instability following such injury. The talar dome articulates with the tibial plafond and small facets on the medial and lateral malleoli. The malleoli contribute to the joint stability and provide attachments for the collateral ligaments, which are themselves important stabilisers of the ankle. The distal tibiofibular joint is a fibrous joint that contains a synovial recess extending from the ankle joint. Several tendons crossing the ankle joint are also prone to injury.
Ligaments
Injuries sustained to the ankle usually result from inversion or eversion. Inversion injuries are significantly more common than eversion injuries, with the result that the lateral ankle ligaments are torn more frequently than the medial. Three components of the lateral collateral ligament complex are recognised: the anterior and posterior talofibular ligaments and the calcaneofibular ligament. The anterior talofibular ligament is the most vulnerable to injury, followed by the calcaneofibular ligament. The posterior talofibular ligament is rarely injured except in the most severe cases. MRI or ultrasound may be used for assessment of these structures. On imaging, ligament damage may appear as altered signal/echogenicity, thickening, thinning, or absence (indicating a complete tear) (Fig. 46-54).36 Damage to the lateral ligaments may lead to chronic anterolateral impingement in the absence of frank instability. Anterolateral impingement describes repetitive soft-tissue injury in the anterolateral gutter, causing synovitis and haemorrhage, which may be identified on MRI.37
The most important medial ankle ligaments include the anterior and posterior tibiotalar (also known as deltoid), tibio-spring and spring ligaments. The spring ligament extends from the calcaneus to the navicular and functions as an important stabiliser of the foot arch together with the posterior tibial tendon. The distal tibiotalar syndesmosis comprises anterior, interosseous and posterior tibiofibular ligaments. Strong forces are usually required to disrupt the syndesmotic ligaments such as those resulting in an ankle fracture. However, syndesmotic ligament injuries do occur, typically as a sports injury.
Tendons
Tendon abnormalities are common about the ankle. The tendons crossing the ankle anteriorly, medially and laterally do so in tendon sheaths and symptoms may relate to tenosynovitis as well as to tendinopathy if there is symptomatic intrinsic degeneration, tear, or subluxation/dislocation of the tendon itself. The last of these may occur if there is retinacular injury. The Achilles tendon is the largest tendon in the body. It is also vulnerable to tendinopathy and tears. Like the patellar tendon, the Achilles does not have a tendon sheath, but its surrounding tissues may still become inflamed. This is known as paratenonitis. Ultrasound and MRI are both excellent techniques for assessing the tendons. Ultrasound has the advantage of greater spatial resolution, Doppler flow to show inflammatory hyperaemia and dynamic imaging with ankle movement.
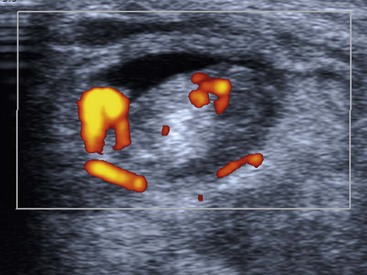
The posteromedial ankle tendons comprise the tibialis posterior (TP), flexor digitorum longus (FDL) and flexor hallucis longus (FHL) tendons. TP is the strongest of these, with approximately twice the cross-sectional area of FDL. It is also the most frequently affected by pathology. TP function is important in maintaining the medial arch of the foot (with the spring ligament) and tears of TP may lead to flat foot deformity. An os naviculare is a sesamoid bone located at the insertion of TP. Tenosynovitis appears as increased fluid in the tendon sheath, sometimes with altered appearance of the tendon itself. Ultrasound can help confirm the diagnosis by demonstrating hyperaemia on Doppler interrogation of the tendon or its sheath (Fig. 46-55). On MRI, a greater cross-sectional area of fluid than tendon is suggestive of tenosynovitis. The FHL and very occasionally the FDL tendon sheaths communicate with the ankle joint in a minority of individuals. Therefore fluid in these tendon sheaths may relate to an ankle joint effusion.
The peroneal tendons pass posterior to the lateral malleolus, where the peroneus brevis (PB) tendon is normally located between the peroneus longus (PL) tendon and the malleolus in the fibular groove. Both tendons are retained by the superior peroneal retinaculum (SPR). The SPR extends from the posterolateral fibular periostium to the Achilles tendon aponeurosis. The PB tendon is prone to longitudinal tears or ‘splits’. In the early stages the PB tendon adopts a semilunar or boomerang shape which progresses to a split with inter-positioning of the PL tendon between the split fibres of PB. Tears of the SPR may lead to peroneal tendon dislocation (Fig. 46-56). Dynamic imaging with ultrasound shows lateral dislocation of the peroneal tendons from the fibular groove with provocative movements.38 A sesamoid os peroneum within the PL tendon is present in a minority of individuals. The os peroneum may be associated with PL tendinopathy or may itself be fractured or inflamed, giving rise to pain. Tears of PL tend to occur at the level of the cuboid tunnel or just distal to an os perineum, if present. Pathology of the anterior ankle tendons, comprising the tibialis anterior, extensor hallucis longus and extensor digitorum longus tendons, is infrequent. Tears of tibialis anterior occur more commonly in older age groups particularly close to the insertion of the medial cuneiform.

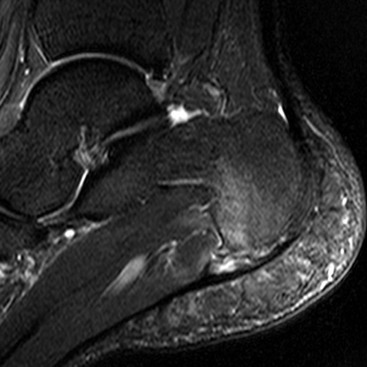
Achilles tendinopathy is common and may be related to athletic activities in young adults. However, more typically it occurs in the middle aged. It results from chronic microtrauma to the tendon, leading to tendon degeneration. Typically there is focal fusiform thickening of the tendon involving the mid-portion, with increased signal on short and long TE MRI and low reflectivity and loss of normal tendon echotexture on US. The insertion is less often involved, although this can be affected by enthesopathy or by mechanical impingement from a prominent posterior calcaneal process (Haglund's bump). Ultrasound also demonstrates hyperaemia on Doppler interrogation of the tendon or deep fat pad (Kager's fat pad). The Achilles tendon lacks a tendon sheath. However, inflammation of the surrounding tissues or paratenon, (paratenonitis) may be seen, particularly in runners. The paratenon is found on the superficial, medial and lateral aspects of the tendon and when inflamed appears on MRI as a rim of ill-defined increased signal on these aspects of the tendon. On ultrasound the paratenon appears as a hyporeflective rim. Acute tears of the Achilles tendon may be partial or complete. Complete tears (which are much more common) exhibit no continuity of fibres and may show retraction (Fig. 46-57). Dynamic ultrasound imaging is useful for measuring the separation of the tendon ends for surgical planning.39 The retrocalcaneal bursa is located deep to the insertion of the Achilles tendon. Inflammation of this bursa may be found in association with Achilles tendinopathy and usually results from chronic and repetitive microtrauma, frequently described as overuse injury. Systemic inflammatory disorders including rheumatoid and seronegative arthritis may also cause inflammation of the Achilles tendon insertion or retrocalcaneal bursa. Retro-Achilles bursitis involves the bursa superficial to the Achilles tendon.

Bone
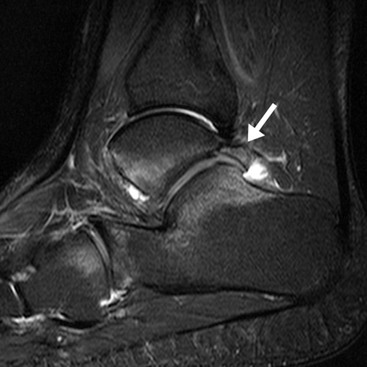
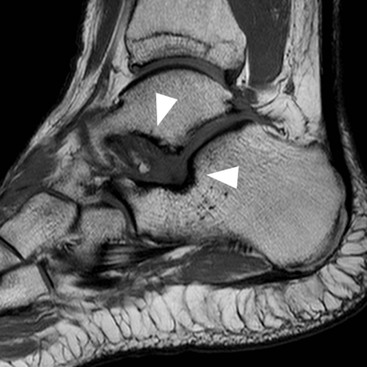
Osteochondral lesion (OCL) of the talar dome is a common cause of persisting deep ankle pain. Most talar OCL occur following trauma, though some medial lesions arise without a history of injury.40 OCL is easily missed on conventional radiographs of the ankle. MRI is very sensitive for OCL, allowing assessment of location and size (Fig. 46-58). The presence of fluid signal around the lesion helps to determine whether the lesion is partially detached, detached or displaced.
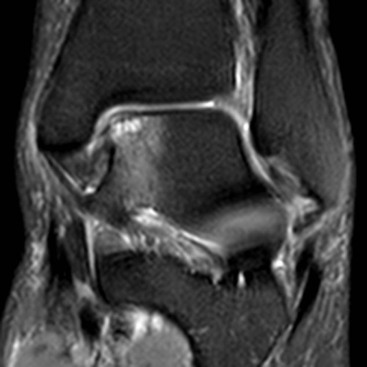
Impingement may occur in various locations around the ankle, the commonest types being anterolateral (see above), anterior and posterior. Anterior impingement occurs between bony spurs on the dorsal talar neck and anterior tibial plafond, a condition associated with kicking activities like soccer. These spurs can be readily identified on lateral radiographs. MRI may additionally reveal synovitis and lateral ankle ligament damage.41 Posterior impingement is most frequently associated with a large os trigonum or Stieda process of the talus (Fig. 46-59). These give rise to chronic compression of soft tissues against the posterior tibia in activities that involve repetitive forced plantar flexion as in ballet dancing.42
Tarsal Coalition
Tarsal coalition refers to developmental fusion of two (rarely three) bones in the hind-foot. Coalition may be osseous or non-osseous (the latter may be fibrous or cartilaginous). The most common type is calcaneonavicular followed by subtalar, other types being much less common. In calcaneonavicular coalition the navicular is fused to the calcaneus through an elongated anterior calcaneal process (Fig. 46-60). In subtalar coalition there is fusion between the talus and calcaneus at or adjacent to the middle subtalar joint. This results in a characteristic ‘C-sign’ on a lateral radiograph reflecting continuation of the bone contour through the coalition. MRI and CT are much more sensitive than plain radiographs for tarsal coalition. Stress changes may also be demonstrated at the site of coalition or in nearby structures.

Other Soft-Tissue Abnormalities
Plantar fasciitis is a common cause of heel pain thought to result from chronic microtrauma of the plantar fascia from biomechanical stress. The central band is most frequently involved near its calcaneal origin. The diagnosis is made on ultrasound when there is thickening of the fascia (normally measuring up to 5 mm43) and loss of normal echogenic fibrillar texture. MRI reveals thickening and increased signal on fluid-sensitive sequences, indicating inflammation (Fig. 46-61). A calcaneal spur may be present but this is often found in the absence of plantar fasciitis and there is no role for conventional radiographs in the diagnosis of plantar fasciitis. Other less common causes of plantar fascia thickening to consider include seronegative arthropathy, plantar fibroma and hyperlipidaemia.
The sinus tarsi is a cone-shaped space between the anterior and posterior subtalar joints containing fat surrounding ligaments, small vessels and nerve endings. Sinus tarsi syndrome describes pain arising from this structure, typically occurring with a history of an ankle sprain. The exact aetiology is unclear and it may be that this syndrome has a number of different causes. The condition is identified on MRI as loss of the normal high T1 fat signal in the sinus tarsi (Fig. 46-62).44
Tarsal tunnel syndrome is an entrapment neuropathy of the posterior tibial nerve giving rise to pain/paraesthesia on the plantar aspect of the foot and a positive Tinel's sign. Muscle weakness is less common. The posterior tibial nerve is compressed within the tarsal tunnel, a compartment in the posteromedial ankle which is bounded by the flexor retinaculum. The tunnel transmits the posterior tibial nerve as part of a neurovascular bundle and the tendons of TP, FDL and FHL. MRI or ultrasound may be used to identify a lesion compressing the nerve such as a ganglion, bone fracture, nerve sheath tumour or accessory FDL. MRI may additionally reveal oedema in denervated muscles supplied by the nerve.
The plantar plate is a fibrocartilaginous structure extending from the metatarsal neck to the base of the proximal phalanx of each toe. Its function is to resist hyperextension of the MTP joint. Plantar plate rupture most commonly affects the great toe. It may be diagnosed with ultrasound or MRI. MRI with injection of contrast medium into the MTP joint dorsally demonstrates escape of the contrast agent through the torn plantar plate, leading to opacification of the flexor tendon sheath.
Morton neuroma is another cause of metatarsalgia, most commonly arising in the third web space. It is thought to result from repetitive compression of the plantar common digital nerve, leading to perineural fibrosis. On ultrasound a Morton's neuroma typically appears as a rounded hypoechoic mass. On MRI it appears as a low-to-intermediate signal intensity mass in a characteristic position. The advantage of ultrasound in this setting is to guide injection therapy after the diagnosis has been confirmed.
For a full list of references, please see ExpertConsult.