Cardiac Arrhythmias
The polysomnogram (PSG) provides a good opportunity to evaluate cardiac rhythms. Although medically threatening abnormalities are seen less frequently today than in the past, sleep specialists and technicians must be able to recognize the basic abnormalities. This chapter highlights some of the cardiac arrhythmias seen during overnight PSG recording (Figs. 8.1 to 8.13).
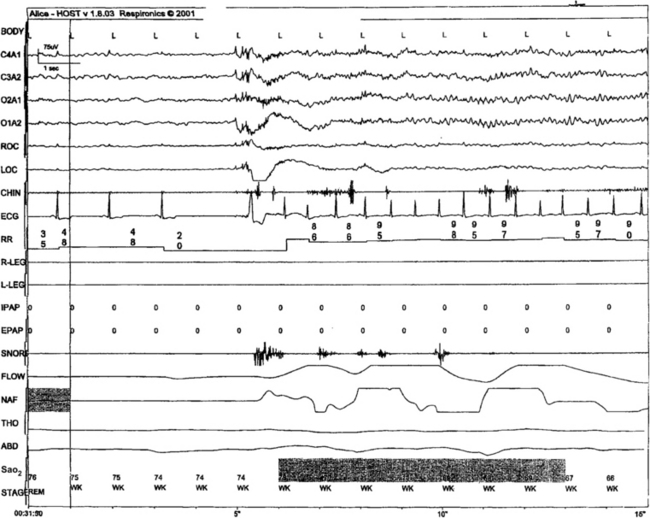
FIGURE 8.1 Severe disease-related bradyarrhythmia in rapid eye movement (REM) sleep.
A 56-year-old man with severe daytime sleepiness. The left side of the snapshot shows a heart rate less than 50 beats/min, the termination of an apnea, and severe hypoxia (saturation in the mid-70s). Just before the arousal there is a 4-second period with no electrocardiographic (ECG) rhythm (possible sinus arrest or sinoatrial exit block), followed by a ventricular escape, and postarousal tachycardia, with a near doubling of heart rate. The ECG R-wave amplitude also shows fluctuations that track respiratory effort: This ECG-derived respiration signal is secondary to changes in the cardiac axis generated by positional variation of the heart in the thoracic cavity associated with respiration.
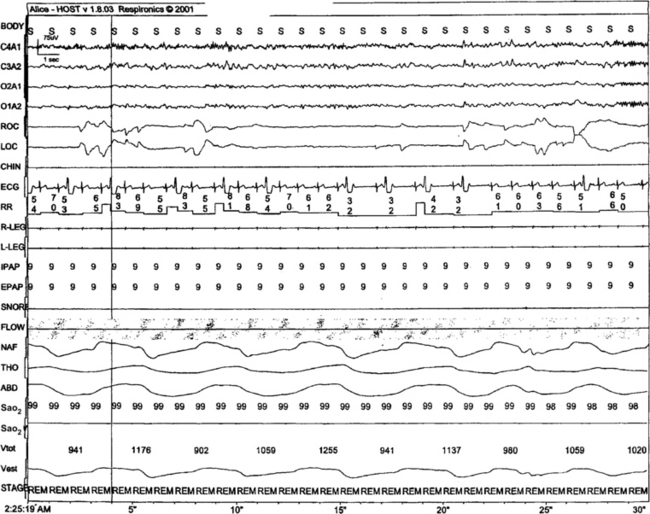
FIGURE 8.2 Ventricular ectopy in rapid eye movement (REM) sleep.
Bigeminy and trigeminy are noted in this 26-year-old woman who presented with nonhypoxic obstructive sleep-disordered breathing. This finding was not seen in non-REM (NREM) sleep. There was excessive use of caffeine (four to five large cups of strong coffee across the day). The patient has no palpitations during the day or night.
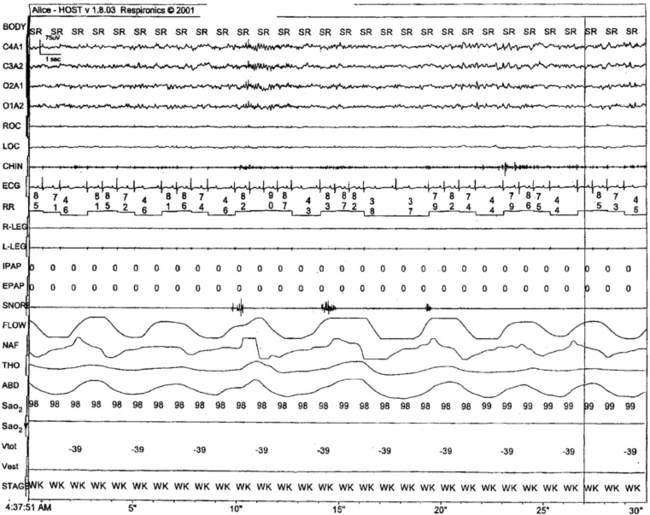
FIGURE 8.3 Second-degree heart block, Wenckebach.
Progressive increase in PR interval preceding dropped beats in a 48-year-old patient with delayed sleep phase disorder, seen unchanged during wake and sleep. This is an innocent arrhythmia and requires no treatment.
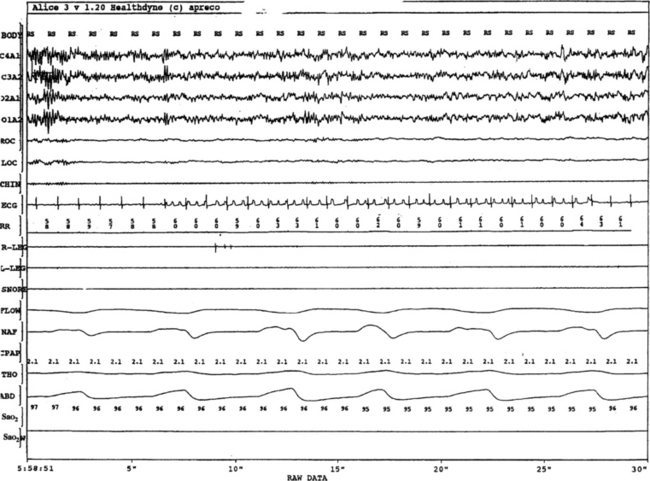
FIGURE 8.4 Supraventricular tachycardia.
Atrial tachycardia with varying block or a run of atrial flutter with varying block. The abrupt change in P-wave morphologic characteristics is not associated with any change in QRS morphologic characteristics. The ability of a single ECG channel in precisely determining the origin of rhythms can be limited. This patient was not on any medication such as digitalis.
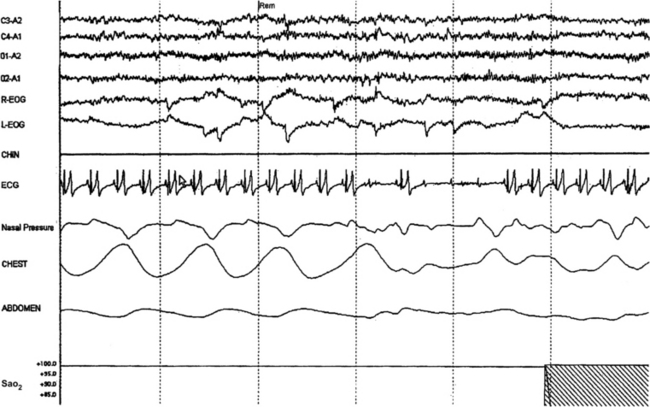
FIGURE 8.5 Bradyarrhythmia with intermittent complete heart block in rapid eye movement sleep in a 26-year-old asymptomatic man who presented for the evaluation of snoring.
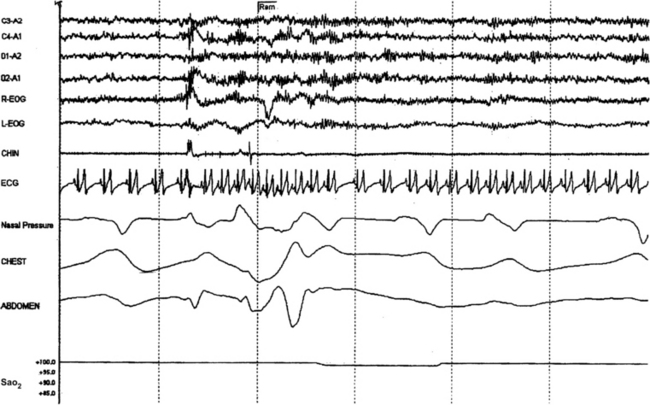
FIGURE 8.6 Postarousal tachycardia.
A 36-year-old woman presents for the evaluation of excessive sleepiness in the setting of refractory depression. This pattern of postarousal bursts of heart rate increase was noted throughout the study. Such cyclic variations in heart rate have been used to develop ECG-based screening tools for sleep-disordered breathing. One disadvantage of such tools is that severity information cannot be assessed from the degree of heart rate change, and some patients with the worst disease (e.g., heart failure) may show very little RR variability.
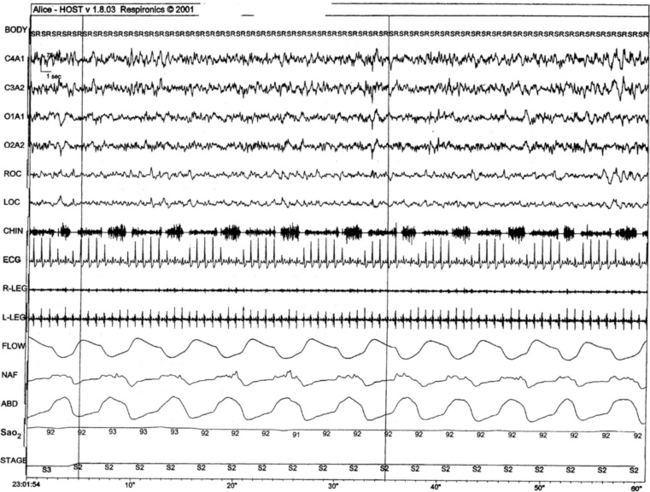
FIGURE 8.7 ECG-derived respiration signal.
Cyclic variation in RR amplitude (rather than interval) induced by respiratory-related fluctuations in cardiac positions. This signal has also been evaluated as a noninvasive ECG-derived method to assess sleep respiration. The disadvantages are similar to RR variability—it is rarely as prominent as in this sample.
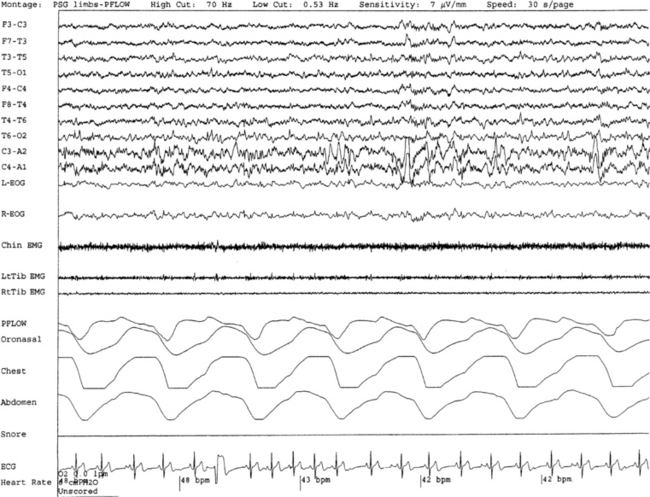
FIGURE 8.8 Ventricular premature contractions.
A 30-second epoch from an overnight polysomnographic study of a 40-year-old woman with a history of restless legs syndrome reveals the presence of ventricular ectopic beats. The patient reported occasional palpitations. This phenomenon may be rate dependent, and a faster heart rate may not be associated with the ventricular ectopic beats. Sinus arrhythmia is also noted.
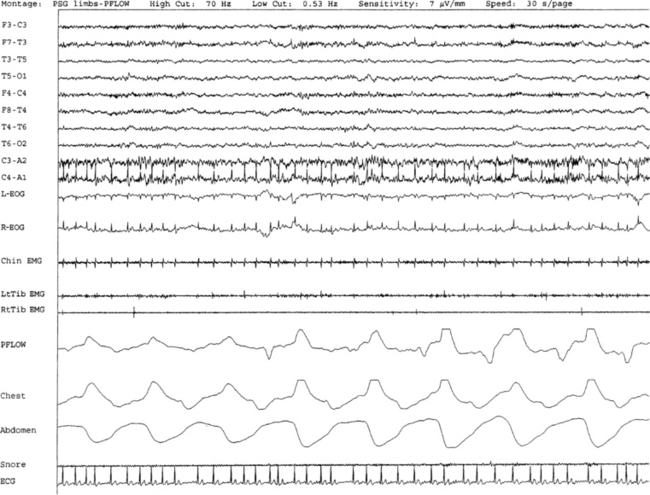
FIGURE 8.9 Atrial fibrillation.
A 47-year-old man with a history of atrial fibrillation was referred for evaluation of sleep apnea. A 30-second epoch of rapid eye movement sleep from an overnight polysomnogram demonstrates the presence of atrial fibrillation. The association of sleep apnea and recurrence/triggering of atrial fibrillation has been reported.
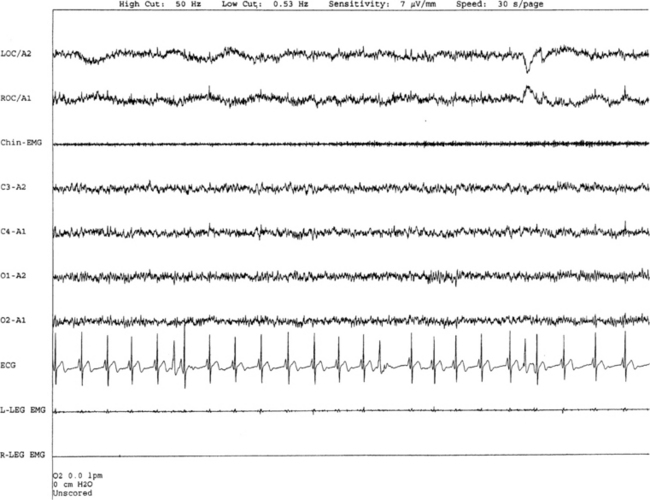
FIGURE 8.10 Aberrant conduction.
A 51-year-old woman was referred for the evaluation of sleep apnea. A 30-second epoch from the polysomnogram shows premature ventricular complexes with slight widening of the QRS but maintained axis. This may be an aberrant beat secondary to a junctional ectopic beat.
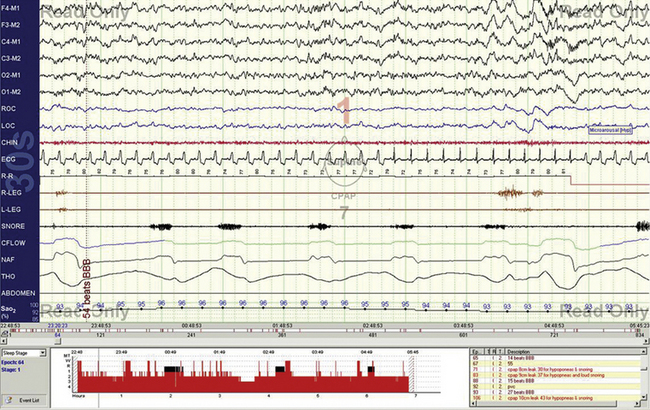
FIGURE 8.11 A 30-second epoch during N2 sleep showing intermittent bundle branch block.
A 68-year-old woman with fragmented nocturnal sleep, reflux esophagitis, and stable ischemic heart disease (two stents, remote anterior myocardial infarction). During the polysomnogram, intermittent QRS complex widening is noted, while the PR interval is unchanged. Note respiratory flow limitation and respiratory arousal. Left versus right bundle branch block cannot be differentiated on the single ECG channel.
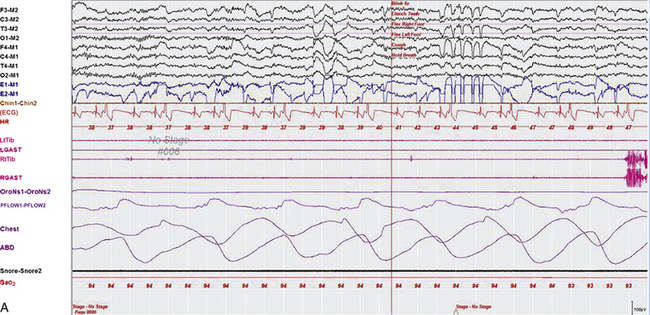
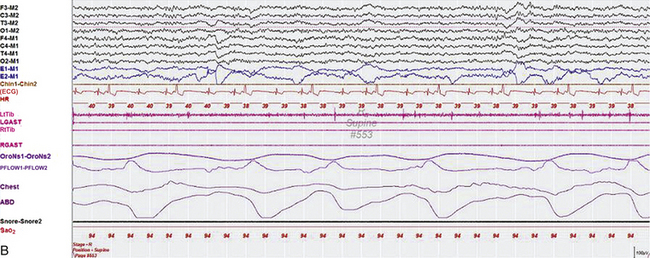
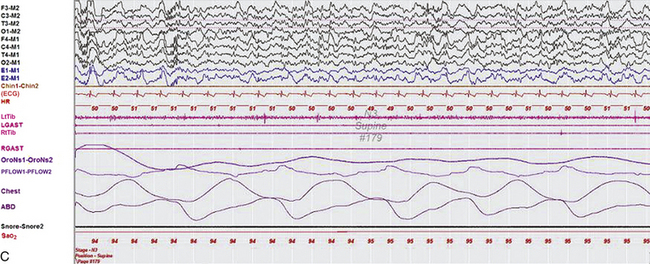
FIGURE 8.12 Snapshots from overnight polysomnogram (PSG) in a 24-year-old man with idiopathic cardiomyopathy presenting with dizziness and palpitations. The PSG showed predominantly central sleep apnea (apnea index of 17.4/hr), unrelated to frequent ventricular trigeminy present in wakefulness (A) and rapid eye movement (REM) sleep (B) but absent in non-REM sleep (C). This is an example of antiarrhythmic effect of sleep on ventricular ectopy. Top eight channels, Electroencephalogram (international nomenclature); E1-M1 and E2-M1, electro-oculograms of left (E1) and right (E2) eyes referred to left mastoid (M1); Chin1-Chin2, mentalis muscle electromyogram (EMG); ECG, electrocardiogram; HR, heart rate; LtTib and RtTib, left and right tibialis anterior muscle EMG; LGAST and RGAST, left and right gastrocnemius muscle EMG; OroNs1-OroNs2 and PFLOW1-PFLOW2, air flow by thermistor and nasal pressure transducer; Chest and ABD, effort channels; Sao2, arterial oxygen saturation by finger oximetry.
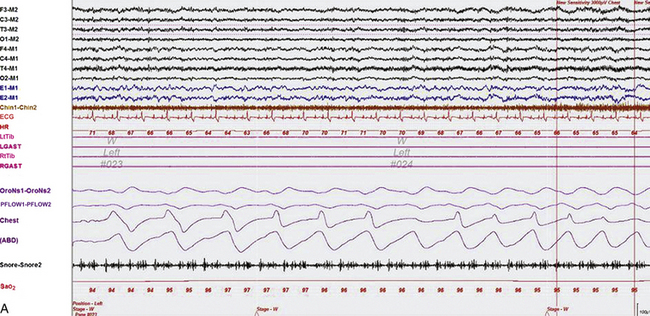
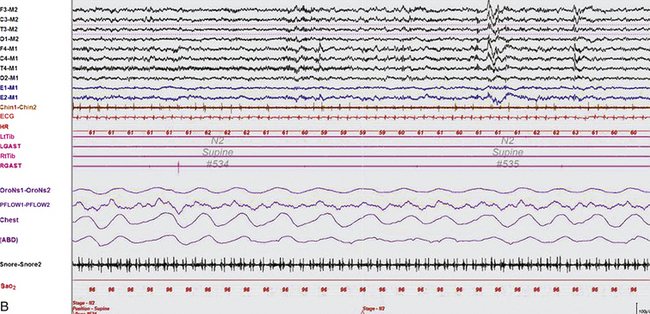
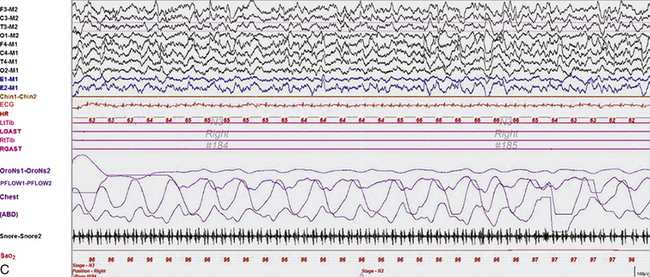
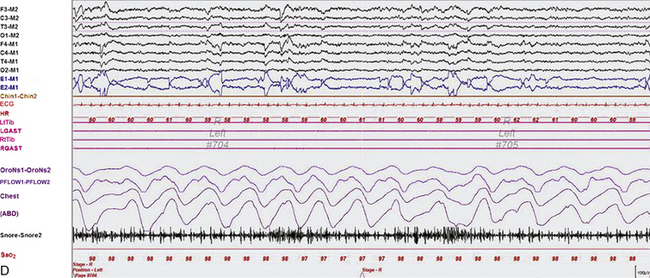
FIGURE 8.13 Excerpts from an overnight polysomnogram (PSG) tracing recorded in a 48-year-old man with restless legs syndrome (Willis-Ekbom disease), depression, and snoring. The PSG showed no evidence of sleep apnea but did show ventricular trigeminy with occasional bigeminy and quadrigeminy in wakefulness (A) and beginning of N2, but those arrhythmias are absent in most of N2 (B), all of N3 (C), and rapid eye movement (D) sleep. These ventricular premature contractions are seen frequently during the first half of the night but are absent in the last half of the night even during wakefulness. This is another example of antiarrhythmic effect of sleep and possibly also a circadian effect on ventricular ectopy. Montage design: same as in Figure 8.12.