Pelvis and Perineum
1 Introduction
The bowl-shaped pelvic cavity is continuous superiorly with the abdomen and bounded inferiorly by the perineum, the region between the thighs. The bones of the pelvic girdle demarcate the following two regions:
• Greater or false pelvis: the lower portion of the abdomen that lies between the flared iliac crests.
• Lesser or true pelvis: demarcated by the pelvic brim, sacrum, and coccyx, and contains the pelvic viscera.
The pelvis contains the terminal gastrointestinal tract and urinary system and the internal reproductive organs. The perineum lies below the “pelvic diaphragm,” or muscles that form the pelvic floor, and contains the external genitalia. Our review of the pelvis and perineum focuses on the musculoskeletal structures that support the pelvis and then examines the viscera, blood supply, and innervation of these two regions.
2 Surface Anatomy
Key landmarks of the surface anatomy of the pelvis and perineum include the following (Fig. 5-1):
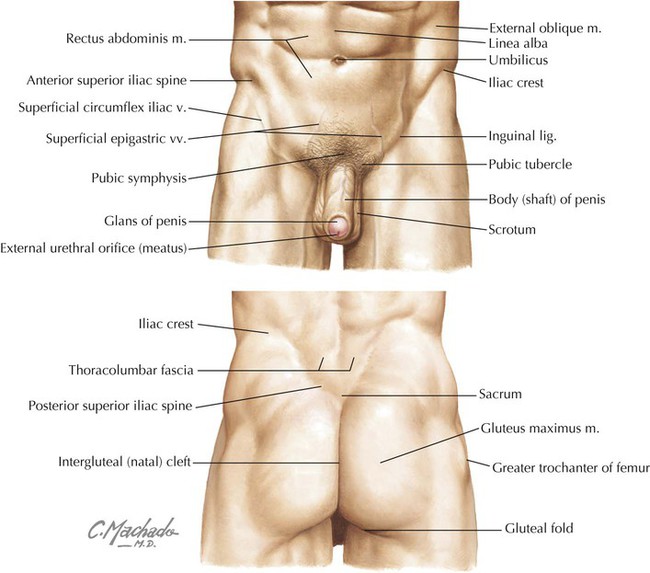
• Umbilicus: site that marks the T10 dermatome, that lies at the level of the intervertebral disc between L3 and L4; can lie slightly lower in infants or morbidly obese individuals and higher in late pregnancy.
• Iliac crest: rim of the ilium that lies at approximately the L4 level; also the approximate level of the bifurcation of the abdominal aorta into its two common iliac branches.
• Anterior superior iliac spine: superior attachment point for the inguinal ligament.
• Inguinal ligament: ligament formed by the aponeurosis of the external abdominal oblique muscle; forms a line of demarcation separating the lower abdominopelvic region from the thighs.
• Pubic tubercle: the inferior attachment point of the inguinal ligament.
• Posterior superior iliac spine: often seen as a “dimpling” of the skin just above the intergluteal (natal) cleft; often more obvious in females.
3 Musculoskeletal Elements
Bony Pelvic Girdle
The pelvic girdle is the attachment point of the lower limb to the body's trunk. (The pectoral girdle is its counterpart for the attachment of the upper limb.) The bones of the pelvis include the following (Fig. 5-2):

• Right and left pelvic bones (coxal or hip bones): fusion of three separate bones—the ilium, ischium, and pubis—that join in the acetabulum (cup-shaped surface where pelvis articulates with head of femur).
• Sacrum: fusion of the five sacral vertebrae; the two pelvic bones articulate with the sacrum posteriorly.
• Coccyx: terminal end of the vertebral column; a remnant of our embryonic tail (see also Table 2-2).
The pelvis protects the pelvic viscera, supports the weight of the body, aids in ambulation by swinging side to side in a rotary movement at the lumbosacral articulation, provides for muscle attachments, and provides a bony support for the lower birth canal. The pelvic inlet is the circular opening where the lower abdominal cavity is continuous with the pelvic cavity; the promontory of the sacrum protrudes into this opening and is its posterior midline margin (Fig. 5-3). The pelvic outlet is diamond shaped and bounded by the pubic symphysis anteriorly, the pubic arches, the inferior pubic rami and ischial rami, the sacrotuberous ligament, and the coccyx. The perineum is enclosed by these boundaries and lies below the pelvic floor (see Fig. 5-17).

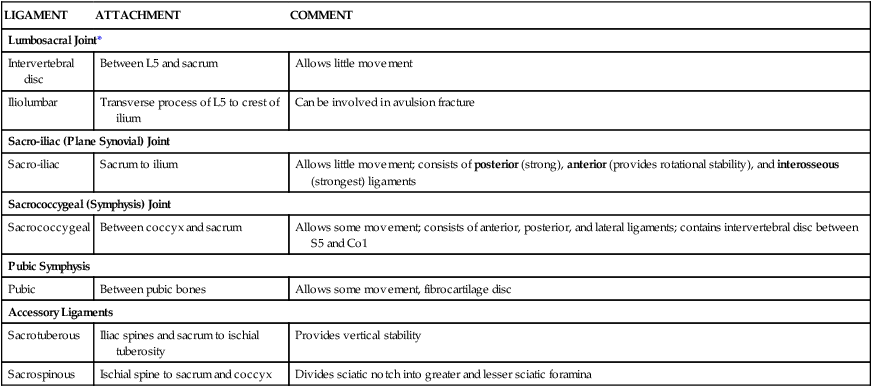
The pelvic girdle forms a stable articulation to support the transfer of weight from the trunk to the lower limb. Weight is transferred from the lumbar vertebral column to the sacrum, across the sacro-iliac joints to the coxal (pelvic or hip) bones, and then to the femur (thigh bone). The joints and ligaments reflect this stability (Fig. 5-3 and Table 5-1). The sacro-iliac ligaments are strong, and the posterior sacro-iliac ligament, posterior to the articular joints, is one of the strongest ligaments in the body and supports its entire weight (see Chapter 2).
TABLE 5-1
Joints and Ligaments of the Pelvis
| LIGAMENT | ATTACHMENT | COMMENT |
| Lumbosacral Joint* | ||
| Intervertebral disc | Between L5 and sacrum | Allows little movement |
| Iliolumbar | Transverse process of L5 to crest of ilium | Can be involved in avulsion fracture |
| Sacro-iliac (Plane Synovial) Joint | ||
| Sacro-iliac | Sacrum to ilium | Allows little movement; consists of posterior (strong), anterior (provides rotational stability), and interosseous (strongest) ligaments |
| Sacrococcygeal (Symphysis) Joint | ||
| Sacrococcygeal | Between coccyx and sacrum | Allows some movement; consists of anterior, posterior, and lateral ligaments; contains intervertebral disc between S5 and Co1 |
| Pubic Symphysis | ||
| Pubic | Between pubic bones | Allows some movement, fibrocartilage disc |
| Accessory Ligaments | ||
| Sacrotuberous | Iliac spines and sacrum to ischial tuberosity | Provides vertical stability |
| Sacrospinous | Ischial spine to sacrum and coccyx | Divides sciatic notch into greater and lesser sciatic foramina |
*Other ligaments include those binding any two vertebrae and facet joints.
Anatomical differences in the female bony pelvis reflect the adaptations for childbirth. The differences from the male pelvis include the following:
• The bones of the female pelvis usually are smaller, lighter, and thinner.
• The pelvic inlet is oval in the female and heart shaped in the male.
• The female pelvic outlet is larger because of everted ischial tuberosities.
• The female pelvic cavity is wider and shallower.
• The female pubic arch is larger and wider.
• The greater sciatic notch is wider in females.
• The female sacrum is shorter and wider.
• The obturator foramen is oval or triangular in the female and round in the male.
The female pelvis may assume variable shapes, as follows:
• Gynecoid: normal, and most common form in Caucasian women.
• Android: a masculine pelvic type.
• Platypelloid: foreshortened in the anteroposterior dimension and wider in the transverse dimension.
• Anthropoid: resembling the pelvis of an anthropoid ape, with a greatly elongated anteroposterior dimension and a shortened transverse dimension.
Various asymmetric shapes may also result from scoliosis, poliomyelitis, fractures, and other pathologies.
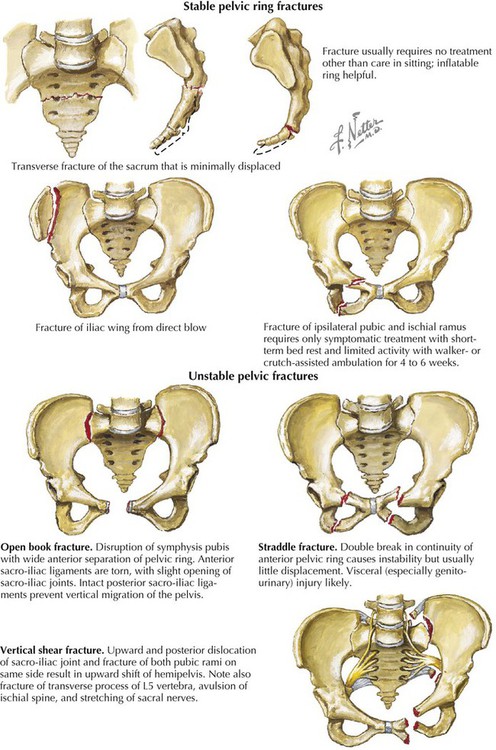
Clinical Focus 5-1 Pelvic Fractures
Clinically, the term pelvic fractures is used to describe fractures of the pelvic ring and does not typically include acetabular fractures, which are a separate type of fracture, usually from high-impact falls or automobile crashes. Pelvic fractures may be high or low impact; high-impact fractures often involve significant bleeding and may be life threatening. Pelvic ring fractures are classified as stable, involving only one side of the ring, or unstable, involving both parts of the pelvic ring.
Muscles of the Pelvis
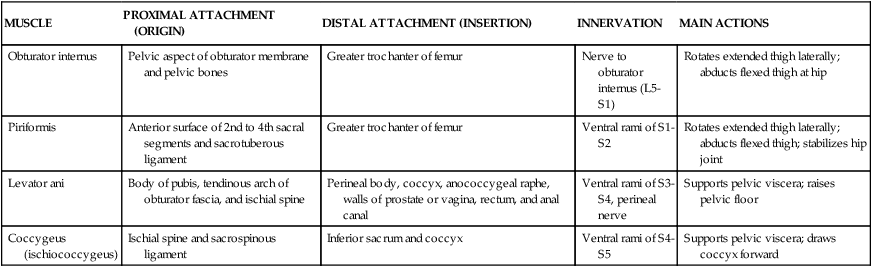
The muscles of the true pelvis line its lateral wall and form a floor over the pelvic outlet. (The pelvic inlet is demarcated by the pelvic brim.) Two muscles line the lateral wall (obturator internus and piriformis) and attach to the femur (see Table 6-5), and two muscles form the floor, or pelvic diaphragm (levator ani and coccygeus) (Fig. 5-4 and Table 5-2). The levator ani muscle consists of three muscle groups intermingled to form a single sheet of muscle (iliococcygeus, pubococcygeus, and puborectalis). The levator ani muscle is an important support structure for the pelvic viscera in bipeds (upright-walking humans) and helps maintain closure of the vagina and rectum. Bipedalism places greater pressure on the lower pelvic floor, and the coccygeus and levator ani muscles have been “co-opted” for a different use than originally intended in most land-dwelling quadruped mammals. Thus, the muscles once used to tuck the tail between the hind legs (coccygeus) and wag the tail (levator ani) now subserve a support function as we have evolved as bipeds and have lost our tail.
TABLE 5-2
| MUSCLE | PROXIMAL ATTACHMENT (ORIGIN) | DISTAL ATTACHMENT (INSERTION) | INNERVATION | MAIN ACTIONS |
| Obturator internus | Pelvic aspect of obturator membrane and pelvic bones | Greater trochanter of femur | Nerve to obturator internus (L5-S1) | Rotates extended thigh laterally; abducts flexed thigh at hip |
| Piriformis | Anterior surface of 2nd to 4th sacral segments and sacrotuberous ligament | Greater trochanter of femur | Ventral rami of S1-S2 | Rotates extended thigh laterally; abducts flexed thigh; stabilizes hip joint |
| Levator ani | Body of pubis, tendinous arch of obturator fascia, and ischial spine | Perineal body, coccyx, anococcygeal raphe, walls of prostate or vagina, rectum, and anal canal | Ventral rami of S3-S4, perineal nerve | Supports pelvic viscera; raises pelvic floor |
| Coccygeus (ischiococcygeus) | Ischial spine and sacrospinous ligament | Inferior sacrum and coccyx | Ventral rami of S4-S5 | Supports pelvic viscera; draws coccyx forward |

4 Viscera
Distal Gastrointestinal Tract
In both genders the distal gastrointestinal tract passes into the pelvis as the rectum and anal canal. The rectosigmoid junction superiorly lies at about the level of the S3 vertebra, and the rectum extends inferiorly to become the anal canal just below the coccyx (Fig. 5-5). As the rectum passes through the pelvic diaphragm, it bends posteriorly at the anorectal flexure and becomes the anal canal. The anorectal flexure helps maintain fecal continence through the muscle tone maintained by the puborectalis portion of the levator ani muscle. During defecation this flexure straightens, and fecal matter can then move into the anal canal. Superiorly, the rectum is covered on its anterolateral surface with peritoneum, which gradually covers only the anterior surface, while the distal portion of the rectum descends below the peritoneal cavity (subperitoneal) to the anorectal flexure. Features of the rectum and anal canal are summarized in Table 5-3.
TABLE 5-3
Features of the Rectum and Anal Canal
| STRUCTURE | CHARACTERISTICS |
| Pelvic diaphragm | Consists of levator ani and coccygeus muscles; supports pelvic viscera |
| Internal sphincter | Smooth muscle anal sphincter |
| Pectinate line | Demarcates visceral (above) from somatic (below) portions of anal canal by type of epithelium, innervation, and embryology |
| External sphincter | Skeletal muscle sphincter (subcutaneous, superficial, and deep) |

Distal Urinary Tract
The distal elements of the urinary tract lie within the pelvis and include the following (Fig. 5-6):

• Distal ureters: pass retroperitoneally into the pelvic inlet and are crossed anteriorly by the uterine artery in females and the ductus deferens in males before terminating in the urinary bladder. The ureter enters the bladder and passes obliquely through the smooth muscle wall; this arrangement provides for a sphincter-like action.
• Urinary bladder: lies behind the pubic symphysis in a subperitoneal position; holds up to 800 mL of urine (less in women and even less during pregnancy), and contains a smooth triangular area internally between the openings of the two ureters and the single urethral opening inferiorly, the trigone of the bladder. The smooth muscle of the bladder wall is the detrusor muscle.
• Urethra: short in the female (3-4 cm) and contains two small para-urethral mucous glands (Skene's glands) at its aperture; longer in the male (20 cm) and divided into the prostatic, membranous, and spongy portions. The prostatic portion (about 3 cm) traverses the prostate gland, the membranous portion (2 cm) traverses the external urethral sphincter (skeletal muscle), and the spongy portion (15 cm) traverses the corpus spongiosum on the ventral aspect of the penis.
Females have an external urethral sphincter composed of skeletal muscle under voluntary control and innervated by the somatic nerve fibers in the pudendal nerve (S2-S4). Males have the following urethral sphincters:
• Internal sphincter: smooth-muscle involuntary sphincter at the neck of the bladder and innervated by sympathetic fibers from L1 to L2; during ejaculation, it contracts and prevents semen from entering the urinary bladder.
• External sphincter: skeletal muscle voluntary sphincter surrounding the membranous urethra and innervated by the somatic nerve fibers in the pudendal nerve (S2-S4).
Micturition (urination/voiding) occurs by the following sequence of events:
• Normally, the sympathetic fibers relax the bladder wall and constrict the internal urethral sphincter (smooth muscle around the bladder neck, present only in males), thus inhibiting emptying.
• Micturition is initiated by the stimulation of stretch receptors (afferents enter the spinal cord via the pelvic splanchnic nerves, S2-S4) located in the detrusor (smooth) muscle of the bladder when it begins to fill.
• Parasympathetic efferents (pelvic splanchnics) induce a reflex contraction of the detrusor muscle and relaxation of the internal sphincter (males only), enhancing the urge to void.
• When appropriate (and sometimes not!), somatic efferents via the pudendal nerve (S2-S4) cause voluntary relaxation of the external urethral sphincter, and the bladder begins to empty.
• When complete, the external urethral sphincter contracts (in males the bulbospongiosus muscle contracts to expel the last few drops of urine from the spongy urethra), and the detrusor muscle relaxes under sympathetic control.
Clinical Focus 5-2 Urinary Tract Infections
Urinary tract infection (UTI) is more common in females, likely directly related to their shorter urethra, urinary tract trauma, and exposure to pathogens in an environment conducive for growth and propagation. As illustrated, a number of other risk factors also may precipitate infections in either gender. Escherichia coli is the usual pathogen involved. UTI may lead to urethritis, cystitis (bladder inflammation), and pyelonephritis. Symptoms of cystitis include the following:

Clinical Focus 5-3 Stress Incontinence in Women
Involuntary loss of urine after an increase in intraabdominal pressure is often associated with a weakening of the support structures of the pelvic floor, including the following:
• Medial and lateral pubovesical ligaments
• Pubovesical fascia at the urethrovesical junction (blends with the perineal membrane and body)
• Levator ani (provides support at the urethrovesical junction)
Common predisposing factors for stress incontinence include multiparity, obesity, chronic cough, and heavy lifting.

Female Pelvic Reproductive Viscera
The female pelvic reproductive viscera include the midline uterus and vagina and the adnexa (paired ovaries and uterine tubes).
The uterus is pear shaped, about 7 to 8 cm long, and exhibits a body (fundus and isthmus) and cervix. While the uterine cavity looks triangular in coronal section (see Fig. 5-8), in sagittal section it appears only as a thin slit (Fig. 5-6, top). The normal position of the uterus is in an anteflexed (anteverted) position and lies almost in the horizontal plane. A double sheet of peritoneum (actually a mesentery) called the broad ligament envelops the ovaries, uterine tubes, and uterus (Figs. 5-7 and 5-8). During embryonic development the ovaries are pulled into the pelvis by a fibromuscular band (homologue of the male gubernaculum). This ovarian ligament attaches the inferomedial pole of the ovary to the uterus, then reflects anterolaterally off the uterus as the round ligament of the uterus, enters the deep inguinal ring, courses down the inguinal canal, and ends in the labia majora of the perineum as a fibrofatty mass. Features of the female pelvic reproductive viscera are summarized in Table 5-4.
TABLE 5-4
Features of the Female Pelvic Viscera
| STRUCTURE | CHARACTERISTICS |
| Urinary bladder | Covered by peritoneum |
| Uterus | Consists of a body (fundus and isthmus) and cervix; supported by pelvic diaphragm and ligaments; enveloped in broad ligament |
| Ovaries | Suspended between suspensory ligament of ovary (contains ovarian vessels, nerves, and lymphatics) and ovarian ligament (tethered to uterus) |
| Uterine tubes (fallopian tubes) | Courses in mesosalpinx of broad ligament and consists of fimbriated end (collects ovulated ova), infundibulum, ampulla, isthmus, and intrauterine portions |
| Vagina | Fibromuscular tube that includes the fornix, a superior recess around protruding uterine cervix |
| Rectum | Distal retroperitoneal portion of large intestine |
| Vesico-uterine pouch | Peritoneal recess between bladder and uterus |
| Recto-uterine pouch (of Douglas) | Peritoneal recess between rectum and uterus and lowest point in female pelvis |
| Broad ligament | Peritoneal fold that suspends uterus and uterine tubes; includes mesovarium (enfolds ovary), mesosalpinx (enfolds uterine tube), and mesometrium (remainder of ligament) |
| Round ligament of uterus | Reflects off uterus and keeps uterus anteverted and anteflexed; passes into inguinal canal and ends as fibrofatty mass in labia majora |
| Transverse cervical (cardinal or Mackenrodt's) ligaments | Fibrous condensations of subperitoneal pelvic fascia that support uterus |
| Uterosacral ligaments | Extend from sides of cervix to sacrum, support uterus, and lie beneath peritoneum (form uterosacral fold) |
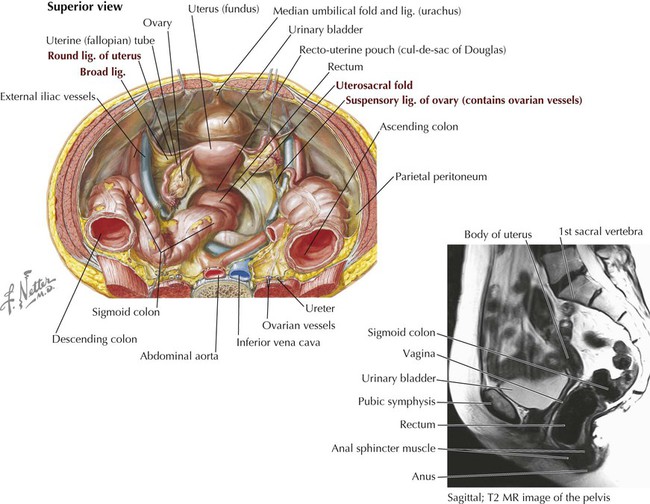

The vagina, about 8 to 9 cm long, is a fibromuscular tube that surrounds the uterine cervix and passes inferiorly through the pelvic floor to open in the vestibule (area enclosed by the labia minora). Because the uterine cervix projects into the superoanterior aspect of the vagina, a continuous gutter surrounds the cervical opening, shallower anteriorly and deeper posteriorly, forming the anterior, lateral, and posterior fornices.
The ovaries are almond-shaped female gonads 3 to 4 cm long (but smaller in older women) attached to the broad ligament by its mesovarium portion. The ovary is suspended between two attachments: laterally to the pelvic wall by the suspensory ligament of the ovary (contains the ovarian vessels, lymphatics, and autonomic nerve fibers) and medially to the uterus by the ovarian ligament.
The uterine tubes (fallopian tubes), about 10 cm long, are suspended in the mesosalpinx portion of the broad ligament and are subdivided into four parts:
• Infundibulum: fimbriated, expanded distal portion that opens at the ostium into the peritoneal cavity and lies close to the ovary.
• Ampulla: wide portion of the tube lying between the infundibulum and the isthmus; the usual site of fertilization.
• Isthmus: proximal, narrow, straight, and thickened portion of the tube that joins the body of the uterus.
• Intramural portion: traverses the uterine wall to open into the uterine cavity.
Clinical Focus 5-4 Uterine Prolapse
Uterine prolapse may occur when the support structures of the uterus, especially the cardinal ligaments, uterosacral ligaments, and levator ani muscle, are weakened.

Clinical Focus 5-5 Cervical Carcinoma
Approximately 85% to 90% of cervical carcinomas are squamous cell carcinomas, whereas 10% to 15% are adenocarcinomas. Most carcinomas occur near the external cervical os, where the cervical epithelium changes from simple columnar to stratified squamous epithelium (the transformation zone). The most common cause of cervical carcinoma is contraction of human papillomavirus (HPV) during sexual intercourse.

Clinical Focus 5-6 Uterine Leiomyomas (Fibroids)
Leiomyomas are benign tumors of smooth muscle and connective tissue cells of the myometrium of the uterus. These “fibroids” are firm and can range in size from 1 to 20 cm. The composite drawing shows various sizes and sites of potential leiomyomas.

Clinical Focus 5-7 Endometriosis
Endometriosis is a progressive benign condition characterized by ectopic foci of endometrial tissue, called implants, that grow in the pelvis—on the ovaries and in the recto-uterine pouch, uterine ligaments, and uterine tubes—or in the peritoneal cavity. As with the uterine lining, these estrogen-sensitive ectopic implants can grow and then break down and bleed in cycle with the woman's normal menstrual cycle.

Clinical Focus 5-8 Uterine Endometrial Carcinoma
Endometrial carcinoma is the most common malignancy of the female reproductive tract. It often occurs between the ages of 55 and 65 years, and risk factors include the following:
• Obesity (increased estrogen synthesis from fat cells without concomitant progesterone synthesis)
• Estrogen replacement therapy without concomitant progestin
• Early menarche or late menopause (prolonged estrogen stimulation)

Clinical Focus 5-9 Chronic Pelvic Inflammatory Disease
Recurrent or chronic infections of the uterine tubes or other adnexa (uterine appendages) result in cystic dilation (hydrosalpinx) and can account for approximately 40% of female infertility cases. Chronic pelvic inflammatory disease (PID) can cause scarring, causing problems with fertility, pelvic pain, or tubal (ectopic) pregnancy. The most affected age group is 15 to 25 years of age, and risk factors include the following:
Unilateral or bilateral adnexal masses are usually sausage shaped and may be palpable.

Clinical Focus 5-10 Dysfunctional Uterine Bleeding
Dysfunctional uterine bleeding (DUB) involves an irregular cycle or intermenstrual bleeding (painless) with no clinically identifiable cause. The etiology and pathogenesis are extensive and include local uterine, ovarian, or adnexal disorders, as well as systemic and pregnancy-related disorders. Hormonal imbalance is a common cause.

Clinical Focus 5-11 Ectopic Pregnancy
Ectopic pregnancy involves implantation of a blastocyst outside the uterine cavity, most often in the fallopian tube. Because of the potential medical danger of an ectopic pregnancy, the pregnancy is usually terminated medically (if detected early enough) or surgically (often laparoscopically).

Clinical Focus 5-12 Assisted Reproduction
Approximately 10% to 15% of infertile couples may benefit from various assisted reproductive strategies.

Clinical Focus 5-13 Ovarian Cancer
Ovarian cancer is the most lethal cancer of the female reproductive tract. From 85% to 90% of all malignancies occur from the surface epithelium, with cancerous cells often breaking through the capsule and seeding the peritoneal surface, invading the adjacent pelvic organs, or seeding the omentum, mesentery, and intestines. Additionally, the cancer cells spread via the venous system to the lungs (ovarian vein and inferior vena cava) and liver (portal system) and via lymphatics. Risk factors include the following:
• Family history of ovarian cancer
• Early menarche or late menopause (prolonged estrogen stimulation)

Male Pelvic Reproductive Viscera
The male pelvic reproductive viscera include the prostate gland and paired seminal vesicles. These structures lie in a subperitoneal position and are in close association with the urethra (Fig. 5-9). The testes descend into the scrotum late in human prenatal development and are connected to the seminal vesicles by the ductus (vas) deferens, which ascends in the scrotum, passes through the inguinal canal, and then courses retroperitoneally to join the duct of the seminal vesicles (ejaculatory ducts) (Table 5-5).
TABLE 5-5
Features of the Male Pelvic Viscera
| STRUCTURE | CHARACTERISTICS |
| Urinary bladder | Lies retroperitoneal and has detrusor muscle (smooth muscle) lining its walls |
| Prostate gland | Walnut-sized gland with five lobes (anterior, middle, posterior, right lateral, left lateral); middle lobe prone to benign hypertrophy and surrounds prostatic urethra |
| Seminal vesicles | Lobulated glands whose ducts join ductus deferens to form ejaculatory duct; secretes alkaline seminal fluid |
| Rectum | Distal portion of large intestine that is retroperitoneal |
| Rectovesical pouch | Recess between bladder and rectum |
| Testes | Develop in retroperitoneal abdominal wall and descend into scrotum |
| Epididymis | Consists of head, body, and tail and functions in maturation and storage of sperm |
| Ductus (vas) deferens | Passes in spermatic cord through inguinal canal to join duct of seminal vesicles (ejaculatory duct) |

The testes are paired gonads about the size of a chestnut with the following features (Fig. 5-10):
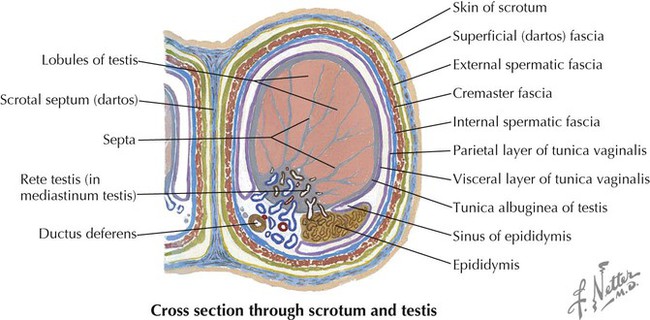
• During descent of the testes into the scrotum, a pouch of peritoneum called the tunica vaginalis attaches to the anterior and lateral aspect of the testes (has visceral and parietal layers).
• Testes are encased within a thick capsule, the tunica albuginea.
• Testes are divided into lobules that contain seminiferous tubules.
• The seminiferous tubules are lined with germinal epithelium that gives rise to spermatozoa.
• Testes drain spermatozoa into the rete testes (straight tubules) and efferent ductules of the epididymis.
• Sperm mature and are stored in the epididymis, a long coiled tube about 23 feet in length.
It is within the seminiferous tubules that spermatogenesis occurs. The testis is divided into about 250 lobules, each containing one to four seminiferous tubules, each about 50 cm (20 inches) long on average at full length. The complete cycle of spermatogenesis takes about 74 days and 12 more days for the sperm to mature and pass through the epididymis. About 300 million sperm cells are produced daily in the human testis.
The ductus deferens is 40 to 45 cm long and joins the ducts of the seminal vesicles to form the ejaculatory ducts, which empty into the prostatic urethra, the first portion of the male urethra leaving the urinary bladder (Fig. 5-11; see Fig. 5-9 and Table 5-5). The seminal vesicles have the following features:
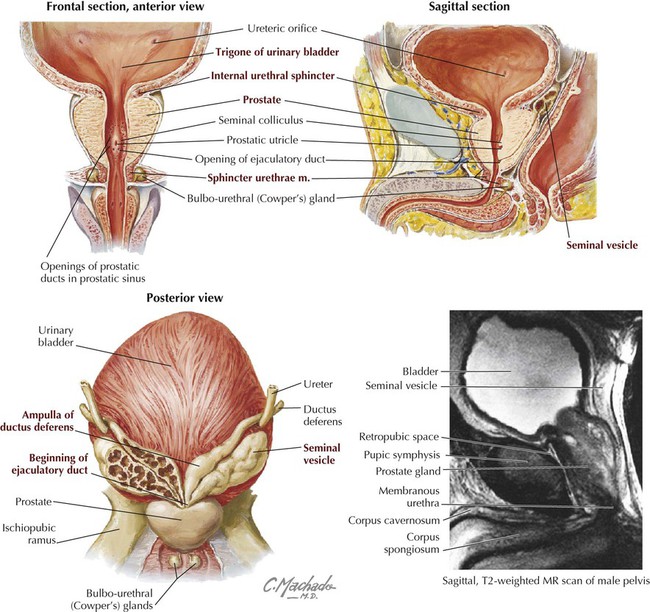
• Contribute fluid to the ejaculate; produce about 70% of the ejaculate volume.
• Produce a viscous and alkaline fluid that nourishes the spermatozoa and protects them from the acidic environment of the female vagina.
The prostate is a walnut-sized gland that surrounds the proximal urethra and has the following features:
• Contributes fluid to the ejaculate; produces about 20% of the ejaculate volume.
• Produces a thin, milky, slightly alkaline fluid that helps to liquefy coagulated semen after it is deposited in the vagina; contains citric acid, proteolytic enzymes, sugars, phosphate, and various ions.
About 3 to 5 mL of semen and 100 million sperm/mL are present in each ejaculation. The pH is between 7 and 8.
Clinical Focus 5-14 Vasectomy
Vasectomy offers birth control with a failure rate below that of the pill, condom, intrauterine device, and tubal ligation. It can be performed as an office procedure with a local anesthetic. (Approximately 500,000 are performed each year in the United States.) One approach uses a small incision on each side of the scrotum to isolate the vas deferens; another uses a small puncture (no incision) in the scrotal skin to isolate both the right and left vas. The muscular vas is identified, and a small segment is isolated between two small metal clips or sutures. The isolated segment is resected, the clipped ends of the vas are cauterized, and the incision is closed (or, in the nonincisional approach, the puncture wound is left unsutured).

Clinical Focus 5-15 Testicular Cancer
Testicular tumors are heterogeneous neoplasms, with 95% arising from germ cells and almost all malignant. Of the germ cell tumors, 60% show mixed histologic features, and 40% show a single histologic pattern. Surgical resection usually is performed using an inguinal approach (radical inguinal orchiectomy) to avoid spread of the cancer to the adjacent scrotal tissues.

Clinical Focus 5-16 Hydrocele and Varicocele
The most common cause of scrotal enlargement is hydrocele, an excessive accumulation of serous fluid within the tunica vaginalis (usually a potential space). An infection in the testis or epididymis, trauma, or a tumor may lead to hydrocele, or it may be idiopathic.
Varicocele is an abnormal dilation and tortuosity of the pampiniform venous plexus. Almost all varicoceles are on the left side, perhaps because the left testicular vein drains into the left renal vein, which has a slightly higher pressure, rather than into the larger inferior vena cava, as the right testicular vein does. A varicocele is evident at physical examination when a patient stands, but it usually resolves when the patient is recumbent.

Clinical Focus 5-17 Transurethral Resection of the Prostate
Benign prostatic hypertrophy (BPH) occurs in about 20% of men by age 40, increasing with age to 90% of males older than 80. BPH is really a nodular hyperplasia, not hypertrophy, and results from proliferation of epithelial and stromal tissues, often in the periurethral area. This growth can lead to urinary urgency, decreased stream force, frequency, and nocturia. Symptoms may necessitate transurethral resection of the prostate (TURP), in which the obstructing periurethral part of the gland is removed using a resectoscope. Although relatively rare, several surgical complications are illustrated.

Clinical Focus 5-18 Prostatic Carcinoma
Prostatic carcinoma is the most common visceral cancer in males and the second leading cause of death in men older than 50, after lung cancer. Primary lesions invade the prostatic capsule, then spread along the ejaculatory ducts into the space between the seminal vesicles and bladder. The pelvic lymphatics and rich venous drainage of the prostate (prostatic venous plexus) facilitate metastatic spread to distant sites.

Pelvic Fascia
The pelvic (endopelvic) fascia is the extraperitoneal layer just deep to the peritoneum that covers the lateral pelvic walls. The pelvic fascia covers the bladder, uterus, upper portion of the vagina, rectum, and anterior and lateral prostate. This fascia envelops the neurovascular bundles and condenses around the pelvic viscera, forming significant support structures, especially in the female. The major fascial condensations in the female include the following (Fig. 5-12):
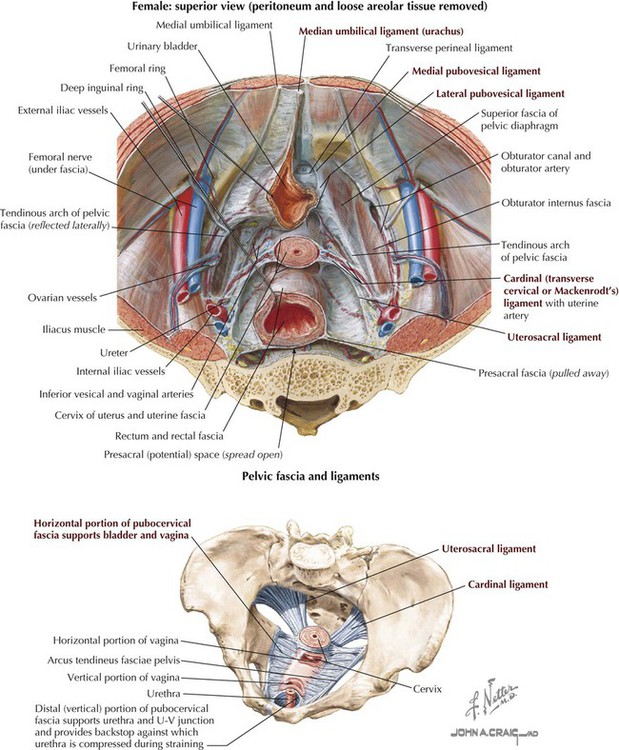
• Median umbilical ligament: midsagittal anterior ligament in both genders that extends to the umbilicus (a remnant of the embryonic urachus).
• Medial pubovesical ligament: connects the bladder to the pubis in both genders.
• Lateral ligament of the bladder (pubovesical): provides lateral support that conveys the superior vesical vessels supplying the bladder in both genders.
• Pubocervical ligaments: fascial condensations that course from the cervix to the anterior pelvic wall, passing on either side of the female bladder.
• Transverse cervical ligaments: provide important posterolateral support of the uterus and upper vagina and convey the uterine vessels; also called cardinal, lateral cervical, or Mackenrodt's ligaments.
• Uterosacral ligaments: fascial condensations that course from the cervix posteriorly to the pelvic walls.
• Rectovaginal septum: fascial condensations between the rectum and vagina.
The same ligaments that support the female urinary bladder also support the male bladder. Males have a condensation called the prostatic fascia that surrounds the anterolateral aspect of the prostate gland, envelops the prostatic venous plexus, and extends posteriorly to envelop the prostatic arteries and nerve plexus (rectoprostatic septum (fascia) or Denonvilliers' fascia; see Fig. 5-9).
The peritoneum of the pelvis forms the following structures (see Figs. 5-7 and 5-9):
• Covers the pelvic viscera in both genders and forms the broad ligament in females.
• Forms the median umbilical (urachus) fold and the medial umbilical folds (remnants of the fetal umbilical arteries) in both genders.
• Forms the vesico-uterine and recto-uterine (pouch of Douglas) pouches in females.
• Forms the rectovesical pouch in males.
• Forms the uterosacral fold in females and the vesicosacral fold in males.
5 Blood Supply
The arterial supply to the pelvis arises from the paired internal iliac arteries, which not only supply the pelvis but also send branches into the perineum, the gluteal region, and the medial thigh. The arteries in the female pelvis are shown in Figure 5-13 and summarized in Table 5-6.
TABLE 5-6
Branches (Divisions) of the Female Pelvic Arteries
| ARTERIAL BRANCH* | COURSE AND STRUCTURES SUPPLIED |
| Common iliac | Divides into external (to thigh) and internal (to pelvis) iliac |
| Internal iliac | Divides into posterior division (P) and anterior division (A) |
| Iliolumbar (P) | To iliacus muscle (iliac artery), psoas, quadratus lumborum, and spine (lumbar artery) |
| Lateral sacral (P) | To piriformis muscle and sacrum (meninges and nerves) |
| Superior gluteal (P) | Between lumbosacral trunk and S1 nerves, through greater sciatic foramen and to gluteal region |
| Inferior gluteal (A) | Between S1 or S2 and S2 or S3 to gluteal region |
| Internal pudendal (A) | To perineal structures through greater sciatic foramen and into lesser sciatic foramen to perineum |
| Umbilical (A) | Gives rise to superior vesical artery to bladder and becomes medial umbilical ligament when it reaches anterior abdominal wall |
| Obturator (A) | Passes into medial thigh via obturator foramen (with obturator nerve) |
| Uterine (A) | Runs over levator ani muscle and ureter to reach uterus (may give rise to vesical arteries) |
| Vaginal (A) | From internal iliac or uterine, passes to vagina |
| Middle rectal (A) | To lower rectum and superior part of anal canal |
| Ovarian | From abdominal aorta, runs in suspensory ligament of ovary |
| Superior rectal | Continuation of inferior mesenteric artery to rectum |
| Median sacral | From aortic bifurcation, unpaired artery to sacrum and coccyx (caudal artery) |

The arteries in the male are similar, except that the uterine, vaginal, and ovarian branches are replaced by arteries to the ductus deferens (from a vesical branch), the prostatic artery (from the inferior vesical artery), and the testicular arteries (from the abdominal aorta). Significant variability exists for these arteries, so they are best identified and named for the structure they supply. Corresponding veins, usually multiple, course with each of these arterial branches and drain into the internal iliac vein directly or into other larger veins. (Multiple connections among veins are common.) Extensive venous plexuses are associated with the bladder, rectum, vagina, uterus, and prostate, referred to as the pelvis plexus of veins. The veins surrounding the rectum form an important portosystemic anastomosis via the superior rectal (portal system) vein and the middle and inferior rectal (caval system) veins (see Figs. 4-26 and 5-19).
Overview of Pelvic and Perineal Arteries
The aorta bifurcates at about the L4 vertebral level into the common iliac artery (1) (right and left branches), which then bifurcates into the internal iliac artery (2) and the external iliac artery (3) at about the L5-S1 intervertebral level. The external iliac artery passes inferiorly to the thigh, where it becomes the femoral artery after passing deep to the inguinal ligament (Fig. 5-14).
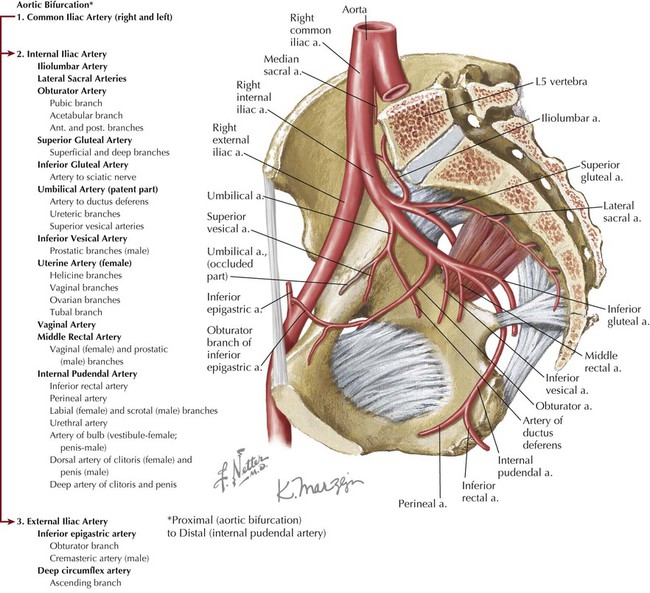
The internal iliac artery (2) provides branches to the sacrum, the obturator artery to the medial compartment of the thigh (adductor muscles of hip), the gluteal arteries to the gluteal muscles, and a partially patent umbilical artery (becomes the medial umbilical ligament as it approaches the anterior abdominal wall). The internal iliac also gives rise to arteries to the urinary bladder (the vesical artery, usually from the umbilical artery), the uterus and vagina in females, and the middle rectal artery to the rectum (with vaginal and prostatic branches, depending on the sex).
The internal pudendal artery passes out the greater sciatic foramen and around the sacrospinous ligament and enters the pudendal canal through the lesser sciatic foramen to pass forward and inferiorly to the perineum. The internal pudendal artery supplies the skin, external genitalia, and muscles of the perineum (anal and urogenital triangle).
Some anatomists divide the branches of the internal iliac artery into anterior and posterior trunks for descriptive purposes. The posterior branches are the iliolumbar, lateral sacral, and superior gluteal arteries; all the other major arteries are from the anterior trunk.
The veins of the pelvis and perineum course with the arteries and generally have the same names. They drain largely back into the internal iliac vein, common iliac vein, inferior vena cava, and then to the heart. Important portosystemic anastomoses occur between the superior rectal vein (from the inferior mesenteric vein of the portal system) and the middle (internal iliac vein) and inferior (internal pudendal vein) rectal veins of the caval system (Fig. 5-19).
6 Lymphatics
Much of the lymphatic drainage of the pelvis parallels the venous drainage and drains into lymph nodes along the internal iliac vessels (Fig. 5-15 and Table 5-7). The major exception is the drainage from the ovaries and the adjacent uterine tubes and upper uterus, and from the testes and scrotal structures, which flows directly back to the aortic (lumbar) nodes of the midabdomen. Because some lymph from the uterus may drain along the round ligament of the uterus to the inguinal nodes, physicians must be aware that uterine cancer could spread to these nodes as well as the external iliac nodes.
TABLE 5-7
| LYMPH NODES | DRAINAGE |
| Superficial inguinal | Receive lymph from perineum (and lower limb and lower abdomen) and deep pelvic viscera and drain lymph to external iliac nodes |
| Deep inguinal | Receive lymph from perineum (and lower limb) and drain lymph to external iliac nodes |
| Internal iliac | Receive lymph from pelvic viscera and drain lymph along iliac nodes, ultimately to reach aortic (lumbar) nodes |
| External iliac | Convey lymph along iliac nodes to reach aortic (lumbar) nodes |
| Gonadal lymphatics | Drain lymph from gonads directly to aortic (lumbar) nodes |

7 Innervation
The skin and skeletal muscle of the pelvis are innervated by the somatic division of the peripheral nervous system. The muscle innervation is reviewed in Table 5-2 and is derived from the ventral rami of the sacral (L4-S4) and coccygeal plexus. Although most of the sacral plexus is involved in innervation of the gluteal muscles and muscles of the lower limb, several small twigs innervate the pelvic musculature (nerve to the obturator internus and nerves to the pelvic diaphragm) and the perineum, which is supplied by the pudendal nerve (S2-S4). Somatic afferent fibers convey pain, touch, and temperature from the skin, skeletal muscle, and joints via nerves from these plexuses to the same relative spinal cord levels.
The smooth muscle and glands of the pelvis are innervated by the autonomic division of the peripheral nervous system via the pelvic splanchnics (S2-S4; parasympathetic) and the lumbar and sacral splanchnics (L1-L2; sympathetic) (Fig. 5-16 and Table 5-8).
TABLE 5-8
| NERVE | INNERVATION |
| Lumbar splanchnics | From L1 to L2 or L3: sympathetics to hypogastric plexus (superior and inferior) to innervate hindgut derivatives and pelvic reproductive viscera |
| Sacral splanchnics | From L1 to L2 or L3: sympathetics to inferior hypogastric plexus that first travel down sympathetic chain before synapsing in plexus |
| Pelvic splanchnics | From S2 to S4: parasympathetics to inferior hypogastric plexus to innervate hindgut derivatives and pelvic reproductive viscera |
| Inferior hypogastric plexus | Plexus of nerves (splanchnics) and ganglia where sympathetic and parasympathetic preganglionic fibers synapse |
| Pudendal nerve | From S2 to S4: somatic nerve that innervates skin and skeletal muscle of pelvic diaphragm and perineum (from sacral plexus) |
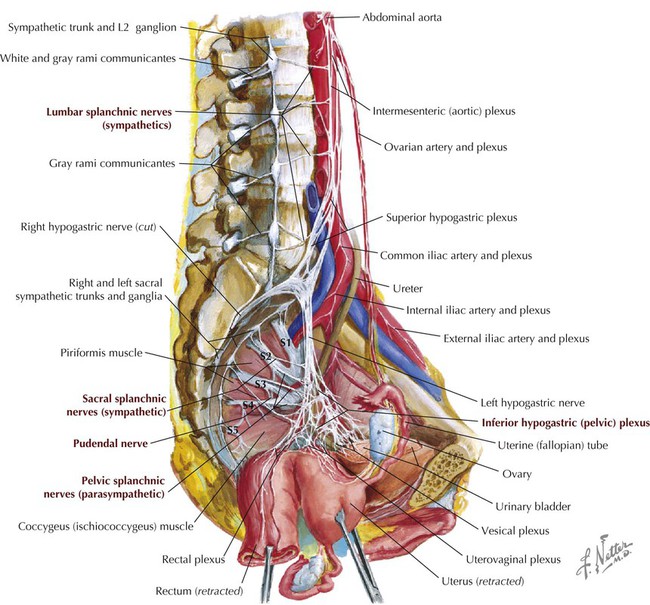
The parasympathetic efferent fibers generally do the following:
• Contract the bladder's detrusor smooth muscle.
• Stimulate engorgement of the erectile tissues.
• Modulate the enteric nervous system's control of the distal bowel (from splenic flexure to rectum).
• Inhibit contraction of both the male internal urethral sphincter for urination and the internal anal sphincter for defecation in both genders.
The sympathetic efferent fibers generally do the following:
• Vasoconstrict and/or maintain vasomotor tone.
• Increase secretion from sweat glands.
• Contract the male internal urethral sphincter and the internal anal sphincters in both genders.
• Through smooth muscle contraction, move the sperm along the male reproductive tract and stimulate secretion from the seminal vesicles and prostate.
• Stimulate secretion from the greater vestibular (Bartholin's) glands in females and the bulbo-urethral (Cowper's) glands in males, along with minor lubricating glands associated with the reproductive tract in both genders.
Visceral afferent fibers convey pelvic sensory information (largely pain) via both the sympathetic fibers (to the upper lumbar spinal cord [L1-L2] or lower thoracic levels [T11-T12]) and parasympathetic fibers (to the S2-S4 levels of the spinal cord).
8 Female Perineum
The perineum is a diamond-shaped region between the thighs and is divided descriptively into an anterior urogenital triangle and a posterior anal triangle (Fig. 5-17). The boundaries of the perineum include the following:

• Ischial tuberosities laterally (lateral margins are demarcated by the ischiopubic rami anteriorly and the sacrotuberous ligaments posteriorly; see Fig. 5-3.)
Anal Triangle (Both Genders)
The key feature of the anal triangle is the anal opening and the external anal sphincter, which has the following attachments (Fig. 5-18):

• Subcutaneous part: just beneath the skin
• Superficial part: attaches to the perineal body and coccyx
Similar to the skin and all the skeletal muscles of the perineum, the external anal sphincter is innervated by the pudendal nerve (S2-S4) (inferior rectal branches; see Fig. 5-23) from the sacral plexus and supplied by the internal pudendal artery (rectal branches), a branch of the internal iliac artery in the pelvis (see Figs. 5-13 and 5-14). The venous drainage of the lower rectum and anal canal provides an important portosystemic anastomosis between the superior rectal vein (portal system) and the median sacral vein and middle and inferior rectal branches (caval system) (Fig. 5-19 and Table 5-9).
TABLE 5-9
Rectal Portosystemic Anastomoses
| VEIN | COURSE AND STRUCTURES DRAINED |
| Superior rectal | Tributary of inferior mesenteric vein (portal system) |
| Middle rectal | Drains into internal iliac, vesical, or uterine (female) veins, draining pelvic diaphragm, rectum, and proximal anal canal |
| Inferior rectal | Drains into internal pudendal vein from external anal sphincter |
| Median sacral | Drains into external iliac vein from sacrum, coccyx, and rectum |

The anal canal and external anal sphincter are flanked on either side by a wedge-shaped fat-filled space called the ischio-anal (ischiorectal) fossa (Fig. 5-20). This space allows for the expansion of the anal canal during defecation and accommodates the fetus during childbirth. The ischio-anal fossa can become infected (e.g., glandular, abrasive lesions, boils), and because the two fossae communicate posterior to the anal canal, the infection can easily spread from side to side or, in extreme cases, burst through the levator ani and infect the pelvis.


Urogenital Triangle
The urogenital triangle is divided into a superficial pouch, containing the external genitalia and associated skeletal muscles, and a deep pouch, largely occupied by the urethrovaginalis–skeletal muscle sphincter complex surrounding the urethra and vaginal apertures. Superior to the deep pouch lies the levator ani muscle, with an intervening anterior extension of the ischio-anal fossae (fat) separating the deep pouch and muscle.
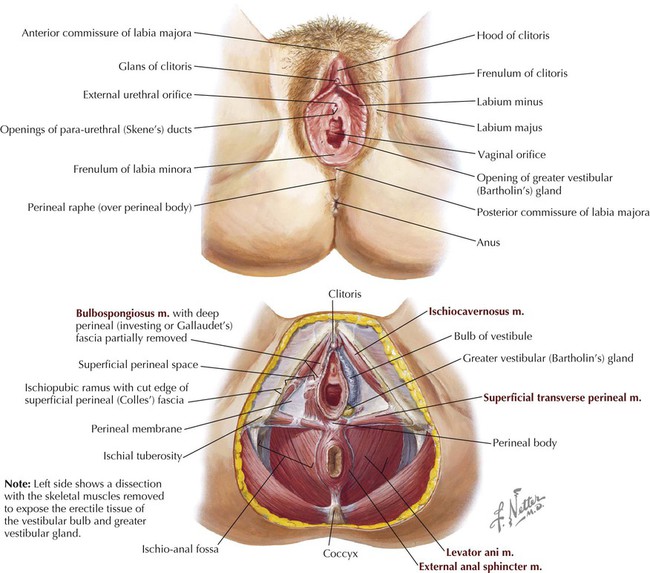
The female external genitalia (vulva) are shown in Figure 5-21 and summarized in Table 5-10.
TABLE 5-10
Features of the Female External Genitalia
| STRUCTURE | CHARACTERISTICS |
| Mons pubis | Anterior fatty eminence overlying pubic symphysis |
| Anterior labial commissure | Site where two labia majora meet anteriorly |
| Labia majora | Folds of pigmented skin, mainly fat and sebaceous glands; in the adult, covered with pubic hair externally but smooth and pink on internal aspect |
| Clitoris | Erectile tissue, distinguished by midline glans covered with prepuce (foreskin), body, and two crura (corpora cavernosa) that extend along ischiopubic rami, and covered by ischiocavernosus muscles |
| Labia minora | Fat-free hairless pink skin folds that contain some erectile tissue; course anteriorly to form frenulum and prepuce of clitoris; posteriorly, unite to form frenulum of labia minora (fourchette) |
| Vestibule | Space surrounded by labia minora that contains openings of urethra, vagina, and vestibular glands |
| Greater vestibular glands | Paired mucous glands lying posterior to bulbs of vestibule that produce secretions during arousal |
| Bulbs of vestibule | Paired erectile tissues lying deep and lateral to labia minora that flank vaginal and urethral openings and extend anteriorly to form small connection to glans of clitoris; covered by bulbospongiosus skeletal muscle |
| Posterior labial commissure | Site where two labia majora meet posteriorly; overlies perineal body |
Clinical Focus 5-20 Episiotomy
Occasionally, if there is danger of tearing of the perineal body during childbirth, the physician may perform an incision called an episiotomy to enlarge the vaginal opening to accommodate the head of the fetus. The incision is easier to repair and heals better than a tear. Episiotomies usually are either directly in the midline through the perineal body or posterolateral, to avoid the perineal body.

The perineal body (central tendon of the perineum) is an important fibromuscular support region lying just beneath the skin midway between the two ischial tuberosities and an important attachment point for the perineal muscles, especially the urethrovaginalis complex in women, and the levator ani superiorly (see Fig. 5-21).
The deep perineal pouch contains the following (Fig. 5-22):
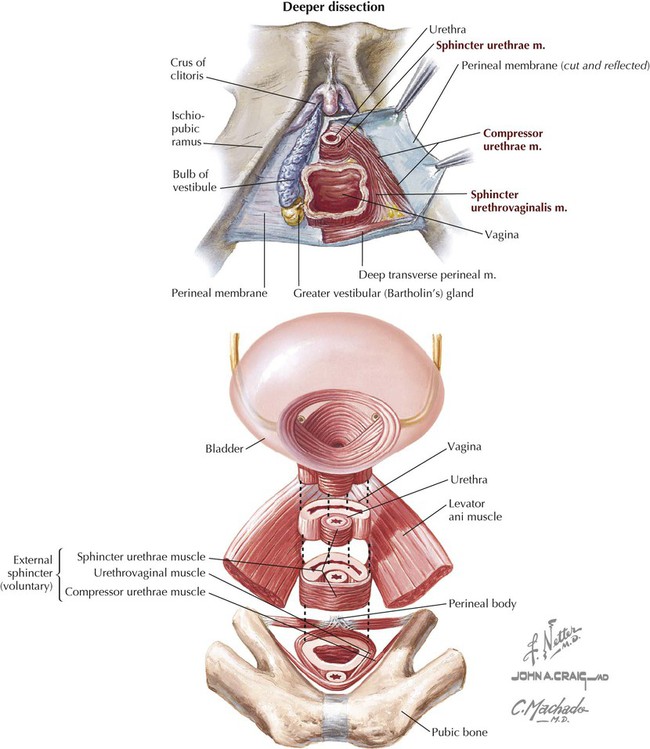
• Urethra: extends from the bladder, runs through the deep pouch, and opens into the vestibule.
• Vagina: distal portion passes through the deep pouch and opens into the vestibule.
• External urethral sphincter: skeletal muscle sphincter
• Compressor urethrae: two thin skeletal muscle bands that extend from the ischiopubic rami and fuse in the midline around the anterior aspect of the urethra.
• Sphincter urethrovaginalis muscle: extends from the perineal body around the lateral sides of the vagina and fuses in the midline around the anterior aspect of the urethra.
• Deep transversus perineal muscles: extend from the ischial tuberosities and rami to the perineal body; stabilize the perineal body.
These structures, along with their respective neurovascular bundles, lie between the perineal membrane (thick fascial sheath) and the fascia covering the inferior aspect of the levator ani muscle. The neurovascular components include the following (Fig. 5-23):
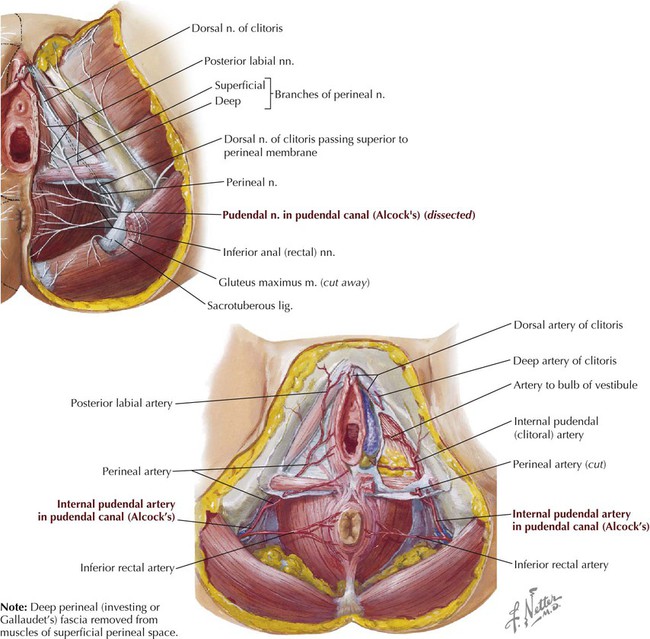
• Pudendal nerve: passes out the greater sciatic foramen around the sacrospinous ligament and into the lesser sciatic foramen to enter the pudendal (Alcock's) canal; represents the somatic innervation (S2-S4) of the skin and skeletal muscles of the perineum; includes the inferior rectal (anal), perineal, labial, and dorsal clitoral branches.
• Internal pudendal artery: arises from the internal iliac artery, passes out the greater sciatic foramen around the sacrospinous ligament and into the lesser sciatic foramen to enter the pudendal (Alcock's) canal, and distributes to the perineum as the inferior rectal, perineal, labial, artery of the bulb, and dorsal clitoral branches.
Clinical Focus 5-21 Sexually Transmitted Diseases
Human papillomavirus (HPV) and Chlamydia trachomatis infections are the two most common STDs in the United States. HPV infections (>90% benign) are characterized in both genders by warty lesions caused most often by serotypes 6 and 11. The virus is typically spread by skin-to-skin contact; the incubation period is 3 weeks to 8 months. HPV is highly associated with cervical cancer in women. Chlamydial infection is the most common bacterial STD, with antibodies present in up to 40% of all sexually active women (which suggests prior infection). Infected structures include the urethra, cervix, greater vestibular glands, and uterine tubes in females and the urethra, epididymis, and prostate in males.

9 Male Perineum
The boundaries of the perineum and the anal triangle in both genders are discussed in the previous section; this section focuses on the male urogenital triangle. The urogenital triangle is divided into a superficial pouch containing the external genitalia and associated skeletal muscles and a deep pouch largely occupied by the external urethral sphincter surrounding the membranous urethra.
The male external genitalia are shown in Figure 5-24 and summarized in Table 5-11.
TABLE 5-11
Features of the Male External Genitalia
| STRUCTURE | CHARACTERISTICS |
| Bulb of penis | Erectile tissue anchored to perineal membrane; proximal part of corpus spongiosum; covered by bulbospongiosus skeletal muscle |
| Crura of penis | Paired erectile tissues attached to pubic arch that form proximal part of corpora cavernosa of penis; covered by ischiocavernosus skeletal muscles |
| Superficial transverse perineal muscle | Thin skeletal muscle extending from ischial tuberosity to perineal body; stabilizes perineal body |
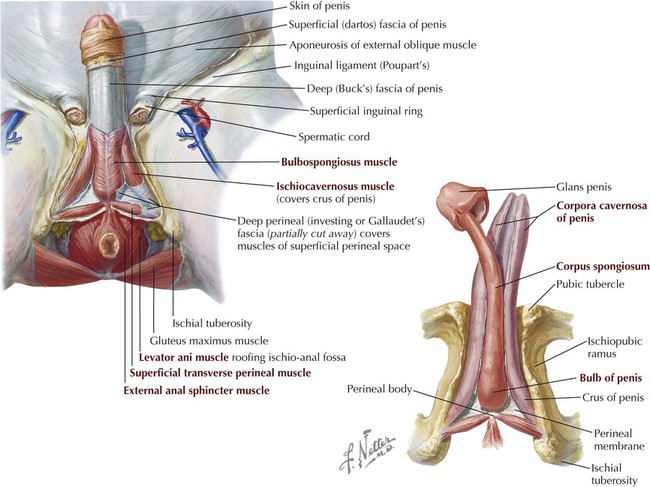
The bulb and crura form the root of the penis, whereas the corpus spongiosum and the two corpora cavernosa compose the shaft of the penis. They are bound tightly together by the investing deep (Buck's) fascia of the penis and a superficial (dartos) fascia of the penis.
The superficial fascia (subcutaneous tissue) of the perineum includes a fatty and membranous layer (Colles' fascia) similar to the anterior abdominal wall (Fig. 5-25). The fatty layer contributes to the labia majora and mons pubis in women but is minimal in men. In the male the membranous layer of the superficial fascia (called Scarpa's fascia on the abdominal wall but Colles' fascia in the perineum) is continuous with the dartos (smooth muscle) fascia of the penis and scrotum and envelops the superficial perineal pouch, thus providing a potential conduit for fluids or infections from the superficial pouch to the lower abdominal wall. The deep perineal (Gallaudet's) fascia invests the ischiocavernosus, bulbospongiosus, and superficial transverse perineal muscles in both genders and is continuous with the deep (Buck's) fascia of the penis and the deep investing fascia of the external abdominal oblique muscle and rectus sheath (see Fig. 5-24).

Features of the penis are summarized in Table 5-12 and illustrated in Figure 5-26.
TABLE 5-12
| STRUCTURE | CHARACTERISTICS |
| Root of penis | Composed of bulb (proximal part of corpus spongiosum) and two crura (proximal part of corpora cavernosa) |
| Body of penis | Covered by skin, dartos fascia, and deep (Buck's) fascia of penis, which envelops the corpora cavernosa and corpus spongiosum, which contains spongy urethra |
| Glans penis | Expanded distal end of corpus spongiosum where spongy urethra expands (navicular fossa) and opens externally (external urethral meatus) |
| Prepuce (foreskin) | Thin, double layer of skin that extends over most of glans penis* |
| Suspensory ligament | Deep fascia that extends from dorsum of penis to pubic symphysis |
| Fundiform ligament | Subcutaneous tissue that extends from dartos fascia superiorly to midline linea alba (see Fig. 5-9) |

Erection of the penis (and clitoris in the female) and ejaculation involve the following sequence of events:
1. Friction and sexual stimulation evoke the excitation of parasympathetic fibers (pelvic splanchnics S2-S4), which leads to relaxation of the cavernous vessels and engorgement of the erectile tissue with blood.
2. Sympathetic fibers then initiate contraction of the smooth muscle of the epididymal ducts, ductus deferens, seminal vesicles, and prostate, in that order.
3. Sperm and the seminal and prostatic secretions enter the prostatic urethra and combine with secretions of the bulbo-urethral and penile urethral glands (semen). (The seminal vesicles provide 70% of the seminal fluid volume and produce a viscous alkaline fluid that nourishes and protects the sperm from the acidic environment of the vaginal tract.)
4. Under sympathetic stimulation (L1-L2), the internal urethral sphincter contracts to prevent ejaculation into the urinary bladder. Through rhythmic contractions of the bulbospongiosus muscle and somatic stimulation from the pudendal nerve, the semen moves along the spongy urethra with help from parasympathetic stimulation of urethral smooth muscle and is ejaculated (orgasm).
Clinical Focus 5-22 Urethral Trauma in the Male
Although rare, direct trauma to the corpora cavernosa can occur. Rupture of the thick tunica albuginea usually involves the deep fascia of the penis (Buck's fascia), and blood can extravasate quickly, causing penile swelling. Urethral rupture is more common and involves one of three mechanisms:
• External trauma or a penetrating injury
• Internal injury (caused by a catheter, instrument, or foreign body)
• Spontaneous rupture (caused by increased intraurethral pressure or periurethral inflammation)

Clinical Focus 5-23 Urine Extravasation in the Male
Rupture of the male urethra can lead to urine extravasation into various pelvic or perineal spaces that are largely limited by the fascial planes.

Clinical Focus 5-24 Erectile Dysfunction
Erectile dysfunction (ED) is an inability to achieve and maintain penile erection sufficient for sexual intercourse. Its occurrence increases with age, and some of the probable causes are illustrated. Normal erectile function occurs when a sexual stimulus causes the release of nitric oxide from nerve endings and endothelial cells of the corpora cavernosa, thus relaxing the smooth muscle tone of the vessels and increasing blood flow into the erectile tissues. As the erectile tissue becomes engorged with blood, it compresses the veins in the tunica albuginea so that the blood remains in the cavernous bodies. The available drugs to treat ED aid in relaxing the smooth muscle of the blood vessels of the erectile tissues. Erectile dysfunction can also occur from damage to the nerves innervating the perineum (e.g., a complication of prostatic surgery). Afferent impulses conveying stimulation/arousal sensations are conveyed by the pudendal nerve (S2-S4, somatic fibers), whereas the autonomic efferent innervation of the cavernous vasculature is via the pelvic splanchnics (S2-S4, parasympathetic fibers).

The deep perineal space in males includes the following (Fig. 5-27):

• Membranous urethra: a continuation of the prostatic urethra.
• Deep transversus perineal muscles: extend from the ischial tuberosities and rami to the perineal body; stabilize the perineal body.
• Bulbo-urethral glands: their ducts pass from the deep pouch to enter the proximal part of the spongy urethra; provide a mucus-like secretion that lubricates the spongy urethra.
• External urethral sphincter: skeletal muscle that encircles the membranous urethra, is under voluntary control (via the pudendal nerve), and extends superiorly over the anterior aspect of the prostate gland but does not possess sphincter action on the gland.
These structures, along with their respective neurovascular bundles, lie between the perineal membrane (thick fascial sheath) and the fascia covering the inferior aspect of the levator ani muscle. The neurovascular components include the following:
• Pudendal nerve: passes out the greater sciatic foramen with the internal pudendal vessels, around the sacrospinous ligament, and into the lesser sciatic foramen to enter the pudendal (Alcock's) canal; provides the somatic innervation (S2-S4) of the skin and skeletal muscles of the perineum and includes the inferior rectal (anal), perineal, scrotal, and dorsal nerves of the penis.
• Internal pudendal artery: arises from the internal iliac artery; passes out the greater sciatic foramen with the pudendal nerve, around the sacrospinous ligament, and into the lesser sciatic foramen to enter the pudendal (Alcock's) canal and distribute to the perineum as the inferior rectal, perineal, scrotal, and dorsal arteries of the penis as well as the artery of the bulb.
10 Embryology
Development of the Reproductive Organs
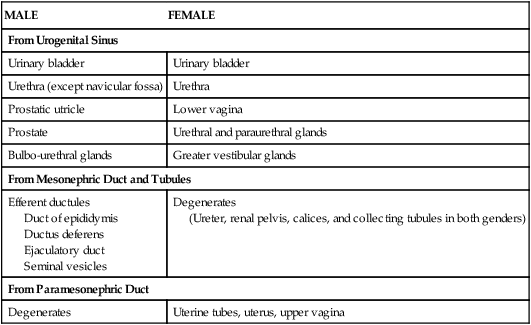
The reproductive systems of the female and male develop from undifferentiated primordia and follow the sexual differentiation of each gender based on the genetic makeup of the embryo (XX for females and XY for males). In females, mesonephric ducts degenerate while the paramesonephric ducts develop into the uterine tubes, uterus, and upper portion of the vagina (Fig. 5-28 and Table 5-13). In males the mesonephric ducts persist and become the ductus deferens, ejaculatory ducts, and seminal vesicles.
TABLE 5-13
Derivatives of the Urogenital System
| MALE | FEMALE |
| From Urogenital Sinus | |
| Urinary bladder | Urinary bladder |
| Urethra (except navicular fossa) | Urethra |
| Prostatic utricle | Lower vagina |
| Prostate | Urethral and paraurethral glands |
| Bulbo-urethral glands | Greater vestibular glands |
| From Mesonephric Duct and Tubules | |
| Efferent ductules Duct of epididymis Ductus deferens Ejaculatory duct Seminal vesicles |
Degenerates (Ureter, renal pelvis, calices, and collecting tubules in both genders) |
| From Paramesonephric Duct | |
| Degenerates | Uterine tubes, uterus, upper vagina |

Development of the External Genitalia
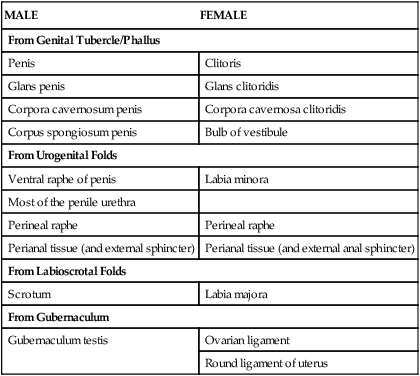
The female and male external genitalia develop from the genital tubercle (the phallic structures), paired urogenital folds, and labioscrotal folds (Fig. 5-29 and Table 5-14). Initially these tissues are undifferentiated, but after 10 weeks recognizable external genital features associated with each sex begin to form.
TABLE 5-14
Homologues of the External Genitalia
| MALE | FEMALE |
| From Genital Tubercle/Phallus | |
| Penis | Clitoris |
| Glans penis | Glans clitoridis |
| Corpora cavernosum penis | Corpora cavernosa clitoridis |
| Corpus spongiosum penis | Bulb of vestibule |
| From Urogenital Folds | |
| Ventral raphe of penis | Labia minora |
| Most of the penile urethra | |
| Perineal raphe | Perineal raphe |
| Perianal tissue (and external sphincter) | Perianal tissue (and external anal sphincter) |
| From Labioscrotal Folds | |
| Scrotum | Labia majora |
| From Gubernaculum | |
| Gubernaculum testis | Ovarian ligament |
| Round ligament of uterus | |

Clinical Focus 5-25 Hypospadias and Epispadias
Hypospadias and epispadias are congenital anomalies of the penis. Hypospadias is much more common (1 in 300 male births) and is characterized by failure of fusion of the urogenital folds, which normally seal the penile (spongy) urethra within the penis. The defect occurs on the ventral aspect of the penis (corpus spongiosum). Hypospadias may be associated with inguinal hernias and undescended testes. Epispadias is rare (1 in 30,000 male births) and is characterized by a urethral orifice on the dorsal aspect of the penis.

Clinical Focus 5-26 Uterine Anomalies
Incomplete fusion of the distal paramesonephric (müllerian) ducts can lead to septation of the uterus or partial or complete duplication of the uterus (bicornuate uterus). The prevalence is up to 3% for septate uterine anomalies but only about 0.1% for bicornuate anomalies. If only one paramesonephric duct persists and develops, a unicornuate uterus results. These conditions seem to be transmitted by a polygenic or multifactorial pattern and carry a higher risk for recurrent spontaneous abortions (15-25%), premature labor, uterine pain, breech or transverse deliveries, and dysmenorrhea.

Clinical Focus 5-27 Ovarian Tumors
Most malignancies arise from the surface epithelial stroma (85-90%). Germ cells and the sex cord stroma account for the remaining malignancies. About 50% of tumors in women over age 50 are malignant. Risk factors include a family history of ovarian cancer, high-fat diet, age, nulliparity, early menarche, late menopause, white race, and higher socioeconomic status.
